
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 07 September 2023
Sec. Public Health Education and Promotion
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1162993
This article is part of the Research TopicPatient-Centered Communication Skills for Health Professions Education and HealthcareView all 8 articles
 Xuejing Li1,2,3†
Xuejing Li1,2,3† Dan Yang1,2,3†
Dan Yang1,2,3† Meiqi Meng1,2,3
Meiqi Meng1,2,3 Junqiang Zhao4,5
Junqiang Zhao4,5 Yiyi Yin1,2,3Hefang Wang1,2,3Xiaoyan Zhang1,2,3Qian Liu1,2Mengdi Li1,2
Yiyi Yin1,2,3Hefang Wang1,2,3Xiaoyan Zhang1,2,3Qian Liu1,2Mengdi Li1,2 Jianping Liu6*
Jianping Liu6* Yufang Hao1,2,3*
Yufang Hao1,2,3*Background: Shared decision-making (SDM) facilitates the participation of healthcare professionals and patients in treatment decisions. We conducted a scoping review to assess SDM’s current status in mainland China, referencing the Ottawa Decision Support Framework (ODSF).
Methods: Our review encompassed extensive searches across six English and four Chinese databases, and various gray literature until April 30, 2021. Results were synthesized using thematic analysis.
Results: Out of the 60 included studies, we identified three key themes based on the ODSF framework: decisional needs, decision support, and decisional outcomes. However, there appears to be a lack of comprehensive understanding of concepts related to decisional needs in China. Only a few studies have delved into feasibility, preference, choice, and outcome factors in the SDM process. Another challenge emerges from an absence of uniform standards for developing patient decision aids (PDAs). Furthermore, regarding health outcome indicators, their predominant focus remains on physiological needs.
Conclusion: SDM is in its infancy in mainland China. It is important to explore the concept and expression of decisional needs in the context of Chinese culture. Subsequent studies should focus on constructing a scientifically rigorous and systematic approach for the development of PDAs, and considering the adaptation of SDM steps to the clinical context in China during SDM implementation. Concurrently, The focus on health outcomes in Chinese SDM studies, driven by the unique healthcare resource landscape, underscores the necessity of prioritizing basic needs within limited resources.
Systematic review registration: https://inplasy.com/?s=202130021.
Shared decision-making (SDM) has been increasingly advocated as an ideal approach to clinical practice (1). Patient engagement in the decision-making process has numerous benefits, including decreased decisional conflict, increased patient knowledge, and improved health outcomes such as patient satisfaction and quality of life (2, 3). The introduction of SDM in China can be traced back to 1998 (4). Since the advent of the 21st century, the long-established physician-led paternalistic medical decision-making model in China has gradually transformed into a patient-centered shared decision-making model involving both patients and physicians (5, 6). Preliminary research indicates that in recent years, SDM has been gradually gaining attention and experiencing a certain level of application in mainland China, covering areas such as diagnosis, treatment, screening, and care models (7–13). In contrast, across the international landscape, SDM has gained recognition as a prominent trend in Western societies, serving as the prevailing model for facilitating patient-centered healthcare decisions (14) and achieving patient-value based care (15). SDM studies conducted in Western countries have generated a wealth of valuable resources, including not only theoretical models (16) but also practical tools (17). Some models (1, 18) and tools (19–21) have been empirically tested and possess strong guidance and applicability. However, the significant differences in healthcare systems and cultures between Western countries and China raise questions about the feasibility of simply transferring Western SDM products into China (22). For instance, in mainland China, the uneven distribution of medical resources and disparities between patient expectations and reality poses challenges to patient participation in medical decision-making (23). These challenges further exacerbate distrust and dissatisfaction among some patients with the diagnosis and treatment process (24, 25). Limited medical knowledge, varying educational levels among patients, and regional economic disparities further complicate the implementation of SDM (26). To accurately identify the current hotspots and gaps in SDM research, a comprehensive summary of SDM-related research in China at this stage is necessary. A systematic review conducted by Rongchong Huang et al. evaluated the relevant research on SDM in China, including trials and surveys (27). While the findings of this study were disappointing, they provided a groundbreaking overview of the current status and barriers of SDM research conducted in China at that time. To date, there has been no published review specifically focusing on SDM-related research in mainland China.
To understand the current state of research in the field of SDM in mainland China, we reviewed whether research in mainland China was included in systematic reviews covering SDM concepts. When studying a complex and new field, choosing an appropriate theoretical framework is essential. The framework can facilitate conceptualizing the topics covered by the field in question and comprehensively guide the research direction (28). The Ottawa Decision Support Framework (ODSF) conceptualizes the support patients, families, and their practitioners need when deliberating about options (29–31). It guides practitioners and researchers in assessing participants’ decisional needs, providing decision support interventions, and evaluating the effects of decision support on decisional outcomes. In the context of decision-making, the focus of a needs assessment is on identifying: what a patient population needs to make better decisions; and what a population of health practitioners needs to improve the support they provide to patients during decision-making. In 2020, a systematic review (31) of decision needs included 45 studies covering research from seven countries, but we have yet to find evidence from China. A Cochrane systematic review in 2018 determined the effectiveness of interventions for increasing the use of SDM by healthcare professionals (2). It included 87 studies. The four most represented countries were the United States, Germany, Canada, and the Netherlands. None of the studies were from mainland China. Studies related to SDM are typically designed to investigate how SDM might improve outcomes that are relevant to patients. Many measurement approaches to SDM have been developed (32–34). The integration and summary of outcome indicators have been suggested to standardize subsequent studies. Shay and Lafata included 41 relevant studies in their integration of outcome information from studies related to SDM and developed a framework of SDM outcome indicators (35). Gärtner FR used this framework in his 2018 review and included 51 studies (36). However, no Chinese studies were identified in either of these systematic reviews.
It is evident that there is still a lack of studies that systematically present the current status of SDM research in China, and no eligible Chinese studies have been included in any of the systematic reviews published in recent years. Comparing the current status of SDM implementation in China with the international status may help us find implementation strategies and address these gaps. Given that the three core structures of ODSF cover a significant portion of the current focus of SDM-related research and it is one of the most widely applied SDM theoretical frameworks internationally (30), this study provides a comprehensive and systematic mapping of SDM research in mainland China from the dimensions of decisional needs, decision support, and decisional outcomes, guided by this framework. Additionally, due to the broad nature of our research question, the SDM field being in its early stages in mainland China with limited research available, and our anticipated research design and methods (37), we conducted a scoping review instead of a systematic review.
Scoping studies are an increasingly popular approach to reviewing health research evidence. To guide authors undertaking scoping studies, Arksey and O’Malley (38) developed a five-stage methodological framework: (1) identifying the research question, (2) searching for relevant studies, (3) selecting studies, (4) charting the data, (5) collating, summarizing, and reporting the results. This framework provided an excellent methodological foundation. The study findings will be reported following the Preferred Reporting Items for Systematic reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) reporting guidelines (39). The protocol was registered prospectively in the Inplasy (202130021). The Supplementary material provides the PRISMA-ScR checklist (Supplementary file S1).
The purpose of this study is to describe the current research on SDM in mainland China. Based on the ODSF, the objective of this scoping review is to map accessible research literature to answer the research questions systematically: (1) What were the general characteristics of SDM studies in mainland China? (2) What decisional needs of patients were focused on in these studies? (3) What SDM decision support (SDM theories, process, tools) were described to address the healthcare decisional needs? and (4) What SDM outcomes were reported?
With the assistance of an experienced research librarian, we searched six English databases: PubMed, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), EMBASE, Cochrane Library, PsycINFO and Web of Science. We also searched four Chinese databases: China National Knowledge Infrastructure, WanFang Database, VIP Database, and China Biology Medicine. All databases were searched from 1968 (this year was chosen as the starting year due to the prevalence of SDM publications since that time (40)) to April 2021. The retrieval also included unpublished gray literature. Gray literature were searched using Baidu Scholar1 and Google scholar. These strategies will ensure that documents on SDM in mainland China are identified in search of the literature. The finalized search strategy is shown in Appendix 1.
This study will integrate all the studies on SDM in mainland China as thoroughly as possible, so we developed relatively broad initial criteria inclusion criteria based on clearly identifiable populations, concepts, and contexts (PCC) (41). Table 1 illustrates how the PCC acronym was applied. In addition to the PCC, we also limited the study design and language in the inclusion criteria.
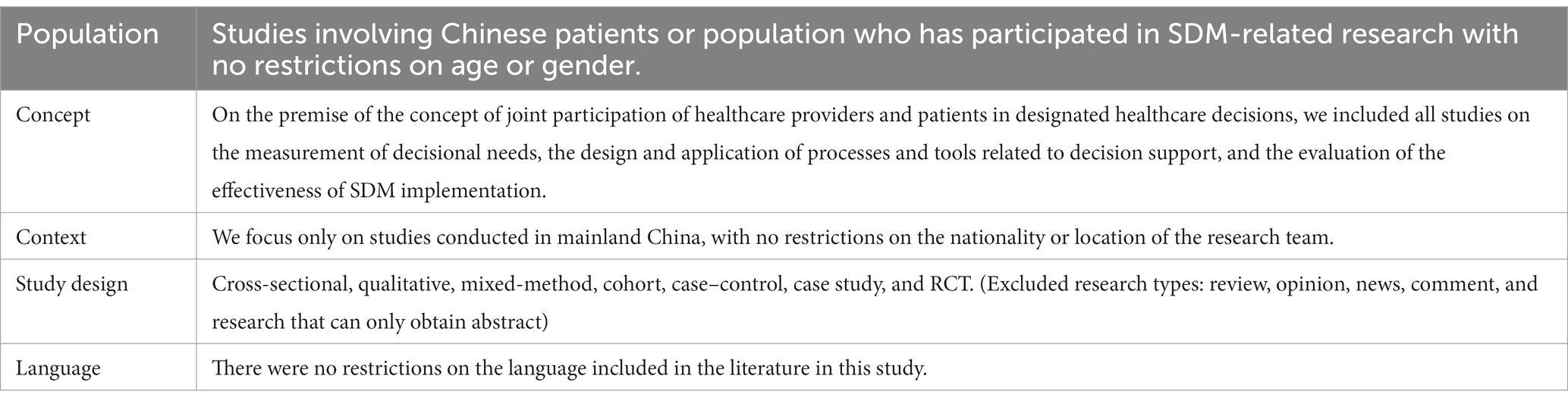
Table 1. Inclusion criteria.
Study selection was performed in several steps. First, after de-duplication, review authors (DY and XJL) double-screened all titles and abstracts in duplicate using NoteExpress 3.2.0 document management software. Then, reviewers (DY and XJL) double-screened the full text for all studies included. Disagreements were further discussed by the third reviewing author (YFH) to reach a consensus.
The literature screening gave us a general overview of the objectives of the studies. We found two main kinds of SDM studies conducted in China: descriptive studies focusing on decisional needs and influencing factors of SDM; and analytical studies focusing on the construction of SDM-related tools and the effects of SDM implementation. Because of the significant differences in the presentation of information between these two kinds of studies, we developed two content extraction forms using Excel. In the descriptive study, we extracted: study identifications, concepts, methods, theories, models utilization, and outcomes. For the analytical study, we mainly extracted: study identifications, concepts, methods, patient characteristics of the intervention group, patient characteristics of the control group, theories and models utilization, decision support tools, SDM process, outcomes, and influencing factors.
This stage involves collating, summarizing and reporting the results of the selected evidence, which was undertaken by the whole research team in an iterative process until consensus on the thematic results and implications of the scoping review were agreed. We used two main strategies to analyze the data in this study: (1) descriptive number statistics for general information about the included literature and (2) qualitative thematic analysis.
In the first step, we employed a framework analysis approach to map the extracted data into the three core concepts of the Ottawa Decision Support Framework (ODSF), namely Decisional needs, Decisional support, and Decisional Outcomes. Subsequently, a comprehensive analysis of the three core concepts was conducted. Step 2: Analyze the content of Decisional needs (31). The ODSF Decisional needs Coding Manual (31) was used as the primary coding tool to conduct a thematic analysis for the classification of decisional needs. Step 3: The content of Decision support was divided into two parts, the SDM process and decisional support tools. In the SDM process, we classified the implementation process of SDM based on the Interprofessional Shared Decision Making (IP-SDM) Model (42), and classified the doctor-patient conversation time in the SDM process using the three-talk model (43). In the decisional support tools section, we organized the extracted Patient Decision Aids (PDAs) construction process according to the National Health Service Standards framework for shared decision-making support tools (NHS Standards framework) (44). Step 4: Outcomes were classified into three categories: cognitive-affective, behavioral, and health outcomes, according to Shay and Lafata’s classification model (35) for outcomes in SDM-related studies.
The lead author (XL) wrote the scoping analysis, which was then checked independently by three collaborators (DY, MM, and JZ) who fed back their comments. Any disagreements were discussed and resolved.
Of the 6,966 and 2,108 records retrieved from the database and gray literature search, 60 papers were finally included after screening (see Appendix 2 for a list of included studies). The literature search and screening diagram are shown in Figure 1. The basic characteristics of those 60 papers are presented in Table 2. According to the research contents, the 60 papers included were divided into two main categories: one is descriptive research focusing on decision needs and influencing factors of patient participation in decision-making (29/60, 48.33%); the other is decision support focusing on the development and implementation effects of decision aids (31/60, 51.67%). For better analysis, the included studies were analyzed as a whole or in groups, according to the research questions for the review detailed above.

Figure 1. Scoping review flowchart.
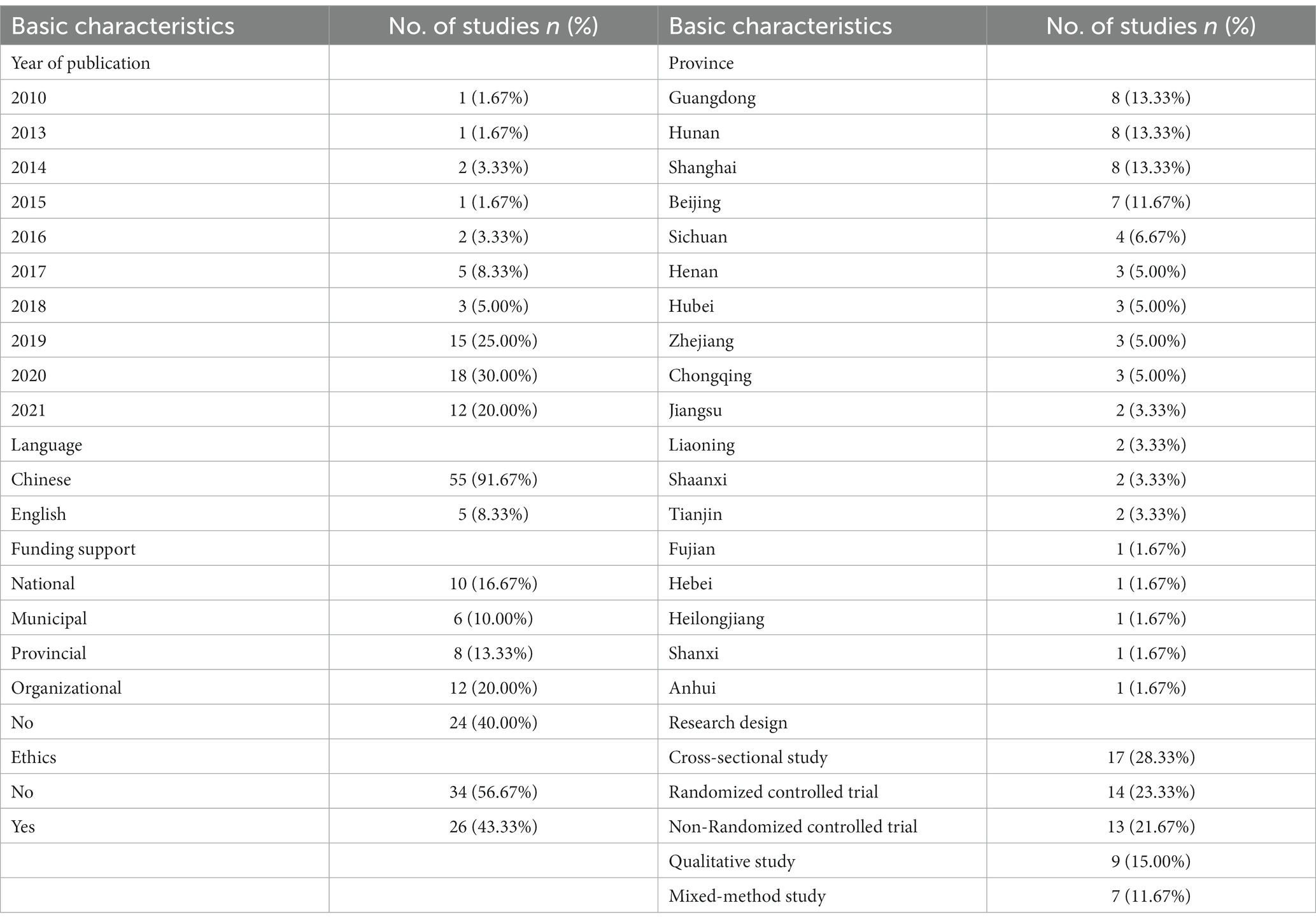
Table 2. Basic characteristics of included studies (n = 60).
Overall, the publication has shown an increasing trend in recent years, with the first publication dating back to 2010 and a greater proportion of research literature written in the previous 3 years (2019–2021). The studies were published predominately in Chinese journals (55/60, 91.67%). 36 (60%) of the included studies got funding support. Most of the included studies (56.67%) did not explicitly describe the ethical considerations. The commonly used research designs for SDM were cross-sectional study (17/60, 28.33%), randomized controlled trial (14/60, 23.33%), and non-Randomized controlled trial (13/60, 21.67%). The Types of patients included in those SDM research mainly focused on oncology (e.g., breast cancer; 18/60, 30.00%), cardiovascular diseases (e.g., atrial fibrillation; 7/60, 11.67%), chronic diseases (e.g., diabetes mellitus; 7/60, 11.67%), and mental diseases (e.g., schizophrenia; 7/60, 11.67%; see Table 3).
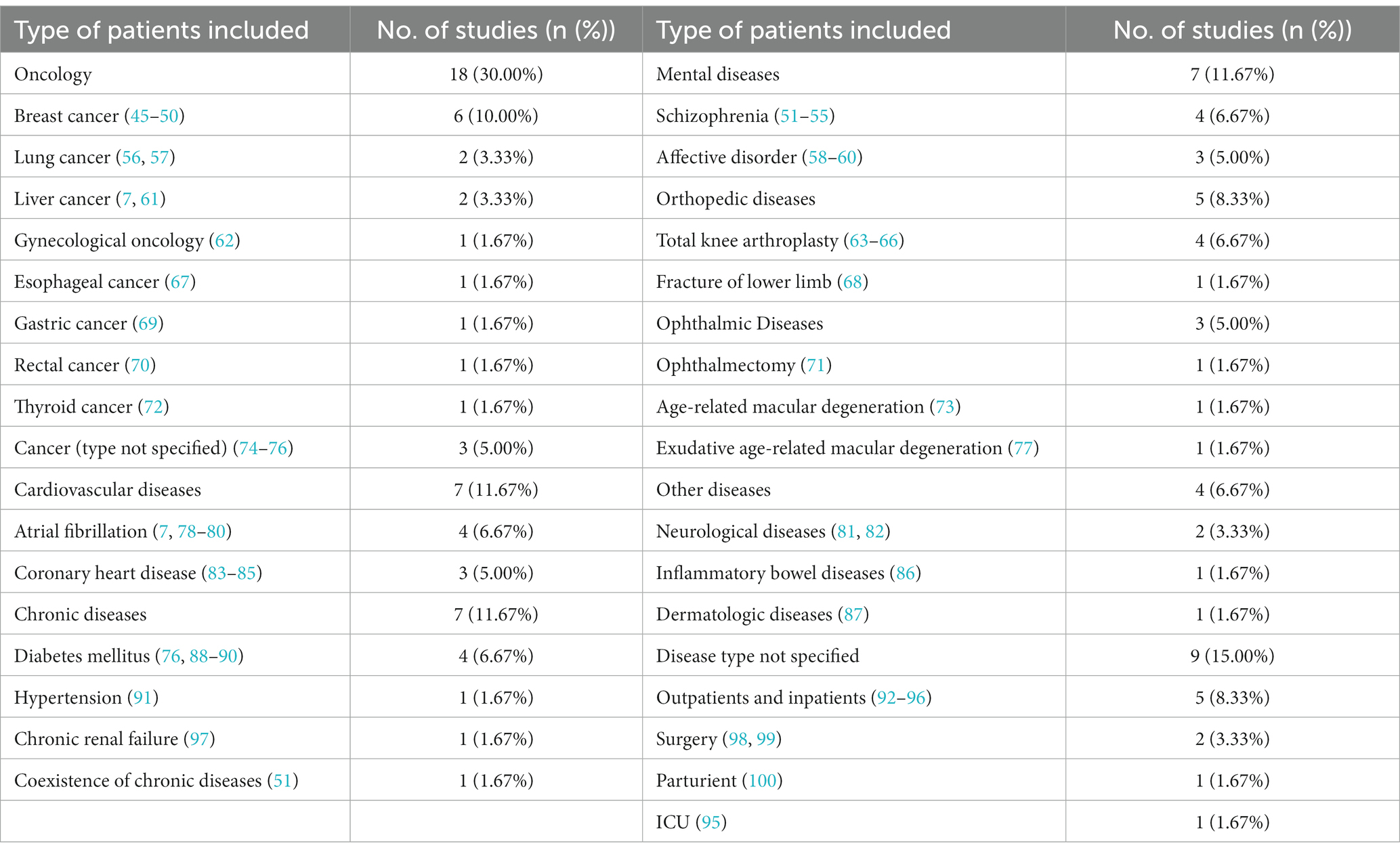
Table 3. Types of patients included (n = 60).
A total of 13 theories/models/frameworks to guide SDM studies were reported in 13 studies (21.67%) (7, 9, 45, 46, 61–63, 72, 74, 78, 79, 83, 92), among which ODSF was the most frequently used one (8/13, 61.54%) (7, 9, 46, 61–63, 72, 79) and was mainly used to guide the construction of decision aids, the implementation of decision making needs assessment and the design of the interview outline. The remaining 12 frameworks (45, 61, 72, 74, 83, 92, 93) all appeared only once in the included studies. The specific theories/models/frameworks and their role in the study are shown in Appendix 3.
The ODSF Decisional Needs Coding Manual defines all aspects of decision requirements in detail and provides rich coding examples. Decisional needs were the focus of 56 out of the 60 included studies (93.33%). Based on the ODSF Decisional Needs Coding Manual (31), seven main themes were identified: (1) Decisional conflict; (2) Inadequate knowledge; (3) Unrealistic expectations; (4) Unclear values; (5) Inadequate support or resources; (6) Complex decision characteristics; and (7) Personal and clinical needs. Of the 56 studies, all ODSF decisional needs were reported in 1 (2%) to 33 (58.93%) studies (see Table 4). In this study, the three most frequent manifestations of decisional needs were feeling uninformed about the health problem, condition or situation to make a decision (33/56, 58.93%) (46–53, 58, 59, 61–65, 68, 70, 72, 74–77, 79, 81, 82, 87, 88, 93, 94, 98–101); lacking instrumental help (24/56, 42.86%) (9, 49, 50, 61, 62, 64–69, 71, 77, 79, 81–85, 87–89, 91, 102); feeling lacking confidence in the ability to implement chosen option (22/56, 39.29%) (46, 48–50, 53, 54, 56, 58, 61, 63, 65, 72, 75, 77, 81, 82, 84, 86, 87, 97, 99, 100) (see Appendix 4).
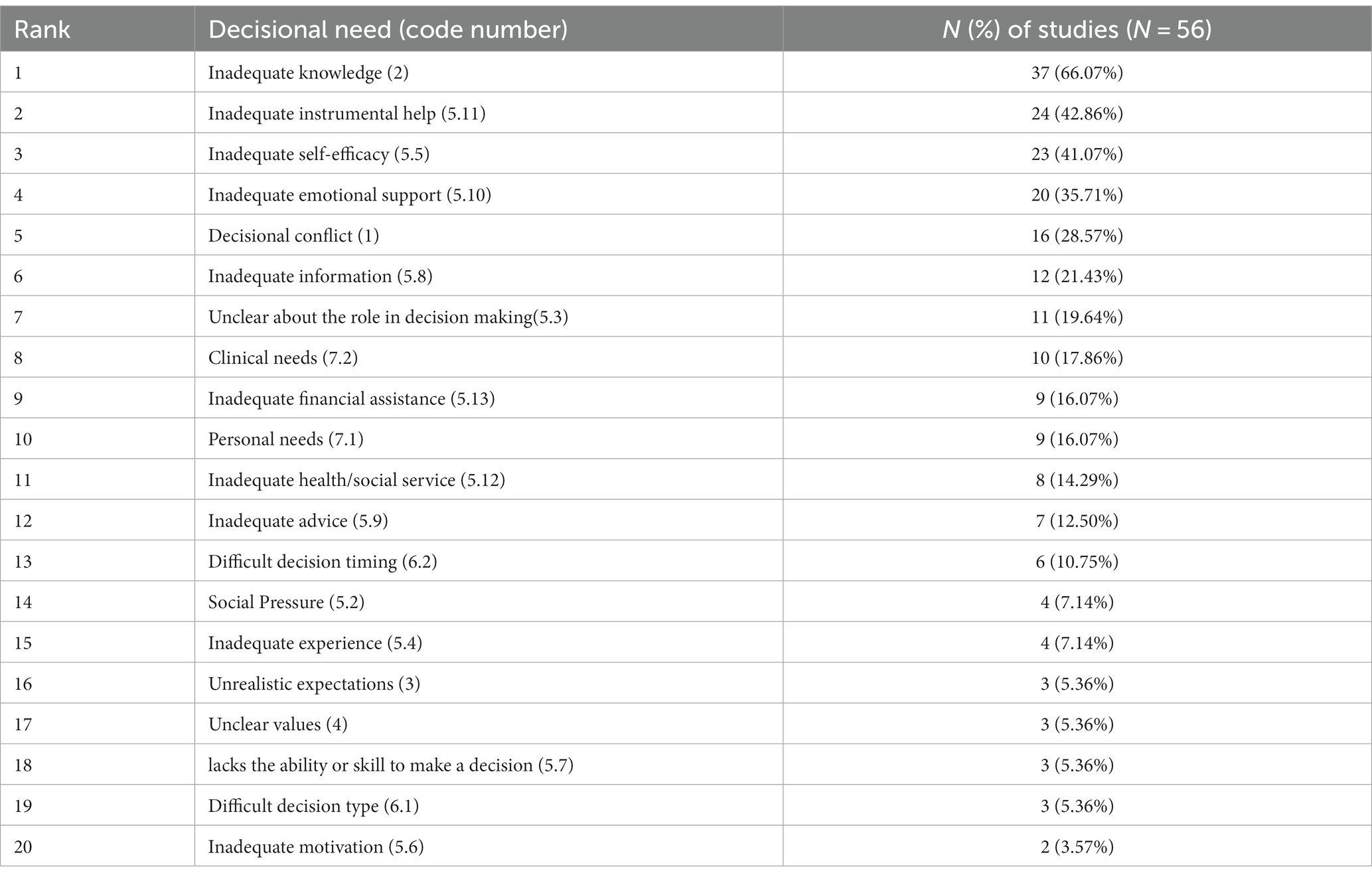
Table 4. Frequency (%) of studies reporting ODSF decisional needs.
A variety of experiences triggered a series of decisional conflicts faced by patients during the SDM process (16/56,28.57%). Uncertainty of action emerged when their choices were challenged by risk, loss, regret, and personal life values. Five studies (48, 57, 61, 84, 96) (5/56,8.93%) reported that, when involved in decision-making, patients often described that they faced decision difficulties because they were unsure of what is the best course of action. In addition, other common manifestations of patient decision-makers in decisional conflict are worrying about possible problems (7/56,12.50%) (45, 46, 48, 54, 73, 80, 93) or feeling upset in making decisions (7/56,12.50%) (45, 62–65, 80, 98).
Patient decision-makers in 37 studies (37/56, 66.07%) identified inadequate knowledge in their decision-making. In these studies, the most reported manifestation (49, 56, 70, 76, 77, 84, 86, 98, 99) of this need was feeling uninformed about the health problem, condition, or situation to attempt a decision (33/56, 58.93%), followed by lacking awareness of what decision needs to be made (9/56, 16.07%) and feeling uninformed enough about options (56, 73, 86) (3/56, 5.36%).
Few studies (64, 77, 90) (3/56, 5.36%) found that patients reported unrealistic expectations in the decision-making process. These participants reported that they did not know the odds of benefits versus harms and described that it is hard to believe that the outcome probabilities applied to them. Moreover, in three studies (45, 70, 90) (3/56, 5.36%), patient decision-makers reported feeling unclear values.
Most studies (51/56, 91.07%) have reported that patient decision-makers feel inadequately supported and resourced in the decision-making process. Forty-five of these studies reported a lack of social support for patient decision-makers when making or implementing decisions. The most common manifestation (9, 49, 50, 61, 62, 64–69, 71, 77, 79, 81–85, 87–89, 91, 102) (24/56, 42.86%) was lacking tools to help patient decision-makers in making and implementing decisions, although some studies mentioned that patient decision aids had been used in some patient decisions. Other manifestations are lacking access to information, advice from significant others involved in the decision, and emotional support from others. Twenty-three of these studies (45, 46, 48, 50, 53, 54, 56, 58, 61, 63, 65, 72, 75, 77, 82, 84, 86, 87, 97, 99) (41.07%) reported a lack of internal resources for patient decision-makers in making or implementing decisions. Many of them lacked self-efficacy, mainly in terms of lacking confidence in their ability to participate in decision-making and in implementing the chosen option.
Complex decision characteristics are composed of three main types of decisional needs: difficult decision types, difficult decision timing, and unreceptive decision stages. Of 56 studies, only three studies (76, 78, 96) (3.57%) mentioned difficult decision types. Only six studies (45, 48, 51, 54, 73, 77) of 56 studies (6/56 10.71%) reported difficult decision timing, including delays in decision times that exacerbated surgical patients’ uncertainty about their surgical options (48, 77) and tight decision times that made it difficult for healthcare workers to communicate in detail with each patient (51, 54).
Of 56 studies, 19 (19/56, 33.93%) describe at least one personal or clinical need of patient decision-makers. In terms of individual needs, one study [49]highlighted the need to consider demographic characteristics, and eight (45, 47, 54, 58, 61, 75, 77, 91) studies described tailored information, such as information on medication use and self-management that matched patient preferences. Furthermore, In terms of clinical needs, 10 studies (49, 63, 64, 66, 67, 70, 78, 82, 84, 97) reported the need to tailor decision support to patients’ psychological perceptions, health status, emotional state, and preferences when providing decision support.
IP-SDM model takes into account the involvement of multiple professionals in the SDM process, including patients, physicians, and other healthcare workers. In this study, it helps us to understand and classify the implementation process of SDM. The implementation process of shared decision-making is exemplified by 31 papers. We mapped the themes according to the IP-SDM model. According to the core constructs of the IP-SDM model, we divided the SDM process into nine steps, of which 22 studies (22/31,70.97%) (7, 50, 52, 53, 59, 61–68, 79, 81–85, 91, 97, 102) referred to “patient with a health condition.” We subdivided this theme into informing consent (3/31,9.68%) (59, 83, 102), assembling a team (10/31,32.26%) (50, 53, 59, 64–67, 81, 84, 91, 97), developing tools (6/31,19.35%) (50, 59, 62, 85, 91, 92), instruction for installation of tools (2/31,6.45%) (7, 62) conventional care (4/31,12.90%) (52, 53, 63, 68), creation of atmosphere (8/31,25.81%) (59, 61, 67, 79, 81–84). Please refer to Appendix 5 for references related to these steps. Figure 2 shows the corresponding results.
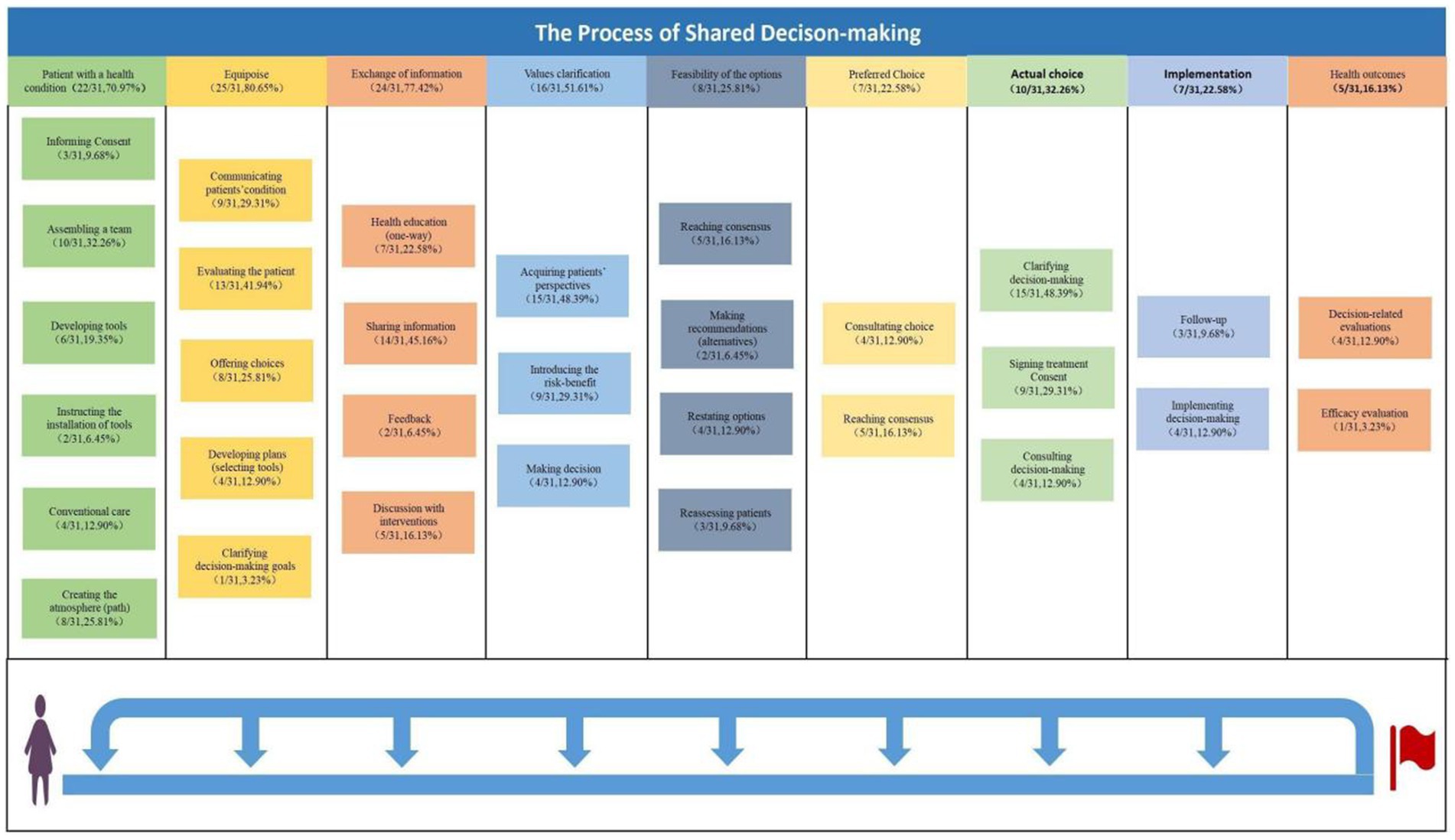
Figure 2. The process of SDM.
The role of the implementer was mentioned in all 31 studies on the shared decision-making process and 27 studies (27/31,87.10%) (9, 49, 50, 52, 53, 57, 59–69, 71, 79, 82–84, 87–91, 97, 102) mentioned the shared decision-making implementer’s role as physician. In 22 studies (22/31,70.97%) (9, 49, 52, 57, 59, 61–64, 66–69, 81, 83, 84, 87, 91, 97) the implementer was nurse, in nine studies (9/31,29.03%) (49, 62, 67, 69, 81–83, 91, 97) the implementer was nursing managers, four studies (4/31,12.90%) (9, 61, 79, 84) in which the implementer was the member of the research team, three studies (3/31,9.68%) (49, 84, 91) in which the implementer was mentioned as a medical manager, and two studies (2/31,6.45%) (50, 62) in which the implementer was a rehabilitator or technician. Information technology personnel (62), counselors (49), and volunteers (49) were mentioned as implementers in one study each (1/31,3.23%). In addition to the above population, patients and their families were also involved in the shared decision-making. A total of 1876 patients and their families were included in 31 studies, of which 29 (29/31,93.55%) mentioned the involvement of patients and 20 (20/31,64.52%) mentioned the involvement of patients’ families.
The doctor-patient communication process is an essential component of SDM. The three-talk model divides doctor-patient communication into three steps: information exchange, emotion handling and decision making. Twenty-three studies referred to (23/31) conversation timing categorized according to the three core constructs of the three-talk model, of which 18 studies (18/31) (50, 52, 53, 59–62, 65–68, 71, 79, 81, 82, 84, 87–89, 91, 102) are related to team talk. Team talk-related content was divided into establishing relationships (13/31,41.94%) (50, 57, 59, 63, 65, 66, 79, 81, 84, 87, 89, 91, 102); communicating patients’ condition (8/31,25.81%) (50, 52, 53, 59–62, 65–68, 79, 81, 84, 87, 89, 91, 102); offering options (5/31,16.13%) (61, 68, 81, 84, 102); evaluating patients (3/31,9.68%) (57, 59, 63). Nineteen studies mentioned option talk (19/31) (49, 52, 53, 57, 59–61, 63–68, 79, 81, 84, 87, 91, 97) were divided into introducing options (in-depth; 6/31,19.35%) (64–67, 79, 87); discussing options (risk–benefits; 13/31,41.94%) (49, 52, 53, 57, 59, 60, 63, 66, 68, 81, 84, 91, 97); offering choice list (2/31,6.45%) (61, 84). Eleven studies mentioned decision talk (11/31) (50, 53, 59–63, 67, 84, 87, 97) were related to discussing risk–benefits (in-depth)(3/31, 9.68%) (53, 59, 87), reaching consensus (7/31, 22.58%) (60–63, 67, 84, 97), explaining confusions (1/31,3.23%) (50). Ten studies (10/31) (52, 59, 62, 64–68, 79, 89) addressed new themes that could not be categorized, including post-decisional interviews (7/31,22.58%) (62, 64–67, 79, 89), conversations on psychology and emotions (3/31, 9.68%) (52, 59, 68). See Figure 3 for a detailed description.
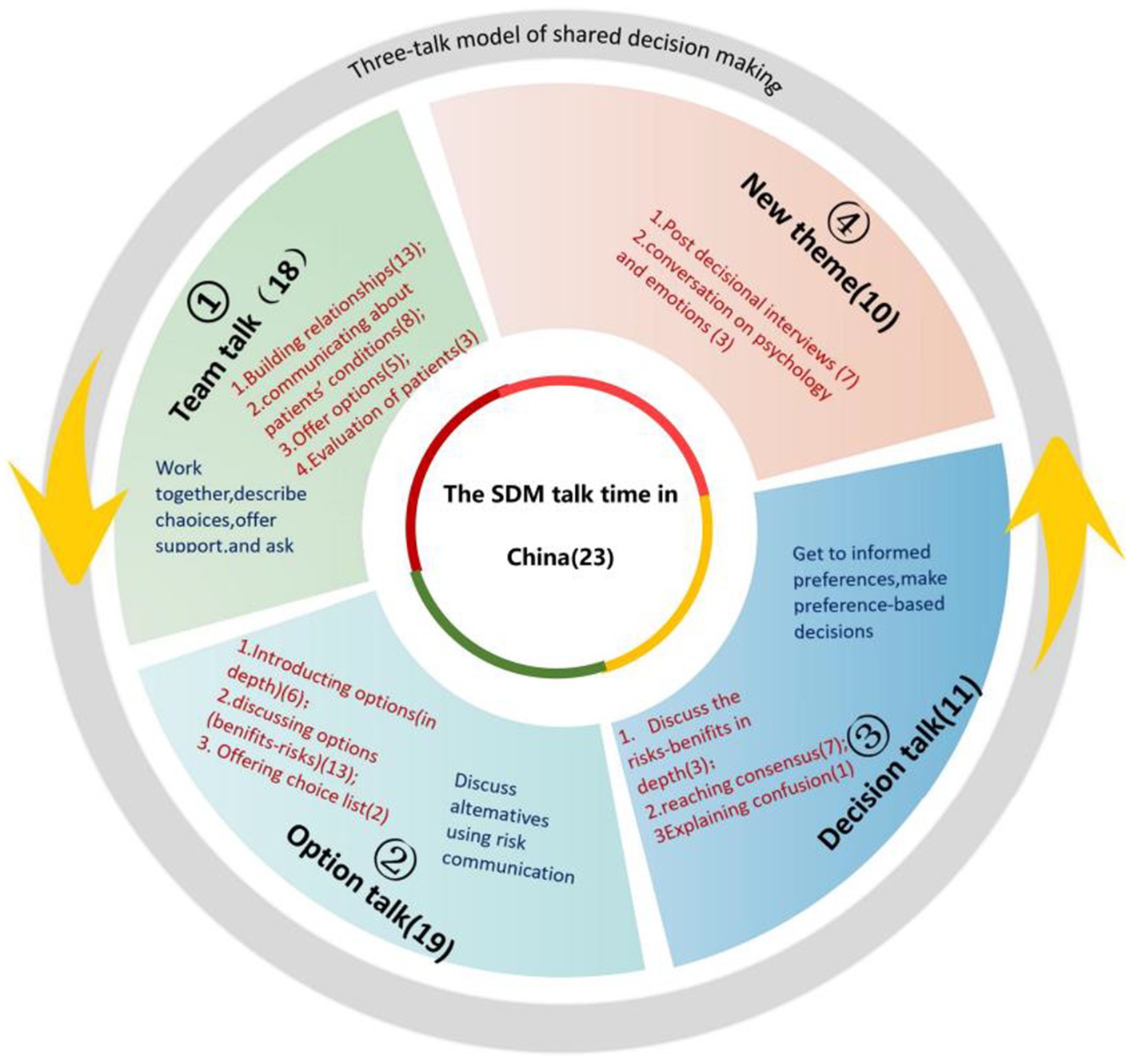
Figure 3. The SDM talk time in China.
Thirty studies mentioned the presence of the interventions, including online tools, paper booklets, and courses. Seven studies mentioned online tools (7/30,23.33%), of which one was an app (1/30, 3.33%) (62), two were WeChat groups (2/30, 6.67%) (49, 50), two were public websites (2/30, 6.67%) (50, 69), one was an applet (1/30, 3.33%) (7), and one was an online decision aid (1/30,3.33%) (85). Fifteen studies (15/30,50.00%) mentioned paper-based tools, of which one was a chart (1/30,3.33%) (49), one was a process picture (no specific; 1/30,3.33%) (81), 12 were booklet (12/30,40.00%) (9, 50, 61, 64–66, 84, 85, 87–89, 91), and one was a patient selection form (1/30,3.33%) (91). The interventions in 8 eight studies were in the category of courses (8/30, 26.67%), of which six were videos (6/30, 20.00%) (49, 50, 64–66, 87), and two were lectures (2/30, 6.67%) (50, 66).
We mapped the results of this part to the construction process of PDAs in NHS’s Standards framework for shared decision-making support tools, including patient decision aids. This guideline sets out a standard to support people in designing patient decision aids (PDAs). In this study, nine studies (9/30,30%) (7, 9, 49, 61, 62, 82, 84, 85, 89) were extracted from 30 articles about the interventions. There were 12 steps in the construction process in the NHS standard. However, corresponding to the standard, only 8 of these steps could be reflected in our study. For comprehensive construction procedures and relevant literature sources please refer to Appendix 5. A detailed classification is presented in Figure 4.
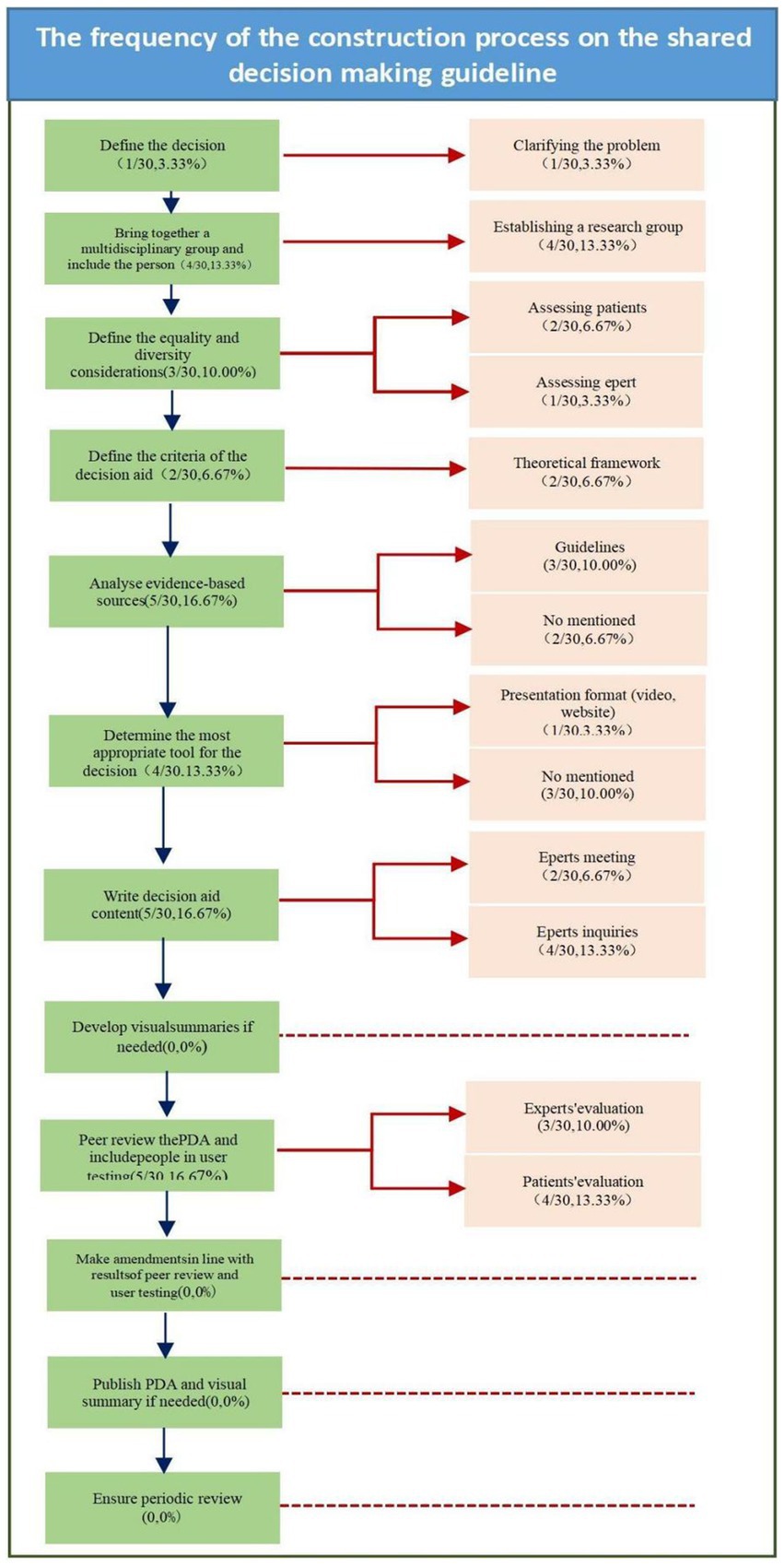
Figure 4. The frequency of the construction process on the SDM guideline.
Shay and Lafata’s classification model classifies outcomes into cognitively affective, behavioral, and health outcomes. Based on the model proposed by Shay and Lafata for the categorization analysis of decision outcome indicators, a total of 68 outcome indicators addressed in the 60 included papers were grouped into four domains of affective-cognitive outcomes (36/60,60.00%) (47, 48, 52, 55–58, 61, 62, 66–68, 70, 72, 74–78, 81, 82, 84, 86, 87, 91–102), behavioral outcomes (22/60,36.67%) (48, 49, 51, 53, 58–61, 63, 68, 69, 72, 74, 75, 81, 83, 84, 86, 87, 89, 97, 99), health outcomes (25/60,41.67%) (49, 50, 52, 53, 57, 59, 60, 62–69, 74, 78, 82, 83, 87, 88, 90, 97, 100, 102). The length of time and cost of hospitalization could not be classified in the model (2/60,3.33%) (66, 102). The specific categorization of outcome indicators is shown in Figure 5. See Appendix 6 for specific corresponding references.
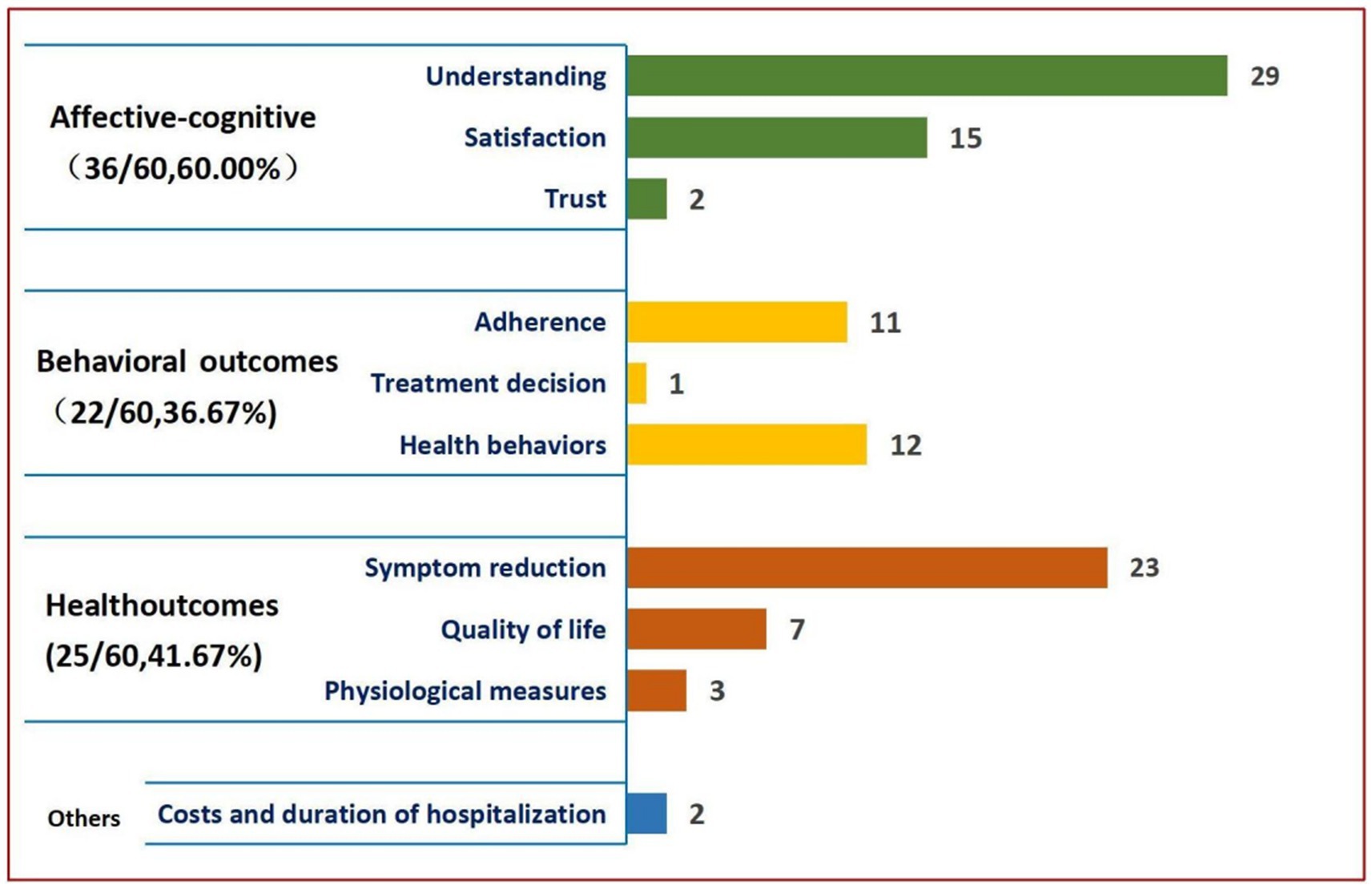
Figure 5. The presentation of decision related outcome analysis results.
To the best of our knowledge, this is the first scoping review of SDM studies in mainland China. We systematically examined the development of SDM in healthcare in mainland China. The following discussion section is organized according to the research questions.
The introduction of SDM in China was influenced primarily by foreign research hotspots, and can be traced back to 1998, when ethics expert Professor Mingjie Zhao first introduced the concept of SDM to Chinese peers and emphasized the important role of patients in medical practice (6). However, the first clinical practice study of SDM in China was not published until 2015 (8). Therefore, SDM research still has much room for improvement, and the patient population needs further refinement. In addition, the absence of formally issued SDM-related policies in China’s mainland has weakened the enthusiasm of physicians to some extent. Policy support is a strong incentive for SDM implementation.
With the development of SDM, scholars from various countries have proposed different models to promote its implementation in medical care. As SDM research in China is still at the stage of theoretical planning and small-scale explorative applications, implementation has been limited. Only about one-fifth of the SDM studies (7, 9, 45, 46, 61–63, 72, 74, 78, 79, 83, 92) in our review used theoretical guidance, all of which originated from foreign countries. Consequently, the adaptation of SDM theorical systems to local contexts is necessary in mainland China. The results of early attempts in this area have been encouraging. Zhang et al. (74) explored the process factors that influence SDM participation from the perspective of Chinese cancer patients and developed a conceptual framework for their involvement (103). The framework takes into consideration the special “filial culture” of China and focuses on the difficulties encountered by older adult patients in the decision support process. However, the framework has been published only recently and is limited in its target group, and is consequently in need of further validation.
Our review found that patient decision-makers face numerous challenges in SDM and need external support. These difficulties include three of the common types of decisional needs related to knowledge, decision aids, and aspects of self-efficacy. The three most common clinical manifestations were inadequate knowledge of the disease or condition to inform a decision (59%), lack of decision-support tools (43%), and low confidence in the ability to implement the chosen option (39%). Therefore, healthcare professionals should focus more on these aspects of the SDM process to promote patient involvement in decision-making.
Identifying patient decision needs is critical to facilitating patient participation in decision-making, as decision needs may be a determinant of sub-optimal decisions (104). Healthcare professionals can implement SDM by prioritizing screening for common manifestations of decision needs, which helps to quickly identify patients’ decision needs, implement shared decisions, and improve patient outcomes (31, 105, 106). In western countries, institutions represented by the University of Ottawa in Canada have conducted in-depth research on decision needs. They have clearly defined the concepts related to decision needs basing on the ODSF framework theory, so that medical practitioners can identify and assess the decision needs of patients and stakeholders in the decision-making process (107). Over 45 foreign studies have conducted decisional needs assessments based on the concept of decision needs in this theoretical framework (31), but we found no evidence from China. Even though research teams in the Chinese region have translated the concepts related to ODSF (108), they have not yet localized and debugged the relevant concepts to fit their own clinical context. The difficulty (rigidly understanding) in recognizing decision needs concepts by Chinese researchers and the gap in results from foreign studies (25) may be due to this difficulty. For example, “decision motivation” is a relatively low-frequency patient decision need in this study, which may be influenced by the traditional Chinese culture, where Chinese people are more introverted. In the long-term doctor-led decision-making model, patients are used to relying on doctors (54, 72, 86, 99) and passively participating in decision-making, making it difficult to detect decision motivation, which researchers often overlook. In addition, there are no uniform methodology standards for developing local and disease-appropriate decision needs survey tools/methods based on ODSF. Therefore, how to effectively define the concept of decision needs applicable to the Chinese cultural and medical scenario is a more pressing research problem and a key component in determining the successful implementation of shared decision making in the Chinese context. At the same time, to facilitate smooth SDM, it is necessary to understand further the common manifestations of decision needs faced by patient decision-makers in different decision areas, which will facilitate further understanding of the strategies used by Chinese patient decision-makers to cope with decision difficulties. These efforts have helped to explore the development of decision actively needs assessment tools or methods that are appropriate to the current state of local healthcare scenarios and populations and have helped to increase the chances that patient decision-makers will be supported in shared decision-making.
In this review, we developed initial codes based on the IP-SDM model (42). The model has the potential to improve decision-making processes and working practices currently exercised in many industrialized healthcare systems. The primary reason for the selection of the IP-SDM model was the chronological order of its constructs. By mapping the extracted contents to its constructs, we can identify the hotspots and developmental stages of Chinese SDM research. As depicted in Figure 2, Our analysis reveals that most Chinese SDM studies have focused on initiation, decision problems, information exchange, values, and preferences. In comparison, fewer studies have focused on factors such as feasibility, preferences, actual choices, implementation, and outcomes. The main reason for this finding may be that Chinese SDM research has just begun and is still in the tool development and localization process. Consequently, most studies may focus on the theoretical connotations of the SDM process, while fewer studies may address implementation (109). Such results provide our researchers with directions for future research. The successful implementation of SDM in China could present a substantial challenge.
Next, we can consider drawing on theories and methods from the field of implementation science to advance implementation research of SDM (110, 111). We found that physicians and nurses were the primary implementers of SDM in China. However, only a few studies mentioned other stakeholders, such as psychologists and volunteers. Such a status contrasts with the internationally promoted concept of multidisciplinary medical teams (112, 113). However, not all studies have proven that multidisciplinary medical teams yield better SDM outcomes; for example, patients may have difficulty in judging the most critical information after being presented with an overwhelming amount of factual detail. Furthermore, increased time costs are often required for multiple participants to reach a final agreement (114, 115). In a developing country such as China, where the doctor-patient ratio is meager, an emphasis on multidisciplinary team participation in SDM may not be an optimal choice. However, this issue is controversial and needs further discussion.
We also applied the Three Talk model to map the timing of the doctor-patient conversation. In the model, SDM is described in three key steps: team talk, option talk, and decision talk (43). The meanings of “build relationships” and “work together” used in SDM and the Three Talk model are substantially different. In the Chinese medical context, establishing relationships usually comprises the building of trust between the doctor and the patient (116). Western doctor-patient relationships are usually based on “institutional trust,” (117) but in China, multiple historical and cultural influences, professional ethics, medical and cultural institutions, and kinship-based ethical relationships are the general mechanisms for building trust in the medical experience (118, 119). Geographic ties, a sense of community membership, and local social opinions also play a significant role (120). Neither interpersonal nor purely institutional trust are established between doctors and patients; this process is culturally specific (121) and deserves to be explored in depth by SDM researchers. As shown in Figure 3, We also found new themes in the “post-decisional interview” “conversation on psychology and emotions.” Decision-making does not end with a decision but also requires attention to the patient’s short-term and long-term feedback (122). Post-decisional talk not only benefits the evaluation of SDM effectiveness, but also enhances the cultural adaptation of the talk model, which contributes to sustainable SDM application.
Most studies that refer to decision support tools are unnamed, and less than half of the tools are designated as patient decision aids. The tools are currently presented in a variety of formats; half are paper-based materials. Less than 1/3 of the studies of support tools mentioned the process of tool development. Illustrated by Figure 4, We mapped our results to the National Institute for Health and Care Excellence framework for shared-decision-making support tools, and found that none of the studies described step 8: Supporting resources, step 10: Release and dissemination, and step 11: Update instructions. Only one study explicitly stated that it evaluated the tool using International Patient Decision Analysis Standards (IPDAS) guidance (9). Despite the proliferation of patient decision aids, information on their development processes is limited. Our finding that many of the patient decision aid trial reports failed to provide clear information regarding tool development was disappointing. Consequently, we systematically searched Chinese websites and found that the only Chinese article that systematically introduced specific IPDAS content was published in 2020 (123). Furthermore, no report on the production of a final version for use and/or further evaluation has been published by Chinese researchers. We can therefore conclude that the introduction and local adaptation of standards and development guidelines are urgently needed.
The conceptual framework to guide analysis of outcome indicators was adapted from Street and colleagues’ and Kreps and colleagues’ (124, 125) models by Shay and Lafata (35). Shay and Lafata adapted models by Street and colleagues and Kreps and colleagues to build a conceptual framework to guide analysis of outcome indicators. Street and Kreps reported 68 outcomes, most of which were classified as affective-cognitive outcomes, followed by health outcomes. The fewest were classified as behavioral outcomes. In comparison, Shay and Lafata assessed 97 unique patient outcomes. Most were classified as affective-cognitive outcomes, followed by behavioral outcomes, and finally by health outcomes. Another study on personal health record technology showed the same trend as Shay and Lafata’s results (126). Referring to Figure 5, Our findings were congruent with these two SDM system evaluations in that most focused indicators belong to affective-cognitive outcomes. However, the focus on health outcomes has been higher in Chinese SDM studies than in the other two reports. Maslow classified human needs in a hierarchy that ascends through physiological, security, social, esteem, and self-actualization needs (127) Higher-level needs can only emerge after the previous lower-level needs are satisfied (127). The health outcomes of this study are physiological needs. Chinese research of SDM and also of the entire healthcare-related field generally focus more on health outcomes than western studies. This prioritization is necessitated by the large population size and the unbalanced and insufficient development and discrepant supply and demand of healthcare resources in China (128). The imbalance in healthcare resources is the major factor that necessitates the reporting of health outcomes in healthcare research in mainland China. This research can aid healthcare professionals in decision-making regarding the adoption or non-adoption of interventions to prioritize the basic needs of most patients in the context of limited resources (129).
Our results also showed that economic effects such as length of stay and costs could not be classified in Shay and Lafata’s model. An alternative outcome imputation model that considers all SDM consequences was proposed by Elwyn et al. (130) Their model includes proximal, distal, and distant effects; and considers the economic outcomes of SDM as distant effects because they take longer to manifest and are therefore less relevant as short-term metrics (130). Whether patient decision aids will generate savings is unclear. Greater consensus on what constitutes a patient decision aid and comparisons of their use to usual care over a sufficient timespan are required for the valid assessment of cost outcomes (131).
The main strength of this integrated approach is that we can take a broader perspective when analyzing the current state of shared decision making implementation in the Chinese region. Understanding the current state of decision needs, decision support, and decision closure for shared decision making is critical to designing or developing more effective shared decision solutions for mainland China and facilitating effective implementation of SDM. For the decision needs analysis, the original studies we included were not initially based on the ODSF, so matching using ODSF decision needs codes may have been biased. In addition, due to the lack of perspectives on the decision-making needs of families supporting patient decision-makers and healthcare professionals makers in the included literature, we only analyzed the decision-making needs of decision-makers regarding patients. We did not explore the decision-making needs of families supporting patient decision-makers and healthcare professionals involved in SDM. This may have overlooked very important caregiver and healthcare worker-related information. In extracting the content of the articles, we did not refer to IP-SDM, Three-Talk, NICE guideline, Shay and Lafata’s model, which resulted in more work and less “linguistic” fit for the content analysis. However, this method of extraction also ensured that we obtained constructs that were not available in the above models, making our findings more informative. The results were presented and discussed in relation to the SDM implementation process, the timing of the conversation, and the tool development process without exploring the coverage of each study as an individual study, but with a broader perspective on the overall research process. This may have caused us to overlook some studies that are very representative of the current state of SDM in China. The minimal representation of Organizational and system level characteristics that influence the implementation of SDM in the full-text presentation may reflect the neglect of these factors in SDM research in China. However, it may also be that the extraction basis chosen for this study the theoretical framework ignored these factors, resulting in the omission of this study.
In this scoping review, we set out to map the findings of existing studies on SDM in mainland China. In terms of decisional needs, we found that patient decision-makers require more external support to overcome challenges in knowledge, decision assistance, and self-efficacy. However, the current lack of local definition of decisional needs will be detrimental to the development of SDM in mainland China. Therefore, it is necessary to conduct a follow-up study on the concept and expression of decisional needs in the Chinese cultural context. The review and summary of the implementation process of SDM and the construction process of PDAs in this study suggested that the scientific and systematic construction of PDAs should be paid attention to in the subsequent research process, and the combination of steps and context should be paid attention to in the implementation of SDM. Moreover, the focus on health outcomes in Chinese SDM studies, driven by the unique healthcare resource landscape, underscores the necessity of prioritizing basic needs within limited resources.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
XL, JZ, and YH: conceptualization. DY, MM, YY, XZ, HW, QL, and ML: data curation. XL and DY: formal analysis. DY, XL, and MM: methodology and writing-original draft. XL: project administration. JZ, YH, and JL: writing-review and editing. All authors contributed to the article and approved the submitted version.
This paper was supported by basic Research Grant Program for 2023 at Beijing University of Chinese Medicine (project level; Grant Number 2023-JYB-XJSJJ019). The funders are not involved in the study design, data collection and analysis, manuscript writing or the decision to submit the manuscript for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1162993/full#supplementary-material
1. Elwyn, G, Frosch, D, Thomson, R, Joseph-Williams, N, Lloyd, A, Kinnersley, P, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. (2012) 27:1361–7. doi: 10.1007/s11606-012-2077-6
2. Legare, F, Adekpedjou, R, Stacey, D, Turcotte, S, Kryworuchko, J, Graham, ID, et al. Interventions for increasing the use of shared decision making by healthcare professionals. Cochrane Database Syst Rev. (2018) 2018. doi: 10.1002/14651858.CD006732.pub4
3. Rose, A, Rosewilliam, S, and Soundy, A. Shared decision making within goal setting in rehabilitation settings: a systematic review. Patient Educ Couns. (2017) 100:65–75. doi: 10.1016/j.pec.2016.07.030
4. Huang, RC. A new chapter has been opened in the study of doctor-patient joint clinical decision-making in the field of cardiovascular diseases in China. Chin Circ J. (2015) 30:756. doi: CNKI:SUN:ZGXH.0.2015-08-011
5. Liu, PL, and Jiang, S. Patient-centered communication mediates the relationship between health information acquisition and patient Trust in Physicians: a five-year comparison in China. Health Commun. (2021) 36:207–16. doi: 10.1080/10410236.2019.1673948
6. Yao, M, Finnikin, S, and Cheng, KK. Call for shared decision making in China: challenges and opportunities. Z Evid Fortbild Qual Gesundhwes. (2017) 123–124:32–5. doi: 10.1016/j.zefq.2017.05.004
7. Wang, ST, Ye, ZX, Pan, ZY, Yang, N, Li, Y, and Li, L. Design of decision-making platform for treating patients with primary liver cancer. Hosp Adm J Chin Peoples Liber Army. (2021) 28:129–33. doi: 10.16770/J.cnki.1008-9985.2021.02.009
8. Yu, L, Yang, S, Guo, PP, Zhang, XH, Liu, N, Wang, J, et al. The application status and prospect of decision aids in breast cancer screening. Chin Nurs Manage. (2020) 20:1591–5. doi: 10.3969/j.issn.1672-1756.2020.10.033
9. Shi, RZ, Hao, YX, Fan, XY, Zhang, SY, Li, Z, and Kang, XF. Development of decision aid with Ottawa decision support framework for patients with implantable cardioverter defibrillator. J Nurs China. (2019) 26:35–40. doi: 10.16460/j.issn1008-9969.2019.05.035
10. Li, Q, and Liu, JR. A new clinical model of shared decision-making between doctors and patients undergoing thyroid carcinoma resurgery. Med Philos. (2018) 39:21–5. doi: CNKI:SUN:YXZX.0.2018-10-007
11. Liu, HJ, Wu, ML, Liao, ZF, Jin, D, and Fang, HP. Applied effect of decision aids in arthroplasty patient. Orthopaedics. (2017) 8:66–9. doi: 10.3969/j.issn.1674-8573.2017.01.016
12. Guo, YR, Liu, YJ, Cai, LB, Wang, Q, Guo, LN, Wang, YY, et al. Application advances of decision aids in joint replacement patients. Chin Nurs Res. (2020) 34:2884–7. doi: CNKI:SUN:SXHZ.0.2020-16-014
13. Shao, SY, Li, T, and Liu, WJ. Research progress on surrogate decisional conflict for children with cancer. J Nurs Sci. (2021) 36:92–5. doi: 10.3870/j.issn.1001-4152.2021.16.092
14. Pieterse, AH, and Finset, A. Shared decision making-much studied, much still unknown. Patient Educ Couns. (2019) 102:1946–8. doi: 10.1016/j.pec.2019.09.006
15. Allen, M. The value of values: shared decision-making in person-centered, value-based oral health care. J Public Health Dent. (2020) 80:S86–8. doi: 10.1111/jphd.12394
16. Bomhof-Roordink, H, Gärtner, FR, Stiggelbout, AM, and Pieterse, AH. Key components of shared decision making models: a systematic review. BMJ Open. (2019) 9:e031763. doi: 10.1136/bmjopen-2019-031763
17. Coronado-Vázquez, V, Canet-Fajas, C, Delgado-Marroquín, MT, Magallón-Botaya, R, Romero-Martín, M, and Gómez-Salgado, J. Interventions to facilitate shared decision-making using decision aids with patients in primary health care: a systematic review. Medicine (Baltimore). (2020) 99:e21389. doi: 10.1097/MD.0000000000021389
18. Légaré, F, Stacey, D, Gagnon, S, Dunn, S, Pluye, P, Frosch, D, et al. Validating a conceptual model for an inter-professional approach to shared decision making: a mixed methods study. J Eval Clin Pract. (2011) 17:554–64. doi: 10.1111/j.1365-2753.2010.01515.x
19. Lee, DL, Hammond, JW, Finkel, K, Gardner, DD, Nelson, B, and Baptist, AP. An electronic shared decision-making app to improve asthma outcomes: a randomized controlled trial. J Allergy Clin Immunol Pract. (2023) 2023:660–8. doi: 10.1016/j.jaip.2023.06.016
20. Chenel, V, Mortenson, WB, Guay, M, Jutai, J, and Auger, C. Cultural adaptation and validation of patient decision aids: a scoping review. Patient Prefer Adherence. (2018) 12:321–32. doi: 10.2147/PPA.S151833
21. Ankolekar, A, Vanneste, BGL, Bloemen-van Gurp, E, van Roermund, JG, van Limbergen, EJ, van de Beek, K, et al. Development and validation of a patient decision aid for prostate Cancer therapy: from paternalistic towards participative shared decision making. BMC Med Inform Decis Mak. (2019) 19:130. doi: 10.1186/s12911-019-0862-4
22. Li, XJ, Zhao, JQ, Zhang, XY, Han, L, Meng, MQ, Peng, K, et al. The concept and clinical implementation status of Ottawa decision support framework−a scoping review. Chin J Nurs. (2022) 6:756–62. doi: 10.3761/j.issn.0254-1769.2022.06.017
23. Zhang, QW, Liu, Y, and Dong, XX. A survey analysis of Patients' perceptions of difficulties in shared clinical decision-making. Chinese j Evid Based Med. (2010) 10:3. doi: 10.3969/j.issn.1672-2531.2010.01.006
24. Yu, W, Liu, X, Zhao, F, Li, M, and Zhang, L. Control of unreasonable growth of medical expenses in public hospitals in Shanghai, China: a multi-agent system model. BMC Health Serv Res. (2020) 20:490. doi: 10.1186/s12913-020-05309-z
25. Liu, J, Hou, S, Evans, R, Xia, C, Xia, W, and Ma, J. What do patients complain about online: a systematic review and taxonomy framework based on patient centeredness. J Med Internet Res. (2019) 21:e14634. doi: 10.2196/14634
26. Xu, RH, Cheung, A, and Wong, E. The relationship between shared decision-making and health-related quality of life among patients in Hong Kong SAR. China Int J Qual Health Care. (2017) 29:534–40. doi: 10.1093/intqhc/mzx067
27. Huang, R, Gionfriddo, MR, Zhang, L, Leppin, AL, Ting, HH, and Montori, VM. Shared decision-making in the People's Republic of China: current status and future directions. Patient Prefer Adherence. (2015) 9:1129–41. doi: 10.2147/PPA.S82110
28. Varpio, L, Paradis, E, Uijtdehaage, S, and Young, M. The distinctions between theory, theoretical framework, and conceptual framework. Acad Med. (2020) 95:989–94. doi: 10.1097/ACM.0000000000003075
29. Hoefel, L, Lewis, KB, O’Connor, A, and Stacey, D. 20th anniversary update of the Ottawa decision support framework: part 2 subanalysis of a systematic review of patient decision aids. Med Decis Mak. (2020) 40:522–39. doi: 10.1177/0272989X20924645
30. Stacey, D, Légaré, F, Boland, L, Lewis, KB, Loiselle, MC, Hoefel, L, et al. 20th anniversary Ottawa decision support framework: part 3 overview of systematic reviews and updated framework. Med Decis Mak. (2020) 40:379–98. doi: 10.1177/0272989X20911870
31. Hoefel, L, O’Connor, AM, Lewis, KB, Boland, L, Sikora, L, Hu, J, et al. 20th anniversary update of the Ottawa decision support framework part 1: a systematic review of the decisional needs of people making health or social decisions. Med Decis Mak. (2020) 40:555–81. doi: 10.1177/0272989X20936209
32. Stacey, D, Légaré, F, Col, NF, Bennett, CL, Barry, MJ, Eden, KB, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. (2014) 1:D1431. doi: 10.1002/14651858.CD001431.pub4
33. Clauser, SB, Taplin, SH, Foster, MK, Fagan, P, and Kaluzny, AD. Multilevel intervention research: lessons learned and pathways forward. J Natl Cancer Inst Monogr. (2012) 2012:127–33. doi: 10.1093/jncimonographs/lgs019
34. Sepucha, KR, and Scholl, I. Measuring shared decision making: a review of constructs, measures, and opportunities for cardiovascular care. Circ Cardiovasc Qual Outcomes. (2014) 7:620–6. doi: 10.1161/CIRCOUTCOMES.113.000350
35. Shay, LA, and Lafata, JE. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med Decis Mak. (2015) 35:114–31. doi: 10.1177/0272989X14551638
36. Gärtner, FR, Bomhof-Roordink, H, Smith, IP, Scholl, I, Stiggelbout, AM, and Pieterse, AH. The quality of instruments to assess the process of shared decision making: a systematic review. PLoS One. (2018) 13:91747. doi: 10.1371/journal.pone.0191747
37. Peters, M, Marnie, C, Colquhoun, H, Garritty, CM, Hempel, S, Horsley, T, et al. Scoping reviews: reinforcing and advancing the methodology and application. Syst Rev. (2021) 10:263. doi: 10.1186/s13643-021-01821-3
38. Arksey, H, and O'Malley, L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
39. Tricco, AC, Lillie, E, Zarin, W, O'Brien, KK, Colquhoun, H, Levac, D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
40. Reimann, HL. Shared decision making and shared responsibility-a problem of modern educational establishments. Agnes Karll Schwest Krankenpfleger. (1968) 22:102–3.
41. The Joanna Briggs Institute. The joanna briggs institute reviewers’ manual 2015 methodology for JBI scoping reviews. Australia, pp. 1–24. (2015).
42. Légaré, F, Stacey, D, Pouliot, S, Gauvin, FP, Desroches, S, Kryworuchko, J, et al. Interprofessionalism and shared decision-making in primary care: a stepwise approach towards a new model. J Interprof Care. (2011) 25:18–25. doi: 10.3109/13561820.2010.490502
43. Elwyn, G, Durand, MA, Song, J, Aarts, J, Barr, PJ, Berger, Z, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. (2017) 359:j4891. doi: 10.1136/bmj.j4891
44. NICE Guideline Updates Team (UK). Evidence review for decision aids for people facing health treatment or screening decisions: shared decision making. London: National Institute for Health and care excellence (NICE), pp. 1–181. (2021).
45. Zheng, HY, Yang, LN, You, TT, Hu, J, and Yang, Y. The barriers and facilitators of breast cancer patients' participation in shared decision-making: a descriptive qualitative study. Chin Nurs Manage. (2020) 20:1492–149. doi: 10.3969/j.issn.1672-1756.2020.10.013
46. Cai, C, Fang, HP, Liu, HJ, Xia, Y, Wang, WD, and Zhou, YR. Participation of patients with breast neoplasms in decision-making regarding treatment and nursing care: a qualitative study. Mod Clin Nurs. (2020) 19:26–31. doi: 10.3969/j.issn.1671-8283.2020.09.005
47. Fu, JQ, and He, LJ. Investigation and analysis of requirements to participate in medical decision making in patients with breast cancer. Chin J Mod Nurs. (2016) 22:1881–4. doi: 10.3760/cma.j.issn.1674-2907.2016.13.028
48. Tang, H, Wang, S, Dong, S, Du, R, Yang, X, Cui, P, et al. Surgery decision conflict and its related factors among newly diagnosed early breast cancer patients in China: a cross-sectional study. Nurs Open. (2021) 8:2578–86. doi: 10.1002/nop2.791
49. Yang, H. Effect of health care shared decision-making mode on functional exercise in patients with breast cancer after operation. Chin J Pract Nurs. (2019) 11:836–41. doi: 10.3760/cma.j.issn.1672-7088.2019.11.007
50. Qian, YF, Zhang, XF, Jin, AX, and Zhang, X. The effect of shared decision-making model on chemotherapy integrity rate and decision participation satisfaction of breast cancer patients. J Nurs Rehabil. (2020) 19:54–6. doi: 10.3969/j.issn.1671-9875.2020.04.013
51. Wang, J, Liu, YX, Wang, RX, et al. Study on participation in medication decision-making in older adult patients with multiple chronic diseases in Wuhan. Med Soc. (2021) 34:46–50.
52. Li, YL, Luo, WL, Chen, SY, et al. Application of doctor-patient shared decision making intervention in schizophrenic patients with persistent auditory hallucinations. J Qilu Nurs. (2020) 26:53–5.
53. Liang, QS, Du, Y, Pan, J, et al. Influences of shared decision making on schizophrenic treatment compliance. J Clin Psychosom Dis. (2015) 5:116–8.
54. Huang, C, Plummer, V, Wang, Y, and Lam, L. I am the person who knows myself best: perception on shared decision-making among hospitalized people diagnosed with schizophrenia in China. Int J Ment Health Nurs. (2020) 29:846–55.
55. Yang, HL. Related factors affecting the desires of patients with schizophrenia to be involved in medical decision. Med J Chin Peoples Health. (2014) 26:3–7.
56. Zhang, ZH, Xie, FL, Chen, AP, Bai, LH, and Guo, YB. A qualitative study of the psychological experience and supportive needs of patients with advanced lung cancer participating in and implementing treatment decisions. Mod Clin Nurs. (2020) 19:30–6. doi: 10.3969/j.issn.1671-8283.2020.07.005
57. Meng, Y, Gai, BJ, Kan, LL, Liu, C, and Cao, ZR. Effects of treatment decision aid on decision-making difficulties and anxiety, depression in patients with lung cancer. Chin J Mod Nurs. (2018) 24:1692–5. doi: 10.3760/cma.j.issn.1674-2907.2018.14.021
58. Huang, C, Plummer, V, Lam, L, and Cross, V. Shared decision-making in serious mental illness: a comparative study. Patient Educ Couns. (2020) 103:1637–44. doi: 10.1016/j.pec.2020.03.009
59. Ou, YH, Lu, T, and Li, YL. Application of doctor-patient SDM intervention model in patients with bipolar disorder. Mod Diagn Treatment. (2021) 32:137–8.
60. Zhao, XM, and Wu, GH. Influence of diagnosis and treatment mode of doctor-patient joint decision-making on medication compliance and clinical efficacy of community patients with psychiatric disorders. China Med Eng. (2017) 25:16–8. doi: 10.19338/j.issn.1672-2019.2017.12.005
61. Li, Y. Construction and application of treatment decision aids for early-stage primary liver Cancer patients. (2017).
62. Ye, M, Wang, AL, Qiao, CP, Yu, GY, Mao, WW, Han, J, et al. Design and implementation of PICC informed consent mobile medical decision aid program for gynecological tumor patients. Journal of. Nurs Sci. (2021) 36:5–9. doi: 10.3870/j.issn.1001-4152.2021.08.005
63. Guo, YR. Construction and application of decision aids program for functional exercise in patients with Kinesiophobia of unilateral Total knee arthroplasty. (2020). doi: 10.27466/d.cnki.gzzdu.2020.003408
64. Zhang, DM, Zhao, YL, and Feng, ZJ. The application value of shared decision nursing in rapid rehabilitation of knee arthroplasty. Mod J Integr Tradit Chin Western Med. (2019) 28:1117–20. doi: 10.3969/j.issn.1008-8849.2019.10.023
65. Du, LY. Effects of shared decision-making rapid rehabilitation nursing on anxiety level and joint function recovery of patients with knee arthroplasty. J Pract Med Tech. (2021) 28:714–6. doi: 10.19522/j.cnki.1671-5098.2021.05.070
66. Liu, XF, Xie, JH, Yi, YZ, Tan, J, Mo, SS, and Dong, L. Application of shared decision making in rapid rehabilitation of congenital tibial pseudarthrosis in children. Mod Nurs. (2020) 27:93–6. doi: 10.19793/j.cnki.1006-6411.2020.30.039
67. Zhang, WJ, Zhang, DY, Li, HH, and Wang, L. Application of doctor-nurse-patient sharing decision-making in perioperative ERAS model for patients with esophageal cancer. Chin J Surg Oncol. (2020) 12:493–7. doi: 10.3969/j.issn.1674-4136.2020.05.024
68. Chen, HH, Chen, SY, and Chen, XZ. Application of doctor-patient SDM in preventing postoperative thrombosis in older adult patients with lower limb fracture surgery. J Qilu Nurs. (2020) 26:78–80. doi: 10.3969/j.issn.1006-7256.2020.24.027
69. Liu, N, Li, Q, Ji, MM, and Wang, LH. Effect of medical staff-family members combined intervention based on shared decision on gastric Cancer patients. J Qilu Nurs. (2021) 27:1–3. doi: 10.3969/j.issn.1006-7256.2021.08.001
70. Guo, Y, Wen, XL, Xin, X, Qiao, LN, Jin, XZ, Qu, Z, et al. Inform consent or conceal the truth: a qualitative study on the real experience of sharing decision-making between doctors and patients in rectal Cancer patients undergoing Enterostomy. Chin Med Ethics. (2020) 33:80–4. doi: 10.12026/j.issn.1001-8565.2020.01.18
71. Su, J, Bian, W, Zhou, FJ, Liu, MQ, Tan, MQ, and Guo, WM. Qualitative study of treatment decision experience in patients with enucleation of eyeball. J Clin Pathol Res. (2020) 40:124–9. doi: 10.3978/j.issn.2095-6959.2020.01.021
72. Li, YZ. A study on status quo and influencing factors of thyroid Cancer Patients’ Participation in treatment decision-making. (2019). doi: 10.27465/d.cnki.gzzyc.2019.000061
73. Bian, W, Wan, JL, Su, J, Tan, MQ, and Wang, LH. Experience of shared decision making in patients with age-related macular degeneration: a qualitative research. Hosp Adm J Chin Peoples Liber Army. (2019) 26:1039–41.
74. Zhang, YZ, Fang, HP, Zhu, LS, Liu, HJ, Li, BW, and Zhang, YL. Construction of conceptual framework for sharing decision of cancer patients based on clinical decision theory. Chin Nurs Res. (2020) 34:136–41. doi: 10.12102/j.issn.1009-6493.2020.01.026
75. Zhang, HW, Hou, XT, and Bai, DL. The patients satisfaction with participation in medical and nursing decision making among cancer patients: a cross-sectional study. BMC Med Inform Decis Mak. (2017) 33:1805–9. doi: 10.3760/cma.j.issn.1672-7088.2017.23.013
76. Feng, XM, and Zou, YS. Diabetic Patients’ attitudes towards the patient decision aids in shared decision-making. Med Philos. (2021) 42:62–6. doi: 10.12014/j.issn.1002-0772.2021.10.14
77. Wan, JL, Bian, W, and Liu, MQ. Qualitative study on factors influencing co-decision in patients with wet age-related macular degeneration. J Clin Pathol Res. (2020) 40:417–22. doi: 10.3978/j.issn.2095-6959.2020.02.026
78. Wu, Q. Study on process, influencing factors and information processing feature of atrial fibrillation patient engagement in treatment decision making. (2019).
79. Shi, RZ. Development and application of a decision aid for implantable cardioverter defibrillator candidates. (2019). doi: 10.27648/d.cnki.gzxhu.2019.000473
80. Xie, MK, Yang, QF, and Que, J. Atrial fibrillation patients’ involvement in anticoagulation therapy decision-conflict: a qualitative study. Nurs J Chin Peoples Liber Army. (2020) 37:18–21. doi: 10.3969/j.issn.1008-9993.2020.12.005
81. Li, L, and Lang, CY. The effect analysis of shared decision-making nursing model on neurology patients. J Wenzhou Med Univ. (2019) 49:301–5. doi: 10.3969/j.issn.2095-9400.2019.04.015
82. Mou, CY, Qu, Y, and Cao, N. Effect of patient-participation decision-making model based on nurse-patient harmony vision on patients' decision intention and disease management in neurology department. J Nurs Train. (2019) 34:2169–73. doi: CNKI:SUN:FSJX.0.2019-23-013
83. Zhou, JJ. The influence of shared decision perception intervention on patients with coronary heart disease under the guidance of goal control theory. Int Med Health Guid News. (2020) 26:2323–5. doi: 10.3760/cma.j.issn.1007-1245.2020.15.049
84. Wu, LY. Influence of shared decision intervention on treatment decision conflict and decision satisfaction of patients with coronary heart disease. J Qilu Nurs. (2020) 26:9–12. doi: 10.3969/j.issn.1006-7256.2020.01.003
85. Huang, R, Song, X, and Wu, J. Assessing the feasibility and quality of shared decision making in China: evaluating a clinical encounter intervention for Chinese patients. Patient Prefer Adherence. (2016) 10:2341–50. doi: 10.2147/PPA.S115115
86. Liu, QM, Yu, Q, and Le, MX. Effect of expectation and ability of patients with inflammatory bowel disease participating in clinical decision making on their satisfaction with clinical participation. Shanghai Nurs. (2021) 21:19–22. doi: 10.3969/j.issn.1009-8399.2021.01.005
87. Chen, Y, Duan, XC, and Zhang, YJ. The influence of shared decision-making on negative emotion, compliance behavior and treatment effect in patients with acne. Chin J Aesthetic Med. (2021) 30:156–9. doi: 10.15909/j.cnki.cn61-1347/r.004258
88. Deng, JX, Dong, ZH, and Yin, ZF. The value of decision assistance in controlling risk factors of atherosclerotic cardiovascular disease in diabetic patients. Shanxi Med J. (2019) 48:56–8. doi: 10.3969/j.issn.0253-9926.2019.01.019
89. Li, Y, Qiao, J, and Wang, Y. Application of doctor-patient SDM-based individualized management mode in T2DM patients receiving insulin therapy. Chin J Clin Res. (2019) 32:1501–6. doi: 10.13429/j.cnki.cjcr.2019.11.011
90. Wang, YJ. Analysis of doctor-patient shared decision-making on prognosis of diabetes mellitus complicated with cerebral infarction. Chin J Urban Rural Enterprise Hyg. (2019) 34:192–4. doi: 10.16286/j.1003-5052.2019.04.086
91. Xie, CF. Application and research of share decision making in emergency patients with hypertension. China Health Stand Manage. (2021) 12:139–42. doi: 10.3969/j.issn.1674-9316.2021.02.051
92. Ming, J, Wei, Y, and He, LY. Corelation analysis of physician-patient shared decision-making and the adoption of new medical technologies. Chin Hosp Manage. (2018) 38:19–22. doi: CNKI:SUN:YYGL.0.2018-03-009
93. Zhang, QW, Wan, XL, and Liu, Y. A survey analysis of Patients’ perceptions of difficulties in shared clinical decision-making. Chin J Pract Nurs. (2010) 10:10–3. doi: 10.3969/j.issn.1672-2531.2010.01.006
94. Zhang, LJ, Zhang, QW, and Wang, HQ. A survey analysis of the feasibility of a bidirectional way for encouraging shared decision-making between physicians and patients. Med Philos. (2013) 34:94–7. doi: CNKI:SUN:YXZL.0.2013-02-035
95. Zhao, Y, Zhang, Q, and Liang, LZ. Study on the theory and practical problem of“patient participation” in clinical decision making. Chin Med Ethics. (2018) 31:799–803. doi: 10.12026/j.issn.1001-8565.2018.06.27
96. Luo, H, Liu, G, Lu, J, and Xue, D. Association of shared decision making with inpatient satisfaction: a cross-sectional study. BMC Med Inform Decis Mak. (2021) 21:25. doi: 10.1186/s12911-021-01385-1
97. Ding, WY. Application of doctor-patient shared decision-making in hemodialysis patients. Mod Pract Med. (2020) 32:1124–6. doi: 10.3969/j.issn.1671-0800.2020.09.050
98. Yuan, YJ, Wu, Y, and Yan, MQ. Study on the patients’ preferences for involvement in surgical decision-making and influencing factors. J Nurs Sci. (2014) 29:23–5. doi: 10.3870/hlxzz.2014.10.023
99. Yuan, N, Liu, CE, and Yu, L. Status quo of participation of surgery patients in surgical decision-making and its influence factors. J Nurs. (2017) 24:47–50. doi: 10.16460/j.issn1008-9969.2017.04.047
100. Zheng, HX. Multi-dimensional research on the influence of maternal delivery decision from the perspective of shared decision making. (2019).
101. Bai, DL, Hou, XT, Liu, XH, et al. Expectation for participation in medical decision making among advanced cancer patients: a cross-sectional study. J Nurs Sci. (2017) 32:35–8.
102. Wu, SB, and Lv, AL. Application value of shared decision-making on doctor-patient communication in ICU. Med Philos. (2019) 40:25–7. doi: 10.12014/i.issn.1002-0772.2019.06.06
104. O'Connor, AM, Tugwell, P, Wells, G, Elmslie, T, Jolly, E, Hollingworth, G, et al. A decision aid for women considering hormone therapy after menopause: decision support framework and evaluation. Patient Educ Couns. 33:267–79. doi: 10.1016/s0738-3991(98)00026-3
105. O’Connor, A. Developing a program of research: An essential process for a successful research career. Vancouver, Canada: CHNET Press, pp. 1–390. (2018).
106. Legare, F, Kearing, S, Clay, K, Gagnon, S, D’Amours, D, Rousseau, M, et al. Are you SURE?: assessing patient decisional conflict with a 4-item screening test. Can Fam Physician. (2010) 56:e308–14.
107. Jacobsen, MJ, O’Connor, AM, and Stacey, D. Decisional needs assessment in populations: a workbook for assessing patients’and practitioners’decision making needs. (2013). Available at: https://decisionaid.ohri.ca/docs/implement/Population_Needs.pdf.
108. ODSF. Chinese version of The Ottawa decision support framework. (2013). Available at: https://guide.medlive.cn/guidelinesub/8443.
109. Zhai, H, Lavender, C, Li, C, Wu, H, Gong, N, and Cheng, Y. Who decides? Shared decision-making among colorectal cancer surgery patients in China. Support Care Cancer. (2020) 28:5353–61. doi: 10.1007/s00520-020-05391-3
110. Scholl, I, Larussa, A, Hahlweg, P, Kobrin, S, and Elwyn, G. Organizational- and system-level characteristics that influence implementation of shared decision-making and strategies to address them - a scoping review. Implement Sci. (2018) 13:40. doi: 10.1186/s13012-018-0731-z
111. Kostick, KM, Trejo, M, Volk, RJ, Estep, JD, and Blumenthal-Barby, JS. Using nudges to enhance Clinicians' implementation of shared decision making with patient decision aids. MDM Policy Pract. (2020) 5:850402908. doi: 10.1177/2381468320915906
112. Rocque, GB, Williams, CP, Halilova, KI, Borate, U, Jackson, BE, Van Laar, ES, et al. Improving shared decision-making in chronic lymphocytic leukemia through multidisciplinary education. Transl Behav Med. (2018) 8:175–82. doi: 10.1093/tbm/ibx034
113. Rocque, G, Miller-Sonnet, E, Balch, A, Stricker, C, Seidman, J, Stiles, S, et al. Engaging multidisciplinary stakeholders to drive shared decision-making in oncology. J Palliat Care. (2019) 34:29–31. doi: 10.1177/0825859718810723
114. Bohmeier, B, Schellenberger, B, Diekmann, A, Ernstmann, N, Ansmann, L, and Heuser, C. Opportunities and limitations of shared decision making in multidisciplinary tumor conferences with patient participation-a qualitative interview study with providers. Patient Educ Couns. (2021) 104:792–9. doi: 10.1016/j.pec.2020.09.007
115. De Angst, IB, Kil, P, Bangma, CH, and Takkenberg, JJM. Should we involve patients more actively? Perspectives of the multidisciplinary team on shared decision-making for older patients with metastatic castration-resistant prostate cancer. J Geriatr Oncol. (2019) 10:653–8. doi: 10.1016/j.jgo.2018.12.003
116. Zhou, H, Zhang, J, and Su, J. Internet access, usage and trust among medical professionals in China: a web-based survey. Int J Nurs Sci. (2020) 7:S38–45. doi: 10.1016/j.ijnss.2020.07.003
117. Garvelink, MM, Boland, L, Klein, K, Nguyen, DV, Menear, M, Bekker, HL, et al. Decisional conflict scale use over 20 years: The anniversary review. Med Decis Mak. (2019) 39:301–14. doi: 10.1177/0272989X19851345
118. Nie, JB, Li, L, Gillett, G, Tucker, JD, and Kleinman, A. The crisis of patient-physician trust and bioethics: lessons and inspirations from China. Dev World Bioeth. (2018) 18:56–64. doi: 10.1111/dewb.12169
119. Du, L, Xu, J, Chen, X, Zhu, X, Zhang, Y, Wu, R, et al. Rebuild doctor-patient trust in medical service delivery in China. Sci Rep. (2020) 10:21956. doi: 10.1038/s41598-020-78921-y
120. Chen, J, Zhou, MY, Ye, L, Cheng, YR, Wang, MW, Liu, QY, et al. High time for ease the doctor-patient relationship in China. J Forensic Legal Med. (2020) 72:101961. doi: 10.1016/j.jflm.2020.101961
121. Yang, Q, Zhang, H, Yu, M, Hu, X, Gu, Y, Sun, X, et al. Chinese minority perceives the doctor-patient relationship differently: a cultural and economic interpretation. Front Public Health. (2019) 7:330. doi: 10.3389/fpubh.2019.00330
122. Mishra, MK, Saunders, CH, Rodriguez, HP, Shortell, SM, Fisher, E, and Elwyn, G. How do healthcare professionals working in accountable care organisations understand patient activation and engagement? Qualitative interviews across two time points. BMJ Open. (2018) 8:e23071. doi: 10.1136/bmjopen-2018-023068
123. Mu, W, Lu, Cui, Wang, YY, Li, Y, and Jin, YH. Cross-cultural adaptation and assessment of the international patient decision aids standards v4.0 for Chinese version. Med Philos. (2019) 40:11–7. doi: 10.12014/i.issn.1002-0772.2019.18.03
124. Street, RJ, Makoul, G, Arora, NK, and Epstein, RM. How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Educ Couns. (2009) 74:295–301. doi: 10.1016/j.pec.2008.11.015
125. Kreps, GL, O’Hair, D, and Clowers, M. The influences of human communication on health outcomes. Am Behav Sci. (1994) 38:248–56. doi: 10.1177/0002764294038002006
126. Stacey, D, Légaré, F, Lewis, K, Bennett, CL, Barry, MJ, Eden, KB, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. (2011) 10:D1431. doi: 10.1002/14651858.CD001431.pub5
127. Healy, K. A theory of human motivation by Abraham H. Maslow–reflection. Br J Psychiatry. (2016) 208:313. doi: 10.1192/bjp.bp.115.179622
128. Chai, KC, Zhang, YB, and Chang, KC. Regional disparity of medical resources and its effect on mortality rates in China. Front Public Health. (2020) 8:8. doi: 10.3389/fpubh.2020.00008
129. Li, Q, Han, T, Zhang, Y, Zhang, Q, Kong, X, Yang, Y, et al. A nationwide survey on neonatal medical resources in mainland China: current status and future challenges. BMC Pediatr. (2019) 19:436. doi: 10.1186/s12887-019-1780-4
130. Elwyn, G, Frosch, DL, and Kobrin, S. Implementing shared decision-making: consider all the consequences. Implement Sci. (2016) 11:114. doi: 10.1186/s13012-016-0480-9
Keywords: shared decision-making, Ottawa decision support framework, healthcare, patients decision aids, decisional needs
Citation: Li X, Yang D, Meng M, Zhao J, Yin Y, Wang H, Zhang X, Liu Q, Li M, Liu J and Hao Y (2023) Shared decision-making in healthcare in mainland China: a scoping review. Front. Public Health. 11:1162993. doi: 10.3389/fpubh.2023.1162993
Edited by:
Rosaria Indah, Syiah Kuala University, IndonesiaReviewed by:
Shams A. M. Issa, Al-Azhar University, EgyptCopyright © 2023 Li, Yang, Meng, Zhao, Yin, Wang, Zhang, Liu, Li, Liu and Hao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianping Liu, TGl1anBAYnVjbS5lZHUuY24=; Yufang Hao, YnVjbW51cnNpbmdAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.