
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 04 July 2023
Sec. Public Health Education and Promotion
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1129056
 Seyed Hassan Nikookar1
Seyed Hassan Nikookar1 Mahmood Moosazadeh2
Mahmood Moosazadeh2 Mahmoud Fazeli-Dinan1
Mahmoud Fazeli-Dinan1 Morteza Zaim3Mohammad Mehdi Sedaghat3Ahmadali Enayati4*
Morteza Zaim3Mohammad Mehdi Sedaghat3Ahmadali Enayati4*Background: Dengue fever is a rapidly emerging infection worldwide with a high public health burden. Adequate training of healthcare workers is essential to warrant the timely provision of health services to improve the outcome of dengue management.
Methods: This is an analytical cross-sectional study, conducted to assess the knowledge, attitudes and practice (KAP) of healthcare workers regarding dengue from April 2021 to March 2022 in Mazandaran Province, northern Iran. Data was collected using a researcher-made structured questionnaire, prepared as Google Forms, and sent to target groups through social media and email. Data analysis was performed by SPSS 22 software using descriptive and inferential statistics (Chi-square) at a significant level of 5%.
Results: Most of the respondents had heard about dengue (83.8%); media (32.7%) and academic education (25%) were the main sources of information. Respondents had less knowledge associated with dengue symptoms (52%) than prevention and control (69%), transmission (72.2%) and clinical management (81%). Based on the 70% cut-off point, the majority of the participants had a good attitude (81%) and practice (73%). However, only 49.6% of the respondents showed good practice regarding dengue local transmission. A significant difference was observed between participants knowledge on clinical management with occupation; attitude with gender and occupation; and practice with gender (p < 0.05).
Conclusion: The results of this study revealed gaps in some dimensions of KAP in healthcare workers, therefore, a greater focus should be placed on future training programs to raise knowledge and attitude leading to sound practice and behavior for adequate management of dengue.
Dengue fever (DF) is considered a global public health concern as it is the fastest-growing vector-borne disease over the past five decades (more than 30-fold) in the world (1). The disease is caused by a single-stranded positive-sense RNA virus, a member of the family Flaviviridae and genus Flavivirus (2). There are four distinct immunologically related serotypes of the virus. It is believed that recovery from infection provides lifelong immunity to that serotype, but does not provide cross-protective immunity against each other (3). Although dengue is a self-limiting disease, some patients may progress to severe and life-threatening stages such as dengue hemorrhagic fever or dengue shock syndrome, with a relatively high fatality rate (4). In addition to complications and mortality, dengue can impose a significant economic burden on infected individuals and countries (5), highlighting the importance of the problem.
The first dengue epidemic in Asia, Africa, and North America was recorded between 1779 and 1780. The almost simultaneous outbreak in three continents shows that the virus and its vectors have been distributed around the world in tropical and subtropical regions for more than 200 years. The dengue pandemic began in Southeast Asia after World War II and has since expanded across the world (6). At present, 3.9 billion people are at risk of dengue infection in tropical and subtropical areas (7), with an estimated 390 million cases annually (8), in about 128 countries around the world (7).
Dengue has been an emerging concern in Iran since 2008 when the first imported case was detected in a 58-year-old woman with a history of travel to Malaysia (9). After that, in a retrospective study on suspected cases of Crimean-Congo haemorrhagic fever (CCHF) with haemorrhagic symptoms, 15 probable dengue cases were detected, 8 had a history of travel to Malaysia, India and Thailand, and in 7 cases, the history of travel was not clear, of which 6 cases were from Sistan and Baluchestan Province (10). Reports of imported (11) and suspicious local cases (12) of dengue has been increasing in recent years in Iran. In addition, the presence of dengue vectors, i.e., Ae. aegypti and Ae. albopictus have been documented in Iran in recent years, highlighting a major concern. In 2008 and 2013, Ae. albopictus was reported but not established in Sistan and Baluchestan Province. However, Ae. aegypti, the main vector of dengue fever, has been introduced and established in Hormozgan Province, South of Iran (13, 14). To date, no local transmission of the disease is evident in Iran, however, given the establishment of Ae. aegypti in southern Iran and the outbreaks/epidemics of dengue in neighboring countries (15, 16), as well as significant travel of Iranians to endemic countries (17), Iran is at risk of dengue epidemics.
Mazandaran ecosystem and weather conditions attract tourists and at the same time provide ideal breeding places for mosquito vectors. There are an international airport and three ports that link the province with Eurasia through the Volga Don Canal (18). In addition, high travel and trade between Mazandaran and Hormozgan Province, where Ae. aegypti has newly been established, predispose the province for the entry and spread of Aedes vectors and dengue transmission.
Since there is no effective vaccine and specific treatment for the disease, health education and vector control are considered the most important tools for dengue prevention and control. Education of healthcare workers is crucial as they are responsible for prevention (4), control and management of the disease. Capacity is defined as “the ability to carry out stated objectives” (19). “Capacity building” is a systematic process of education, human resources development, individual, collective and organizational knowledge management for the continuous development and improvement of the competencies and capabilities of health personnel, health organization and health system for timely identification, evaluation, selection and application of disease prevention and management protocols (20). For this end, in the past years (before the present study), training workshops and seminars in the form of continuing medical education were held for the healthcare workers in almost all priority provinces regarding dengue fever. The main goal of these workshops was change in the behavior of the healthcare workers to provide adequate services (21). As there are no studies regarding KAP of dengue in Iran, this study is undertaken for the first time to assess the impact of previous health education programs and to plan for further education of healthcare workers regarding the disease and its prevention and control.
Mazandaran Province is laid in northern Iran between 50°34′–54°10′E and 35°47′–36°35′N, with an area of approximately 23,842 square kilometers and a population of approximately 3,283,582. The province is surrounded by Golestan Province in the East, Guilan Province in the West, Tehran and Semnan Provinces in the South, and the Caspian Sea to the North. Sari is the capital city of the province. The main occupation of the people of the region is agriculture (rice cultivation), horticulture and animal husbandry (cattle, sheep and goats), poultry and fishing. The province is the most popular tourist destination for its natural and historical attractions. There are three active maritime ports and an international airport in the province. The suitable ecosystem and also the points of entry of the province are causes for concern for the entry and spread of the Aedes vectors from the northern regions to the country.
This is an analytical cross-sectional study, designed in June 2020 after holding workshops and continuing medical education for the health personnel of health centers of the province regarding dengue fever and its vectors. The actual study was conducted to assess KAP in healthcare workers regarding dengue in Mazandaran Province from April 2021 to March 2022 followed by data analysis and synthesis of the results and conclusion in 2023. The individuals who are involved in the diagnosis, prevention, control and management of dengue; and have electronically given consent to take part in the study are eligible to be enrolled in the study population. It includes physicians (n = 853), diseases control staff (n = 186), environmental health engineering (n = 384) and health education (n = 450). The level of education of the respondents was bachelor and master degree for the health experts (i.e., health staff) and general practitioner for the physicians. Considering a 50% knowledge, a 6% margin of error, and a 95% confidence interval, the sample size was calculated 267 according to the sample size formula to estimate proportion or prevalence. However, in practice 284 participants filled in the questionnaires.
The study was designed and planned in two phases, i.e., 1: the questionnaire design and 2: the assessment. In the first phase, a questionnaire was constructed using literature on dengue KAP studies (22) and expert opinions. The questionnaire consisted of four sections: (1) demographic information (gender, workplace, occupation and health information relating to whether the respondent had heard about dengue or not); (2) knowledge of symptoms, transmission routes, clinical management, prevention and control of the disease; (3) attitude towards dengue; (4) preventive measures against dengue, e.g., methods used to reduce breeding places, and potential human-mosquito contact (repellents, bed nets and etc.). The reliability and validity of the questionnaire were evaluated to determine the most appropriate phrases with Cronbach’s alpha coefficient and quantitative-qualitative face and content validity, the results of which was published earlier (23). The English version of the survey instrument is available in appendix 1. In the second phase, the questionnaire was transformed into the Google Forms, and its link was made available to the healthcare workers (health experts and doctors) on the website of the health department. An administration team was devised and followed up the whole process of data collection including sending monthly reminders through social media (WhatsApp) and e-mails to the study participants as well as dealing with the respondents in case any assistance deemed necessary. The study period was coincided with the COVID-19 that caused some limitations in data collection, therefore, available individuals were recruited and enrolled in the study.
All completed questionnaires were double-checked and confirmed for structural completion and compatibility. KAP assessment was executed using a scoring system. In Knowledge and practice assessment, responses to questions were coded such that correct answers (supported by current literature) were scored 1 and incorrect answers were scored 0. The total score for knowledge and practice was 50 and 16, respectively. Knowledge was assessed based on the questions grouped under the following four categories: Knowledge regarding (1) symptoms (2) transmission (3) clinical management (4) prevention and control. For attitude, a five-point Likert-like scale was applied to answers to the questions, i.e., 1 = strongly disagree; 2 = somewhat disagree; 3 = neither agree nor disagree; 4 = somewhat agree; and 5 = strongly agree. The attitude score was computed as the sum of the participant’s correct responses. A range of cut-offs for the different components of KAP (70–75%) was devised and used by other researches (24), therefore, in this study a cut-off point of 70% was set to differentiate between the groups “poor” and “good” KAP; the respondents were considered to have adequate knowledge, attitude and practice if the score in each was above 70%.
The obtained data were analyzed using descriptive statistics (frequency, mean and standard deviation) and inferential statistics (Chi-square). SPSS software version 22 was used for the analysis value of p ≤0.05 was considered statistically significant.
A total of 284 participants successfully filled in and returned the questionnaire, of whom 66.2% were female. Most of the study population were health experts (60.9%%) and the rest were physicians (39.1%). The majority worked in the public health sector (87.7%) and stated that they had heard of dengue (83.8%) (Table 1). Regarding the information sources about dengue fever (Figure 1), most participants reported that they heard about dengue fever through media (32.7%) and academic education (25%) followed by continuing education (11.1%), workshops (4%), academic education plus media (3.9%).
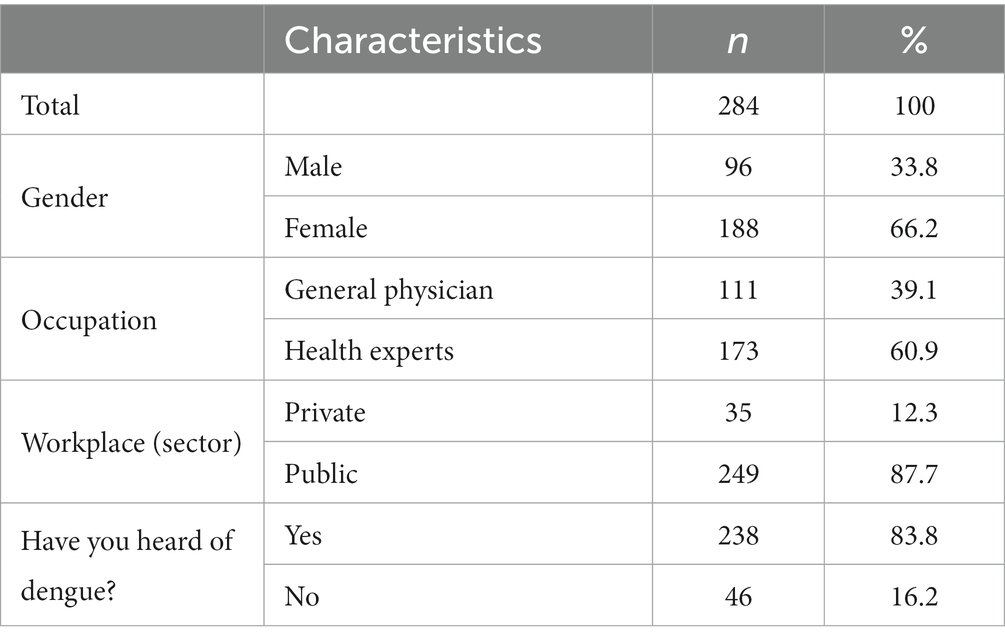
Table 1. Demographic characteristics of healthcare workers participating in the knowledge, attitude and practice study on dengue disease in Mazandaran Province, northern Iran, 2022.
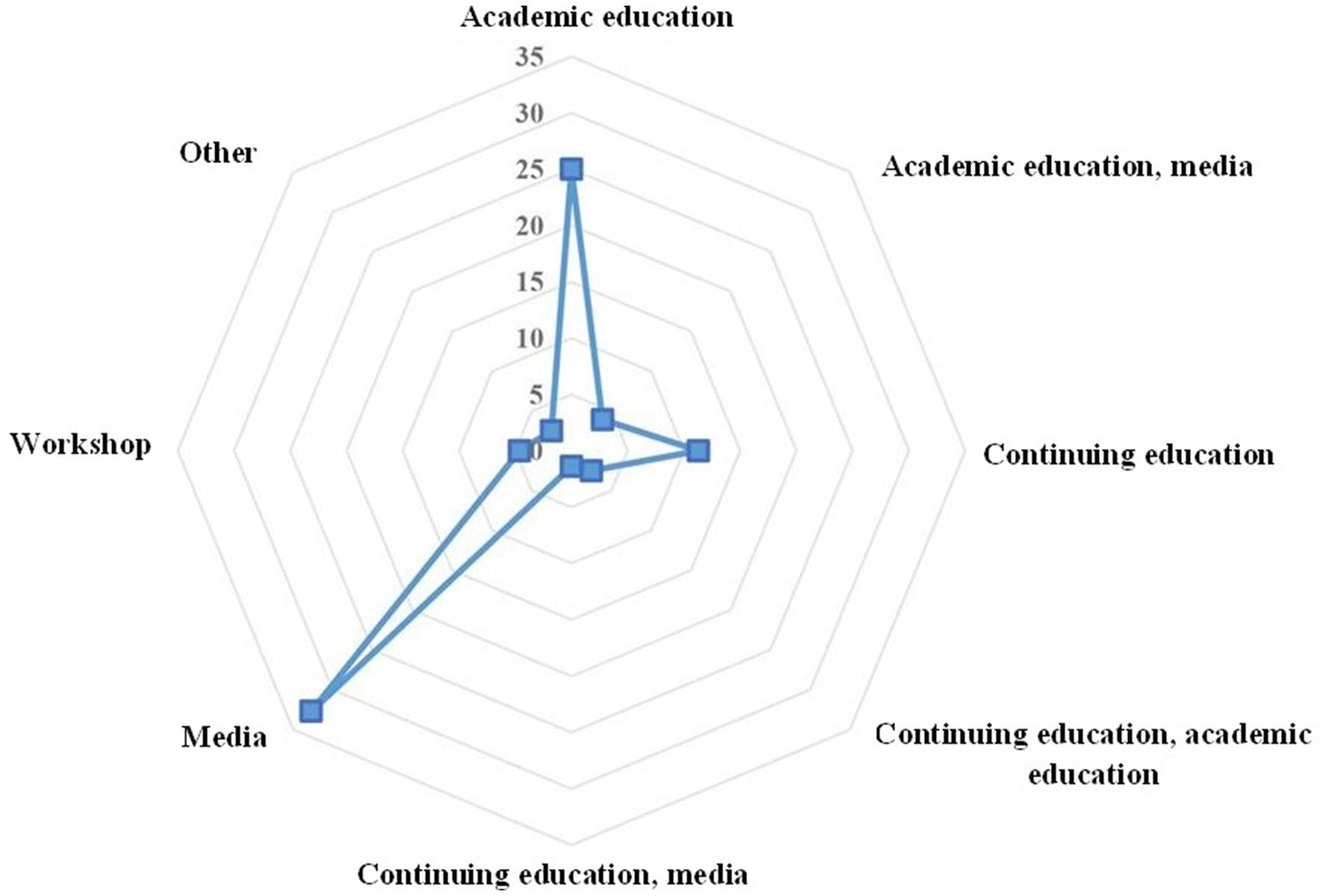
Figure 1. Source of information on dengue fever among healthcare workers in Mazandaran Province, northern Iran, 2022.
More than half of the participants (n = 149, 52.5%) were able to correctly identify general symptoms of dengue disease such as fever, headache, joint and muscle pain, pain behind the eyes, rash and abdominal pain. Fifty-three percent of females, 56.8% (n = 63) of physicians, 65.7% (n = 23) of those in the private sector responded correctly to the questions regarding the symptoms of dengue.
Seventy-two percent of respondents were aware of the fact that Aedes mosquitoes are the main vector of dengue, mostly transmitted during the day by biting Aedes. The knowledge regarding transmission was 71.9% (n = 179) in public sector, 74.3% (n = 26) in private sector, and 77.1% (n = 74) in male, 69.7% (n = 131) in female, and 69.9% (n = 121) in health experts and 75.7% (n = 84) in physicians.
Eighty-one percent (n = 230) and 69% (n = 196) of the respondents knew about clinical management and prevention and control of dengue disease, respectively. There was no significant difference between the respondents’ knowledge about symptoms, transmission, or clinical management of dengue based on workplace demographic variables and gender, while it was statistically significant between physicians and health experts (90.1% vs. 75.1%, respectively, p = 0.001) regarding clinical management, and the private and public sectors (85.7% vs. 66.7%, respectively, p = 0.015) regarding disease prevention and control (Table 2).
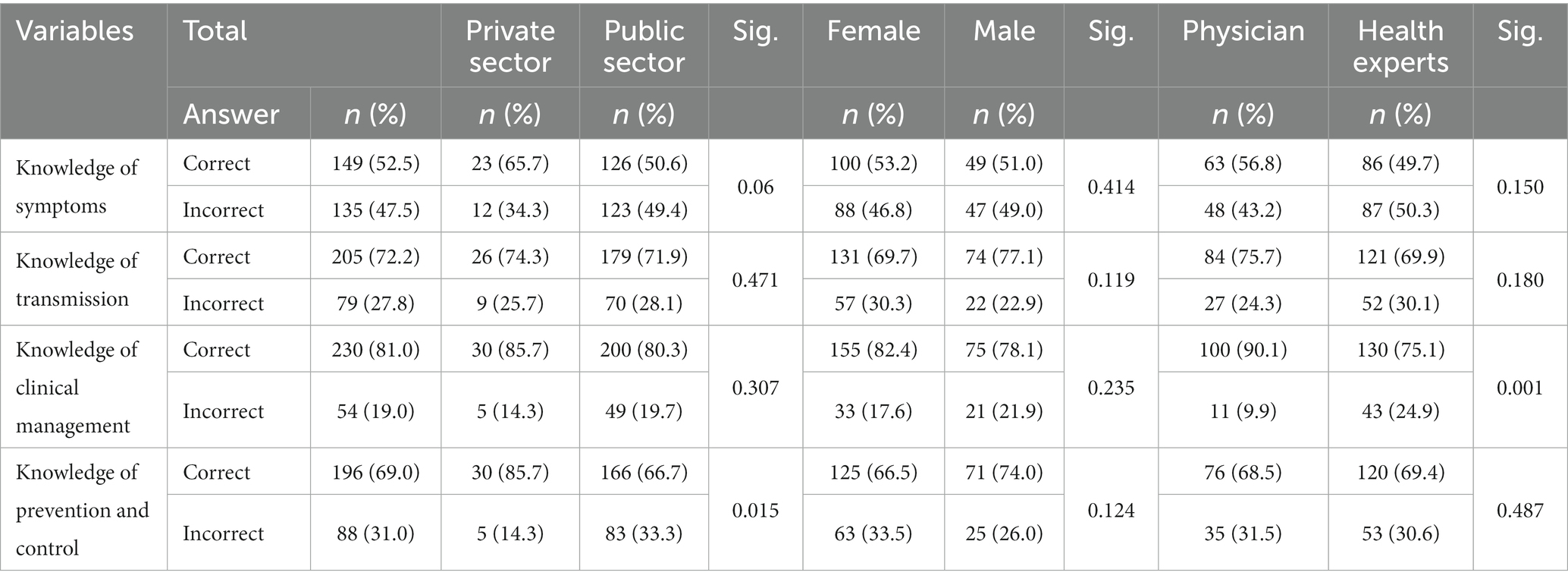
Table 2. Knowledge on symptoms, transmission, clinical management and prevention of dengue fever (DF) among healthcare workers in Mazandaran Province, northern Iran, 2022.
Table 3 shows that the majority of the respondents strongly agreed (47.2%) and agreed (46.8%) that dengue is a dangerous illness with a significant difference between the private and public sectors (p = 0.05) and gender (p = 0.032). Eighty-seven percent had a positive attitude towards the fact that Iran is at risk of invasive vectors of dengue with a significant difference in gender (p = 0.007). The majority of the respondents strongly agreed/agreed (91.9%) that dengue is a preventable disease and source reduction of dengue vectors is a control strategy [strongly agreed (64.4%) and agreed (31.7%)], figures statistically different between health experts and physicians (p = 0.039).
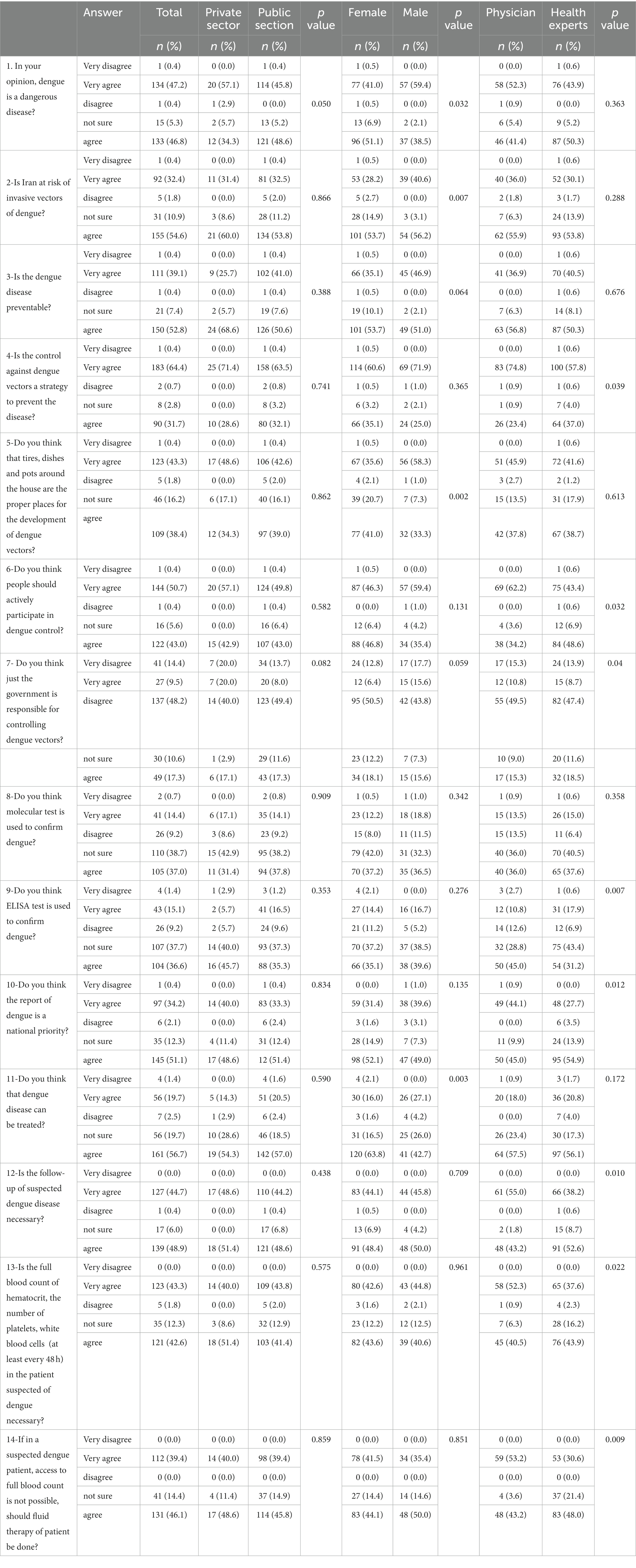
Table 3. Attitude towards dengue fever (DF) among healthcare workers in Mazandaran Province, northern Iran, 2022.
Eighty-one percent of respondents had a positive attitude about the fact that tires, containers, and pots around the houses are suitable places for the development of dengue vectors, which was statistically significant between men and women (p = 0.002). Sixty-two percent of the respondents believed that the government alone is not responsible for controlling dengue fever, and people should be actively involved (93.7%), which was statistically significant between physicians and health experts, while 26.8% considered that the government is solely responsible. Fifty-one percent of the respondents strongly agreed and agreed that PCR and ELISA techniques are used to confirm dengue and 38% were not sure. Seventy-six percent believed that dengue is treatable, with a significant difference in gender (p = 0.003), and its reporting should be a national priority (85.3%). Most respondents (93.6%) believed that follow-up of a patient with suspected dengue is a necessity and that a complete blood count should be done at least every 48 h (85.9%), and if this was not possible, fluid therapy should be initiated in a patient with warning signs (85.5%), which was statistically significant between physicians and health experts (p = 0.05). There was no significant difference in the attitude of respondents in the public and private sectors regarding ELISA technique (Table 3).
The result of dengue-related practice is shown in Table 4. Seventy-three percent of the respondents knew what control measures would be appropriate in the scenario where dengue vectors are not yet establishment in the country. On the other hand, almost half of the respondents, of whom 53.7% were female, with a value of p of 0.03, answered correctly regarding control measures during local dengue transmission.
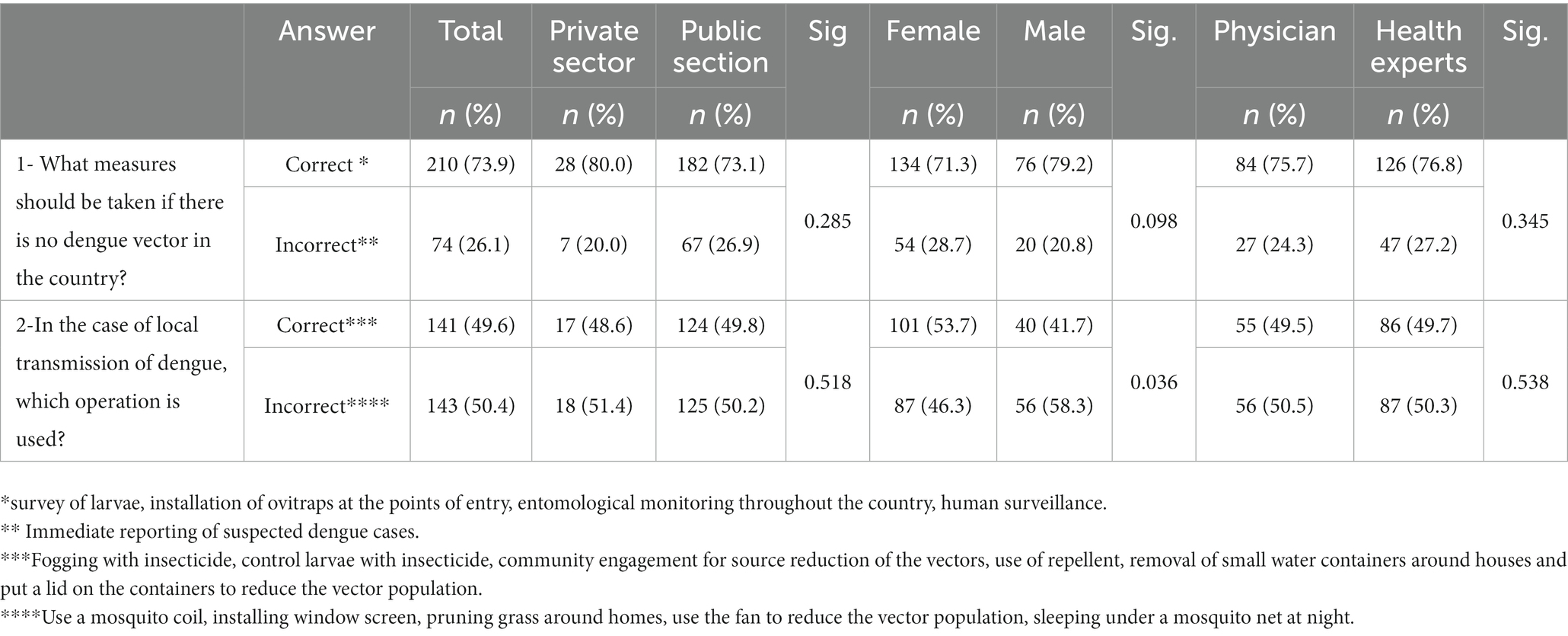
Table 4. Practice towards dengue fever (DF) among healthcare workers in Mazandaran Province, northern Iran, 2022.
Aedes-borne diseases, especially dengue fever, are considered important health issues in many tropical and subtropical countries due to the alarming increase in the number of infected people, disease burden and geographical spread (25). To adopt health development policies in society, increasing knowledge and practice of healthcare workers as well as the general population for mobilizing community actions in the development, maintenance and improvement of the collective and individual health of the people is very important and needed (26). Therefore, the assessment of KAP regarding dengue and its vectors is a research priority both in knowing the extent and impact of health education programs implemented in the past, and at the same time, to understand the health education and training needs of healthcare workers. As no study has been conducted to assess the knowledge, attitude and practice regarding dengue among any target groups in Iran, KAP of healthcare workers regarding dengue was assessed in the northern Province of Mazandaran where the modeling studies highlighted the high risk of the area for the entry and establishment of the invasive Aedes species (27).
The present study showed that most of the respondents had heard about dengue (83.8%), and media followed by academic education were the main sources of information. In a study conducted in several countries including India, Indonesia, Myanmar, the Philippines and Thailand, the vast majority of the respondents (> 90%) had heard of the disease in the media (28). Most respondents in other studies, reported that media had been their main source of information on dengue fever followed by healthcare providers (29, 30). This may indicate the important role of media as well as healthcare workers in providing health education programs to change behavior in the community. Despite the fact that a few workshops and continuing medical education were held in the Mazandaran Province about dengue and its vectors before the present study, only a limited number of respondents mentioned it as their source of information. It could probably be either because the participants in the workshops and continuing education did not pass on the information to the health personnel in a cascade education, or the information provided in the workshops and continuing education did not fully cover the relevant objectives. In accordance with our findings, systematic reviews have also highlighted that the effects of continuing medical education on professional practice and health care outcomes is variable and usually unsatisfactory (31, 32). Probably, newer forms of continuing medical education, for example, continuing professional development, are necessary in response to the needs of primary health care workers (4). Nevertheless, these gaps should be revised, planned or modified at the level of the country and/or province, which emphasizes the importance of further studies in this direction.
Our study revealed that healthcare workers had higher knowledge associated with the transmission, clinical management, and prevention and control of dengue compared with its symptoms. In accordance with the present study, several pieces of research conducted in Bangladesh, Malaysia, India and Turkey (33), India (30) and Nepal (1) reported poor knowledge about dengue fever symptoms (6). This lack of awareness of symptoms could be due to (1) the wide range of clinical manifestations observed in patients, (2) the focus of past educational campaigns on transmission, clinical management, and prevention and control rather than on symptoms and primary care, (3) and the disease may be easily confused with other common causes of fever, such as influenza, COVID-19, malaria, typhoid, etc. This has consequences of great importance, because referral to clinics and receiving timely medical care may be delayed until the appearance of severe complications (22, 34).
In contrast, many studies also stated that most participants have a good knowledge of dengue fever symptoms and were able to detect high fever, joint pain and headaches as the main symptoms of the disease (29, 35, 36). One reason for the discrepancy between the results of our study and those aforementioned studies might well be that dengue is not yet epidemic in Iran.
Although, there was a gap in knowledge about the symptoms of dengue diseases, healthcare workers had good knowledge about transmission, clinical management, and prevention and control. Most of them were aware of the transmission routes of dengue (72%) and knew that dengue is both rural and urban disease, which is mostly transmitted after dawn and before sunset by Aedes invasive species (37). In agreement with the present study, the same results were also found in other studies in Pakistan including in Punjab (83.8%) by Arif et al. (38), in Karachi (86.9%) by Itrat et al. (39) and in Malakand Khyber Pakhtunkhwa (81.2%) by Khana et al. (39). In contrast to our results, a study from Nepal reported that only 19% (1) of the respondents knew Aedes mosquitoes transmit Dengue fever (40).
In the present study, the majority of the respondents were aware of clinical management (82.1%), especially regarding the avoidance of aspirin during dengue compared to other studies in Jamaica (29.8%) (22) and Sri Lanka (42%) (24). Our findings on knowledge of prevention and control (69%) are consistent with those of other studies which reported a fairly good level of knowledge (41) but contrary to those that had reported a low level of Knowledge in this regard (42).
In our investigation, the majority of respondents were classified as having a good attitude (81%) according to the cut-off point described in the methodology (above 70%). This shows that most of them understood the risk of dengue in the country and seem to be ready to support and implement the dengue control programs and measures provided in Iran CDC guidelines for the prevention and control of invasive Aedes vectors (13). Similarly, in a study in Central Nepal, high attitude was reported among the healthy population of highland and lowland communities (1). In the present study, 62.6% the respondents had a suitable attitude that the government alone is not responsible for dengue control and believed that it is impossible to reduce the prevalence of dengue without community participation (43). In Karachi Pakistan, 61 % of the respondents believed that dengue control should be the responsibility of the government (44). In addition, there was also a low attitude in response to whether ELISA and PCR methods were suitable for dengue confirmation. Therefore, this reinforces the need to improve the level of respondents’ attitudes in these regards.
A significant difference was observed in the respondents’ knowledge about the clinical management of the disease between the physicians and health experts (p < 0.05), which is probably due to the fact that the physicians are more familiar with the relevant concepts than the health experts. This is supported by a study by Huang, Chiu (35). In terms of attitude and practice, females have shown a better attitude and practice than males in response to the questions (attitude: Q1,2,3,5,11) and (practice: Q2). It can be attributed to the higher attention and intension of females in receiving educational concepts due to their major role in households including worrying about children getting sick, collecting and storing water for domestic uses, and home environment sanitation in line with the fact that dengue vectors are mainly domestic and peri-domestic breeders (37). In conformity with our findings, gender as a predictor showed that females have better attitudinal and practical behavior than males (p < 0.05) (45, 46). In addition, physicians had a better attitude compared with health experts in response to the question (attitude: Q4,6,7,12,13,14), showing that they are more familiar with the relevant concepts than health experts. The attitude towards PCR and ELISA as diagnostic tools in physicians were less than the cut off of 70%, indicating the necessity of more emphasis on these elements in future continuing education.
In the present study, a translation of knowledge and attitude into practice was observed. Seventy-three percent of the respondents stated that a survey of larvae, installation of ovitraps at the points of entry, entomological surveillance across the country and disease surveillance are the most important strategies to prevent dengue when vectors of the disease are absent in the country. In a study conducted in Central Nepal by Dhimal et al., 90% of participants had translated their knowledge and attitude into actual practice (1). However, there was a difference in the translation of knowledge and attitude into practice in response to the question “What are the appropriate control operations in cases of local dengue transmission.” Forty-nine percent of the respondents stated that fogging with insecticide, controlling larvae with insecticide, promoting community participation to reduce vector breeding sites, use of repellents, removal of small water containers around houses and putting a lid on the containers are useful to reduce the population of mosquitoes.
In accordance with our research, less than half of the respondents with good knowledge about dengue had poor preventive practice, indicating that the translation from knowledge to practice was not properly implemented among the respondents (1, 22, 47). These researchers believed that the socioeconomic status of the participants was likely a limiting factor in translating knowledge into practice. Since there are no reports of local transmission of dengue in Iran, it likely had an impact on translating knowledge into practical measures among the respondents of the present study. Therefore, there is a concern that poor practice in some aspects along with high travel and trade, tourism, and suitable environmental conditions for the establishment and distribution of vector species, may put the province at greater risk. In addition, it should be noted that other parts of the country may be at risk of invasion of the dengue vectors, therefore, continuing education followed by KAP studies should be planned and implemented with priority in high risk provinces based on forecasting, entomological and remote sensing studies (27, 48).
As discussed, there were some discrepancies between the results of our study and those in the literature, which could be due to the different methodologies implemented in the studies including a difference in data analyses, scoring systems or cut off points for “poor” and “good” KAP, the focus of questions in the questionnaire and demographic background of the respondents. Also undertaking this study by virtual means during COVID-19 pandemic might have caused some of these discrepancies. Therefore, the comparison of the results of this research and those of the others should be interpreted with caution.
The present study provides important insights into the knowledge, attitude and practice of healthcare workers regarding dengue in northern Iran where it is considered a potential focus for the entry of invasive Aedes species and-related diseases. The results can help health authorities determine the level of KAP in the healthcare workers to be considered in planning for future training programs. This study showed that although the majority of the study population had good general knowledge, attitude and practice toward dengue, there were gaps in the knowledge of symptoms, the attitude of confirmation techniques (ELISA and PCR), and the role of government in control of dengue, and practice on what control measures are appropriate in case of local transmission of dengue in the country. Considering the importance of high levels of KAP in healthcare workers in providing adequate public health services, it is recommended to design and implement various educational interventions with the aim of improving the knowledge, attitude, and their translation into practice in healthcare workers about various dimensions of dengue, especially where there was a gap. Designing and implementation of the COMBI program for behavior change regarding dengue can also be beneficial.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Mazandaran University of Medical Sciences (with ethic code (IR.MAZMS.REC.1398.1107). The patients/participants provided their written informed consent to participate in this study.
AE, MZ, and SHN: conceptualization, visualization, supervision, and project administration. SHN and MF-D: methodology. SHN and MM: formal analysis. SHN: investigation, resources, data curation, and writing—original draft preparation. AE, MZ, and MMS: writing—review and editing. AE and SHN: validation. AE: funding acquisition. All authors contributed to the article and approved the submitted version.
This work was supported by the Vice-Chancellor of Research and Technology of Mazandaran University of medical Sciences [6053]. The funder of the study had no role in study design, data collection, data analysis, data interpretation, writing of the manuscript, or the decision to submit for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1129056/full#supplementary-material
1. Dhimal, M, Aryal, KK, Dhimal, ML, Gautam, I, Singh, SP, Bhusal, CL, et al. Knowledge, attitude and practice regarding dengue fever among the healthy population of highland and lowland communities in Central Nepal. PLoS One. (2014) 9:e102028. doi: 10.1371/journal.pone.0102028
2. Guzman, MG, Halstead, SB, Artsob, H, Buchy, P, Farrar, J, Gubler, DJ, et al. Dengue: a continuing global threat. Nat Rev Microbiol. (2010) 8:S7–S16. doi: 10.1038/nrmicro2460
3. WHO. (2023) Dengue and severe dengue 2023. Available at: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed 17 March 2023).
4. Ho, T-S, Huang, M-C, Wang, S-M, Hsu, H-C, and Liu, C-C. Knowledge, attitude, and practice of dengue disease among healthcare professionals in southern Taiwan. J Formos Med Assoc. (2013) 112:18–23. doi: 10.1016/j.jfma.2012.11.004
5. Shepard, DS, Coudeville, L, Halasa, YA, Zambrano, B, and Dayan, GH. Economic impact of dengue illness in the Americas. Am J Trop Med Hyg. (2011) 84:200–7. doi: 10.4269/ajtmh.2011.10-0503
6. Nalongsack, S, Yoshida, Y, Morita, S, Sosouphanh, K, and Sakamoto, J. Knowledge, attitude and practice regarding dengue among people in Pakse, Laos. Nagoya J Med Sci. (2009) 71:29–37.
7. Brady, OJ, Gething, PW, Bhatt, S, Messina, JP, Brownstein, JS, Hoen, AG, et al. Refining the global spatial limits of dengue virus transmission by evidence-based consensus. PLoS Negl Trop Dis. (2012) 6:e1760. doi: 10.1371/journal.pntd.0001760
8. Bhatt, S, Gething, PW, Brady, OJ, Messina, JP, Farlow, AW, Moyes, CL, et al. The global distribution and burden of dengue. Nature. (2013) 496:504–7. doi: 10.1038/nature12060
9. Mardani, M, Abbasi, F, Aghahasani, M, and Ghavam, B. First Iranian imported case of dengue. Int J Prev Med. (2013) 4:1075–7.
10. Chinikar, S, Ghiasi, SM, Shah-Hosseini, N, Mostafavi, E, Moradi, M, Khakifirouz, S, et al. Preliminary study of dengue virus infection in Iran. Travel Med Infect Dis. (2013) 11:166–9. doi: 10.1016/j.tmaid.2012.10.001
11. Ebrahimi, M, Abadi, A, Bashizadeh-Fakhar, H, and Fahimi, E. Dengue fever in Iran: a case report. Zahedan J Res Med Sci. (2016) In Press:e9953. doi: 10.17795/zjrms-9953
12. Heydari, M, Metanat, M, Rouzbeh-Far, M-A, Tabatabaei, SM, Rakhshani, M, Sepehri-Rad, N, et al. Dengue fever as an emerging infection in Southeast Iran. Am J Trop Med Hyg. (2018) 98:1469–71. doi: 10.4269/ajtmh.17-0634
13. Zaim, M, Enayati, A, Sedaghat, MM, and Goya, MM. Guide to prevention and control of Ae. Aegypti and Ae. Albopictus in Iran. 1st ed. Gorgan: Mazandaran University of Medical Sciences and Health Services Virasat (2020). 91 p.
14. Dorzaban, H, Soltani, A, Alipour, H, Hatami, J, Jaberhashemi, SA, Shahriari-Namadi, M, et al. Mosquito surveillance and the first record of morphological and molecular-based identification of invasive species Aedes (Stegomyia) aegypti (Diptera: Culicidae), southern Iran. Exp Parasitol. (2022) 236-237:108235. doi: 10.1016/j.exppara.2022.108235
15. Ahmad, S, Aziz, MA, Aftab, A, Ullah, Z, Ahmad, MI, and Mustan, A. Epidemiology of dengue in Pakistan, present prevalence and guidelines for future control. Int J Mosq Res. (2017) 4:25–32.
16. Elyan, DS, Moustafa, L, Noormal, B, Jacobs, JS, Aziz, MA, Hassan, KS, et al. Serological evidence of Flaviviruses infection among acute febrile illness patients in Afghanistan. J Infect Dev Ctries. (2014) 8:1176–80. doi: 10.3855/jidc.4183
17. Manouchehr, F, and Abadi, AA. Assessment and zoning of tourism climate of Iran using tourism climate index (TCI). Phys Geography Res Quarterly. (2010) 71:31–42.
18. Tennenbaum, J. The new Eurasian land-bridge infrastructure takes shape. Executive Intell Rev. (2001) 28:17–41.
19. Goodman, RM, Speers, MA, McLeroy, K, Fawcett, S, Kegler, M, Parker, E, et al. Identifying and defining the dimensions of community capacity to provide a basis for measurement. Health Educ Behav. (1998) 25:258–78. doi: 10.1177/109019819802500303
20. Brown, L, LaFond, A, and Macintyre, KE. Measuring capacity building: Carolina population center. United States: University of North Carolina at Chapel Hill (2001).
21. Guad, RM, Mangantig, E, Low, WY, Taylor-Robinson, AW, Azzani, M, Sekaran, SD, et al. Development and validation of a structured survey questionnaire on knowledge, attitude, preventive practice, and treatment-seeking behaviour regarding dengue among the resident population of Sabah, Malaysia: an exploratory factor analysis. BMC Infect Dis. (2021) 21:1–11. doi: 10.1186/s12879-021-06606-6
22. Shuaib, F, Todd, D, Campbell-Stennett, D, Ehiri, J, and Jolly, PE. Knowledge, attitudes and practices regarding dengue infection in Westmoreland, Jamaica. West Indian Med J. (2010) 59:139–46.
23. Nikookar, SH, Fazeli-Dinan, M, Khazaee-Pool, M, Mosazadeh, M, Zaim, M, and Enayati, A. Designing and determining the validity and reliability of a questionnaire to assess knowledge, attitude, and practice of healthcare workers about dengue in Mazandaran Province, north of Iran. J Mazandaran Univ Med Sci. (2022) 32:127–39.
24. Gunasekara, T, Velathanthiri, V, Weerasekara, M, Fernando, S, Peelawattage, M, Guruge, D, et al. Knowledge, attitudes and practices regarding dengue fever in a suburban community in Sri Lanka. Galle Med J. (2012). 17:10–17
25. Nadeeka, P, Padhn, G, and Amarasinghe, L. Geographic, economic and socio-cultural factors which defining the risk of dengue transmission in Kelaniya, Sri Lanka. J Exp Biol Agric Sci. (2014) 2:158–64.
26. Van Benthem, B, Khantikul, N, Panart, K, Kessels, P, Somboon, P, and Oskam, L. Knowledge and use of prevention measures related to dengue in northern Thailand. Tropical Med Int Health. (2002) 7:993–1000. doi: 10.1046/j.1365-3156.2002.00950.x
27. Shirzad, R, Alesheikh, AA, Ahmadkhani, M, and Naddaf, SR. Aedes albopictus: a spatial risk mapping of the mosquito using geographic information system in Iran. Appl Geomatics. (2021) 13:691–700. doi: 10.1007/s12518-021-00375-2
28. Arunachalam, N, Tana, S, Espino, F, Kittayapong, P, Abeyewickrem, W, Wai, KT, et al. Eco-bio-social determinants of dengue vector breeding: a multicountry study in urban and periurban Asia. Bull World Health Organ. (2010) 88:173–84. doi: 10.2471/BLT.09.067892
29. Harish, S, Srinivasa, S, Shruthi, P, Devaranavadagi, RA, Bhavya, G, and Anjum, SK. Knowledge, attitude and practice regarding dengue infection among parents of children hospitalized for dengue fever. Curr Pediatr Res. (2018) 22:33–7.
30. Mohapatra, S, and Aslami, AN. Knowledge, attitude and practice regarding dengue fever among general patients of a rural tertiary-care hospital in Sasaram, Bihar. Int J Community Med Public Health. (2016) 3:586–91. doi: 10.18203/2394-6040.ijcmph20160455
31. Davis, DA, Thomson, MA, Oxman, AD, and Haynes, RB. Changing physician performance: a systematic review of the effect of continuing medical education strategies. JAMA. (1995) 274:700–5. doi: 10.1001/jama.1995.03530090032018
32. Bloom, BS. Effects of continuing medical education on improving physician clinical care and patient health: a review of systematic reviews. Int J Technol Assess Health Care. (2005) 21:380–5. doi: 10.1017/S026646230505049X
33. Koonisetty, KS, Aghamohammadi, N, Urmi, T, Yavaşoglu, Sİ, Rahman, MS, Nandy, R, et al. Assessment of knowledge, attitudes, and practices regarding dengue among physicians: a web-based cross-sectional survey. Behav Sci. (2021) 11:105. doi: 10.3390/bs11080105
34. Kumaran, E, Doum, D, Keo, V, Sokha, L, Sam, B, Chan, V, et al. Dengue knowledge, attitudes and practices and their impact on community-based vector control in rural Cambodia. PLoS Negl Trop Dis. (2018) 12:e0006268. doi: 10.1371/journal.pntd.0006268
35. Huang, HL, Chiu, TY, Huang, KC, Cheng, SY, Yao, CA, and Lee, LT. Travel-related mosquito-transmitted disease questionnaire survey among health professionals in Taiwan. J Travel Med. (2011) 18:34–8. doi: 10.1111/j.1708-8305.2010.00483.x
36. Mansour, AI, and Abu-Naser, SS. Knowledge based system for the diagnosis of dengue disease. Int JAcademic Health Med Res (IJAHMR). (2019) 3:12–19.
37. Nikookar, SH, Fazeli-Dinan, M, Enayati, A, and Zaim, M. Zika; a continuous global threat to public health. Environ Res. (2020) 188:109868. doi: 10.1016/j.envres.2020.109868
38. Arif, MM, Ali, MA, and Arif, A. Knowledge, attitude and practice (KAP) of dengue fever in adult semi-urban and rural population of Central Punjab Pakistan. Annals of Punjab Med Col. (2015) 9:129–35.
39. Itrat, A, Khan, A, Javaid, S, Kamal, M, Khan, H, Javed, S, et al. Knowledge, awareness and practices regarding dengue fever among the adult population of dengue hit cosmopolitan. PLoS One. (2008) 3:e2620. doi: 10.1371/journal.pone.0002620
40. Mayxay, M, Cui, W, Thammavong, S, Khensakhou, K, Vongxay, V, Inthasoum, L, et al. Dengue in peri-urban Pak-Ngum district, Vientiane capital of Laos: a community survey on knowledge, attitudes and practices. BMC Public Health. (2013) 13:434. doi: 10.1186/1471-2458-13-434
41. Khan, W, Rahman, A, Zaman, S, Kabir, M, Khan, R, Ali, W, et al. Knowledge, attitude and practices regarding dengue and its vector among medical practitioners in Malakand region, Pakistan. Braz J Biol. (2022) 83:83. doi: 10.1590/1519-6984.244966
42. Khalil, KR, Malik, FR, and Faisal, MS. Knowledge, attitude and practices (KAP) study on dengue among rural and urban areas of Peshawar, Pakistan. Rawal Med J. (2016) 41:153.
43. Selvarajoo, S, Liew, JWK, Tan, W, Lim, XY, Refai, WF, Zaki, RA, et al. Knowledge, attitude and practice on dengue prevention and dengue seroprevalence in a dengue hotspot in Malaysia: a cross-sectional study. Sci Rep. (2020) 10:1–13. doi: 10.1038/s41598-020-66212-5
44. Syed, M, Saleem, T, Syeda, U-R, Habib, M, Zahid, R, Bashir, A, et al. Knowledge, attitudes and practices regarding dengue fever among adults of high and low socioeconomic groups. J Pak Med Assoc. (2010) 60:243–7.
45. Ahmed, N, and Taneepanichskul, S. Knowledge, attitude and practice of dengue fever prevention among the people in male. Maldives J Health Res. (2008) 22:33–7.
46. Hairi, F, Ong, C-H, Suhaimi, A, Tsung, T-W, Bin Anis Ahmad, MA, Sundaraj, C, et al. A knowledge, attitude and practices (KAP) study on dengue among selected rural communities in the Kuala Kangsar district. Asia Pac J Public Health (2003). 15(1) 7–43. doi: 10.1177/101053950301500107
47. Harapan, H, Rajamoorthy, Y, Anwar, S, Bustamam, A, Radiansyah, A, Angraini, P, et al. Knowledge, attitude, and practice regarding dengue virus infection among inhabitants of Aceh, Indonesia: a cross-sectional study. BMC Infect Dis. (2018) 18:1–16. doi: 10.1186/s12879-018-3006-z
Keywords: knowledge, attitude, practice, dengue, Aedes, Mazandaran, northern Iran
Citation: Nikookar SH, Moosazadeh M, Fazeli-Dinan M, Zaim M, Sedaghat MM and Enayati A (2023) Knowledge, attitude, and practice of healthcare workers regarding dengue fever in Mazandaran Province, northern Iran. Front. Public Health. 11:1129056. doi: 10.3389/fpubh.2023.1129056
Edited by:
Jalil Nejati, Zahedan University of Medical Sciences, IranReviewed by:
Muruganandam Nagarajan, Regional Medical Research Centre (ICMR), IndiaCopyright © 2023 Nikookar, Moosazadeh, Fazeli-Dinan, Zaim, Sedaghat and Enayati. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ahmadali Enayati, YWVuYXlhdGkxMzcyQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.