 Carla Marina Román-Montes1,2
Carla Marina Román-Montes1,2 Yesenia Flores-Soto1
Yesenia Flores-Soto1 Guillermo Arturo Guaracha-Basañez3
Guillermo Arturo Guaracha-Basañez3 Karla María Tamez-Torres1
Karla María Tamez-Torres1 José Sifuentes-Osornio4
José Sifuentes-Osornio4 Ma. Fernanda González-Lara1*
Ma. Fernanda González-Lara1* Alfredo Ponce de León2
Alfredo Ponce de León2- 1Clinical Microbiology Laboratory, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
- 2Infectious Diseases Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
- 3Emergency Department, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
- 4General Direction, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
Introduction: Post-COVID-19 syndrome (PCS) usually occurs 3 months after the onset of COVID-19 with a symptom duration of at least 2 months without an alternative diagnosis.
Objective: This study aimed to describe the prevalence, characteristics, and impact on the quality of life (QoL) of post-COVID-19 syndrome in patients with a history of hospitalization for COVID-19.
Materials and methods: We conducted a cross-sectional study. Patients who required hospitalization due to COVID-19 between March 2020 and October 2021 were invited to answer a PCS questionnaire and the EQ-5D instrument. A total of 246 patients were included: 187 (76%) met the definition of PCS and 54% were men, with a median age of 50 years (IQR 41–63).
Results: From 187 patients with PCS, the median time to symptom onset after hospital discharge was 1 day (IQR 1–20), and the median symptom duration was 150 days (IQR 90–225). A total of 27 different symptoms were reported; the most frequent were difficulty concentrating (81%), dyspnea (75%), arthralgia (71%), fatigue (68%), and hair loss (60%). Some symptoms, such as difficulty concentrating, arthralgia/myalgia, and hair loss, were more prevalent in women with PCS. Patients with PCS had a higher frequency of tobacco smoking (37 vs. 4%, p = 0.02) and increased severity of lung involvement in the initial chest tomography (75 vs. 58%, p = 0.01) than those without PCS. Patients with PCS were less likely to receive antivirals (15.5 vs. 27%, p = 0.04). No difference between ICU admission, mechanical ventilation, and length of hospital stay was found. Patients with PCS had a lower visual analog scale result for EQ-5D vs. those without (80 [IQR 70–90] vs. 89.5 [IQR 75–90], p = 0.05). All five QoL dimensions were affected in PCS patients, showing increased pain/discomfort (67 vs. 39%, p = <0.001), difficulties in performing usual activities (39.2 vs. 20.3%, p = 0.03), and anxiety/depression (57.5 vs. 37%, p = 0.02).
Conclusion: PCS occurred in 76% of hospitalized patients with prolonged duration and QoL impairment. Neurological symptoms such as difficulty concentrating were the most frequent symptoms. Timely diagnostic and therapeutic interventions are required.
Introduction
Coronavirus disease-19 (COVID-19) is still a critical comorbidity and mortality cause worldwide. SARS-CoV-2 infection no longer carries the same risks of adverse outcomes as it did in the early months of the pandemic because of the vaccines and the new subvariants of SARS-CoV-2 with a diverse rate of transmission and virulence (1). Post-COVID-19 syndrome (PCS) was defined by the World Health Organization (WHO) in late 2021 as symptoms occurring in individuals within 3 months of a history of probable or confirmed SARS-CoV-2 infection, with at least 2 months that cannot be explained by an alternative diagnosis (2). Common symptoms of PCS include shortness of breath, fatigue, difficulty thinking or concentrating (referred to as “brain fog”), changes in smell and taste, sleep problems, and hair loss. Before this definition, different terms such as long COVID syndrome, persistent post-COVID syndrome, and post-acute COVID-19 syndrome were used. Symptoms may be new onset following initial recovery or persistent since the initial COVID-19 episode. Symptoms may also fluctuate or relapse over time.
A meta-analysis reported a high prevalence of up to 80% (95% CI 65–92%) (3). Other cohorts report a lower prevalence, such as 32.6% in Michigan, USA, with limitations such as the study date and lack of PCS definition (4). Another study in Wuhan, China, using questionnaires, physical examination, 6-min walk tests (6MWT), laboratory tests, pulmonary function tests (PFTs), and high-resolution computed tomography described that 76% had at least one symptom. Lopez-León et al. described more than 50 symptoms as part of PCS; among them, the most frequent were fatigue (58%), headache (44%), attention disorder (27%), hair loss (25%), and dyspnea (24%) (3, 5). Other reviews and meta-analyses in the UK also found fatigue (37%) as the most prevalent, followed by dyspnea (6).
The quality of life (QoL) definition encompasses individual perceptions of their position in life in the context of the culture and value systems concerning goals, expectations, standards, and worries (7). Hence, QoL is used as a general predictor of health and is essential to understand the repercussions of COVID-19 on physical health status, social restrictions, and psychological states. Several tools measure the QoL; some are generic, such as SF-36 (36-item Short-Form Health Survey) and EQ-5D (EuroQol-5 Dimension), and they are used to assess multiple domains of the health and wellbeing of the patient. Specific tools are also used in diseases such as rheumatoid arthritis and metabolic disorders (8).
In other pandemic scenarios, such as influenza, QoL impairment was described (9). After the COVID-19 pandemic, it has been published that survivors' QoL is generally affected, particularly in patients with PCS (10–12).
In this study, we aimed to describe the prevalence of PCS, the frequency of symptoms, and the impact on the QoL of patients with an initial episode of severe or critical COVID-19.
Methods
Patients and data collection
A retrospective, cross-sectional study was done. We found 1,379 patients ≥18 years of age hospitalized with COVID-19 between 1st July 2020 and 31st December 2021. Among these, 317 who had been hospitalized 3, 6, 9, and 12 months before were randomly selected and invited to answer an adapted questionnaire to identify the presence of PCS and EQ-5D. Among 312 patients who were invited to participate, only 246 patients were included who then answered both the questionnaires (Figure 1).
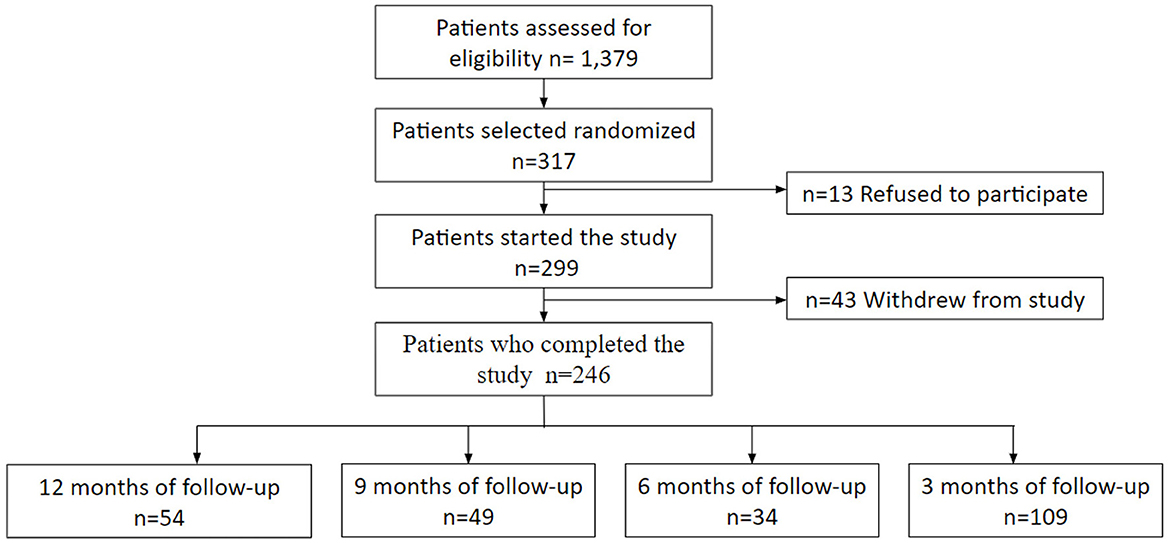
Figure 1. Pacients flowchart. Comments: Patients assessed for eligibility were patients who were hospitalized in the chosen period and who were discharged home.
Research tools and instruments
The content of the PCS questionnaire was adapted from the questionnaire used by Huang et al. on a group of Chinese patients in 2020. A committee comprising a rheumatologist and an infectious diseases specialist performed a translation and adaptation to suit Mexican patients from the original version. The latter is a questionnaire that has been validated in multiple populations worldwide and showed good psychometric properties in Mexico (13); the first part is a visual analog scale, and the second part corresponds to five domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, with three possible response options: no problems, some problems, or extreme problems. The visual analog scale was reported as 0–100, where 0 represents the worst imaginable health and 100 the best imaginable health; the five domains were dichotomized into not affected (answer “no problems”) and affected (answers “some problems,” or “extreme problems”) (14). All reported symptoms, duration, and impact on QoL were recorded.
Definitions
The WHO definition of PCS was used to classify patients into two groups: PCS and no-PCS for comparison (2). Regarding COVID-19 acute episode characteristics, we described severity using the NIH classification. We also describe the clinical, laboratory, and computed tomography (CT) characteristics and the treatment received. Definitions of the compatible or indeterminate chest CT were according to the Radiology Society of North America Expert Consensus (15). In the vaccination record, we considered only those who had a first full scheme before the COVID-19 episode.
Statistics
Sample size calculation estimated 246 subjects considering a prevalence of 80% (2). All analyses were performed in STATA v 14.0 (StataCorp., College Station, TX, USA). Baseline characteristics are reported with descriptive non-parametric statistics, bivariate comparisons were made with the X2 test, Student's T-test, or Mann–Whitney's U-test, as appropriate, and a two-tailed p-value of < 0.05 was considered significant.
Ethics
The protocol was approved by the local research and ethics committee (Local Ref Nr. 3692). Participants' data privacy was preserved during the study. Digital informed consent was signed and kept for record.
Results
The prevalence of PCS in hospitalized patients with severe or critical COVID-19 was 76% (n = 187). Table 1 shows the demographic and clinical characteristics of the initial COVID-19 episode among groups. Patients with PCS had a median age of 55 years (IQR 41–63), and 54% (n = 101) were men. We found no statistical differences in obesity and overweight in both groups, and BMI at the time of acute COVID-19 was a median of 27.74 kg/m2 (IQR 25.31–32.39) vs. 29.41 kg/m2 (IQR 26.12–34.6). Smoking was more frequently reported in the PCS group (19.7 vs. 6.7%, RR 1.23; 95% CI 1.08–1.40, p = 0.02). Other comorbidities were not statistically different between the groups.
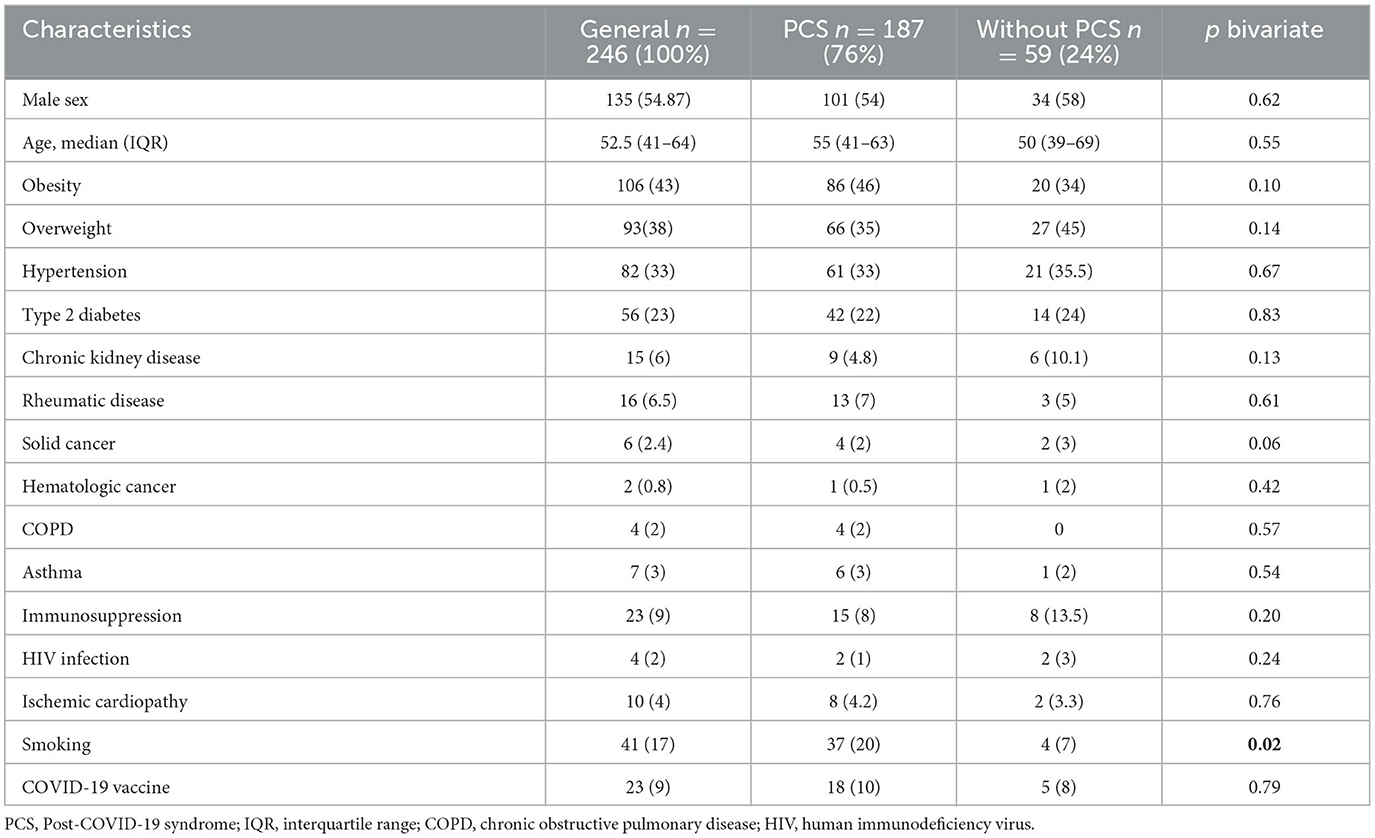
Table 1. Demographic and clinical characteristics of patients with and without post-COVID-19 syndrome.
Table 2 shows the characteristics of the index hospitalization. More than 90% in both groups had a chest CT scan compatible with COVID-19 (PCS 97% (181/187) vs. without PCS 92% (54/59), p = 0.08). The remaining percentage in both groups was described as indeterminate for COVID-19.
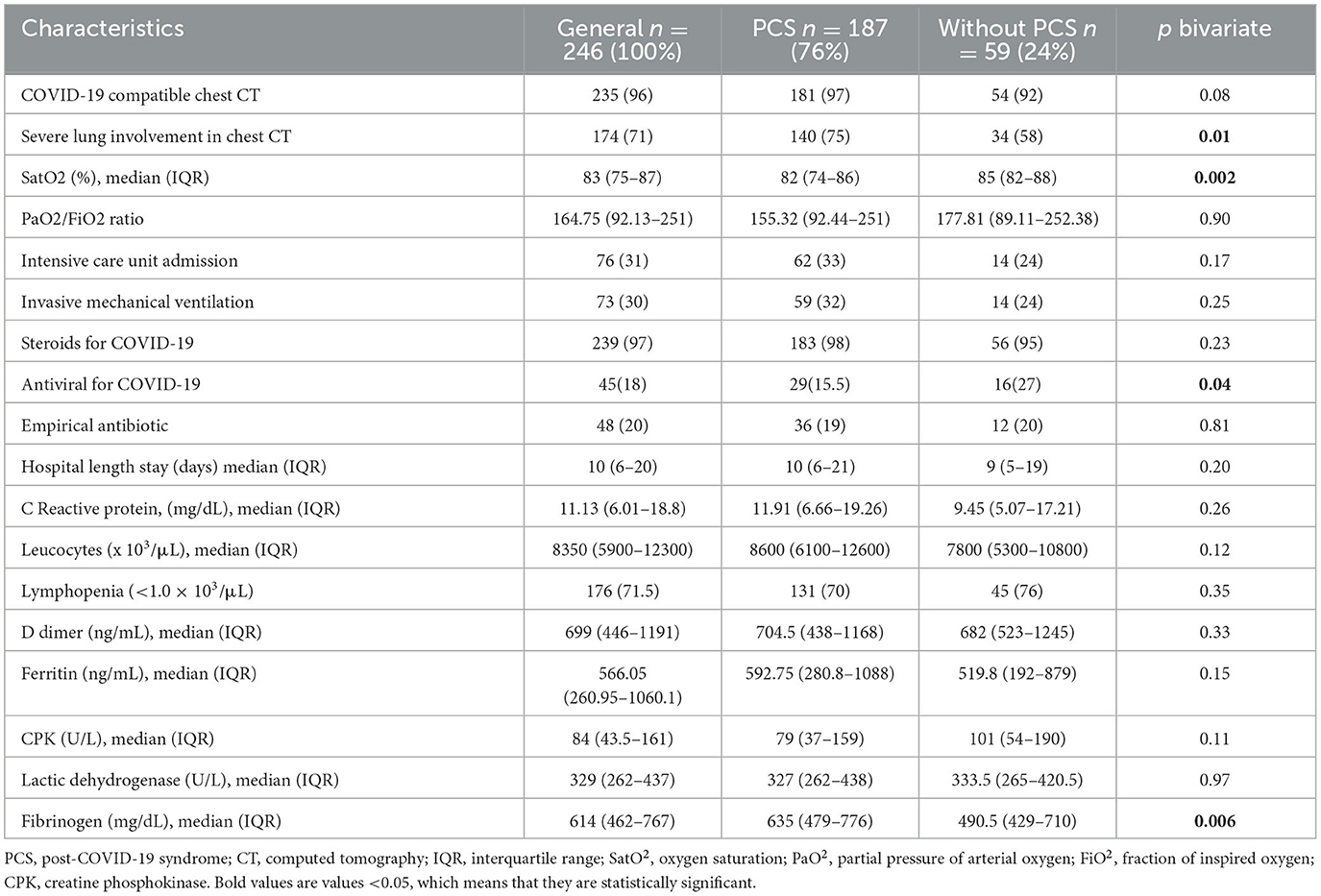
Table 2. Index hospitalization for COVID-19 among patients with and without PCS.
During the initial episode of COVID-19, PCS patients had low room air SatO2 levels (oxygen saturation) (82% IQR 74–86 vs. 85% IQR 82–88, p = 0.002), and their chest CT scans had severe lung involvement more frequently (75 vs. 58%, p = 0.01). Furthermore, 97% (182/187) of PCS patients had severe COVID-19 as per NIH classification; 33% (n = 62) of patients in the PCS group were admitted to the intensive care unit (ICU), and 32% (n = 59) required mechanical ventilation at any time during their hospitalization, with no statistical differences between groups.
The most frequent symptoms of PCS were difficulty concentrating in 81% (n = 152), dyspnea in 75% (n = 141), arthralgias in 71% (n = 132), weakness in 69.5% (n = 130), fatigue in 68% (n = 127), hair loss in 60% (n = 112), myalgia in 53% (n = 99), sleep disturbances in 52% (n = 97), dizziness in 47% (n = 88), and palpitations in 41% (n = 76). A total of 27 different symptoms were described. We decided to classify them into clusters by system (Figure 2). The median time between hospital discharge and symptom onset was 1 day (IQR 1–20 days), and the median symptom duration was 150 days (IQR 90–225 days). When comparing smoking with respiratory symptoms such as dyspnea, we do not find differences, and only 18% of patients with dyspnea are smokers (p = 0.42). Among female patients with PCS, difficulty concentrating (87 vs. 76%, p = 0.05), arthralgias (79 vs.63%, p = 0.02), hair loss (82.5 vs. 40%, p ≤ 0.0001), myalgia (63 vs. 44.5%, p = 0.01), and dizziness (56 vs. 39%, p = 0.02) were more frequent compared to their male counterparts (Table 3).
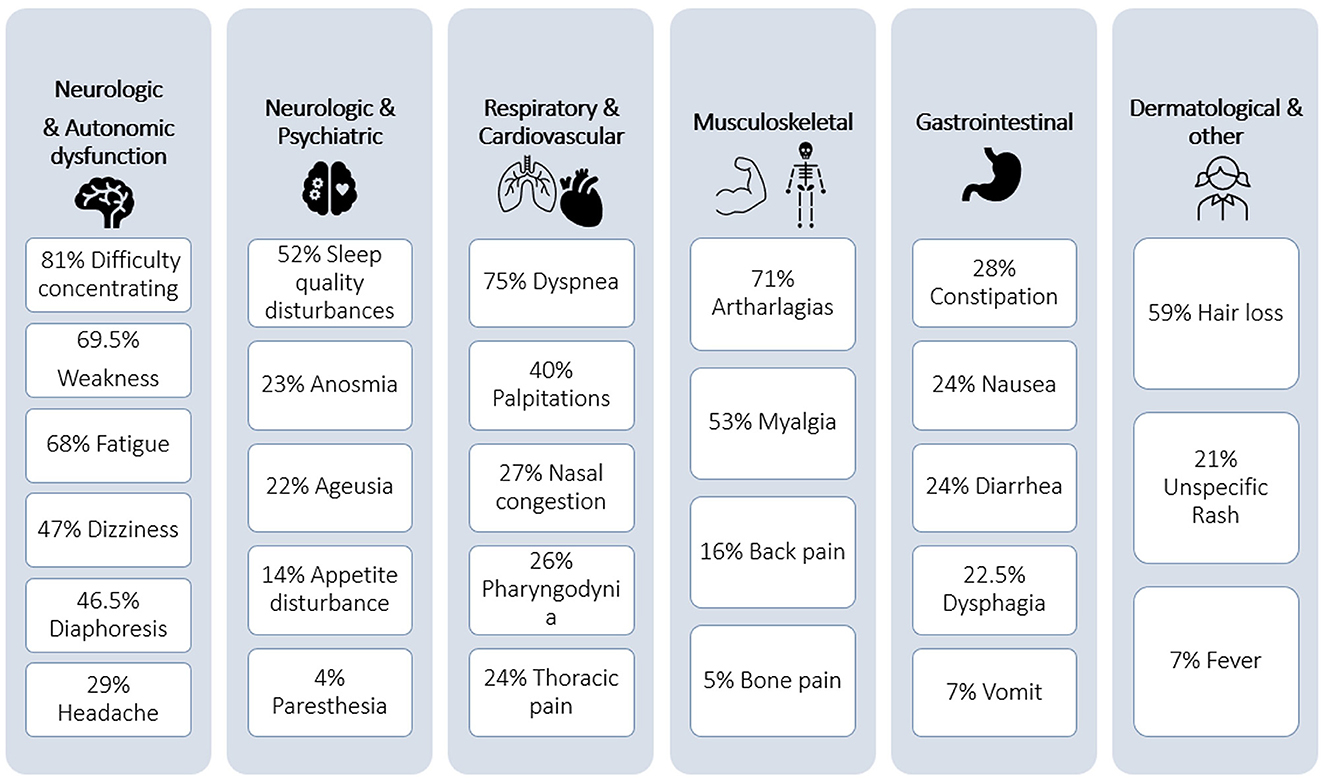
Figure 2. Symptoms in post-COVID-19 syndrome classify into clusters.
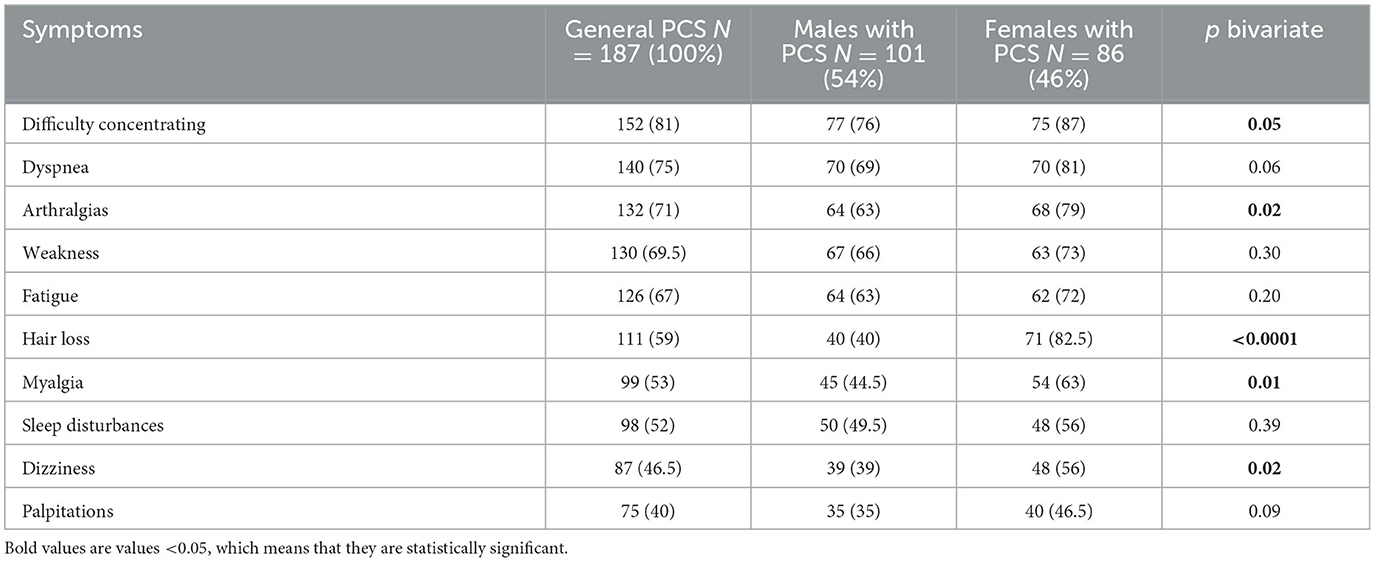
Table 3. Frequency and differences of PCS symptoms between men and women.
Regarding health status and QoL, 63% (n = 117) of PCS patients described their health status as “worse” than before COVID-19 (OR 9.2, 95% CI 4.1–22.6, p ≤ 0.0001). In the EQ-5D instrument, we found disturbances in all five domains; the pain and discomfort domain was the most affected in PCS at 65.5 vs. 39% without PCS (p < 0.001). Also, patients with PCS were referred to a worse QoL (visual analog scale) compared to those without PCS [80 IQR (70–90) vs. 89.5 (75–90), p = 0.05]. Affected domains are described in Table 4 and Figure 3.
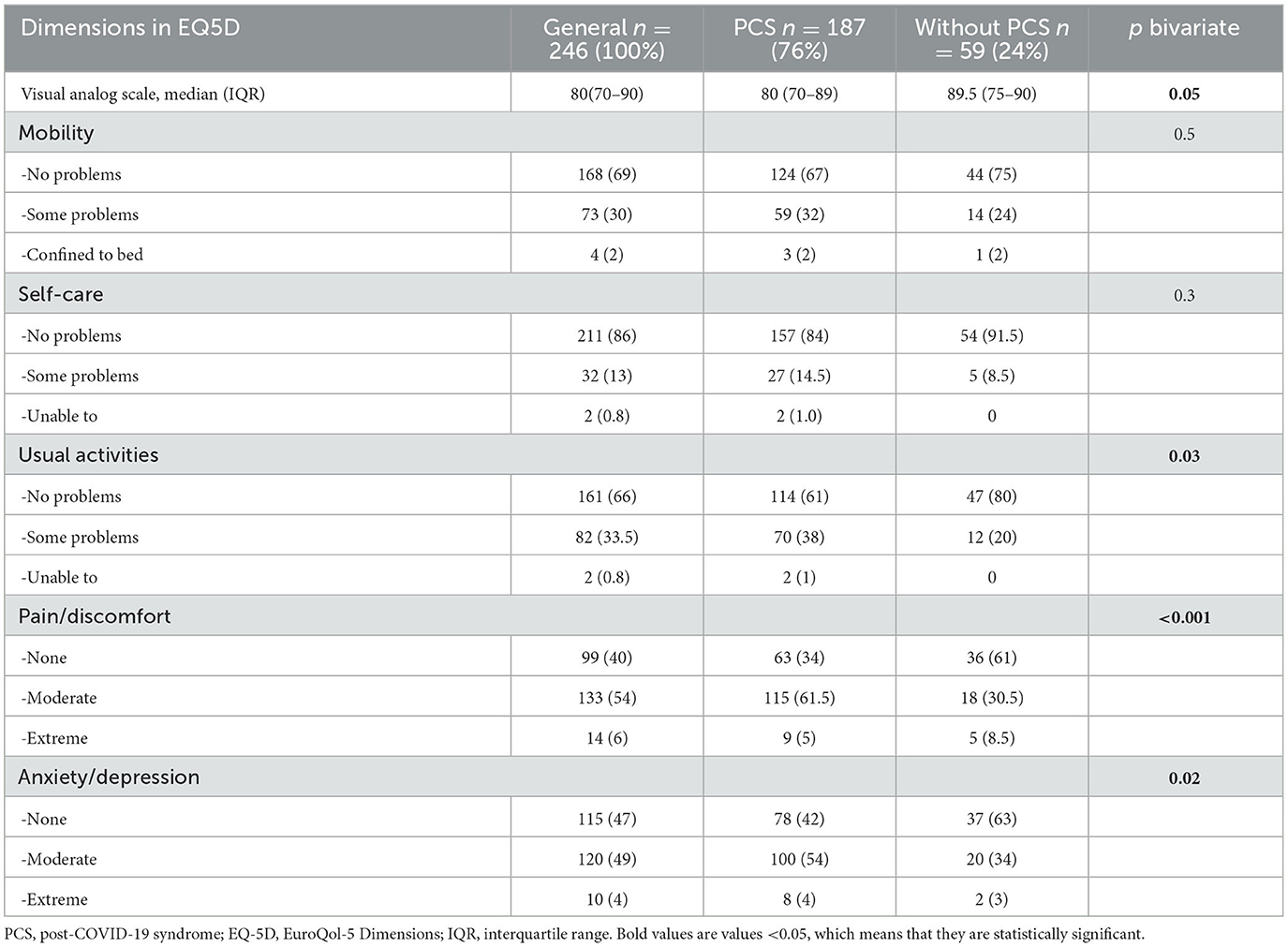
Table 4. Distribution of the VAS and dimensions of the EQ-5D among patients with and without PCS.
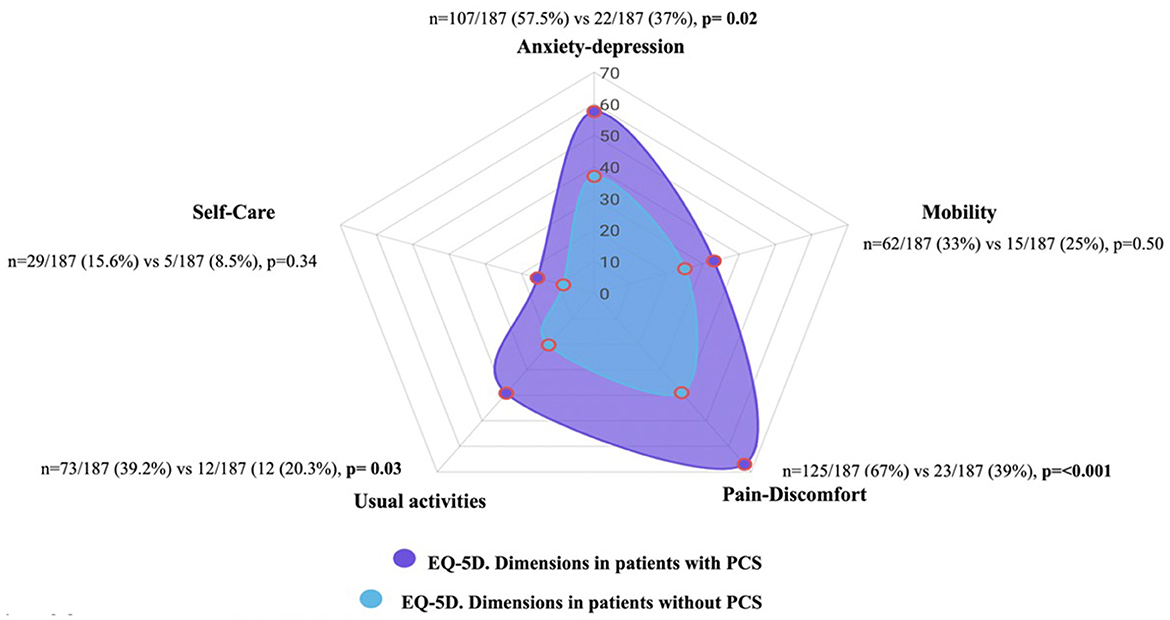
Figure 3. Distribution of the dimensions affected in EQ-5D.
Discussion
We found a 76% prevalence of post-COVID-19 syndrome in patients hospitalized for severe or critical SARS-CoV-2 infection. This rate is comparable to a systematic review describing over 50 symptoms but lower. Of note, the WHO definition we used had not been published at that time (2, 3). The definition used in the systematic review considered symptoms, signs, or abnormal clinical parameters persisting 2 or more weeks after COVID-19 onset that do not return to a healthy baseline; but given our prevalence, the defining factor does not have much impact. According to the literature, the prevalence of PCS ranges between 5 and 50%. Some extensive surveys describe a prevalence of 39%, including infections by different SARS-CoV-2 variants (16). Therefore, the variability is due to various factors: the definition of PCS, the hospitalized and non-hospitalized population, the variants, and even other additional factors such as vaccination or the treatments received.
In addition, we found 27 different symptoms as well as slightly more than half of those described in other research may be due to the strategies of searching for or questioning the presence of symptoms; the questionnaire and the interview strategy can influence the finding of more or fewer symptoms.
A few publications on PCS prevalence in Mexico were found. In a study from Guanajuato, Mexico, Muñoz-Corona et al. reported 75.9% of persistent symptoms in COVID-19 patients at 90 days of hospital discharge (17). In a study from Zacatecas, Mexico, long-term symptoms were found in 85% of patients; however, it was carried out in 2020 with a different PCS definition (18).
Some studies have associated older age and women with a higher risk for PCS (19, 20), but we did not find significant differences in age between groups nor in the proportion between sexes; this last finding may be associated with our hospitalized cohort comprising more men, with the male sex being at higher risk of severe COVID-19. However, we found some differences in the frequency of symptoms according to sex; difficulty concentrating, arthralgia, myalgia, dizziness, and hair loss are more frequent and with statistical significance in women. Fernandez DPC et al. also described that some PCS symptoms are more frequent in women such as fatigue, dyspnea, hair loss, ocular problems, depression, and poor sleep quality (20).
Fatigue is one of the predominant symptoms in PCS (21); however, respiratory manifestations, such as dyspnea, persistent cough, and chest pain, remain frequent and presumably associated with the lungs as the primary site of infection (3). Our patients referred to difficulties with concentration and attention, the so-called “brain fog,” as the main neurological complaint, with a higher than reported frequency. This has been linked to direct viral damage to the limbic system after entering through the nasal sensory cells (22). Other theories explaining cognitive abnormalities include direct neuronal infection and autoimmune/inflammatory CSF and brain tissue abnormalities (23). Ongoing studies, at our institution, found a prevalence of psychopathological PCS manifestations, memory complaint, and mild cognitive impairment a year after the acute COVID-19 episode, in 42, 45, and 30%, respectively (unpublished data, personal communication from Flores-Silva F.) The frequency of neurological symptoms during acute COVID-19 might explain the high prevalence of these symptoms. Another study from our center found that up to 65% of patients hospitalized for COVID-19 had neurological symptoms on admission, and 15% developed some neurological event, such as seizures, delirium, altered alertness, or weakness during hospitalization (24). Moreover, Wong-Chew et al. showed that the most frequent post-COVID-19 symptoms were neurological (25).
Interestingly, some overlapping with the ME/CFS (myalgic encephalomyelitis/chronic fatigue syndrome) pathogenesis has been found. Other hypotheses explaining PCS vary from changes in host-microbiome diversity leading to dysbiosis and persistent autoimmune or inflammatory stimuli, the persistence of viral reservoirs in specific tissues, alterations in the coagulation cascade, or a complex combination of multiple mechanisms (26).
In our study, any degree of hair loss was reported by 60% of PCS patients. The most accepted mechanism for alopecia is telogen effluvium (TE), which is associated with systemic stress, although other mechanisms have been described (27). It has been reported in different proportions in post-COVID patients, and some studies report a higher prevalence in women than in men, as we found, even in the sequelae initially described in patients from Wuhan, China, at the beginning of the pandemic (28, 29). Of note, arthralgias and myalgias were frequent. A physical examination and inflammatory marker determination would clarify whether arthritis occurs as a PCS manifestation or whether another condition may be unmasked. The descriptive nature of this study is a major limitation.
Our patients with PCS reported smoking more frequently, which has been described in a study from France, where smoking was the main factor associated with tachycardia or hypertension 2 months post-COVID-19 (30). Studies from the UK and Turkey found smoking was more frequently reported in patients with post-COVID-19 symptoms (31, 32). These findings underscore the importance of focusing on strategies to quit tobacco consumption among vulnerable patients as a measure to reduce PCS.
We did not find other previously described differences between groups, such as female sex, obesity, or older age. However, this study involved more than 600,000 people and included both hospitalized and outpatients, perhaps leading to a mix in various extents of viral damage, symptom duration, and baseline clinical features (31).
Regarding COVID-19 vaccination, we found no differences between our groups. However, the proportion of vaccinated patients was small at the time of the study. A systematic review by Notarte et al. (33) showed a reduction of PCS after vaccination, although this finding remains controversial with a lack of evidence to make conclusions.
A high proportion of our patients with PCS had a severe acute COVID-19 episode, although ICU stay was not associated with increased PCS. This has been inconsistently seen in studies. Kamal et al. observed that the severity of COVID-19 was related to post-COVID-19 manifestations, although 80% of patients with PCS had mild COVID-19 (5, 34, 35).
The only inflammatory marker that we found associated with PCS was a higher fibrinogen level. Fibrin amyloid micro-clotting and platelet dysfunction have been demonstrated in PCS models, unveiling a possible association between coagulation dysregulation and chronic COVID-19 symptoms (36).
A much-anticipated effect of antivirals, such as remdesivir, is the ability to protect from or ameliorate symptoms of PCS. A prospective cohort showed a 35.9% reduction of PCS at a 6-month follow-up in patients receiving remdesivir (37). Antivirals may halt the cytokine response and inflammatory cascade that activate clotting and fibrosing factors playing a role in the pathogenesis of PCS. In addition, tissue damage inflicted by SARS-CoV-2 has been linked to chronic sequelae and manifestations of organ dysfunction even months after resolution (26).
Quality of life was significantly affected in patients with PCS. This finding is consistent with Muñoz-Corona et al., who found that 75.9% of PCS patients had the lowest scores in the roles of physical dimension and general health dimension (SF-36 questionnaire) studied 90 days after discharge (17); Tobada et al. showed a decrease in QoL measured with the EQ-5D 6 months after the acute infection with moderate-to-severe disturbances in the following domains: 56% in mobility, 48% in pain/discomfort, 46% in anxiety/depression, 37% in usual activities, and 13% in self-care; these findings are similar to ours (38). In addition, a systematic review confirmed that QoL in PCS patients was significantly affected, regardless of time elapsed since discharge or recovery, although the tools applied to measure QoL were heterogeneous (39, 40). Thiolliere et al. (41) compared the QoL of older patients with COVID-19 who required ICU with other ICU patients and found no differences between the EQ-5D scores or autonomy at day 180. This finding supports that in older people, the deterioration of QoL is more likely linked to the infection per se and not to the ICU stay (41).
Our study has various limitations: The cross-sectional design does not allow for follow-up data at different times. However, the survey was conducted at different times after the acute COVID-19 episodes. Although memory bias was likely present, the survey strategy was the most efficacious approach to surpass the decline in COVID-19 cases over time, for reasons such as the circulation of variants and the current use of vaccines. In addition, none of the patients had a QoL assessment before their acute COVID-19, so direct comparisons cannot establish a strong causal relationship with SARS-CoV-2 infection. On the other hand, the patient's clinical characteristics and comorbidities were fully analyzable, which gives our results and study strength when compared with other works. Finally, a prospective approach with clinical evaluation and intervention is undoubtedly required for these patients, from the moment they are diagnosed with COVID-19, to assess the development of PCS. We consider the descriptive nature of our approach to be a limitation since we did not have any studies or interventions in those who had PCS. During the pandemic, our institution focused solely on caring for patients with COVID-19. However, due to these findings, we are currently developing multidisciplinary care for patients with PCS.
Regarding the diagnosis and management of PCS, it took not long for the scientific community to understand the complexity of PCS. Thus, since early 2021, several multidisciplinary programs and ambulatory rehabilitation clinics and projects have been launched, whether virtual or hybrid, to be able to cope with this ever-growing population. Diagnostic criteria have been set through a Delphi consensus (2). However, treatment strategies are still under investigation, mainly to ascertain the best type and duration of therapy necessary for a patient suffering from PCS to restore health and QoL (42).
Although in the future, the prevalence and severity of PCS will be modified by factors such as more robust vaccination schemes, antivirals, or anticoagulants. Furthermore, infections with new viral strains and host-derived factors may impact PCS incidence (43). Comprehensive multidisciplinary studies are needed to set the ground for better understanding and managing this disease.
Conclusion
A high prevalence of PCS in previously hospitalized patients with COVID-19 was found. Smoking, severe COVID-19, lower SatO2 on admission, increased lung involvement, and elevated fibrinogen levels were associated with increased frequency of PCS. Some symptoms, such as difficulty concentrating, arthralgia/myalgia, and hair loss, were more prevalent in women with PCS. A significant QoL impairment was evident in PCS.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics and Research Committee, Instituto Nacional de Ciencias Médicas y Nutrición “Salvador Zubirán”. The patients/participants provided their written informed consent to participate in this study.
Author contributions
YF-S conducted the surveys. CR-M, YF-S, and GG-B performed the clinical data search and capture. CR-M, YF-S, GG-B, KT-T, and MG-L aided in interpreting the results and worked on the manuscript. All authors discussed the results and commented on the manuscript. MG-L, JS-O, and AL supervised the research, provided critical feedback, and helped shape the research, analysis, and manuscript. All authors participated in the idea, general objectives, and design of the study.
Acknowledgments
The authors want to acknowledge the patients who responded to the survey and all the medical and paramedical personnel working at our institution, involved in the care of patients with COVID-19 since February 2020; without your valuable presence, none of these data would be available. Thank you.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. El-Sadr WM, Vasan A, El-Mohandes A. Facing the New Covid-19 Reality. N Engl J Med. (2023) 388:385–7. doi: 10.1056/NEJMp2213920
2. Organisation WH. A clinical case definition of post COVID-19 condition by a Delphi consensus data. (2021). Available online at: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed December 23, 2021).
3. Leon SL, Ostrosky TW, Perelman C, Sepulveda R, Rebolledo PA, Cuapio A, et al. More than 50 long - term effects of COVID - 19 : a systematic review and meta - analysis Middle East respiratory syndrome. Nat Sci Reports. (2021) 11:1–12. doi: 10.1038/s41598-021-95565-8
4. Among SO, Hospitalized P. Sixty-day outcomes among patients hospitalized with. Ann Intern Med Med. (2022) 174:2021–3. doi: 10.7326/M20-5661
5. Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. (2021) 397:220–32. doi: 10.1016/S0140-6736(20)32656-8
6. Healey Q, Sheikh A, Daines L, Vasileiou E. Symptoms and signs of long COVID: A rapid review and meta-analysis. J Glob Health. (2022) 12:5014. doi: 10.7189/jogh.12.05014
7. The WHOQOL Group. WHO Quality of Life Scale (WHOQOL). Psychol Med. (1998) 28:551–8. doi: 10.1017/S0033291798006667
8. Pequeno N, Cabral N, Marchioni D, Lima S, Lyra C. Quality of life assessment instruments for adults: a systematic review of population-based studies. Health Qual Life Outcomes. (2020) 18:1–13. doi: 10.1186/s12955-020-01347-7
9. Hollmann M, Garin O, Galante M, Ferrer M, Dominguez A, Alonso J. Impact of Influenza on Health-Related Quality of Life among Confirmed (H1N1)2009 Patients. PLoS ONE. (2013) 8:1–10. doi: 10.1371/journal.pone.0060477
10. Amdal CD, Pe M, Falk RS, Piccinin C, Bottomley A, Arraras JI, et al. Health-related quality of life issues, including symptoms, in patients with active COVID-19 or post COVID-19; a systematic literature review. Qual Life Res. (2021) 30:3367–81. doi: 10.1007/s11136-021-02908-z
11. Lapin B, Katzan IL. Health-related quality of life mildly affected following COVID-19: a retrospective pre-post cohort study with a propensity score–matched control group. J Gen Intern Med. (2022) 37:862–9. doi: 10.1007/s11606-021-07340-0
12. Poudel AN, Zhu S, Cooper N, Roderick P, Alwan N, Tarrant C, et al. Impact of Covid-19 on health-related quality of life of patients: A structured review. PLoS ONE. (2021) 16:1–20. doi: 10.1371/journal.pone.0259164
13. Gutierrez-Delgado C, Galindo-Suárez RM, Cruz-Santiago C, Shah K, Papadimitropoulos M, Feng Y, et al. EQ-5D-5L Health-State Values for the Mexican Populaton.pdf. Appl Health Econ Health Policy. (2021) 19:905–14. doi: 10.1007/s40258-021-00658-0
14. Group TE. EuroQol - a new facility for the measurement of health-related quality of life. Health Policy (New York). (1990) 16:199–208. doi: 10.1016/0168-8510(90)90421-9
15. Simpson S, Kay FU, Abbara S, Bhalla S, Chung JH, Chung M, et al. Radiological society of North America expert consensus document on reporting chest CT findings related to COVID-19: Endorsed by the society of thoracic radiology, the American college of radiology, and RSNA. Radiol Cardiothorac Imaging. (2020) 2:e200152. doi: 10.1148/ryct.2020200152
16. Perlis RH, Santillana M, Ognyanova K, Green J, Druckman J, Lazer D, et al. Factors associated with self-reported symptoms of depression among adults with and without a previous COVID-19 diagnosis. JAMA Netw Open. (2021) 4:9–12. doi: 10.1001/jamanetworkopen.2021.16612
17. Muñoz-Corona C, Gutiérrez-Canales LG, Ortiz-Ledesma C, Martínez-Navarro LJ, Macías AE, Scavo-Montes DA, et al. Quality of life and persistence of COVID-19 symptoms 90 days after hospital discharge. J Int Med Res. (2022) 50:03000605221110492. doi: 10.1177/03000605221110492
18. Galván-Tejada CE, Herrera-García CF, Godina-González S, Villagrana-Bañuelos KE, Amaro JDDL, Herrera-García K, et al. Persistence of covid-19 symptoms after recovery in mexican population. Int J Environ Res Public Health. (2020) 17:1–12. doi: 10.3390/ijerph17249367
19. Sugiyama A, Miwata K, Kitahara Y, Okimoto M, Abe KEB, et al. Long COVID occurrence in COVID-19 survivors. Sci Rep. (2022) 12:1–11. doi: 10.1038/s41598-022-10051-z
20. Fernández-De-las-peñas C, Martín-Guerrero JD, Pellicer-Valero ÓJ, Navarro-Pardo E, Gómez-Mayordomo V, Cuadrado ML, et al. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J Clin Med. (2022) 11:1–10. doi: 10.3390/jcm11020413
21. Crook H, Raza S, Nowell J, Young M, Edison P. Long covid - Mechanisms, risk factors, and management. BMJ. (2021) 374:1–18. doi: 10.1136/bmj.n1648
22. Meinhardt J, Radke J, Dittmayer C, Franz J, Thomas C, Mothes R, et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat Neurosci. (2021) 24:168–75. doi: 10.1101/2020.06.04.135012
23. Del Brutto OH. Cognitive sequelae of COVID-19, a post-pandemic threat: Should we be worried about the brain fog? Arq Neuropsiquiatr. (2022) 80:215–6. doi: 10.1590/0004-282x-anp-2022-e003
24. Flores-Silva FD, García-Grimshaw M, Valdés-Ferrer SI, Vigueras-Hernández AP, Domínguez-Moreno R, Tristán-Samaniego DP, et al. Neurologic manifestations in hospitalized patients with COVID-19 in Mexico City. PLoS ONE. (2021) 16:1–12. doi: 10.1371/journal.pone.0247433
25. Wong-Chew RM, Rodríguez Cabrera EX, Rodríguez Valdez CA, Lomelin-Gascon J, Morales-Juárez L, de la Cerda ML, et al. Symptom cluster analysis of long COVID-19 in patients discharged from the Temporary COVID-19 Hospital in Mexico City. Ther Adv Infect Dis. (2022) 9:1–17. doi: 10.1177/20499361211069264
26. Proal AD, VanElzakker MB. Long COVID or Post-acute Sequelae of COVID-19 (PASC): an overview of biological factors that may contribute to persistent symptoms. Front Microbiol. (2021) 12:1–24. doi: 10.3389/fmicb.2021.698169
27. Ohyama M, Matsudo K, Fujita T. Management of hair loss after severe acute respiratory syndrome coronavirus 2 infection: Insight into the pathophysiology with implication for better management. J Dermatol. (2022) 49:939–47. doi: 10.1111/1346-8138.16475
28. Xiong Q, Xu M, Li J, Liu Y, Zhang J, Xu Y, et al. Clinical sequelae of COVID-19 survivors in Wuhan, China: a single-centre longitudinal study. Clin Microbiol Infect. (2021) 27:89–95. doi: 10.1016/j.cmi.2020.09.023
29. Seyfi S, Alijanpour R, Aryanian Z, Ezoji K, Mahmoudi M. Prevalence of telogen effluvium hair loss in COVID-19 patients and its relationship with disease severity. J Med Life. (2022) 15:631–4. doi: 10.25122/jml-2021-0380
30. Barthélémy H, Mougenot E, Duracinsky M, Salmon-Ceron D, Bonini J, Péretz F, et al. Smoking increases the risk of post-acute COVID-19 syndrome: Results from a French community-based survey. Tob Induc Dis. (2022) 20:1–10. doi: 10.18332/tid/150295
31. Whitaker M, Elliott J, Chadeau-Hyam M, Riley S, Darzi A, Cooke G, et al. Persistent COVID-19 symptoms in a community study of 606,434 people in England. Nat Commun. (2022) 13:1–10. doi: 10.1038/s41467-022-29521-z
32. Emecen AN, Keskin S, Turunc O, Suner AF, Siyve N, Basoglu Sensoy E, et al. The presence of symptoms within 6 months after COVID-19: a single-center longitudinal study. Ir J Med Sci. (2022) 192:741–50. doi: 10.1007/s11845-022-03072-0
33. Notarte KI, Catahay JA, Velasco JV, Pastrana A, Ver AT, Pangilinan FC, et al. Impact of COVID-19 vaccination on the risk of developing long-COVID and on existing long-COVID symptoms: A systematic review. eClinicalMedicine. (2022) 53:1–19. doi: 10.1016/j.eclinm.2022.101624
34. Kamal M, Abo Omirah M, Hussein A, Saeed H. Assessment and characterisation of post-COVID-19 manifestations. Int J Clin Pract. (2021) 75:1–5. doi: 10.1111/ijcp.13746
35. Peghin M, Palese A, Venturini M, Martino M De, Gerussi V, Graziano E, et al. Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin Microbiol Infect. (2021) 27:1507–13. doi: 10.1016/j.cmi.2021.05.033
36. Pretorius E, Vlok M, Venter C, Bezuidenhout JA, Laubscher GJ, Steenkamp J, et al. Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol. (2021) 20:1–18. doi: 10.1186/s12933-021-01359-7
37. Boglione L, Meli G, Poletti F, Rostagno R, Moglia R, Cantone M, et al. Risk factors and incidence of long-COVID syndrome in hospitalized patients: does remdesivir have a protective effect? QJM. (2022) 114:865–71. doi: 10.1093/qjmed/hcab297
38. Taboada M, Moreno E, Pita-romero R, Leal S, Sanduende Y, Rodri A, et al. Quality of life, functional status, and persistent symptoms after intensive care of COVID-19 patients. Br J Anaesth. (2020) 126:e110–3. doi: 10.1016/j.bja.2020.12.007
39. Jacobs LG, Paleoudis EG, Bari DL Di, Nyirenda T, Friedman T, Gupta A, et al. Persistence of symptoms and quality of life at 35 days after hospitalization for COVID-19 infection. PLoS ONE. (2020) 15:1–14. doi: 10.1371/journal.pone.0243882
40. Nandasena HMRKG, Pathirathna ML, Atapattu AMMP, Prasanga PTS. Quality of life of COVID 19 patients after discharge: Systematic review. PLoS ONE. (2022) 17:1–12. doi: 10.1371/journal.pone.0263941
41. Thiolliere F, Falandry C, Allaouchiche B, Geoffray V, Bitker L, Reignier J, et al. Intensive care-related loss of quality of life and autonomy at 6 months post-discharge: Does COVID-19 really make things worse? Crit Care. (2022) 26:1–8. doi: 10.1186/s13054-022-03958-6
42. Vance H, Maslach A, Stoneman E, Harmes K, Ransom A, Seagly K, et al. Addressing post-COVID symptoms: A guide for primary care physicians. J Am Board Fam Med. (2021) 36:1229–42. doi: 10.3122/jabfm.2021.06.210254
Keywords: post-COVID-19 syndrome, long-COVID-19, quality of life, chronic COVID-19 syndrome, severe COVID-19, Mexican
Citation: Román-Montes CM, Flores-Soto Y, Guaracha-Basañez GA, Tamez-Torres KM, Sifuentes-Osornio J, González-Lara MF and León APd (2023) Post-COVID-19 syndrome and quality of life impairment in severe COVID-19 Mexican patients. Front. Public Health 11:1155951. doi: 10.3389/fpubh.2023.1155951
Received: 01 February 2023; Accepted: 14 April 2023;
Published: 15 May 2023.
Edited by:
Vanesa Vicens-Zygmunt, Bellvitge University Hospital, SpainReviewed by:
Seyed Morteza Tayebi, Allameh Tabataba'i University, IranFilippo Gozzi, University Hospital of Modena, Italy
Copyright © 2023 Román-Montes, Flores-Soto, Guaracha-Basañez, Tamez-Torres, Sifuentes-Osornio, González-Lara and León. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ma. Fernanda González-Lara, ZmVyZ29ubGFAZ21haWwuY29t