
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health, 20 September 2023
Sec. Aging and Public Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1169192
This article is part of the Research TopicQuality of Life Improvement: Smart Approaches for the Working and Aging PopulationsView all 22 articles
 Ishaya Gambo1,2*
Ishaya Gambo1,2* M. Victoria Bueno-Delgado3
M. Victoria Bueno-Delgado3 Kerli Mooses1
Kerli Mooses1 Francisco J. Melero Muñoz3,4
Francisco J. Melero Muñoz3,4 Rina Zviel-Girshin5
Rina Zviel-Girshin5 Aliaksei Andrushevich6,7
Aliaksei Andrushevich6,7 Michael Mrissa8,9Agnieszka Landowska10
Michael Mrissa8,9Agnieszka Landowska10 Kuldar Taveter1
Kuldar Taveter1While several technological solutions are available for older adults to improve their wellbeing and quality of life, little is known about the gaps between the needs, provided solutions, and their adoption from a more pragmatic perspective. This paper reports on reviewing existing technological solutions for older adults, which span the work life, life in the community, and wellbeing at home. We analyzed 50 different solutions to uncover both negative and positive features of these solutions from the perspective of the impact of technology adoption on the quality of life of older adults. Our approach harnesses holistic reasoning to determine the most suitable technologies available today and provides suggestions for improvement toward designing and implementing better solutions.
Recently, technological solutions have been discovered to cater for the challenges associated with the ageing population (1). Consequently, technology adoption is increasingly important in public health intervention programs to improve the older population's Quality of Life (QoL). Indeed, both mature and evolving technologies have been successfully applied for improving the QoL and health of older adults (2–4).
However, despite the proliferation of technological solutions, and their inherent benefits in improving the QoL of older adults, there seems to be a considerable gap in terms of technology adoption. On one hand, the low level of adoption of new technologies in the ageing population is due to the frequent reluctance and lack of motivation of older adults, and insufficient support available to them (5, 6). On the other hand, the low level of adoption rate is connected to the lack of compliance with policies and strategic frameworks of healthcare and wellbeing. Besides, other complexities associated with multiple factors, such as lack of awareness of potential impact and prevailing bureaucracy, have had a negative impact on technology adoption (1, 7, 8). In addition, there is a lack of quality studies of technology adoption (9–11).
From a more technical perspective, the inability to meet older adults' requirements, including emotional requirements (12), in the design of the technological solutions could endanger human lives (13), which eventually also leads to a low level of adoption. Remarkably, several researchers have pointed out that if the needs of older adults are not adequately captured in the analysis and design process, the system's functionality will not be trusted and reliable (14–16).
The overarching goal of this paper is to analyze the existing technical solutions, as contained in the publications, projects, and patents. In the paper, we answered two important research questions: (i) What are the gaps reported in the literature between the needs, production, and adoption of technology for ageing? and (ii) what are the prevalent challenges associated with technology adoption?
This paper analyzes a selection of recent and most relevant technical solutions from the technology adoption perspective. The technologies have been selected as part of the SHELDON COST action number CA16226 based on a review of existing work by the members of the action. Due to the very large amount of activity in this domain, it does not constitute an exhaustive overview, however it provides a selection of the current most relevant initiatives identified by the members of the COST action. Firstly, our analysis unveils both negative and positive aspects of technology adoption on QoL of older adults. Secondly, we further evaluate the results of the analysis by means of statistical measures. Thirdly, the main contribution of this paper are the recommendations and policy implications we can deduce from the analysis. Clearly, the focus is to understand the gaps between the needs, production, and adoption of solutions targeted at older adults.
The structure of the paper is as follows. Section 2 describes the background and motivation, while Section 3 discusses the theoretical frameworks used as guidelines for analyzing the technical solutions. This is followed by the description of our methodological approach in Section 4. Section 5 contains the analysis of the results and Section 6 presents the discussions. Section 7 presents the strengths and limitations of the study. Finally, Section 8 concludes the paper with some recommendations and suggestions.
There is a rapid growth in the number of older adults across all continents. According to Ollevier et al., (17), the expected growth of the number of older adults would be well above 60% in another 15 years. According to the reports on the ageing of the world population by the United Nations (18, 19), by 2030, ~1 billion older adults will make up 12% of the whole world population (20). In this context, a number of challenging problems will have to be solved because of the ageing population (21).
Technology has a great potential in providing the support needed for enhancing the healthy lifestyle of older adults (22–24). The development and adoption of this kind of technology is a crucial factor for older adults to compensate for psychological, social, and biological changes occurring in them over time (2), such as the loss of adaptability and functional impairments (25).
Interestingly, the technologies available for older adults have engendered significant changes in recent times. Notably, we have witnessed the use of assistive technologies (22, 26, 27), health monitoring systems, the Internet of Things (IoT) solutions (e.g., wearable devices) (23, 28, 29), smart sensors (3, 30), medication reminders (31), telemedicine applications (32), and social networking applications (9) for enhancing the QoL of older adults.
It is noteworthy that the Ambient Assisted Living (AAL) and Enhanced Living Environments (ELE) technologies comprise significant contributions from researchers in ICT and psychology (33–35). Remarkably, the idea of an ELE refers to the ICT-related part of AAL, which means that ELEs incorporate all ICT advancements to assist AAL (36). The psychological aspects of AAL deal with human behaviors, affects, emotions, and desires. On the other hand, ELE focuses on designing and implementing suitable technologies based on psychological theories of automated systems (37). Additionally, ELE incorporates the most recent innovative achievements in IoT to create better ICT solutions for improving the health and wellbeing of older adults (36).
Encouraging older adults to adopt the technologies aimed to improve their health and wellbeing has received a lot of attention in the research literature (38–40). It is worth of mentioning that technology is repeatedly mentioned to support ageing in place (41, 42). For example, in the FeelGood project (43), a framework was created for supporting and promoting self-management of wellbeing concerns through technology adoption. Also, technological innovations in the Netherlands have enabled to increase the number of dwelling places suitable for older adults (44). However, while most organizations are optimistic about the impact of technology on improving healthy lifestyles of older adults, they tend to focus on its cost rather than its benefits (45–49).
Although technological innovation promises to continuously enhance the health and wellbeing of older adults, the seamless adoption of such technologies from both the human and technical perspectives can be a limiting factor for a sustainable breakthrough or progress (50, 51). Therefore, there is a need to identify and investigate existing solutions and analyze them for their strengths and weaknesses from the technology adoption perspective.
Although the terms “technology acceptance” and “technology adoption” are sometimes used interchangeably, they are not synonymous. On the one hand, “technology acceptance” is a perception of technology that is impacted by various factors. These factors include frequency of use, usage experience, ease of use, usefulness, attitude, usage knowledge and enjoyment (52). On the other hand, “technology adoption” is a process that starts with knowledge of the technology and ends with acceptance and full utilization of the technology. Accepting technology without adopting it is therefore conceivable, but full adoption is impossible without acceptance (53). In the literature, several technology adoption theories exist. However, this paper examines technology adoption among older adults using two theoretical frameworks. The first is the Technology Acceptance Model (TAM) by Davis (54), and the second is Everett Rogers' Diffusion of Innovation (DOI) theory (55).
TAM is a widely used adoption theory (56–58) that focuses on how people make technology adoption decisions (59, 60). It was derived from the Theory of Reasoned Action (TRA), which is a socio-psychological theory that determines how people will act given their preceding attitudes and Behavioral Intentions (BI) (61, 62). BI is “the degree to which an individual has formulated conscious plans to perform or not to perform some specified behavior in the future (54).” It is predicted by both attitude and perceived usefulness (53).
Further, TAM was formulated to predict and explain technology acceptance and use. In this regard, Davis et al. (59) proposed two significant factors as critical determinants of technology adoption: Perceived Usefulness (PU) and Perceived Ease of Use (PEOU). According to Davis (54), Perceived Usefulness is “the degree to which a person believes that using a particular system would enhance his or her job performance,” while Perceived Ease Of Use is “the degree to which a person believes that using a particular system would be free of effort.” Thus, PU and PEOU are technological variables that emphasize people's attitudes, perceptions, and interactions with technology (63).
Over the years, this area has further developed and TAM has been extended. One such extension is TAM 2, which replaced the attitudinal component of TAM with a social element termed as Subjective Norm (SN) (64). The theory behind TAM 2 claims that cognitive instrumental processes explain perceived utility and usage intentions (e.g., job relevance, output quality, outcome demonstrability, and perceived simplicity of use) as well as social influence processes (subjective norm, voluntariness, and image) (64). Another extension of standard TAM is the Unified Theory of Acceptance and Use of Technology (UTAUT). UTAUT differs from TAM in that it includes social and environmental variables and technological factors as determinants of behavioral intention (65).
Notably, many studies have shown that a strong intention of technology usage results in a high probability of actual usage (66). This implies that a person intending to use technology will most likely use it. As a foundational technology adoption theory, TAM is useful in examining the potential adoption of a given technology among older adults. Yap et al. (67) divided the antecedents of technology usage among older adults into the following seven categories: technological, psychological, social, behavioral, cost-related, personal, and environmental. Antecedent, in this case, indicates pre-existing factors that determine or influence technology adoption by older adults. The source (67) reviewed twenty-six (26) research articles on technology adoption, most of them focusing on TAM and its variables PU and PEOU.
Everett Rogers did put forward the Diffusion of Innovation (DOI) theory for examining technology adoption and determining how technological innovations diffuse within communities (55, 68). On one hand, diffusion is the process by which an innovation spreads over time and through specific channels among the people within a social system (69, 70). On the other hand, innovation is “an idea, practice, or object perceived as new by an individual or other unit of adoption (69, 70).”
Rogers et al. (69) distinguished between the processes of innovation decisions by individuals and groups. To reduce innovation uncertainty, decision-making units must follow a specific procedure before deciding whether to accept or reject an innovation (69, 70). As observed by Zhang (71), communication channels, innovation attributes, adopter characteristics, time, and the social system are the five essential variables that determine the success of innovation. Regarding technology adoption, the DOI theory recognizes the following five stages: knowledge or awareness, persuasion, decision, implementation, and confirmation.
We observed that TAM is limited as a theory because of its position that technology adoption by older adults solely depends on the features of particular technologies to be adopted. In reality, older adults also think about how a technology enables their lifestyle in ways they value (67). Therefore, TAM does not sufficiently explain the adoption of technologies by older adults. To compensate for that, we have also incorporated the Diffusion of Innovation (DOI) theory to complement TAM for a more holistic analysis. Overall, the growing impact of technology on older adults cannot be underestimated. It has been observed that technology usage improves social, mental, and emotional wellbeing of older adults, while also decreasing their feeling of loneliness (72). Therefore, we used both TAM and DOI as the significant drivers of technology adoption among older adults as has also been reported in Heo et al., Mahoney, Hastall et al., and Cahill et al. (73–76).
Differently, we blended the TAM and DOI theories to provide adequate insight into the analysis of technology adoption among older adults for improving the QoL and facilitating healthy lifestyle. In particular, we used from the TAM model as technological issues the improved wellbeing, ease of use, willingness to accept technology, and understandability. At the same time, we used from the DOI model as technological issues the technological awareness, willingness to accept technology, effectiveness, and understandability. Based on these technological issues identified from the two theories, we formulated hypotheses for statistical analysis.
We designed our study using a mixed method consisting of the methods of qualitative explorative approach (77), and quantitative research (78), which have been synthesized as is described by Dixon-Woods et al. (79). The qualitative explorative approach focuses on a critical and extensive review of the existing solutions, while the quantitative research involves using statistical measures to further improve the analysis.
We followed the systematic process described in Figure 1 to analyze the shreds of evidence reported about the existing solutions by answering the research questions mentioned in Section 1. Figure 1 is a modified version of the three-step process of systematic review: planning, execution (i.e., carrying out the research), and result analysis (80).
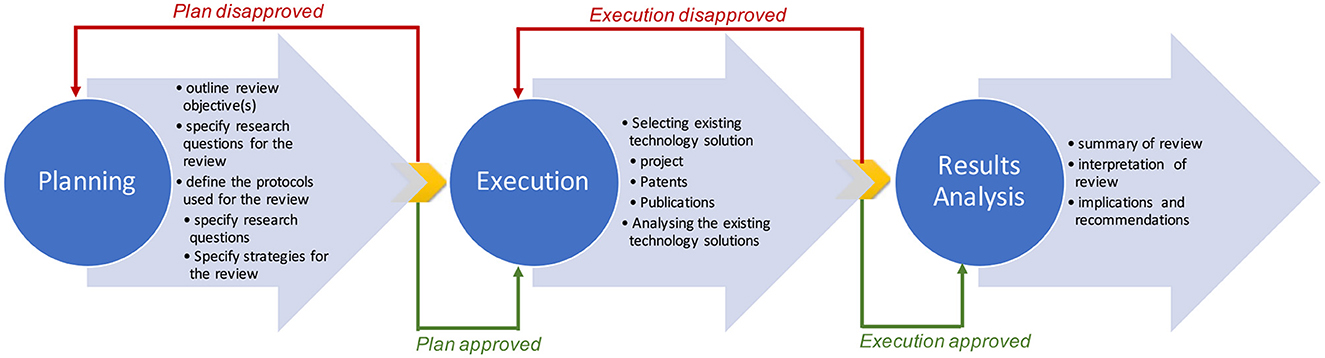
Figure 1. Systematic process for technology adoption review: adapted from Kitchenham (80).
In the “planning” phase, we outlined our review objective(s), specified the questions for the review, and defined the protocols used for the review. In the “execution” phase, we selected and analyzed the existing technology solutions. Finally, we summarized the review during the “result analysis” phase.
Overall, we analyzed 50 existing solutions1—projects, patents, and publications—to uncover both negative and positive examples of technology adoption and their impact on QoL of older adults. The selected 50 solutions used for the technology adoption review are part of the SHELDON COST action number CA16226 by the SHELDON Working Group 4.4, which aims to review the current state of the art in technologies for smart living environments. The technologies presented are chosen by the action members based on their relevance and impact in this domain, especially for improving the QoL of older adults. The authors and other COST action members selected the most relevant technologies, projects, patents, and papers for this paper's analysis. We used keyword-based queries in the main online search tools that give a representative sample of the most promising initiatives from the COST action, which include projects, patents, or technological systems.
All the authors were involved in reviewing the 50 existing solutions. Based on the guidelines provided by Kitchenham (80), we adopted the random selection technique to determine the reviewers of particular existing solutions. Consequently, each author decided on the document—project, patent, or technological system—to be reviewed from the list of the documents provided by the SHELDON Working Group 4.4 on technology adoption. The last author coordinated the review process. The objective of the review was 2-fold. The first goal was to understand the gap between the need, solutions, and technology adoption. The second goal was to understand the adoption challenges and the features of the solutions reported in various documents. Based on the resulting reviews, we analyzed from the technology adoption perspective the technical solutions provided by different projects.
We summarize the reviews provided by the authors by identifying the strengths and weaknesses of each existing solution that was analyzed. For that purpose, three analysis questions were asked for each solution as guides for understanding the gap between the need, solution, and technology adoption. These questions also served as the roadmap for understanding the adoption challenges faced by these solutions that have been reported in various documents. The analysis questions were as follows:
1. AQ1: Has the technology been tried out?
2. AQ2: Has the technology been tried out in a case study involving real end users?
3. AQ3: How well did the end users adopt the solution?
Additionally, we used ten (10) criteria based on the above analysis questions to elaborate our analysis. Table 1 describes the criteria that were applied to the analysis.
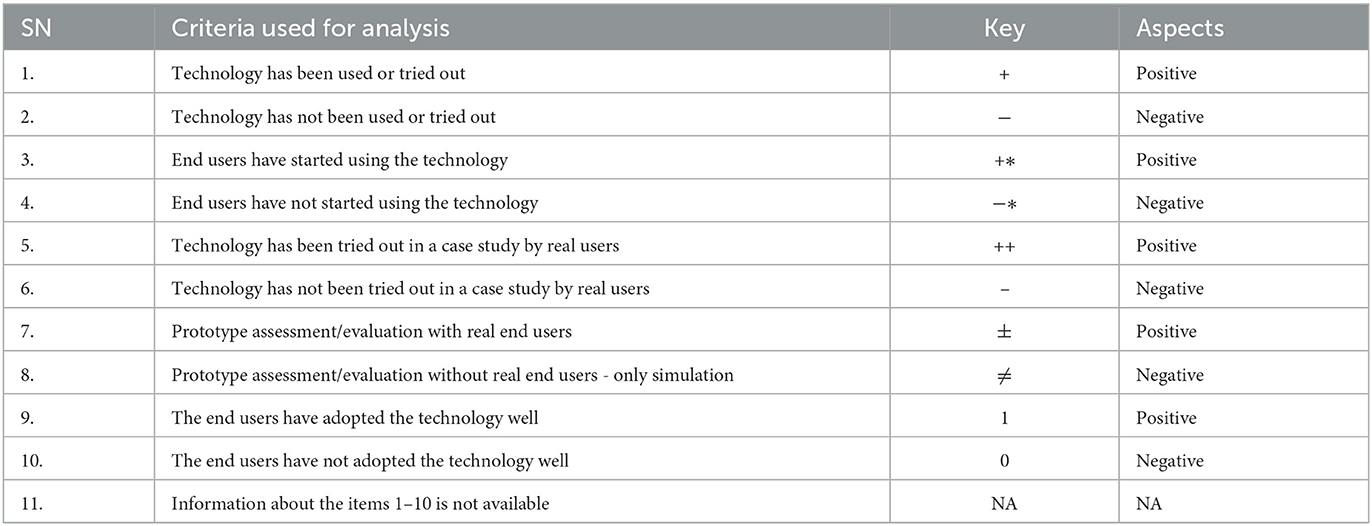
Table 1. Criteria for analyzing technology adoption.
We employed a quantitative assessment method to establish the suitability of a particular technology for ageing well. Regarding that, we formulated the null hypothesis H0 and alternative hypothesis H1, which were later subjected to a statistical test to verify their validity. In particular, we used the T-test and correlation analysis. We tested H0 with ten (10) randomly selected people within the age range between 60 and 75 by asking them a number of questions based on the TAM and DOI theoretical frameworks.
The structure of the questions that were used to source data from the 10 randomly selected persons is shown in Table 2. The 10 randomly chosen persons are from Tartu, Estonia. Following their verbal consent, they were interviewed informally. As Table 2 reflects, the given technology adoption issues were selected because they have been regarded as the most prevalent ones in the literature (73–76). The questions were designed to capture the individual's opinions on the possible use of a particular technology for improving the QoL of older adults. This is important for determining the levels of technology acceptance of end users for using these technologies.
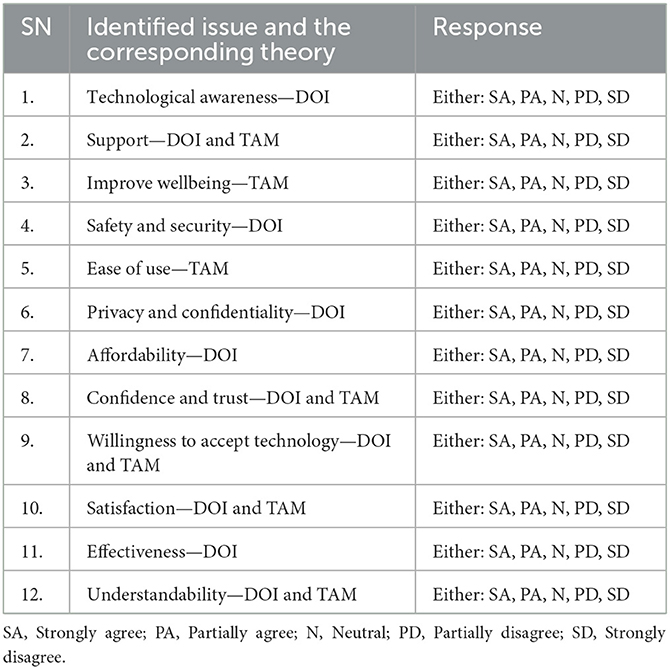
Table 2. The identified technology adoption issues.
As Table 2 shows, technological awareness is a factor aligned with DOI. It is one of the innovation model's stages of technology adoption. For this study, technological awareness refers to the knowledge of older adults about the existing technology.
Additionally, support focuses on improving wellbeing, safety, security, ease of use, privacy and confidentiality, affordability, confidence, trust, willingness to accept technology, satisfaction, effectiveness, and understandability. All these are a mixture of TAM and DOI.
This section presents the results based on the theoretical framework explained in Section 3 and methodology presented in Section 4.
According to the objectives of our analysis, six of the technological issues identified in Table 2 were analyzed to see if a relationship exists between technology adoption and technological issues and if one technological issue depends on another.
Based on the criteria described in Table 1, we critically analyzed the existing solutions. Table 3 presents details of the analysis showing the positive and negative aspects of the existing solutions.

Table 3. Analysis of the existing solutions.
From our initial discussion with selected respondents, we found out that they have a significant ability to use technology, especially operating their mobile devices and other digital devices they currently use, to adopt healthier lifestyles. The responses that we received are presented in Table 4.
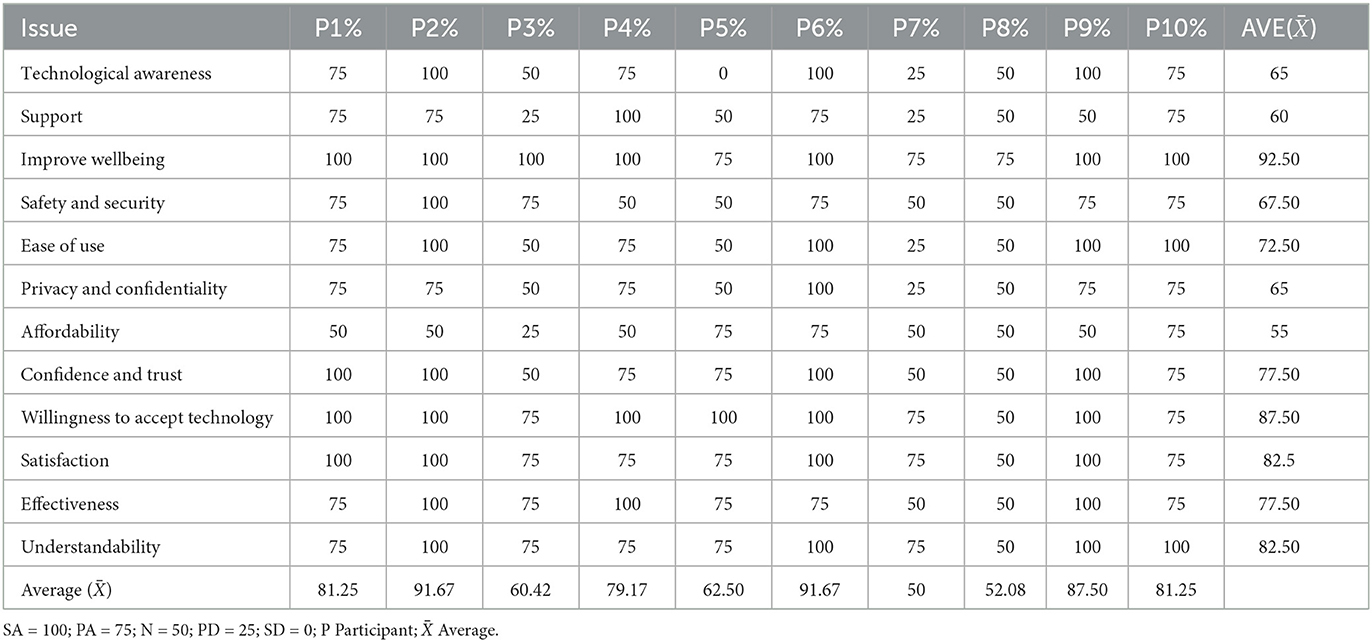
Table 4. Responses from randomly selected people.
As Table 4 reflects, the response by each participant was captured for each issue that we identified as the major driver that positively affects technology adoption by older adults, based on the TAM and DOI theoretical frameworks.
We categorized the responses as “Yes,” “No,” and “Neutral.” “Yes” means that the respondent either strongly agreed or partially agreed that a given issue should be among the technology adoption issues to be considered. If the participant strongly agreed that a given issue should be included, 100% was assigned. If the participant partially agreed, 75% was assigned. If the participant's response was neutral and they neither agreed nor disagreed, 50% was assigned. “No” means that the respondent either partially disagreed or strongly disagreed on the matter. If the participant partially disagreed, 25% was assigned and if the participant strongly disagreed, 0% was assigned. The percentages reflecting the responses by the participants to the technology adoption issues are shown in Table 4.
Additionally, we identified from the responses by the participants shown in Table 4 the degrees of their agreement about the importance of different technology adoption issues. The degrees of agreement are shown in Figure 2. According to the results, the technology adoption issue improve wellbeing has the highest relevance.
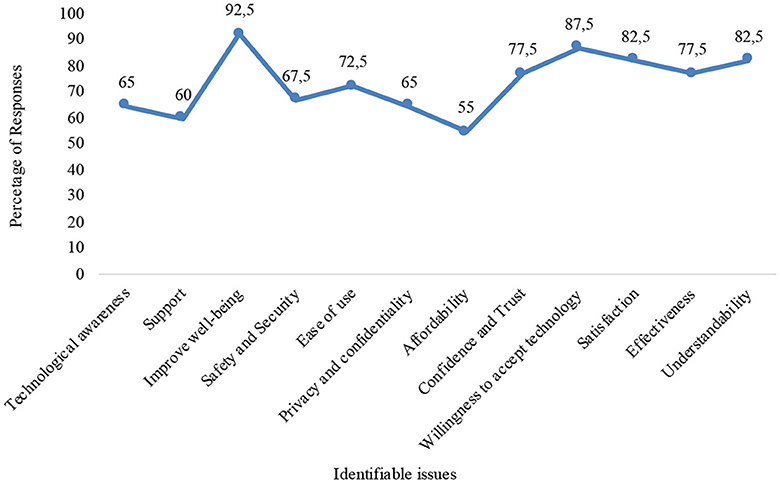
Figure 2. Technology adoption issues.
We first conducted a statistical test to check the validity of the following null hypotheses (H0) and alternative hypotheses (H1). Table 4 shows that the data is normal and meets the assumption for basic t-test analysis. The hypotheses were as follows:
• H0: Adopting technologies by older adults cannot improve their wellbeing.
• H1: Adopting technologies by older adults can improve their wellbeing.
The input data: improve_wellbeing, t = 24.222, df = 9, p-value = 1.667e-09, 95% confidence interval: 83.86124–101.13876, sample estimates: mean of x = 92.5.
The average percentage of each response was calculated and the H0 test was applied to it. Adopting a sample t-test technique at ± = 0.05, the t- value of 24.222 was obtained. Using the standard t-table for 9 degrees of freedom, we reject the null hypothesis if the calculated value of t is greater than the critical value of t, which is 2.262. Since the obtained t-value of 24.222 is greater than the critical value of t, we reject the null hypothesis and accept the alternative hypothesis, which states that adopting technologies by older adults can improve their wellbeing.
• H0: Technological awareness is not statistically significant for technology adoption by older adults.
• H1: Technological awareness is statistically significant for technology adoption by older adults.
The data input: technological_awareness, t = 6.0908, df = 9, p-value = 0.000181; 95% confidence interval: 40.85854–89.14146; Sample estimates: mean of x = 65.
The statistical test presented above shows that at the confidence interval of 95%, degree of freedom of 9, and alpha value of 0.05, the t-value is 6.0908, which is greater than the critical value of t, which is 2.262. Therefore, we reject the null hypothesis and accept the alternative hypothesis, which states that technological awareness is statistically significant for technology adoption by older adults.
• H0: Willingness to accept technologies is not statistically significant for technology adoption by older adults.
• H1: Willingness to accept technologies is statistically significant for technology adoption by older adults.
The input data: willingness_to_accept_technology t = 15.652, df = 9, p-value = 7.79e-08; 95% confidence interval: 74.85416–100.14584; sample estimates: mean of x = 87.5.
The statistical test presented above shows that at the confidence interval of 95%, degree of freedom of 9, and alpha value of 0.05, the t-value is 15.652, which is greater than the critical value of t, which is 2.262. Therefore, we reject the null hypothesis and accept the alternative hypothesis, which states that willingness to accept technologies is statistically significant for technology adoption by older adults.
• H0: Understandability is not statistically significant for technology adoption by older adults.
• H1: Understandability is statistically significant for technology adoption by older adults.
The input data: understandability; t = 15.461, df = 9, p-value = 8.67e-08; 95% confidence interval: 70.42927–94.57073; sample estimates: mean of x = 82.5.
Accordingly, at the confidence interval of 95%, alpha value of 0.05, and 9 degrees of freedom, the t-value is 15.652, which is greater than the critical value of t, which is 2.262. Therefore, we reject the null hypothesis and accept the alternative hypothesis, which states that understandability is statistically significant for technology adoption by older adults.
• H0: Ease of use is not statistically significant for technology adoption by older adults.
• H1: Ease of use is statistically significant for technology adoption by older adults.
The input data: ease_of_use; t = 8.3331, df = 9, p-value = 1.596e-05; 95% confidence interval: 52.81865–92.18135; sample estimates: mean of x = 72.5.
Accordingly, at the confidence interval of 95%, alpha value of 0.05, and 9 degrees of freedom, the t-value is 8.3331, which is greater than the critical value of t, which is 2.262. Therefore, we reject the null hypothesis and accept the alternative hypothesis stating that ease of use is statistically significant for technology adoption by older adults.
• H0: Support is not statistically significant for technology adoption by older adults.
• H1: Support is statistically significant for technology adoption by older adults.
The input data: support; t = 7.8558, df = 9, p-value = 2.559e-05; 95% confidence interval: 42.72249–77.27751; sample estimates: mean of x = 60.
Accordingly, at the confidence interval of 95%, alpha value of 0.05, and 9 degrees of freedom, the t-value is 7.8558, which is greater than the critical value of t, which is 2.262. Therefore, we reject the null hypothesis and accept the alternative hypothesis stating that support is statistically significant for technology adoption by older adults.
The main objective of this study is to understand the gap between the needs, provided solutions, and their adoption. We also identified several technology adoption issues and analysed their relevance. In this section, we analyze the correlation between several identified technology adoption issues by postulating a number of statistical hypotheses.
• H0: There is no statistical relationship between technological awareness and willingness to accept technologies.
• H1: There is a statistical relationship between technological awareness and willingness to accept technologies.
Figure 3 presents the analysis results of the correlation between technological awareness and willingness to accept technologies. The input data: technological_awareness and willingness_to_accept_technology; t = 1.0541, df = 8, p-value = 0.3226; 95% confidence interval: –0.3594439–0.8024112; sample estimates: correlation = 0.3492151.
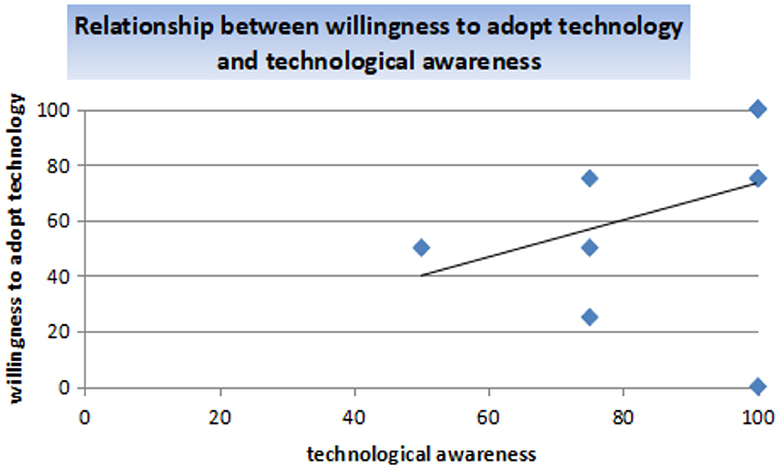
Figure 3. Correlation between technological awareness and willingness to accept technologies.
The correlation between technological awareness and willingness to adopt technologies is 0.3492151, indicating a weak positive relationship between the variables. The p-value of 0.3226 indicates that the correlation coefficient is significant. However, there is a weak relationship between technological awareness and willingness to accept technologies, which may result from sentiments about the device or the inability to operate the device. The alternative hypothesis is accepted.
• H0: There is no statistical relationship between support and improved wellbeing.
• H1: A statistical relationship exists between support and improved wellbeing.
Figure 4 presents the analysis results of the correlation between support and improved wellbeing. The data input: support and improve_wellbeing; t = 1.7393, df = 8, p-value = 0.1202; 95% confidence interval: –0.1578894–0.8673726; sample estimates: correlation = 0.5238095.

Figure 4. Correlation between support and improve wellbeing.
The correlation between support and improve wellbeing is 0.5238095, which shows a moderate positive relationship between the variables, and the p-value of 0.1202 indicates that the relationship between support and improve wellbeing is statistically significant. Therefore, we can conclude that if the support obtained from technological devices increases, the wellbeing of older adults will improve.
• H0: There is no relationship between understandability and ease of use.
• H1: A relationship exist between understandability and ease of use.
Figure 5 presents the analysis results of the correlation between understandability and ease of use. The data input: understandability and ease_of_use; t = 3.6793, df = 8, p-value = 0.006225; 95% confidence interval: 0.3258361–0.9488141; sample estimates: correlation = 0.7928129.
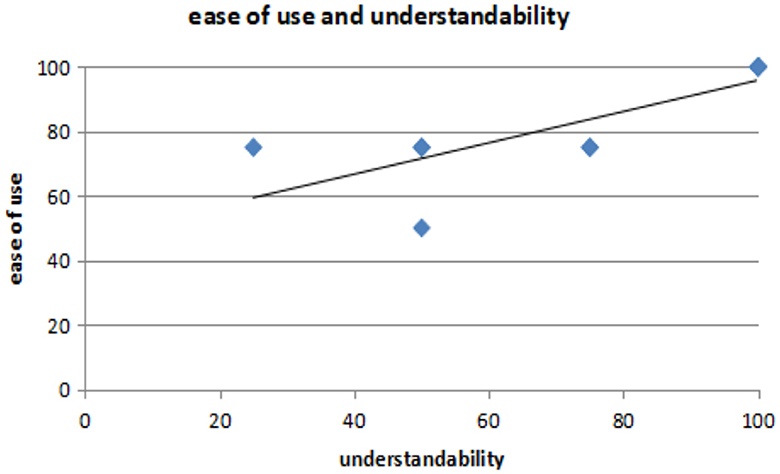
Figure 5. Correlation between understandability and ease of use.
The correlation between understandability and ease of use is 0.3492151, indicating a strong positive relationship between the variables. The p-value of 0.006225 also suggests that the correlation coefficient is significant. Therefore, a statistical relationship exists between understandability and ease of use.
This section discusses the findings from selected existing solutions based on our results. Also, we discussed the implications of the statistical evidences of our analysis.
This subsection further discusses some findings from solutions selected from Table 3.
Solution 1: The older adults found the system worked out in the HOLOBALANCE project encouraging and stimulating. The virtual coach was perceived as an alive, calm, intelligent, and friendly human. However, the usability of the entire virtual reality (VR) system showed a significant negative correlation with the participants' age. In the HOLOBALANCE project, mock-up interfaces were evaluated in semi-structured focus groups. Interviews were performed across three European countries. Also, a set of proof of concept validation studies were deployed, which aimed at assessing the accuracy of the different components of the sub-modules of the motion capture and assessment. The technology worked out in the project has potential for exploitation and commercialization as a service based on the IoT framework and on the accompanying business model of the continuous care and coaching platform. The validation results provide evidence that the proposed system can accurately support and assess physiotherapy exercises to care for balance disorders. This improves a patient's commitment to rehabilitation programs while enhancing the quality of the performed exercises. At the same time, we also indetified several negative aspects of the project in terms of technology adoption.
Solution 2: The My-AHA project is a typical ICT infrastructure with data analytics that is applied to the detection of frailty. The focus is not on technical innovation but on the concept of frailty and how to detect and take care of it. For this project, none of the criteria included by Table 1 were applicable.
Solution 3: The platform worked out in the HOPE project relies on a universal control box to interconnect a variety of devices. For this platform, the technology adoption involves buying the box and configuring the devices for it.
Solution 4: The Agnes project is an integration of ICT and social networking services that aids the detection of user states and activities and meeting the needs of older adults. The solution worked out in the Agnes project has the potential of prolonging for older adults the time spent at home, preserving health and promoting a healthy lifestyle, preventing social isolation, and providing support for (in)formal carers.
Solution 9: The FeelGood project provides a roadmap for an ecosystem for Finnish companies to excel in the international competition for services Personal Health Records (PHR). The PHRs form a part of the foundation of the healthcare system in Finland. The motivation of the project was to encourage the continuous utilization of e-services in the healthcare sector. The roadmap serves as a catalyst to transform the current illness-centered healthcare systems into a service landscape that allows patients and citizens to work in a partnership with healthcare providers to manage health issues. Several stakeholders participated in formulating a strategic roadmap for improving the PHR-based services in Finland. The roadmap focuses on providing an enabling environment for supporting and promoting healthcare concerns for the citizens through technology adoption. Although the formulated roadmap seems promising in terms of the approach and strategy employed, it is not certain whether the roadmap will be accepted by all the healthcare professionals and government.
Solution 10: The MPOWER project involves the cooperation platform, which is a technical integration platform of various services. It is a multisensor and multidevice environment that can provide support for the ageing population. However, technical solutions included by the platform are not directly applicable to senior users and their environments.
Solution 17: This solution systematically extracts and analyzes health and dietary information about older adults. It utilizes the information received from individual devices to form comprehensive and integrated information that can be used by different stakeholders, such as informal caregivers, to gain an insight into the QoL of older adults living at home.
Solution 18: This solution makes dietary recommendations and performs dietary monitoring of older adults. The recommendations are made based on the knowledge about the particular older adult rather than by following generic rules.
Solution 28: The MobileAge project produced the “Best Practice Guide for Co-creation of Open Public Services,” and is meant for co-design experts rather than end-users. The guide was evaluated in six co-creation case studies in Greece, Germany, the UK, and Spain but not in real-life cases. Unfortunately, the guide contains too many different methods without any clear directions as to in which order and situations one or another method should be applied. Furthermore, we could not find evidence of the OSCPSEP platform having been used in real-life case studies.
Solution 30: The SmartHabits project resulted in a system that was validated in a real environment, where a pilot application was set up in the city of Zagreb in cooperation with the foundation taking care of the older adults living alone. The validation confirmed that the proposed system has a potential to improve the quality of care by utilizing simple smart home sensors that can provide essential and continuous information about the occupant's status and environment. This was demonstrated in a scenario focused on prolonging the independence of the older adults living alone while offering peace of mind to their informal and formal caregivers. The system has great potential for adoption because of being non-invasive, self-adaptable to user behavior, zero-touch, and easy to manage. The most significant challenge of the adoption lies in the trust in technology.
Solution 32: The I-CARE-SMART project developed the following three methodological materials: ToolBox for Senior Engagement, ToolBox for Business Engagement, and Handbook on Co-Creation and Open Innovation Methods for Smart Care to Older Adults. These methods have not yet been validated in any real-life case studies.
Solution 33: The validation results of the pilots of the The SustAGE project have not been yet published. There is an extensive exploitation strategy, but its feasibility is hard to assess without knowing the validation results.
Solution 34: In the Intracom Medical ICT Solutions Portfolio project, a cloud-based integrated solution offering the PACS/RIS (Picture Archiving and Communication System / Radiology Information System) functionalities was provided as a service. Older adults are mentioned as potential customers, but there is no information about the actual usage or adoption.
Solution 35: In the “Joint deep learning and Internet of medical things based framework for elderly patients” project, the decision agent provides feedback to an inference engine of the target language analysis agent and the dialogue situation determination agent to allow for subjective interpretation of a given situation experienced by the older adult. However, devices that work and that do not require constant recharging remain challenges for this project.
Solution 36: In this research paper, an Internet platform for activating older adults was put forward. However, if an older person is unfamiliar with technologies, computers, and mobile devices, the platform is of no use. Therefore, a human assistant is required to get the platform started.
Solution 37: For the AIBO robot project, an off-the-shelf animal-like robot was provided to assist patients in hospitals where live animals are not allowed. In this case, a bond with the live animal is required. Additionally, the robot requires charging and has limited capabilities, but can still be beneficial.
The validity test is 2-fold (see Section 5.2). First, the t-test indicates that the various technology adoption issues identified are statistically significant. For example, according to the statistical analysis, the t-value is bigger than the critical value of t, which is 2.262, at the confidence interval of 95%, degree of freedom of 9, and alpha value of 0.05. This means that technological awareness is statistically significant for older persons' embrace of technology. Moreover, the hypotheses postulated for statistical analysis of other technology adoption issues proved substantial based on the t-test. This means that the identified technology adoption issues should be considered when implementing suitable technologies for the aging population.
Secondly, the correlation analysis further clarifies the relationship between the technology adoption issues identified based on our formulated hypotheses. In addition, the correlation analysis provides evidence of the strength and course of action of the technology adoption issues identified. For example, our correlation analysis revealed a strong statistical relationship between understandability and ease of use based on the value 0.349215 and a p-value of 0.006225. However, we noticed a weak relationship between technological awareness and willingness (readiness) to accept technologies, possibly due to negative feelings about the technology hardware or an inability to operate it. Most profoundly, the correlation analysis revealed that support and improved wellbeing have a moderately positive correlation of 0.5238095, statistically significant at a p-value of 0.1202. This means that supports from Governments or organizations in terms of funding and other motivation will improve the wellbeing of the aging population.
Based on our analysis in Section 5.1, many technical solutions are still at the development stages. Because there is no clear implementation plan and funding, only a small percentage of these solutions are currently being used or are about to be used in real life. Therefore, the governments, providers, developers, etc., should be aware that when introducing a technology to older adults, the key drivers that facilitate its adoption should be considered. Also, they should be mindful that older adults may not have the necessary knowledge, skills, motivation, or confidence.
In Section 5.2, we used the quantitative approach to establish the technology's suitability for the ageing population. Regarding that, the null hypotheses and alternative hypotheses were formulated. We subjected these hypotheses to a statistical test to verify their validity. For that, the T-test and correlation analysis are used. While the T-test was used to statistically reveal the significant level of technology adoption issues, we used correlation analysis to understand the relationship between the several technology adoption problems that we identified.
The fundamental ways to improve technology adoption by older adults are (i) ensuring the motivational support in using these technologies (81, 82), (ii) creating an extensive awareness of its potential benefits through education and training exercises toward improving the QoL of older adults (83), (iii) ensuring a sustainable plan and measures toward incorporating these technologies into the lifestyles of older adults, (iv) working out a strategy or framework that ensures support by key organizations and their respective management for design and implementation of suitable technologies, (v) building reliable and trustworthy solutions within older adults' competencies to use the technologies, (vi) making the required facilities, such as Internet services, available, and (vii) involving all stakeholders, especially the older adults themselves in the requirements elicitation process to develop an acceptable technical solution (84). Significantly, a positive attitude toward adopting technologies by older adults can also positively influence their wellbeing.
A strength of this study is that many existing technology solutions were analyzed. The analyzed solutions combine different projects, patents, and publications. This technology adoption review provides insight into the negative and positive features of the analyzed solutions for improving the QoL of older adults. Remarkably, the collaborative nature of the review process among the authors was instrumental to understand the current gaps between the needs, provided solutions, and their adoption from different perspectives.
Although the sample size of the respondents used for testing the hypotheses in Section 5.2 was small, still, there was diversity in the gender, age, ICT proficiency, and educational level of the older adults who answered the questions. In a small sample size, heterogeneity could be advantageous because it draws attention to critical features of the phenomena through a pattern across variance (85, 86). However, as part of our ongoing study, we intend to take into account bigger sample sizes across many nations, not just in Estonia for a more generalized and comparative results.
Another strength of our study is the combination of the TAM and DOI theoretical frameworks, which ensured that we caught pertinent viewpoints regarding analyzing the technology adoption concerns. A qualitative design was used, which made room for new viewpoints in identifying the strengths and weaknesses of each existing solution analyzed. Also, a quantitative method was used, enabling to test and formulate the hypotheses.
There are obviously some drawbacks in this study. First, the sample size used for testing the hypotheses is rather small, which has a detrimental impact on the generalizability of the results. Additionally, the older adults' prevailing circumstances and state of mind when answering the questions may have influenced their narratives and response. This leaves place for future work since a large scale study would bring further benefit to the research community.
This paper investigated the technological solutions from the technology adoption perspective based on the TAM and DOI technology adoption frameworks using the mixed method research approach. First, our analysis reveals both the positive and negative aspects of using technologies by older adults to improve their QoL. Second, we used a statistical metric to establish the appropriateness of our analysis further. Thirdly, we made an essential contribution based on our in-depth analysis by providing crucial recommendations and policy implications for consideration below in this section.
Consequently, we recommend, as a policy, the full support of governments and private organizations to design and implement holistic solutions. In our opinion, the involvement of governments in driving the campaigns for adopting technologies toward increasing the QoL of older adults is inevitable for successful technology adoption. Support by a government can be implemented in terms of funding and enacting laws that give relevance and attention to the ageing population of a society.
Additionally, we recommend that privacy concerns of older adults should be further considered based on, for example, the framework suggested in Khan and Gambo (87), when implementing any technical solution for improving QoL and wellbeing.
IG, KT, KM, RZ-G, AA, MM, MB-D, FM, and AL: conceptualization and writing—review and editing. IG and KT: methodology and data analysis. IG, KT, KM, RZ-G, AA, MM, and AL: formal analysis and investigation. KT: resources, supervision, and funding acquisition. IG: writing—original draft preparation. KT and KM: project administration. All authors have read and agreed to the published version of the manuscript.
The research work presented in this paper is based on work performed in the COST Action CA16226 Indoor living Space Improvement: Smart Habitat for the Elderly, supported by the COST (European Cooperation in Science and Technology) organization. The research work presented in this paper has received funding from the Pilots for Healthy and Active Ageing (Pharaon) project of the European Union's Horizon 2020 research and innovation programme under grant agreement no. 857188 and from the European Social Fund via the IT Academy programme. MM gratefully acknowledges the European Commission for funding the InnoRenew project (Grant Agreement #739574) under the Horizon2020 Widespread-Teaming program and the Republic of Slovenia (investment funding of the Republic of Slovenia and the European Regional Development Fund).
The authors would like to acknowledge and appreciate all the participating institutions in the Pharaon Project collaboration. Also, thanks to the Institute of Computer Science via the IT Academy programme at the University of Tartu, Estonia, for the support in executing the research. Finally, the authors acknowledge the responses from all respondents who participated in the survey.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer DV declared a shared affiliation with the authors KM, KT, and IG to the handling editor at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AAL, Ambient Assisted Living; AQ, Analysis Questions; DOI, Diffusion of Innovation; PEOU, Perceived Ease of Use; PU, Perceived Usefulness; TAM, Technology Acceptance Model; TRA, Theory of Reasoned Action; UTAUT, Unified Theory of Acceptance and Use of Technology; ELE, Enhanced Living Environments; ICT, Information and Communication Technologies; IoT, Internet of Things; TRL, Technology Readiness Level; QoL, Quality of Life; VR, Virtual Reality.
1. Lee C, Coughlin JF. Perspective: older adults' adoption of technology: an integrated approach to identifying determinants and barriers. J Prod Innov Manag. (2015) 32:747–59. doi: 10.1111/jpim.12176
2. Kim KO. The Emotional Responses of Older Adults to New Technology. Champaign, IL: University of Illinois at Urbana-Champaign (2012).
3. Peek S, Luijkx K, Vrijhoef H, Nieboer M, Aarts S, van der Voort C, et al. Understanding changes and stability in the long-term use of technologies by seniors who are aging in place: a dynamical framework. BMC Geriatr. (2019) 19:1–13. doi: 10.1186/s12877-019-1241-9
4. Peek ST, Wouters EJ, Van Hoof J, Luijkx KG, Boeije HR, Vrijhoef HJ. Factors influencing acceptance of technology for aging in place: a systematic review. Int J Med Inform. (2014) 83:235–48. doi: 10.1016/j.ijmedinf.2014.01.004
5. Miguel Cruz A, Lopez Portillo HP, Daum C, Rutledge E, King S, Liu L. Technology acceptance and usability of a mobile app to support the workflow of health care aides who provide services to older adults: pilot mixed methods study. JMIR Aging. (2022) 5:e37521. doi: 10.2196/37521
6. Yau Y, Hsiao CH. The technology acceptance model and older adults' exercise intentions—A systematic literature review. Geriatrics. (2022) 7:124. doi: 10.3390/geriatrics7060124
7. Varajão J, Carvalho JÁ, Silva T, Pereira J. Lack of awareness of IT adoption and use theories by IT/IS project managers: poor relevance, unfocused research or deficient education? Information. (2022) 13:48. doi: 10.3390/info13020048
8. Kavandi H, Jaana M. Factors that affect health information technology adoption by seniors: a systematic review. Health Soc Care Commun. (2020) 28:1827–42. doi: 10.1111/hsc.13011
9. Chen YRR, Schulz PJ. The effect of information communication technology interventions on reducing social isolation in the elderly: a systematic review. J Med Internet Res. (2016) 18:e4596. doi: 10.2196/jmir.4596
10. Klimova B, Poulova P. Older people and technology acceptance. In: Human Aspects of IT for the Aged Population. Acceptance, Communication and Participation: 4th International Conference, ITAP 2018, Held as Part of HCI International 2018, Las Vegas, NV, USA, July 15–20, 2018, Proceedings, Part I 4. Berlin: Springer (2018). p. 85–94.
11. Martín-García AV, Redolat R, Pinazo-Hernandis S. Factors influencing intention to technological use in older adults. The TAM model aplication. Res Aging. (2022) 44:573–88. doi: 10.1177/01640275211063797
12. Iqbal T, Anwar H, Filzah S, Gharib M, Mooses K, Taveter K. Emotions in requirements engineering: A systematic mapping study. In: 2023 IEEE/ACM 16th International Conference on Cooperative and Human Aspects of Software Engineering (CHASE). IEEE (2023). pp. 111–20.
13. Gambo I, Massenon R, Yange TS, Ikono R, Omodunbi T, Babatope K. Software design specification and analysis of insulin dose to adaptive carbohydrate algorithm for type 1 diabetic patients. In:R Patgiri, A Biswas, P Roy, , editors, Health Informatics: A Computational Perspective in Healthcare. Singapore: Springer Singapore (2021). p. 107–32.
14. Samaras GM, Horst RL. A systems engineering perspective on the human-centered design of health information systems. J Biomed Informat. (2005) 38:61–74. doi: 10.1016/j.jbi.2004.11.013
15. Dabbs ADV, Myers BA, Mc Curry KR, Dunbar-Jacob J, Hawkins RP, Begey A, et al. User-centered design and interactive health technologies for patients. Comput Informat Nurs. (2009) 27:175. doi: 10.1097/NCN.0b013e31819f7c7c
16. Dennis A, Wixom B, Tegarden D. Systems Analysis and Design: An Object-Oriented Approach With UML. Hoboken, NJ: John Wiley & Sons (2015).
17. Ollevier A, Aguiar G, Palomino M, Simpelaere IS. How can technology support ageing in place in healthy older adults? A systematic review. Publ Health Rev. (2020) 41:1–12. doi: 10.1186/s40985-020-00143-4
18. Khan HT. Population ageing in a globalized world: risks and dilemmas? J Eval Clin Pract. (2019) 25:754–60. doi: 10.1111/jep.13071
19. DESA U. World Population Ageing. New York, NY: United Nations, Department of Economic and Social Affairs/Population Division (2015).
20. Wan H, Daniel G, Paul K. An Aging World: 2015 US Census Bureau, International Population Reports. P95/16–1. Washington, DC: US Government Publishing Office (2016).
21. Barakovic Husic J, Melero FJ, Barakovic S, Lameski P, Zdravevski E, Maresova P, et al. Aging at work: a review of recent trends and future directions. Int J Environ Res Publ Health. (2020) 17:7659. doi: 10.3390/ijerph17207659
22. Kim Ki, Gollamudi SS, Steinhubl S. Digital technology to enable aging in place. Exp Gerontol. (2017) 88:25–31. doi: 10.1016/j.exger.2016.11.013
23. Tun SYY, Madanian S, Mirza F. Internet of things (IoT) applications for elderly care: a reflective review. Aging Clin Exp Res. (2021) 33:855–67. doi: 10.1007/s40520-020-01545-9
24. Romero M, Vivas-Consuelo D, Alvis-Guzman N. Is Health Related Quality of Life (HRQoL) a valid indicator for health systems evaluation? SpringerPlus. (2013) 2:1–7. doi: 10.1186/2193-1801-2-664
25. Spirduso W, Francis K, MacRae P. Physical Dimensions of Ageing. Champaign, IL: Human Kinetics Publishers (2005).
26. Yusif S, Soar J, Hafeez-Baig A. Older people, assistive technologies, and the barriers to adoption: a systematic review. Int J Med Informat. (2016) 94:112–6. doi: 10.1016/j.ijmedinf.2016.07.004
27. Tinker A, Lansley P. Introducing assistive technology into the existing homes of older people: feasibility, acceptability, costs and outcomes. J Telemed Telecare. (2005) 11(1Suppl.):1–3. doi: 10.1258/1357633054461787
28. Pal D, Triyason T, Funikul S. Smart homes and quality of life for the elderly: a systematic review. In: 2017 IEEE International Symposium on Multimedia (ISM). Taichung: IEEE (2017). p. 413–9.
29. Sokullu R, Akkaş MA, Demir E. IoT supported smart home for the elderly. Internet Things. (2020) 11:100239. doi: 10.1016/j.iot.2020.100239
30. Khosravi P, Ghapanchi AH. Investigating the effectiveness of technologies applied to assist seniors: a systematic literature review. Int J Med Inform. (2016) 85:17–26. doi: 10.1016/j.ijmedinf.2015.05.014
31. Liu P, Li G, Jiang S, Liu Y, Leng M, Zhao J, et al. The effect of smart homes on older adults with chronic conditions: a systematic review and meta-analysis. Geriatr Nurs. (2019) 40:522–30. doi: 10.1016/j.gerinurse.2019.03.016
32. Ekeland AG, Bowes A, Flottorp S. Effectiveness of telemedicine: a systematic review of reviews. Int J Med Inform. (2010) 79:736–71. doi: 10.1016/j.ijmedinf.2010.08.006
33. Goleva RI, Ganchev I, Dobre C, Garcia NM, Valderrama C. Enhanced Living Environments: From Models to Technologies. Stevenage: Institution of Engineering and Technology (2017).
34. Dobre C, x Mavromoustakis C, Garcia N, Goleva RI, Mastorakis G. Ambient Assisted Living and Enhanced Living Environments: Principles, Technologies and Control. Oxford: Butterworth-Heinemann (2016).
35. Ganchev I, Garcia NM, Dobre C, Mavromoustakis CX, Goleva R. Enhanced Living Environments: Algorithms, Architectures, Platforms, and Systems. Vol. 11369. Berlin: Springer (2019).
36. Marques G, Pitarma R, M Garcia N, Pombo N. Internet of things architectures, technologies, applications, challenges, and future directions for enhanced living environments and healthcare systems: a review. Electronics. (2019) 8:1081. doi: 10.3390/electronics8101081
37. Grossi G, Lanzarotti R, Napoletano P, Noceti N, Odone F. Positive technology for elderly well-being: a review. Pat Recogn Lett. (2020) 137:61–70. doi: 10.1016/j.patrec.2019.03.016
38. Heart T, Kalderon E. Older adults: are they ready to adopt health-related ICT? Int J Med Inform. (2013) 82:e209–31. doi: 10.1016/j.ijmedinf.2011.03.002
39. Wang KH, Chen G, Chen HG. A model of technology adoption by older adults. Soc Behav Personal. (2017) 45:563–72. doi: 10.2224/sbp.5778
40. Lai HJ. Investigating older adults' decisions to use mobile devices for learning, based on the unified theory of acceptance and use of technology. Interact Learn Environ. (2020) 28:890–901. doi: 10.1080/10494820.2018.1546748
41. Agree EM. The potential for technology to enhance independence for those aging with a disability. Disabil Health J. (2014) 7:S33–9. doi: 10.1016/j.dhjo.2013.09.004
42. Reeder B, Meyer E, Lazar A, Chaudhuri S, Thompson HJ, Demiris G. Framing the evidence for health smart homes and home-based consumer health technologies as a public health intervention for independent aging: a systematic review. Int J Med Inform. (2013) 82:565–79. doi: 10.1016/j.ijmedinf.2013.03.007
43. Hietala H, Ikonen V, Korhonen I, Lähteenmäki J, Maksimainen A, Pakarinen V, et al. FeelGood: Ecosystem of PHR based products and services. No. VTT-R-07000-09 in VTT Research Report. Tampere: VTT Technical Research Centre of Finland (2009).
44. Peek STM, Luijkx KG, Rijnaard MD, Nieboer ME, Van Der Voort CS, Aarts S, et al. Older adults' reasons for using technology while aging in place. Gerontology. (2016) 62:226–37. doi: 10.1159/000430949
45. Schwartz AP. The economics of a strategy for advanced information technology. Inform Strategy. (1992) 1992:11–7.
46. England I, Stewart D, Walker S. Information technology adoption in health care: when organisations and technology collide. Austr Health Rev. (2000) 23:176–85. doi: 10.1071/AH000176
47. Snoswell CL, Taylor ML, Comans TA, Smith AC, Gray LC, Caffery LJ. Determining if telehealth can reduce health system costs: scoping review. J Med Internet Res. (2020) 22:e17298. doi: 10.2196/17298
48. Snoswell CL, North JB, Caffery LJ. Economic advantages of telehealth and virtual health practitioners: return on investment analysis. JMIR Perioperat Med. (2020) 3:e15688. doi: 10.2196/15688
49. Yein N, Pal S. Analysis of the user acceptance of exergaming (fall-preventive measure)–Tailored for Indian elderly using unified theory of acceptance and use of technology (UTAUT2) model. Entertain Comput. (2021) 38:100419. doi: 10.1016/j.entcom.2021.100419
50. Papa A, Mital M, Pisano P, Del Giudice M. E-health and wellbeing monitoring using smart healthcare devices: an empirical investigation. Technol Forecast Soc Change. (2020) 153:119226. doi: 10.1016/j.techfore.2018.02.018
51. Li JPO, Liu H, Ting DS, Jeon S, Chan RP, Kim JE, et al. Digital technology, tele-medicine and artificial intelligence in ophthalmology: a global perspective. Progr Retinal Eye Res. (2021) 82:100900. doi: 10.1016/j.preteyeres.2020.100900
52. Park ES, Park MS. Factors of the technology acceptance model for construction IT. Appl Sci. (2020) 10:8299. doi: 10.3390/app10228299
53. Renaud K, Van Biljon J. Predicting technology acceptance and adoption by the elderly: a qualitative study. In: Proceedings of the 2008 Annual Research Conference of the South African Institute of Computer Scientists and Information Technologists on IT Research in Developing Countries: Riding the Wave of Technology. New York, NY: Association for Computing Machinery (2008). p. 210–9.
54. Davis FD. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. Management Information Systems Research Center, University of Minnesota, Twin Cities of Minneapolis and Saint Paul, Minnesota (1989). p. 319–40.
55. Rogers EM. Lessons for guidelines from the diffusion of innovations. Joint Commission J Quali Improv. (1995) 21:324–8.
56. McCoy S, Galletta DF, King WR. Applying TAM across cultures: the need for caution. Eur J Inform Syst. (2007) 16:81–90. doi: 10.1057/palgrave.ejis.3000659
57. Silva P. Davis' technology acceptance model (TAM) (1989). Inform Seek Behav Technol Adopt. (2015) 13:205–19. doi: 10.4018/978-1-4666-8156-9.ch013
58. Taherdoost H. A review of technology acceptance and adoption models and theories. Proc Manufact. (2018) 22:960–7. doi: 10.1016/j.promfg.2018.03.137
59. Davis FD, Bagozzi RP, Warshaw PR. User acceptance of computer technology: a comparison of two theoretical models. Manag Sci. (1989) 35:982–1003. doi: 10.1287/mnsc.35.8.982
60. Koul S, Eydgahi A. A systematic review of technology adoption frameworks and their applications. J Technol Manag Innov. (2017) 12:106–13. doi: 10.4067/S0718-27242017000400011
61. Fishbein M, Ajzen I. Belief, attitude, intention, and behavior: an introduction to theory and research. Philos Rhetoric. (1977) 10:2.
62. Azjen I. Understanding Attitudes and Predicting Social Behavior. Englewood Cliffs, NJ: Prentice-Hall, The University of Michigan (1980).
63. Yan M, Filieri R, Gorton M. Continuance intention of online technologies: a systematic literature review. Int J Inform Manag. (2021) 58:102315. doi: 10.1016/j.ijinfomgt.2021.102315
64. Venkatesh V, Davis FD. A theoretical extension of the technology acceptance model: four longitudinal field studies. Manage Sci. (2000) 46:186–204. doi: 10.1287/mnsc.46.2.186.11926
65. Holden RJ, Karsh BT. The technology acceptance model: its past and its future in health care. J Biomed Inform. (2010) 43:159–72. doi: 10.1016/j.jbi.2009.07.002
66. Venkatesh V, Morris MG, Davis GB, Davis FD. User Acceptance of Information Technology: Toward a Unified View. Management Information Systems Research Center, University of Minnesota, Twin Cities of Minneapolis and Saint Paul, Minnesota (2003). p. 425–78.
67. Yap YY, Tan SH, Choon SW. Elderly's Intention to Use Technologies: A Systematic Literature Review. Netherlands: Heliyon (2022). p. e08765.
68. Min S, So KKF, Jeong M. Consumer adoption of the Uber mobile application: insights from diffusion of innovation theory and technology acceptance model. In:Kaye Chon KS, Lee J-S, , editors. Future of Tourism Marketing. London: Routledge (2021). p. 2–15.
69. Rogers EM, Singhal A, Quinlan MM. Diffusion of innovations. In:Stacks DW, Salwen MB, , editors. An Integrated Approach to Communication Theory and Research. London: Routledge (2014). p. 432–48.
70. Dearing JW, Cox JG. Diffusion of innovations theory, principles, and practice. Health Affairs. (2018) 37:183–90. doi: 10.1377/hlthaff.2017.1104
71. Zhang X, Yu P, Yan J, Spil TA, et al. Using diffusion of innovation theory to understand the factors impacting patient acceptance and use of consumer e-health innovations: a case study in a primary care clinic. BMC Health Serv Res. (2015) 15:1–15. doi: 10.1186/s12913-015-0726-2
72. Heo J, Chun S, Lee S, Lee KH, Kim J. Internet use and well-being in older adults. Cyberpsychol Behav Soc Netw. (2015) 18:268–72. doi: 10.1089/cyber.2014.0549
73. Mahoney DF. An evidence-based adoption of technology model for remote monitoring of elders' daily activities. Ageing Int. (2011) 36:66–81. doi: 10.1007/s12126-010-9073-0
74. Hastall MR, Dockweiler C, Mühlhaus J. Achieving end user acceptance: Building blocks for an evidence-based user-centered framework for health technology development and assessment. In: International Conference on Universal Access in Human-Computer Interaction. Berlin: Springer (2017). p. 13–25.
75. Cahill J, McLoughlin S, O'Connor M, Stolberg M, Wetherall S. Addressing issues of need, adaptability, user acceptability and ethics in the participatory design of new technology enabling wellness, independence and dignity for seniors living in residential homes. In: International Conference on Human Aspects of IT for the Aged Population. Springer (2017). p. 90–109.
76. Nysveen H, Pedersen PE, Skard S. Ecosystem adoption of practices over time (EAPT): toward an alternative view of contemporary technology adoption. J Bus Res. (2020) 116:542–51. doi: 10.1016/j.jbusres.2020.01.014
77. Bailey CR, Bailey CA. A Guide to Qualitative Field Research. Thousand Oaks, CA: Sage Publications (2017).
78. Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematic reviews. Ann Intern Med. (1997) 127:820–6. doi: 10.7326/0003-4819-127-9-199711010-00008
79. Dixon-Woods M, Agarwal S, Jones D, Young B, Sutton A. Synthesising qualitative and quantitative evidence: a review of possible methods. J Health Serv Res Pol. (2005) 10:45–53. doi: 10.1177/135581960501000110
80. Kitchenham B. Procedures for Performing Systematic Reviews. Keele: Keele University. (2004). p. 33.
81. Ahn M, Beamish JO, Goss RC. Understanding older adults' attitudes and adoption of residential technologies. Fam Consum Sci Res J. (2008) 36:243–60. doi: 10.1177/1077727X07311504
82. Demiris G, Rantz MJ, Aud MA, Marek KD, Tyrer HW, Skubic M, et al. Older adults' attitudes towards and perceptions of “smart home” technologies: a pilot study. Med Informat Internet Med. (2004) 29:87–94. doi: 10.1080/14639230410001684387
83. Gambo IP, Soriyan AH. ICT implementation in the Nigerian healthcare system. IT Prof . (2017) 19:12–5. doi: 10.1109/MITP.2017.21
84. Mooses K, Camacho M, Cavallo F, Burnard MD, Dantas C, D'Onofrio G, et al. Involving older adults during COVID-19 restrictions in developing an ecosystem supporting active aging: overview of alternative elicitation methods and common requirements from five European countries. Front Psychol. (2022) 13:818706. doi: 10.3389/fpsyg.2022.818706
85. Sandelowski M. Sample size in qualitative research. Res Nurs Health. (1995) 18:179–83. doi: 10.1002/nur.4770180211
86. Boddy CR. Sample size for qualitative research. Qualit Market Res. (2016) 2016:53. doi: 10.1108/QMR-06-2016-0053
87. Khan F, Gambo I. Incorporating privacy requirements in smart communities for older adults: a research vision. In:HG Fill, M van Sinderen, L Maciaszek, , editors, Proceedings of the 17th International Conference on Software Technologies. Lisbon: Science and Technology Publications, Lda (2022). p. 242–9.
Keywords: technology adoption, older adults, ageing well, healthy lifestyle, Internet of Things, Information and Communication Technologies, Quality of Life
Citation: Gambo I, Bueno-Delgado MV, Mooses K, Melero Muñoz FJ, Zviel-Girshin R, Andrushevich A, Mrissa M, Landowska A and Taveter K (2023) Technology adoption review for ageing well: analysis of technical solutions. Front. Public Health 11:1169192. doi: 10.3389/fpubh.2023.1169192
Received: 19 February 2023; Accepted: 07 August 2023;
Published: 20 September 2023.
Edited by:
Jasmina Barakovic Husic, University of Sarajevo, Bosnia and HerzegovinaReviewed by:
Paraskevi Papadopoulou, American College of Greece, GreeceCopyright © 2023 Gambo, Bueno-Delgado, Mooses, Melero Muñoz, Zviel-Girshin, Andrushevich, Mrissa, Landowska and Taveter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ishaya Gambo, aXNoYXlhLmdhbWJvQHV0LmVl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.