
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 31 August 2023
Sec. Public Health Education and Promotion
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1146048
This article is part of the Research TopicClimate Change and Health: From Data and Strategies to Real ActionsView all 9 articles
 Adelaide Lusambili1,2
Adelaide Lusambili1,2 Peter Khaemba2Felix Agoi2Martha Oguna2,3
Peter Khaemba2Felix Agoi2Martha Oguna2,3 Britt Nakstad4,5*
Britt Nakstad4,5* Fiona Scorgie6Veronique Filippi7
Fiona Scorgie6Veronique Filippi7 Jeremy Hess3
Jeremy Hess3 Nathalie Roos8Mathew Chersich6
Nathalie Roos8Mathew Chersich6 Sari Kovats7,9Stanley Luchters2
Sari Kovats7,9Stanley Luchters2Background: Ambient heat exposure is increasing due to climate change and is known to affect the health of pregnant and postpartum women, and their newborns. Evidence for the effectiveness of interventions to prevent heat health outcomes in east Africa is limited. Codesigning and integrating local-indigenous and conventional knowledge is essential to develop effective adaptation to climate change.
Methods: Following qualitative research on heat impacts in a community in Kilifi, Kenya, we conducted a two-day codesign workshop to inform a set of interventions to reduce the impact of heat exposure on maternal and neonatal health. Participants were drawn from a diverse group of purposively selected influencers, implementers, policy makers, service providers and community members. The key domains of focus for the discussion were: behavioral practices, health facilities and health system factors, home environment, water scarcity, and education and awareness. Following the discussions and group reflections, data was transcribed, coded and emerging intervention priorities ranked based on the likelihood of success, cost effectiveness, implementation feasibility, and sustainability.
Results: Twenty one participants participated in the codesign discussions. Accessibility to water supplies, social behavior-change campaigns, and education were ranked as the top three most sustainable and effective interventions with the highest likelihood of success. Prior planning and contextualizing local set-up, cross-cultural and religious practices and budget considerations are important in increasing the chances of a successful outcome in codesign.
Conclusion: Codesign of interventions on heat exposure with diverse groups of participants is feasible to identify and prioritize adaptation interventions. The codesign workshop was used as an opportunity to build capacity among facilitators and participants as well as to explore interventions to address the impact of heat exposure on pregnant and postpartum women, and newborns. We successfully used the codesign model in co-creating contextualized socio-culturally acceptable interventions to reduce the risk of heat on maternal and neonatal health in the context of climate change. Our interventions can be replicated in other similar areas of Africa and serve as a model for co-designing heat-health adaptation.
High temperature are known to have a range of impacts on human health and wellbeing. It has been estimated that by 2009, heat-related child mortality in sub-Saharan Africa was already double what it would have been without climate change and will double again by 2050 if temperatures exceed 1.5°C of warming (1). High temperature are known to increase the risk of pre-term birth and stillbirth (2–5). With about 15 million babies born prematurely and most in sub-Saharan Africa and Asia (6, 7), pregnant women need to reduce their exposure to ambient heat. High temperatures also have negative effects on the mental health and wellbeing of pregnant women and can interfere with breastfeeding and infant care (8). The health consequences of climate change which are important for pregnant women and neonates also include insufficient food, inadequate supply of water, population displacement and infectious disease outbreaks (5). Adaptation to reduce the impact of climate change hazards on health outcomes is necessary. McMichael and Kovats discussed three adaptive modes: biological (individual level), behavioral (personal level) and social (community level) (9).
The benefits of locally led adaptation in climate change has gained traction (10, 11). Many health interventions tested in clinical settings are not as effective when translated into real-life practice (12). To increase uptake and utility of health interventions, the end-user needs to be meaningfully engaged in codesigning the interventions, either through multiple knowledge generation systems (13) or knowledge co-creation models (14, 15). To the best of our knowledge, there are no published interventions that have been codesigned to reduce the impact of ambient heat exposure on pregnant, postpartum and neonatal health, and particularly in hot arid and semi-arid areas such as Kilifi, Kenya. There is a growing body of evidence on the impacts of heat on these populations but limited research on the interventions to reduce such risks (16–22). It is therefore imperative to codesign contextualized interventions for mitigating effects of extreme heat exposure. In this study, we share our experience and lessons learned from co-developing a set of interventions against the impact of heat exposure on maternal and neonatal health.
Our codesign workshop was preceded by a qualitative study conducted in Kilifi County, Kenya, as part of the Climate Heat Maternal and Neonatal Health Africa (CHAMNHA) project. The research was led by the Aga Khan University between February and June 2021 which has worked previously with the local communities. Kilifi County is largely rural (23) with poor infrastructure: water is scarce and of low quality, health facilities are few and far from the community and many homes are grass thatched and unventilated (24). Families are generally large, consisting of 5 to 15 members, and perinatal mortality and morbidity is high (25).
The CHAMNHA research aimed to examine the perceptions toward the effects of high temperatures on women during pregnancy, childbirth and postpartum, and the effects on their neonates. We interviewed community members, including pregnant and postpartum women, key stakeholders from different government ministries, and community members that support women through pregnancy and childbirth. The findings from the qualitative study highlighted the importance of local attitudes to heat and pregnancy in affecting the impacts on pregnant women and newborns (see Table 1) (8, 26).
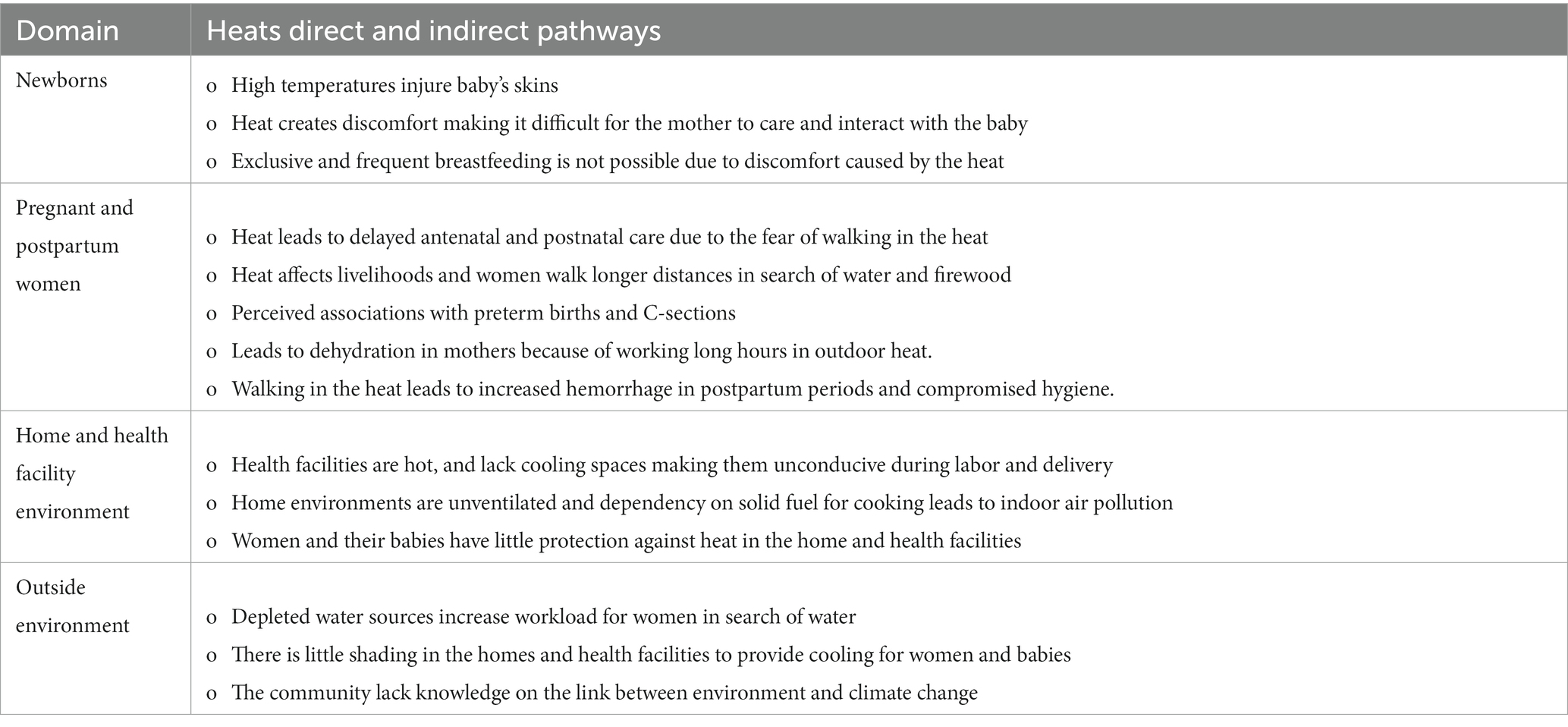
Table 1. Summary of the qualitative study findings.
The codesign workshop was conducted after a series of meetings and discussions with a group of multidisciplinary professionals from social behavioral, environmental and health sciences, including clinicians in maternal and neonatal health. The findings from Table 1 informed the discussions.
Successful collaboration and design require representation of a diverse range of people at different levels of the community, including key influencers, implementers, and end users (27, 28). To have an accurate, representative view of the community, we incorporated diverse participants, including direct beneficiaries or the target group for the intervention (pregnant and postpartum women) and representatives from key ministries that implement and deliver services (ministries of Water, Environment, Housing, Education, Health, Infrastructure and the Department of Meteorology). We also included community leaders and influencers such as religious leaders, local chiefs, community health unit heads and community health volunteers. Women’s household support systems, such as their male spouses and mother-in laws also participated in the codesign workshop (Table 2).
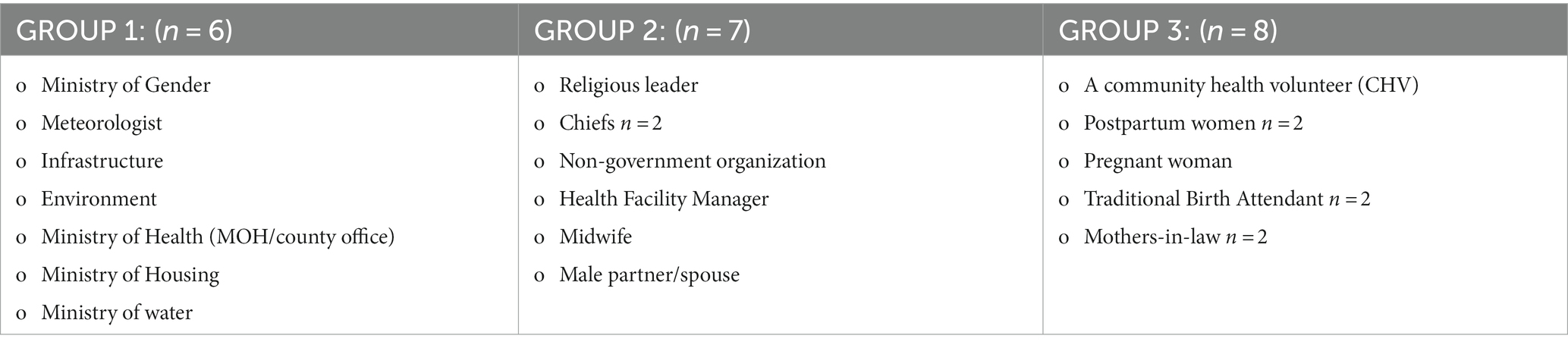
Table 2. Codesign participants.
De Freitas and Martin observed the importance of being sensitive to power differentials when working in marginalized communities such as Kilifi (29). They also impressed on the need to provide creative approaches to ensure safe environments for conversations without necessarily increasing tokenism. The project researchers worked with local facilitators and consulted with community health volunteers in Kilifi to ensure that participants were assigned in groups where they could feel comfortable as illustrated in Table 2. These groups were structured to reflect sensitivity to power differentials (gender roles) and ensure a safe and inclusive environment to discuss issues at hand. For instance, female Community Health Volunteers (CHVs), pregnant and postpartum women, mothers in law and traditional birth attendants (TBAs) (group 3) were put in a separate group as it was deemed inappropriate to mix them with representatives from government ministries (group 1), or community leaders (group 2) due to power dynamics, also amplified by language barriers.
Group discussions were structured to focus on topics that could be discussed easily among the group members. For instance, members who were mainly from government ministries (group 1) were tasked with the responsibility of discussing and suggesting interventions to key issues at policy levels, such as improvements in the home/built environment, water scarcity, reforestation, and the shading of communities.
Both group 2 and 3 were tasked to discuss issues at meso-and micro-levels, such as challenges in the health systems that may be detrimental to maternal and neonatal health in periods of high temperatures. These topics had been discussed and decided by the CHAMNHA consortium members following a series of meetings during data analysis (Table 3).
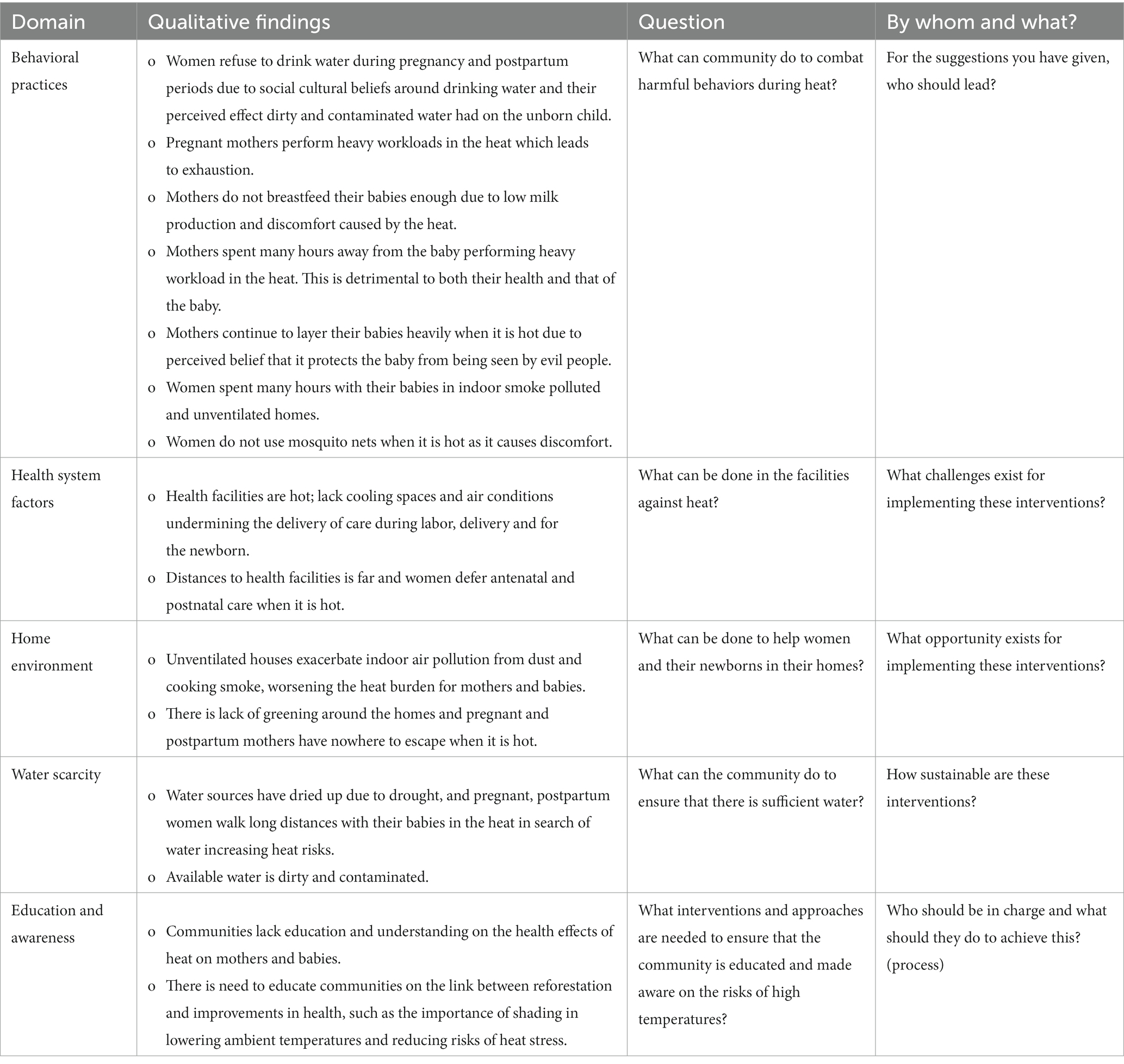
Table 3. Codesign discussion topics.
A total of six facilitators (two females and four males) underwent training prior to the workshop, conducted by the social scientists assigned to the study. The facilitators included individuals who had been part of the formative research (n = 2), while the rest (n = 4) had extensive experience working in the target community. The training included a review of the CHAMNHA study objectives, findings, content for the workshop and consent process. During the training, we used PowerPoint presentations and role playing within each group to ensure that the facilitators were conversant with the scheduled programs, processes, and content. We also discussed gender and power dynamics, professional roles, identities, and language barriers.
The codesign workshop was conducted face to face in June 2021 over 2 days. Recognizing vulnerabilities and being aware of the potential barriers to participation, the CHAMNHA team had reached out to our participants before the workshop and discussed the codesign objectives and compensation. Considering that rural Kilifi is geographically sparse with limited public transportation means, the CHAMNHA team provided all the participants with transport. This was to facilitate them to come to the hotel, where they had a full board accommodation for the 2 days. Since the codesign workshop was conducted during Covid-19, there was limited travel and some CHAMNHA members (AL, FS, BN, SL) joined the presentations and discussions sessions via the Zoom platform.
At the start of the workshop, all the participants were asked to review the qualitative study findings (Table 1), after which they broke out into different rooms in small groups (Table 2) for discussions. Each group had a facilitator and a note taker. Firstly, group facilitators introduced themselves and explained the objectives of the codesign, the group topic of focus and the expected outcomes. Secondly, participants in the small groups introduced themselves to each other and described their roles in the community. Thirdly, facilitators explained methods of participatory design, processes, and active consenting to grant permission for them to record all interactions by photos, audio, and observation notes for further processing. Fourthly, each group and trained facilitator were allocated specific topics to discuss (Table 3) and guided questions to ask the groups. For example, after introducing the group topics, facilitators opened the discussions by asking the group to share their views on what the community can do to help women and their newborns in periods of high temperatures during pregnancy, labor, delivery and postpartum. In addition, participants were asked to discuss the challenges and opportunities that exist in implementing the interventions they had suggested. Lastly, the groups were asked to reflect on the suggested interventions based on their ‘likelihood of success’, ‘cost effectiveness’, ‘effectiveness’ and ‘sustainability’ design characteristics.
Toward the end of the first day, all the groups met together for 15 min to reflect on the day’s activities and explain the program for the second day. Table 3 summarizes the main issues that were deliberated by the groups during the codesign workshop. These topics were discussed and agreed in advance by CHAMNHA consortium after analysis of the qualitative research and a series of meetings.
On the second day, all groups met in the conference hall and each group presented their suggested interventions. The presentation focused on the priority interventions, possible challenges, and opportunities that exist in this community for successful intervention. The presentation was audio-recorded and thematically analyzed by researchers. As summarized in Table 4, interventions to improve water systems, behavior change, and education were mentioned by all the groups.
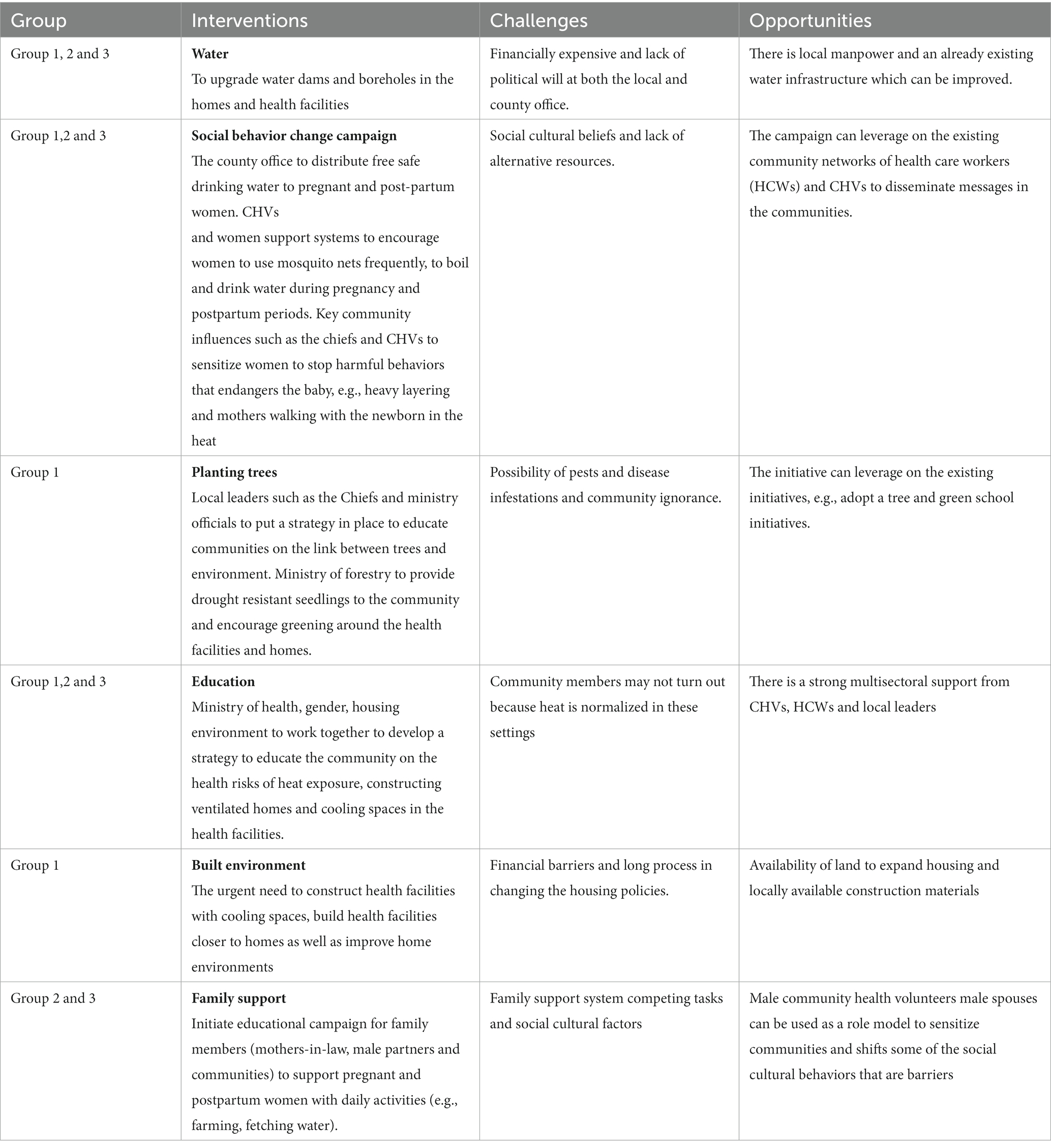
Table 4. Summary of group presentations: interventions, challenges, and opportunities.
Following the group presentations, participants were given the opportunity to reflect and share their thoughts in the light of all the presentations. Reflections from participants shed light on the interventions they considered as a priority.
Overall, the participants acknowledged that there was an urgent need for interventions targeting the whole community to create awareness and educate them on the effects of heat exposure on maternal and newborn health. Education could incorporate behavior change campaigns to shift some of the socio-cultural practices that are harmful to the mother and newborn in periods of high temperatures. These behaviors, as our research found, include: 1. Some women do not drink enough water or refuse to drink water during pregnancy and postpartum periods. In part this is because, generally the water in these settings is scarce and available water is dirty and contaminated which may require women to boil before drinking. In addition, social cultural beliefs among some clans that “water harms the unborn child or freezes breast milk” may discourage some women. 2. Heavy layering of neonates and babies in the first six months due to social cultural belief that leaving the babies skin lightly covered attracts spells and jinx from witchdoctors. 3. Women performing outdoor activities of daily livelihood in the heat with newborns strapped on their backs because the culture expects them to start working immediately after delivery.
Further, the participants argued for the need to have a community campaign not only to sensitize about the heat related health risks, but also to sensitize family members to support pregnant and postpartum women during periods of high temperatures.
Dealing with water scarcity was discussed as the key intervention that can reduce the discomfort of pregnant and postpartum women both at home and in the health facilities during labor and birth. Kilifian women walk with their new-borns strapped on their back for over one hour in the heat in search for water. Many health facilities do not have water and pregnant women are required to carry their own water from home to the health center during labor and delivery. Besides, the need to expand cooling spaces in the health facilities and in the communities was discussed as a priority area of intervention. Participants noted that health facilities could be constructed closer to the homes and the community can be provided with seedlings to plant trees with the aim of improving shading.
On the contrary, there were some interventions that were suggested during the reflection time that most of the participants considered either not appropriate or not a priority in this context. For example, painting the roofs white was seen as inappropriate, as many of the houses in rural Kilifi are built from mud and require no painting. In the same vein, the nature of the houses cannot sustain rain harvesting due to grass thatched roofs. Providing air conditioning fans in the homes to assist pregnant and postpartum women when the temperatures are high was considered unsustainable as most of the homes do not have electricity and even for the few homes that have electricity, this solution would be too expensive for the locals to afford as energy bills were reported to be high.
Following the participants reflections and group presentations, the research team summarized the main priorities and invited the participants to do rankings based on the four design characteristics: the likelihood of success, cost effectiveness, effectiveness of the interventions, and sustainability. The ranking was tabulated, and results announced as in Table 5. Based on the rankings, accessibility to water, social behavior change campaign and education were ranked top three interventions for reducing the impact of climate change-related heat exposure on pregnant and postpartum women, and newborns.
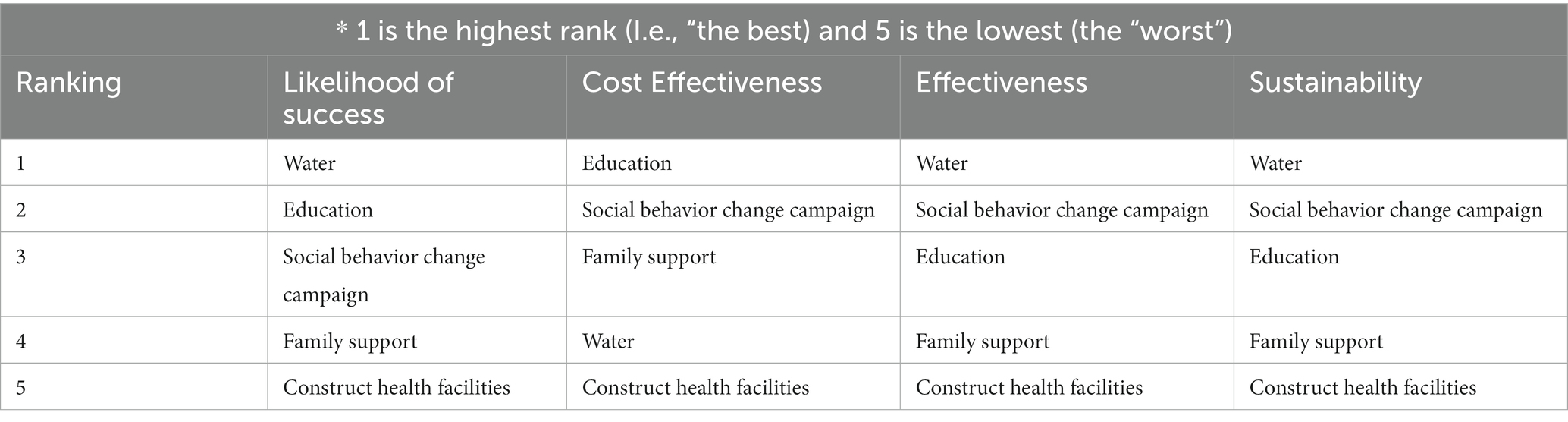
Table 5. Ranking.
Research on the association between heat exposure and overall health risks is an unexplored area in this Kenyan context. Our codesign workshop was used as an opportunity to build capacity among facilitators and participants. Our participants confessed that they were not aware of health-related risks of heat exposure, and that our presentation of the research findings was informative, as it provided insights on experiences, they had been observing in Kilifi County. Building capacity among key community influencers, such as chiefs, religious leaders, community health volunteers and male spouses, was suggested to be of greater impact as these individuals would share the information in various local communities and decisive making authorities. Creating such awareness would help community to begin finding solutions to protect themselves and, particularly, those who are vulnerable.
Our codesign had diverse participants drawn from different levels including the beneficiaries (micro), community influencers (meso) and policy makers at the various ministries (macro). Various topics were also discussed based on the individuals’ roles in the society, such as allocating individuals to groups where they felt comfortable to share their views was key to finding beneficial solutions. During the plenary discussions and reflections, the priority interventions were well in line with all the participants. Participants felt that both water and social behavioral change campaigns should be a priority intervention that can be sustainable, while on the other hand they were very clear on interventions considered not fit for this context. For example, where interventions such as installing air fans and painting roofs white have been used elsewhere and found to have a positive effect (30), in this context, it was not deemed appropriate. This revelation shows that, although the effect of heat exposure across the communities may be the same, interventions may vary based on the context they will adapt to and there is no “one size-fits-all” interventions. As extreme weather continues to ravage many communities in sub-Saharan Africa, it is important that different players and stakeholders at different levels be consulted in making decisions they consider appropriate in their own communities.
A lesson learned from this codesign was the importance of training the facilitators in advance and giving them opportunity to reflect on possible challenges before the codesign workshop. Our group facilitators underwent a thorough two-day training, and one of the foreseen challenges was the possibility of being distracted by participants diverting discussions to their current economic challenges such as unemployment and a lack of livelihood. We felt that sufficiently training facilitators and giving them possible dips on how to negotiate with participants when such emotive questions arose was important in enhancing rapport building with the participants.
CHAMNHA researchers faced various challenges that are key for future codesign workshops in similar settings. The rural communities in Kilifi County are geographically dispersed, with limited public transport. For logistical purposes, we conducted our codesign workshop for 2 days in a hotel where all the participants stayed. The consequence of this was that, recruiting pregnant and postpartum women who had to spend 2 days at the hotel was made by cultural barriers as their male spouses and partners did not consent, a problem experienced by women in these communities. The women who accepted to attend the workshop had to be accompanied with their mothers-in-law. Postpartum women attending the conference came with infants and other young children in their households. This led to additional expenditure for the project. It must be noted that in the Kilifi rural community, male spouses/partners and mothers-in-law feel insecure having young wives spend the nights outside without their presence. Future codesign workshops should invite pregnant and postpartum women, but they should allocate a budget able to cover the need for spouses, childcare and other influential household member such as mothers-in-law who may want to attend and provide protection for their daughters-in law. Alternatively, codesign should be conducted in the communities close to where women live.
There were many interruptions during the session. For religious considerations, many of the participants had to leave the meetings to pray, while some mothers had to be given time to breastfeed. These considerations must be factored in future codesign. Moreover, the codesign was conducted when temperatures were high in Kilifi and participants suffered from symptoms of heat exhaustion.
Lastly, we noticed that during our community entry when we involved and informed different ministries, key influencers and community members about our research, they did not seem to understand the objectives of our community-related research as they did not fully appreciate that ambient heat may have adverse effects on the health of pregnant and postpartum mothers and newborn children. This implied that the facilitators had to spend much time explaining our research to participants before the actual discussions could begin.
The codesign workshop was developed following a series of meetings and reflections where CHAMNHA consortium members closely interrogated and discussed data from the formative research. The process also entailed working closely with field researchers and community health volunteers to further refine some of the findings and areas of interventions that were discussed during the workshop. CHAMNHA successfully utilized the codesign model to identify and prioritize contextualized socio-culturally acceptable interventions to reduce the impact of climate heat exposure hazards on maternal and neonatal health in Kilifi County. Fruitful discussions were carried out and useful conclusions were made. Accessibility to water, social behavior change campaigns and education were ranked the top three sustainable interventions as these were evaluated as effective with the highest likelihood of success.
The codesigned interventions aligned with behavioral and social adaptive models as well as the primary, secondary and tertiary prevention categories (9). On primary prevention, change in social norms where family support would ensure that neonates are wrapped in fewer layers of clothing and staying in the coolest possible places as women carry out their outdoor daily livelihood chores. Additionally, planting trees for shade, cooling spaces, ventilation and insulation in houses or health facilities would reduce the risk of exposure to excess heat. These interventions need significant awareness and knowledge sharing and, therefore could explain why social behavior change campaigns and education ranked among the top recommended interventions. Creating awareness through public education on practices such as avoiding heat and rehydration to replenish lost body fluids have been suggested to reduce illness related to thermal stress (9, 30).
Secondary prevention measures included making water more accessible, which would ensure that women do not walk long distances in search of water while exposing themselves to unbearable heat and dehydration for poor maternal and neonatal health. The availability of safe drinking water will help women and children stay rehydrated and encourage them to drink more water during pregnancy, and improve hygienic practices such as hand washing, food/fruits cleaning and general sanitation.
On tertiary prevention, the construction of additional health facilities would increase accessibility to the healthcare system for curative interventions against the impact of heat exposure. However, this was ranked the least important high across the four designed characteristics. Nevertheless, if health facilities were closer to the population at the community level, then women would commute shorter distances in search of health care, reducing exposure to excess heat. Additionally, this will improve health seeking behavior during the perinatal period that would improve overall health outcomes, as part of primary and secondary prevention strategies against the impact of heat exposures.
It was surprising to see family support ranked in the top three on perceived intervention cost-effectiveness, displacing water intervention which ranked as number four. This suggested that the community feels that making safe water available would require significant investment. Indeed, the coastal Kenyan region relies on sparsely distributed freshwater rivers making accessibility to clean, safe fresh water much harder.
Implementation of this codesign navigated several challenges: overcoming community participants’ level of education through a paired-up approach, accommodating socio-cultural and religious norms and traditional practices during the codesign sessions, flexibility in financial planning to meet unexpected costs related to community participations’ facilitation to attend codesign sessions, and stakeholders’ knowledge gaps on targeted communities requiring extensive recruitment mobilization and intensive study sensitization. Therefore, when planning codesign sessions, prior to this contextualizing of local set up, cross-cultural and religious practices and budget considerations would increase the chances of a successful outcome of interventions to promote neonatal and maternal health in very hot settings.
The link between heat exposure and overall health risks is an unexplored topic in Kilifi, Kenya but is of increasing importance under climate change even globally. Our experience shows that codesign interventions on heat exposure with diverse stakeholder process yielded some unexpected findings. The codesign workshop was successfully utilized as an opportunity to build capacity among facilitators and participants and explore interventions to address the impact of heat exposure on pregnant, and postpartum women and newborns. Accessibility to water, social behavior change campaign and education were ranked as the top three interventions with the highest likelihood of success. Family support was also ranked fourth and could easily be integrated with social and behavior change campaigns. The codesign approach provides unique opportunities for developing interventions with various stakeholders to address the impact of climate change-related heat exposure on pregnant, postpartum women and newborns. Future studies should test the effectiveness of these interventions.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Aga Khan University Ethics Committee ref. 2020/IERC-94 (v2) and National Commission for Science and Technology and Innovation Ref BAHAMAS ABS/P/20/7568, London School of Hygiene and Tropical Medicine Ref: 22685 and from Kilifi County Office ref. DOM/KLF/RESCH/vol.1/66. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
AL wrote the first draft. All authors reviewed the manuscript, contributed to the article, and approved the submitted version.
The CHAMNHA was funded by the Natural Environment Research Council (grant numbers NE/T013613/1 and NE/T01363X/1), the Research Council of Norway (grant number 312601) and The Swedish Research Council for Health, Working Life and Welfare in collaboration with the Swedish Research Council (Forte) (grant number 2019-01570) and the National Science Foundation (NSF) (grant number ICER-2028598), coordinated through a Belmont Forum partnership.
We are grateful to Kilifi community members, including our research and study participants, policy makers and all the facilitators of the codesign workshop. We would like to thank Cathryn Birch and Raphael Ondondo for providing comments on the first draft of this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Chapman, S, Birch, CE, Marsham, JH, Part, C, Hajat, S, Chersich, MF, et al. Past and projected climate change impacts on heat-related child mortality in Africa. Environ Res Lett. (2022) 17:074028. doi: 10.1088/1748-9326/ac7ac5
2. Davenport, F, Dorélien, A, and Grace, K. Investigating the linkages between pregnancy outcomes and climate in sub-Saharan Africa. Popul Environ. (2020) 41:397–421. doi: 10.1007/s11111-020-00342-w
3. Rylander, C, Odland, J, and Sandanger, TM. Climate change and the potential effects on maternal and pregnancy outcomes: an assessment of the most vulnerable – the mother, fetus, and newborn child. Glob Health Action. (2013) 6:19538. doi: 10.3402/gha.v6i0.19538
4. Konkel, L. Taking the heat: potential fetal health effects of hot temperatures. Environ Health Perspect. (2019) 127:102002. doi: 10.1289/EHP6221
5. Mannan, I, Choi, Y, Coutinho, AJ, Chowdhury, AI, Rahman, SM, Seraji, HR, et al. Vulnerability of newborns to environmental factors: findings from community based surveillance data in Bangladesh. Int J Environ Res Public Health. (2011) 8:3437–52. doi: 10.3390/ijerph8083437
6. Sharrow, D, Hug, L, You, D, Alkema, L, Black, R, Cousens, S, et al. Global, regional, and national trends in under-5 mortality between 1990 and 2019 with scenario-based projections until 2030: a systematic analysis by the UN inter-agency group for child mortality estimation. Lancet Glob Health. (2022) 10:e195–206. doi: 10.1016/S2214-109X(21)00515-5
7. Walani, SR. Global burden of preterm birth. Int J Gynaecol Obstet. (2020) 150:31–3. doi: 10.1002/ijgo.13195
8. Lusambili, A, Khaemba, P, Nakstad, B, Kovats, S, Fillipi, V, Roos, N, et al. Too hot to thrive: Community perspectives on the effect of high ambient temperature on postpartum women and neonates in Kilifi, Kenya. Res. Square. (2023). doi: 10.21203/rs.3.rs-3034548/v1
9. McMichael, AJ, and Kovats, RS. Climate change and climate variability: adaptations to reduce adverse health impacts. Environ Monit Assess. (2000) 61:49–64. doi: 10.1023/A:1006357800521
10. Rahman, MF, Falzon, D, Robinson, SA, Kuhl, L, Westoby, R, Omukuti, J, et al. Locally led adaptation: promise, pitfalls, and possibilities. Ambio. (2023). doi: 10.1007/s13280-023-01884-7
11. Cuaton, GP, and Su, Y. Local-indigenous knowledge on disaster risk reduction: insights from the Mamanwa indigenous peoples in Basey, Samar after typhoon Haiyan in the Philippines. Int J Disaster Risk Reduct. (2020) 48:101596. doi: 10.1016/j.ijdrr.2020.101596
12. Ioannidis, JP. Why Most clinical research is not useful. PLoS Med. (2016) 13:e1002049. doi: 10.1371/journal.pmed.1002049
13. Iwama, AY, Araos, F, Anbleyth-Evans, J, Marchezini, V, Ruiz-Luna, A, Ther-Ríos, F, et al. Multiple knowledge systems and participatory actions in slow-onset effects of climate change: insights and perspectives in Latin America and the Caribbean. Curr Opin Environ Sustain. (2021) 50:31–42. doi: 10.1016/j.cosust.2021.01.010
14. Coggan, A, Carwardine, J, Fielke, S, and Whitten, S. Co-creating knowledge in environmental policy development. An analysis of knowledge co-creation in the review of the significant residual impact guidelines for environmental offsets in Queensland, Australia. Environ Challenges. (2021) 4:100138. doi: 10.1016/j.envc.2021.100138
15. Slattery, P, Saeri, AK, and Bragge, P. Research co-design in health: a rapid overview of reviews. Health Res. Policy Syst. (2020) 18:17. doi: 10.1186/s12961-020-0528-9
16. Part, C, Filippi, V, Cresswell, JA, Ganaba, R, Hajat, S, Nakstad, B, et al. How do high ambient temperatures affect infant feeding practices? A prospective cohort study of postpartum women in Bobo-Dioulasso, Burkina Faso. BMJ Open. (2022) 12:e061297. doi: 10.1136/bmjopen-2022-061297
17. Lakhoo, DP, Blake, HA, Chersich, MF, Nakstad, B, and Kovats, S. The effect of high and low ambient temperature on infant health: a systematic review. Int J Environ Res Public Health. (2022) 19:109. doi: 10.3390/ijerph19159109
18. Nakstad, B, Filippi, V, Lusambili, A, Roos, N, Scorgie, F, Chersich, MF, et al. How climate change may threaten Progress in neonatal health in the African region. Neonatology. (2022) 119:644–51. doi: 10.1159/000525573
19. de Bont, J, Stafoggia, M, Nakstad, B, Hajat, S, Kovats, S, Part, C, et al. Associations between ambient temperature and risk of preterm birth in Sweden: a comparison of analytical approaches. Environ Res. (2022) 213:113586. doi: 10.1016/j.envres.2022.113586
20. Part, C, le Roux, J, Chersich, M, Sawry, S, Filippi, V, Roos, N, et al. Ambient temperature during pregnancy and risk of maternal hypertensive disorders: a time-to-event study in Johannesburg, South Africa. Environ Res. (2022) 212:113596. doi: 10.1016/j.envres.2022.113596
21. Lusambili, A, and Nakstad, B. Awareness and interventions to reduce dehydration in pregnant, postpartum women, and newborns in rural Kenya. Afr J Prim Health Care Fam Med. (2023) 15:e1–3. doi: 10.4102/phcfm.v15i1.3991
22. Samuels, L, Nakstad, B, Roos, N, Bonell, A, Chersich, M, Havenith, G, et al. Physiological mechanisms of the impact of heat during pregnancy and the clinical implications: review of the evidence from an expert group meeting. Int J Biometeorol. (2022) 66:1505–13. doi: 10.1007/s00484-022-02301-6
23. Ngugi, AK, Walraven, G, Orwa, J, Lusambili, A, Kimani, M, and Luchters, S. Community-driven data revolution is feasible in developing countries: experiences from an integrated health information and surveillance system in Kenya. J Global Health Rep. (2021) 5:e2021074. doi: 10.29392/001c.25977
24. Lusambili, AM, Naanyu, V, Wade, TJ, Mossman, L, Mantel, M, Pell, R, et al. Deliver on your own: disrespectful maternity care in rural Kenya. PLoS One. (2020) 15:e0214836. doi: 10.1371/journal.pone.0214836
25. Lusambili, AM, Nyanja, N, Chabeda, SV, Temmerman, M, Nyaga, L, Obure, J, et al. Community health volunteers challenges and preferred income generating activities for sustainability: a qualitative case study of rural Kilifi, Kenya. BMC Health Serv. (2021) 21:642. doi: 10.1186/s12913-021-06693-w
26. Scorgie, FAL, Luchters, S, Khaemba, P, Filippi, V, Nakstad, B, Hess, J, et al. “Mothers get really exhausted!” the lived experience of pregnancy in extreme heat: qualitative findings from Kilifi, Kenya. Soc Sci Med. (2023).
27. Mulvale, G, Moll, S, Miatello, A, Murray-Leung, L, Rogerson, K, and Sassi, RB. Co-designing services for youth with mental health issues: novel elicitation approaches. Int J Qual Methods. (2019) 18:160940691881624. doi: 10.1177/1609406918816244
28. Gonzalez, M, Phoenix, M, Saxena, S, Cardoso, R, Canac-Marquis, M, Hales, L, et al. Strategies used to engage hard-to-reach populations in childhood disability research: a scoping review. Disabil Rehabil. (2021) 43:2815–27. doi: 10.1080/09638288.2020.1717649
29. de Freitas, C, and Martin, G. Inclusive public participation in health: policy, practice and theoretical contributions to promote the involvement of marginalised groups in healthcare. Soc Sci Med. (2015) 135:31–9. doi: 10.1016/j.socscimed.2015.04.019
Keywords: codesign, climate change, heat exposure, pregnant and postpartum women, newborns
Citation: Lusambili A, Khaemba P, Agoi F, Oguna M, Nakstad B, Scorgie F, Filippi V, Hess J, Roos N, Chersich M, Kovats S and Luchters S (2023) Process and outputs from a community codesign workshop on reducing impact of heat exposure on pregnant and postpartum women and newborns in Kilifi, Kenya. Front. Public Health. 11:1146048. doi: 10.3389/fpubh.2023.1146048
Edited by:
Alpo Juhani Vuorio, University of Helsinki, FinlandReviewed by:
Santosh Pandipati, e-Lōvu, United StatesCopyright © 2023 Lusambili, Khaemba, Agoi, Oguna, Nakstad, Scorgie, Filippi, Hess, Roos, Chersich, Kovats and Luchters. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Britt Nakstad, YnJpdHQubmFrc3RhZEBtZWRpc2luLnVpby5ubw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.