 Xiao Zhou
Xiao Zhou Xiaohu Zhang3
Xiaohu Zhang3 Paolo Santi
Paolo Santi
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 03 August 2023
Sec. Public Health Policy
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1198973
This article is part of the Research TopicThe Impact of Non-Pharmaceutical Interventions (NPIs) on Communicable DiseasesView all 9 articles
Given that the effectiveness of COVID-19 vaccines and other therapies is greatly limited by the continuously emerging variants, non-pharmaceutical interventions have been adopted as primary control strategies in the global fight against the COVID-19 pandemic. However, implementing strict interventions over extended periods of time is inevitably hurting the economy. Many countries are faced with the dilemma of how to take appropriate policy actions for socio-economic recovery while curbing the further spread of COVID-19. With an aim to solve this multi-objective decision-making problem, we investigate the underlying temporal dynamics and associations between policies, mobility patterns, and virus transmission through vector autoregressive models and the Toda-Yamamoto Granger causality test. Our findings reveal the presence of temporal lagged effects and Granger causality relationships among various transmission and human mobility variables. We further assess the effectiveness of existing COVID-19 control measures and explore potential optimal strategies that strike a balance between public health and socio-economic recovery for individual states in the U.S. by employing the Pareto optimality and genetic algorithms. The results highlight the joint power of the state of emergency declaration, wearing face masks, and the closure of bars, and emphasize the necessity of pursuing tailor-made strategies for different states and phases of epidemiological transmission. Our framework enables policymakers to create more refined designs of COVID-19 strategies and can be extended to other countries regarding best practices in pandemic response.
Since the coronavirus disease 2019 (COVID-19) was initially detected in December 2019, a novel coronavirus designated as the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has rapidly spread across the world and led to a global pandemic (1). Despite increasingly more people getting vaccinated every single day, the world is still struggling to combat the emerging more contagious COVID-19 variants and has witnessed wave after wave of the pandemic here and there. To contain the COVID-19 pandemic, non-pharmaceutical interventions (NPIs) have been widely used as key weapons in some countries that were impacted heavily early on with satisfying effects (2). For instance, the world's first stringent COVID-19 lockdown sparked in Wuhan, the original epicenter of the pandemic. Specifically, China implemented a 76-day travel ban to and from the city and initiated nationally coordinated measures to address the pandemic's impact until the first wave of the pandemic was effectively contained in the country (3). Singapore is another country that adopted aggressive strategies and maintained a low casualty rate (0.15%) compared to the global average (1.38%) (4).
Besides making striking achievements in real-world settings, the effectiveness of COVID-19 NPIs has also been extensively studied in the literature. Among them, a large body of research was targeted at the epidemiological implications of NPIs. Utilizing compartmental models, scholars simulated and predicted the effects of NPIs on multiple epidemic indicators, including infections (2, 3, 5–10), deaths (2, 7–9, 11), the reproduction number (2, 3, 8, 12), and demand for hospital services (5, 9). Touching on similar themes, another line of research focused more on quantifying the effects of NPIs on mobility (13–15) and explored the relationship between human movements and COVID-19 transmission (6, 16–18). Apart from characterizing the unfolding of the pandemic from an epidemiological perspective, there are also studies investigating the impact of NPIs from various angles covering economic contraction (19–22), social issues (23, 24), and mental health (25–28). Adopting a multi-objective perspective, some studies have concentrated on optimizing the socio-economic cost-effectiveness of pandemic mitigation strategies in different countries (29–31). However, these studies did not address the question from the perspective of human mobility.
Some key findings derived from the current state of knowledge can be summarized as follows: (1) Implementing appropriate NPIs is crucial in curbing the spread of the virus (2, 17, 18); (2) The effectiveness of individual interventions alone is often limited, necessitating the combined use of multiple NPIs (7, 32–34); (3) The impact of NPIs on disease burden exhibits nonlinearity (35); (4) Fixed NPI strategies may be less effective compared to those with time-varying adjustment mechanisms (36); and (5) There is an interplay between NPIs and vaccination strategies, particularly concerning highly transmissible variants of concern. Hence, optimizing and tailoring NPIs holds strong potential for reducing both transmission and the clinical burden of the disease.
The encouraging precedents and research basis above demonstrate the role that NPIs can play in controlling the COVID-19 and offer valuable references for other affected regions to handle the spiraling outbreak. However, as time goes by, the situation has become further complicated and highlighted some limitations of the current literature. First, the emphasis of many previous studies is on the pandemic simulation modeling of COVID-19 for more accurate forecasts without a thorough discussion of the relationships between NPIs, human mobility, and virus transmission that are deeply intertwined. In addition, given that the core concern of handling the ongoing COVID-19 pandemic has shifted from containing its spread to restoring the social and economic order in the new normal from a long-term perspective, particular attention should be paid to multi-objective thinking in the design of policy strategies. Moreover, most of the above-mentioned successes were achieved by imposing harsh measures at the beginning of the pandemic, still, opinions are divided sharply on how to devise optimal policy frameworks of NPIs when the population are partly vaccinated against the COVID-19 among different countries.
To contribute in this direction, we choose the U.S. as the focus in the study due to its decentralized decision-making system, which leads to the implementation and enforcement of NPIs highly variable in both time and space across the country with various circumstances for discussion. Using the COVID-19 policy dataset along with epidemiological and mobility data aggregated at the state level, we propose a methodological framework to quantify the underlying relationships between mobility and key measures of population-level transmission in the context of the COVID-19 pandemic both before and after the vaccines became available. We further evaluate the effectiveness of the current combinations of NPIs applied in each state and identify new optimal strategies that can well balance the public health and socio-economic impacts in the fight against COVID-19. Finally, we investigate the similarities and differences across states and phases to provide new insights into the spatio-temporal dynamics for pandemic control. The results of this study provide valuable insights for policymakers to gain a deeper understanding of the ever-changing landscape of the pandemic, enabling them to identify more effective and adaptable solutions that can respond to evolving needs and circumstances.
To gain a comprehensive understanding of each state government's response to COVID-19, we utilize the COVID-19 U.S. State Policy Database (37). This database enables us to consider nine prominent NPIs, namely: Declaration of a state of emergency (P1), Mandatory face mask usage in workplaces (P2), Closure of child care facilities (P3), Closure of restaurants (P4), Closure of movie theaters (P5), Closure of non-essential businesses (P6), Implementation of stay-at-home orders (P7), Closure of bars (P8), and Closure of gyms (P9). The temporal and geographical adoption of these policy responses across U.S. states is visually presented in Figure 1. This work covers the study period spanning from February 24, 2020, to August 18, 2021. We further divide the observation period into two main phases according to when the lockdown restrictions and COVID-19 vaccine distribution started in the country. Some general patterns we find include: (1) most states rolled out the strictest lockdown measures in April 2020 to fight against the first wave and gradually rolled back the restrictions as the curve of infections started to flatten; (2) to control the subsequent waves in late June and mid-November 2020, NPIs were reimplemented, however, the number of states participated is much smaller than previously and; (3) since the COVID-19 vaccines were administered, the NPIs were gradually lifted in most states.
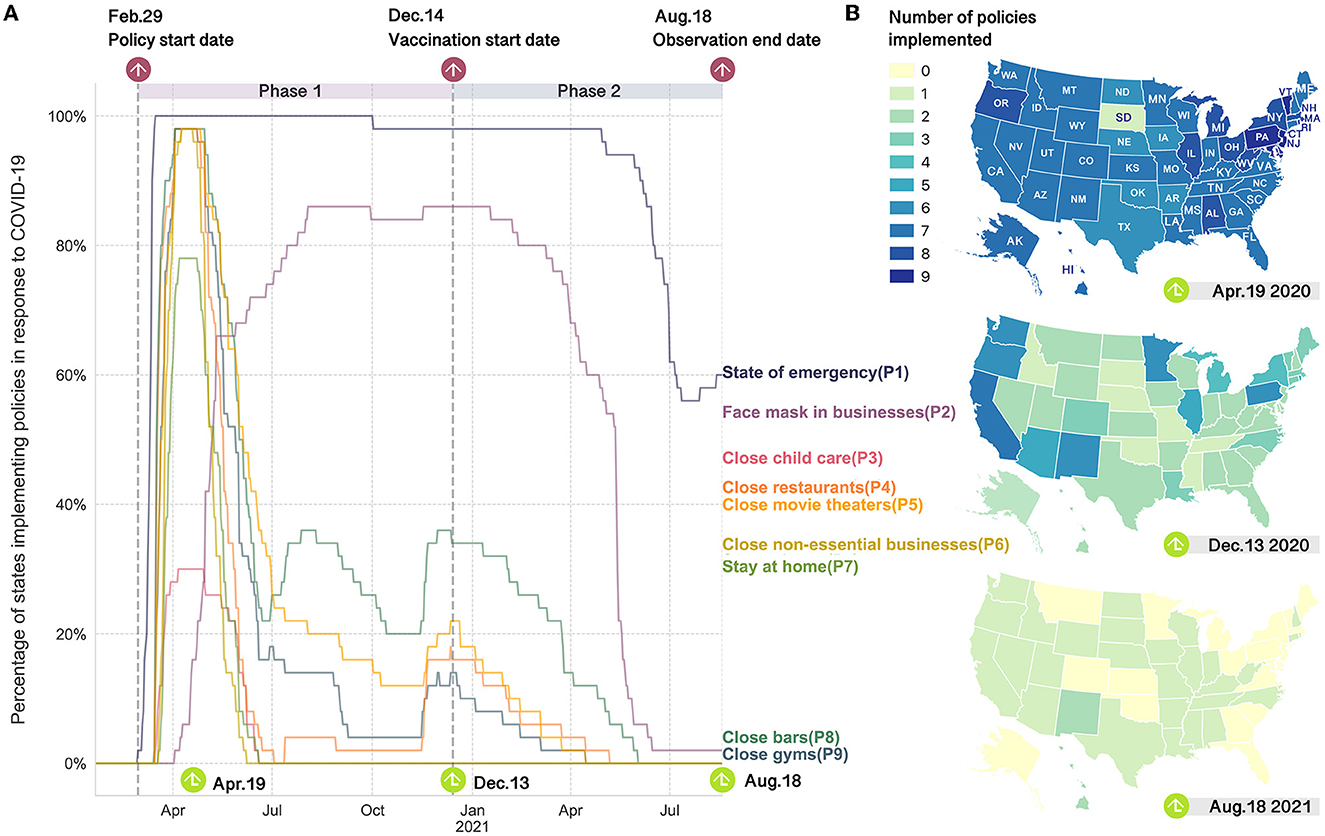
Figure 1. Implementation of anti-contagion policies in response to the COVID-19 over time and space in the United States. (A) Percentage of states with the COVID-19 policies being enacted over time. Two vertical dashed lines represent the start dates of COVID-19 policy deployment and vaccine distribution, respectively. (B) Maps of number of NPIs implemented by the states on three representative dates. April 19, 2020 represents the period with the most stringent lockdowns. December 13, 2020 is the day before COVID-19 vaccines were administered in the U.S.. August 18, 2021 is the last day of the observation period.
Apart from the database of NPIs, we also employ daily COVID-19 case data from the New York Times (38) and aggregated mobility data from Unacast (39) to first draw a comprehensive comparison of the temporal variations in virus transmission, mobility patterns, and policies during the COVID-19 outbreak. Here, two mobility metrics utilized are relative percentage changes in visits to non-essential venues (VD) and average travel distance (TD) compared to the corresponding day of the week prior to the COVID-19 outbreak for a given date. Two COVID-19 case variables include daily new cases (NC) and deaths (ND). Specifically, we map the state government policy actions against these variables as well as the instantaneous reproduction number (Rt) estimated by the susceptible-exposed-infectious-recovered-susceptible (SEIRS) epidemic model (40) (Supplementary material 3). Here, Rt is a key indicator to monitor the real-time transmissibility of the virus and to estimate the impact of local NPIs on the epidemic. The compartmental model SEIRS is fitted with publicly available COVID-19 case data as mentioned (38). Disease-specific parameters in the model were derived from the recent literature, including a mean incubation period of 5.2 days (95% confidence interval [CI] 4.1–7.0) (41), an average recovery time of 8 days (42) and the mean time to death from the onset of 17.8 days (95% CI 16.9–19.2) (43). In addition, patients are assumed to develop temporal immunity of 180 days, after recovering from the initial infection of the virus (44).
Based on the preliminary observations, we further explore multiple temporal dynamic relationships between transmission and mobility variables in a bivariate setting by using vector autoregressive models (45) and the Granger causality tests (46). Here we also employ a sub-period analysis to explore how these variables and the relationships between them changed over time before and after the administration of the COVID-19 vaccines. For clarity, we will take the tests between Rt and VD as an example to illustrate in detail how the techniques are employed below.
Vector autoregression (VAR) (45) is a widely used statistical method for multivariate time series analysis. Granger causality analysis (46) was initially developed in econometrics as a technique for investigating the directed interactions between time-series data (47). This statistical concept of causality is based on the prediction that a time series x (VD) Granger causes another time series y (Rt) if the autoregressive forecast of y can be better explained when the past information from x is considered (48). After determining the maximum order of integration (d) and optimal time lag length (m) for Rt and VD (Supplementary material 5), we establish bivariate augmented VAR models for the two phases in each state, based on the idea of the Toda-Yamamoto Granger causality test (49) (Supplementary material 6) as follows:
where yt denotes the value of the time series y at time t, i is the length of the lag-time moving window, αi and ϕi are the parameters to estimate, ϵt refers to the white noise residual. The variables of x and y can be interchanged to test for the Granger causality in the other direction.
Multiple linear regression analysis is then employed to assess the association between policy types and COVID-19 transmission as well as human mobility changes. Specifically, for each state, we build two multiple linear regression models, in which independent variables are policy types [p1, p2, …, pk], while the continuous dependent variables are vt and , respectively. Here, denotes the temporal lagged reproduction number for date t with individualized temporal relationships between vt and Rt in each state. The assumption here is that the changes in human mobility are visible on the same date when the NPIs are issued, while is determined by the temporal lagged associations between mobility and the spread of the coronavirus investigated using VAR model with Granger causality test. For instance, since there is a significant Granger causality relationship discovered from Rt to vt with a lag of m = 2 in California during phase 1 (Supplementary Table 5), the corresponding for vt is equal to Rt−2. This operation applies to the following two Pareto analysis tasks, the evaluation of existing policy strategies and the design of new policy solutions for each state. To fulfill the second task, the processed data is used to fit multiple linear regression models for each phase in a state as follows:
where k is the number of policy types. The estimated parameters of [λ0, λ1, λ2, …, λk] and [η0, η1, η2, …, ηk] are used for the prediction of and in the generation process of new optimal policy strategies.
Next, we elaborate Pareto approaches for the assessment and optimal design of the NPIs in each state. In multi-objective optimization problems, the Pareto-efficient state is achieved if there is no other solution that can bring improvement to one of the objectives without showing degradation in another objective (50). According to this, our optimization problem can be defined as a vector function f that maps a vector of policy decision variables p to a tuple of two objectives h as follows:
where P is the policy space and H is the objective space.
In our case, the optimization goal is to strike a delicate balance between the control of COVID-19 and the recovery of socio-economic vitality, which are indicated specifically by Rt and VD, respectively. These two variables are chosen because we consider the estimated Rt a more comprehensive metric to measure the transmissibility of the pandemic and visitation frequency a more appropriate indicator of socio-economic vitality. Based on this assumption, one of the objectives of our research task is to minimize the reproduction number of the virus fr(p). In the meanwhile, the value of visitation metric fv(p) is expected to be maximized. Accordingly, we set the values of w1 and w2 to 1 and -1. Consider two policy decision vectors a, b ∈ P. The policy decision vector a is said to dominate b if their objective vectors f(a) and f(b) satisfy:
The set of all the policy decision vectors that are not dominated by any other generates the Pareto optimal set, which provides policymakers with a group of optimal solutions to make a well-informed decision that balances the trade-offs between the public health concerns and socio-economic losses rather than a single-point solution.
In this study, we first use the notion of Pareto optimality to evaluate the performance of existing policy combinations. Specifically, for each given date t, we collect the corresponding value of visitation metric vt and estimate the reproduction number using the SEIRS epidemic model with temporal lagged effects considered. These two features collectively form the two-dimensional space, in which the Pareto-optimal set would be explored. For each Pareto-optimal point obtained, we can figure out the corresponding control measures implemented on a particular date for further investigation.
We then explore possible new policy combinations that might be more effective than the current ones by employing the non-dominated sorting genetic algorithm II (NSGA-II) (51) (Supplementary material 8). Specifically, we adopt multiple regression first to estimate the coefficient for each policy type in the prediction of and during different phases with temporal lags effects considered. These parameters calculated are then fed into the NSGA-II algorithm to generate the Pareto optimal solutions. Then the solutions with an estimated no larger than the maximum mean of the existing optimal policy strategies are further selected. Different from the implementation of existing policies that are dummy-coded, the parameter estimated through the generic algorithm for each type of policy is a continuous variable, which can be interpreted as the strength of the policy enforcement. According to this, public health policymakers in each state would be able to create more refined designs of COVID-19 strategies with expected effects estimated and make more deliberate decisions regarding what kind of adjustments shall be made to the current schemes and how.
We first map the state government NPIs against the timelines of mobility and transmission variables to investigate the temporal associations between them. As shown in Figure 2, state authorities typically implemented measures precisely when the Rt value peaked and reinstated NPIs when COVID-19 cases reached alarming levels during subsequent waves. One can also notice that the mobility level seems to be an indicator of how stringent the local NPIs are. In the beginning, when the states adopted the strictest interventions, population mobility experienced a sharp decline from peak to trough in all the states. Then with the adjustments of the NPIs and the application of vaccines, the relative reduction in mobility also changed accordingly. In terms of the relationships between new infections and human mobility, the relevant curves in Figure 2 hint at the existence of time-lagged associations, which will be further investigated through time series analysis next. Due to space limitations, we provide a detailed analysis of California, which has the highest number of COVID-19 cases and a wide range of NPIs. We also highlight key findings for nine other heavily impacted states as examples in the main text. Additional findings for other states in the U.S. can be found in the Supplementary material.
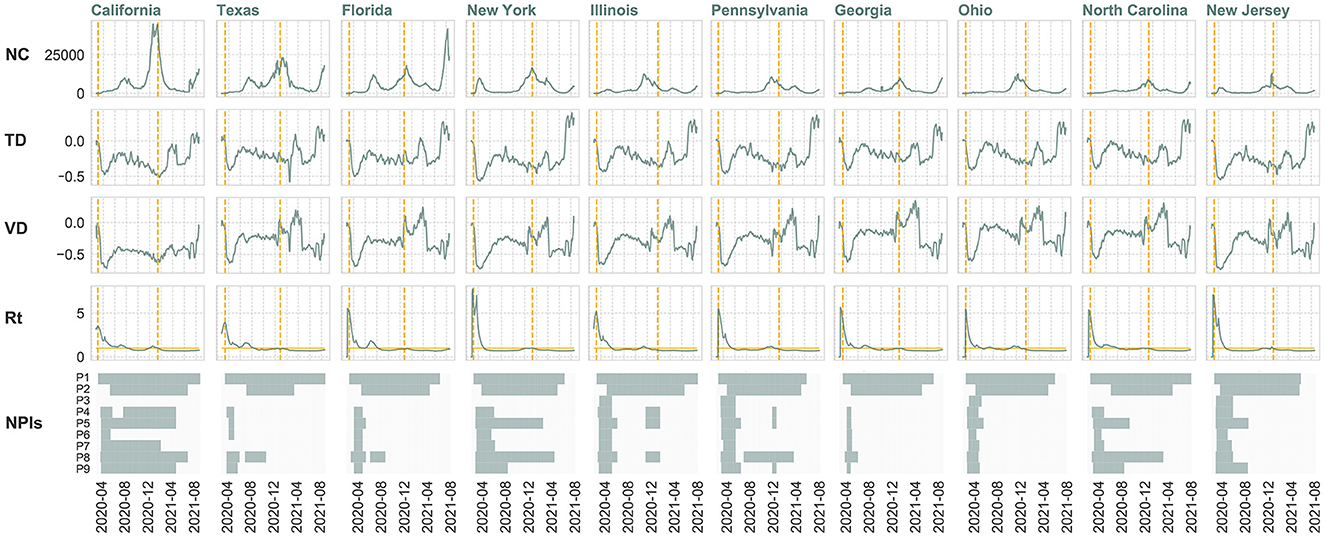
Figure 2. Temporal changes in daily new COVID-19 cases (NC), travel distance difference (TD), visitation difference (VD), instantaneous reproduction number (Rt) and policy implementation in the ten states with highest number of confirmed cases from February 24, 2020 to August 18, 2021. 7-day moving average is utilized to smooth volatile case reporting data and human mobility metrics. The start dates of policy implementation and vaccine distribution are indicated by dashed vertical lines. A horizontal line is drawn at Rt=1. If Rt is greater than 1, the epidemic is expanding at time t, whereas Rt < 1 signals that the epidemic is shrinking.
Based on the preliminary findings, we further investigate the dynamic temporal lagged relationships between transmission and mobility variables in a bivariate setting using VAR (45) and the Granger causality tests (46). After a series of tests (Supplementary material 5), we then build VAR models with the Toda-Yamamoto Granger causality test according to Equation 1 and display the results in Table 1. As can be observed, the Granger causality relationship from Rt to VD is statistically significant at the 1% level during phase 1 in California, but not significant for phase 2. The phenomena can be interpreted as people reacting to the news about confirmed COVID-19 cases by changing their mobility patterns significantly in phase 1. This behavioral response, however, is not that evident after the vaccines were available, hinting at the fact that people felt more protected by vaccines and less keen on constraining their movements. To look in the other direction, it is found that the null hypothesis of no Granger causality from VD to Rt can be rejected at the 10% significance level during phase 2, which implies that the visitation change of individuals Granger causes the transmission of the COVID-19 during the period of phase 2.
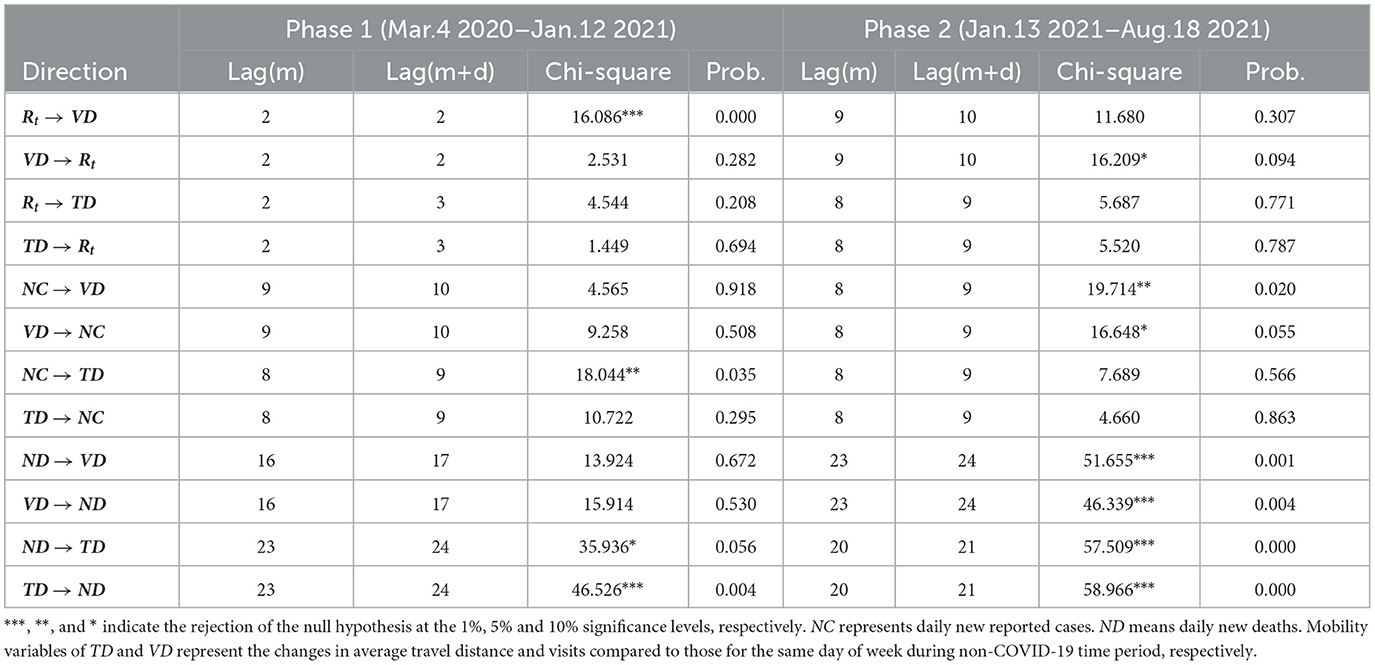
Table 1. Toda-Yamamoto Granger causality test results for transmission and mobility variable pairs in California.
Apart from the variable pair of Rt and VD, the Toda and Yamamoto causality test is also performed between other possible pairs of the epidemiological and mobility variables. It can be observed in the table that bi-directional Granger causality emerged between variable pairs of (ND, TD) in both phases and pair of (ND, VD) in phase 2. Moreover, all the test results for ND during phase 2 reject the null hypothesis at the significance level of 1%. For the corresponding tests between NC and the two mobility variables, no Granger causality relationship is found at the 1% significance level. It is also noticeable that the optimal lag lengths selected according to information criteria for ND and two mobility metrics are higher than those of NC of around one to two weeks, which may correspond to the length of treatment.
The following offers the results of existing optimal solutions discovered using Pareto approaches in the actual scene. As can be observed from Figures 3A, B, there are in total two and three unique Pareto optimal solutions for California in phase 1 and phase 2, respectively. Among them, the state of emergency (P1) is found to be the only individual policy present in all the optimal solutions. To discuss by phases, it is interesting to observe that the closure of restaurants (P4) is the policy type that distinguishes strategy S4 from S7, connected to a considerable reduction in , down to 0.769 from 1.206, confirming the relatively high risks of transmitting the virus during convivial activities such as dining in a group. However, closing restaurants also considerably reduces the mobility index, down to -0.393 from -0.319, confirming the trade-off between the need of containing the virus and socio-economic vitality. However, when it came to phase 2, a larger number of enacted control measures did not guarantee a smaller . Instead, the lowest average is generated by a moderate policy strategy S3. In addition, the slope of the Pareto frontier for phase 2 is greater than that for phase 1 in California, implying that the increase in is accompanied by a relatively larger recovery of vt when the vaccines became available.
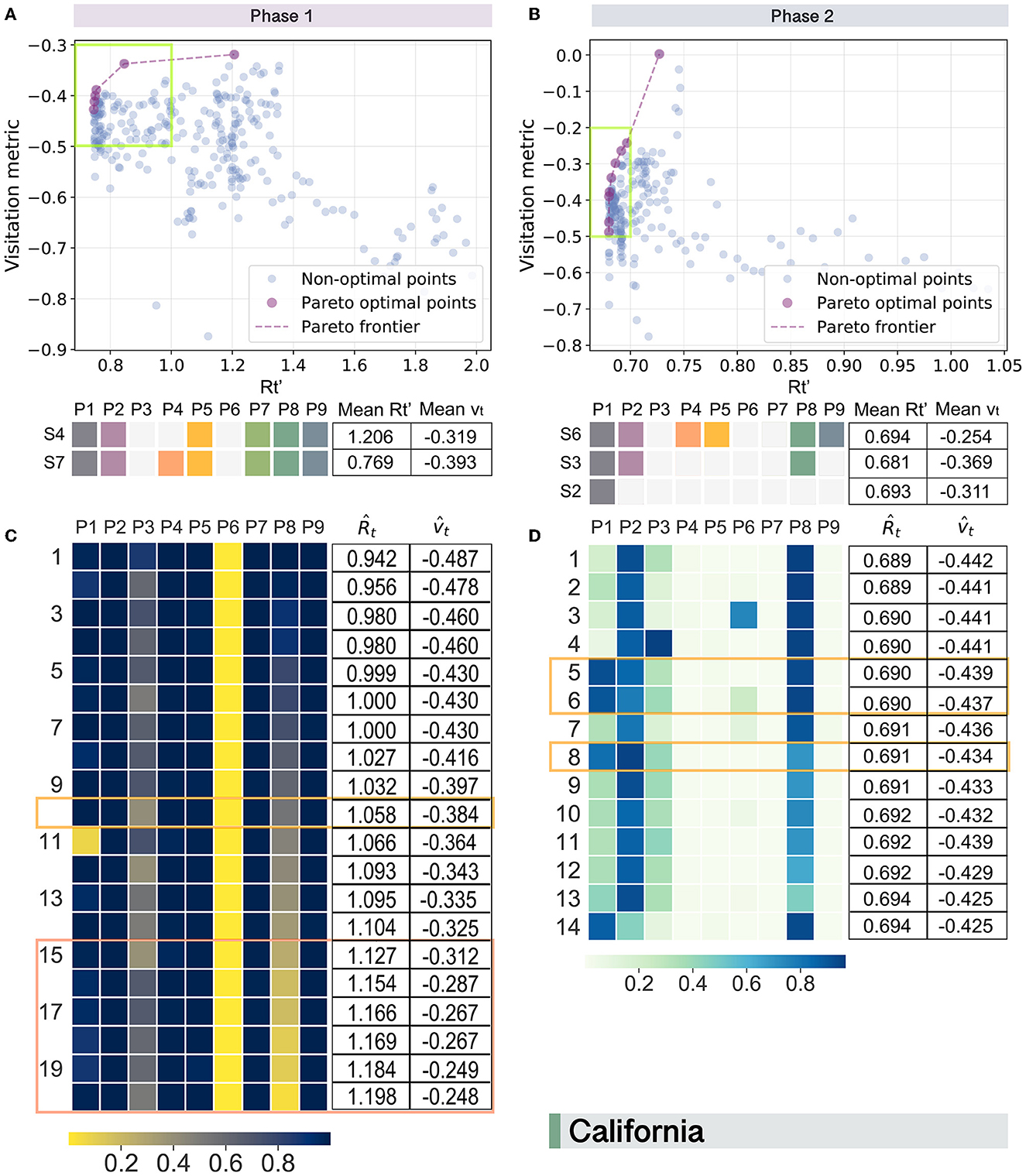
Figure 3. Pareto optimal trade-offs between human mobility (vt) and virus transmission () in California during two phases. For existing solutions in phase 1 (A) and phase 2 (B), purple-colored spots represent optimal solutions that are connected by dashed lines to visually estimate the Pareto frontier. Candidate points with a value of larger than 2 are filtered. Pareto optimal points with a between 0.7 and 1 are enclosed by green boxes for phase 1 (A) and phase 2 (B), respectively. Corresponding optimal policy strategies after duplicate elimination are displayed in lower sub-figures with average and vt listed in the tables beside them. For potential optimal policy strategies generated for California in phase 1 (C) and phase 2 (D), solutions with a less than 1.206 and 0.694 are selected, respectively. Corresponding parameters estimated for the policy types are displayed as heatmaps with predicted and listed in the right tables. Orange rectangle highlights the solutions similar to the existing optimal strategies of S7 and S3; and, coral ones highlight more optimized solutions.
It should also be noticed that the solutions selected are considered equally good according to the Pareto optimality concept. To decide which solution to choose depends on the policy makers' perspectives about the priority of the two objectives in the optimization task. For instance, if the decision-makers in California intend to relax policies to some extent so that they have as little as possible impact on the normal mobility of the residents in phase 1, the corresponding would be as high as 1.206 on average as solution S4 presents.
We then explore possible new policy combinations in each state by employing the NSGA-II (51) and present the optimization results for California in Figures 3C, D. Here, the parameter estimated through the generic algorithm for each type of policy can be interpreted as the strength of the policy enforcement that a value closer to 1 represents the strength is relatively stronger, whereas closer to 0 indicates that the implementation of the policy is weaker.
Comparing the optimal solutions generated for phase 1 with those of the existing policy strategies, the last six potential solutions are found more optimized than the current optimal solution S4 since they have both smaller and larger . This observation suggests that exploring new possible strategies for better trade-offs between virus control and the maintenance of mobility is necessary. Among these six optimal solutions, the NPIs of (P1, P2, P4, P5, P7, P9) are expected to be implemented together with strong strengths. In contrast, the closure of non-essential businesses (P6) seems to be not very necessary, which is in accordance with the phenomenon observed in the evaluation of existing optimal strategies previously. The main distinctions between the potential optimal solutions discovered here from the existing ones for phase 1 lie in the adoption of P3 and P8. Essentially, the new proposed optimal solutions put more emphasis on the importance of closing child care centers (P3) and the flexible adjustment of the shutdown of bars (P8). While for the design of optimal strategies for California in phase 2 (Figure 3D), it presents a significantly different pattern from that for phase 1 (Figure 3C). Specifically, the overall strength of the policies for phase 2 is relatively weaker, and the solutions generated are more heterogeneous. In addition, policymakers in California should also shift the focus of the policy types to wearing face masks in businesses (P2) and closing bars (P8) in the later phase.
To provide a clearer picture of how to sketch out the implementation plans, we then replace policy parameters that fall within the ranges (0, 0.5) and (0.5, 1) as 0 and 1, respectively. This simplified version of the optimal policy scheme is shown in Figure 4, from which we can see that there are five and six types of optimal policy strategies extracted for phase 1 and phase 2 in California, respectively. Among them, the current solutions of S7 and S3 are included, while the other nine potential optimal strategies that may achieve better or equally good performance compared to the existing ones offer decision-makers a list of possible alternatives in the fight against COVID-19.
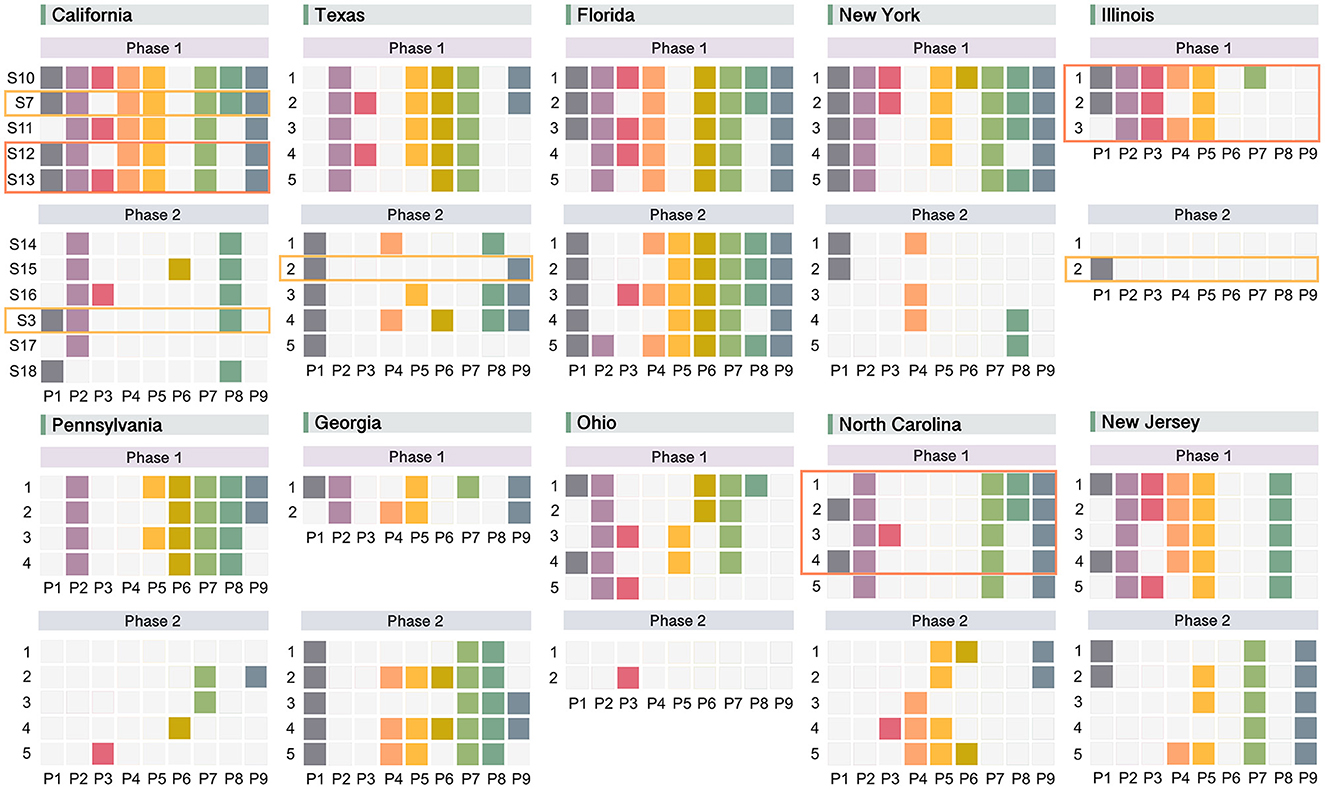
Figure 4. Optimal response strategies generated by NSGA-II for 10 states with the highest number of confirmed COVID-19 cases during different phases. Strategies for each state are listed in ascending order of the average predicted . If more than five optimal solutions are distilled for a certain state and phase, only the top five strategies are retained. Orange rectangles mark solutions already included in the existing strategies for the state; and, coral rectangles highlight more optimized ones.
Following the same framework, we conduct analyses for other states and display their simplified optimal strategies in Figure 4. From the view of comparisons across space and time, following major findings emerge: (1) the differences between optimal policy designs for the ten states studied are evident, indicating the necessity of adopting differentiated and tailor-made COVID-19 response strategies in each individual state; (2) existing policy strategies (enclosed by orange rectangles) seldom appear in the list of new proposed ones, suggesting that there are a considerable number of alternatives available for COVID-19 prevention beyond current policy programs; (3) new solutions generated that are more preferable than the current ones (enclosed by coral rectangles with smaller and higher ) show in the first phase of some states (California, Illinois, and North Carolina), offering potential solutions that could be considered to replace the existing ones to policymakers; (4) for each state, two different phases present widely divergent strategies regarding policy types and amount of enacting policies. Specifically, the designs for Phase 2 include fewer policy types and amounts compared to Phase 1 in general, the phenomenon of which may be explained by the availability of vaccines in Phase 2 when the control of COVID-19 no longer relies solely on the NPIs.
This paper introduces a dynamic modeling framework designed to support decision-making processes for local policymakers. Our framework offers flexibility in evaluating and developing refined COVID-19 policy strategies, emphasizing the delicate balance between safeguarding public health and promoting socio-economic vitality. By analyzing shifts in human mobility, we provide insights into effective policy adjustments and decision-making. Here tailor-made adjustment schemes and novel optimal policies in response to the COVID-19 pandemic are generated for state authorities to choose from, depending on their priorities and current vaccination status. This can be achieved through the joint utilization of epidemiological data, mobility data, NPIs, and in-depth exploration of the dynamic relationships between them by fusing multiple techniques.
We started with a discussion of the intertwined associations among the spread of the virus, policy implementation, and human mobility during different phases and discovered some prevailing patterns across the states (Figure 2 and Supplementary Figures 2–5). For instance, the state governments generally began to implement NPIs when the Rt was at its maximum. In addition, human mobility can be used as a proxy for NPIs since it dropped steeply to the lowest level when the most stringent NPIs were issued in the early stages of the pandemic. Then with the subsequential relaxation and tightening of NPIs later on, human mobility levels also changed accordingly. The emergence of COVID-19 vaccines introduced new variables into these interrelationships. Some states (e.g., CA, IL, PA, MI, MN, WA, IA, and OR) began to loosen their NPIs, which coincided with a virus transmission decline and human mobility increase.
Another key observation that warrants further investigation is the existence of underlying temporal associations between human mobility and virus transmission, which might be bidirectional and dynamic. When adjustments were made to NPIs, human mobility offered relatively immediate responses while the corresponding changes in virus transmission would take some extra time to reflect on confirmed cases. Moreover, the temporal relationships between virus transmission and human mobility might be bidirectional and dynamic. For instance, people would adjust their travel behaviors if they saw a dramatic rise in COVID-19 cases; and the changes in mobility trends would, in turn, affect the confirmed cases in a few days. Furthermore, the relationships would also change with the advent of the vaccines. These observations impel us to ponder over the temporal associations between mobility and virus transmission by employing the VAR model and Granger causality analysis in a phased manner for further investigation. For instance, the results of VAR models prove the existence of temporal lagged effects as well as Granger causality relationships between some transmission and mobility variable pairs during different phases. With regard to the variable pair of (Rt, VD) that we pay particular attention to, significant Granger causality relationships are largely discovered in the states affected the most by COVID-19 in the U.S. (Supplementary Table 7). Here for each state, at least one direction in one phase offers results that are significant at the 5% level. In addition, we observe a relatively stronger Granger causality relationship between ND (death count) and mobility patterns compared to that of NC (daily infections), which aligns with findings from previous studies (52–54). These studies have highlighted the use of death count as a more reliable metric, considering that the actual number of infected cases is expected to be significantly larger than reported. These findings deepen our understanding of the transmission dynamics of COVID-19 and human behaviors by revealing the intricate temporal associations between them. This knowledge enables more comprehensive policy-making that considers the temporal effects, leading to more effective strategies.
We then evaluate the performance of existing policy strategies across the states using Pareto analysis, so as to offer policymakers a lens for looking back to identify effective policy combinations and adjust less effective ones in the future. For the pre-vaccine stage, to measure the contribution of policy types to health-economic balance individually, state of emergency (P1) and wearing face masks (P2) show as the most important NPIs that they appear in all the optimal strategies among the top ten states (Supplementary Table 8). The closure of recreational services (P8, P5, P9, P4) comes next with moderate impact, while essential businesses (P6) and child care centers (P3) do not present in any of the optimal strategies. From the perspective of the policy mix, the co-activation of P1 and P2 accounts for the largest proportion (30%) and is presented in the optimal strategies for six states (TX, FL, IL, GA, OH, NJ). The second most frequent policy combination is (P1, P2, P8), which accounts for 25% of the optimal strategies. This observation implies the importance of ordering bars to close in the COVID-19 fight when vaccines have not been authorized for use. The reason why the closure of bars plays a more significant role in achieving the optimal status than other types of entertainment venues may be due to the fact that the social atmosphere in bars tends to be more lively, mixed, and closer with a relatively shorter social distance. This finding implies that paying closer attention to the control of gathering sites where social scenes are more complex (e.g., bars) is particularly necessary before the advent of vaccines. Then when the COVID-19 vaccines were available, the percentage of each policy type shown in the optimal strategies decreased in general (Supplementary Table 9). However, from a ranking view, what does not change compared to Phase 1 is that the most effective individual policy types are still P1, P2, and P8. In terms of the policy combinations, there are two most dominant strategies, namely (P1, P2) and enacting P1 only. Both of the strategies account of 27% and present in six states out of the ten.
Finally, we employ the NSGA-II algorithm to generate new optimal policy strategies. Here, the results reveal substantial differences between different phases and states, highlighting the necessity of designing spatio-temporal tailor-made policy strategies. For instance, wearing face masks (P2) is particularly important for all the states in the pre-vaccine period (Supplementary Figures 8–16). However, this is not the case in the later phase. The policy type of closing restaurants (P4) is essential for FL and NJ in phase 1, but not that important for the states of TX, NY, PA, and NC. By considering the state-tailored temporal lag effects in Granger causality tests and regression analyses in a phase-wise manner, we provide policymakers with a spatio-temporal context-aware guiding policy formulation reference. It also enables them to compare the expected effects of potential optimal solutions with the performance of existing strategies and make more deliberate decisions regarding what kind of adjustments shall be made to the current schemes and how. Moreover, the implementation strategies proposed by our framework are more fine-grained than the existing ones. This is reflected in the strengths of policy enforcement as outputs for decision-makers. Furthermore, our framework also offers sophisticated implementation strategies that produce the strengths of policy enforcement as outputs for decision-makers.
Our study has several limitations. First, we mainly focus on NPIs implementation in the regions with the most confirmed cases, since they play a more crucial role in combating the COVID-19 pandemic. However, an in-depth analysis of areas with fewer cases may raise other intriguing questions, such as why they performed relatively better in the fight against COVID-19. This sort of exploration may lead to a deeper understanding of how to improve the combined power of NPIs or offer novel insights into reasons for the effectiveness of control measures varying considerably across regions. This future investigation may require the additional use of demographic data, which can also help reveal the underlying logic of the results we have obtained. In addition, we only consider public health and human mobility as two primary objectives in the optimization of this study. Other socio-economic costs due to COVID-19 pandemic like psychological distress, economic recession, job losses, increased government debt, and social unrest can be discussed in future work. It is also important to note that the specific socio-economic costs can vary across countries and regions, and further research can provide a more comprehensive understanding of the impact of COVID-19 on different aspects of society and the economy. One additional limitation of this study is the absence of specific data on the composition of viruses in each state during the observation period. Consequently, we were unable to account for the variations in virus composition. Instead, our study focuses on comparing the optimized combinations of different policies and their potential effects on various variants. Although the precise timing of these effects may differ across variants, conducting more comprehensive analyses for each variant would be an intriguing avenue for future research.
In conclusion, we provide detailed insights into the spatio-temporal dynamics of the COVID-19 pandemic during different stages and highlight the essential role of some core intervention portfolios in controlling the pandemic. The methodology proposed here can offer policymakers reasoned estimates of the potential effectiveness of the NPIs to be attained and becomes even more critical when health systems are facing extreme loads in the U.S. In addition, the framework presented can be useful for populations without access to local COVID-19 data and for similar scenarios in the future involving emerging infectious diseases where relevant outcomes are not yet available.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
XZhou, XZhang, and PS conceived the experiments. XZhang collected the pandemic and mobility data. XZhou conducted the experiments and wrote the paper. PS and CR coordinated the project. All authors participated in the discussion of results, provided critical feedback, and reviewed the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the National Natural Science Foundation of China (NSFC Grant No. 62106274) and the Fundamental Research Funds for the Central Universities, Renmin University of China (No. 22XNKJ24).
We would like to express our gratitude to Dr. Dong, L. for his contribution to the writing of this paper. His support and feedback have been instrumental in improving the clarity and quality of the manuscript. We also wish to acknowledge the support provided by the Intelligent Social Governance Platform, Major Innovation and Planning Interdisciplinary Platform for the Double-First Class Initiative.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1198973/full#supplementary-material
1. World Health Organization. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV), Vol. 30. Geneva: World Health Organization (2020).
2. Flaxman S, Mishra S, Gandy A, Unwin HJT, Mellan TA, Coupland H, et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature. (2020) 584:257–61. doi: 10.1038/s41586-020-2405-7
3. Prem K, Liu Y, Russell TW, Kucharski AJ, Eggo RM, Davies N, et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: a modelling study. The Lancet Public Health. (2020) 5:e261–70. doi: 10.1016/S2468-2667(20)30073-6
4. World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. (2022). Available online at: https://covid19.who.int (accessed July 06, 2022).
5. Davies NG, Kucharski AJ, Eggo RM, Gimma A, Edmunds WJ, Jombart T, et al. Effects of non-pharmaceutical interventions on COVID-19 cases, deaths, and demand for hospital services in the UK: a modelling study. Lancet Public Health. (2020) 5:e375–85. doi: 10.1016/S2468-2667(20)30133-X
6. Cot C, Cacciapaglia G, Sannino F. Mining Google and Apple mobility data: temporal anatomy for COVID-19 social distancing. Sci Rep. (2021) 11:1–8. doi: 10.1038/s41598-021-83441-4
7. Lai S, Ruktanonchai NW, Zhou L, Prosper O, Luo W, Floyd JR, et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature. (2020) 585:410–3. doi: 10.1038/s41586-020-2293-x
8. Forecasting Team IC. Modeling COVID-19 scenarios for the United States. Nature Med. (2020) 27:94–105. doi: 10.1038/s41591-020-1132-9
9. Abueg M, Hinch R, Wu N, Liu L, Probert W, Wu A, et al. Modeling the effect of exposure notification and non-pharmaceutical interventions on COVID-19 transmission in Washington state. NPJ digital medicine. (2021) 4:1–10. doi: 10.1038/s41746-021-00422-7
10. Singh S, Shaikh M, Hauck K, Miraldo M. Impacts of introducing and lifting nonpharmaceutical interventions on COVID-19 daily growth rate and compliance in the United States. Proc Natl Acad Sci USA. (2021) 118:12. doi: 10.1073/pnas.2021359118
11. Ragonnet-Cronin M, Boyd O, Geidelberg L, Jorgensen D, Nascimento FF, Siveroni I, et al. Genetic evidence for the association between COVID-19 epidemic severity and timing of non-pharmaceutical interventions. Nat Commun. (2021) 12:1–7. doi: 10.1038/s41467-021-22366-y
12. Bo Y, Guo C, Lin C, Zeng Y, Li HB, Zhang Y, et al. Effectiveness of non-pharmaceutical interventions on COVID-19 transmission in 190 countries from 23 January to 13 April (2020). Int J Infect Dis. (2021) 102:247–53. doi: 10.1016/j.ijid.2020.10.066
13. Hu S, Xiong C, Yang M, Younes H, Luo W, Zhang L, et al. big-data driven approach to analyzing and modeling human mobility trend under non-pharmaceutical interventions during COVID-19 pandemic. Transp Res Part C Emerg. (2021) 124:102955. doi: 10.1016/j.trc.2020.102955
14. Askitas N, Tatsiramos K, Verheyden B. Estimating worldwide effects of non-pharmaceutical interventions on COVID-19 incidence and population mobility patterns using a multiple-event study. Sci Rep. (2021) 11:1–13. doi: 10.1038/s41598-021-81442-x
15. Levin R, Chao DL, Wenger EA, Proctor JL. Insights into population behavior during the COVID-19 pandemic from cell phone mobility data and manifold learning. Nat Computat Sci. (2021) 1:588–97. doi: 10.1038/s43588-021-00125-9
16. Woskie LR, Hennessy J, Espinosa V, Tsai TC, Vispute S, Jacobson BH, et al. Early social distancing policies in Europe, changes in mobility & COVID-19 case trajectories: Insights from Spring (2020). PLoS ONE. (2021) 16:e0253071. doi: 10.1371/journal.pone.0253071
17. Oh J, Lee HY, Khuong QL, Markuns JF, Bullen C, Barrios OEA, et al. Mobility restrictions were associated with reductions in COVID-19 incidence early in the pandemic: evidence from a real-time evaluation in 34 countries. Sci Rep. (2021) 11:1–17. doi: 10.1038/s41598-021-92766-z
18. Ilin C, Annan-Phan S, Tai XH, Mehra S, Hsiang S, Blumenstock JE. Public mobility data enables COVID-19 forecasting and management at local and global scales. Sci Rep. (2021) 11:1–11. doi: 10.1038/s41598-021-92892-8
19. Demirguc-Kunt A, Lokshin M, Torre I. The sooner, the better: the early economic impact of non-pharmaceutical interventions during the COVID-19 pandemic. In: World Bank Policy Research Working Paper. (2020) p. 9257. doi: 10.1596/1813-9450-9257
20. Sheridan A, Andersen AL, Hansen ET, Johannesen N. Social distancing laws cause only small losses of economic activity during the COVID-19 pandemic in Scandinavia. Proc Nat Acad Sci. (2020) 117:20468–73. doi: 10.1073/pnas.2010068117
21. Zaremba A, Kizys R, Aharon DY, Demir E. Infected markets: novel coronavirus, government interventions, and stock return volatility around the globe. Finance Research Letters. (2020) 35:101597. doi: 10.1016/j.frl.2020.101597
22. Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surg. (2020) 78:185–93. doi: 10.1016/j.ijsu.2020.04.018
23. Zhang J, Litvinova M, Liang Y, Wang Y, Wang W, Zhao S, et al. Changes in contact patterns shape the dynamics of the COVID-19 outbreak in China. Science. (2020) 368:1481–6. doi: 10.1126/science.abb8001
24. Abuhammad S. Violence against Jordanian women during COVID-19 outbreak. Int J Clin Pract. (2021) 75:e13824. doi: 10.1111/ijcp.13824
25. Sutin AR, Luchetti M, Aschwanden D, Lee JH, Sesker AA, Strickhouser JE, et al. Change in five-factor model personality traits during the acute phase of the coronavirus pandemic. PLoS ONE. (2020) 15:e0237056. doi: 10.1371/journal.pone.0237056
26. Luchetti M, Lee JH, Aschwanden D, Sesker A, Strickhouser JE, Terracciano A, et al. The trajectory of loneliness in response to COVID-19. Am Psychol. (2020) 75:897–908. doi: 10.1037/amp0000690
27. Alzueta E, Perrin P, Baker FC, Caffarra S, Ramos-Usuga D, Yuksel D, et al. How the COVID-19 pandemic has changed our lives: A study of psychological correlates across 59 countries. J Clin Psychol. (2021) 77:556–70. doi: 10.1002/jclp.23082
28. Sadiković S, Branovački B, Oljača M, Mitrović D, Pajić D, Smederevac S. Daily monitoring of emotional responses to the coronavirus pandemic in Serbia: a citizen science approach. Front Psychol. (2020) 11:2133. doi: 10.3389/fpsyg.2020.02133
29. Nguyen QD, Prokopenko M, A. general framework for optimising cost-effectiveness of pandemic response under partial intervention measures. Sci Rep. (2022) 12:19482. doi: 10.1038/s41598-022-23668-x
30. Thom H, Walker J, Vickerman P, Hollingworth W. Exploratory comparison of Healthcare costs and benefits of the UK's Covid-19 response with four European countries. Eur J Public Health. (2021) 31:619–24. doi: 10.1093/eurpub/ckab019
31. Reddy KP, Shebl FM, Foote JH, Harling G, Scott JA, Panella C, et al. Cost-effectiveness of public health strategies for COVID-19 epidemic control in South Africa: a microsimulation modelling study. Lancet Global Health. (2021) 9:e120–9. doi: 10.1016/S2214-109X(20)30452-6
32. Ferguson N, Laydon D, Nedjati Gilani G, Imai N, Ainslie K, Baguelin M, et al. Report 9: Impact of Non-pharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand. (2020).
33. Hamimes A, Aouissi HA, Ababsa M, Lounis M, Jayarajah U, Napoli C, et al. The effect of preventive measures and vaccination against SARS-CoV-2 on the infection risk, treatment, and hospitalization: a cross-sectional study of Algeria. Viruses. (2022) 14:2771. doi: 10.3390/v14122771
34. Regmi K, Lwin CM. Factors associated with the implementation of non-pharmaceutical interventions for reducing coronavirus disease (2019). (COVID-19): A systematic review. Int. J. Environm Res public health. (2021) 18:4274. doi: 10.3390/ijerph18084274
35. Chang SL, Cliff OM, Zachreson C, Prokopenko M. Simulating transmission scenarios of the delta variant of SARS-CoV-2 in Australia. Front Public Health. (2022) 10:823043. doi: 10.3389/fpubh.2022.823043
36. Nascimento de. Lima P, Lempert R, Vardavas R, Baker L, Ringel J, Rutter CM, et al. Reopening California: Seeking robust, non-dominated COVID-19 exit strategies. PLoS One. (2021) 16:e0259166. doi: 10.1371/journal.pone.0259166
37. Raifman J, Nocka K, Jones D, Bor J, Lipson S, Jay J, et al. COVID-19 US State Policy Database. (2020). Available online at: www.tinyurl.com/statepolicies (accessed August 21, 2021).
38. The New York Times. Coronavirus (Covid-19) Data in the United States. (2021). Available online at: https://github.com/nytimes/covid-19-data (accessed August 27, 2021).
39. Unacast. Covid-19 Social Distancing Scoreboard. (2021). Available online at: https://www.unacast.com/covid19/social-distancing-scoreboard
40. Bjørnstad ON, Shea K, Krzywinski M, Altman N. The SEIRS model for infectious disease dynamics. Nat Methods. (2020) 17:557–59. doi: 10.1038/s41592-020-0856-2
41. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. (2020) 382:1199–207. doi: 10.1056/NEJMoa2001316
42. Maier BF, Brockmann D. Effective containment explains subexponential growth in recent confirmed COVID-19 cases in China. Science. (2020) 368:742–6. doi: 10.1126/science.abb4557
43. Verity R, Okell LC, Dorigatti I, Winskill P, Whittaker C, Imai N, et al. Estimates of the severity of coronavirus disease 2019: a model-based analysis. Lancet Infect Dis. (2020) 20:669–77. doi: 10.1016/S1473-3099(20)30243-7
44. Seow J, Graham C, Merrick B, Acors S, Pickering S, Steel KJA, et al. Longitudinal observation and decline of neutralizing antibody responses in the three months following SARS-CoV-2 infection in humans. Nat. Microbiol. (2020) 5:1598–607.
46. Granger CWJ. Investigating causal relations by econometric models and cross-spectral methods. Econometrica. (1969) 37:424–38. doi: 10.2307/1912791
47. Stokes PA, Purdon PL. A study of problems encountered in Granger causality analysis from a neuroscience perspective. Proc Nat Acad Sci. (2017) 114:E7063–72. doi: 10.1073/pnas.1704663114
48. Papagiannopoulou C, Gonzalez Miralles D, Decubber S, Demuzere M, Verhoest N, Dorigo WA, et al. A non-linear Granger-causality framework to investigate climate-vegetation dynamics. Geoscientific Model Dev. (2017) 10:1945–60. doi: 10.5194/gmd-10-1945-2017
49. Toda HY, Yamamoto T. Statistical inference in vector autoregressions with possibly integrated processes. J Econom. (1995) 66:225–50. doi: 10.1016/0304-4076(94)01616-8
50. Ngatchou P, Zarei A, El-Sharkawi A. Pareto multi objective optimization. In: Proceedings of the 13th International Conference on, Intelligent Systems Application to Power Systems. Arlington, VA: IEEE. (2005) p. 84–91.
51. Deb K, Pratap A, Agarwal S, Meyarivan T, A. fast and elitist multiobjective genetic algorithm: NSGA-II. IEEE Trans Evol Comput. (2002) 6:182–97. doi: 10.1109/4235.996017
52. Ku CC, Ng T-C, Lin H-H. Epidemiological Benchmarks of the COVID-19 Outbreak Control in China After Wuhan's Lockdown: A Modelling Study With an Empirical Approach. (2020). doi: 10.2139/ssrn.3544127
53. Flaxman S, Mishra S, Gandy A, Unwin H, Coupland H, Mellan T, et al. Report 13: Estimating the Number of Infections and the Impact of Non-pharmaceutical Interventions on COVID-19 in 11 European Countries. (2020).
Keywords: non-pharmaceutical interventions, COVID-19 pandemic, public health policymaking, multi-objective optimization, human mobility, multivariate time series analysis
Citation: Zhou X, Zhang X, Santi P and Ratti C (2023) Phase-wise evaluation and optimization of non-pharmaceutical interventions to contain the COVID-19 pandemic in the U.S. Front. Public Health 11:1198973. doi: 10.3389/fpubh.2023.1198973
Received: 02 April 2023; Accepted: 10 July 2023;
Published: 03 August 2023.
Edited by:
Ramy Mohamed Ghazy, Alexandria University, EgyptReviewed by:
Hani Amir, University of Annaba, AlgeriaCopyright © 2023 Zhou, Zhang, Santi and Ratti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiao Zhou, eGlhb3pob3VAcnVjLmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.