
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health , 26 June 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1136988
 Alejandro G. García-Ruiz de Morales1,2,3*†
Alejandro G. García-Ruiz de Morales1,2,3*† Javier Martínez-Sanz1,3*†
Javier Martínez-Sanz1,3*† María J. Vivancos-Gallego1,3
María J. Vivancos-Gallego1,3 Matilde Sánchez-Conde1,3Manuel Vélez-Díaz-Pallarés4
Matilde Sánchez-Conde1,3Manuel Vélez-Díaz-Pallarés4 Beatriz Romero-Hernández5,6María Dolores González Vázquez7Carmen María Cano de Luque8Ander González-Sarria9
Beatriz Romero-Hernández5,6María Dolores González Vázquez7Carmen María Cano de Luque8Ander González-Sarria9 Juan Carlos Galán5,6Francisco Gea Rodríguez10
Juan Carlos Galán5,6Francisco Gea Rodríguez10 Santiago Moreno1,2,3†María Jesús Pérez-Elías1,3†
Santiago Moreno1,2,3†María Jesús Pérez-Elías1,3†Background: Missed opportunities for Human Immunodeficiency Virus (HIV) and Hepatitis C Virus (HCV) testing remain high. We aimed to ascertain the knowledge of screening guidelines and attitudes of non-infectious disease (ID) hospital physicians and assess the impact of a 1-h session on screening rates and diagnoses.
Methods: This interventional study consisted of a 1-h training session on HIV and HCV epidemiology and testing guidelines for non-ID physicians. Pre-and post-session questionnaires compared the knowledge of the guidelines and attitudes toward screening before and after the session. Rates of screening and diagnoses were compared in three 6 months periods: before, immediately after, and 24 months ±4 after the session.
Results: A total of 345 physicians from 31 departments participated in these sessions. Before the session, 19.9% (28% medical, 8% surgical) and 17.9% (30% medical, 2.7% surgical) were aware of HIV and HCV testing guidelines, respectively. The willingness to routinely test increased from 5.6 to 22%, whereas not ordering tests decreased from 34.1 to 2.4%. HIV screening rates significantly increased by 20% after the session (7.7 vs. 9.3 tests per 103 patients; p < 0.001), and the effect persisted until the long-term period. The HIV diagnosis rate increased globally (3.6 vs. 5.2 HIV diagnoses per 105 patients; p = 0.157), mainly because of medical services (4.7 vs. 7.7 per 105 patients; p = 0.082). The HCV screening rate increased significantly immediately and in the long term only in medical services (15.7 and 13.6%, respectively). The new active HCV infection rates increased immediately and declined steeply thereafter.
Conclusion: A short session for non-ID physicians can improve HIV/HCV screening, increase diagnosis, and contribute to disease elimination.
Human Immunodeficiency Virus (HIV) and Hepatitis C Virus (HCV) infections are two of the leading causes of disease worldwide, and are associated with high morbidity and mortality (1, 2). Delayed diagnosis of both infections poses a significant challenge to public health. It is associated with a higher probability of long-term sequelae, increased mortality, and greater risk of onward transmission (3–6).
Current HIV and HCV treatments are simple, safe, and highly effective in suppressing viral replication and preventing morbidity, mortality, and transmission in HIV (3, 5), curing HCV infection, reducing long-term liver sequelae, and preventing cirrhosis and hepatocellular carcinoma (6). The sooner both treatments are started, the lesser the long-term consequences (4). Despite this, screening of asymptomatic patients is poorly implemented (7–9), and testing in many European countries remains guided by risk behaviors and limited to populations with a known high prevalence of both infections (7, 9).
HIV and HCV testing can be performed by any physician both in hospitals and primary care facilities. Missed testing opportunities in both locations remain high (10–16), although some primary care educational interventions have improved screening rates (17, 18). Nevertheless, among hospital noninfectious disease (ID) specialists, reports on such interventions are scarce.
Given the similarity in risk factors and the population affected by both infections, we aimed to describe the knowledge on screening policies and the current routine HIV and HCV screening practices of non-ID physicians in a tertiary hospital and to assess the impact of a 1-h training session on screening rates of both infections.
We conducted an interventional study at Ramón y Cajal Hospital in Madrid, Spain, a tertiary hospital with 900 beds and 32 medical and surgical departments covering a population of approximately 600,000 inhabitants. From February to November 2019, five physicians (four ID specialists and one gastroenterologist) provided a non-mandatory 1-h training session on HIV, HCV, and other sexually transmitted infections, including epidemiology, risk factors, clinical aspects, and screening, to the other 31 hospital departments (17 medical and 14 surgical, Supplementary Table S1).
First, a brief questionnaire was used before training (Supplementary Tables S2, S3) to evaluate previous attitudes toward screening. After the training, a second questionnaire was used to evaluate the immediate effect of the session on participants’ expressed future attitudes toward testing. We performed a before-after comparative analysis of the responses to both questionnaires. Second, we compared the absolute number of HIV and HCV tests requested, the screening rate per 1,000 patients attended, and the new HIV and HCV diagnoses and positivity rates per 100,000 patients attended in the 6 months before and after the training, globally, and for each department. Finally, we analyzed the long-term effect of the intervention by comparing the rates to those obtained 21 to 28 months after the training sessions. We excluded serologies from known HIV-positive patients and follow-up serologies from HCV-untreated patients.
The number of patients attended per period and department was obtained from the hospital’s electronic records. In contrast, the number of ordered tests, positive tests, and new diagnoses was obtained from the records of the Microbiology, Infectious Diseases, and Gastroenterology departments.
The follow-up for each department in the pre-, post-training, and long-term periods was expected to be 180 days. Nevertheless, due to the impact of the Coronavirus Disease 2019 (COVID-19) pandemic, the normal workflow of each department has changed. To avoid possible biases due to modifications in the number of attended patients and serologies requested by each specific department, we decided to censor follow-up for those departments that had not completed their post-training observation period by March 14, 2020. For each department, the number of evaluated days before the session was matched to that in the post-training and long-term periods (Supplementary Table S1).
We used medians and interquartile ranges (IQR) for descriptive analysis, Fisher’s exact test to compare categorical variables, and Wilcoxon’s signed-rank test to compare paired quantitative variables. All contrasts were bilateral, and p values <0.05 were considered statistically significant. Statistical analysis was performed using Stata® 17.0 software (Stata Corp-LP, College Station, TX, United States) and Microsoft® Excel 16.67 software (Microsoft Corp., Redmond, WS United States,). GraphPad Prism 9 (GraphPad Software Inc.) was used to generate the figures.
The training sessions included 345 physicians from 31 hospital departments, with a median of 16 physicians per department (IQR 6–23). They were mainly women (59.3%) and under 40 years of age (67.3%; only 9.8% were above 55 years old).
According to the pre-training questionnaire, 19.9% (28.0% medical, 8.0% surgical; p < 0.001) and 17.9% (30.0% medical, 2.7% surgical; p < 0.001) of the participants were aware of HIV and HCV testing guidelines, respectively. When asked whether they ordered these tests during their usual practice, 5.6% claimed to ask for them routinely (9.5% medical, 0.7% surgical; p < 0.001), 60.4% if there were identifiable risk factors and/or indicator conditions (72.6% medical, 45.1% surgical; p < 0.001), and 34.1% never ordered them (17.9% medical, 54.3% surgical; p < 0.001; Supplementary Table S2).
Regarding the post-training questionnaire, we observed a significant increase in physicians who showed a positive attitude toward routinely asking for screening tests (5.6% vs. 22.0%; p < 0.001), and a significant decline in those who did not consider ordering a test (34.1% vs. 2.4%; p < 0.001). In addition, 98.2% of the participants (97.9% medical, 98.6% surgical, p = 0.485) considered the training session and potential availability of a tool to guide HIV and HCV testing. Supplementary Tables S2, S3 show the data detailed by medical and surgical specialty pre-and post-training.
Supplementary Table S1 shows the dates of the training sessions and the number of patients who attended each department during the corresponding observation period.
5,257 pre-training and 6,532 post-training HIV serologies were requested (7.7 vs. 9.3 tests per 103 attended patients; p < 0.001). This increase was significant both in medical and surgical departments (6.8 vs. 7.9 tests per 103 attended patients, p < 0.001; and 9.0 vs. 11.3, p < 0.001 respectively; Figure 1; Table 1), although only driven by six medical departments and just one surgical department (Table S4a). Overall, we found 25 pre-training and 37 post-training positive tests (3.6 vs. 5.2 HIV diagnoses per 105 attended patients; p = 0.157), but this increase was only seen in medical departments (19 vs. 32, corresponding to 4.7 vs. 7.7 diagnoses per 105 attended patients; p = 0.082; Figure 1; Table 1). These new diagnoses were concentrated in the Emergency Department (5.0 vs. 12.0 diagnoses per 105 attended patients; p = 0.137), Preventive Medicine Department (99.8 vs. 290.8; p = 0.161), and Nephrology (12.2 vs. 38.1; p = 0.133) (Supplementary Table S4b).
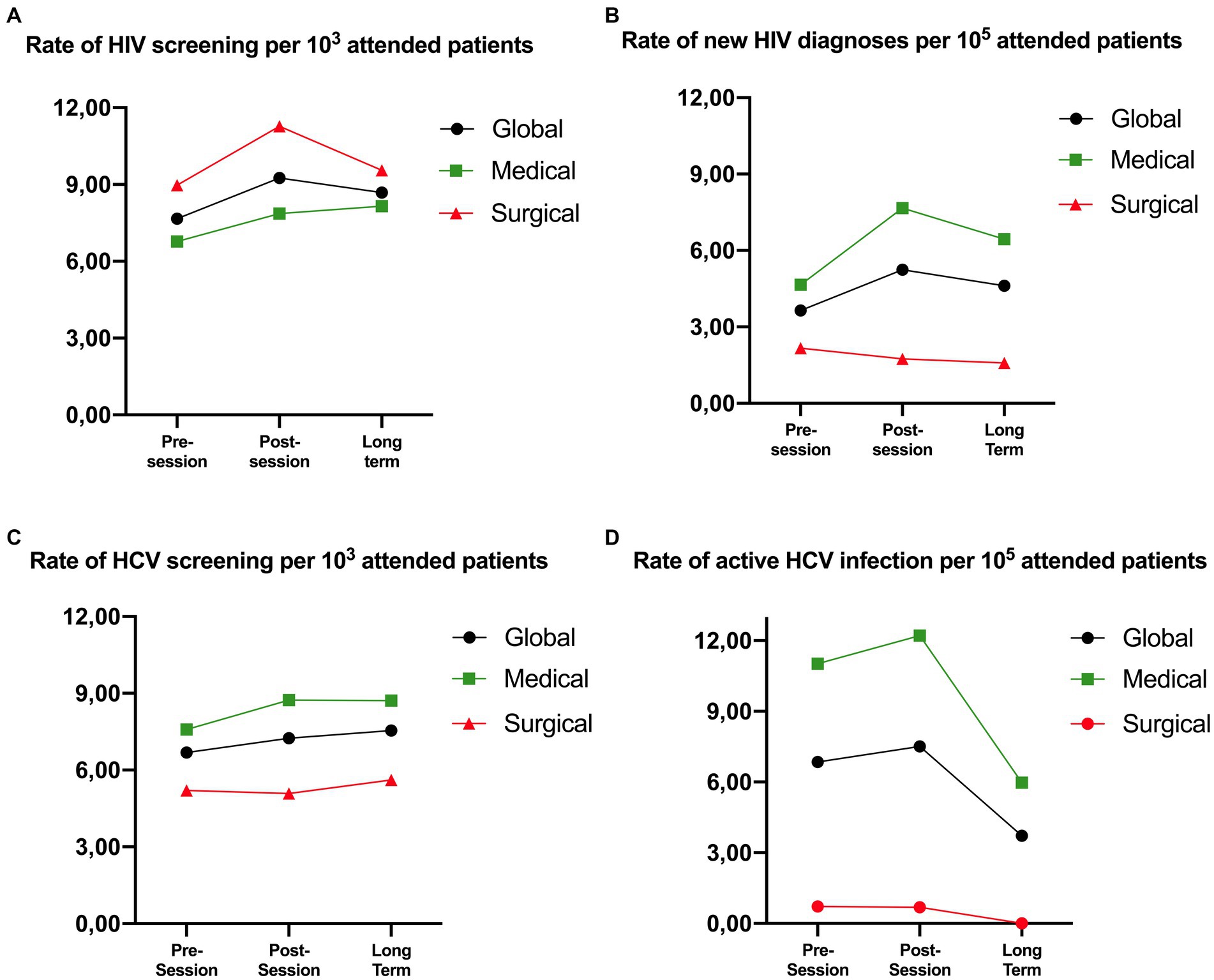
Figure 1. Evolution of the global screening rate and active infection globally, in medical and surgical departments. The figure shows the evolution of the rate of screening (A,C) and active infection (B,D) for HIV (A,B) and HCV (C,D) in the pre-, post-session and long-term periods. Each sub-figure has a representation of the global rates broken down by medical and surgical departments. * Active HCV infection is defined as a positive HCV antigen.
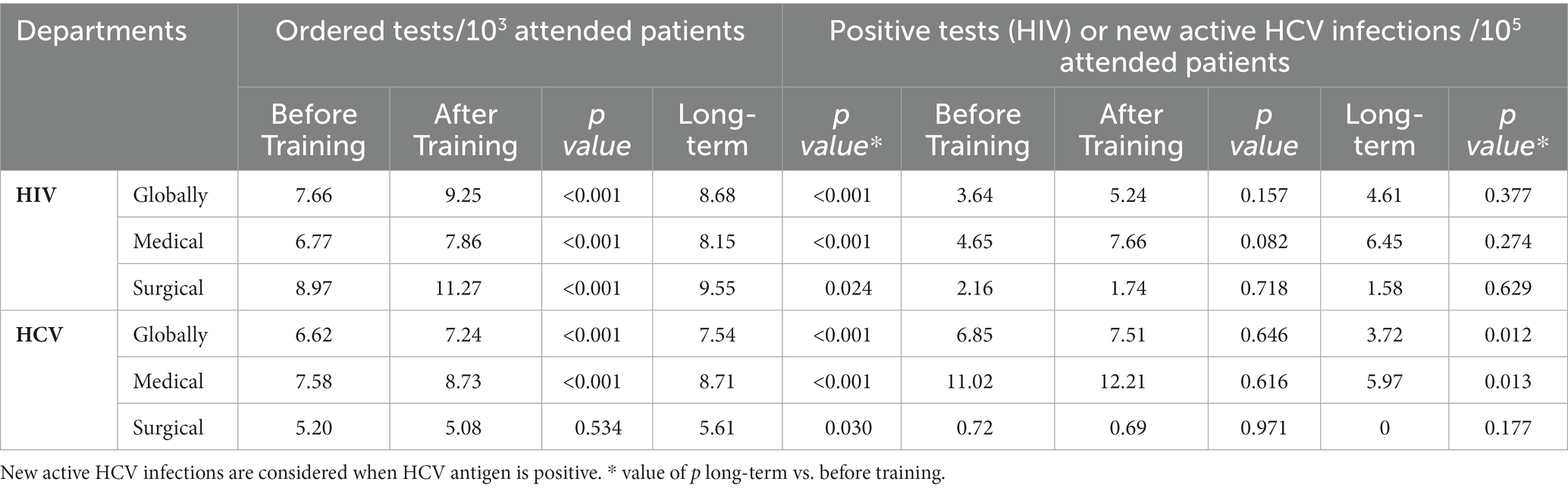
Table 1. HIV and HCV screening and active infection rates globally and split by medical and surgical departments.
For HCV, 4,541 pre-training and 5,113 post-training serologies were requested (6.6 vs. 7.2 tests per 103 attended patients, p < 0.001) with a significant increase in the screening rate in medical departments (+15.2%, p < 0.001) but not in surgical departments (p = 0.534; Figure 1; Table 1). Globally, HCV prevalence among the serologies requested was 3.3% before and 3.4% after training. A total of 47 pre-training and 53 post-training active HCV infections were diagnosed (positive HCV antigen), with a non-significant 9.6% increase in the active infection rate after the training (global active infection rate 6.9 vs. 7.5 per 105 attended patients, p = 0.646; Figure 1; Table 1).
A total of 5,832 HIV tests were requested in the long-term period with a global increase of 13.5% as compared to the pre-training period (7.7 vs. 8.7 tests per 103 attended patients; p < 0.001) (1.39 and 0.58 tests increase per 103 patients, respectively, in medical and surgical departments; p < 0.001 and 0.019, respectively; Figure 1; Table 1). We observed a non-significant 26.7% increase in HIV diagnoses (3.6 vs. 4.6 diagnoses per 105 attended patients; p = 0.377) driven only by medical departments (Figure 1; Table 1).
Overall, physicians increased their HCV screening rate by 13% as compared to the pre-session period (6.6 vs. 7.5 tests per 103 attended patients; p < 0.001; Figure 1, Table 1), with a non-significant increase of 10.9% in positive HCV serologies (22.1 vs. 24.6 per 105 attended patients; p = 0.284) (Table S5b), and a significant decrease in the rates of HCV active infection found (6.9 vs. 3.7 diagnoses per 105 attended patients; p = 0.012; Figure 1; Table 1). Detailed screening rates and diagnoses stratified by department can be found in the Supplementary Tables S4A,B for HIV and S5a, S5b, and S5c for HCV.
Implementing a one-hour teaching intervention for non-ID specialists in this tertiary hospital immediately increased the overall HIV and HCV testing rates, with a more significant effect seen in medical departments. This effect remained evident until at least 2 years after the training, although the impact in surgical departments was milder and wore out faster. This type of intervention has the potential to be widely implemented, as its duration corresponds with the formative sessions of most departments, covers direct and simple concepts, and can be adapted to each specific service. The questionnaire results showed a significant lack of knowledge regarding the testing guidelines.
The rates and absolute number of new HIV diagnoses were higher immediately and 2 years after the intervention. This increase, albeit moderate, has the potential to reduce the number of hidden HIV infections. The HCV diagnostic rates were similar before and after the session but steeply declined 2 years later.
Universal opt-out HIV testing programs offered to all general medical admissions in a hospital have proven effective in improving HIV diagnosis in several studies (19). Formative strategies have proven to be helpful in primary care (17, 18, 20). However, data on these strategies in hospital settings are scarce. We herein show that immediate rates of screening can rise after a simple 1-h training on screening guidelines and general sexually transmitted infections, and that hospital healthcare workers who take part in the sessions improve their willingness to screen for HIV/HCV both routinely and guided by risk factors.
Interestingly, significant differences were observed between the medical and surgical departments regarding their initial knowledge of the guidelines and willingness to order tests. These results could be explained by the fact that, in our hospital, preoperative tests are performed by anesthesiologists, while surgeons frequently rely on them for pre-surgical blood tests. Despite this, our training session greatly impacted the surgeons’ attitudes toward HIV and HCV testing. However, excluding gynecologists and dermatologists, screening and diagnostic rates did not improve, and surgeons’ diagnostic rates remained very low throughout the observed periods. We do not have any evidence on the impact of this type of strategy in surgical departments to compare our results. Since anesthesiologists always have contact with surgical patients before surgery, focusing on improving their screening and diagnostic rates, both with formative sessions and including the tests routinely in preoperative protocols (21), could be more valuable than improving the rates for surgeons.
Although a clear increase was observed in HIV and HCV screening rates, the growth in the rates of active infection found after training was mild, probably due to the low prevalence of infection in the observed population. Nevertheless, HCV screening reached a maximum during the post-training period and declined sharply thereafter. This could be due to the overall low number of diagnoses but also to the decline in the global number of HCV infections in Madrid Region since 2017 and, more importantly, since 2019 (22, 23), Reporting delay due to the COVID-19 pandemic could explain this substantial reduction in the rate of active HCV infection. Moreover, this could also be due to the availability of direct antivirals. These treatments were included by the Spanish Health System in 2014 with many restrictions (24), but by 2017, the use of pangenotypic treatments was extended to any infected patient (25, 26), making Spain the leading country in HCV-treated patients per million inhabitants in 2022, and one of the top contenders to achieve HCV eradication in the present decade (27).
Spain managed to reach two of (Joint United Nations Programme on HIV/AIDS (UNAIDS) 90% goals in 2020, coming short only in the diagnostic goal (28, 29); Therefore, different strategies should be pursued to achieve the 95% goals set by UNAIDS in 2030. Given the latest estimations, Madrid’s current HIV prevalence is 0.33% (30), and 13% of the patients remain undiagnosed (29); hence, we can estimate that approximately 250 patients could remain HIV undiagnosed in our health area. Our session on its own managed to increase the rate of HIV diagnoses 1.6 per 105 attended patients), which would mean diagnosing eight new patients in our assigned population. The results of this easy and reproducible intervention would allow us to diagnose more than 3% of the undiagnosed patients in our population and help progressively reduce the burden of hidden HIV infection. Given that HIV screening is cost-effective, the increase in the number of serologies requested is not expected to have a negative impact on the health system.
Thus far, no strategies based on training sessions to hospital physicians had demonstrated effectiveness up to now (19, 31, 32). Our results demonstrate an easy and feasible way to increase HIV and HCV screening rates in the population. Combined with other strategies, they could be helpful in improving the rate of undiagnosed patients and avoiding missed opportunities for HIV and HCV testing at hospital facilities (13–15); the same way they have proven to be effective at community and primary care levels (17, 18).
Despite the hardwearing effect that can be seen in our study, the impact of a new session, months after the first session, focusing on the lack of each service, could be used to assess whether periodic training could help to further reduce the burden of hidden infections.
Our study has some limitations. First, the COVID-19 pandemic struck before the post-session observation was completed in some departments, so we were obliged to reduce the pre-and post-observation periods in some departments; however, it also disturbed the standard workflow up to the present day (33), and although mild, some effects could still be seen during the long-term period. Second, the positive impact of the training is not consistent between medical and surgical departments, as in the latter, the impact of the intervention is negligible, and further interventions must be implemented to improve screening rates. In addition, the absolute increases in screening rates and active infections are low, and it could be argued that its contribution to effectively decreasing the rate of hidden infections is limited. Although medical training in Spain is homogeneous, we were unable to collect data on participants’ prior HIV-specific training. Nevertheless, we demonstrate that a simple intervention can improve screening rates in several hospital departments and can be used to reduce the burden of hidden HIV and HCV diseases. Further multicenter studies should be conducted to assess whether these interventions can be extrapolated to other hospitals, and whether the intervention should be repeated periodically to consolidate its long-term effect.
In conclusion, a formative session for hospital physicians can improve HIV/HCV screening and diagnostic rates and therefore help eliminate both infections, although other strategies should also be explored. Different strategies to tackle surgeons’ and other medical specialties’ reluctance to test must be added to the formative session to automatize and personalize the different strategies in each department. More extensive multicenter studies are needed to confirm these results.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee at University Hospital Ramón y Cajal (Y2VpYy5ocmNAc2FsdWQubWFkcmlkLm9yZw==) with ID number 001-23. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
MV-G, SM, and MP-E designed the study. AG-R and JM-S performed the research and the statistical analyses. AG-R, JM-S, MV-G, SM, and MP-E wrote the original draft. JM-S, MV-G, MS-C, BR-H, FR, and MP-E gave the formative sessions. MV-D-P, MDV, CL, AG-S, and JG helped with the data collection. All authors contributed to the article and approved the submitted version.
This study has been funded by unrestricted grants 2018/0371, 2021/0193 and 2019/034 and by Instituto de Salud Carlos III (ISCIII) through the project PI22/01878, the Spanish Ministry of Science and Innovation and co-funded by the European Union.
To all the physicians that collaborated giving the sessions and those who attended them.
AG-R reports personal fees for educational events and non-financial support, including support for attending meetings and/or travel from ViiV Healthcare, Gilead Sciences, Merck Sharp & Dohme and Abbvie, outside the submitted work. JM-S reports personal fees for presentations or educational events and non-financial support, including support for attending meetings and/or travel, from ViiV Healthcare, Janssen Cilag, Gilead Sciences, Merck Sharp & Dohme and Abbvie outside the submitted work. MV-G has received honoraria (grants and personal fees) as a speaker in educational programs sponsored by ViiV, and Gilead; and has received support (registration, travel assistance) for expert courses and congresses by MSD and ViiV. BR-H has received funding to attend conferences from Gilead Sciences and obtained a financed project from Roche. SM has been involved in speaking activities and received grants for research from Gilead Sciences, Janssen Cilag, Merck, Sharp & Dohme and ViiV Healthcare. MP-E has received funding to attend conferences, educational activities or advisory, as well as scholarships from the pharmaceutical companies Gilead Sciences, Janssen, Abbvie, MSD, and ViiV. JG has received funding to attend conferences, educational activities or advisory, from the pharmaceutical companies Gilead Sciences, Abbvie, Abbott, MSD and Roche.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1136988/full#supplementary-material
HCV, Hepatitis C virus; HIV, Human Immunodeficiency Virus; ID, infectious diseases; COVID-19, Coronavirus Disease 2019; IQR, interquartile range; vs, versus; UNAIDS, Joint United Nations Programme on HIV/AIDS.
1. WHO. WHO - hepatitis C infography. Available at: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (Accessed October 5, 2022).
2. European Centre for Disease Prevention and Control, WHO Regional Office for Europe. HIV/AIDS surveillance in Europe 2021. 2020 data. (2021) Available at: https://www.ecdc.europa.eu/sites/default/files/documents/2021-Annual_HIV_Report_0.pdf (Accessed October 5, 2022).
3. Sobrino-Vegas, P, Miguel, LG-S, Caro- Murillo, AM, Miro, JM, Viciana, P, Tural, C, et al.. Delayed diagnosis of HIV infection in a multicenter cohort: prevalence, risk factors, response to HAART and impact on mortality. Curr HIV Res (2009) 7:224–230. doi: 10.2174/157016209787581535
4. Lundgren, JD, The INSIGHT START Study Group. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med. (2015) 373:795–807. doi: 10.1056/NEJMoa1506816
5. Rodger, AJ, Cambiano, V, Phillips, AN, Bruun, T, Raben, D, Lundgren, J, et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive PARTNER taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. Lancet. (2019) 393:2428–38. doi: 10.1016/S0140-6736(19)30418-0
6. Janjua, NZ, Chong, M, Kuo, M, Woods, R, Wong, J, Yoshida, EM, et al. Long-term effect of sustained virological response on hepatocellular carcinoma in patients with hepatitis C in Canada. J Hepatol. (2017) 66:504–13. doi: 10.1016/j.jhep.2016.10.028
7. Ministerio de Sanidad G de E. Guía de cribado de la infección por el VHC. (2020) Available at: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/docs/GUIA_DE_CRIBADO_DE_LA_INFECCION_POR_EL_VHC_2020.pdf (Accessed October 6, 2022).
8. Plan Nacional sobre el Sida, Ministerio de Sanidad C y BSocial. Guía para la realización de pruebas rápidas del VIH en entornos comunitarios. (2019) Available at: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/docs/realizacionPrsRapidasVIH_Accesible.pdf (Accessed October 6, 2022).
9. Ministerio de Sanidad SS Plan Nacional sobre Sida. Guía de recomendaciones para el diagnóstico precoz de VIH en el ámbito sanitario. (2014) Available at: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/docs/GuiaRecomendacionesDiagnosticoPrecozVIH.pdf (Accessed October 6, 2022).
10. Marih, L, Sawras, V, Pavie, J, Sodqi, M, Malmoussi, M, Tassi, N, et al. Missed opportunities for HIV testing in patients newly diagnosed with HIV in Morocco. BMC Infect Dis. (2021) 21:48. doi: 10.1186/S12879-020-05711-2
11. Ellis, S, and Curtis, H. Edmund LC Ong, on behalf of the British HIV Association (BHIVA) and BHIVA clinical audit and standards sub-committee. HIV diagnoses and missed opportunities. Results of the British HIV Association (BHIVA) national audit. Clinical Medicine (2012). (2010) 12:430–4. doi: 10.7861/clinmedicine.12-5-430
12. Deblonde, J, van Beckhoven, D, Loos, J, Boffin, N, Sasse, A, Nöstlinger, C, et al. HIV testing within general practices in Europe: a mixed-methods systematic review. BMC Public Health. (2018) 18:1191. doi: 10.1186/S12889-018-6107-0
13. Burke, RC, Sepkowitz, KA, Bernstein, KT, Karpati, AM, Myers, JE, Tsoi, BW, et al. Why don’t physicians test for HIV? A review of the US literature. AIDS. (2007) 21:1617–24. doi: 10.1097/QAD.0B013E32823F91FF
14. Stanley, K, Lora, M, Merjavy, S, Chang, J, Arora, S, Menchine, M, et al. HIV prevention and treatment: the evolving role of the emergency department. Ann Emerg Med. (2017) 70:562–572.e3. doi: 10.1016/j.annemergmed.2017.01.018
15. Zheng, MY, Suneja, A, Chou, AL, and Arya, M. Physician barriers to successful implementation of US preventive services task force routine HIV testing recommendations. J Int Assoc Provid AIDS Care. (2014) 13:200–5. doi: 10.1177/2325957413514276
16. Agustí, C, Montoliu, A, Mascort, J, Carrillo, R, Almeda, J, Elorza, JM, et al. Missed opportunities for HIV testing of patients diagnosed with an indicator condition in primary care in Catalonia. Spain Sex Transm Infect. (2016) 92:387–92. doi: 10.1136/SEXTRANS-2015-052328
17. Martínez-Sanz, J, Vivancos, MJ, Sánchez-Conde, M, Gómez-Ayerbe, C, Polo, L, Labrador, C, et al. Hepatitis C and HIV combined screening in primary care: a cluster randomized trial. J Viral Hepat. (2021) 28:345–52. doi: 10.1111/JVH.13413
18. Gómez-Ayerbe, C, Martínez-Sanz, J, Muriel, A, Elías, PP, Moreno, A, Barea, R, et al. Impact of a structured HIV testing program in a hospital emergency department and a primary care center. PLoS One. (2019) 14:e0220375. doi: 10.1371/JOURNAL.PONE.0220375
19. Desai, S, Tavoschi, L, Sullivan, AK, Combs, L, Raben, D, Delpech, V, et al. HIV testing strategies employed in health care settings in the European Union/European economic area (EU/EEA): evidence from a systematic review. HIV Med. (2020) 21:163–79. doi: 10.1111/HIV.12809
20. Martínez-Sanz, J, Pérez Elías, MJ, Muriel, A, Ayerbe, CG, Vivancos Gallego, MJ, Sanchez Conde, M, et al. Outcome of an HIV education program for primary care providers: screening and late diagnosis rates. PLoS One. (2019) 14:e0218380. doi: 10.1371/JOURNAL.PONE.0218380
21. McGowan, DR, Norris, JM, Smith, MD, and Lad, M. Routine testing for HIV in patients undergoing elective surgery. Lancet. (2012) 380:e5. doi: 10.1016/S0140-6736(12)61537-2
22. Red de Vigilancia Epidemiológica, Subdirección General de Vigilancia en Salud Pública, Comunidad de Madrid INFORME EPIDEMIOLÓGICO SEMANAL COMUNIDAD DE MADRID. Available at: https://www.comunidad.madrid/servicios/salud/vigilancia-epidemiologica (Accessed December 3, 2022).
23. Centro Nacional de Epidemiología, Instituto de Salud Carlos III. Vigilancia epidemiológica de la Hepatitis C en España. (2022) Available at: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/archivos%20A-Z/Hepatitis%20C/Vigilancia_HepatitisC_2020.pdf (Accessed December 3, 2022).
24. AEMPS. Ministerio de Sanidad SS e I. INFORME DE POSICIONAMIENTO TERAPÉUTICO PT-SOFOSBUVIR/V1/01112014. (2014) Available at: https://www.aemps.gob.es/medicamentosUsoHumano/informesPublicos/docs/IPT-sofosbuvir-sovaldi.pdf (Accessed November 9, 2022).
25. Ministerio de Sanidad SS e I. INFORME DE SITUACIÓN DEL PLAN ESTRATÉGICO PARA EL ABORDAJE DE LA HEPATITIS C CRÓNICA PRESENTADO AL CONSEJO INTERTERRITORIAL DEL SNS JUNIO 2017 SECRETARÍA GENERAL DE SANIDAD Y CONSUMO. (2017). Available at: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/hepatitisC/PlanEstrategicoHEPATITISC/docs/informeSituacionPEAHCPresentadoCISNS_Jun2017.pdf (Accessed November 9, 2022).
26. AEMPS - Ministerio de Sanidad SS e I. Informe de Posicionamiento TerapÉutico de sofosbuvir/velpatasvir (Epclusa) en hepatitis C. (2017) Available at: https://www.aemps.gob.es/medicamentosUsoHumano/informesPublicos/docs/IPT-sofosbuvir-velpatasvir-Epclusa-hepatitisC.pdf (Accessed November 9, 2022).
27. Homie Razavi, Yuri Sanchez Gonzalez, Andreas Pangerl, Markus Cornberg. Global timing of hepatitis C virus elimination: estimating the year countries will achieve the World Health Organization elimination targets. (2019) AASLD/EASL HCV special conference (2019) Available at: https://cdafound.org/content/Posters/Global%20timing%20of%20HCV%20elimination%20Final.pdf (Accessed November 9, 2022).
28. UNAIDS. Understanding fast-track: accelerating action to end the AIDS epidemic by 2030. (2015) Available at: https://www.unaids.org/sites/default/files/media_asset/201506_JC2743_Understanding_FastTrack_en.pdf (Accessed October 28, 2022).
29. Centro Nacional de Epidemiología, Instituto de Salud Carlos III, Plan Nacional sobre el Sida, Dirección General de Salud Pública. Unidad de vigilancia del VIH, ITS y hepatitis. Actualización del continuo de atención del VIH en España. (2020) Available at: [https://www.sanidad.gob.es/en/ciudadanos/enfLesiones/enfTransmisibles/sida/vigilancia/ESTIMACION_DEL_CONTINUO_DE_ATENCIoN_DEL_VIH_EN_ESPAnA_Nov2020.pdf]
30. Informe Epidemiológico Vigilancia VIH/SidaRed de Vigilancia Epidemiológica Comunidad de Madrid.. (2022) Available at: https://www.comunidad.madrid/sites/default/files/doc/sanidad/epid/informe_mensual_vih_web.pdf (Accessed November 25, 2022).
31. Hine, P, Wolujewicz, A, Chalwa, A, Atkin, M, and Chaponda, M. The effect of hospital-wide and departmental teaching events on HIV testing rates over time. Poster Abstracts HIV Med. (2015) 16:12–77. doi: 10.1111/hiv.12265
32. Hulley, J.L., and Nurse, K.. HIV: are we testing appropriately? EuroTEST, HepHIV 2017 Malta Conference (2017) Poster category:
33. Romero-Hernández, B, Martínez-García, L, Rodríguez-Dominguez, M, Martínez-Sanz, J, Vélez-Díaz-Pallarés, M, Pérez Mies, B, et al. The negative impact of COVID-19 in HCV, HIV, and HPV surveillance programs during the different pandemic waves. Front Public Health. (2022) 10:80435. doi: 10.3389/FPUBH.2022.880435
Keywords: formative session, hospital intervention, HIV testing, HCV testing, screening, missed opportunities, late diagnosis, diagnostic screening programs
Citation: García-Ruiz de Morales AG, Martínez-Sanz J, Vivancos-Gallego MJ, Sánchez-Conde M, Vélez-Díaz-Pallarés M, Romero-Hernández B, Vázquez MDG, de Luque CMC, González-Sarria A, Galán JC, Rodríguez FG, Moreno S and Pérez-Elías MJ (2023) HIV and HCV screening by non-infectious diseases physicians: can we improve testing and hidden infection rates? Front. Public Health. 11:1136988. doi: 10.3389/fpubh.2023.1136988
Edited by:
Mamta K. Jain, University of Texas Southwestern Medical Center, United StatesReviewed by:
Héctor Armando Rincón León, Mexican Social Security Institute (IMSS), MexicoCopyright © 2023 García-Ruiz de Morales, Martínez-Sanz, Vivancos-Gallego, Sánchez-Conde, Vélez-Díaz-Pallarés, Romero-Hernández, Vázquez, de Luque, González-Sarria, Galán, Rodríguez, Moreno and Pérez-Elías. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alejandro G. García-Ruiz de Morales, YWxlamFuZHJvZ2FyY2lhZ2FyY2lhQGdtYWlsLmNvbQ==; Javier Martínez Sanz, amF2aWVyLm1hcnRpbmV6LnNhbnpAc2FsdWQubWFkcmlkLm9yZw==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.