
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 12 May 2023
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1162711
 Jordi Landier1*
Jordi Landier1* Léa Bassez1
Léa Bassez1 Marc-Karim Bendiane1
Marc-Karim Bendiane1 Pascal Chaud2Florian Franke2Steve Nauleau3Fabrice Danjou3Philippe Malfait2
Pascal Chaud2Florian Franke2Steve Nauleau3Fabrice Danjou3Philippe Malfait2 Stanislas Rebaudet1,4
Stanislas Rebaudet1,4 Jean Gaudart5
Jean Gaudart5Background: Testing was the cornerstone of the COVID-19 epidemic response in most countries until vaccination became available for the general population. Social inequalities generally affect access to healthcare and health behaviors, and COVID-19 was rapidly shown to impact deprived population more drastically. In support of the regional health agency in Provence-Alpes-Côte d’Azur (PACA) in South-Eastern France, we analyzed the relationship between testing rate and socio-demographic characteristics of the population, to identify gaps in testing coverage and improve targeting of response strategies.
Methods: We conducted an ecological analysis of SARS-CoV-2/COVID-19 testing rate in the PACA region, based on data aggregated at the finest spatial resolution available in France (IRIS) and by periods defined by public health implemented measures and major epidemiological changes. Using general census data, population density, and specific deprivation indices, we used principal component analysis followed by hierarchical clustering to define profiles describing local socio-demographic characteristics. We analyzed the association between these profiles and testing rates in a generalized additive multilevel model, adjusting for access to healthcare, presence of a retirement home, and the age profile of the population.
Results: We identified 6 socio-demographic profiles across the 2,306 analyzed IRIS spatial units: privileged, remote, intermediate, downtown, deprived, and very deprived (ordered by increasing social deprivation index). Profiles also ranged from rural (remote) to high density urban areas (downtown, very deprived). From July 2020 to December 2021, we analyzed SARS-CoV-2/COVID-19 testing rate over 10 periods. Testing rates fluctuated strongly but were highest in privileged and downtown areas, and lowest in very deprived ones. The lowest adjusted testing rate ratios (aTRR) between privileged (reference) and other profiles occurred after implementation of a mandatory healthpass for many leisure activities in July 2021. Periods of contextual testing near Christmas displayed the largest aTRR, especially during the last periods of 2021 after the end of free convenience testing for unvaccinated individuals.
Conclusion: We characterized in-depth local heterogeneity and temporal trends in testing rates and identified areas and circumstances associated with low testing rates, which the regional health agency targeted specifically for the deployment of health mediation activities.
In recent years, social epidemiology has made a significant contribution to showing and explaining health inequalities. Some authors are now advocating an integrative approach based on interdisciplinarity and integrating social science theory more deeply (1). The role played by socio-economic status (SES) in access to care, use of care and health behaviors (2) must thus be taken into account to study the disparities observed within the population in the recent COVID-19 pandemic, especially in access and use of diagnostic tests.
During the 18 months after the first hard lockdown in France, mass testing, tracking and isolating was the only way to attempt controlling the spread until generalized vaccination became available. Testing also provided knowledge on transmission dynamics and variant detection, as well as anticipating surges in hospitalized cases. Testing was even more crucial in countries aiming for zero-COVID strategies. In such contexts, ensuring access to testing for the population is paramount. However, the distribution of tests can largely be heterogeneous in terms of time, space, but also population groups.
The link between COVID-19 outcomes and socio-economic deprivation was pointed out early in the pandemic, in multiple settings (3, 4). Outcomes included incidence, severe morbidity, mortality, and seroprevalence, following individual-based or ecological study designs. They highlighted the role of deprivation, often combined to population density to increase COVID-19 burden in settings of Europe (5–8), America (9, 10) or Asia (11, 12).
Deprivation was also associated with lower testing rates (5, 6, 13). Studies often relied on deciles or quintiles of the national distribution of deprivation indices. These categories may not reflect accurately local disparities, due to different standards of living between regions (e.g., housing costs between Paris and Marseille, the two largest cities in France). Limits inherent to building indices may also bias results when applied at large scale, when specific situations are difficult to capture accurately. For example, well-off urban population may live without a car, and conversely rural populations across a wide range of socio-economic conditions likely own at least one car and live in a personal house. In addition, these studies only accounted for population density and did not adjust for access to healthcare, nor for the age structure of the population.
We aimed to analyze the relationship between socio-economic profile and SARS-CoV-2 testing and incidence rates during the different phases of the epidemic. We also aimed to support intervention allocation by the regional public health agency of the Provence-Alpes-Côte d’Azur (PACA), a geographically heterogeneous region combining dense urban coastal regions and rural mountainous areas in South-Eastern France.
We conducted an ecological analysis of SARS-CoV-2/COVID-19 testing rate in the Provence-Alpes-Côte d’Azur (PACA) region in south-eastern France, at the highest spatial resolution available for aggregated epidemiological data in France: “regrouped islets for statistical information” (French acronym: IRIS used hereafter). IRIS correspond to contiguous geographical areas regrouping between 1,000 and 5,000 inhabitants. Municipalities (lowest local authority level) with a population <5,000 inhabitants typically correspond to a single IRIS, while municipalities >5,000 are divided into several IRIS. The PACA region counts 946 municipalities and 2,446 IRIS, corresponding to 5.04 million inhabitants.
We analyzed COVID-19 testing rate from the start of the second wave in the PACA region on 21 July 2020 to the regional upsurge in incidence corresponding to the onset of the omicron wave on 23 December 2021. We combined dates of implementation of public health measures and local incidence minima to account for the multiple distinct testing incentives or constraints faced by the population. We distinguished 10 epidemic periods (Supplementary Figure S1; Supplementary Table S1). The delimitations were: the two nationwide lockdowns starting dates (30 October 2020 and 24 March 2021) and first easing up dates (28 November 2020 and 3 May 2021); the end of Christmas holidays (4 January 21); the lowest regional incidence in June before delta-variant wave 4 (23 June 2021); the decree establishing a mandatory health pass for recreational and cultural events >50 participants (16 July 2021), which required a complete vaccination or a negative test result of less than three days, or evidence of a COVID-19 infection for >10 days and ≤ 6 months; end of convenience test gratuity for unvaccinated individuals (15 October 2021); the regional onset of the delta variant-associated fifth wave (8 November 2021).
COVID-19 tests and confirmed cases were available as 7 day cumulative counts aggregated by IRIS from the French National Public Health Agency (Santé Publique France) SI-DEP information system, which aggregates results of all SARS-CoV-2 RT-PCR and antigenic tests performed in the French healthcare system. People presenting for a test provided their home address systematically and a pre-processing algorithm mapped them to the corresponding IRIS.
We excluded IRIS with ≤30 inhabitants because of incomplete covariate data due to non-disclosure of local income statistics when the number of inhabitants is insufficient to preserve anonymity. In addition, we excluded “activity” IRIS hosting >1,000 workers during the day with twice as many workers as inhabitants, as well as “diverse” IRIS corresponding to low population areas (e.g., a protected natural area in the periphery of a city), because the resident population profile could be very different from the actual population frequenting and influencing the transmission. We also excluded IRIS where the average monthly number of tests exceeded three times the actual population over multiple periods, due to likely address errors in laboratories.
We obtained data describing the population of each IRIS from the French National Institute of Statistics and Economic Studies (INSEE). We used the national census database, which provides descriptive data on the population by IRIS and the equipment public database, which provides an exhaustive list of equipment located in each unit, with geographical coordinates (Supplementary Table S2).
We characterized the population inhabiting each IRIS using the following variables: (i) percentage of the population ≥ 15 years old in each social and professional categories (8-category job classification: agriculture, business owners/independent, white-collar, intermediate, employees, blue-collar, pensioned/retired, unemployed/other-including students), (ii) percentage of total IRIS population of foreign origin, (iii) percentage of immigrants in total IRIS population, (iv) four variables used to calculate the French deprivation index (percentage of high-school graduates in population ≥15 years old not studying; percentage of unemployed in the active 15–64 years old population; percentage holding a blue-collar job in the active 15–64 years old population; median income) (14), (v) proportion of overcrowded main residences, (vi) European deprivation index (EDI), which combines ten census-based variables aggregated at the IRIS-level, and deprivation variables at the individual level (proportion of individuals of foreign nationality, of households without a car, of individuals employed as managers or intermediate professionals, of single-parent families, of households with at least two individuals, of non-owner-occupied households, of unemployed individuals, of individuals without post-secondary school education, of overcrowded dwellings, and of non-married individuals) (15), (vii) population density, and (viii) percentage of inhabitants belonging to 4 age groups: <18, 18–39, 40–64, ≥65.
We considered separately the general access to healthcare and the specific access to SAR-CoV-2 tests.
We characterized the general access to healthcare at IRIS level as the number of primary healthcare practitioners (medical doctor (MD), nurse, physiotherapist…) present in the IRIS. We also used localized potential accessibility (LPA), an indicator defined at municipal level corresponding to the number of MD consultations available per year for each person based on their residence (Supplementary Table S2). This composite indicator takes into account the number of MDs relative to the population in the corresponding catchment area, population expected needs and the travel time to the nearest MD.
We considered the specific access to SAR-CoV-2 tests following two main options available for general population testing: medical laboratories, which conducted RT-PCR-based tests throughout all periods; and pharmacies, which deployed antigenic testing from period 3 onwards. We considered distance from a IRIS to the nearest facility and the number of facilities in the IRIS. Preliminary analysis showed a strong correlation between distance to pharmacies and distance to laboratories (Spearman correlation coefficient = 0.6); and the minimal distance to either facility corresponded to the distance to a pharmacy (Spearman correlation coefficient = 1; Supplementary Figure S2). Numbers of pharmacies and laboratories were also correlated (Spearman correlation coefficient = 0.4).
Exploratory analysis of all variables by Spearman correlation confirmed by principal component analysis (PCA) indicated strong positive correlations between general access to healthcare and specific access to testing: a negative correlation between distance to testing facilities and LPA, and strong correlations between the numbers of primary healthcare practitioners and laboratories or pharmacies in IRIS. There was only limited correlation between number of equipment and LPA or distances to testing facilities (Supplementary Figure S2). As a result, we used LPA and number of primary healthcare practitioners in our main analyses, and replaced LPA with distance to pharmacy in the sensitivity analysis.
Statistical analyses were performed using R software (version 4.0.5., R Core Team 2020. R Foundation for Statistical Computing, Vienna, Austria) and packages {mgcv}, {factominer} and {sf}.
In order to evaluate socio-demographic characteristics of IRIS, we grouped them into one age- and one socio-demographic profile using an unsupervised clustering method based on PCA followed by hierarchical clustering on principal components (HCPC) (16, 17). We defined socio-demographic profile using all socio-demographic variables except age variables, and we generated age profiles separately using the 4 age variables. We studied direct effects of EDI, proportion of inhabitants older than 65 years and population density in a sensitivity analysis.
Variable selection in the multivariable model was done based on prior assumptions using a directed acyclic graph (Dagitty v3.0, Supplementary Figure S3) (18). For testing rate, we considered that two main factors could explain the testing rate in a IRIS in the different periods: first, characteristics of general accessibility to tests in the IRIS, due to its geographical location and pre-epidemic access to healthcare and second, elements related to individual testing behavior of IRIS population, such as age, presence of a retirement home, and socio-demographic characteristics.
We used a generalized additive multilevel model [GAMM, (19)] with a random-effect at municipality level to account for similarities in IRIS of the same municipality and for the LPA variable definition available at municipality-level only. As appropriate for count variables, we used a negative binomial distribution to take into account overdispersion, with a log link and included IRIS census-defined log population as an offset. We also included a Gaussian kriging smoother based on the geographical coordinates of each IRIS to account for spatial autocorrelation. Continuous variables were first tested without linear assumption (as splines) in univariate analysis. Sensitivity analyses were conducted by substituting distance to the nearest pharmacy to LPA, as these indicators were too correlated for all to be included in the same model (see Supplementary material). In a second sensitivity analysis, we adjusted for population density and proportion of population above 65 years as spline individual predictors (not requiring linear approximation), and studied the effect of the social deprivation directly including EDI as a linear predictor or as a spline.
Access to information was controlled and SI-DEP data were obtained in accordance with privacy laws (General Data Protection Regulation [EU] 2016/679). Clearance was obtained through a specific convention (number 22DIRA41-0) between Aix-Marseille University and Santé Publique France, from the Aix-Marseille University Ethics committee (number 2022-10-20-006), and from the Aix-Marseille University Data Protection Officer (number 513087).
Out of the 2,446 IRIS in the Provence-Alpes-Cote d’Azur region, we analyzed 2,306 after excluding 74 activity IRIS, 40 diverse IRIS, 25 residential IRIS with population <30 inhabitants, and one single unit corresponding to a rural municipality with 36 inhabitants with monthly test rates >3 times larger than the IRIS population (Figure 1).
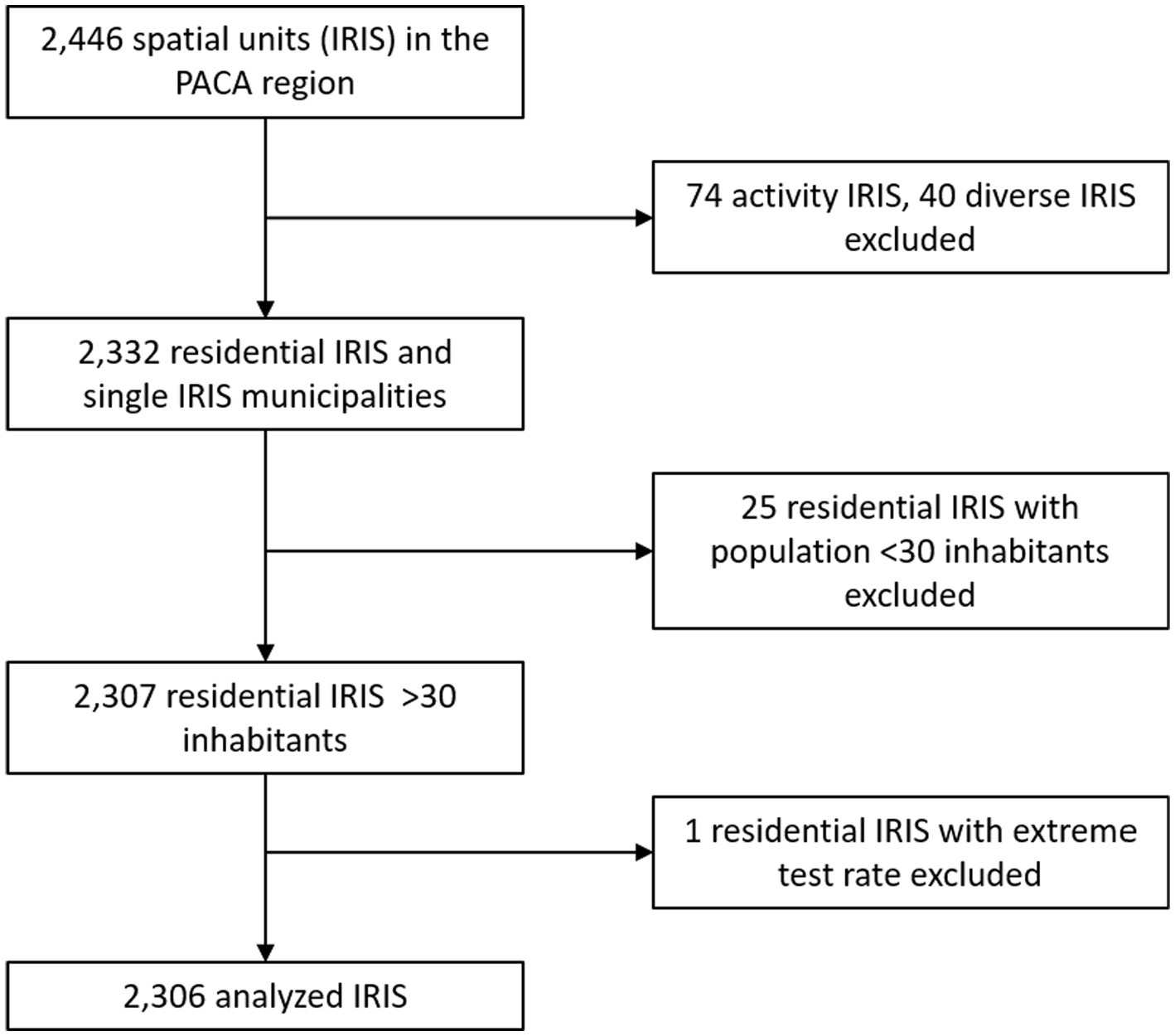
Figure 1. IRIS (spatial units) selection flow chart.
IRIS classification for socio-demographic variables identified 6 profiles ordered by increasing deprivation and exhibiting strong contrasts in terms of population density (Figures 2A,B). The first intermediate-density profile corresponded to the lowest EDI, high income, high proportion of white collar, and densities ranging from peri-urban to urban (profile 1, “privileged”) (Figures 2A-E). A very low-density profile included an important proportion of agriculture workers (profile 2, “remote”) and a second intermediate-density profile ranged from rural to peri-urban IRIS (profile 3, “intermediate”). A high-density urban profile corresponding to young adults, intermediate income with a high proportion of white collars (profile 4, “downtown”). Another high-density urban profile corresponded to areas with a high proportion of blue collar, lower income and intermediate density (profile 5, “deprived”). The third and last urban profile corresponded to very deprived urban areas with highest EDI, highest densities, i.e., neighborhoods of large social housing projects (profile 6, “very deprived”). IRIS profiles presented less heterogeneity in terms of age, with only two profiles displaying higher (remote) or lower proportion (very deprived) of population ≥65 (Figure 2F). Access to healthcare variables by profiles generally reflected the urban vs. rural accessibility issue, access to healthcare being highly variable for rural IRIS (“remote” + “intermediate”) profiles (Figures 2G,H).
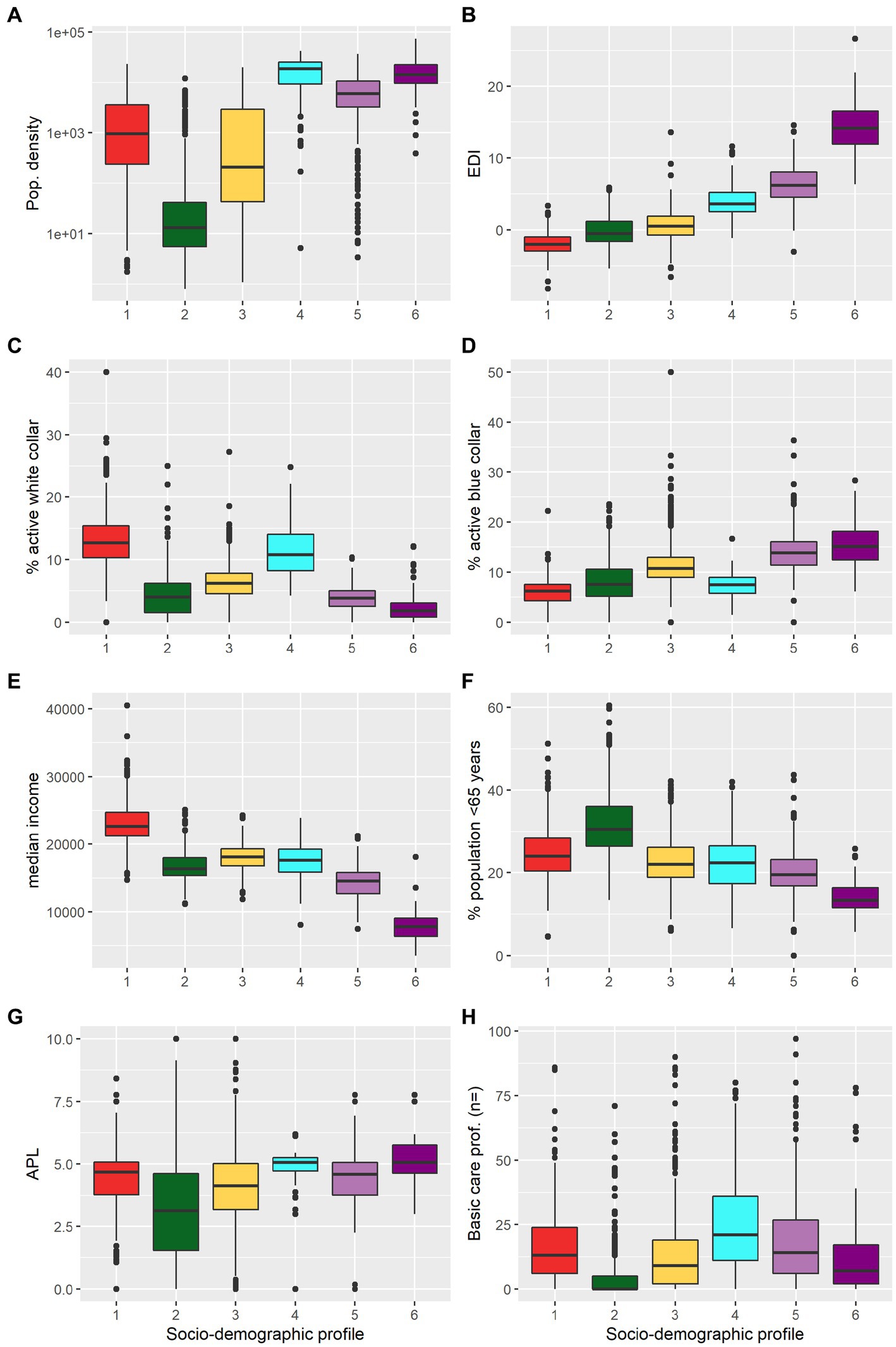
Figure 2. Characteristics of the socio-demographic profiles of the IRIS (spatial units). (A) population density (log scale), (B) European Deprivation Index (EDI), (C) proportion of white collars among active individuals aged ≥15 years, (D) proportion of blue collar among active individuals aged ≥15-years, (E) median income, (F) proportion of population aged ≥65 years, (G) localized potential accessibility (LPA) to healthcare indicator based on the average number of potential medical doctor visits available per inhabitant (defined at municipality level), and (H) number of primary healthcare professionals active in the IRIS. Socio-demographic profiles: (1) “privileged” (red); (2) “remote” (green); (3) “intermediate” (yellow); (4) “downtown” (cyan); (5) “deprived” (light purple); (6) “very deprived” (dark purple). Corresponding histograms are presented in Supplementary Figure S4.
IRIS classification in age profiles identified 4 profiles. The three profiles “families,” “young adults,” and “older adults” were characterized, respectively, by a higher proportion of <18 years old; 18–39 years old, and ≥65 years old. The fourth profile, “balanced” exhibited similar proportions of inhabitants for each age category.
The geographical distribution of IRIS profiles matched expected patterns based on descriptive variables. “Remote” IRIS were mostly located in the mountainous areas of the region. “Privileged” IRIS mostly clustered in a vast area comprising and around Aix-en-Provence city, in the south and east of Marseille city, in along the coast between Marseille and Toulon city, along the coast between Cannes and Nice city. Lastly, “deprived” and “very deprived” IRIS concentrated in the northern part of Marseille city, or particular neighborhoods of Toulon and Nice (Figure 3).
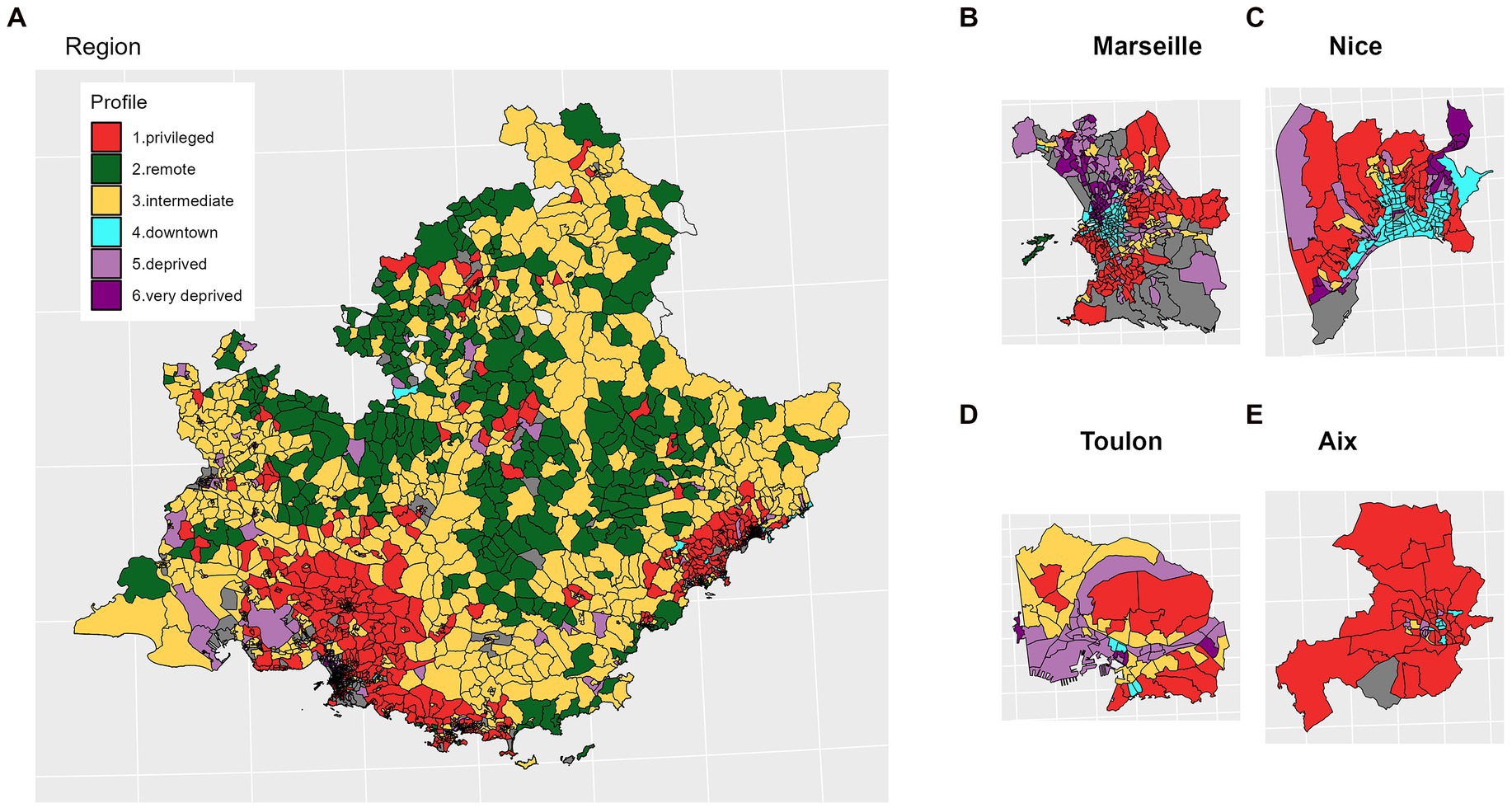
Figure 3. Spatial distribution of the socio-demographic profiles. (A) Provence Alpes Côte d’Azur (PACA) region; (B–E) main cities.
From July 2020 to December 2021, 5 peaks of SARS-CoV-2 testing rate were observed, in parallel with 4 waves of incidence (Figure 4). Testing peaks generally responded to increasing transmission periods, except for the 5th testing rate peak that occurred during Christmas 2020. “Privileged” and “downtown” IRIS exhibited the highest testing rate overall, whereas the “very deprived” IRIS exhibited the lowest test rate, except during summer 2021 (after the health pass establishment; Figure 4A). During that period, urban profiles (“downtown,” “deprived,” and “very deprived”) displayed a general increase and “remote” or “intermediate” profiles showed the lowest testing rates.
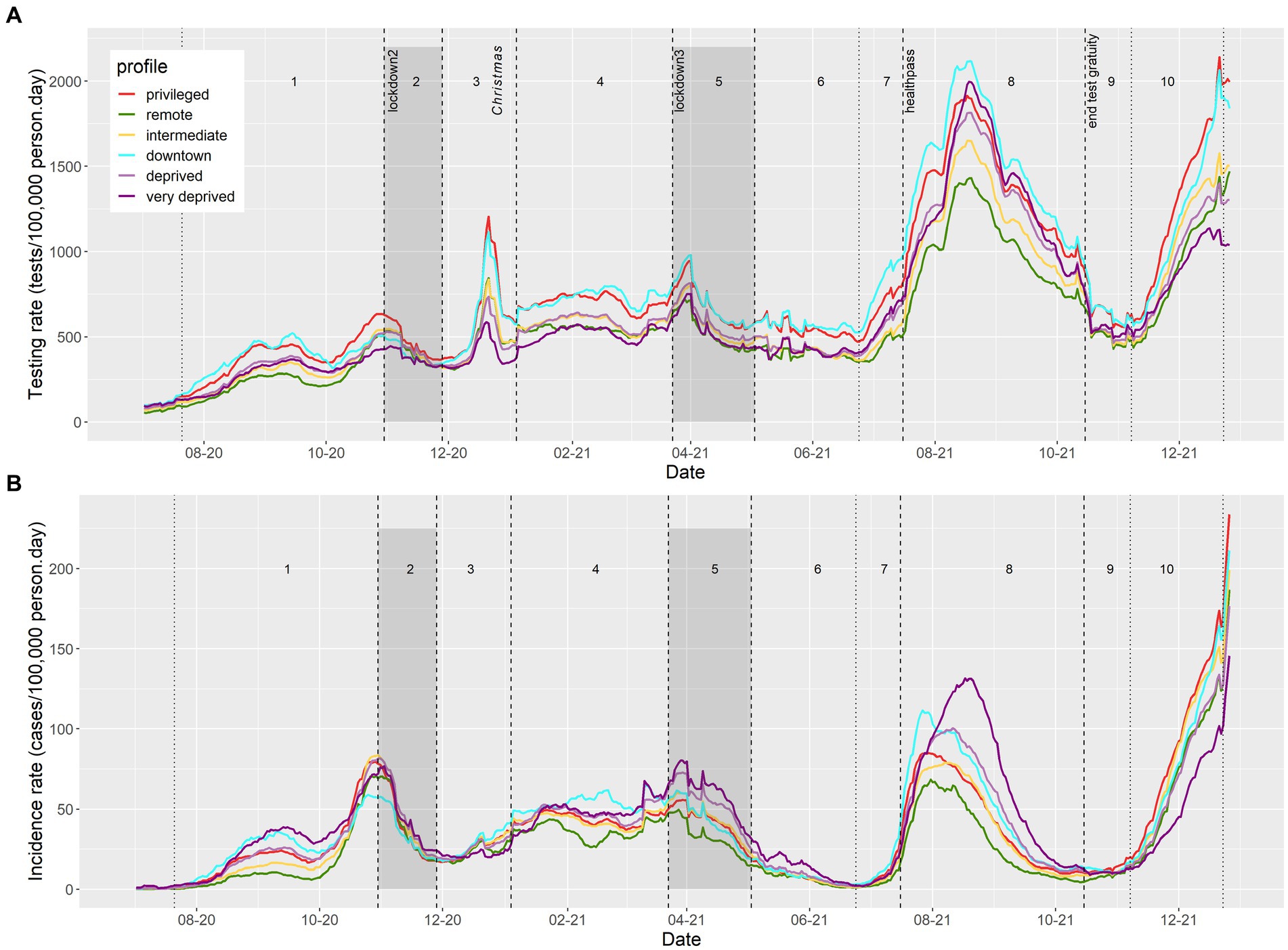
Figure 4. Evolution of daily SARS-CoV-2/COVID-19 (A) testing and (B) incidence rates, by sociodemographic profile in PACA region, from July 2020 to December 2021.
In comparison, COVID-19 incidence rates were highest in the “very deprived,” “downtown,” and “privileged” units, despite contrasted testing rates (Figure 4B). The dynamics in these profiles were also different. In 2020, the “privileged” and “downtown” IRIS reached their maximum incidence rate one week before the October lockdown (period 1), while “very deprived” IRIS reached their peak during the week after the lockdown (period 2). Likewise, in July 2021 (period 8), “privileged” and “downtown” IRIS reached a maximum incidence rate at the end of July, compared to early August for “deprived” and mid-August for “very deprived” profiles, in a context of general high testing rates in these largely urban IRIS.
We analyzed each period separately to identify factors associated with testing rate at IRIS level.
During period 1 (wave 2 rising), “privileged” IRIS showed a higher testing rate than all others and were chosen as a reference class. The adjusted testing rate ratio (aTRR) ranged from a 5% difference for “downtown” IRIS (aTRR = 0.95, 95% confidence interval = [0.91–0.97]) to a 21% difference for “very deprived” IRIS (aTRR = 0.79 [0.79–0.74]) (Table 1). The presence of older adults also played a role, with an independent effect of the presence of a retirement home (aTRR = 1.07 [1.04–1.09]) and of the “older adults” age profile [aTRR = 1.11 (1.06 to 1.15), with “families” age profile as the reference class; Table 1]. LPA and number of primary healthcare professionals showed non-linear relationships with testing rate ratio (Table 1). For lower values of both variables, an increase was associate with a strong increase in aTRR. For LPA above 3 general practitioner consultations available per inhabitant and per year, no additional effect on the aTRR was observed, while for IRIS with >10 primary healthcare practitioners, the increase of aTRR associated with supplementary practitioners was limited.
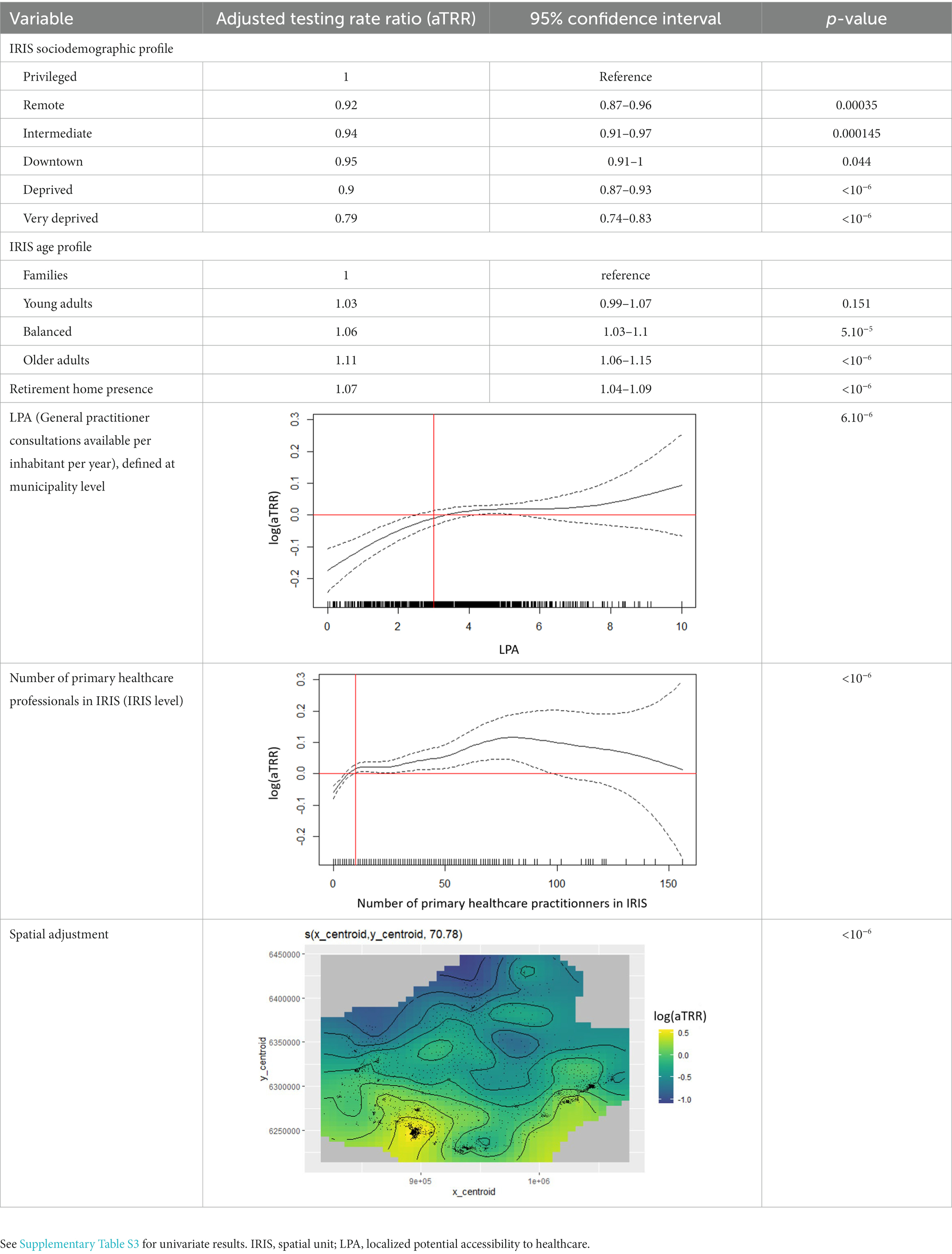
Table 1. Adjusted factors associated with SARS-CoV-2/COVID-19 cumulative testing rate between 22 July and 29 October 2020: multivariate model results for period 1.
After adjusting for structural indicators of access to healthcare (LPA and number of primary healthcare practitioners) and spatial autocorrelation, “remote” and “intermediate” IRIS exhibited only limited gaps in SARS-CoV-2 testing rates compared to “privileged” IRIS (Figure 5A). “Intermediate” IRIS had higher testing rates compared to “remote” IRIS, with a parallel dynamic.
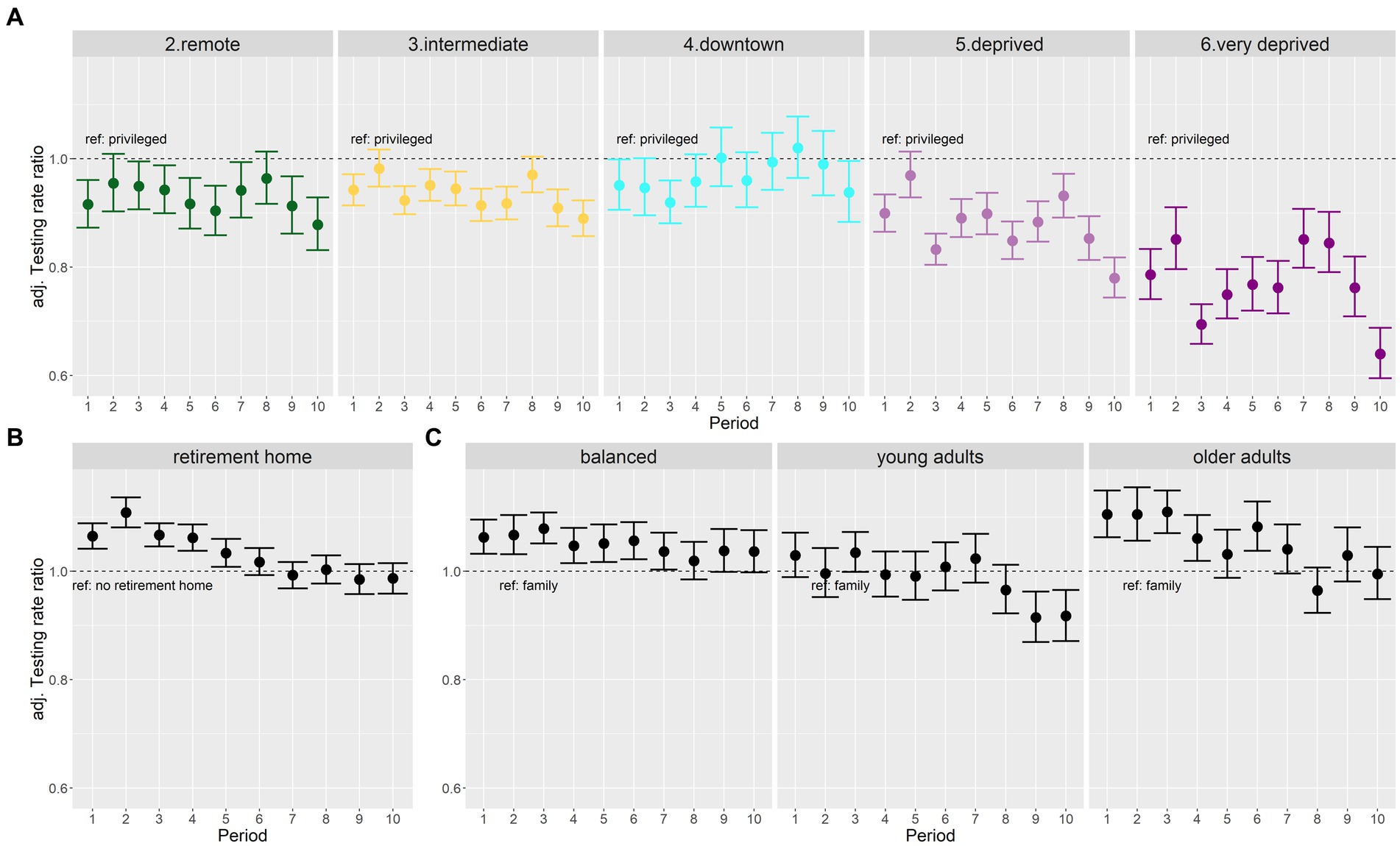
Figure 5. Forest plots of adjusted testing rate ratios (aTRR) across all 10 periods: (A) changing patterns between socio-demographic profiles (reference class, “privileged” profile), (B) decreasing effect of retirement homes over time, and (C) changing patterns according to age profiles (reference class, “family” profile).
Likewise, “downtown” IRIS did not have significantly lower aTRR except during period 3 and 10, corresponding to Christmas 2020 and 2021 periods (Figure 5A). On the other hand, aTRR were consistently lower for “deprived” IRIS (except during lockdown period 2) and for “very deprived” Sus (during all periods). The lowest differences (approximately 15%) between “privileged” and “very deprived” profiles were observed for periods 7 and 8 after health pass implementation. But in spite of massively available tests, periods 9 and 10 exhibited a sharp drop of testing in “deprived” and “very deprived” as compared to the “privileged” IRIS (Figure 5A).
The effect of the presence of a retirement home waned over the different periods (Figure 5B). The effect of age profile also changed gradually from early periods: older adults profile IRIS had higher testing than the family IRIS reference during early periods, and young adults profile IRIS had lower testing rate in the last two periods (Figure 5C).
The effect of LPA remained similar across periods, reaching a plateau around 2.5–3 available consults per inhabitant and per year (Supplementary Figure S5). The effects associated to the number of primary healthcare professionals were more heterogeneous, with strongly non-linear shapes during the three “rising wave” periods 1, 7, 10 (Supplementary Figure S6).
We conducted a sensitivity analysis replacing municipality-level LPA by IRIS-level distance to nearest pharmacy, which did not change the results (Supplementary Figure S7). The direct analysis of EDI indicated that increasing deprivation was consistently associated with lower testing rates, but that this relationship was not linear for all periods. It also confirmed the periods of highest disparity between privileged and deprived profiles (Supplementary Figures S8, S9).
This geo-epidemiological study analyzed factors associated with SARS-CoV-2 testing rates at the finest spatial scale available in the south-eastern French region across 10 periods spanning 18 months and corresponding to political measures (lockdowns, health pass), contextual events (Christmas) and epidemic waves. Our analysis showed strong contrasts in terms of socio-demographic profiles, access to healthcare, and population structure across the different periods analyzed. It suggests that individuals living in “privileged” and “downtown” IRIS of the main regional cities sustained high testing rates. In contrast, individuals living in “remote” and “intermediate” IRIS displayed stable, slightly lower testing levels, after taking into account their more limited access to healthcare.
Looking away from large metropolitan areas, “remote” and “intermediate” IRIS presented parallel dynamics. While they exhibited only marginal differences in terms of income or EDI, and largely corresponded to rural areas, “intermediate” IRIS extended from rural to suburban areas with a higher population density and a better access to care (LPA and basic care professionals), whereas “remote” IRIS corresponded to smaller villages with low density, aging population, far from health services. These communities had generally poor access to testing facilities, and studies mainly relied on seroprevalence/seroconversion analyses or on massive increase in access to testing to shed light on the rural extent and dynamics of COVID-19 (20, 21).
IRIS in “deprived” and “very deprived” profiles exhibited lower testing rates compared to “privileged” IRIS. Contextual testing periods (Christmas, periods 3 and 10) led to increasingly large testing gaps. Requirement of a health pass to access specific activities led to drastic testing increases in urban populations. However, the following period ending convenience test gratuity for unvaccinated asymptomatic individuals was associated with a dramatic drop in testing rates, mainly within “deprived” and “very deprived” areas, aggravating the underestimation of incidence rates.
Indeed, our results underline how testing disparities could affect the local monitoring of the epidemic: the highest incidence rates were recorded in “deprived,” “very deprived”, and “privileged” profiles, however the epidemic situation could only be interpreted in the light of the much larger underestimation of cases in IRIS with higher levels of deprivation.
We studied drivers of SARS-CoV-2 testing at the finest spatial scale available in France, IRIS. We benefited from a wealth of contextual data provided by the French national census. Combining multiple data sources to characterize IRIS beyond population density, we could adjust for the general access to healthcare using different variables, and for the presence of older adults most likely to receive tests in the first periods before generalized vaccination. Presence of older adults was associated with a specific risk increase until the vaccination campaign reached sufficient coverage (period 5, ending in April 2021).
Access to healthcare is difficult to estimate at the IRIS level. Using a municipality-level localized potential accessibility (LPA) indicator may overestimate access in “very deprived” areas of metropolitan cities, where gaps in public transportation may isolate specific populations/neighborhoods. On the other hand, many rural areas usually rely on the primary healthcare practitioners of the nearest town. Our strategy was thus to combine a distance-driven indicator (LPA or distance to pharmacy) and a presence-driven indicator (number of primary healthcare practitioners). This approach also allowed us to differentiate “remote” IRIS and “intermediate” IRIS, the latter showing a better access to care.
The IRIS-level vaccine coverage data was not available for our study, which precluded the analysis of factors associated with SARS-CoV-2 incidence rate after the onset of the vaccination campaign during the first quarter 2021. As a result, we could only show distinct incidence dynamics according to the IRIS profile, without quantifying the contribution of respective factors. We hypothesize that higher testing rates, better isolation abilities in more spacious housing, and enhanced ability to work remotely could explain the earlier incidence peak in “privileged” versus “very deprived” IRIS during period 2 and 5. In period 8, the different dynamics for the august peak are probably linked to differential vaccine coverage matching deprivation.
Based on our ecological approach, results excluded all individual components involved in population health behaviors. The decision whether or not to get screened stems from a particular psychological mechanism whose theoretical models are numerous (22) and whose determinants are not associated with social characteristics only, even if they play a certain role (23). The simple economic dimension cannot by itself account for the complexity of health behaviors in the multiple dimensions in which they are deployed (24); other elements must be considered in order to better understand them (25). For example, some international studies have shown the influence of socio-cultural factors on health behaviors, and argue for further exploration of these (26). Identified barriers to COVID-19 testing thus also include low health literacy, low trust in the healthcare system, or stigma and consequences of testing positive (27).
Our analysis displays stronger contrasts between most deprived and privileged areas compared to the analysis conducted at national level in France during comparable periods or in Switzerland (5, 6). It also highlights the important contribution of older adults testing until April 2021. Our regional scale analysis based on socio-demographic profiles rather than national quintiles (France) or deciles (Switzerland) of deprivation indices allowed a precise characterization of local specific aspects: indeed, in our study region >30% of IRIS belonged to the highest deprivation quintile defined at French national level, respectively only 10% to the lowest quintile (Supplementary Figure S10). In PACA region, deprivation was also associated with higher severity in very deprived areas compared to privileged ones (28).
Our results show that the disparity in testing rate between socio-demographic profiles was not stable over time, a factor often overlooked. Studies analyzing detected cases as their numerator (incidence rate, dynamics) or denominator (positivity rate, severity ratio, lethality) may therefore be confounded by heterogeneous testing, and appreciate the effect of deprivation incorrectly. Conversely, studies analyzing the relationship between deprivation and mortality or hospitalization rates with a total population denominator may not separate the effects of higher incidence from those of higher severity. When available, sero-prevalence data can contribute to de-bias heterogenous testing (8).
The underlying causes of lower testing rates in higher deprivation areas were more rarely addressed. We show that testing rates were associated with socio-demographic profile even after adjusting for pre-pandemic proxies for access to healthcare. Specific COVID-19 testing stations availability contributed to increasing testing availability for nearby vulnerable populations in deprived areas (29, 30). In urban neighborhoods of PACA region, lateral flow device testing became widely available during the “healthpass” period, with a strong incentive to perform tests: this period displayed the narrowest gap between very deprived and privileged areas. However other periods, such as the end of year holiday season, saw testing increase disproportionately among privileged or downtown populations, as reported elsewhere (13, 31).
We initiated this study in support of the regional public health agency of the PACA region (South-Eastern France) during the fourth quarter of 2020 to document the main drivers and inequalities in testing rate in the region and to identify areas with structurally low testing rates. Specific interventions (community engagement, home-visits for testing and supporting isolation efforts…) targeted these areas specifically. The “very deprived” IRIS profile was included as a contextual indicator in addition to weekly epidemic trends to prioritize health mediation interventions deployed by the regional health agency from October 2020 to June 2022 (32). This fine spatial scale local profiling (infra-neighborhood) is now included for general health mediation intervention projects in the city of Marseille.
The data analyzed in this study is subject to the following licenses/restrictions: SARS-CoV-2 testing and positive case data are government public health agency data not available openly. The aggregated data are accessible to researchers upon reasonable request for data sharing to the corresponding author. Requests for data require approval by Santé Publique France. Requests to access these datasets should be directed to am9yZGkubGFuZGllckBpcmQuZnI=.
The studies involving human participants were reviewed and approved by the Aix-Marseille University Ethics Committee (number 2022-10-20-006). Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
JL and JG designed the study with contributions of SR. LB and JL collected and analyzed the data with support of PC, FF, and SN. JL, SR, M-KB, and JG drafted the first version of the manuscript. All authors interpreted the results and contributed to the article and approved the submitted version.
This work was supported by the grant no. 22DIRA41-0 on 28 October 2022 from 2. Santé Publique France (the French National Public Health agency). The funding source had no role in the design, analysis, result interpretation and reporting for this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1162711/full#supplementary-material
1. Diez Roux, AV. Social epidemiology: past, present, and future. Annu Rev Public Health. (2022) 43:79–98. doi: 10.1146/annurev-publhealth-060220-042648
2. Phelan, JC, Link, BG, and Tehranifar, P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Soc Behav. (2010) 51:S28–40. doi: 10.1177/0022146510383498
3. Warszawski, J, Beaumont, AL, Seng, R, De, LX, Rahib, D, Lydié, N, et al. Prevalence of SARS-CoV-2 antibodies and living conditions: the French national random population—based EPICOV cohort. BMC Infect Dis. (2022) 22:1–13. doi: 10.1186/s12879-021-06973-0
4. Pollán, M, Pérez-Gómez, B, Pastor-Barriuso, R, Oteo, J, Hernán, MA, Pérez-Olmeda, M, et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. Lancet. (2020) 396:535–44. doi: 10.1016/S0140-6736(20)31483-5
5. Riou, J, Panczak, R, Althaus, CL, Junker, C, Perisa, D, Schneider, K, et al. Articles socioeconomic position and the COVID-19 care cascade from testing to mortality in Switzerland: a population-based analysis. Lancet Public Heal. (2021) 6:e683–91. doi: 10.1016/S2468-2667(21)00160-2
6. Vandentorren, S, Smaïli, S, Chatignoux, E, Maurel, M, Alleaume, C, Neufcourt, L, et al. Articles the effect of social deprivation on the dynamic of SARS-CoV-2 infection in France: a population-based analysis. Lancet Public Health. (2022) 7:e240–9. doi: 10.1016/S2468-2667(22)00007-X
7. Willeit, P, Krause, R, Lamprecht, B, Berghold, A, Hanson, B, Stelzl, E, et al. Prevalence of RT-qPCR-detected SARS-CoV-2 infection at schools: first results from the Austrian school-SARS-CoV-2 prospective cohort study. Lancet Reg Heal Eur. (2021) 5:100086. doi: 10.1016/j.lanepe.2021.100086
8. Padellini, T, Jersakova, R, Diggle, PJ, Holmes, C, King, RE, and Lehmann, BCL. Time varying association between deprivation, ethnicity and SARS-CoV-2 infections in England: a population-based ecological study. Lancet Reg Heal Eur. (2022) 15:100322. doi: 10.1016/j.lanepe.2022.100322
9. Mena, GE, Mena, GE, Martinez, PP, Mahmud, AS, and Marquet, PA. Socioeconomic status determines COVID-19 incidence and related mortality in Santiago. Chile. (2021) 5298:1–16. doi: 10.1126/science.abg5298
10. Ortiz-Prado, E, Simbaña-Rivera, K, Barreno, LG, Diaz, AM, Barreto, A, Moyano, C, et al. Epidemiological, socio-demographic and clinical features of the early phase of the COVID-19 epidemic in Ecuador. PLoS Negl Trop Dis. (2021) 15:1–18. doi: 10.1371/journal.pntd.0008958
11. Hwang, M-J, Park, SY, Yoon, T-H, Jang, J, Lee, S-Y, Yoo, M, et al. Effect of socioeconomic disparities on the risk of COVID-19 in eight metropolitan cities, the Republic of Korea: a community-based study. Epidemiol Health. (2022) 44:e2022107. doi: 10.4178/epih.e2022107
12. Chung, GKK, Chan, SM, Chan, YH, Woo, J, Wong, H, Wong, SY, et al. Socioeconomic patterns of covid-19 clusters in low-incidence city, Hong Kong. Emerg Infect Dis. (2021) 27:2874–7. doi: 10.3201/eid2711.204840
13. Green, MA, García-Fiñana, M, Barr, B, Burnside, G, Cheyne, CP, Hughes, D, et al. Evaluating social and spatial inequalities of large scale rapid lateral flow SARS-CoV-2 antigen testing in COVID-19 management: an observational study of Liverpool, UK (November 2020 to January 2021). Lancet Reg Heal Eur. (2021) 6:100107. doi: 10.1016/j.lanepe.2021.100107
14. Rey, G, Jougla, E, Fouillet, A, and Hémon, D. Ecological association between a deprivation index and mortality in France over the period 1997–2001: variations with spatial scale, degree of urbanicity, age, gender and cause of death. BMC Public Health. (2009) 9:1–12. doi: 10.1186/1471-2458-9-33
15. Pornet, C, Delpierre, C, Dejardin, O, Grosclaude, P, Launay, L, Guittet, L, et al. Construction of an adaptable European transnational ecological deprivation index: the French version. J Epidemiol Community Heal. (2012) 66:982–9. doi: 10.1136/jech-2011-200311
16. Gaudart, J, Landier, J, Huiart, L, Legendre, E, Lehot, L, Bendiane, MK, et al. Factors associated with the spatial heterogeneity of the first wave of COVID-19 in France: a nationwide geo-epidemiological study. Lancet Public Health. (2021) 6:e222–31. doi: 10.1016/S2468-2667(21)00006-2
17. Lê, S, Josse, J, and Husson, F. FactoMineR: an R package for multivariate analysis. J Stat Softw. (2008) 25:1–18. doi: 10.18637/jss.v025.i01
18. Textor, J, van der Zander, B, Gilthorpe, MS, Liśkiewicz, M, and Ellison, GT. Robust causal inference using directed acyclic graphs: the R package dagitty. Int J Epidemiol. (2016) 45:1887–94. doi: 10.1093/ije/dyw341
19. Wood, SN. Generalized additive models: an introduction with R. 2nd ed. New York: CRC Press and Chapman & Hall (2017).
20. Li, Z, Lewis, B, Berney, K, Hallisey, E, Williams, AM, Whiteman, A, et al. Social vulnerability and rurality associated with higher SARS-CoV-2 infection-induced seroprevalence: a nationwide blood donor study, United States, July 2020–June 2021. Clin Infect Dis. (2022) 75:e133–43. doi: 10.1093/cid/ciac105
21. Ortiz-Prado, E, Henriquez-Trujillo, AR, Rivera-Olivero, IA, Freire-Paspuel, B, Vallejo-Janeta, AP, Lozada, T, et al. Massive SARS-CoV-2 RT-PCR testing on rural communities in Manabi Province (Ecuador) reveals severe COVID-19 outbreaks. Am J Trop Med Hyg. (2021) 104:1493–4. doi: 10.4269/ajtmh.20-1208
22. Saulle, R, Sinopoli, A, De Paula, BA, Mannocci, A, Marino, M, de Belvis, AG, et al. The precede-proceed model as a tool in public health screening: a systematic review. Clin Ter. (2020) 171:E167–77. doi: 10.7417/CT.2020.2208
23. Chorley, AJ, Marlow, LAV, Forster, AS, Haddrell, JB, and Waller, J. Experiences of cervical screening and barriers to participation in the context of an organised programme: a systematic review and thematic synthesis. Psychooncology. (2017) 26:161–72. doi: 10.1002/pon.4126
24. Travert, AS, Annerstedt, K, and Daivadanam, M. Built environment and health behaviors: deconstructing the black box of interactions—a review of reviews. Int J Environ Res Public Health. (2019) 16:1454. doi: 10.3390/ijerph16081454
25. Assari, S, Khoshpouri, P, and Chalian, H. Combined effects of race and socioeconomic status on cancer beliefs, cognitions, and emotions. Healthcare. (2019) 7:30–6. doi: 10.3390/healthcare7010017
26. Milstein, G, Palitsky, R, and Cuevas, A. The religion variable in community health promotion and illness prevention. J Prev Interv Community. (2019) 48:1–6. doi: 10.1080/10852352.2019.1617519
27. Embrett, M, Sim, SM, Caldwell, HAT, Boulos, L, Yu, Z, Agarwal, G, et al. Barriers to and strategies to address COVID-19 testing hesitancy: a rapid scoping review. BMC Public Health. (2022) 22:1–10. doi: 10.1186/s12889-022-13127-7
28. Gaubert, G, Nauleau, S, Franke, F, Rebaudet, S, Mosnier, E, and Landier, J. Deprivation effect on COVID-19 cases incidence and severity: a geo-epidemiological study in PACA region, France. medRxiv (2023) pre-print. doi: 10.1101/2023.04.18.23288723
29. Hernandez, JH, Karletsos, D, Avegno, J, and Reed, CH. Is Covid-19 community level testing effective in reaching at-risk populations? Evidence from spatial analysis of New Orleans patient data at walk-up sites. BMC Public Health. (2021) 21:1–8. doi: 10.1186/s12889-021-10717-9
30. Hendricks, B, Price, BS, Dotson, T, Kimble, W, Davis, S, and Khodaverdi, M. If you build it, will they come? Is test site availability a root cause of geographic disparities in COVID-19 testing? Public Health. (2023) 216:21–6. doi: 10.1016/j.puhe.2022.09.009
31. Dalili, MN, Long, J, Wadley, E, Sloan, J, Cross, A, Thomas, KH, et al. Who is accessing community lateral flow device testing and why? Characteristics and motivations of individuals participating in COVID-19 community testing in two English local authority areas. BMC Public Health. (2022) 22:1–10. doi: 10.1186/s12889-022-12986-4
Keywords: testing, access to health care, deprivation, COVID-19, geoepidemiology, France, population-based
Citation: Landier J, Bassez L, Bendiane M-K, Chaud P, Franke F, Nauleau S, Danjou F, Malfait P, Rebaudet S and Gaudart J (2023) Social deprivation and SARS-CoV-2 testing: a population-based analysis in a highly contrasted southern France region. Front. Public Health 11:1162711. doi: 10.3389/fpubh.2023.1162711
Edited by:
Miguel Angel Garcia Bereguiain, University of the Americas, EcuadorReviewed by:
Esteban Ortiz-Prado, University of the Americas, EcuadorCopyright © 2023 Landier, Bassez, Bendiane, Chaud, Franke, Nauleau, Danjou, Malfait, Rebaudet and Gaudart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jordi Landier, am9yZGkubGFuZGllckBpcmQuZnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.