 Kathryn M. Yount1*
Kathryn M. Yount1* Dawn Comeau2Sarah C. Blake3
Dawn Comeau2Sarah C. Blake3 Jessica Sales2
Jessica Sales2 Michael Sacks4
Michael Sacks4 Hannah Nicol5Irina Bergenfeld1Ameeta S. Kalokhe5Aryeh D. Stein1
Hannah Nicol5Irina Bergenfeld1Ameeta S. Kalokhe5Aryeh D. Stein1 Daniel J. Whitaker6Dominic Parrott6
Daniel J. Whitaker6Dominic Parrott6 Hoang Thi Hai Van7
Hoang Thi Hai Van7- 1Hubert Department of Global Health, Rollins School of Public Health, Emory University, Atlanta, GA, United States
- 2Department of Behavioral, Social, and Health Education Sciences, Rollins School of Public Health, Emory University, Atlanta, GA, United States
- 3Department of Health Policy and Management, Rollins School of Public Health, Emory University, Atlanta, Georgia
- 4Goizueta Business School, Emory University, Atlanta, GA, United States
- 5School of Medicine, Emory University, Atlanta, GA, United States
- 6Georgia State University, Atlanta, GA, United States
- 7Hanoi Medical University, Hanoi, Vietnam
Background: Gender-based violence (GBV) and violence against children (VAC) are two prevalent and highly interconnected global health challenges, yet data and research capacities to study these forms of violence and to generate evidence-based policies and programs remain limited. To address critical shortages in research capacity in Vietnam and to establish a model for other Low- and Middle-Income Countries (LMICs), we are establishing CONVERGE—the Consortium for Violence Prevention Research, Implementation, and Leadership Training for Excellence.
Methods: Based on a needs assessment with partners in Vietnam, CONVERGE will provide a comprehensive research training program supporting 15 long-term, postdoctoral trainees with multi-disciplinary research training in GBV and VAC. We also will offer in-country trainings and short-courses to 40 short-term mid-career academic trainees and 60 short-term practitioner/stakeholder trainees over 5 years to build productive GBV and VAC academic, scientific, and practitioner networks. The CONVERGE training program has four components: (1) 14 h of virtual/in-person annual mentorship training to prepare research mentors and to create a pipeline of future mentors in Vietnam; (2) a one-month intensive research training for long-term postdoctoral fellows at Emory University; (3) a structured 17-month, in-country mentored research project for long-term trainees that results in a peer-reviewed manuscript and a subsequent grant submission; and, (4) week-long in-country intensive translational trainings on implementation science, advanced topics in leadership, and advanced topics in science dissemination. Opportunities for on-going virtual training and professional networking will be provided for CONVERGE trainees and mentors in Vietnam with other trainees and mentors of D43s focused on injury/violence prevention, D43s housed at Emory, and D43s with other institutions in Southeast Asia. To assess the reach, implementation, fidelity, and effectiveness of these four components, we will implement a rigorous, mixed-methods, multi-level evaluation strategy using process and outcome measures. Findings from the evaluation will be used to refine program components for future trainee and mentor cohorts and to assess long-term program impact.
Discussion: Led by Emory University in the US and Hanoi Medical University in Vietnam, CONVERGE represents leading institutions and experts from around the world, with a goal of providing mentorship opportunities for early-career scientists with an interest in violence prevention.
Introduction
Gender-based violence (GBV) entails any harmful act perpetrated against a person’s will because of their biological sex or gender presentation (1, 2). Acts of GBV inflict physical, sexual, mental, or economic harm, threats of harm, coercion, or other deprivations of liberty in public or private. Violence against children (VAC) includes all forms of violence against people under age 18 years, whether by parents or other caregivers, peers, romantic partners, or strangers. When directed against girls or boys because of their biological sex or gender presentation, acts of VAC are forms of GBV. Common forms of GBV against women, girls, and trans-gender or gender-non-conforming (TGNC) persons include intimate partner violence (IPV) (3–6) and homicide (7, 8), sexual violence (4–6, 9), harmful practices like child, early, or forced marriage (CEFM) (10), honor crimes (11), and human trafficking (12). GBV and VAC are important to consider jointly because they may share risk factors (13–21), often co-occur in households, are linked over the life course (15, 18, 22), can have common and compounding consequences over the life course, can have inter-generational effects, and can co-occur in adolescence, when vulnerability to violence is heightened. Moreover, GBV and VAC are related to a host of negative outcomes as either a cause or consequence, including mental health outcomes, such as depression or anxiety; physical health outcomes, such as immediate injury and long-term physical health problems such as cancer or diabetes; and behavioral health outcomes, such as substance use or unsafe sexual practices (23–27). Thus, GBV and VAC are “hub” foci, such that capacity building to strengthen related scholarship and public health responses will likely have positive ripple effects well beyond the prevention of violence.
Despite the global burden of GBV and VAC, data and research capacities to study these forms of violence and to generate evidence-based policies and programs remain limited (6). Our objective is to address critical shortages in research capacity in Vietnam, where political will is high to expand capacity for research and programs on GBV and VAC and to become a model for other LMICs. We will train mentors, post-doctoral researchers, and practitioners involved in studying and addressing GBV and VAC. To achieve this objective, we have established CONVERGE—the Consortium for Violence Prevention Research, Implementation, and Leadership Training for Excellence. Collaborating institutions are led by Emory University (United States, US) and Hanoi Medical University (HMU, Vietnam) and include the following partners in Atlanta and Vietnam: Georgia State University; the Division of Violence Prevention, Center for Injury Prevention and Control, Centers for Disease Control and Prevention; Haiphong University of Medicine and Pharmacy (UMP); Hue UMP; Ho Chi Minh City UMP. CONVERGE draws on and expands successful training initiatives between Emory University and institutions of excellence in Ethiopia (D43TW009127), Georgia (D43TW007124), India and Ethiopia (D43TW011404), and Nigeria (D43TW010934) for building research and leadership capacity while tailoring curricula to address the identified needs of universities in Vietnam. Our training initiative has three specific aims:
Aim 1: To cultivate a diverse group of mentors for research on GBV and VAC in Vietnam by implementing a formal mentorship program that trains productive researchers to be strong scientific and professional mentors (15 early-career long-term trainees; 40 mid-career short-term trainees). This mentorship program will strengthen CONVERGE mentoring teams and institutional capacity in Vietnam.
Aim 2a: Strengthen research capacity and enhance human capabilities for robust GBV and VAC research in Vietnam by providing long-term post-doctoral research training and career opportunities to a diverse group of researchers with exceptional potential (15 early-career long-term trainees).
Aim 2b: Strengthen capacity to fast-track the translation of evidence into practice by providing in-country short-courses on implementation science, leadership, and science dissemination that connect scholars and practitioners (15 early-career long-term trainees; 40 mid-career short-term trainees; 60 practitioners).
Aim 3: Implement a training evaluation plan that assesses the reach, implementation, fidelity, and effectiveness of our four short- and long-term training program components. We will use these findings iteratively to improve the program in real time, and thereby, to maximize favorable individual and institutional impacts.
Our program aligns with national research priorities of Vietnam (28) and leverages over 12 years of collaboration between Emory University and partners in Vietnam, demonstrating the feasibility of achieving our aims. Our empowerment-based approach (29) to mentorship training will create a pipeline of early- and mid-career researchers who are skilled mentors. Our long-term post-doctoral research training is grounded in successful integrated, interdisciplinary training programs with Emory University and other partners and meets identified needs in Vietnam. Our implementation science, leadership, and science dissemination short courses address identified gender gaps in leadership training (30), build on Emory’s successful leadership programs (D43TW009135), and will accelerate the translation of evidence into practice. Our training plan addresses the priorities of several divisions within the National Institutes of Health (NIH) related to women’s health, child health and human development, mental health, minority health and health disparities, alcohol abuse and alcoholism, drug abuse, and general medicine.
CONVERGE members are energized to meet the demand for violence-prevention research, implementation, and leadership training in Vietnam. Over the program period, we expect to train a critical mass of 115 research mentors, post-doctoral scholars, and practitioners in Vietnam in GBV and VAC research, implementation, and leadership. Through successful strategies tested in our prior training programs, we will promote high trainee retention and strengthen institutional capacity in Vietnam. In doing so, we will prepare a consortium of universities in Vietnam to conduct locally relevant GBV and VAC research, training, and best practice that shapes national research and program priorities into the twenty-first century.
Burden of GBV and VAC in low- and middle-income countries
Estimated rates GBV and VAC are high worldwide (3, 8, 9, 31), but the burden is disproportionate in LMICs. First, 89% of the world’s 3.19 billion youth 0–24 years live in LMICs (31, 32). Among 2–17-year-olds in 2014, 1.35 billion children in LMICs and 135 million in high income countries (HICs) were exposed to any violence, and rates of any violence were higher in LMICs (78% vs. 60%) (31). Second, some gendered forms of VAC—such as the CEFM of girls—are more common in LMICs (11, 33). Third, exposure to gendered and non-gendered violence in childhood increases the risks of revictimization (34), poly-victimization (35, 36), and perpetration (7, 18, 22, 37–41) in adulthood and inter-generationally (42). Fourth, violence against TGNC persons is understudied in LMICs, but limited data from HICs suggest that child abuse, early stigma and discrimination, and physical or sexual violence may be as or more common in TGNC persons than in cisgender persons, whose gender identity matches their assigned sex at birth (43). Fifth, VAC and GBV at all ages have cumulative and intersecting mental, physical, and behavioral sequelae (42, 44), some of which are more common or specific to women, girls, and TGNC persons (45). Such sequelae include poor mental health; suicidal ideation and behavior; depression and posttraumatic stress; eating disorders (46), number of sexual partners; sexually transmitted infections, including HIV; unwanted or unplanned pregnancy and abortion; and poor maternal and child health outcomes (47). Thus, despite limited data on many forms of VAC and GBV, larger numbers of youth and some evidence of higher risk create a heavy burden of VAC, GBV, and their intersecting sequelae in LMICs.
Common social ecology of GBV and VAC: rationale for early, integrated intervention
According to socio-ecological theories (13, 14, 48), nested inequalities in power and control as well as norms of masculine dominance influence multiple forms of GBV and VAC (Figure 1). This framework supports an integrated approach to study these forms of violence, noting common and specific multilevel risk factors for victimization and/or perpetration. Individual-level factors include early exposure to violence, situational factors, such as alcohol or substance use, poor mental health, low victim empathy, and for TGNC persons, early stigma and discrimination (18, 38, 42, 49, 50). Interpersonal factors include low relationship quality characterized by power and control, household poverty and low family support, peer-networks that condone violence, and for TGNC persons, heightened social isolation (38, 42, 51). Community-level factors include living in a socio-economically disadvantaged neighborhood with low collective efficacy, high violent crime, norms accepting of gender inequality and violence (15, 18, 19, 42, 52, 53), and for TGNC persons, cis-normativity. Also important at the community level are factors in schools (54) and workplaces (55), such as organizational tolerance for GBV or VAC, gender and other occupational inequalities, and weak or absent anti-discrimination policies, prevention and response programs, bystander training, and leadership training. Societal or national factors include laws, policies, and systems that privilege cismen, that limit opportunities for women and TGNC persons, and that promote narrow definitions of GBV or VAC, rigid gender norms and norms of masculinity tied to dominance and honor, and acceptance of interpersonal violence (21, 42, 56, 57). Global factors include the internet, which may increase access to education and prevention programs as well as exposure to violent sexually explicit material, cyber-bullying, cyber-stalking, and sexual exploitation (58, 59). Other global factors include international displacement, which may elevate the risks of GBV and VAC by weakening community cohesion (60); international treaties and organizations that support the diffusion of anti-GBV and anti-VAC norms and practices (61, 62); and economic liberalization, which may elevate organized crime and, in turn, the diffusion of criminal laws against human trafficking in economically interdependent countries (63). Thus, GBV and VAC share many risk factors across the social ecology (42), and early integrated interventions targeting shared risks may help to prevent both forms of violence.
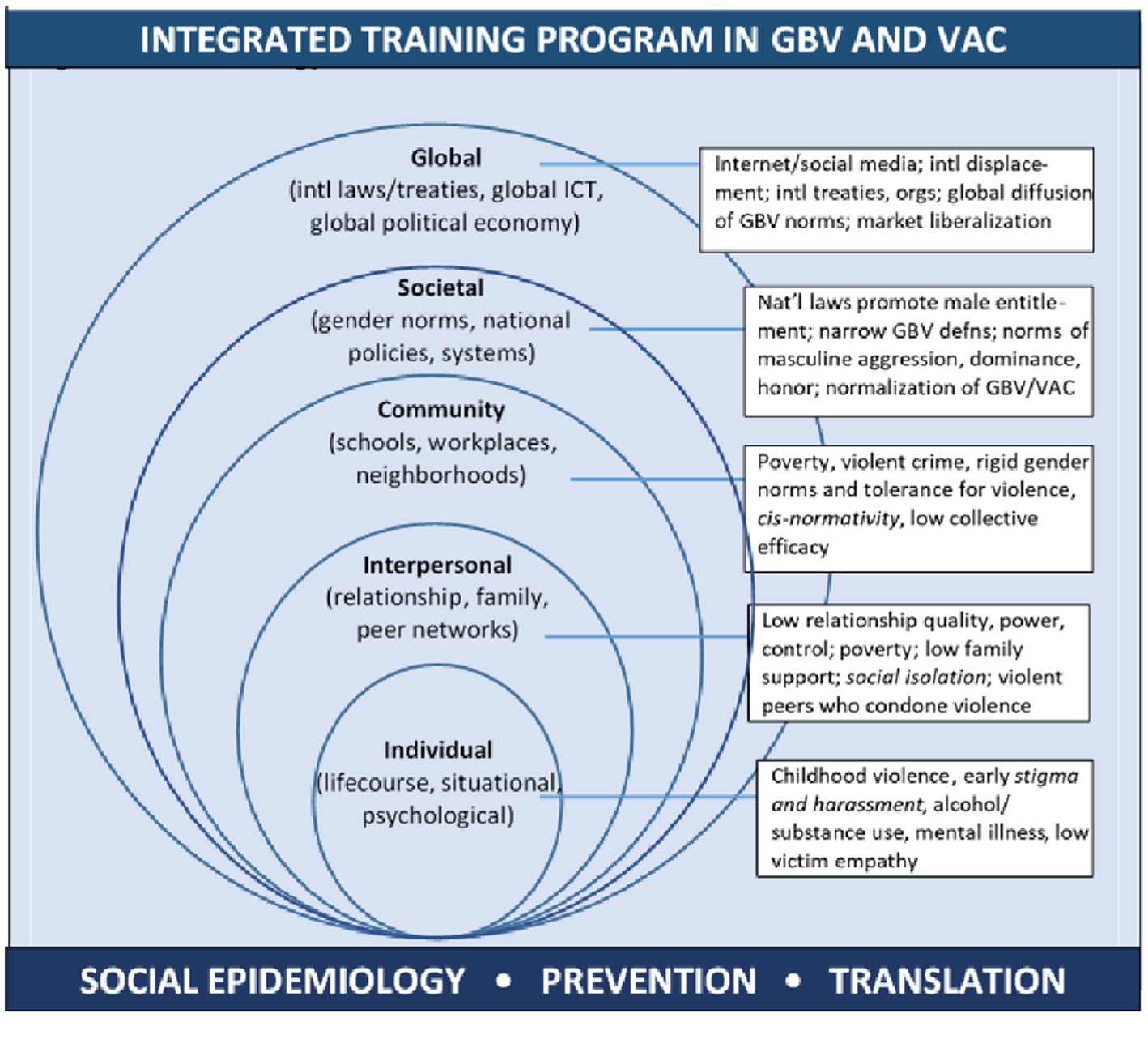
Figure 1. Socio-Ecological Model of Common Risk Factors for Gender-Based Violence and Violence against Children.
Research gaps in LMICs
Recognizing the global burden of GBV and VAC, the 2015 Sustainable Development Goals (SDGs) called on national governments to eliminate all forms of violence against women and girls (SDG5.2), harmful practices such as CEFM (SDG5.3), as well as abuse, exploitation, trafficking, and all forms of violence against children (SDG16.2) (64). This call has prompted a need for valid measures to monitor all forms of GBV (65, 66) and VAC (31) and to understand what works to prevent these forms of violence. Despite increased attention to GBV, research has come largely from HICs, which may or may not apply to LMICs. In LMICs, research on GBV has focused on adult women in urban settings and selected regions (Africa, South Asia), leaving the experiences of adolescent girls, young women, TGNC persons, and entire regions underexplored (36). Studies also focus on certain forms of GBV (e.g., IPV and non-partner sexual violence), lack attention to poly-victimization, use variable, unvalidated measures, and focus prevention programs on single forms of GBV (36, 46, 67). Likewise, despite increasing data collection on VAC, internationally agreed standards of measurement are lacking (68), and the quality of data is uneven. Moreover, reliance on partial definitions of VAC (69) and oversight of hard-to-measure forms (70) likely result in under-estimates of exposure. Attention to social variation in the burdens of VAC or GBV also is limited. Measures to ensure the rigorous implementation of study protocols and to safeguard the protection of participants are lacking (68). As a result, few national research institutes in LMICs have the technical expertise to collect data on GBV and VAC (68).
Asia Pacific and Vietnam: high prevalence of GBV and VAC but capacity and data gaps
Based on available data from Vietnam (71), lifetime (63%) and prior-year (32%) IPV is common in women 15–64 years. From 2010 to 2019, women’s reports of lifetime physical IPV declined (32–26%), but their reports of lifetime sexual IPV increased (10–13%), especially in women 18–24 years (5–14%). Half of women who report marital IPV never tell anyone, and few (10%) seek formal help. Of women who report physical IPV in marriage, 61% report their child witnessed or overheard the violence, and report behavioral problems in their child (5–12 years) more often than women not reporting physical IPV.
Outside of intimate partnerships, more than 4% of women report child sexual abuse before age 15 years. One in 10 women (11%) report non-partner physical violence since age 15 years, the majority (61%) of whom report a male relative as the perpetrator. Nearly one in 10 women (9%) report non-partner sexual violence since age 15, mostly perpetrated by non-family male acquaintances, co-workers, or strangers. High and increasing rates of some forms of intimate-partner, child, and non-partner violence against women may reflect changing exposure and more openness to discuss sex and sexual violence. Violence against women costs Vietnam an estimated 1.8% of gross domestic product (GDP) and profound individual consequences: 23% who experience physical and/or sexual IPV report physical injuries. Women victims more often than non-victims have a husband who was beaten as a child or whose mother was beaten.
In Vietnam, research on VAC is uncommon. More widely, according to the 2019 Global School-based Student Health Survey in Viet Nam (72), a decline was observed between 2013 and 2019 in the percentage of physical attacks, physical fights, and bullying at school (from 21 to 10% for attacks; from 17 to 8% for fights; and from 23 to 6% for bullying). However, according to the Ministry of Labour, Invalids, and Social Affairs, more than 4,000 children were abused between June 2019 and June 2021 (73). Of these cases, about 90% were girls, more than 66% were children 13–16 years old, and over 293 were children under age 6 years. Based on our research outside Hanoi, 75% of men experience violence in childhood and/or exposure to IPV, and their odds of IPV perpetration (74) and sexually violent behavior (75) increase with such exposure. Across East Asia and the Pacific, the economic loss from DALYS attributable to child maltreatment is an estimated $206 billion in 2012 dollars, or 2% of aggregate GDP (76), and is highest in the Western Pacific region, including Vietnam, at 3% of GDP (76).
Research on TGNC persons in the region is limited, but practices of gender variance, gender pluralism, and non-normative sexualities have long histories in Southeast Asia and Vietnam. These histories are shaped by ethnicity, spirituality, colonialism, HIV-related public-health campaigns, and legal recognition of the rights of gender-variant persons (77). Given the higher lifetime risk of adversity among sexual-minority than non-sexual-minority men (78), and the intersectional stigma experienced by gender-non-conforming, sexual-minority women (79) in parts of Southeast Asia, violence research that jointly considers the intersection of gender and sexuality is needed in Vietnam and the region.
Needs assessment
Thus, despite the high burdens of GBV and VAC in Vietnam, infrastructure and opportunities for interdisciplinary, integrated research training are nascent. Our history of collaboration in Vietnam and informal needs assessments with HMU revealed several research-training gaps (Table 1). Developing investigator capacity at the post-doctoral level is a critical pipeline to address these needs, and combined with strengthening mentorship capacity, is a powerful strategy toward building institutional capacity for research and programming in violence prevention.
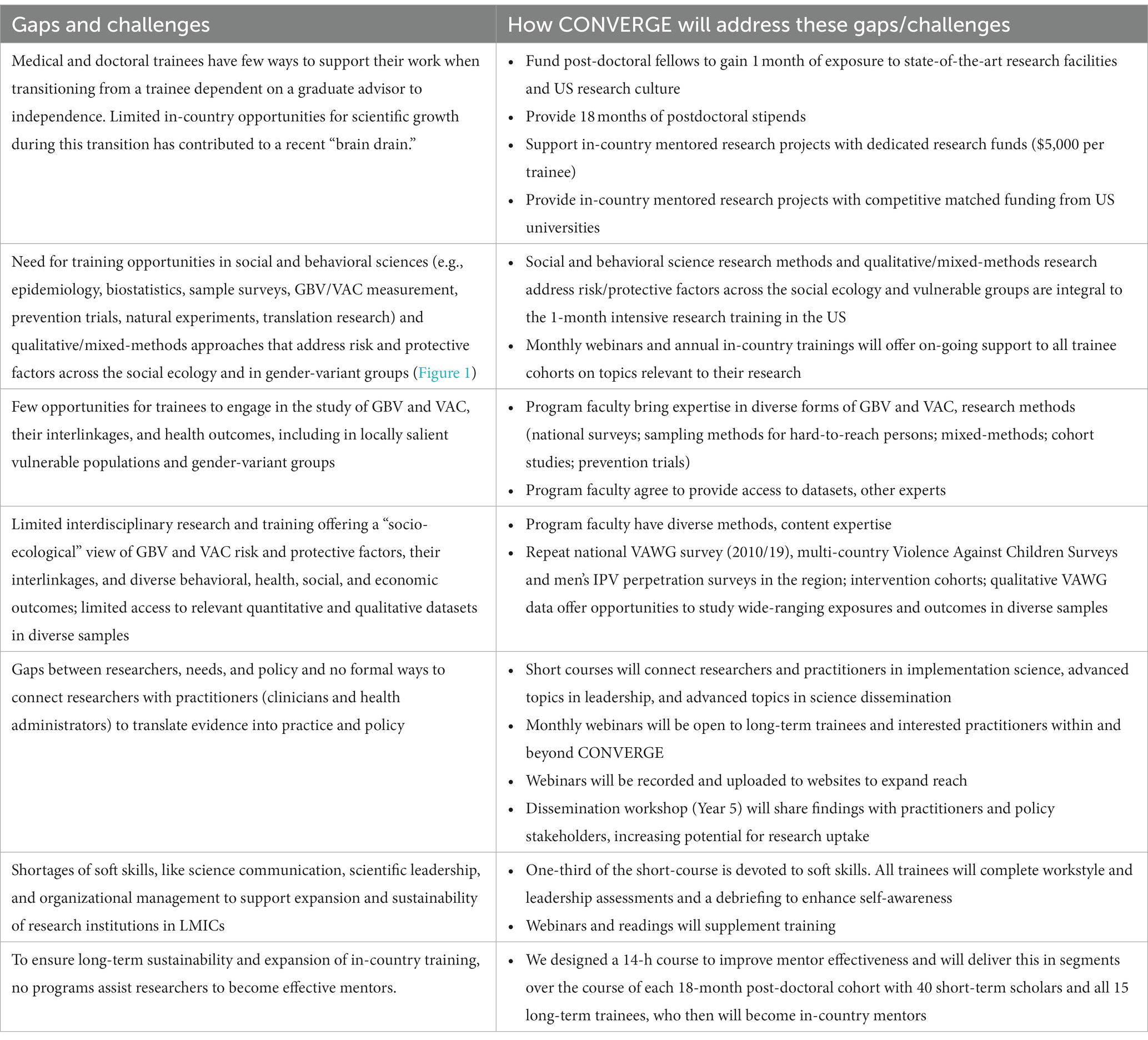
Table 1. Needs and challenges researching gender-based violence and violence against children in Vietnam.
Feasibility: adapting prior training successes
To strengthen research training in the long term, retaining skilled investigators in-country is essential. Emory University has shown through its other D43 training grants the feasibility of training and retaining research scholars in-country by offering them quality opportunities for research and career development (D43HD065249, D43TW009135, D43TW009127, D43TW007124). The present D43 applies this institutional learning and critical design innovations, such as: a revised mentor-training program that engages in-country mentors over the course of each of three 18-month post-doctoral fellowship training periods; competitive funding for follow-on research projects and research-dissemination activities; foundational and advanced training in leadership that is attentive to cross-cultural issues of diversity, equity, and inclusion; the seamless integration of graduates from our long-term post-doctoral training program into an expanding network of CONVERGE mentors; co-hosting of trainee and mentor training opportunities that facilitate cross-cultural learning and networking across D43 training programs at Emory, in Southeast Asia, and focused on violence prevention; and a comprehensive and rigorous plan to evaluate the reach, fidelity, effectiveness, and public-health impact of the program. Together, these innovations are designed to develop a cadre of early-career scientific leaders; an expanded network of scientific mentors; multi-institutional scientific capacity; and translational public-health impact in Vietnam.
Methods/Design
Converge global training program and program evaluation
Administrative structure
CONVERGE is a collaboration of partners with expertise in GBV and/or VAC at universities and scientific agencies in the US, Vietnam, and internationally. The primary institution in the US is Emory University, and US partner institutions include Georgia State University and the Division of Violence Prevention, Center for Injury Control and Prevention, Centers for Disease Control and Prevention (CDC). In Vietnam, the primary partner is Hanoi Medical University (HMU), and consortium partners include Haiphong University of Medicine and Pharmacy (UMP), Ho Chi Minh UMP, and Hue UMP. Other international partners are based in Europe and South Africa (Figure 2).
CONVERGE has assembled a world-class, diverse, and interdisciplinary Executive Committee and Program Faculty (Figure 2). The leadership team brings multi-disciplinary and complementary expertise, and extends a successful collaboration since 2010 between the PI at Emory University and institutions in Vietnam, which has expanded opportunities for early-career and senior investigators. The Executive Committee includes Program Directors providing programmatic leadership and oversight following a Multi-Program Director Leadership Plan. The PI and Program Director at Emory ensures adherence to program vision, grant management, financial accountability, and reporting to NIH. The MPI and co-Director at HMU oversees the recruitment of all long-term and short-term trainees, identification of appropriate in-country research mentors, in-country mentored research training, coordination of partner universities in Vietnam, and annual in-country trainings with long-term trainees, mentors, and practitioners. The Director for Research oversees the review and selection of long-term post-doctoral applicants, the matching of selected trainees with primary US mentors and mentoring teams, and research progress of each long-term trainee. The Director for Training oversees the one-month post-doctoral training intensive at Emory, mentorship training, and monthly journal-club webinars for long-term trainees. The Director of Evaluation oversees a comprehensive, mixed-methods evaluation plan for the entire training program. A collaborating investigator at HMU partners on all training and research activities, and early-career representatives from the US and Vietnam participate in programming and have opportunities for career-development on the CONVERGE Executive Committee.
To support this leadership team, a Training Advisory Committee (TAC) includes members from Atlanta-based institutions, Vietnam-based institutions, and international institutions. The CONVERGE TAC includes global experts in research on women’s health, GBV, VAC, and strategies to prevent injury and violence in LMICs. Members of the TAC were selected for their experience as current Directors of NIH-funded D43 training grants and/or Centers for research and training in the U.S., Vietnam, and globally. A women’s leadership sub-committee of the TAC monitors the selection and progress of women trainees to ensure the successful completion of their training program and opportunities for leadership development.
Program overview
CONVERGE provides a comprehensive research training program to support 15 long-term, postdoctoral trainees with multi-disciplinary research training in GBV and VAC. We also offer in-country trainings and short-courses to 40 short-term, mid-career academic trainees and 60 short-term practitioner/stakeholder trainees over 5 years (n = 115) to build productive GBV and VAC academic, scientific, and practitioner networks in Vietnam. Training components are based on the needs assessment conducted with partner institutions in Vietnam.
The CONVERGE research training program has four components: (1) an annual three-day mentorship training to prepare research mentors to build local mentoring capacity, effective and sustainable mentoring relationships, and a pipeline of future mentors in GBV and VAC in Vietnam; (2) a one-month multi-disciplinary intensive research training at Emory University that provides long-term trainees opportunities to acquire skills and expertise in rigorous, state-of-the-art, and reproducible research methodologies in GBV and VAC research; (3) a structured 17-month, in-country mentored research project for long-term trainees to apply state-of-the-art methods in GBV and VAC research to their project that results in a peer-reviewed manuscript and a grant submission to support the next phase of their research careers; and (4) a week-long in-country intensive translational training on implementation science, leadership, and research dissemination for long-term and short-term trainees to strengthen capacity and build networks between science and practice communities. These training initiatives will increase the number of scientists and health professionals who are able to implement rigorous GBV and VAC research and evidence-based programming at their home institutions as well as throughout national and global GBV and VAC research and professional networks. Based on our needs assessment, the CONVERGE training program is unique and offers training opportunities not yet available from in-country institutions or other externally funded training programs at our partner institutions. Moreover, training is developmentally appropriate for post-doctoral researchers, with the anticipation of building impactful careers as scientific investigators.
Below, program components are reviewed sequentially in their expected order of implementation: (1) selection and training of long-term post-doctoral trainees, (2) training of in-country research mentors, and (3) translational trainings and program evaluation.
Phase 1: long-term postdoctoral training eligibility, recruitment, and selection
Phase 1a: eligibility
A core aim of our training program is to build research capacity and enhance human capabilities for robust GBV and VAC research in Vietnam by providing long-term post-doctoral research training and professional opportunities to a diverse group of early-career researchers. Over the five-year program, we aim to support 15 post-doctoral research scholars across three cohorts. Eligible long-term trainees include early-career faculty, post-doctoral fellows, or PhD-level scientists at a partner institution in Vietnam who seek to obtain didactic and experiential, mentored training foundational for a research career in GBV or VAC. Long-term trainees are selected with attention to: (a) academic and research-related qualifications, (b) quality of the match with institutional and mentored support; (c) commitment to research on GBV or VAC; (d) inclusion of under-represented scientists (e.g., on gender, ethnicity); (e) disciplinary balance; and (f) balanced recruitment to create “clusters of capacity” across partner institutions. Candidate qualifications include a minimum of MD and/or PhD degree or equivalent, passion and commitment to research on GBV or VAC, quantitative or qualitative and critical analysis skills, aptitude for interdisciplinary and collaborative work, and commitment to reduce violence among vulnerable populations in Vietnam. When possible, trainees are selected to balance research interests that span the areas identified as gaps in Vietnam and within Vietnamese institutions (Table 1).
Phase 1b: recruitment
The team’s in-country MPI/co-Program Director oversees the recruitment of all trainees, with attention to the aforementioned criteria (Phase 1a). Each year, opportunities for long-term post-doctoral-level training are advertised widely through in-country advertisements, websites, listservs, word of mouth, and the extensive networks of the MPIs, in-country mentors, and current long-term trainees at partner institutions in Vietnam. Attention is given first to potential candidates at partner institutions, to strengthen individual and institutional research capacity with our core partners. Candidates from other institutions who have the appropriate institutional support and commitment to the field also are considered. Advertisements target candidates who are committed to continue GBV- and VAC-related topics in Vietnam. To expedite the recruitment and selection of the first cohort of trainees, partner institutions identified potential individuals at their institutions at the application stage of this training program.
Phase 1c: application and selection process
All cohorts of long-term trainee candidates are selected competitively using an application process adapted from existing Emory D43 training programs. Applications are completed in English, the language of most international biomedical, social science, and public health journals. All applications require a: (1) Curriculum Vita, (2) responses to a short demographic and informational survey, (3) letter of support from the applicant’s home institution, (4) letter of recommendation from a local research mentor, and (5) short statement of interest and one-page research proposal. Letters of recommendation should come from faculty in a graduate education program who are current or former supervisors and potential program mentors and should describe why the applicant is a strong candidate for the CONVERGE program. The institutional letter of support should describe the quality and relevance of research conducted at the institution, express commitments to support the trainee throughout the program, and outline a strategy to support the trainee’s integration into a research position upon completion of the program. The statement of interest and research proposal should describe their interest in GBV/VAC research, outline a hypothesis-driven research question on GBV/VAC they wish to pursue during the training period, and describe the data they plan to collect and analyze, timeline, and a statement of the study’s feasibility. Because written and oral proficiency in English is necessary for this training program, all finalists interview with the review committee and respond to questions about their training and research proposal.
The CONVERGE Director for Research (DR) facilitates the selection process for each long-term trainee cohort. For each admission cycle, the DR invites reviewers from the CONVERGE Executive Committee or the extensive pool of program faculty. Reviewers screen each application. Applications are scored and ranked using a modified NIH-style trainee grant scoring system (Supplemental material). Reviewers consider academic qualifications, potential for a successful career in GBV/VAC-related research, quality and feasibility of the research proposal, ability of the candidate to bring a novel perspective and diversity to the researcher pool (e.g., women and other, under-represented gender-, sexual-, and ethnic-minority scientists), and relevance of the research proposal to the Vietnamese national research priorities around GBV and VAC. Rankings are provided to the CONVERGE Executive Committee, who make final decisions that consider reviewer rankings as well as diversity, balance of disciplines, and commitment of collaborating institutions to support the candidates upon completion of their training program.
Phase 1d: virtual onboarding and matching long-term post-doctoral trainees with research Mentor teams
Upon acceptance and before coming to Emory for the one-month intensive training, trainees complete a virtual onboarding and orientation with the DR and a collaborator in Vietnam. This virtual orientation covers the logistics of traveling to the US and connecting with Emory IT systems (email, outlook, online library system); an overview of training program goals and expectations; required deliverables of the one-month intensive, and timeline for completion. Selected trainees begin work on an NIH-style biosketch and continue development of their research proposals. The CONVERGE Executive Committee suggests suitable US research mentors based on the selected trainees’ application materials.
Phase 2: CONVERGE mentor teams and mentorship training
Phase 2a: Pre-arrival creation of mentor teams
Following best practices for mentoring in the health sciences (80), the DR and MPI at HMU match each selected trainee with a mentoring team that includes: (1) a primary research mentor from their parent institution in Vietnam, (2) a primary, US-based research mentor with subject-area expertise; and (3) an early-career peer mentor with recent experience in a similar training setting. The mentor team is created immediately after selecting each long-term training cohort. This allows time for mentorship training before long-term post-doctoral trainees begin their training program. As needed, trainees also may consult other CONVERGE mentors who have relevant expertise.
US mentors take primary responsibility for training during the one-month intensive research training at Emory. In this capacity, US mentors shepherd the trainee through the intensive research training; guide the development of the trainee’s research protocol; identify and connect trainees with appropriate experts to enhance the quality of the research proposal; provide guidance and resources to improve scientific writing; and provide opportunities to develop the scholarly research network of the trainee (e.g., making introductions; identifying suitable conferences; publications). Female trainees are connected with mentors from the Women’s Research Career Development Sub-Committee (Figure 2) to receive additional support to succeed in environments that historically have been male dominated. In-country primary mentors take primary responsibility for the in-country mentored research project(s). These mentors provide ongoing scientific feedback and navigate institutional logistics relevant to the mentored research project; foster a collaborative research environment; supervise and critically evaluate research activities toward timely delivery of outputs; and offer guidance on career development opportunities. We routinely evaluate mentorship as part of our program evaluation to ensure a good fit between mentors and mentees and make course corrections, as needed.
Phase 2b: in-country mentorship training: rationale and eligibility
The success of each CONVERGE long-term post-doctoral trainee depends, in part, on strong in-country mentorship. Such mentorship involves guidance on trainees” research projects as well as support in acquiring academic positions, promotions, and recognition for professional achievements through nominations for awards and accolades (29, 81, 82). Although this kind of mentoring has been instituted throughout the US as a crucial aspect of research training, mentorship at academic institutions in LMICs can experience challenges, such as a limited number of qualified mentors, misunderstandings between mentors and mentees about roles and responsibilities, a lack of institutional support for mentoring, and little recognition for the value of mentorship for building research capacity (83–85). Furthermore, the effects of mentoring may not be apparent in academic outputs (81). To overcome these challenges, building mentoring capacity in LMICs is crucial to support collaboration among investigators, increase the quality and quantity of funded studies, enhance the research productivity of funded studies, and ultimately, strengthen research infrastructure (86). For these reasons, Drs. Katz and Glass at the National Institutes of Health (NIH), Fogarty International Center (FIC) have highlighted the general importance of comprehensive mentorship training in LMICs (87).
According to our needs assessment (Table 1), mentorship training remains a nascent part of research training in Vietnam. Therefore, CONVERGE emphasizes training in the knowledge and art of mentoring for mid-career research faculty at partner institutions in Vietnam, as well as for graduates of the long-term post-doctoral training program. Specifically, we offer mentorship training through a combined virtual and in-country short-course with 40 eligible short-term trainees. Eligible mentor trainees include approximately 25 mid-career faculty at partner institutions in Vietnam and approximately 15 long-term trainee graduates. Mentorship trainees should have (1) a strong research record, and ideally, experience in GBV/VAC research or an intersecting area in mental, physical, or behavioral health; (2) the desire to mentor trainees, and ideally, the research support and experience to mentor trainees; and (3) support from their institution to take part in 14 contact-hours of virtual and in-country mentorship-training learning modules. This approach to mentorship training creates a network of trained research mentors at diverse career stages, who can effectively mentor CONVERGE trainees and other aspiring researchers in Vietnam into the future, optimizing the sustained impact of CONVERGE.
Phase 2c: mentorship training curriculum
All short-term mentorship trainees complete a virtual 14-contact hour course before each 18-month, long-term postdoctoral training cycle. Mentorship training continues through virtual and in-country sessions during each 18-month postdoctoral training cycle. Virtual sessions include a mix of Vietnam-mentor only sessions and cross-cultural mentor training sessions with in-country mentors who are participating in other D43s supported by Emory University, focused on injury/violence prevention research, and underway in Southeast Asia. The mentorship training curriculum, summarized in Table 2, is adapted from the book, Influential mentors: A guidebook for building mentoring skills and capacity, developed with support from the NIH/FIC (D43TW010143-05S1; D43TW009127; D43TW007124) (88). This curriculum is based on adult learning theory and includes didactic training, panel discussions, group work, interactive exercises, and case studies. The curriculum has been implemented and favorably evaluated with Division Chairs at Calmette Hospital, Cambodia. In 2020–2021, due to the COVID-19 pandemic, Dr. Comeau adapted and implemented the curriculum virtually for five research programs, including several NIH/FIC-funded training programs (D43TW009127; D43TW010934; D43TW011404; D43TW007124).
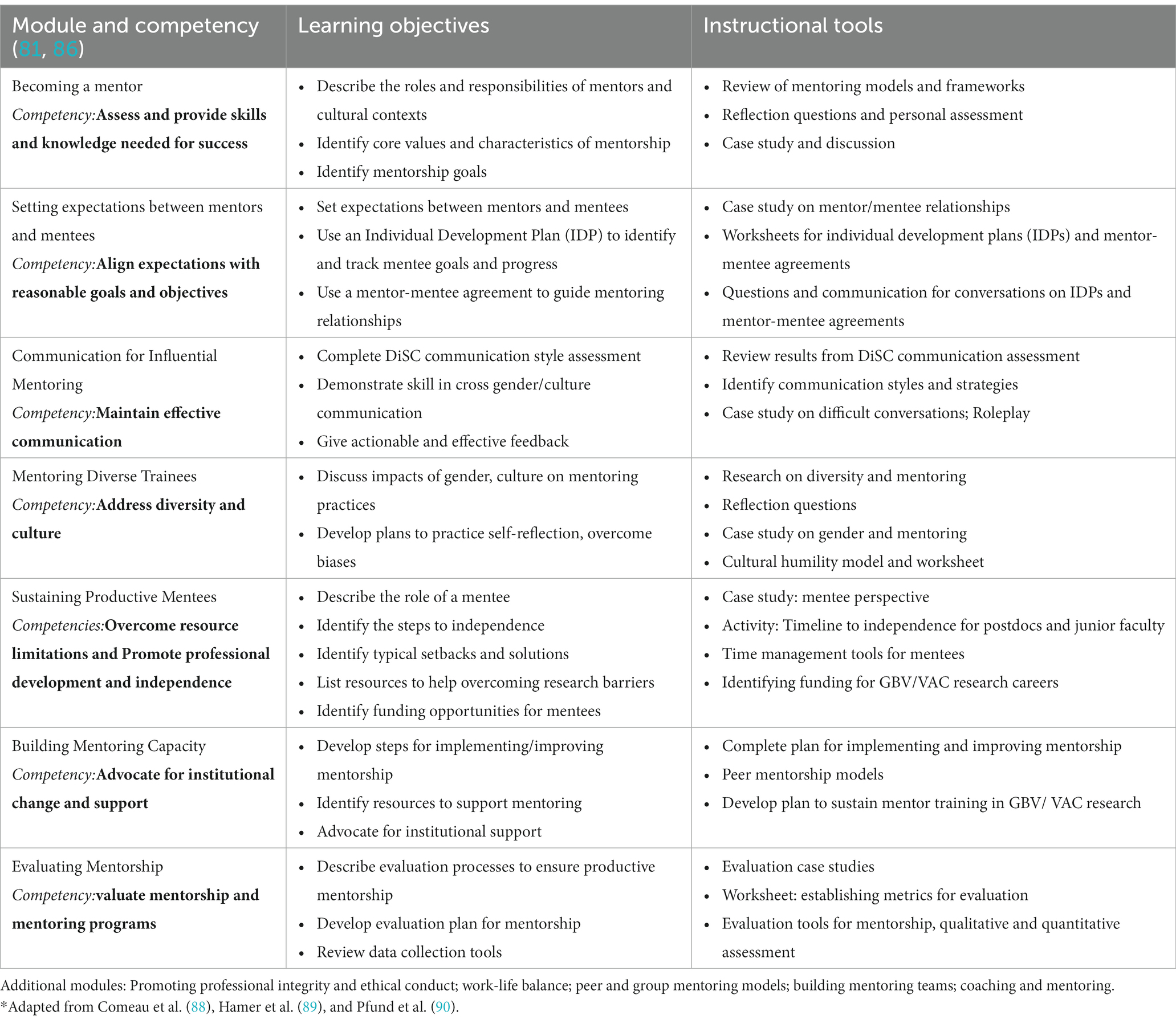
Table 2. Mentorship training for CONVERGE mentors*.
The core curriculum includes seven modules and competency areas on: (1) becoming a mentor; (2) setting expectations between mentors and mentees; (3) communication for influential mentoring; (4) mentoring diverse trainees; (5) sustaining productive mentees; (6) building mentoring capacity; and (7) evaluating mentorship (81). This curriculum includes skill-building to implement Individual Development Plans (IDPs) for trainees, mentor-mentee agreements, and checklists and timelines for program deliverables (Supplemental material). Some tools are adapted from prior NIH/FIC training programs and have been favorably evaluated by mentors and trainees (D43TW009127; D43TW007124; D43TW010143; D43TW010934; D43TW011404). The curriculum also involves completion of a working style assessment to identify communication and problem-solving styles as well as motivators and barriers to productive relationships and teamwork (91). This curriculum will be adapted for mid-career mentorship trainees to enhance topical knowledge of GBV and VAC research and to ensure suitability for Vietnam, based on feedback from the year-one evaluation.
Phase 2d: mentorship training delivery
The COVID-19 pandemic made travel to Vietnam for in-person training uncertain. Also, mid-career mentor trainees have fulltime professional obligations that can preclude multiday, in-person trainings. Thus, a combined virtual and in-person format for delivering the mentorship training curriculum over an 18-month cycle provides maximum flexibility to accommodate these contingencies. In general, we expect that mid-career mentor trainees will take part in four 90-min virtual sessions before the arrival of each cohort of long-term postdoctoral trainees. These sessions will cover three core topics: (1) foundations of mentoring (defining roles and responsibilities, recent research on positive outcomes of mentoring); (2) use of mentoring tools, such as individual development plans (IDPs) and mentor-mentee agreements; and (3) communication and working styles. To enhance learning on topic three, mentorship trainees complete the Myers Briggs personality test1 to reflect on the working styles of themselves and their mentees. After the one-month training intensive training is complete, the instructor holds additional virtual and in-country mentorship training sessions with mentors to ensure their use of mentoring tools adapted for CONVERGE and to cover the remaining topics in the adapted curriculum. To the extent possible and to allow for cross-cultural learning and professional networking, some of the virtual sessions are collaborative with mentors participating in other D43 training programs at Emory, in Southeast Asia, and focused on violence prevention. This flexible, extended format for delivery provides the additional advantages of time to make real-time course corrections and customizations for each cohort of mentor trainees, based on feedback from the evaluation. We will evaluate the mentorship training each year for this purpose.
Phase 3: one-month training intensive of post-doctoral research fellows
Phase 3a: 1-month intensive research training: deliverables and curriculum
Each cohort of long-term trainees travel to Atlanta for a one-month intensive research training at Emory University to optimize the resources available to train independent investigators. Deliverables of this training include: (1) an NIH-style Specific-Aims page, (2) online CITI certification, and (3) a written research proposal that is presented and defended to an audience of peers and faculty for implementation during their 17-month in-country mentored research training period. Deliverables to be completed in Vietnam include an ethics/institutional review board protocol of their research project to be submitted at their home institution within 8–10 weeks upon completion of the one-month intensive training. To apply learning from course-work for higher-level synthesis and to meet the required deliverables, all course assignments enable trainees to make progress on their research proposal throughout the month-long training. Course instructors and Atlanta-based research mentors review all course assignments throughout the month-long intensive to ensure regular, constructive feedback that culminates in a draft research proposal. Key dimensions of this feedback focus on the relevance of their research project to current research on GBV and VAC and the feasibility of completing their project during their 17-month period of program support in-country. Following NIH guidelines, mentors ensure that the trainees’ research projects are rigorous, ethical, and considering the impact of age, sex, gender, and other differences in the design and analysis.
All course content is foundational to completing the course assignments, which lead to a rigorous research proposal. Table 3 provides a sample curriculum, and six core topics are covered: (1) concepts, measurement, and ethics in GBV and VAC research, (2) principles of mentee-mentor relationships, (3) responsible conduct of research, (4) research methods, (5) proposal development, and (6) managing and leading teams. The content of each topic, to some extent, is customized for each cohort, and core competencies associated with each topic are described, below.
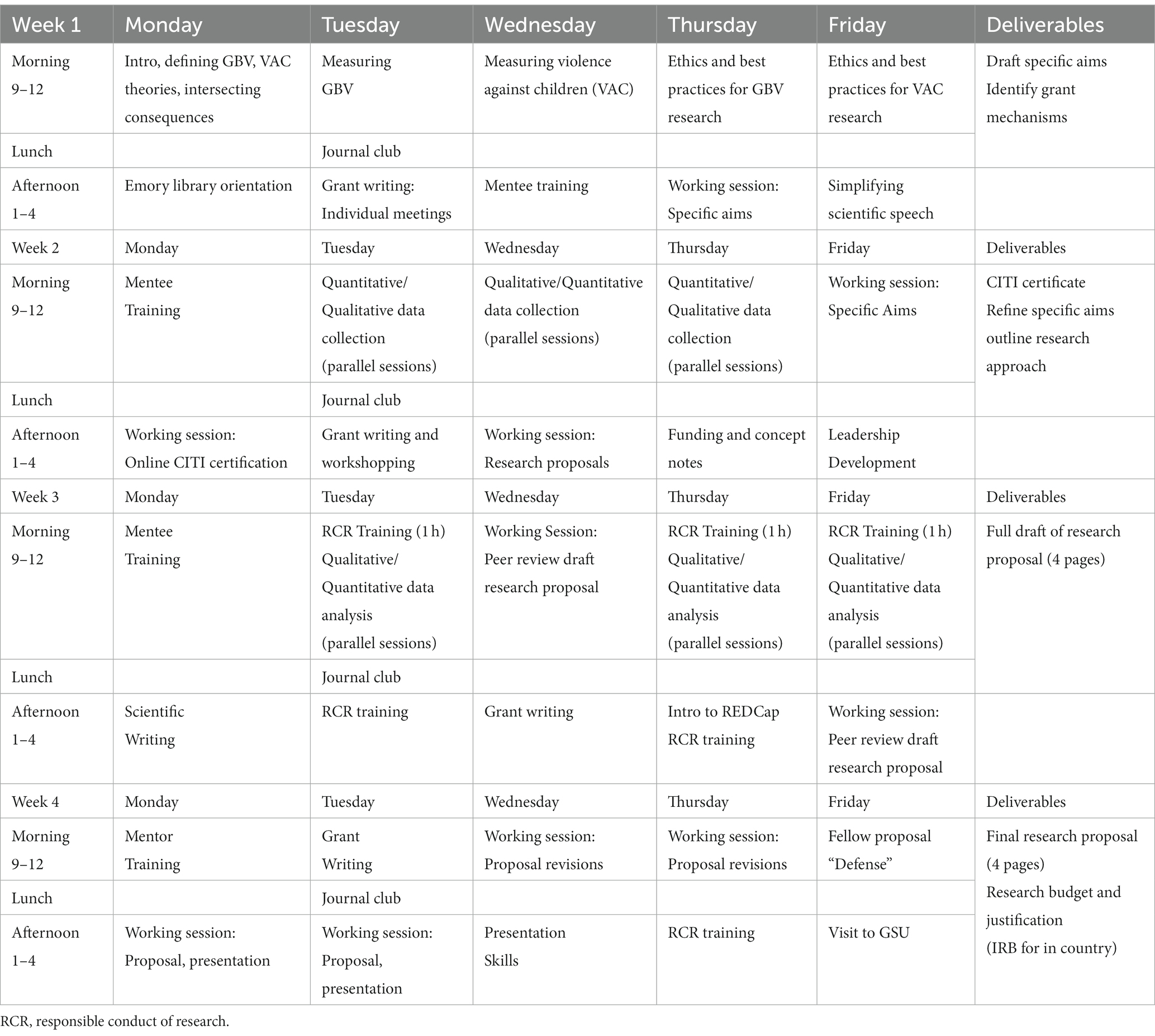
Table 3. CONVERGE 1-month training intensive summary curriculum.
Concepts, measurement, and ethics in GBV and VAC research
CONVERGE training faculty with specific expertise in GBV and VAC research cover foundational topics on (1) defining GBV and VAC, including specific forms, (2) etiological theories of GBV and VAC and intersecting mental, physical, and behavioral health outcomes, (3) measurement of GBV and VAC, and (4) ethical consideration and best-practices for conducting research on GBV and VAC. Content is tailored to focus on the forms of GBV/VAC and populations that are the foci of the trainees planned research projects. Topics also may include understanding violence as a public-health issue and translating data on GBV/VAC into action.
Principles of mentor-mentee relationships
The mentoring instructor and a collaborator in Vietnam facilitate at least one module on mentor-mentee relationships with CONVERGE trainees. The curriculum is based on Comeau et al.’s book, Influential Mentors: Building Mentoring Skills and Capacity (2019). The session provides foundational background and context on mentoring, a case study discussion on aligning expectations between mentors and mentees, and how to understand and incorporate feedback from mentors. Specific topics may include aligning mentor and mentee expectations, typical roles of a mentee, communicating with mentors, and trouble-shooting mentee missteps. The session also includes discussion on the cultural differences between mentors in Vietnam and the US, and strategies for the mentees to optimize mentoring relationships in the CONVERGE program. This session is designed to ensure that trainees interact confidently and coordinate well with their US and Vietnamese mentors.
Responsible conduct of research
NIH has established competencies in the Responsible Conduct of Research (RCR) (92). NIH mandates that this training be primarily face-to-face and tailored to the specific needs of the trainees. In this D43, which focuses on GBV and VAC, special attention is paid to the topics of Human Subjects in Research, and data security. RCR is addressed through multiple modalities. During the one-month intensive session at the Emory campus, at least five in-person sessions are provided, and if needed, the remainder are covered during annual in-country trainings. Topics include human-subjects research, ethics in data handling, authorship, maintaining participant privacy and data confidentiality, conflict of interest and commitment, mentor/mentee responsibilities and relationship, safe research environment, collaborative research, and research misconduct. Sessions are led by the Faculty Director for the Responsible Conduct of Research course, coordinated by the Office of Post-Doctoral Education within the Emory University School of Medicine. Mentorship is built into the overall training program, as described elsewhere in this paper.
Research methods
Course content is tailored to the specific needs of each trainee cohort. For trainee cohorts implementing projects mainly involving primary data collection, the focus of the one-month intensive sessions is on quantitative and qualitative field methods in GBV and VAC research. For trainee cohorts implementing projects mainly involving secondary data analysis, the focus is on the salient methods for quantitative and qualitative data analysis. Trainees also are exposed to useful software applications for data collection and/or analysis, such as REDCap or MaxQDA.
Research proposal development
These sessions guide trainees through the core steps of developing a research concept using publicly available data from their home country or collecting their own data during their in-country training. Topics focus on finding sources of federal funding, developing an NIH-style biosketch, crafting an NIH-style specific-aims page, and crafting the research strategies section of an NIH-style proposal. Didactic sessions are followed by “working sessions” in which fellows apply what they have learned to their own research proposals.
Scientific writing and science dissemination
A key component of strengthening research capacity among CONVERGE trainees is developing the communication skills needed to present and publish findings internationally. Therefore, foundational science dissemination sessions designed to support CONVERGE orientation program deliverables are included in the training curriculum. Sessions cover (1) scientific writing: paper-writing mechanics, peer review, predatory publishing, good scholarship practices, (2) presentation skills: slide design, presentation organization, public speaking, and (3) simplifying scientific speech: concise, effective communication across linguacultural contexts. These sessions are facilitated by training faculty who specialize in advancing global health research through applied linguistics.
Foundations of leadership
CONVERGE trainees are expected to manage a cross-cultural mentoring team, to develop and manage a project budget, and to develop and manage a project timeline. Yet post-doctoral trainees rarely receive formal training in such topics. In the absence of this training, people do the best they can; however, the process often takes longer with poorer results compared to those who receive foundational training. Post-doctoral fellows’ who receive such foundational training are well-positioned for success on these crucial leadership skills. CONVERGE training faculty with expertise in cross-cultural leadership development provide sessions on: managing teams, project management, influence without authority, and other leadership-related topics that are customized to each post-doctoral trainee cohort. We design experiential sessions that provide crucial leadership skills, yet also allow for some flexibility to serve the unique needs of each cohort.
Phase 3b: delivery of 1-month training intensive
The entire one-month training intensive is delivered at Emory University. In general, the delivery format involves in-person didactic (knowledge- and skills-based) sessions in the morning and interactive and working sessions in the afternoons (Table 3). All lectures are recorded, and all session materials and recordings are saved on Emory’s Canvas course platform, so trainees can access the materials anytime during the 18-month fellowship period. The final week of training applies the learning from the prior 3 weeks to finalize a draft research proposal and presentation, and to defend the research proposal with peers and faculty at the end of the intensive. The delivery of the one-month training adheres to the planned protocol, described above, with flexibility for revisions to meet the specific interests and skill domains of each cohort of long-term CONVERGE trainees. For example, we may add additional sessions on the responsible conduct of research; the use of REDCap as a secure system for the collection, transfer, storage, and analysis of study data; and finding grant funding from foundations. We also may revise the final set of deliverables to accommodate the initial skill levels of each cohort of trainees.
Phase 4: mentored research project in Vietnam and concurrent training
Phase 4a: IRB protocol development
After completing their research protocol and before beginning their research project, these research protocols must receive the Institutional Review Board (IRB)'s approval in Vietnam. The IRBs at partner institutions in Vietnam are available for the fellows to apply. The fellows submit all institutional forms, as needed, which may include research protocols, questionnaires, and other documents, like informed consent forms that provide participants with information about potential benefits and risks. The IRB committee must receive application materials in Vietnamese for approval. When the draft IRB application is complete, the fellow’s primary mentor in Vietnam and a CONVERGE collaborator at HMU review all IRB applications before submission. If there are any modifications to the research protocol while it is being implemented, they must be submitted to the IRB Committee for approval before moving further. The trainee can start data collection after receiving the IRB certificate.
Phase 4b: on-going support of fellows’ research progress
Several strategies are in place to support the completion of long-term trainees’ mentored research projects. First, trainee develop a project timeline for self-checking of the timely completion of project milestones (Supplemental material). Second, trainees organize weekly meetings with in-country research mentors to provide real-time guidance on project implementation. Third, trainees organize monthly meetings with their mentor teams so conceptual, methodological, or operational challenges that may emerge can be addressed with the appropriate expertise. Fourth, the DR and an in-country collaborator host monthly check-ins to identify and address any challenges with mentoring teams or projects as they arise. Fifth, the Emory project coordinator administers a brief REDCap survey to trainees to ensure mentor meetings are occurring and meeting minutes are documented for evaluation. Sixth, a regular journal club and annual in-country trainings are provided to advance the research and dissemination skills of trainees. Finally, periodic virtual sessions are hosted by the CONVERGE mentorship instructor or other program faculty to support the professional development and networking of trainees supported across D43s at Emory, in Southeast Asia, and focused on injury/violence prevention.
Phase 4c: deliverables of the CONVERGE fellowship
Trainees are expected to complete two primary deliverables by the end of their 18-month fellowship. These deliverables include (1) the submission of an abstract and the presentation of research findings at an international scientific meeting, and (2) the drafting and submission of one research article to an international, peer-reviewed journal. The format of the research article depends on the nature of each trainee’s research project (e.g., qualitative versus quantitative) and is expected to follow the guidelines of the journal to which they submit. Finally, 6 months after the completion of their 18-month fellowship, trainees are expected to submit a second proposal, to a competitive funding pool within CONVERGE, to a private foundation, or to NIH. This follow-up proposal should build on the findings from their CONVERGE fellowship and further advance their research training toward becoming an independent investigator and future mentor of students at their respective institutions.
Phase 5: concurrent monthly journal club during research project implementation
A CONVERGE journal club begins during the one-month intensive training (Table 3) and continues virtually during the trainees’ in-country mentored research projects. The journal club is designed to build a peer-network of GBV/VAC researchers across partner institutions in Vietnam. It also provides a space to discuss articles on GBV or VAC that are timely, high-impact, of interest to the trainees, or cover advanced research methods that trainees might consider in their own GBV/VAC research projects. Building on the format of existing journal clubs within Emory doctoral programs and other D43 training programs, sessions are small and informal, but structured to encourage discussion and questions, enable critical evaluation of the research design and manuscript, and ultimately, inform the work of the trainees. Sessions are one-hour and held monthly using an in-person or virtual format. One trainee is responsible for leading each journal club session. Leadership includes selection and circulation of a peer-reviewed article among the trainee group 2 weeks in advance of the journal club, presenting a summary and critical evaluation of the article during the journal club, and responding to questions that arise from other trainees. Leadership also includes preparing a short PowerPoint presentation the includes: (1) a brief description of why they selected the article, (2) the research question and study aims, (3) the study design (including unique ethical considerations given the GBV/VAC research context), (4) a summary of the major findings and discussion points, (5) a brief statement of how the study impacts their own future work, and (6) 2–3 questions for the group to discuss. The other trainees read the article in advance and come prepared to discuss the article in detail. The lead trainee for the journal club moderates the discussion, and a faculty member is present for each journal club to answer questions and to ensure critical points from the article are discussed.
Phase 6: strategies to ensure long-term postdoctoral trainee retention
CONVERGE provides several sources of support to promote trainee retention. First, we create multiple-mentor teams, with appropriate expertise and a structure in which long-term trainees meet weekly with trained in-country mentors and monthly with US mentors and mentor teams. Second, trainees participate in a customized one-month intensive course at Emory University in the United States, which allows trainees to receive needs-based training and to develop in-person, professional relationships with their US mentors. Third, trainees receive a monthly stipend to allow for protected time for mentored research and research training in the CONVERGE program. Fourth, trainees receive research funding to support their proposed in-country research project. Fifth, trainees receive support for computing and an Emory email account, which provide them with access to Emory electronic resources including e-journals, e-textbooks, and proprietary funding resource databases. Sixth, trainees receive multiple, ongoing opportunities for training during their 17-month in-country research project, such as an on-going virtual monthly journal club, annual in-country training sessions, and virtual networking opportunities with other D43 trainees in other countries. Seventh, trainees have opportunities to share confidential feedback to the CONVERGE evaluation team for real-time course corrections, and feedback during regular check-in meetings with the Director of Research. This feedback enables trainees to communicate challenges they are having in the CONVERGE program that the leadership team can discuss and address proactively. This combination of human capital investment, professional network development, and financial investment builds on the PI’s experience with empowerment-based training of under-represented early-career scientists (29), and should result in a high retention rate of long-term postdoctoral trainees in the CONVERGE program, as well as continued GBV/VAC research after program completion.
Phase 7: advanced in-country trainings and developing a science-to-practice network
In Years 4 and 5 of the project period, CONVERGE will host in-country trainings that will advance the methodological, leadership, and science-dissemination skills of all three cohorts of long-term trainees. One short-course will focus on the concepts, theories, and methods of implementation science. A second short-course will focus on advanced topics in leadership training, and a third short-course will focus on skills and strategies for various types of science dissemination (89, 90).
Implementation science
Training in implementation science will take the form of a short course on Dissemination and Implementation (D/I) science. Course content will start with a review of theoretical perspectives on D/I science and will cover several current theoretical models, including Diffusion of Innovation (93), RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) (94), EPIS (Exploration, Preparation, Implementation, Sustainment) (95), and CFIR (Consolidated Framework for Implementation Research) (96). The course will cover methodology of D/I research including etiological methods, methods from D/I trials, and combined effectiveness/implementation trials, and the use of mixed methods in D/I research (97). Another module will focus on measurement of key constructs and will review methods for identifying common outcomes in D/I research (98). Additional content will be focused special topics including systemic and organizational influence on D/I (99), the use of technology in D/I research (100), processes for adapting evidence-based programs (101), sustainment of implementation (102), and “real-world” implementation conducted in a non-research setting.
Advanced topics in leadership
This short-course will build on the foundational topics covered in the one-month intensive—on managing projects, leading teams, and influence without authority. Advanced topics in leadership development will include, for example, making ethical decisions through emotional intelligence, effective negotiation, and conflict management. The goal in the advanced course is to help our trainees build skills to manage issues that commonly arise in the process of team projects. We will design the content to help participants recognize early when team issues arise, diagnose the nature of the problems that have surfaced, and tactfully communicate with their teams to overcome the challenges. Conflict is a key example, as many research teams struggle to resolve differences of opinion, divide responsibilities thoughtfully across team members, and other process issues related to working with one another. These challenges can lead to team dysfunction and damaged relationships among its members, thus a focus on emotional intelligence to attend to the relationships among team members. The short course also will cover the qualities and skills needed to become a transformational leader, leadership qualities needed to spearhead intra-organizational change, and strategies to manage cross-cultural organizational collaborations. After participating in these sessions, post-doctoral trainees will be more savvy and holistic proponents of change, including team members in the process and ensuring that all voices are heard in the plans and implementation of ideas.
Advanced topics in science dissemination
This short course will build on the foundational topics covered in the one-month intensive by focusing on strategies for communicating scientific research findings effectively across diverse contexts and audiences. In this task-supported course, trainees will develop in-progress research presentation and writing projects through hands-on, peer-review activities. Topics include simplifying scientific speech, presenting at international conferences, communicating across cultural contexts, and composing professional correspondences. Trainees will develop strategies for crafting concise and compelling abstracts, posters, and PowerPoint presentations for international scientific conferences. The course will explore intercultural conventions for professional communications such as emails, cover letters, revisions, and revise-and-resubmit responses. It also may focus on skills for developing effective press releases about the findings of research projects and interacting effectively with local, national, and international media about the findings of research projects. Finally, this short course also may cover strategies for communicating with local, regional, and national officials to convey the findings of research projects in concise, lay terms.
Scientist-practitioner network
CONVERGE also will support the development of an in-country science-to-practice network to optimize the public-health impact of the program. To do so, we will offer these in-country short-courses to 60 practitioners and to our growing pool of research mentors. Eligible short-term practitioner trainees will include professionals working in universities, schools, community-based organizations, healthcare systems, and political organizations that are salient for the GBV and VAC evidence being generated by CONVERGE trainees. Examples include those working in mother and child protection in the Department of Health and Human Services; Child Protection Department, Ministry of Labor, War Invalids, and Social Affairs; Maternal and Child Health Protection Department, Ministry of Health; Vietnam woman’s group; and Child Rights Working Group, a consortium of international and domestic organizations who cooperate and share information to promote children’s rights in Vietnam. Eligible practitioner trainees should (1) have a history of working on policies or programs related to GBV/VAC or a cognate field, such as mental health or sexual health; (2) be sensitive to the vulnerability of certain groups in Vietnam to the risks of experiencing GBV and VAC, (3) have an interest in the implementation of evidence-based GBV and VAC programs, and (4) have an interest in science-practitioner collaboration. We also provide mentorship training to practitioners. In project year 2, CONVERGE leadership will conduct needs assessment meetings with a purposive sample of practitioners to determine the most suitable topics and format of the training. Possible topics include: how to mentor new professionals who are entering a career in GBV and VAC, mentoring staff on how to manage competing priorities; mentoring professionals through essential and new skills required in the field; and, mentoring professionals on self-care as they work on topics and research that require emotional work.
CONVERGE training program evaluation
To accomplish our program aims, CONVERGE will implement a rigorous, multi-level evaluation to assess the implementation, reach, fidelity, and effectiveness of the CONVERGE training program. Guided by an established evaluation framework and detailed evaluation plan, our evaluation will accomplish three specific goals: (1) to provide data for decisions that enhance modification and improvements of CONVERGE program activities; (2) to determine the individual and aggregate success of program activities and aims; and (3) to identify strategies for long-term sustainment and expansion of in-country research training to address GBV and VAC in Vietnam. The program evaluation is carried out under the direction of the Director for Evaluation (Figure 2).
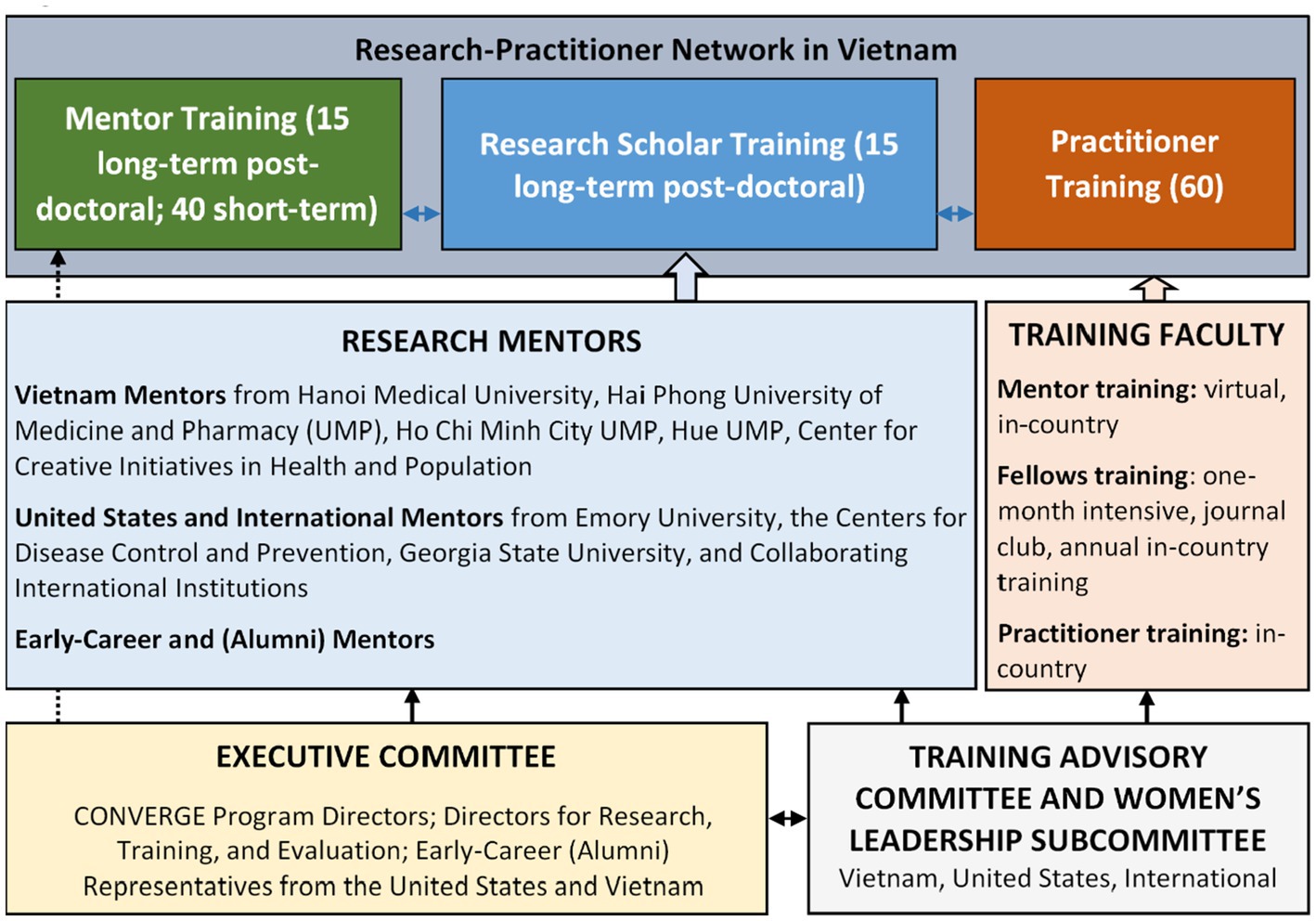
Figure 2. CONVERGE administrative structure.
Evaluation framework
To achieve these goals, the evalution of CONVERGE is guided by the Kirkpatrick Model (103), an established framework for evaluating training programs in health care and international settings (104, 105). The Kirkpatrick model employs four levels of evaluation of training programs (Figure 3). The first level, Reaction, refers to the level of reaction by learners to the training. A measure of reaction is the degree to which training participants find the training favorable, engaging, and relevant to their jobs (106, 107). The second level, Learning, refers to the type and scope of changes in the participants’ learning caused by participation in the program. We can measure this level by addressing the degree to which the participants acquire the intended knowledge, skills, attitudes, confidence, and commitment based on their participation in the training. The third level, Behavior, indicates whether or not the program has created a desired change in the participants’ behavior. A measure of behavior is the degree to which participants apply what they learned during training when they are back on the job (108, 109). The fourth level of the Kirkpatrick Model is Results. This level reflects the degree to which targeted outcomes occur as a result of the training. These outcomes may be directly related to the individual’s work or the work of the organization (110).
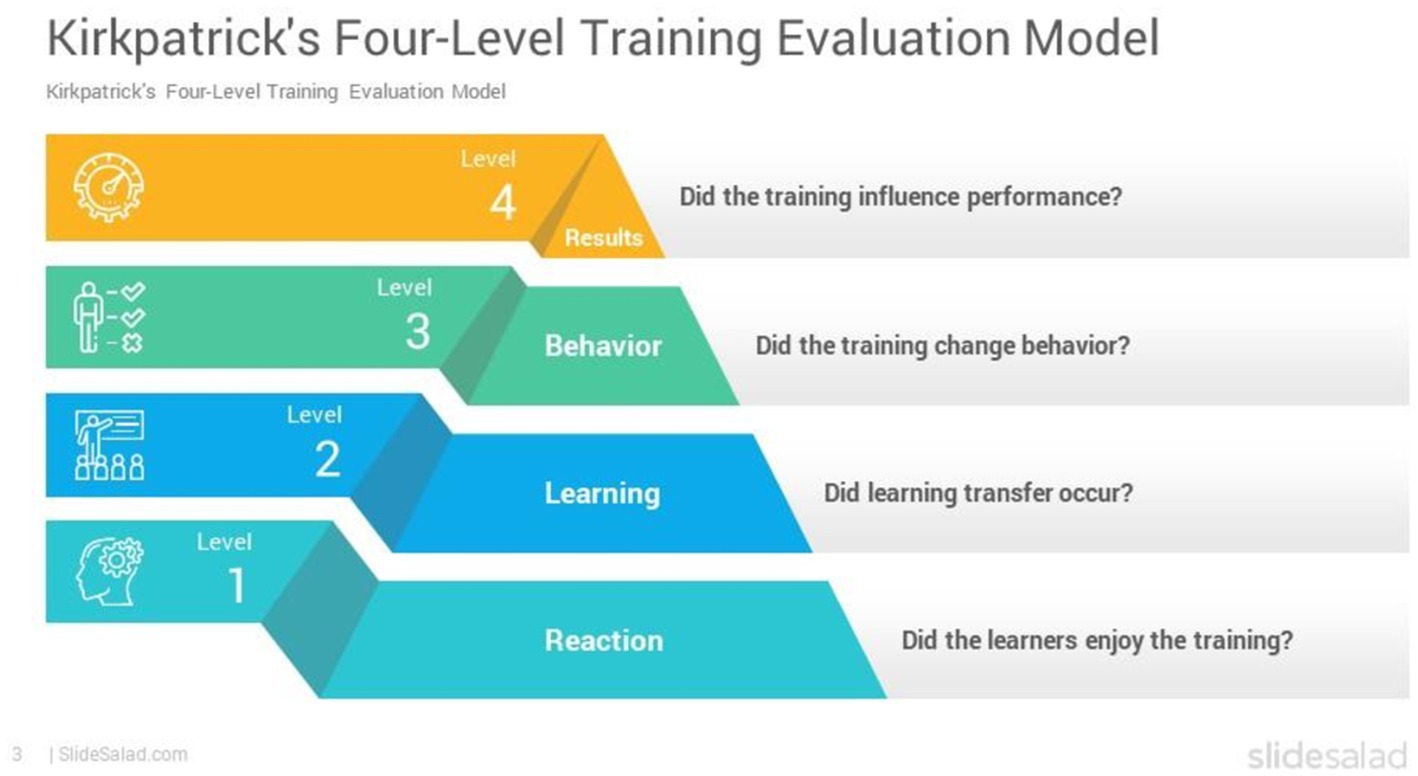
Figure 3. Kirkpatrick four-level training evaluation. Licensed for inclusion from slidesalad.cpm https://www.slidesalad.com/our-licenses/.
Data collection
We will use a mix of quantitative methods (surveys, course evaluations) and qualitative methods (in-depth interviews, focus group discussions) to assess trainee and mentor experiences with the program, achievement of program competencies, and progress with GBV and VAC research. We will adopt a bi-directional approach to evaluation, in which we obtain feedback from trainees and mentors about the program and assess trainee and mentor progress. Data collection instruments are developed and informed by each of the Four Levels of the Kirkpatrick Model.
Quantitative surveys and course evaluations are developed and deployed using the Research Electronic Data Capture (REDCap) system, a secure web platform for building and managing online databases and surveys. Its streamlined process for creating and designing projects offers an array of customizable tools for a specific data-collection strategy. Quantitative data is analyzed using descriptive, and as the number of CONVERGE trainees grows, multivariate statistical techniques. Qualitative methods include in-depth interviews and focus group discussions conducted with trainees and their mentors. Data collection occurs in person during annual in-country training and planning meetings as well as online via Zoom and email. Using a team-based approach, all qualitative data will be coded, and standard content analysis will be applied to develop themes. Triangulation of the quantitative and qualitative data will occur during a stage of final interpretation. Evaluation data will be collected continuously over the program period and used iteratively to inform decisions to improve program content, design, delivery, and implementation. See Supplemental material for sample evaluation forms.
CONVERGE evaluation logic model
We developed a logic model that operationalizes the Kirkpatrick model and provides a guiding framework to evaluate CONVERGE. This logic model provides a systematic and visual guide to the relationships that exist among resources allocated to the CONVERGE program, planned programmatic activities, and anticipated changes as a result of the program. We developed this logic model to refine: (1) the focus of the evaluation; (2) the evaluation questions, or what is to be measured; (3) the indicators and information that best answer the evaluation questions; (4) timing for data collection; and (5) types of data to be collected using appropriate sources, methods, samples, and instruments (Figure 4). The evaluation logic model is organized by process, outcome, and impact measures. Process measures are those that identify the inputs or resources, activities, and outputs of a program that are needed to ensure successful implementation of a program. Outcome measures include short-term and intermediate-term outcomes that are expected once successful implementation occurs. Finally, impact measures identify effectiveness of achieving a program’s long-term goals.
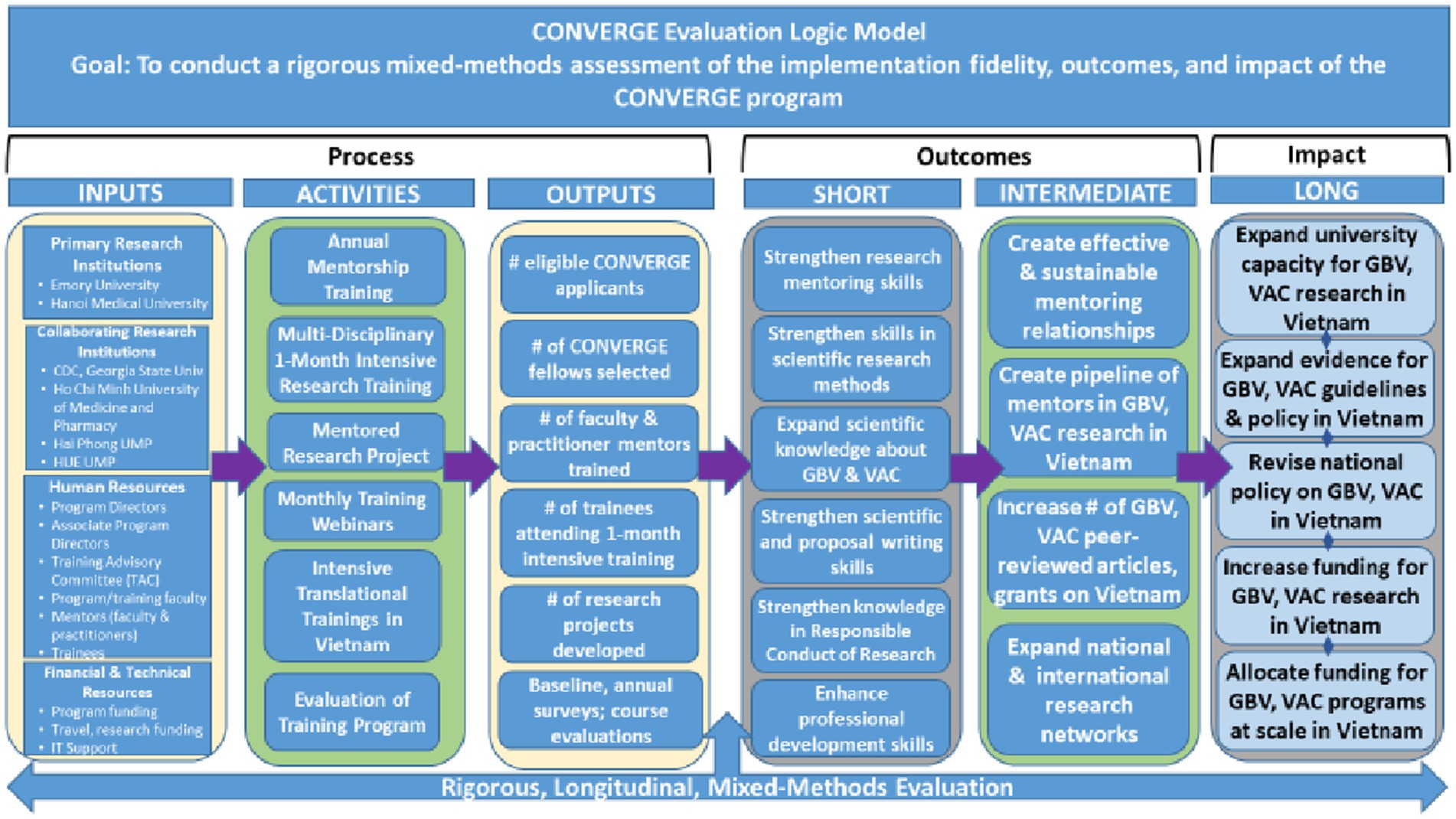
Figure 4. CONVERGE evaluation logic model.
CONVERGE evaluation plan
We developed an evaluation plan to help document program effectiveness and to inform decisions about future program development and/or needed improvements (Table 4). This evaluation plan identifies and describes each component of the training program to be evaluated and maps each component to the relevant evaluation measures, and data-collection activities. Details of each evaluation component are described below.
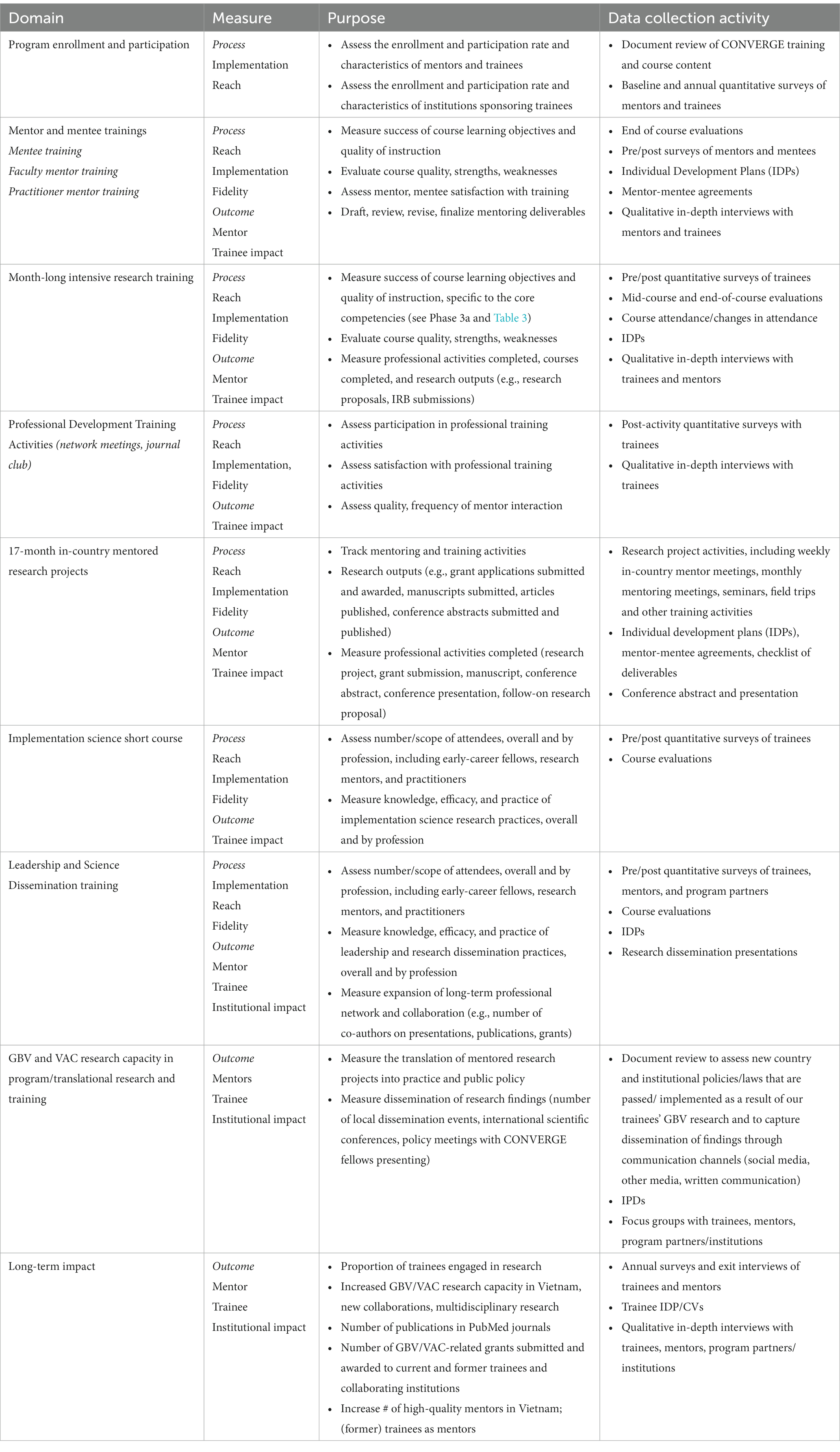
Table 4. Evaluation plan for the CONVERGE research training program.
Program enrollment and participation
To assess program implementation and reach, we distribute quantitative surveys to track mentor and trainee enrollment and progress and engagement of US/international, Vietnam program partners and institutions. Ongoing monitoring of the program is conducted through a systematic review and updating of CONVERGE program and training materials.
Mentor and mentee training evaluations
We collect multiple sources of data to evaluate the impact of the mentor and mentee trainings on mentoring practices and perceived competence in mentorship. We evaluate the faculty mentor trainings as well as the practitioner mentor trainings. For both mentor trainings, we develop and distribute pre- and post-training surveys of mentors to gauge changes in knowledge, attitudes, and beliefs regarding the value and understanding of mentorship. We conduct qualitative in-depth interviews with select mentors to explore further their experiences with the mentor training and perceived competence in mentorship. Our evaluation of the mentee training includes pre- and post-training surveys of mentees to gauge their knowledge, attitudes, and beliefs regarding the value and understanding of mentorship and the mentee-mentor relationship. We also conduct an end-of-course evaluation of the training to gauge satisfaction with the training and recommendations for mentee training enhancement. Finally, we conduct qualitative in-depth interviews with mentees to explore further their experiences with the mentee training and their mentoring relationships.
One-month intensive research training
Our evaluation of the one-month intensive research training assesses success with course learning objectives, perceived quality of instruction, satisfaction with the training, and progress with professional development and research activities, such as the research proposal and IRB submission. We distribute pre- and post-training surveys to gauge changes in trainee knowledge, attitudes, and beliefs about GBV/VAC research. We also conduct mid-course and end-of-course evaluations of the training to gauge satisfaction with the training and recommendations to enhance mentee training. Finally, we conduct a select number of qualitative in-depth interviews with the trainees to explore their experiences with the month-long intensive, and with the mentors to assess trainee’s professional progress.
Professional development training activities
During the one-month intensive research training, trainees also attend several weekly professional development activities, including mentor meetings, peer network meetings, journal club, and project management. We evaluate each activity independently and at the end of the month-long intensive research training. Trainees complete a post-training activity survey to assess participation in, satisfaction with, and knowledge gained. We also conduct qualitative interviews with select trainees to explore experiences with training activities and recommendations for program improvement.
Seventeen-month in-country mentored research project
To monitor trainees’ progress with their in-country mentored research project, we track their attendance and participation in (1) weekly in-country mentor meetings; (2) monthly U.S/in-country/alumni mentor team meetings; (3) virtual training seminars; (4) review meetings to provide advice and support with executive committee members from HMU; and (5) innovation field visits to GBV/VAC research centers. We also analyze trainees’ IDPs and monthly mentor meeting notes. Trainees also are required to submit their research conference abstract and presentation to the evaluator.
Implementation science short course
We evaluate this short course implemented in Year 4. We conduct pre- and post-training surveys to assess changes in knowledge and skill, as well as satisfaction with the training. We conduct an end-of-course evaluation to gauge satisfaction with the course and recommendations for program improvement. We also conduct qualitative in-depth interviews with trainees to gain further insight about the training as well as recommendations for program improvement.
Leadership and science dissemination training
We evaluate the leadership training and science dissemination training in Year 5. We conduct pre- and post-training surveys to assess changes in knowledge, skill, and satisfaction with the trainings. These surveys incorporate measures of leadership with which the team is familiar (111). We also conduct an end-of-training evaluation to gauge satisfaction and recommendations for program improvement. Furthermore, we conduct qualitative in-depth interviews with trainees, mentors, and program/institutional partners to gain additional insight about the training as well as recommendations for program improvement. Copies of the trainee’s research dissemination presentations also will be collected, as well as their IDPs to assess the impact/translation of the training on trainees’ research and career development.
GBV and VAC research capacity in program/translational research and training
A long-term goal of CONVERGE is to build capacity of trainees to conduct research related to GBV and VAC, in Vietnam and with their practice partners and institutions. We monitor the reach and translation of GBV and VAC research conducted by CONVERGE trainees through a review of peer-reviewed and gray (non-academic) literature. We assess the impact of this research on changes in national and local policy through additional document reviews and an inventory of engagements with in-country policy-makers. Focus group discussions are to be conducted and organized by group (mentor, trainee, program partners/institutions) to elicit further information about the research and translation of GBV/VAC research developed in the program.
Long-term impact
To measure attainment of program goals and long-term program impact, we assess outcomes of individual trainees, mentors, and institutions participating in the CONVERGE program. Individual trainee outcomes include publications, grants, new roles in CONVERGE and at their home institutions. Mentor outcomes include increased mentor competence and new roles in CONVERGE and at their home institutions. Institutional outcomes for in-country institutions include increases in institutional GBV/VAC grants secured, number of articles on GBV/VAC produced, and spillover efforts to faculty outside the CONVERGE program. Several data sources are used to inform the evaluation of outcomes and long-term impact of the program, including quantitative surveys, annual and exit interviews (mentors and trainees), IDPs/CVs to track trainee publications and grants, and qualitative interviews with trainees, mentors, and institutional leaders.
Discussion
Summary of CONVERGE training program
Gender-based violence (GBV) and violence against children (VAC) are prevalent and interconnected global health challenges; however, data and research capacities to study these forms of violence and to generate evidence-based policies and programs remain limited in LMICs, including Vietnam. To address these shortages in Vietnam and to establish a model for other LMICs, we are establishing CONVERGE—the Consortium for Violence Prevention Research, Implementation, and Leadership Training for Excellence. CONVERGE connects experts from Emory University, HMU, partner institutions in Atlanta and Vietnam, and partners from around the world, with the goal of providing mentorship opportunities for early-career scientists in GBV and VAC research and prevention. Based on a needs assessment with partners in Vietnam, the CONVERGE training program has four components: (1) 14 h of virtual/in-person annual mentorship training to prepare research mentors and to create a pipeline of future mentors in Vietnam; (2) a one-month intensive research training for long-term postdoctoral fellows at Emory University; (3) a structured 17-month, in-country mentored research project for long-term trainees that results in a peer-reviewed manuscript and a grant submission; and (4) annual in-country trainings, including advanced training on implementation science, leadership, and science dissemination. CONVERGE will support 15 long-term, postdoctoral trainees with multi-disciplinary research training in GBV and VAC, 40 short-term mid-career academic trainees, and 60 short-term practitioner/stakeholder trainees over 5 years to build productive GBV and VAC academic, scientific, and practitioner networks. CONVERGE also will connect long-term trainees and mentors to peers who are participating in other D43s focused on violence/injury prevention, D43s at Emory, and D43s in Southeast Asia. To assess the reach, implementation, fidelity, and effectiveness of these four training components, we will implement a rigorous, mixed-methods, multi-level evaluation using process and outcome measures. Evaluation findings will be used to refine program components for future trainee and mentor cohorts and to assess long-term program impact.
Implications for capacity-strengthening, evidence generation, and public-health impact
CONVERGE aligns with national research priorities of Vietnam (28) and leverages over 12 years of collaboration between consortium partners in Atlanta and Vietnam, demonstrating the high feasibility of achieving our program aims. Our mentorship training, which emphasizes trainee empowerment (29), transparent mentor-mentee collaboration, and team-based mentoring with trained mentors, will create a pipeline of early- and mid-career researchers who are skilled mentors. Our long-term post-doctoral research training is grounded in successful integrated, interdisciplinary training programs with Emory and other partners and is tailored to meet identified needs in Vietnam. Our advanced leadership, science dissemination, and implementation science short courses address documented needs in Vietnam (30), build on and amplify Emory’s successful leadership training programs (D43TW009135), and will accelerate the translation of evidence into contextually relevant policies, programs, and best practices. Our training plan addresses the priorities of several divisions within the National Institutes of Health (NIH) related to women’s health, child health and human development, mental health, minority health and health disparities, alcohol abuse and alcoholism, drug abuse, and general medicine. Our intentional integration of GBV and VAC research with intersecting health conditions and health disparities creates a platform for future grant submissions by CONVERGE trainee graduates.
Several events illustrate the favorable political climate for CONVERGE trainees to have favorable impacts in Vietnam. First, on January 13, 2021, the Prime Minister of Vietnam authorized the Vietnamese national program on avoiding and combating domestic abuse until 2025. Second, in a joint statement on January 5, 2022, the Child Rights Working Group committed to implement child protection measures in Vietnam and to support the Vietnamese government in its efforts. Third, on November 14, 2022, the National Assembly of Vietnam approved a revised Law on Domestic Violence Prevention and Control. This climate will enable CONVERGE trainees to collaborate with practitioners, organizational officials, and local advocates to make evidence-based recommendations to improve prevention and response services for those most vulnerable to GBV/VAC in Vietnam.
Our team anticipates potential pitfalls and unintended effects of CONVERGE for GBV/VAC research and practice in Vietnam. First, fellows’ research projects are selected with care to ensure local acceptability, given the potential sensitivity of topics related to GBV/VAC. Second, efforts are invested to expand the pool of in-country mentors to avoid local mentor burnout and to expand capacity for mentoring across all local partner universities. Third, long-term trainees and local mentors often have competing demands on their time, which may contribute to delays in the completion of trainees’ research projects. To mitigate this risk, CONVERGE has developed supports and “cross-checks” to ensure that project milestones are met or appropriately revised and that trainees cultivate effective problem-solving skills when they encounter time-related demands that may delay their progress. Fourth, fellows may lack the local professional networks to ensure the timely translation of their research into practice and policy with local influencers. To facilitate the favorable local impact of their research, the CONVERGE Executive Committee has integrated opportunities into the 18-month fellowships for trainees to present their work sequentially to the CONVERGE Executive Committee, subsequent cohorts of trainees, and influential local practitioners at annual in-country meetings. In these ways, and others, CONVERGE includes safeguards against unintended consequences of the program to ensure its long-term sustainment.
For these reasons, CONVERGE members are energized to meet the demand for locally relevant violence prevention research, implementation, and leadership training in Vietnam. Over the program period, we expect to train a critical mass of 115 research mentors, post-doctoral fellows, and practitioners in Vietnam in GBV and VAC research, implementation/dissemination research and practice, and leadership. Based on learning from prior training programs as well as novel training elements, we will promote high trainee retention and strengthen institutional capacity in Vietnam, with a strategic focus on CONVERGE partner institutions for maximum institutional impact. In doing so, we will prepare a consortium of universities and experts in Vietnam to conduct locally relevant GBV and VAC research and to translate evidence into recommendations that shape national research and program priorities into the 21st century.
Program adaptations to mitigate the impact of the COVID-19 pandemic
CONVERGE is poised to adapt all programming from in-person to virtual formats, to be responsive to the uncertainties of in-person meetings resulting from an on-going COVID-19 pandemic. At the same time, our team recognizes that training in the responsible conduct of research requires a high degree of in-person training, based on guidance from the NIH (92). Therefore, in-person training in the responsible conduct of research will be prioritized in our one-month training intensive and our in-country training meetings to meet NIH requirements. Otherwise, in-person program components may be adapted to be sequential, hybrid (in-person; virtual) formats or entirely virtual, as needed. Transitioning to a virtual format also may require extending the duration of training over a longer period to ensure adequate coverage of material. These contingencies will be considered to ensure that each group of trainees receives high-quality, comprehensive training in relevant areas of expertise.
Conclusion
CONVERGE—Consortium for Violence-Prevention Research, Implementation, and Leadership Training for Excellence—is an innovative D43 training program and multi-institutional partnership led by Emory University and HMU that supports the development of a national network of scientific mentors, the career development of three cohorts of post-doctoral fellows to become scientific leaders, and institutional capacity strengthening in implementation research, science dissemination, leadership, and best practice in the prevention of gender-based violence and violence against children. The program benefits from a comprehensive mixed-methods evaluation plan that provides real-time feedback for continual process improvement. CONVERGE aspires to achieve the long-term impacts of expanding the evidence base in these thematic areas in ways that increase the allocation of funding to contextually relevant, efficacious violence-prevention programming that contributes to sustained, positive public-health impacts in Vietnam.
Ethics statement
Ethical review and approval are not required for this study in accordance with the local legislation and institutional requirements. The participants will provide their written informed consent to participate in this study prior to their participation.
Author contributions
KY: conceptualization, methodology, resources, investigation, writing—original draft, writing—review and editing, visualization, supervision, project administration, funding acquisition. SB: writing—original draft, writing—review and editing, visualization, methodology. DC and JS: writing—original draft, writing—review and editing, methodology, project administration. HV: funding acquisition, project administration, supervision, writing—original draft, writing—review and editing. AK: writing—original draft, methodology (of journal club), project administration. HN, IB, DP, MS, and AS: writing—original draft, writing—review and editing. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the National Institutes of Health, Fogarty International Center International, training grant number D43TW012188 (PI KY; MPI Giang). Provided monetary support for the CONVERGE training program’s implementation, completion, and evaluation.
Acknowledgments
The authors thank Mohammed Ali for guidance on the original proposal submission. The authors also thank Le Minh Giang (MPI) for comments on the protocol manuscript. The authors thank further the following individuals at Emory University for their generous letters of support: James Curran, former Dean of the Rollins School of Public Health; Linda McCauley, Dean of the Nell Hodgson Woodruff School of Nursing; Vikas Sukhatme, Dean of the School of Medicine; Jonathan Lewin, former Executive Vice President for Health Affairs; Jonathan Rupp, Director of the Injury Prevention Research Center; Jeffrey Lesser, Director of the Halle Institute for Global Research; and Parminder Suchdev, former Associate Director of the Emory Global Health Institute. The authors also thank the following individuals at Georgia State University (GSU) for their support of this initiative and of participating GSU faculty: Rodney Lyn, Dean of the School of Public Health, and Sara Rosen, Dean of the College of Arts and Sciences, for their support of this initiative and specifically of faculty at Georgia State University. Letters of support from university leadership in Vietnam also are valued: PHAM Van Manh, Vice Rector of Haiphong University of Medicine and Pharmacy (UMP); Nguyen Hoang BAC, Vice President of the Ho Chi Minh City UMP; Doan Quoc Hung, Vice Rector of Hanoi Medical University; and Nguyen Minh Tam, Vice Rector of Hue UMP. The authors also thank the following individuals for their willingness to serve on the CONVERGE Technical Advisory Committee: James Mercy, Director, Division of Violence Prevention, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; Heidi Stöckl, Professor at the Ludwig-Maximilians-University of Munich; and Ighoverha Ofotokun, Professor of Medicine, Emory University. The authors also thank all of the program faculty at Emory University, Georgia State University, the CDC, international Centers of Excellence for violence prevention research, and partner institutions in Vietnam who have offered to serve as training faculty, research mentors, and resources to our CONVERGE fellows. Finally, we thank Suha Khan, Maria Sullivan, Yvette Higgins-Sparks, Denise Catbay, Meghan Macaulay, Emily Chuba, and Robert Durr for administrative assistance at Emory University and Pham Phuong Mai for administrative assistance on the sub-award to Hanoi Medical University.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1181543/full#supplementary-material
Footnotes
References
1. Inter-Agency Standing Committee . Guidelines for integrating gender-based violence interventions in humanitarian action: reducing risk, promoting resilience and aiding recovery. Inter-Agency Standing Committee (2015).
2. Erickson-Schroth, L, Wu, SX, and Glaeser, E. Sexual and gender-based violence in lesbian, gay, bisexual, transgender, and queer communities. pp. 113–126 In: V. Ades, editor. Sexual and gender-based violence: a complete clinical guide. Cham, Switzerland: Springer Nature (2020).
3. Devries, KM, Mak, JYT, Garcia-Moreno, C, Petzold, M, Child, JC, Falder, G, et al. The global prevalence of intimate partner violence against women. Science. (2013) 340:1527–8. doi: 10.1126/science.1240937
4. Blondeel, K, Say, L, Chou, D, Toskin, I, Khosla, R, Scolaro, E, et al. Evidence and knowledge gaps on the disease burden in sexual and gender minorities: a review of systematic reviews. Int J Equity Health. (2016) 15:1–9. doi: 10.1186/s12939-016-0304-1
5. Decker, M, Latimore, A, Yasutake, S, Haviland, M, Ahmed, S, Blum, R, et al. Gender-based violence against adolescent and young adult women in low- and middle-income countries. J Adolesc Health. (2015) 56:188–96. doi: 10.1016/j.jadohealth.2014.09.003
6. Murray, CJ, Aravkin, AY, Zheng, P, Abbafati, C, Abbas, KM, Abbasi-Kangevari, M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1223–49. doi: 10.1016/S0140-6736(20)30752-2
7. Spencer, CM, and Stith, SM. Risk factors for male perpetration and female victimization of intimate partner homicide: a meta-analysis. Trauma Violence Abuse. (2020) 21:527–40. doi: 10.1177/1524838018781101
8. Stöckl, H, Devries, K, Rotstein, A, Abrahams, N, Campbell, J, Watts, C, et al. The global prevalence of intimate partner homicide: a systematic review. Lancet. (2013) 382:859–65. doi: 10.1016/S0140-6736(13)61030-2
9. Abrahams, N, Devries, K, Watts, C, Pallitto, C, Petzold, M, Shamu, S, et al. Worldwide prevalence of non-partner sexual violence: a systematic review. Lancet. (2014) 383:1648. doi: 10.1016/S0140-6736(13)62243-6
10. Kidman, R. Child marriage and intimate partner violence: a comparative study of 34 countries. Int J Epidemiol. (2017) 46:662–75. doi: 10.1093/ije/dyw225
11. Leonard, MM. Honor violence, crimes d'honneur, Ehrenmorde: improving the identification, risk assessment, and estimation of honor crimes internationally. Doctoral Dissertation, Universitaet Mannheim, Mannheim, Germany (2020).
12. Chong, NG, and Clark, JB. Human trafficking: a complex phenomenon of globalization and vulnerability. New York: Routledge (2017).
13. Heise, L. Violence against women: an integrated, ecological framework. Violence Against Women. (1998) 4:262–90. doi: 10.1177/1077801298004003002
14. Fulu, E, and Miedema, S. Violence against women: globalizing the integrated ecological model. Violence Against Women. (2015) 21:1431–55. doi: 10.1177/1077801215596244
15. James-Hawkins, L, Cheong, YF, Naved, RT, and Yount, KM. Gender norms, violence in childhood, and men’s coercive control in marriage: a multilevel analysis of young men in Bangladesh. Psychol Violence. (2018) 8:580. doi: 10.1037/vio0000152
16. James-Hawkins, L, Salazar, K, Hennink, MM, Ha, VS, and Yount, KM. Norms of masculinity and the cultural narrative of intimate partner violence among men in Vietnam. J Interpers Violence. (2019) 34:4421–42. doi: 10.1177/0886260516674941
17. Hynes, ME, Sterk, CE, Hennink, M, Patel, S, DePadilla, L, and Yount, KM. Exploring gender norms, agency and intimate partner violence among displaced Colombian women: a qualitative assessment. Glob Public Health. (2016) 11:17–33. doi: 10.1080/17441692.2015.1068825
18. Yount, KM, James-Hawkins, L, Cheong, YF, and Naved, RT. Men’s perpetration of partner violence in Bangladesh: community gender norms and violence in childhood. Psychol Men Masculinity. (2018) 19:117. doi: 10.1037/men0000069
19. Grose, RG, Hayford, SR, Cheong, YF, Garver, S, Kandala, N-B, and Yount, KM. Community influences on female genital mutilation/cutting in Kenya: norms, opportunities, and ethnic diversity. J Health Soc Behav. (2019) 60:84–100. doi: 10.1177/0022146518821870
20. Yount, KM, Crandall, A, Cheong, YF, Osypuk, T, Naved, RT, Bates, LM, et al. Child marriage and intimate partner violence in rural Bangladesh: a multilevel longitudinal analysis. Demography. (2016) 53:1821–52. doi: 10.1007/s13524-016-0520-8
21. Heise, LL, and Kotsadam, A. Cross-national and multilevel correlates of partner violence: an analysis of data from population-based surveys. Lancet Glob Health. (2015) 3:e332–40. doi: 10.1016/S2214-109X(15)00013-3
22. Yount, KM, Pham, HT, Minh, TH, Krause, KE, Hoang, TA, Schuler, SR, et al. Violence in childhood, attitudes about partner violence, and partner violence perpetration among men in Vietnam. Ann Epidemiol. (2014) 24:333–9. doi: 10.1016/j.annepidem.2014.02.004
23. Krug, EG, Mercy, JA, Dahlberg, LL, and Zwi, AB. The world report on violence and health. Lancet. (2002) 360:1083–8. doi: 10.1016/S0140-6736(02)11133-0
24. Campbell, J, Jones, AS, Dienemann, J, Kub, J, Schollenberger, J, O'Campo, P, et al. Intimate partner violence and physical health consequences. Arch Intern Med. (2002) 162:1157–63. doi: 10.1001/archinte.162.10.1157
25. Gilbert, R, Widom, CS, Browne, K, Fergusson, D, Webb, E, and Janson, S. Burden and consequences of child maltreatment in high-income countries. Lancet. (2009) 373:68–81. doi: 10.1016/S0140-6736(08)61706-7
26. Felitti, VJ, Anda, RF, Nordenberg, D, Williamson, DF, Spitz, AM, Edwards, V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the adverse childhood experiences (ACE) study. Am J Prev Med. (1998) 14:245–58. doi: 10.1016/S0749-3797(98)00017-8
27. Widom, CS, Schuck, AM, and White, HR. An examination of pathways from childhood victimization to violence: the role of early aggression and problematic alcohol use. Violence Vict. (2006) 21:675–90. doi: 10.1891/0886-6708.21.6.675
28. The Government of the Socialist Republic of Viet Nam, Nam TUNiV . One strategic plan 2017–2021. Vietnam: The Government of the Socialist Republic of Viet Nam, The United Nations in Viet Nam (2017).
29. Yount, K, Miedema, S, Krause, K, Clark, C, Chen, J, and del Rio, C. GROW: a model for mentorship to advance women's leadership in global health. Glob Health Epidemiol Genom. (2018) 3:3. doi: 10.1017/gheg.2018.5
30. Yount, KM, Cheong, YF, Miedema, SS, Chen, JS, Menstell, E, Maxwell, L, et al. Gender equality in global health leadership: cross-sectional survey of global health graduates. Glob Public Health. (2020) 15:852–64. doi: 10.1080/17441692.2019.1701057
31. Hillis, S, Mercy, J, Amobi, A, and Kress, H. Global prevalence of past-year violence against children: a systematic review and minimum estimates. Pediatrics. (2016) 137:e20154079. doi: 10.1542/peds.2015-4079
32. United Nations, Division of Economic and Social Affairs, Population Division In: U Nations, editor. World population prospects 2019. Online edition. Rev. 1 ed. New York, NY: (2019)
33. Keeley, B, Little, C, and Zuehlke, E. The state of the World's children 2019: children, food and nutrition--growing well in a changing world. New York: UNICEF (2019).
34. Dunkle, KL, Jewkes, RK, Brown, HC, Yoshihama, M, Gray, GE, McIntyre, JA, et al. Prevalence and patterns of gender-based violence and revictimization among women attending antenatal clinics in Soweto. S Afr Am J Epidemiol. (2004) 160:230–9. doi: 10.1093/aje/kwh194
35. Finkelhor, D, Ormrod, RK, and Turner, HA. Poly-victimization: a neglected component in child victimization. Child Abuse Negl. (2007) 31:7–26. doi: 10.1016/j.chiabu.2006.06.008
36. Yount, KM, Krause, KH, and Miedema, SS. Preventing gender-based violence victimization in adolescent girls in lower-income countries: systematic review of reviews. Soc Sci Med. (2017) 192:1–13. doi: 10.1016/j.socscimed.2017.08.038
37. Fleming, PJ, McCleary-Sills, J, Morton, M, Levtov, R, Heilman, B, and Barker, G. Risk factors for men’s lifetime perpetration of physical violence against intimate partners: results from the international men and gender equality survey (IMAGES) in eight countries. PLoS One. (2015) 10:e0118639. doi: 10.1371/journal.pone.0118639
38. Fulu, E, Jewkes, R, Roselli, T, and Garcia-Moreno, C. Prevalence of and factors associated with male perpetration of intimate partner violence: findings from the UN multi-country cross-sectional study on men and violence in Asia and the Pacific. Lancet Glob Health. (2013) 1:e187–207. doi: 10.1016/S2214-109X(13)70074-3
39. Yount, KM, Miedema, S, Martin, C, Crandall, A, and Naved, RT. Men’s coercive control, partner violence perpetration, and life satisfaction in Bangladesh. Sex Roles. (2016) 74:450–63. doi: 10.1007/s11199-016-0584-3
40. Yount, KM, Roof, KA, and Naved, RT. Multilevel influences on men’s partner violence justification, control over family decisions, and partner violence perpetration in Bangladesh. Psychol Violence. (2018) 8:367. doi: 10.1037/vio0000171
41. Swedo, EA, Sumner, SA, Hillis, SD, Aluzimbi, G, Apondi, R, Atuchukwu, VO, et al. Prevalence of violence victimization and perpetration among persons aged 13–24 years — four sub-Saharan African countries, 2013–2015. MMWR Morb Mortal Wkly Rep. (2019) 68:350–5. doi: 10.15585/mmwr.mm6815a3
42. Guedes, A, Bott, S, Garcia-Moreno, C, and Colombini, M. Bridging the gaps: a global review of intersections of violence against women and violence against children. Glob Health Action. (2016) 9:31516. doi: 10.3402/gha.v9.31516
43. Nadal, KL, Whitman, CN, Davis, LS, Erazo, T, and Davidoff, KC. Microaggressions toward lesbian, gay, bisexual, transgender, queer, and genderqueer people: a review of the literature. J Sex Res. (2016) 53:488–508. doi: 10.1080/00224499.2016.1142495
44. Hillis, SD, Mercy, JA, and Saul, JR. The enduring impact of violence against children. Psychol Health Med. (2017) 22:393–405. doi: 10.1080/13548506.2016.1153679
45. Nguyen, KH, Padilla, M, Villaveces, A, Patel, P, Atuchukwu, V, Onotu, D, et al. Coerced and forced sexual initiation and its association with negative health outcomes among youth: results from the Nigeria, Uganda, and Zambia violence against children surveys. Child Abuse Negl. (2019) 96:104074. doi: 10.1016/j.chiabu.2019.104074
46. Grose, RG, Roof, KA, Semenza, DC, Leroux, X, and Yount, KM. Mental health, empowerment, and violence against young women in lower-income countries: a review of reviews. Aggress Violent Behav. (2019) 46:25–36. doi: 10.1016/j.avb.2019.01.007
47. Yount, KM, DiGirolamo, AM, and Ramakrishnan, U. Impacts of domestic violence on child growth and nutrition: a conceptual review of the pathways of influence. Soc Sci Med. (2011) 72:1534–54. doi: 10.1016/j.socscimed.2011.02.042
48. Lorenzetti, L, Wells, L, Logie, CH, and Callaghan, T. Understanding and preventing domestic violence in the lives of gender and sexually diverse persons. Can J Hum Sex. (2017) 26:175–85. doi: 10.3138/cjhs.2016-0007
49. Treves-Kagan, S, El Ayadi, AM, Morris, JL, Graham, LM, Grignon, JS, Ntswane, L, et al. Sexual and physical violence in childhood is associated with adult intimate partner violence and nonpartner sexual violence in a representative sample of rural south African men and women. J Interpers Violence. (2019) 36:NP7415–38. doi: 10.1177/0886260519827661
50. Yount, KM, Pham, HT, Krause, KE, Minh, TH, Hoang, TA, Vander Ende, KE, et al. Violence in childhood, attitudes about partner violence, and partner violence perpetration among men in Vietnam. Ann Epidemiol. (2014) 24:333–9. doi: 10.1016/j.annepidem.2014.02.004
51. Semenza, DC, Roof, KA, James-Hawkins, L, Cheong, YF, Naved, RT, and Yount, KM. Gender-equitable parental decision making and intimate partner violence perpetration in Bangladesh. J Marriage Fam. (2019) 81:920–35. doi: 10.1111/jomf.12579
52. Vander Ende, KE, Yount, KM, Dynes, MM, and Sibley, LM. Community-level correlates of intimate partner violence against women globally: a systematic review. Soc Sci Med. (2012) 75:1143–55. doi: 10.1016/j.socscimed.2012.05.027
53. Clark, CJ, Ferguson, G, Shrestha, B, Shrestha, PN, Oakes, JM, Gupta, J, et al. Social norms and women's risk of intimate partner violence in Nepal. Soc Sci Med. (2018) 202:162–9. doi: 10.1016/j.socscimed.2018.02.017
54. Bondestam, F, and Lundqvist, M. Sexual harassment in higher education–a systematic review. Eur J High Educ. (2020) 10:397–419. doi: 10.1080/21568235.2020.1729833
55. Cortina, LM, and Areguin, MA. Putting people down and pushing them out: sexual harassment in the workplace. Annu Rev Organ Psych Organ Behav. (2021) 8:285–309. doi: 10.1146/annurev-orgpsych-012420-055606
56. Chon, DS, and Clifford, JE. The impacts of international rape Laws upon official rape rates. Int J Offender Ther Comp Criminol. (2021) 65:244–61. doi: 10.1177/0306624X20952399
57. Omidakhsh, N, and Heymann, J. Improved child marriage laws and its association with changing attitudes and experiences of intimate partner violence: a comparative multi-national study. J Glob Health. (2020) 10:010707. doi: 10.7189/jogh.10.010707
58. Murthy, P, and Ogulnick, J. The role of technology in women’s empowerment and well-being and addressing gender-based violence. pp. 57–68. In. (Eds.) P. Murthy and A Ansehl. Technology and Global Public Health. Cham, Switzerland: Springer Nature (2020).
59. Bergenfeld, I, Cheong, YF, Minh, TH, Trang, QT, and Yount, KM. Effects of exposure to sexually explicit material on sexually violent behavior among first-year university men in Vietnam. PLoS One. (2022) 17:e0275246. doi: 10.1371/journal.pone.0275246
60. Treves-Kagan, S, Peterman, A, Gottfredson, NC, Villaveces, A, Moracco, KE, and Maman, S. Love in the time of war: identifying neighborhood-level predictors of intimate partner violence from a longitudinal study in refugee-hosting communities. J Interpers Violence. 37:NP10170-NP10195. doi: 10.1177/0886260520986267
61. Kim, J. The diffusion of international Women’s rights norms to individual attitudes: the differential roles of world polity and world society. Sociol Dev. (2020) 6:459–92. doi: 10.1525/sod.2020.6.4.459
62. Pierotti, RS. Increasing rejection of intimate partner violence: evidence of global cultural diffusion. Am Sociol Rev. (2013) 78:240–65. doi: 10.1177/0003122413480363
63. Simmons, BA, Lloyd, P, and Stewart, BM. The global diffusion of law: transnational crime and the case of human trafficking. Int Organ. (2018) 72:249. doi: 10.1017/S0020818318000036
64. García-Moreno, C, and Amin, A. The sustainable development goals, violence and women’s and children’s health. Bull World Health Organ. (2016) 94:396. doi: 10.2471/BLT.16.172205
65. Yount, KM, Cheong, YF, Khan, Z, Bergenfeld, I, Kaslow, N, Clark, CJ, et al. Global measurement of physical intimate partner violence to monitor sustainable development goal 5. medRxiv. (2021). doi: 10.1101/2021.07.01.21259594
66. Yount, KM, Cheong, YF, Khan, Z, Bergenfeld, I, Kaslow, N, and Clark, CJ. Global measurement of intimate partner violence to monitor sustainable development goal 5. BMC Public Health. (2022) 22:465. doi: 10.1186/s12889-022-12822-9
67. Grose, R, Chen, JS, Roof, K, Rachel, S, and Yount, KM. Sexual and reproductive health outcomes of violence against women and girl in lower-income countries: a review of reviews. J Sex Res. (2020) 58:1–20. doi: 10.1080/00224499.2019.1707466
68. Cappa, C, and Petrowski, N. Thirty years after the adoption of the convention on the rights of the child: progress and challenges in building statistical evidence on violence against children. Child Abuse Negl. (2020). doi: 10.1016/j.chiabu.2020.104460
69. Child Protection Monitoring and Evaluation Reference Group . Measuring violence against children: inventory and assessment of quantitative studies. New York, NY: UNICEF (2014).
70. United Nations Committee on the Rights of the Child . General comment no. 13 (2011): the right of the child to freedom from all forms of violence, UN document CRC/C/GC/13. Geneva: Office of the High Commissioner for Human Rights (2011).
71. MOLISA, GSO, UNFPA . National Study on violence against women in Vietnam 2019 - journey for change. Hanoi: UNFPA (2020).
72. World Health Organization, Vietnam Ministry of Health, Vietnam Ministry of Training and Education . The 2019 global school-based student health survey in Viet Nam. Hanoi: World Health Organization, Western Pacific Region; Vietnam Ministry of Health, Vietnam Ministry of Education and Training (2021).
73. Voice of Vietnam: More than 4,000 were abused for two years 2019–2021. Available at: https://vov.vn/xa-hoi/tin-24h/hon-4000-tre-em-bi-xam-hai-trong-2-nam-qua-900908.vov.
74. Yount, KM, Higgins, EM, VanderEnde, KE, Krause, KH, Minh, TH, Schuler, SR, et al. Men’s perpetration of intimate partner violence in Vietnam: gendered social learning and the challenges of masculinity. Men Masculinities. (2016) 19:64–84. doi: 10.1177/1097184X15572896
75. Anderson, KM, Bergenfeld, I, Cheong, YF, Minh, TH, and Yount, KM. Childhood maltreatment class and sexually violent behavior among university men in Vietnam. SSM Popul Health. (2022) 18:101103. doi: 10.1016/j.ssmph.2022.101103
76. Fang, X, Fry, DA, Brown, DS, Mercy, JA, Dunne, MP, Butchart, AR, et al. The burden of child maltreatment in the East Asia and Pacific region. Child Abuse Negl. (2015) 42:146–62. doi: 10.1016/j.chiabu.2015.02.012
77. Nguyen, HT. Navigating identity, ethnicity and politics: a case study of gender variance in the central highlands of Vietnam. Int J Mascul Stud. (2016) 11:255–69. doi: 10.1080/18902138.2016.1259845
78. Miedema, SS, Yount, KM, Chirwa, E, Dunkle, K, and Fulu, E. Integrating male sexual diversity into violence prevention efforts with men and boys: evidence from the Asia-Pacific region. Cult Health Sex. (2017) 19:208–24. doi: 10.1080/13691058.2016.1214747
79. Miedema, SS, Browne, I, and Yount, KM. An intersectional burden: gender and sexual stigma against toms in Thailand. Soc Sci Med. (2022) 292:114591. doi: 10.1016/j.socscimed.2021.114591
80. Halvorson, MA, Finney, JW, Bi, X, Maisel, NC, Hayashi, KP, Weitlauf, JC, et al. The changing faces of mentorship: application of a developmental network framework in a health services research career development program. Clin Transl Sci. (2015) 8:824–9. doi: 10.1111/cts.12355
81. Chi, BH, Belizan, JM, Blas, MM, Chuang, A, Wilson, MD, Chibwesha, CJ, et al. Evaluating academic mentorship programs in low- and middle-income country institutions: proposed framework and metrics. Am J Trop Med Hyg. (2019) 100:36–41. doi: 10.4269/ajtmh.18-0561
82. Cole, DC, Johnson, N, Mejia, R, McCullough, H, Turcotte-Tremblay, A-M, Barnoya, J, et al. Mentoring health researchers globally: diverse experiences, programmes, challenges and responses. Glob Public Health. (2016) 11:1093–108. doi: 10.1080/17441692.2015.1057091
83. Prasad, S, Sopdie, E, Meya, D, Kalbarczyk, A, and Garcia, PJ. Conceptual framework of mentoring in low- and middle-income countries to advance global health. Am J Trop Med Hyg. (2019) 100:9–14. doi: 10.4269/ajtmh.18-0557
84. Comeau, D, Mishkin, K, Tukvadze, N, Avaliani, Z, Kempker, R, Sthreshley, L, et al. Mentoring in global health: formative evaluation of tuberculosis research training programs in Ethiopia and Georgia. Am J Trop Med Hyg. (2018) 99:565–77. doi: 10.4269/ajtmh.17-0746
85. Lescano, AG, Cohen, CR, Raj, T, Rispel, L, Garcia, PJ, Zunt, JR, et al. Strengthening mentoring in low- and middle-income countries to advance global health research: an overview. Am J Trop Med Hyg. (2019) 100:3–8. doi: 10.4269/ajtmh.18-0556
86. Hamer, DH, Hansoti, B, Prabhakaran, D, Huffman, MD, Nxumalo, N, Fox, MP, et al. Global health research mentoring competencies for individuals and institutions in low- and middle-income countries. Am J Trop Med Hyg. (2019) 100:15–9. doi: 10.4269/ajtmh.18-0558
87. Katz, F, and Glass, RI. Mentorship training is essential to advancing global health research. Am J Trop Med Hyg. (2019) 100:1–2. doi: 10.4269/ajtmh.18-0694
88. Comeau, DL, Derbew, M, and Mariam, DH. Influential mentors: a guidebook for building mentoring skills and capacity (Ethiopia edition). Atlanta, GA: Emory University and Addis Ababa University (2019) Available at: https://www.influentialmentors.com/.
89. Hamer, DH, Hansoti, B, Prabhakaran, D, Huffman, MD, Nxumalo, N, Fox, MP, et al. Global health research mentoring competencies for individuals and institutions in low-and middle-income countries. Am J Trop Med Hyg. (2019) 100:15. doi: 10.4269/ajtmh.18-0558
90. Pfund, C, House, SC, Asquith, P, Fleming, MF, Buhr, KA, Burnham, EL, et al. Training mentors of clinical and translational research scholars: a randomized controlled trial. Acad Med. (2014) 89:774. doi: 10.1097/ACM.0000000000000218
91. DiSC® E . Available at: https://www.discprofile.com/what-is-disc.
92. Health NIo . NOT-OD-22-055. (2022). Available at: https://grants.nih.gov/grants/guide/notice-files/NOT-OD-22-055.html.
94. Glasgow, RE, Vogt, TM, and Boles, SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. (1999) 89:1322–7. doi: 10.2105/AJPH.89.9.1322
95. Aarons, GA, Hurlburt, M, and Horwitz, SMC. Advancing a conceptual model of evidence-based practice implementation in public service sectors. Adm Policy Ment Health Ment Health Serv Res. (2011) 38:4–23. doi: 10.1007/s10488-010-0327-7
96. Damschroder, LJ, Aron, DC, Keith, RE, Kirsh, SR, Alexander, JA, and Lowery, JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. (2009) 4:50. doi: 10.1186/1748-5908-4-50
97. Palinkas, LA, Aarons, GA, Horwitz, S, Chamberlain, P, Hurlburt, M, and Landsverk, J. Mixed method designs in implementation research. Adm Policy Ment Health Ment Health Serv Res. (2011) 38:44–53. doi: 10.1007/s10488-010-0314-z
98. Proctor, E, Silmere, H, Raghavan, R, Hovmand, P, Aarons, G, Bunger, A, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health Ment Health Serv Res. (2011) 38:65–76. doi: 10.1007/s10488-010-0319-7
99. Birken, SA, Bunger, AC, Powell, BJ, Turner, K, Clary, AS, Klaman, SL, et al. Organizational theory for dissemination and implementation research. Implement Sci. (2017) 12:1–15. doi: 10.1186/s13012-017-0592-x
100. Self-Brown, S, and Whitaker, DJ. Introduction to the special issue on using technology to address child maltreatment: prevention, intervention, and research. Child Maltreat. (2008) 13:319. doi: 10.1177/1077559508323764
101. Aarons, GA, Green, AE, Palinkas, LA, Self-Brown, S, Whitaker, DJ, Lutzker, JR, et al. Dynamic adaptation process to implement an evidence-based child maltreatment intervention. Implement Sci. (2012) 7:1. doi: 10.1186/1748-5908-7-32
102. Chambers, DA, Glasgow, RE, and Stange, KC. The dynamic sustainability framework: addressing the paradox of sustainment amid ongoing change. Implement Sci. (2013) 8:1–11. doi: 10.1186/1748-5908-8-117
103. Kirkpatrick, D, and Kirkpatrick, J. Evaluating training programs: the four levels. San Francisco: Berrett-Koehler Publishers (2006).
104. Upadhyay, K, Goel, S, and John, P. Developing a capacity building training model for public health managers of low and middle income countries. PLoS One. (2023) 18:e0272793. doi: 10.1371/journal.pone.0272793
105. Gamtessa, LC, Tiyare, FT, and Kebede, KM. Evaluation of helping babies breathe and essential care for every baby training in southern nations nationalities and people’s region, Ethiopia: applying a Kirkpatrick training evaluation model. BMC Res Notes. (2020) 13:1–4. doi: 10.1186/s13104-020-05394-7
106. Kazemi Shishavan, M, and Alizadeh, M. Evaluation of a research methods course for clinical residents. Res Dev Med Educ. (2019) 8:124–30. doi: 10.15171/rdme.2019.022
107. Dorri, S, Akbari, M, and Sedeh, MD. Kirkpatrick evaluation model for in-service training on cardiopulmonary resuscitation. Iran J Nurs Midwifery Res. (2016) 21:493. doi: 10.4103/1735-9066.193396
108. Hamilton, J, Stevens, G, and Girdler, S. Becoming a mentor: the impact of training and the experience of mentoring university students on the autism spectrum. PLoS One. (2016) 11:e0153204. doi: 10.1371/journal.pone.0153204
109. Nightingale, J, Fowler-Davis, S, Grafton, K, Kelly, S, Langham, C, Lewis, R, et al. The role of allied health professions and nursing research internships in developing a research culture: a mixed-methods exploration of stakeholder perspectives. Health Res Policy Syst. (2020) 18:1–7. doi: 10.1186/s12961-020-00638-1
110. Smidt, A, Balandin, S, Sigafoos, J, and Reed, VA. The Kirkpatrick model: a useful tool for evaluating training outcomes. J Intellect Dev Disabil. (2009) 34:113:266–74. doi: 10.1080/13668250903093125
111. Carless, SA, Wearing, AJ, and Mann, L. A short measure of transformational leadership. J Bus Psychol. (2000) 14:389–405. doi: 10.1023/A:1022991115523
Glossary
Keywords: gender-based violence, implementation science, leadership, mentorship, research capacity strengthening, Vietnam, violence against children
Citation: Yount KM, Comeau D, Blake SC, Sales J, Sacks M, Nicol H, Bergenfeld I, Kalokhe AS, Stein AD, Whitaker DJ, Parrott D and Van HTH (2023) Consortium for violence prevention research, leadership training, and implementation for excellence (CONVERGE): a protocol to train science leaders in gender-based-violence and violence-against-children research for impact. Front. Public Health. 11:1181543. doi: 10.3389/fpubh.2023.1181543
Edited by:
Julie Ann Robinson, Flinders University, AustraliaReviewed by:
Phuong Thi Thu Dinh, Hue University, VietnamCatherine Baillie Abidi, Mount Saint Vincent University, Canada
Copyright © 2023 Yount, Comeau, Blake, Sales, Sacks, Nicol, Bergenfeld, Kalokhe, Stein, Whitaker, Parrott and Van. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kathryn M. Yount, a3lvdW50QGVtb3J5LmVkdQ==