
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health , 06 November 2023
Sec. Public Health Education and Promotion
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1182582
 Tatjana Nemeth Blažić1*
Tatjana Nemeth Blažić1* Ivana Božičević2
Ivana Božičević2 Mirjana Lana Kosanović Ličina3
Mirjana Lana Kosanović Ličina3 Aleksandar Štulhofer4
Aleksandar Štulhofer4 Iskra Alexandra Nola2
Iskra Alexandra Nola2Introduction: The aim of this study was to determine self-reported human papillomavirus (HPV) vaccination status among emerging adults in Croatia, intention to get the HPV vaccine among unvaccinated individuals and correlates of HPV vaccine hesitancy.
Methods: Data were collected via a cross-sectional survey based on a probabilistic national sample. The sample included 1,197 individuals aged 18–25 years (50.6% were women) who were recruited from November 2021 to February 2022 as part of the commercial online panel. Analyses included 981 participants who correctly answered two “attention trap” questions using descriptive statistics and multivariate analyses. The data were post-hoc weighted for gender and age and adjusted for clustering effect. To adjust standard errors for the sampling design, multivariate analyses were carried out using the complex samples module in the IBM SPSS 27 statistical software package.
Results: Overall, 18.3% of participants (25.0% of women and 11.7% of men) reported that they were HPV vaccinated, while 21.9% did not know their HPV vaccination status. Of those vaccinated, 65.6% were women. The odds of being HPV-vaccinated were significantly higher among female participants. Among the unvaccinated, 35.4% expressed a willingness to get the vaccine. The odds of vaccination hesitancy were significantly lower among women, participants who reported a higher perceived risk of STIs, those who recognized that HPV could result in cervical cancer, and significantly higher among those who were more religious.
Conclusion: Our findings suggest a need to increase HPV vaccination uptake in Croatia through raising awareness about HPV vaccine effectiveness and also through the implementation of strategies to make vaccination more available.
Vaccination against human papillomavirus (HPV) is an important biomedical intervention for the prevention of HPV infection and associated cancers in women and men (1). HPV vaccination against the most common low- and high-risk HPV subtypes has been introduced in publicly funded HPV national immunization programs in many European countries since 2006 (2). Though there is strong evidence of HPV vaccination effectiveness, HPV vaccine hesitancy and low HPV vaccination coverage rates (HPV-VCR) remain a challenge (1).
In Croatia, HPV vaccination became available at the national level in 2007 for girls and women, aged 9–26 years, as an out-of-pocket payment. Some counties provided free HPV vaccinations for 13-year-old girls, accompanied by public campaigns (3, 4). Since 2016, HPV vaccination has been included in the national immunization program, covered by health insurance, and recommended for girls and boys aged 14–15 years. Starting in 2019, a catch-up campaign was introduced for all young, unvaccinated people aged up to 25 years. Since 2023, HPV vaccination has been recommended and offered on a voluntary basis to all children aged 10/11–14/15 years. Specialists in school and adolescent medicine actively recommend HPV vaccination to schoolchildren during their routine preventive activities. The catch-up free vaccination for individuals up to 25 years of age is available on request (3, 4). According to the unpublished implementation data of the Service for School Medicine of the Croatian Institute of Public Health, in the school year 2019/2020, 38% of the first-grade high school female students (aged 15–16 years) and 24% of the male students had been fully vaccinated.
HPV-VCRs in Croatia are not regularly monitored, unlike mandatory vaccinations that are included in the national immunization program during childhood and adolescence, where VCRs are set at 95% for all vaccinated cohorts. Therefore, population-based studies done at the national level can give much-needed information about the coverage of vaccination against HPV in the absence of routinely collected data.
The aim of this study was to determine self-reported HPV vaccination status against HPV in a population-based sample of emerging Croatian adults (young people aged 18–25 years), intention to get the vaccine among unvaccinated individuals and correlates of HPV vaccination and vaccine hesitancy.
The sample included 1,197 emerging adults aged 18–25 years (Mage = 21.7, SD = 2.21; 50.6% women). Two-stage stratified sampling by region (n = 6) and settlement size (n = 4) was used to randomly draw participants in the selected age range from a commercial panel database (n = 5,000) based on quotas for age, gender, and education from 19 November 2021 to 11 January 2022. The database, maintained by a range of international professional research companies, consisted of participants who were recruited to join the panel while taking part in national, probability-based, face-to-face, or phone surveys and those who joined through the agency's web portal. Panel membership is incentivized.
Considering the COVID-19 restrictions, a commercial panel was the most feasible and efficient recruitment method. The study response rate was 29%, and the questionnaire completion rate was 83%. After excluding participants who failed to correctly answer one or both “attention trap” questions, the sample was reduced to 981 participants (52.1% women). The basic sociodemographic characteristics of this analytical sample (n = 981) are presented in the Supplementary Table 1.
To be broadly representative of the respective population, the sample was weighted for gender and age based on the most recent (2021) census data by the Croatian Bureau of Statistics and adjusted for the clustering effect. The basic sociodemographic characteristics of this analytical sample (n = 976) are presented in Table 1.
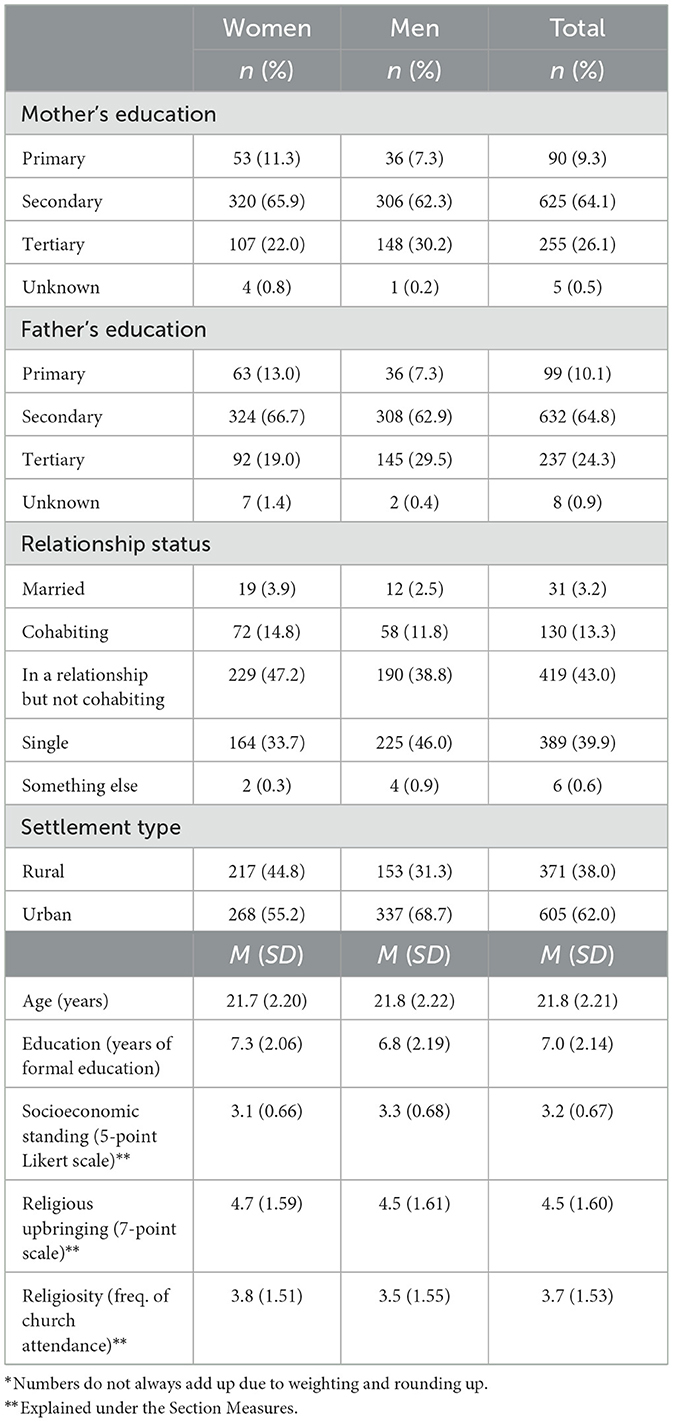
Table 1. Basic sociodemographic characteristics of the sample by gender (weighted data; n = 976)*.
The study was conducted as the third wave of a repeated cross-sectional national study on sexual and reproductive health in emerging adults (5). It entailed a behavioral and a biological part (testing for Chlamydia trachomatis, which will be reported on separately). Here, data from the behavioral part of the study are presented. Online recruitment was initiated with a letter announcing the study and its contents. To access the questionnaire, participants needed to provide informed consent. Following the completion of the questionnaire, we used incentives to increase the chance of a better response (increasing the response rate) and better data quality. Participants received a small token of appreciation for a completed questionnaire (5 EUR voucher). Participation in the biological part of the study was awarded with a 20-EUR voucher. All study procedures were approved by the Ethical Committees of Faculty of the Humanities and Social Science and the Croatian Institute of Public Health.
Dependent variables. Within the questionnaire, the HPV vaccination status (customarily takes place at the age of 14–15 years) was checked (investigated). Individuals who were either unvaccinated or could not remember being vaccinated were asked if they would like to “get vaccinated against HPV” (“yes”; “no”).
Independent variables. Participant's education (measured in years of formal education), comparative socioeconomic standing (answers were recorded on a 5-point Likert-like scale ranging from 1 = “my household income is much lower compared to most other households to 5 = “my household income is much higher compared to most other households”), relationship status (married or cohabiting, in a relationship but not cohabiting, and single), and religious upbringing (a 7-point scale ranging from 1 = “I was not brought up in a religious spirit” to 7 = “I was brought up to strictly follow religious principles” was used to explore family religiosity) were asked. Religiosity was assessed using a standard indicator of the frequency of attending religious ceremonies (1 = not religious, 2 = never… to 7 = almost every day). The self-assessed personal risk of acquiring sexually transmitted infections (STI) (1 = “the risk is negligible” to 10 = “the risk is extremely high”) was also queried. Basic knowledge about the potential consequences of HPV infection was indicated by the following question: “Is the protracted infection with HPV the main cause of cervical cancer?” (“no”; “yes”; and “I do not know”). Finally, settlement type (rural vs. urban) was included to control for possible differential availability of the HPV vaccine.
Following the description of HPV vaccination prevalence and the prevalence of vaccine hesitancy, two multivariate logistic regression analyses were carried out. The first explored correlates of ever being vaccinated against HPV and the second correlates with vaccine hesitancy (defined as not wanting to be vaccinated). Independent variables in the former regression analysis were demographic (age and gender) and family characteristics (parents' education and religious upbringing), while the latter included participants' socio-demographic characteristics, knowledge about HPV, religiosity, and self-assessed STI risks. To adjust standard errors for clustered sampling design, multivariate analyses were carried out using the complex samples module in the IBM SPSS 27 statistical software package. Very few missing information (<3%) was observed in the dataset, which is probably due to the fact that participants were contractual members of a commercial online panel (i.e., used to filling out questionnaires).
Less than one-fifth (18.3%) of participants, 25.0% of women and 11.7% of men from the sample, reported ever being vaccinated against HPV. Almost two-thirds of vaccinated individuals (65.6%) were women. Approximately one in every five participants (21.9%) was unable to recall their HPV vaccination status. There was no substantial gender difference in this lack of recall (p = 0.263).
Willingness to get the vaccine was reported by slightly over a third of non-vaccinated participants (35.4%; 37.5% of women and 33.4% of men). Men were significantly more reluctant to vaccinate against HPV compared to women [ = 12.02, p < 0.001, Cramer's V = 0.12].
The majority of sampled emerging adults (59.1%) knew about the link between HPV and cervical cancer. Of the rest, 36.1% reported that they did not know the answer. No significant gender difference in knowledge that HPV infection causes cervical cancer was observed (p = 0.612).
Next, the correlates of being vaccinated against HPV were assessed (Table 2). Participants who could not remember if they were ever vaccinated against HPV were excluded from the analyses. In the multivariate model, it was found that the odds of reporting being vaccinated against HPV were significantly higher in women compared to men [odds ratio (OR) = 2.46; 95% confidence interval (CI) 1.76–3.46; p < 0.001].
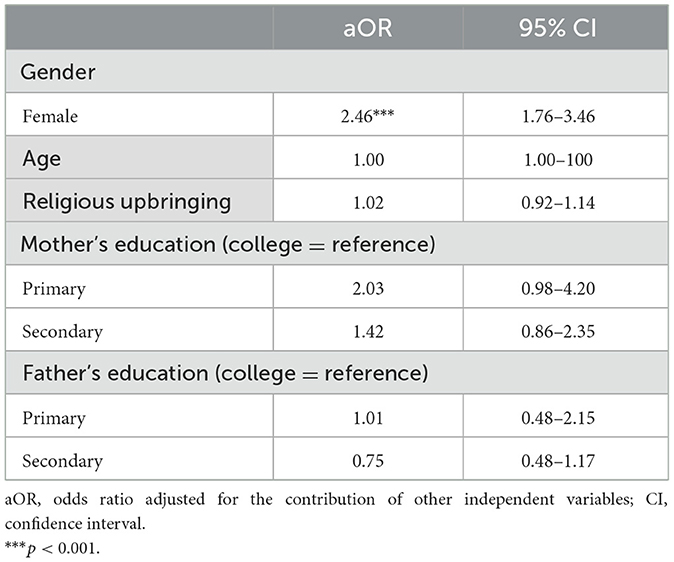
Table 2. Predictors and correlates of reporting ever being vaccinated against HPV (n = 751).
Finally, we explored the correlates of the HPV vaccine hesitancy (Table 3). Only sexually active participants were included in the analysis. In the adjusted model, the odds of vaccine hesitancy (i.e., the individual does not want to get vaccinated) were lower among female participants (aOR = 0.60, p < 0.001), individuals who believed that they were at higher STI risk (aOR = 0.89, p = 0.010), and those who knew that HPV causes cervical cancer (aOR = 0.66, p = 0.005). In contrast, higher religiosity substantially increased the odds of reporting vaccine hesitancy (aOR = 1.16, p = 0.001).
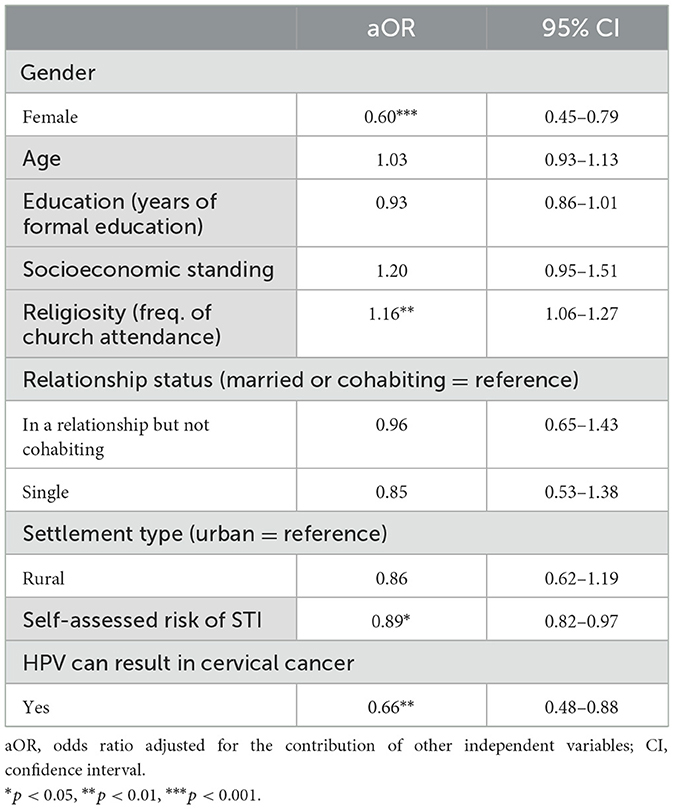
Table 3. Predictors and correlates of HPV vaccine hesitancy, Croatia (n = 809).
The results of this study indicate low self-reported uptake of HPV vaccination among emerging adults in Croatia and a high level of HPV vaccine hesitancy. By 2017, several European countries achieved a full course HPV vaccine coverage of over 70% in female individuals in target age groups: Iceland (12–13), the United Kingdom (11–13), Norway (12–13), Spain (12), and Sweden (10–12) (2, 6). Some countries geographically close to Croatia with a similarly organized healthcare system achieved a substantially higher HPV-VCR in 2017, such as Slovenia (46% target age 11–12 years), Czech Republic (58% target age 13 years), and Italy (62% target age 11 years) (2, 6). The most common determinants of HPV vaccine hesitancy identified in European countries include the quality and quantity of available information about the HPV vaccine and its safety, and the lack of trust in health authorities (7). This indicates a large need for improvement of HPV-VCR in Croatia.
Low perceived risk of contracting an STI as one of the correlates of HPV vaccine hesitancy in our study could be explained by perceived feelings of invulnerability, which characterize the period of adolescence (8). The association that we found between religiosity and vaccine hesitancy has been well-explained in the literature and includes concerns that vaccination will promote sexual disinhibition and sex before marriage among emerging adults (9, 10).
A large proportion of participants in this survey did not know whether they had been vaccinated or not, which suggests a possible low perception and awareness of vaccination benefits. Low vaccination uptake overall among respondents and lower HPV vaccination status reported among men, as well as their higher reluctancy to HPV vaccination, were identified in our study, pointing out the need for targeted intervention, e.g., educational peer workshops. One of the cornerstones is the promotion of HPV vaccination awareness and uptake among adolescents and young adults and their parents (11, 12), as well as the implementation of male-specific HPV campaigns emphasizing the double benefit of HPV vaccination (individual protection and transmission prevention). Campaigns should also be aimed specifically at emerging adults, given that they are at an age when they still could be vaccinated through catch-up programs, and also because the information that they obtain about HPV prevention could have an impact on their decision to vaccinate their children in the future (13).
Our study highlighted the HPV knowledge gaps and indicates the need for more thorough health education and awareness-raising strategies regarding HPV transmission and the consequences of HPV infection, targeting a general population and in particular emerging adults. Increases in HPV-VCR can be achieved in Croatia by addressing these knowledge gaps and increasing awareness about HPV vaccine effectiveness and its availability through school-based interventions, as well as efficient and innovative vaccine delivery strategies.
School-based interventions should include the provision of educational materials about the efficacy and safety of the HPV vaccine for parents, children, and teachers. During primary and secondary education in Croatia, the health education of children is provided by biology teachers and school medicine practitioners. Education on sexual health, however, is very limited and often considered controversial. Since evidence shows that additional parental education on the efficacy of HPV can increase vaccine uptake in children, specialists in school and adolescent medicine should increase their efforts to educate parents about the benefits of vaccination (11). Improvements in vaccine delivery strategies should include the implementation of online tools that facilitate vaccination scheduling, according to the national vaccination program (for all students aged 10/11–14/15 years), and obtaining parental consent.
Apart from its strengths, the current study also has some limitations. Although our population-based sample is broadly representative of the national 18–25 years age cohort, the question of whether members of commercial panels, who routinely participate in various (incentivized) surveys, may be specific in some way remains relevant, e.g., professional respondents vs. altruistic ones, in that sense as well (14). In addition, the fact that we assessed vaccination against HPV in retrospect entailed the risk of memory bias. Finally, the fact that data collection took place during the COVID-19 pandemic may have affected participants' self-assessment of STI risk exposure.
Given the potential public health ramifications of low HPV vaccination uptake, multidisciplinary approaches conducted in educational and healthcare settings should be undertaken to promote the benefits of the HPV vaccine for both women and men among parents and emerging adults, as well as to address misperceptions around vaccine side effects and effectiveness. HPV vaccination procedures with broader availability should be implemented. Further research is needed to elucidate the factors behind HPV vaccine hesitancy in Croatia, including associated social interaction, as that would additionally help in planning targeted interventions.
The current study provided the first population-level estimates of HPV vaccination coverage and HPV vaccine hesitancy in emerging Croatian adults. Its findings are of particular relevance for public health specialists and school and adolescent medicine practitioners who are responsible for vaccination against HPV. School settings should be used more effectively to raise awareness about the benefits of the HPV vaccine among students and their parents, as well as to scale up vaccination coverage in Croatia to reach the EU average.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Committee on Ethics Issues in Science and research of the Faculty of Humanities and Social Science, University of Zagreb, Zagreb, Croatia (Approval number 2019-14), and by the Ethical Committee of the Croatian Institute of Public Health, Zagreb, Croatia (Approval number 030-02/21-01/6−381-15-20-3). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
TNB, IB, AŠ, and IAN contributed to the conceptualization and design of the manuscript. AŠ, TNB, IB, and MK contributed to the conceptualization and the methodology of the study and participated in research implementation and data collection. IB and AŠ participated in organizing the database, performed the statistical analysis, and results validation. TNB wrote the first draft of the manuscript. AŠ was responsible for investigation, data curation, and funding acquisition. All authors contributed to manuscript revision and editing, and have read and approved the submitted version.
This work was funded by the Croatian Science Foundation, Research Project IP-2019-04 (Grant No. IP-2019-04-3609). Funding for biological part of the study (testing for Chlamydia trachomatis infection) was partly supported by the Croatian Institute for Public Health.
The authors would like to express their gratitude to Goran Koletić and Ivan Landripet for their help with data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1182582/full#supplementary-material
1. WHO. Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem. Geneva: World Health Organization (2020). Available online at:https://www.who.int/publications/i/item/9789240014107 (accessed January 9, 2022).
2. Nguyen-Huu NH, Thilly N, Derrough T, Sdona E, Claudot F, Pulcini C, et al. Human papillomavirus vaccination coverage, policies, and practical implementation across Europe. Vaccine. (2020) 38:1315–31. doi: 10.1016/j.vaccine.2019.11.081
3. Croatian Institute for Public Health. Vaccination Against Human Papilloma Virus (in Croatian). (2022). Available online at: https://www.hzjz.hr/sluzba-skolska-medicina-mentalno-zdravlje-prevencija/cijepljenje-protiv-humanog-papiloma-virusa-hpv/ (accessed February 6, 2022).
4. Posavec M. HPV vaccination in the Republic of Croatia. Paediatr Croatica (in Croatian). (2018) 62:48–51. doi: 10.13112/PC.2018.8
5. Landripet I, Stulhofer A, Bacak V. Changes in human immunodeficiency virus and sexually transmitted infections-related sexual risk taking among young Croatian adults: 2005 and 2010 population-based surveys. Croat Med J. (2011) 52:458–68. doi: 10.3325/cmj.2011.52.458
6. Bruni L, Diaz M, Barrionuevo-Rosas L, Herrero R, Bray F, Xavier Bosch F, et al. Global estimates of human papillomavirus vaccination coverage by region and income level: a pooled analysis. Lancet Global Health. (2016) 4:E453–63. doi: 10.1016/S2214-109X(16)30099-7
7. Karafillakis E, Simas C, Jarrett C, Verger P, Peretti-Watel P, Dib F, et al. HPV vaccination in a context of public mistrust and uncertainty: a systematic literature review of determinants of HPV vaccine hesitancy in Europe. Hum Vaccin Immunother. (2019) 15:1615–27. doi: 10.1080/21645515.2018.1564436
8. Štulhofer A, Jureša V, Mamula M. Problematic pleasures: risky sexual behavior in late adolescence (In Croatian) Druš. Istraž Zagreb. (2000) 9:867–93.
9. Repalust A, Sevic Š, Rihtar S, Stulhofer A. Childhood vaccine refusal and hesitancy intentions in Croatia: insights from a population-based study. Psychol Health Med. (2017) 22:1045–55. doi: 10.1080/13548506.2016.1263756
10. Redd DS, Jensen JL, Hughes SJ, Pogue K, Sloan-Aagard CD, Miner DS, et al. Effects of religious practice and teachings about sexual behavior on intent to vaccinate against human papillomavirus. Vaccines. (2022) 410:397. doi: 10.3390/vaccines10030397
11. Belavic A, Pavic Simetin I. Educational intervention for increasing knowledge of human papillomavirus and vaccination amongst parents of first year high school students in Croatia. J Public Health. (2022) 44:165–73. doi: 10.1093/pubmed/fdaa201
12. Dilley SE, Peral S, Straughn, JM, Scarinci IC. The challenge of HPV vaccination uptake and opportunities for solutions: lessons learned from Alabama. Prev Med. (2018) 113:124–31. doi: 10.1016/j.ypmed.2018.05.021
13. Ganczak M, Owsianka B, Korze M. Factors that predict parental willingness to have their children vaccinated against HPV in a country with low HPV vaccination coverage. Int J Environ Res Public Health. (2018) 15:645. doi: 10.3390/ijerph15040645
Keywords: HPV, HPV vaccination, self-reported HPV vaccination status, vaccine hesitancy, emerging adults, Croatia
Citation: Nemeth Blažić T, Božičević I, Kosanović Ličina ML, Štulhofer A and Nola IA (2023) Self-reported HPV vaccination status and HPV vaccine hesitancy in a nationally representative sample of emerging adults in Croatia. Front. Public Health 11:1182582. doi: 10.3389/fpubh.2023.1182582
Received: 09 March 2023; Accepted: 29 September 2023;
Published: 06 November 2023.
Edited by:
Charles Darkoh, University of Texas Health Science Center at Houston, United StatesReviewed by:
Ernest Groman, Medical University Vienna, AustriaCopyright © 2023 Nemeth Blažić, Božičević, Kosanović Ličina, Štulhofer and Nola. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tatjana Nemeth Blažić, dGF0amFuYS5uZW1ldGgtYmxhemljQGh6anouaHI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.