 Xiaoning Zhang
Xiaoning Zhang Qiong Zhou4†
Qiong Zhou4†
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 11 September 2023
Sec. Children and Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1122645
This article is part of the Research TopicThe Developmental Origin of Childhood ObesityView all 4 articles
Introduction: Childhood eating behaviors and temperament may have important implication for constructing the pathways from maternal feeding practices to childhood overweight and obesity (OW/OB). Examining multiple feeding styles simultaneously to childhood OW/OB is critical through the mediators of early childhood temperament and eating behaviors.
Methods: This cross-sectional study recruited mothers mainly responsible for child care from two hospitals and two healthcare centers in eastern China. Sociodemographic characteristics, and data from the Infant Feeding Style Questionnaire (IFSQ), the short form of Children Behavior Questionnaire [Revised (IBQ-RSF)], and the Child Eating Behavior Questionnaire for toddler (CEBQ-T) were collected. Weight and recumbent length were measured to calculate the age- and sex-specific body mass index (BMI) z-scores (BMIz). The structural equation modeling (SEM) approach was used to examine direct and indirect pathways from five maternal feeding styles to childhood OW/OB through temperament and eating behaviors.
Results: A total of 486 children were recruited, 73 (15.02%) children were OW/OB; the age of the children was 14.55 (SD = 5.14) months, and the age of the mothers was 29.90 (SD = 3.63) years. The responsive feeding exerted significant direct (β = −0.098), indirect (β = −0.136) and total (β = −0.234) effects on childhood OW/OB. Restrictive feeding had significant direct (β = 0.222), indirect (β = 0.102) and total (β = 0.324) effects on childhood OW/OB. Indulgent feeding had significant direct (β = 0.220), indirect (β = 0.063), and total (β = 0.283) effects on childhood OW/OB. Pressuring feeding had significant direct (β = −0.116), indirect (β = −0.096) and total (β = −0.212) effects on childhood OW/OB.
Discussion: There was a direct effect of feeding practices on childhood OW/OB; feeding practices indirectly predicted childhood OW/OB through temperament and eating behaviors in children aged 6–23 months. This study could help governments agencies, policymakers, and healthcare workers to establish optimal intervention programs targeting feeding practices through childhood eating behaviors and temperament to prevent childhood OW/OB.
Infancy and young childhood (0–24 months) are critical periods for developmental plasticity, with long-lasting behavioral consequences and may potential influence long-term risk of obesity (1). During this time, eating behaviors develop as children transition from exclusive milk to a modified adult diet, including main meals and snacks, to achieve stability over time (2). Complementary feeding (CF) introduces solid and semi-solid foods to satisfy nutritional requirements of children aged 6–23 months (3). Developmental theories suggest that parent–child interaction through feeding practices may influence child health outcomes (4). Recently, global approaches to feeding practices have emerged to address childhood overweight and obesity (OW/OB) (5). Feeding practice include parental beliefs and behaviors concerning feeding, as well as interactions with children in relation to food and food-related parenting (6). Feeding practices are key factors influencing eating behaviors through the quantity and quality of food provisions and the interactions around feeding, as infants learn to eat and parents shape the physical and social environment of eating (2). Infant and young child feeding practices (IYCF) (6–23 months) have been identified as an under-prioritized strategy to prevent childhood OW/OB (3), which include the following: (1) responsive parents are attentive to the satiety and hunger cues of their children and monitor the dietary quality; (2) restrictive parents limit the quantity and quality of unhealthy foods; (3) pressuring parents are concerned about the increasing amount of food, pressuring children to finish bottle or plate, or soothing children with food instrumentally; (4) indulgent parents do not limit the quantity or quality of food; and (5) laissez-faire parents do not limit dietary quality or quantity, with little interaction (7).
Study on feeding practices indicate that parents socialize with children to create an emotional climate around eating, and individual differences should be considered in the parent–child feeding process (8). Temperament refers to constitutionally based individual differences in the reactivity and self-regulation aspects of behavior (4), which is a long-standing research area in emotional development and well-being (9). Childhood characteristics can be approached from a broader perspective through temperament, a range of direct relationships between temperament and weight status in predicting childhood OW/OB has been reported (10). Current conceptualizations of childhood temperament have gained research attention, and the early emerging basic dispositions in three domains (11): (1) Surgency/Extraversion refers to the level of impulsivity, activity, sensation seeking, and positive anticipation; (2) Negative affectivity encompasses the propensity to experience emotions, e.g., frustration, fear, sadness, and anger; (3) Effortful control refers to the infant’s ability to inhibit behavioral responses to stimuli, concentrate and shift attention, exhibit perceptual sensitivity, have a lower threshold for experiencing pleasure, and demonstrate soothability, including the capacity for orientation and regulation in various aspects of the infant’s behavior and responses (12). There is evidence of moderate temperament stability from infancy to young childhood, and the assumption linking temperament in early childhood to later behavioral problems has been extensively documented (13). In response to childhood temperament, feeding practices have the potential to change (14), temperament may indirectly affect weight by prompting specific responses from maternal feeding practices; higher negative levels of temperament are associated with weight gain (15).
With the growth of the Chinese economy, there has been a significant increase in people migrating away from their hometowns. A commonly heard saying, “happiness is the taste of mom (in childhood),” implies that maternal feeding practices may serve as an additional predictor of eating behaviors. Feeding and eating in East Asian cultures has unique significance, previous studies showed that Chinese mothers reported higher responsive feeding and lower indulgent feeding (3, 7). Eating behaviors among young children include two traits: food approach and food avoidance. Food approach is characterized by a higher avid appetite and interest in food, and it has been associated with higher childhood weight, including the following: (1) food responsiveness (FR) involves assessing the extent to which children are demanding when being fed and how responsive they are to external food cues, e.g., children would be fed when they see or smell food; (2) enjoyment of food (EF) captures the perceived pleasure childhood experience from food and the general feeding process, e.g., the extent to which children favor and derive satisfaction from eating; and (3) emotional overeating (EOE) captures the tendency of children to eat more in response to stress and negative emotions. Food avoidance is characterized by lower appetite and interest in food and has been associated with lower weight, including the following: (1) food fussiness (FF) measures the tendency of children to be highly selective in accepting the texture and flavor of foods, including a reluctance to try new food; (2) satiety responsiveness (SR) measures the satiety sensitivity to internal cues of children, e.g., how easily children become full around mealtime; and (3) slowness in eating refers to the measurement of the speed at which children consume typical food, e.g., the overall feeding pace during childhood (16).
Feeding practices influence childhood eating behaviors during processes by communicating of behaviors and beliefs about food and eating (17). Eating behaviors can contribute to poor nutritional status among children (18), and are associated with childhood OW/OB (19). Parents directly control childhood food intake as they may pressure children to eat more or restrict children their consumption of unhealthy foods, controlling feeding may be exerted indirectly by monitoring the intake of unhealthy foods in children (17). Study has found associations between parental food restriction and childhood food approach behaviors and OW/OB, e.g., enjoyment of food and food responsiveness (20). Childhood food-avoidant behaviors, e.g., food fussiness and satiety responsiveness, are also associated with pressure feeding and lower childhood weight status (21). While higher parental food restriction is associated with a higher childhood OW/OB, higher pressuring feeding is associated with higher childhood underweight (22), which in turn may influence childhood lower interest in food (23) or the development of obesogenic eating behaviors (24).
External feeding practices have been found to be associated with the development of childhood eating behaviors (25), and genetic and antenatal factors are important contributors to childhood eating behaviors (2). Feeding practices influence the eating environment through food provisions and parent–child interactions around feeding (4). Considering the impact of eating behaviors on the development of childhood OW/OB, research endeavors to identify adaptable feeding practices that encourage the formation of healthy eating behaviors during childhood (2). Evidence shows that maternal feeding practices may influence the development of childhood eating behaviors, which is associated with the risk of childhood OW/OB (26). Eating behaviors in infancy and young childhood are heritable traits; healthy eating behaviors is an important feeding strategy to combat childhood OW/OB (7). Eating behaviors influence OW/OB and disordered eating patterns, hence, it is imperative to identify modifiable feeding practices during infancy and young childhood that may promote the development of a healthy appetite and regulation of energy intake later in childhood and adulthood (2). Mothers often perceive their children as being attracted to food, e.g., higher score for the “enjoyment of food,” lower scores for the “satiety responsiveness,” “slowness in eating” and “food fussiness,” show that higher eating rates in children contribute to increase energy intake and are associated with higher BMI (27).
In contemporary temperament models, childhood temperament interacts with the parenting environment and contributes to early childhood development (4). Childhood temperament may have positive or negative health consequences depending on feeding practices (4). Temperamental avoidance of novelty appears to be strongly associated with negative responses to new foods after the emergence of wariness and self-locomotion (28). The relationship between negative childhood temperament and OW/OB has produced mixed results, as negative emotionality is related to both emotional overeating and undereating (29). Eating behaviors have been found to be related to temperament, which is distinct from individual differences referred to as “appetitive traits” (30). Higher negative levels of temperament are associated with increased food approach and higher food intake (15). Temperament interacts with the parenting environment, influencing childhood eating behaviors and OW/OB; and may evoke parental feeding decisions, influence childhood dysregulated eating and OW/OB (4). Therefore, when examining the predictors of childhood eating behaviors and OW/OB, it is important to consider the impact of temperament (4).
Pathways to childhood OW/OB include the environmental models, in which feeding practices are daily interactional activities dependent on the parenting environment (4). The existing body of research on the relationship between feeding practices and childhood eating behaviors primarily originates from studies conducted in developed western countries, with a specific emphasis on childhood OW/OB (17). Whereas an association between childhood temperament, feeding practices, childhood eating behaviors, and OW/OB may exist (4), with a significant implication in constructing the pathways from feeding practices to childhood OW/OB. Efforts to prevent childhood OW/OB have limited the consideration of maternal feeding practices through childhood eating behaviors and temperament. Sociocultural circumstances are critical in shaping maternal feeding practices, childhood eating behaviors, and OW/OB (31). Hence, understanding the local feeding context is imperative, considering the impact of ethnicity on childhood eating behaviors and preferences (31). The fast-tracked urbanization and lifestyle changes in China may disrupt for childhood access to food and feeding practices.
To the best of our knowledge, to date, no study has explored the effect of feeding practices on childhood OW/OB to examine the mediators of temperament and eating behaviors in children aged 6–23 months (32). Developmental reactivity and regulation contribute to refining the conceptual framework of the associations between feeding practices, childhood temperament, eating behaviors, and OW/OB (33). Examining the impact of multiple feeding styles simultaneously on childhood OW/OB may be critical for exploring the mediators of childhood temperament and eating behaviors (34). Socioeconomic status has been found to predict an increase in emotional overeating and food responsiveness during childhood (35). Therefore, it is crucial to appropriately control for the impact of the differences in sociodemographic characteristics, which allows for a more accurate understanding of independent effects of feeding practices on childhood eating behaviors (2). This study provided a conceptual framework that aimed to explain the pathways from feeding practices to childhood OW/OB (33) with regard to childhood temperament and eating behaviors (Figure 1) as follows: (1) there may exist a direct effect from feeding practices to childhood OW/OB; (2) five styles of feeding practices may indirectly predict childhood OW/OB through the sequential mediation of three domains of temperament and five traits of eating behaviors.
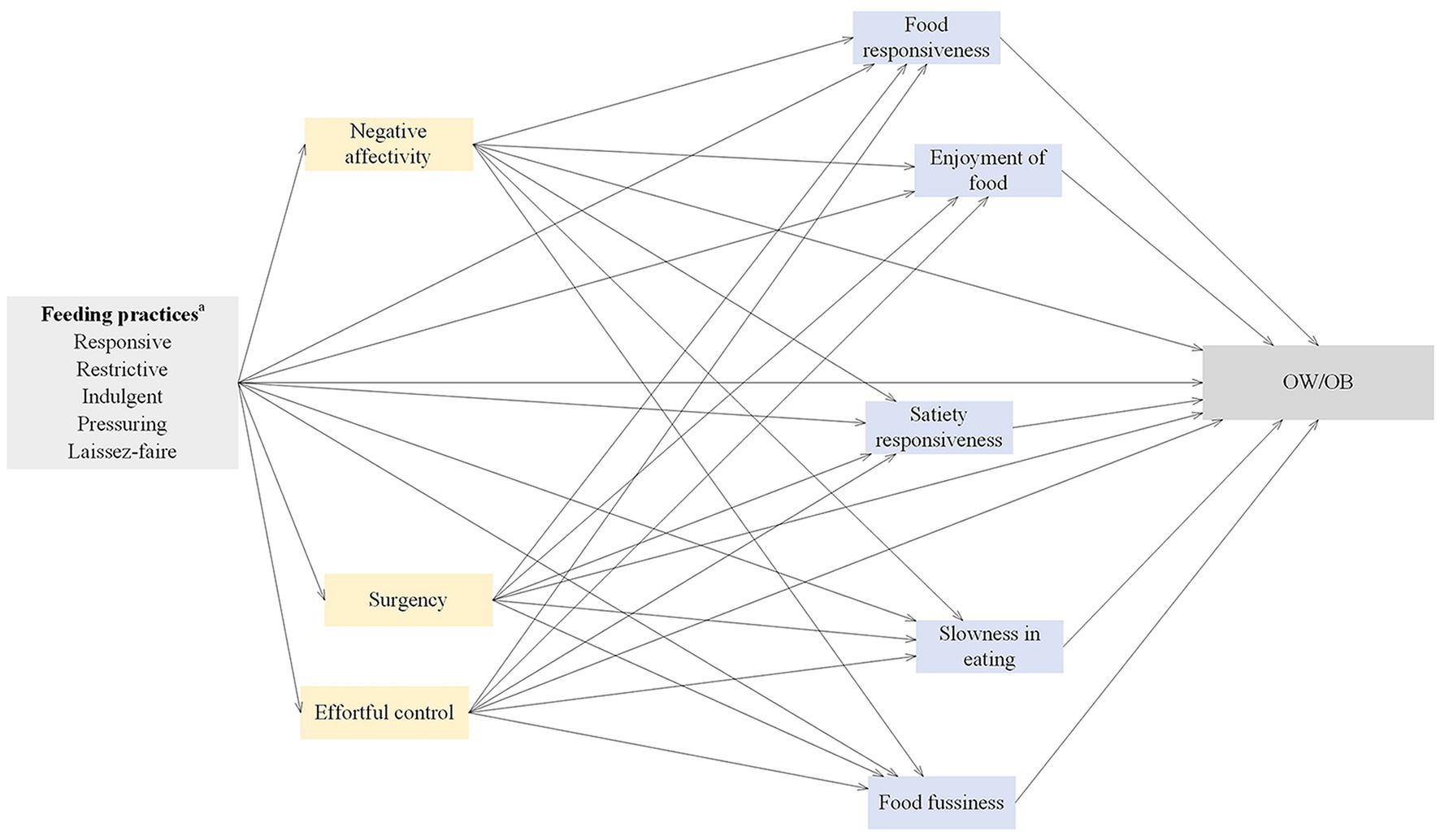
Figure 1. Conceptual framework and hypotheses. aAll feeding practices were examined in separate structural equation models. OW/OB, overweight and obesity.
This cross-sectional study was a snapshot taken at a point when vaccination was necessary for children, recruited mothers who were mainly responsible for child care (n = 486) from two hospitals (n = 234) and two healthcare centers (n = 252) in Xuzhou and Suqian, Jiangsu, China between April 5, 2020, and May 31, 2021. A purposive sampling method was used to recruit participants during vaccination. Inclusion criteria were as follows: mothers older than 18 years, with at least one child aged 6–23 months, born full-term with a birth weight of 2,500–4,000 g. Exclusion criteria were mothers with mental illness or children with health issues.
The sample size was calculated based on the prevalence of childhood OW and OB (15%), according to the calculation formula (36). The marginal error was within 3.2% with a 95% confidence level, p = 0.5; thus, the estimated maximum sample size was 479.
The sociodemographic characteristics collected included: child age, sex (female, male), maternal age, education level (middle school or below, high school, college/university or above), employment status (unemployed, employed), area of residence (urban, rural) and annual household income (<100,000, 100,000–150,000, >150,000 RMB).
The Infant Feeding Style Questionnaire (IFSQ) is an 83-item measure, including 5 maternal feeding styles (37): responsive (12 items), restrictive (11 items), indulgent (32 items), pressuring (17 items), and laissez-faire (11 items). Each item was coded on a 5-point Likert scale ranging from 1 (strongly disagree/never) to 5 (strongly agree/always), each subscale was scored as the mean of responses, and higher scores indicated higher level of each feeding style. The IFSQ has been validated in Chinese mothers and the Cronbach’s alpha value was higher than 0.898 for each subscale (7).
The short form of Infant Behavior Questionnaire-Revised – (Revised IBQ-RSF) (11) with 91 items, and the Early Child Behavior Questionnaire (ECBQ-SF) (38) with 107 items were used to assess the childhood temperament of children aged between 6–15, and 16–24 months, respectively. The IBQ-RSF and ECBQ-SF included three dimensions: negative affectivity, surgency and effortful control, rated on a 7-point Likert scale ranging from 1 (never) to 7 (always). The negative affectivity consisted of four subscales assessing infant sadness, falling reactivity, fear, and distress to limitations (39). Surgency/Extraversion consisted of six subscales, assessing infant approach, high-intensity pleasure, vocal reactivity, smiling and laughter, activity level, and perceptual sensitivity (39). Orienting/Regulation consisted of four subscales of infants’ cuddliness/affiliation, duration of orientation, low-intensity pleasure, and soothability (39). Higher mean scores indicated a higher presence of temperamental traits. In this study, the Cronbach’s alpha values for negative affectivity, surgency, and effortful control in the IBQ-RSF were 0.94, 0.73 and 0.85 respectively; in the ECBQ-SF were 0.91, 0.82, and 0.87, respectively, which showed that IBQ-RSF was validated in Chinese children.
The Child Eating Behavior Questionnaire for toddler (CEBQ-T) is a 26-item measure, including six subscales (16): food responsiveness (4 items), enjoyment of food (4 items), emotional overeating (3 items), satiety responsiveness (5 items), slowness in eating (4 items), and food fussiness (6 items). As mothers reported that their children did not engage in emotional overeating, this subscale was removed. Items were scored on a 5-point Likert scale ranging from 1 (never) to 5 (always), and higher mean scores indicated higher expression of eating behaviors. In this study, Cronbach’s alpha values for food responsiveness, enjoyment of food, satiety responsiveness, slowness in eating, and food fussiness were 0.76, 0.78, 0.86 0.88 and 0.90, respectively. A five-factor model’s confirmatory factor analysis (CFA) of indicated an acceptable model fit (Tables 1, 2).
The weight and recumbent length of children were measured following standard procedures, weight was measured while the children were wearing light clothes without shoes to the nearest 0.1 kg using a calibrated digital scale (Seca 354, China), and length was measured to the nearest 0.1 cm using a stadiometer (Seca 416, China) (40). The weight and recumbent length were measured in duplicate and recorded as the average values, and a third measurement was undertaken in case of a difference higher than 0.05 kg for weight or 1 cm for length. The average of the two closest values was used when three measurements were made. The age- and sex-specific BMI z-scores (BMIz) were calculated based on the World Health Organization (WHO) Child Growth Standards, and children were classified into overweight and obese (OW/OB; BMIz > +2) and non-OW/OB (BMIz ≤ +2) (41).
Statistical analyses were performed using the STATA 15.0 software (Stata Corporation, College Station, TX, USA) and AMOS 23.0 software (IBM Corporation, Armonk, NY, USA). Data were double-checked for any errors, no missing values were reported in this study. Sociodemographic differences between hospitals and healthcare centers were examined using ANOVA and chi-square test. Pearson’s correlation analysis was conducted to evaluate the relationships among sociodemographic characteristics, feeding practices, temperament, eating behaviors, and OW/OB in childhood.
The structural equation modeling (SEM) was used with the maximum likelihood estimation to examine the direct and indirect pathways from five maternal feeding styles to childhood OW/OB through temperament and eating behaviors. Sociodemographic variables were included in the SEM as covariates if they were significantly associated with mediators (temperament and eating behaviors) or outcome variable (childhood OW/OB). Multiple goodness-of-fit indices were used to achieve the acceptable model fit, including the Comparative Fit Index (CFI) > 0.90, Adjusted Goodness-of-fit Index (AGFI) > 0.90, Goodness-of-fit Index (GFI) > 0.90, Root Mean Square Error of Approximation (RMSEA) < 0.08 and Standardized Root Mean Square Residual (SRMR) < 0.08 (42, 43). The bootstrap resampling procedures (n = 2000 samples) and a bias-corrected 95% confidence interval (BC 95% CI) were used to estimate the significant effects (44, 45). The total effects were calculated as the sum of the direct and indirect effects, mathematically expressed as follows: c = c′ + ab, where c = total effect, c′ = direct effect, and ab = indirect effect (46). The ratio was calculated as 100 × (indirect effect/total effect). A value of p < 0.05 indicated a statistically significant difference. According to the empirical estimates of the sample size for mediation models, the sample size of this study was 486 exceeding the required size for small-to-medium a and b paths with power = 0.80 (47).
A pilot study was conducted with a sample of 10 mothers to enhance the clarity and consistency of the questionnaires. The aim of the pilot study was to ensure a comprehensive understanding of the CEBQ-T. No amendments were necessary for the questionnaires and the data collected from the pilot study were integrated into the final sample for subsequent analysis.
Potential mothers were approached through word of mouth and flyers distributed during child vaccination visits. All mothers were asked to participate; if they agreed, they were provided with an information sheet detailing the study’s objectives, procedures, expected outcomes, benefits and risks. All mothers provided written informed consent, and were informed of the right to withdraw at any given time. All data were anonymized concerning data protection. Researchers were available to assist if necessary, e.g., by answering questions about this study, and assessing the completeness of the questionnaires. Mothers who completed the questionnaires received 30 RMB as compensation for their participation in the study. This study was conducted in accordance with the Declaration of Helsinki and approved by the Xuzhou Medical University Ethics Committee (ID number: XZ2018728).
Sociodemographic differences between hospitals and healthcare centers are presented in Table 3. A total of 73 (15.02%) children were OW/OB; the age of children was 14.55 (SD = 5.14) months and 260 (53.50%) were males. The age of the mothers was 29.90 (SD = 3.63) years, 168 (34.57%) attended a high school, 264 (54.32%) were unemployed, 288 (59.26%) resided in urban areas, and 201 (41.36%) reported household income of less than 100,000 RMB per year. There was no statistically significant difference in sociodemographic comparison between hospitals and healthcare centers (Table 3).
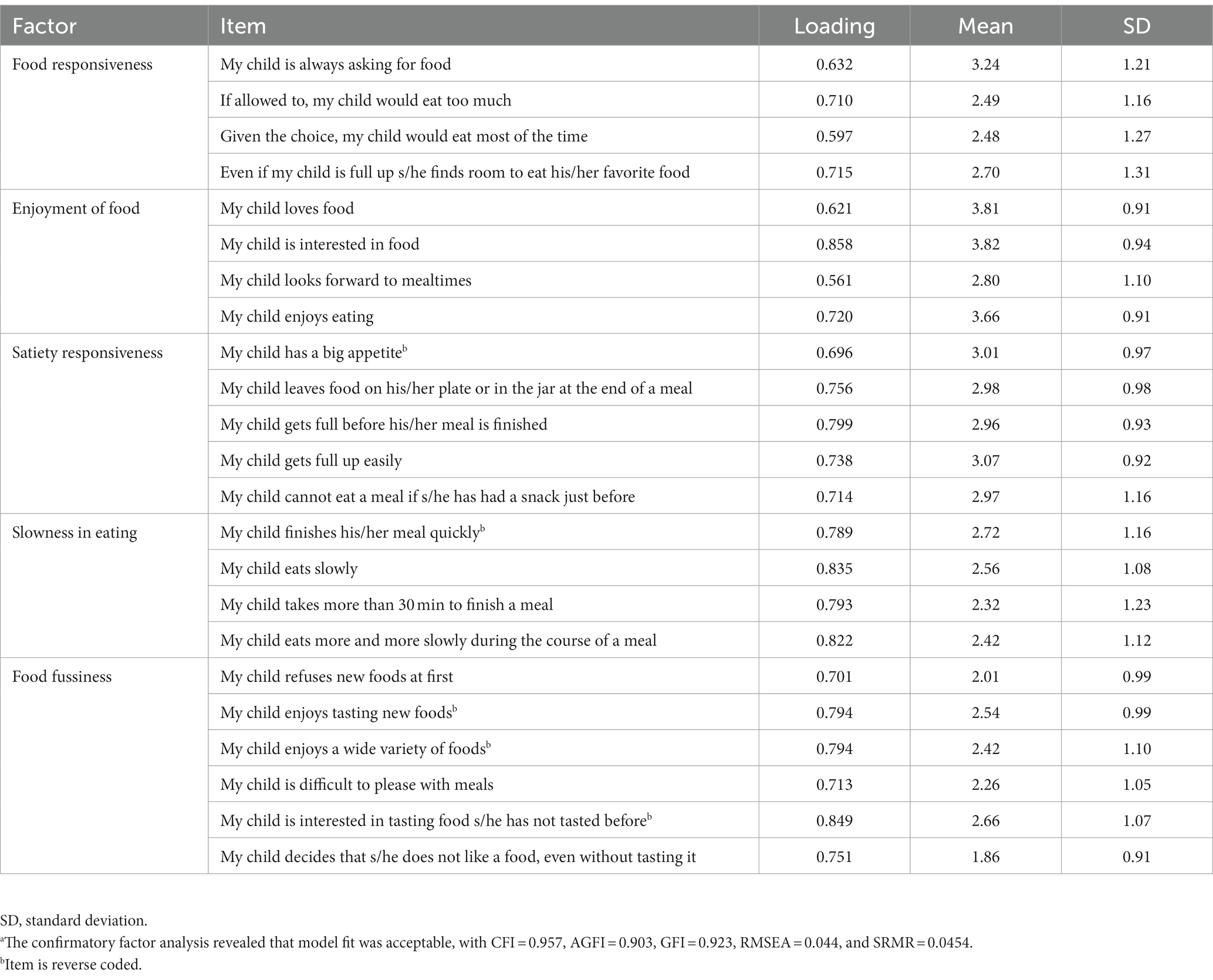
Table 1. Standardized factor loadings for items of the CEBQ-T according to confirmatory factor analysis – 5 factors, 23 itemsa.
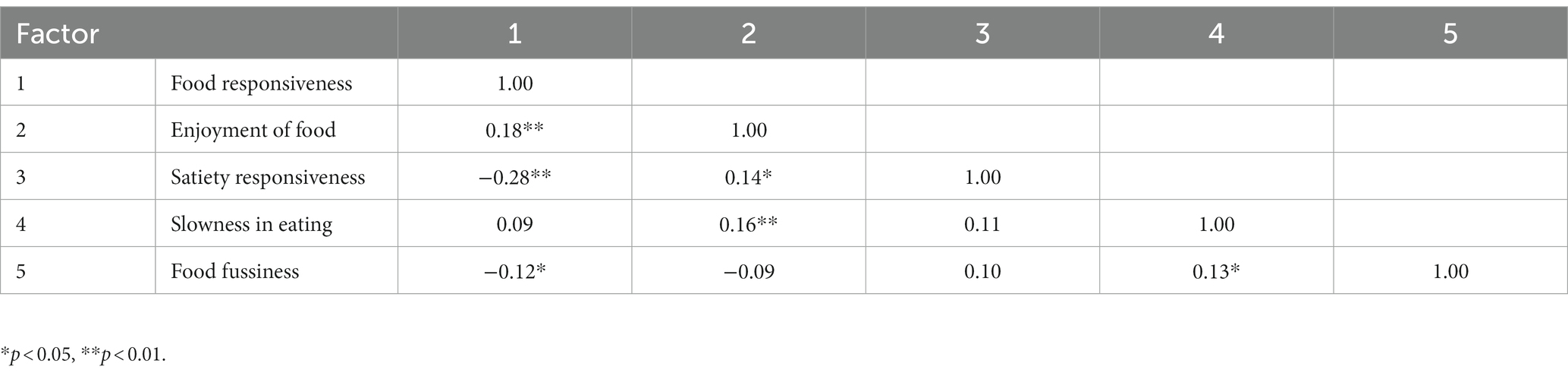
Table 2. Factor-factor correlations of 5 eating behaviors (based on 23 items, CEBQ-T).
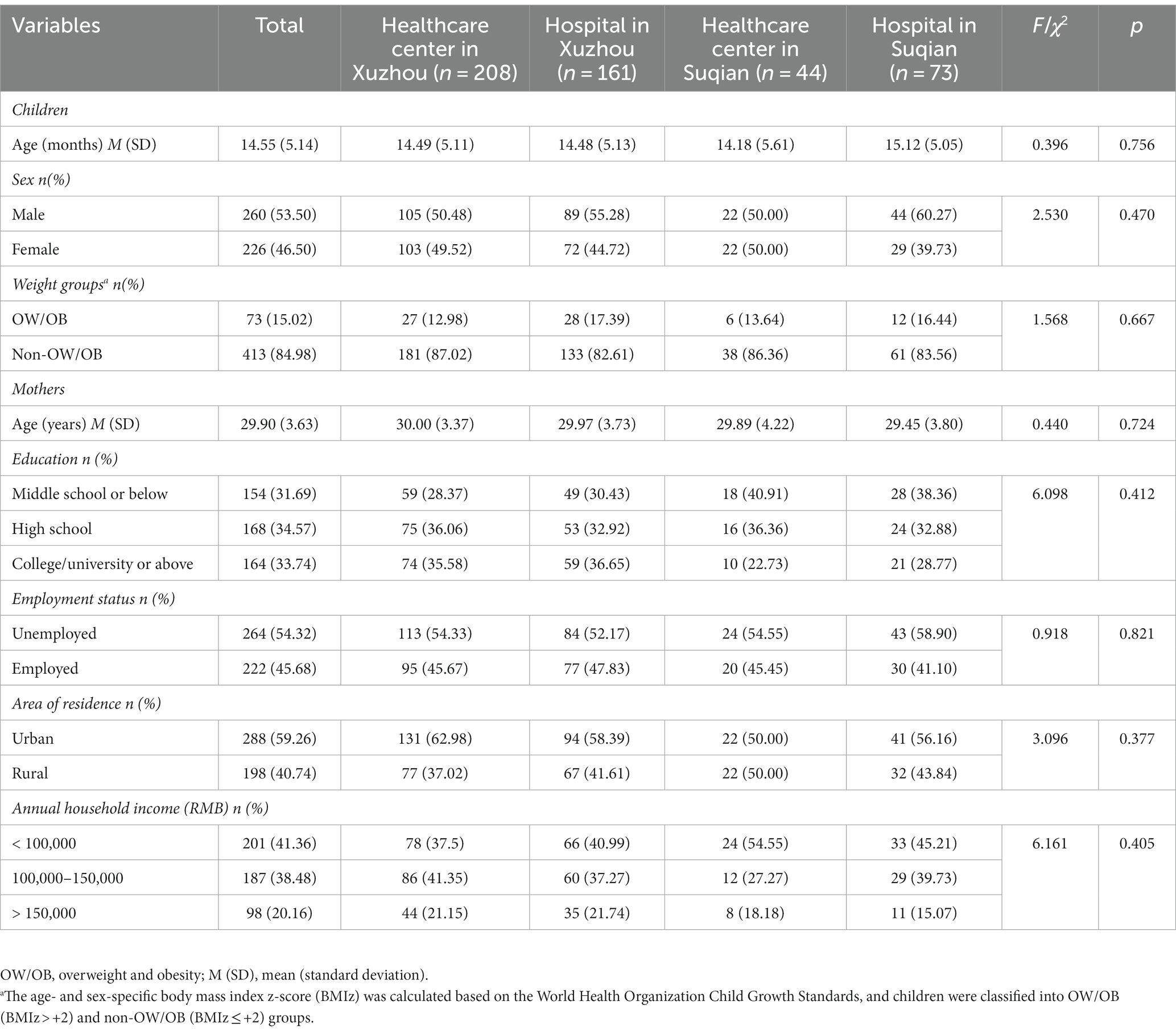
Table 3. Sociodemographic characteristics by hospitals and healthcare centers (N = 486).
The results of the correlation analysis between sociodemographic characteristics, feeding practices, temperament, eating behaviors, and childhood OW/OB are listed in Table 4. Childhood OW/OB was positively correlated with restrictive feeding (r = 0.33, p < 0.05), indulgent feeding (r = 0.30, p < 0.05), food responsiveness (r = 0.27, p < 0.05), negative affectivity (r = 0.25, p < 0.05), and surgency (r = 0.13, p < 0.05); and negatively correlated with children sex (r = − 0.28, p < 0.05), maternal education (r = −0.14, p < 0.05), responsive feeding (r = −0.23, p < 0.05), pressuring feeding (r = −0.23, p < 0.05), effortful control (r = −0.34, p < 0.05), satiety responsiveness (r = −0.35, p < 0.05), slowness in eating (r = −0.17, p < 0.05), and food fussiness (r = −0.24, p < 0.05). Maternal education was positively correlated with effortful control (r = −0.14, p < 0.05). Children sex and maternal education were included as covariates in the SEM approach.
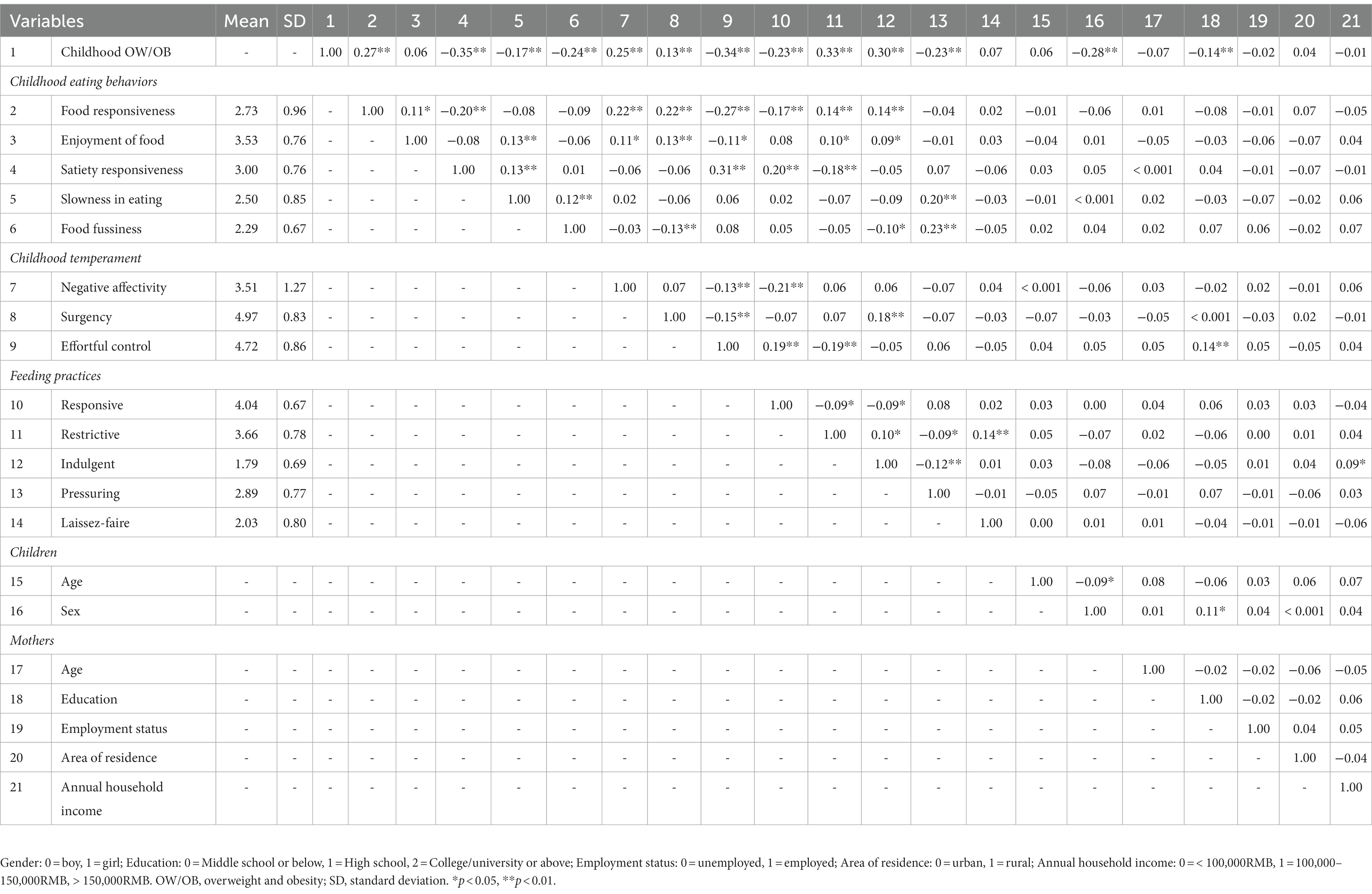
Table 4. Descriptive statistics and correlations of sociodemographic characteristics, feeding practices, temperament, eating behaviors, and OW/OB in childhood.
The standardized path estimates of the pathways from responsive feeding to childhood OW/OB are shown in Figure 2 and Table 5. Responsive feeding exerted significant direct (β = −0.098), indirect (β = −0.136), and total (β = −0.234) effects on childhood OW/OB. 41.88% of the total effect was direct, and 58.12% was indirect. Responsive feeding negatively predicted childhood OW/OB through lower negative affectivity (β = −0.034), higher satiety responsiveness (β = −0.032), and higher effortful control (β = −0.031), explaining 14.53, 13.68, and 13.25% of the total effect, respectively. Responsive feeding negatively predicted childhood OW/OB through the sequential mediation of higher effortful control and higher satiety responsiveness (β = −0.012), accounting for 5.13% of the total effect; the sequential mediation of higher effortful control and lower food responsiveness (β = −0.003), explaining 1.28% of the total effect; the sequential mediation of lower negative affectivity and lower food responsiveness (β = −0.003), accounting for 1.28% of the total effect. The SEM approach indicated an acceptable model fit, with CFI = 0.914, AGFI = 0.943, GFI = 0.977, RMSEA = 0.050 and SRMR = 0.046.
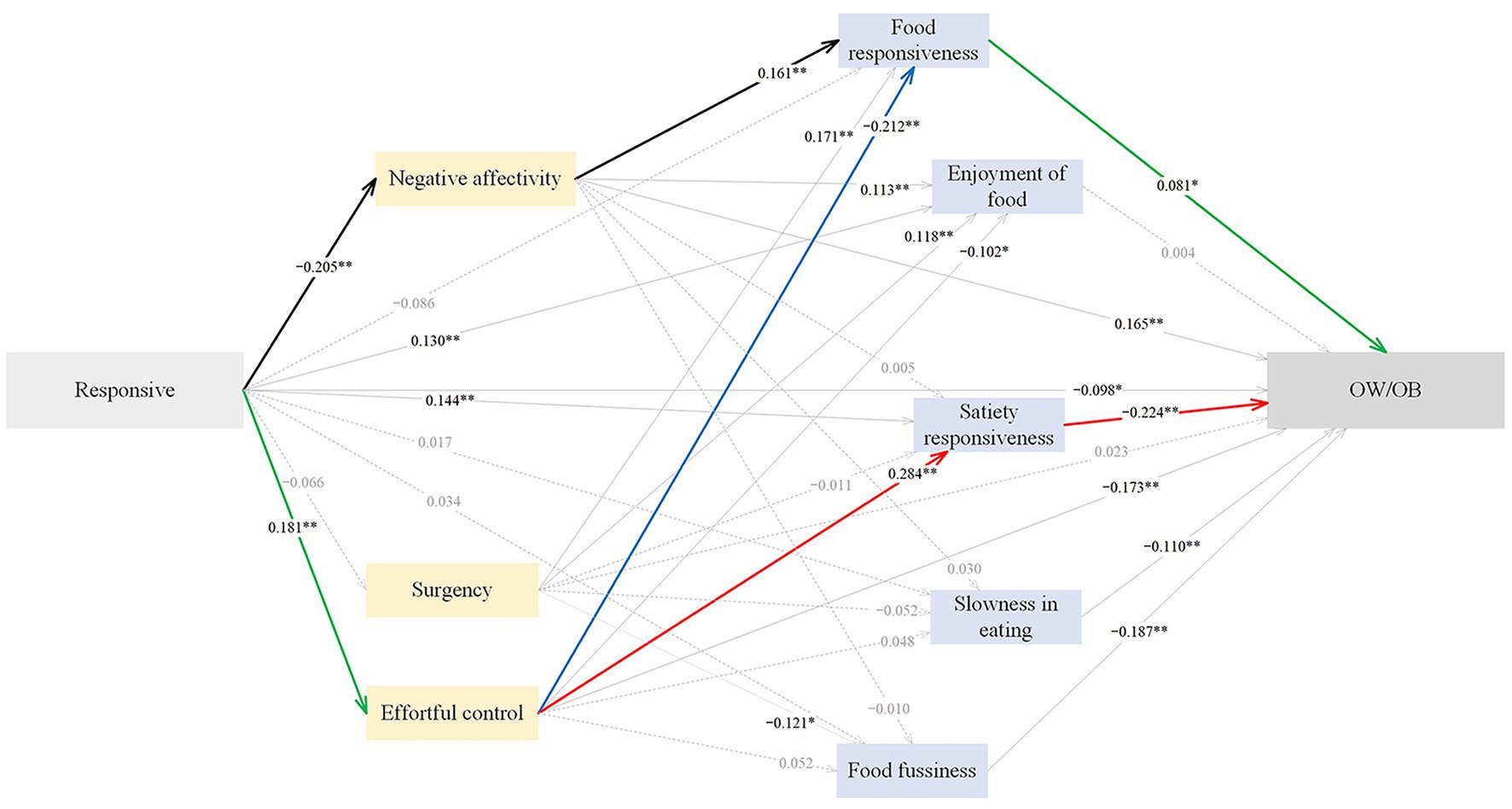
Figure 2. The standardized direct effects of responsive feeding on OW/OB via temperament and eating behaviors in childhood. For simplicity the covariates (children sex and maternal education) and measurement error terms are not shown. Dotted lines depict non-significant direct effect. Solid lines denote significant direct effect, and the bold black, green, blue and red solid lines represent sequential mediation effects. Model fit: CFI = 0.914, AGFI = 0.943, GFI = 0.977, RMSEA = 0.050, SRMR = 0.0455. OW/OB, overweight and obesity. *p < 0.05, **p < 0.01.
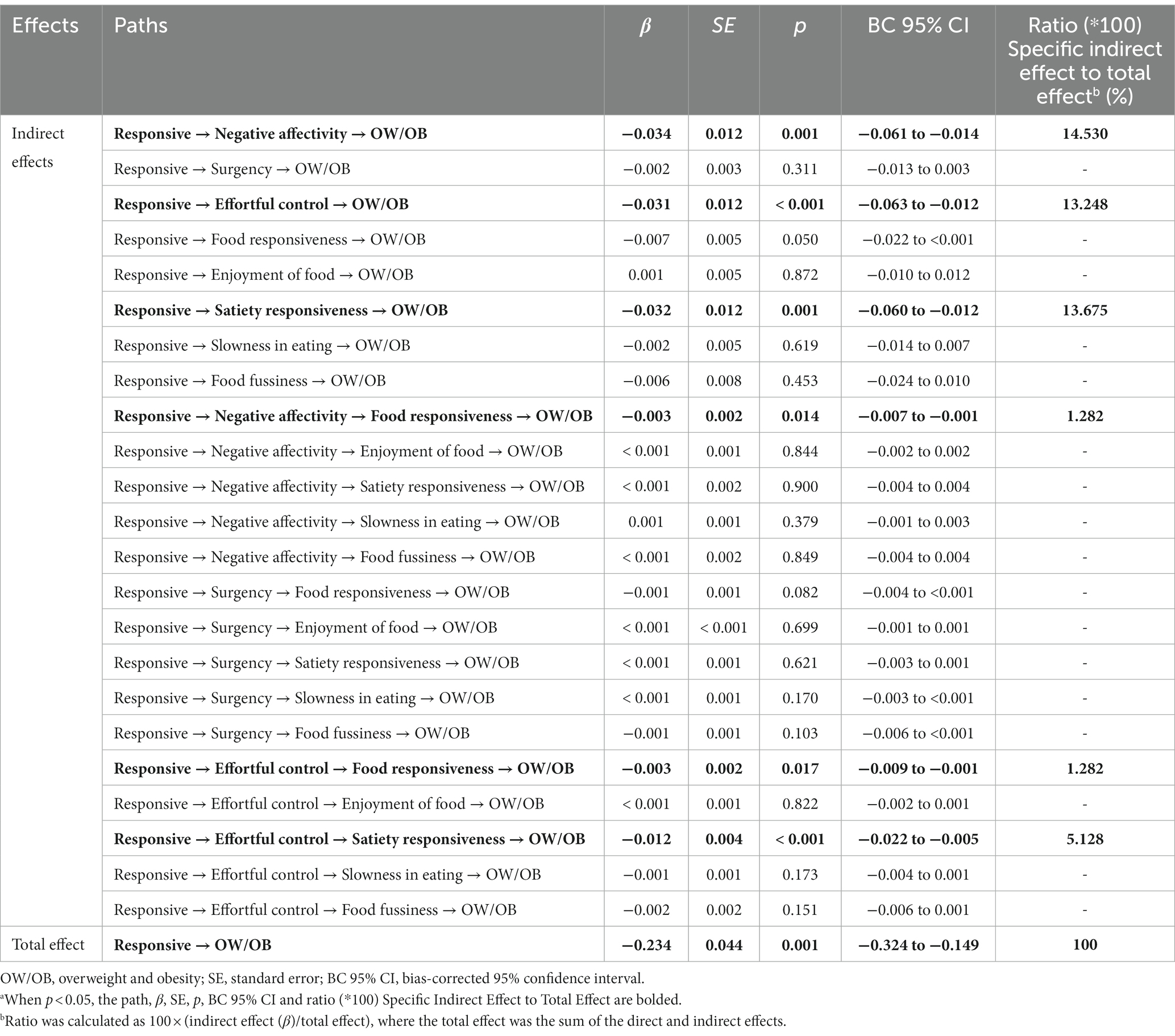
Table 5. Standardized indirect and total effects of responsive feeding on OW/OB via temperament and eating behaviors in childhooda.
The standardized path estimates of the pathways from restrictive feeding to childhood OW/OB are shown in Figure 3 and Table 6. Restrictive feeding had significant direct (β = 0.222), indirect (β = 0.102) and total (β = 0.324) effects on childhood OW/OB; 68.52% of the total effect was direct, and 31.48% was indirect. Restrictive feeding positively predicted childhood OW/OB through lower effortful control (β = 0.029), lower satiety responsiveness (β = 0.026), and higher food responsiveness (β = 0.006), accounting for 8.95, 8.03 and 1.85% of the total effect; the sequential mediation of lower effortful control and lower satiety responsiveness (β = 0.011), accounting for 3.40% of the total effect; the sequential mediation of lower effortful control and higher food responsiveness (β = 0.003), explaining 0.93% of the total effect. The SEM approach indicated an acceptable model fit, with CFI = 0.913, AGFI = 0.942, GFI = 0.977, RMSEA = 0.050, and SRMR = 0.047.
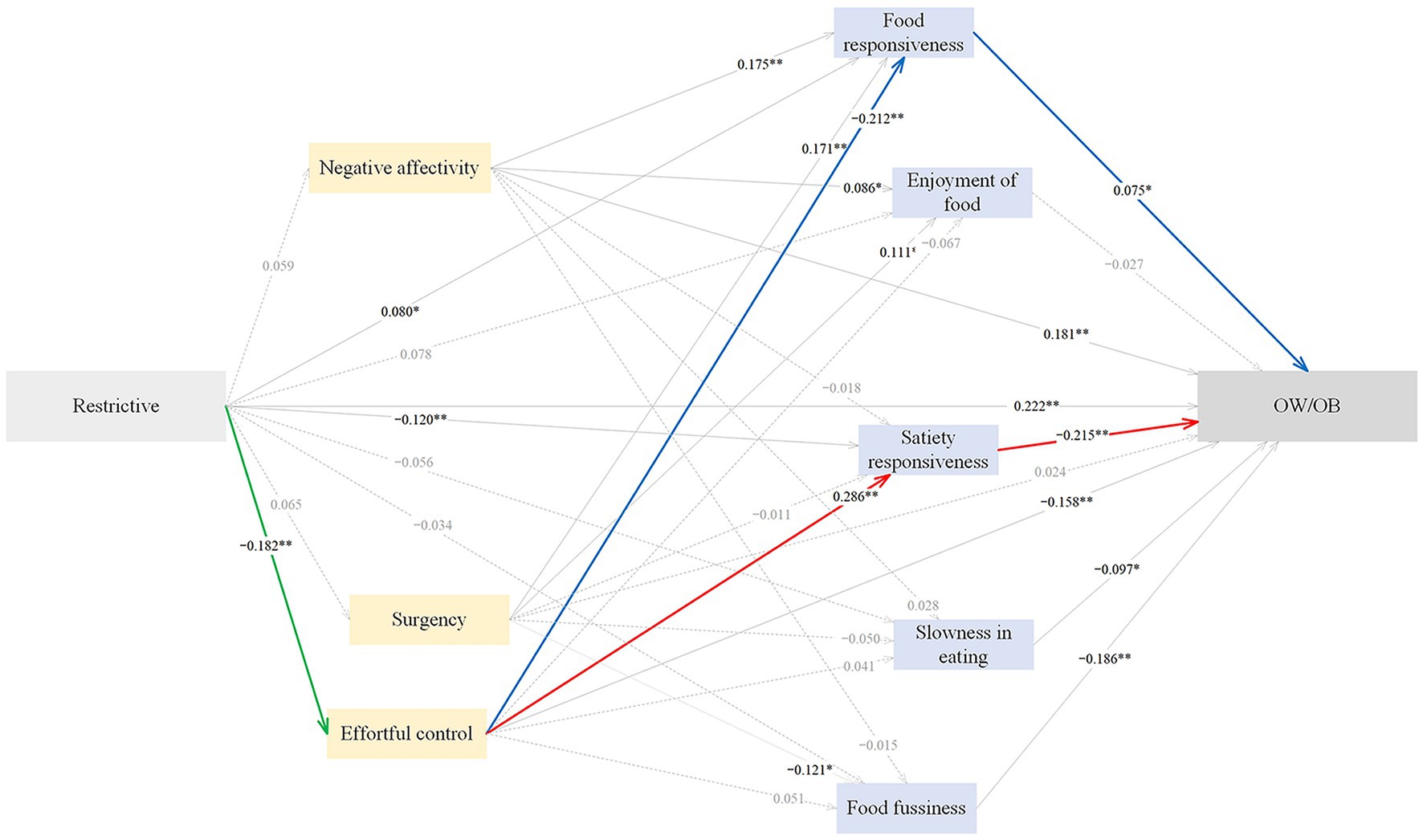
Figure 3. The standardized direct effects of restrictive feeding on OW/OB via temperament and eating behaviors in childhood. For simplicity the covariates (children sex and maternal education) and measurement error terms are not shown. Dotted lines depict non-significant direct effect. Solid lines denote significant direct effect, and the bold green, blue and red solid lines represent sequential mediation effects. Model fit: CFI = 0.913, AGFI = 0.942, GFI = 0.977, RMSEA = 0.050, SRMR = 0.0470. OW/OB, overweight and obesity. *p < 0.05, **p < 0.01.
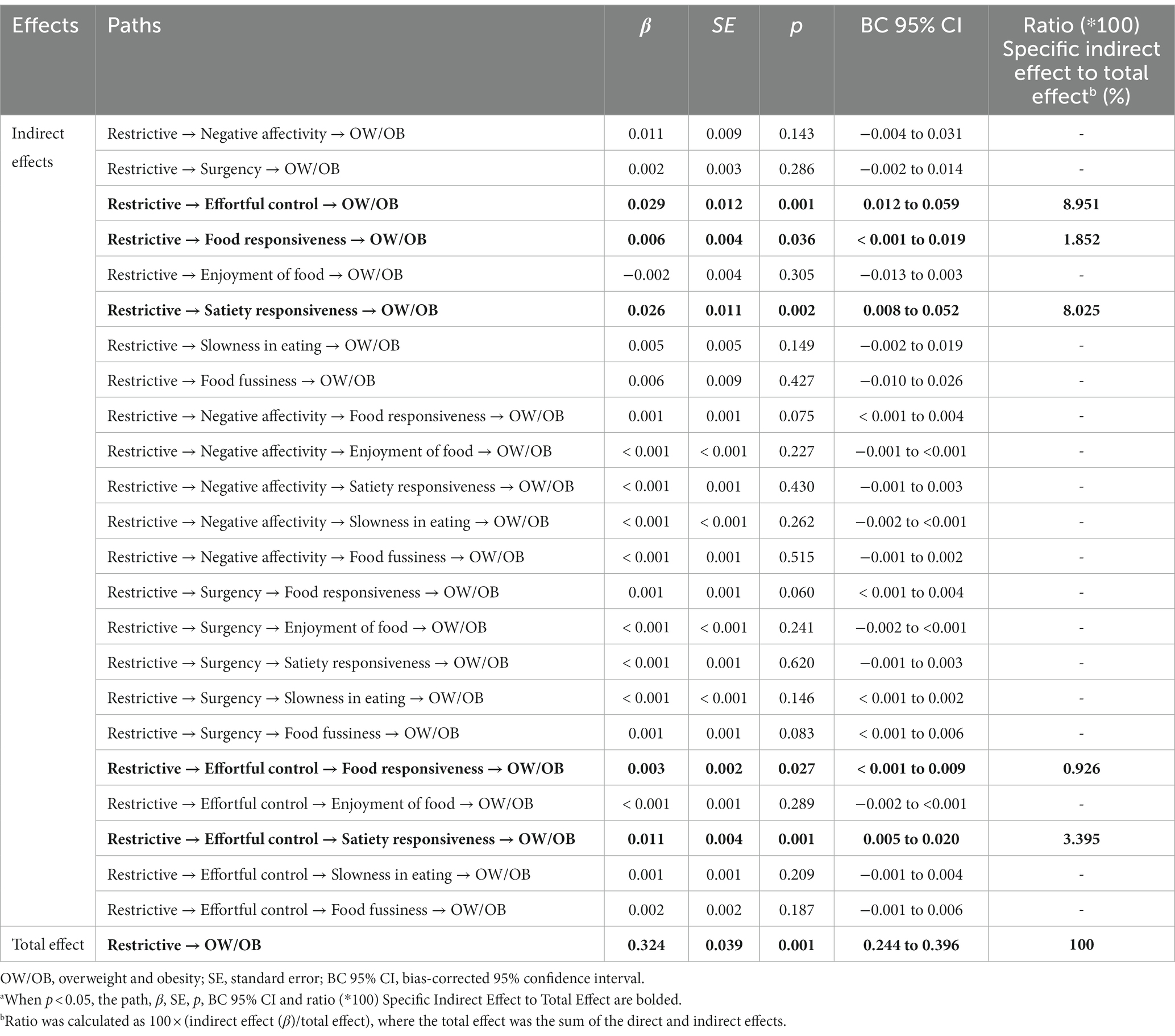
Table 6. Standardized indirect and total effects of restrictive feeding on OW/OB via temperament and eating behaviors in childhooda.
The standardized path estimates of the pathways from pressuring feeding to childhood OW/OB are shown in Figure 4 and Table 7. Indulgent feeding had significant direct (β = 0.220), indirect (β = 0.063) and total (β = 0.283) effects on childhood OW/OB. 54.72% of the total effect was direct, and 22.26% was indirect. Indulgent feeding positively predicted childhood OW/OB through higher food fussiness (β = 0.007), accounting for 2.47% of the total effect; the sequential mediation of higher surgency and lower food fussiness (β = 0.003), explaining 1.06% of the total effect; the sequential mediation of higher surgency and higher food responsiveness (β = 0.002), accounting for 0.71% of the total effect. The SEM approach indicated an acceptable model fit, with CFI = 0.908, AGFI = 0.940, GFI = 0.976, RMSEA = 0.052, and SRMR = 0.048.
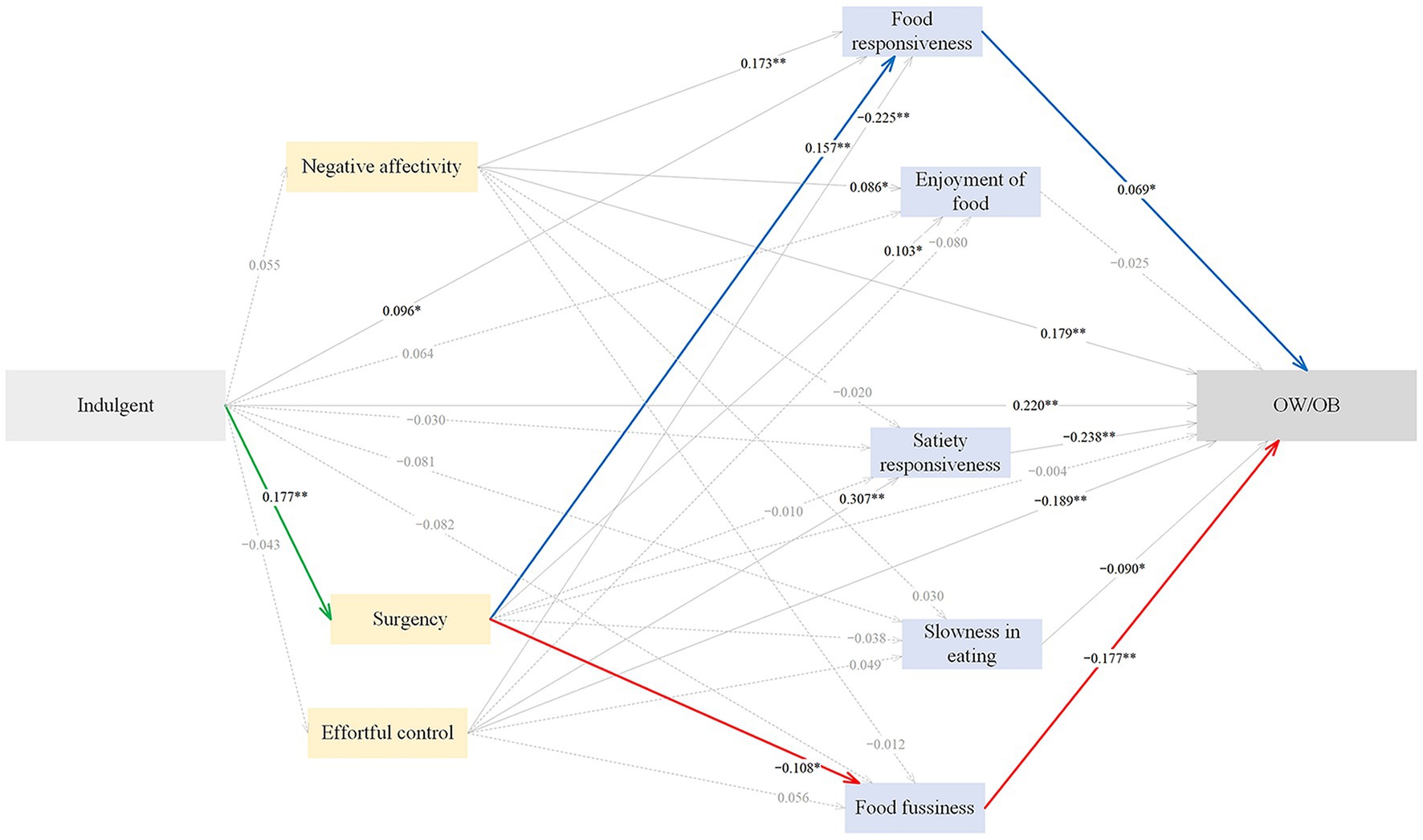
Figure 4. The standardized direct effects of indulgent feeding on OW/OB via temperament and eating behaviors in childhood. For simplicity the covariates (children sex and maternal education) and measurement error terms are not shown. Dotted lines depict non-significant direct effect. Solid lines denote significant direct effect, and the bold green, blue and red solid lines represent sequential mediation effects. Model fit: CFI = 0.908, AGFI = 0.940, GFI = 0.976, RMSEA = 0.052, SRMR = 0.0478. OW/OB, overweight and obesity. *p < 0.05, **p < 0.01.
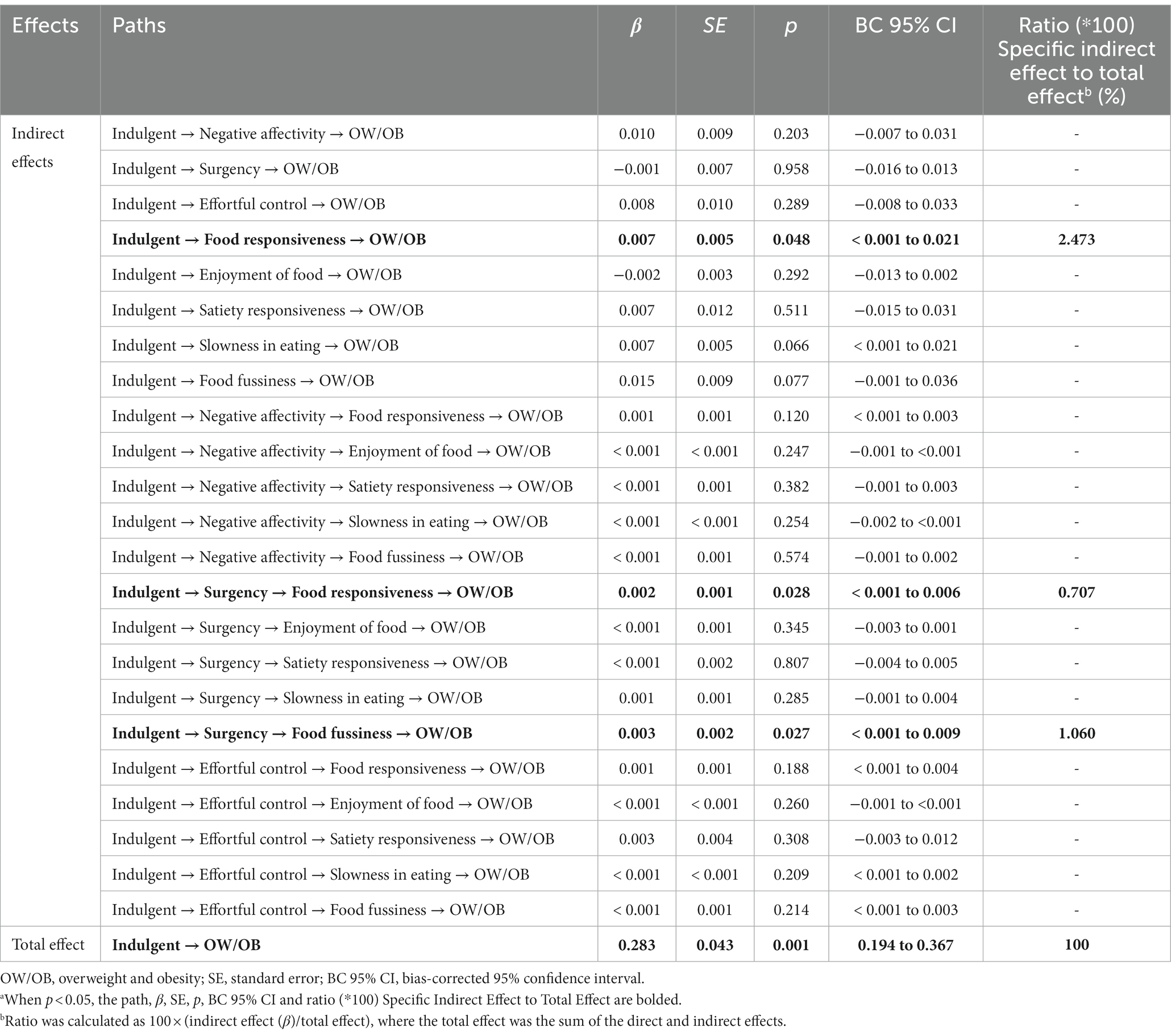
Table 7. Standardized indirect and total effects of indulgent feeding on OW/OB via temperament and eating behaviors in childhooda.
The standardized path estimates of the pathways from pressuring feeding to childhood OW/OB through temperament and eating behaviors are shown in Figure 5 and Table 8. Pressuring feeding had significant direct (β = −0.116), indirect (β = −0.096) and total (β = −0.212) effects on childhood OW/OB. 54.72% of the total effect was direct, and 45.28% was indirect. Pressuring feeding negatively predicted childhood OW/OB through higher food fussiness (β = −0.036) and higher slowness in eating (β = −0.017), accounting for 16.98 and 8.02% of the total effect, respectively. The SEM approach indicated an acceptable model fit, with CFI = 0.909, AGFI = 0.941, GFI = 0.976, RMSEA = 0.051, and SRMR = 0.048.
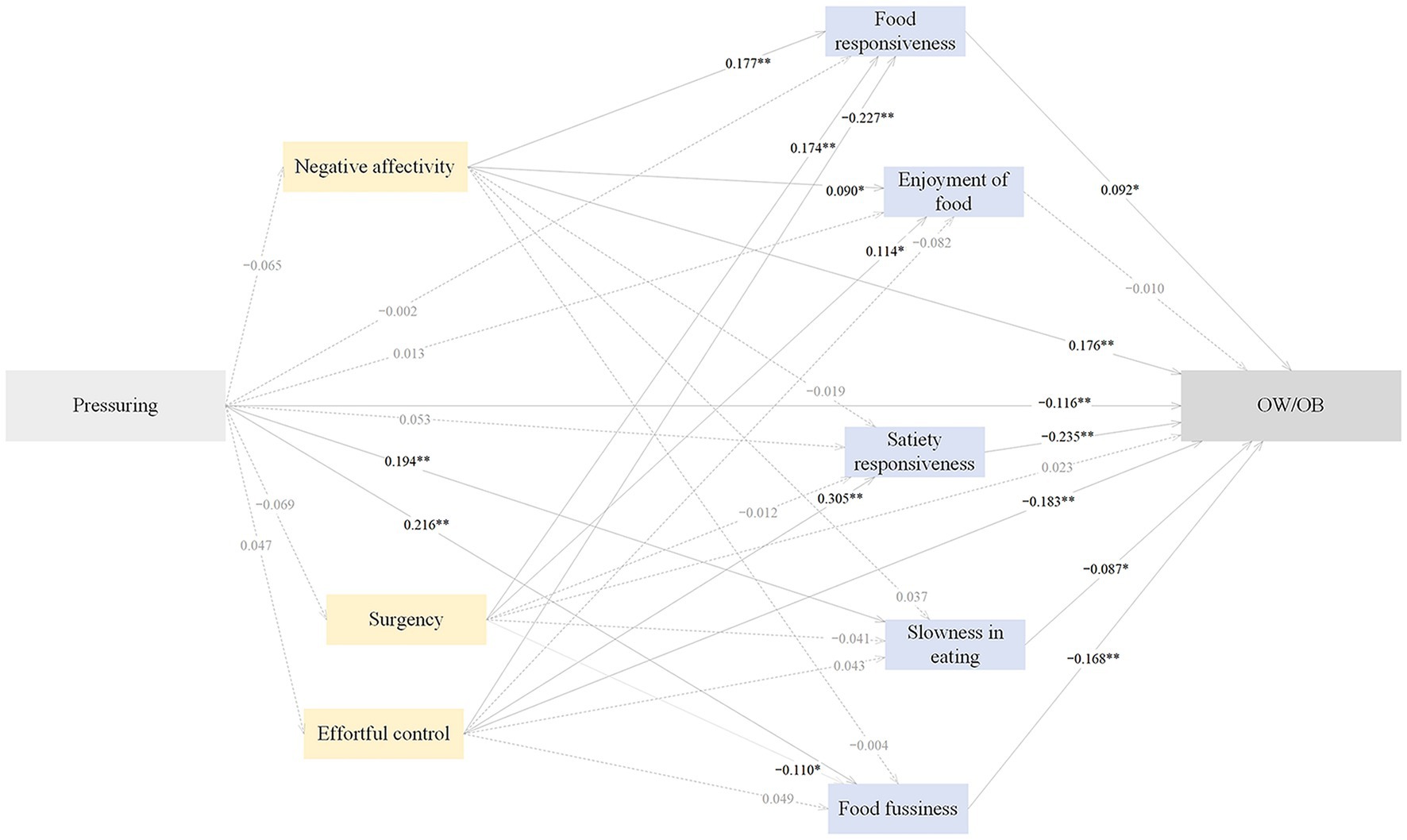
Figure 5. The standardized direct effects of pressuring feeding on OW/OB via temperament and eating behaviors in childhood. Note. For simplicity the covariates (children sex and maternal education) and measurement error terms are not shown. Dotted lines depict non-significant direct effect. Solid lines denote significant direct effect. Model fit: CFI = 0.909, AGFI = 0.941, GFI = 0.976, RMSEA = 0.051, SRMR = 0.0476. OW/OB, overweight and obesity. *p < 0.05, **p < 0.01.
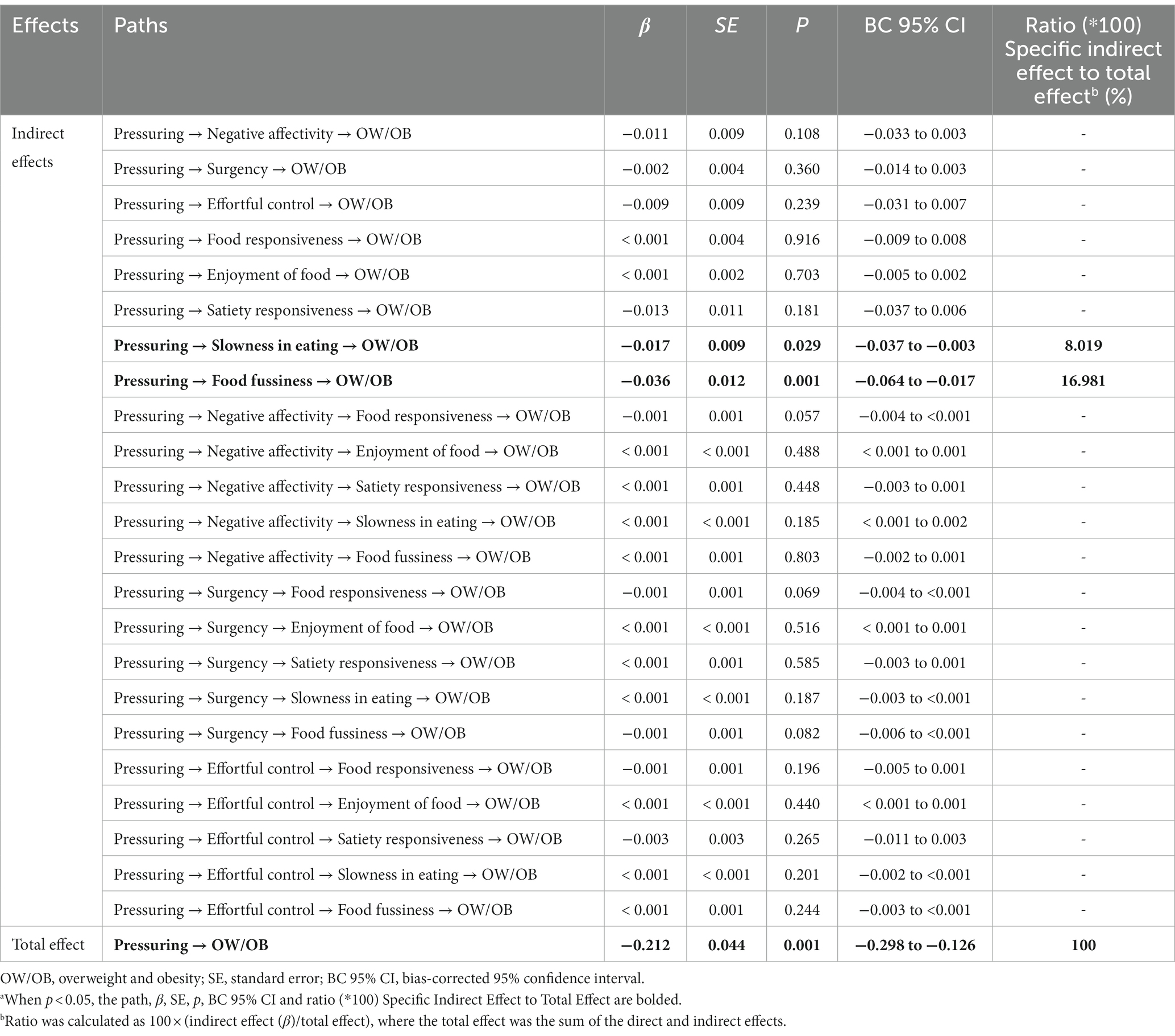
Table 8. Standardized indirect and total effects of pressuring feeding on OW/OB via temperament and eating behaviors in childhooda.
The pathways from laissez-faire feeding to childhood OW/OB through temperament and eating behaviors were non-significant (p > 0.05) (Figure 6; Table 9).
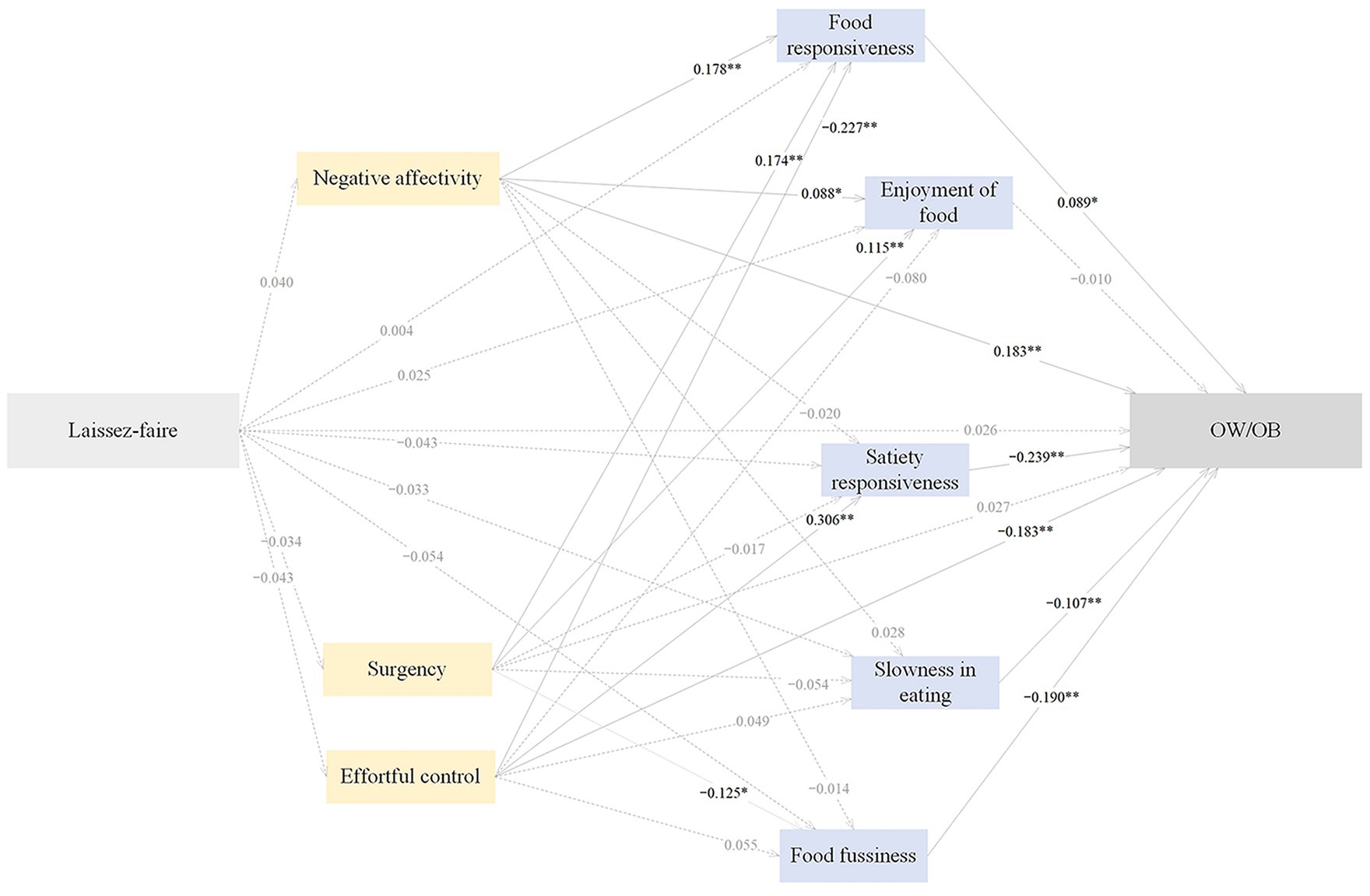
Figure 6. The standardized direct effects of laissez-faire feeding on OW/OB via temperament and eating behaviors in childhood. For simplicity the covariates (children sex and maternal education) and measurement error terms are not shown. Dotted lines depict non-significant direct effect. Solid lines denote significant direct effect. Model fit: CFI = 0.892, AGFI = 0.940, GFI = 0.976, RMSEA = 0.052, SRMR = 0.0483. OW/OB, overweight and obesity. *p < 0.05, **p < 0.01.
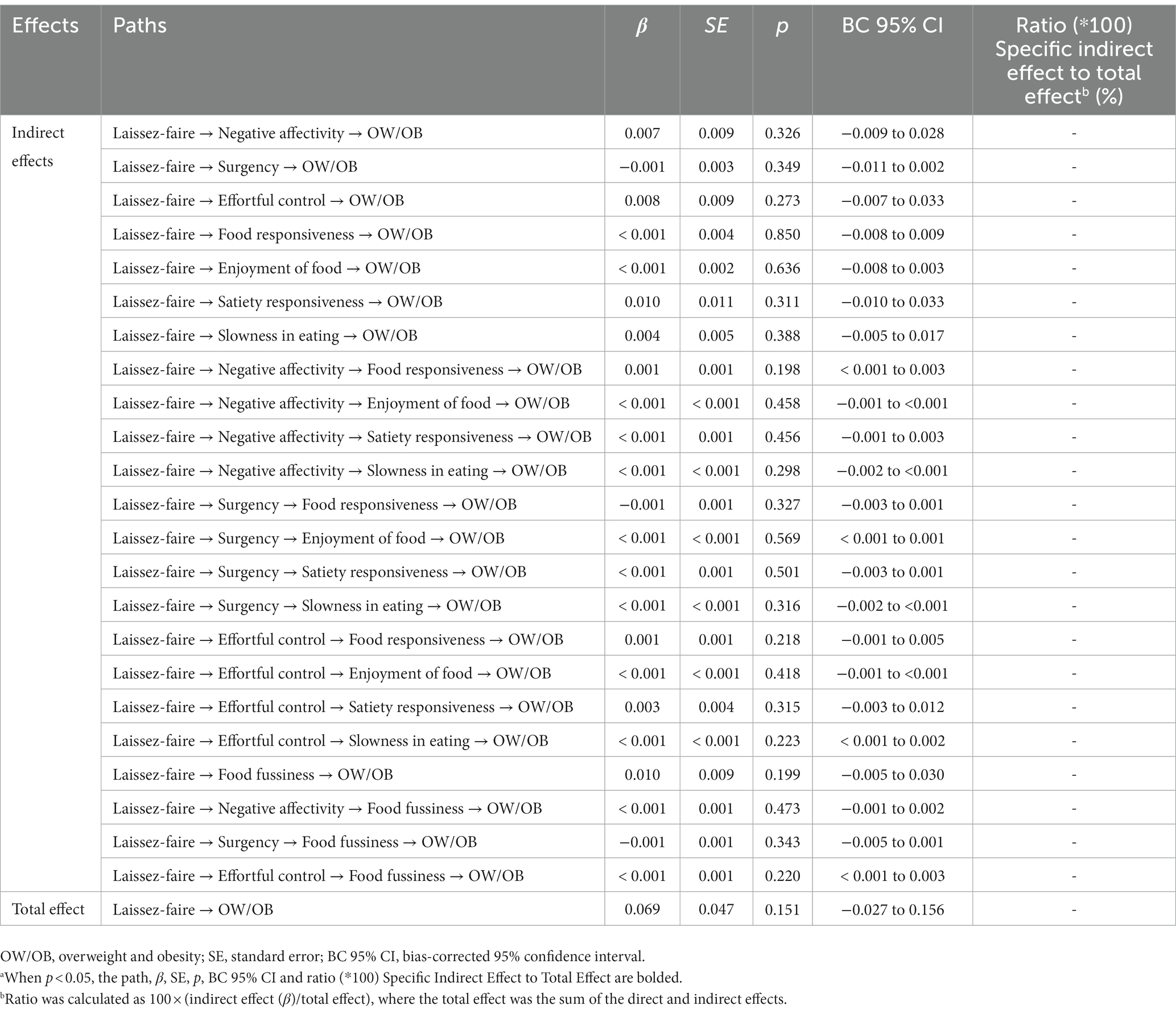
Table 9. Standardized indirect and total effects of laissez-faire feeding on OW/OB via temperament and eating behaviors in childhooda.
The novelty of this cross-sectional study lies in attempting to identify the pathways from feeding practices to childhood OW/OB through eating behaviors and temperament among children aged 6–23 months in the setting of low and middle-income countries (LMICs). Responsive feeding negatively predicted childhood OW/OB through the sequential mediation of higher effortful control and satiety responsiveness, and the sequential mediation of higher effortful control and lower food responsiveness, the sequential mediation of lower negative affectivity and food responsiveness, respectively. Restrictive feeding positively predicted childhood OW/OB through the sequential mediation of lower effortful control and satiety responsiveness, the sequential mediation of lower effortful control and higher food responsiveness, and the sequential mediation of higher surgency and lower food fussiness, respectively. Indulgent feeding positively predicted childhood OW/OB through the sequential mediation of higher surgency and food responsiveness.
Infant and young child with higher appetites and weight gains in the first 2 years of life, had a higher feeding frequency and were less sensitive to satiety cues (48). Responsive feeding promotes healthy weight gain by enhancing the development of self-regulation, highly controlling feeding that may disrupt the development of self-regulation in childhood and lead to the overconsumption of restricted foods (34). Responsive feeding is characterized by high responsivity and moderate restriction of diet quality and quantity (34), is associated with higher diet quality (49), lower weight status (50), and a reduced risk of obesity (51), compared with highly controlling feeding (52). In this study, Chinese mothers reported higher responsive feeding, consistent with previous study (3), directly predicted lower childhood OW/OB; and indirectly predicted lower childhood OW/OB through the sequential mediation of childhood eating behaviors and temperament. Responsive feeding encourages children to eat autonomously in response to physiological needs, encouraging self-regulation in eating and supporting cognitive, emotional, and social development in infants and young children (53). Children with responsive mothers were a lower proportion of those classified as OW/OB (54), and mothers were less likely to pressure children to eat or use food as a reward (50). Responsive mothers less frequently used food to soothe distressed children and their children had lower perceived emotional overeating, while mothers responding to distressed children in early life had implications for the development of maladaptive eating in later childhood (55). However, in this study, mothers did not report emotional overeating. Due to the escalating sociometric ratings and obesogenic environment over the past four decades in China, children are likely to develop obesogenic eating behaviors. In response, parents who engage in responsive feeding may improve childhood satiety responsiveness behavior to prevent childhood OW/OB (56).
Non-responsive feeding involving the restriction of food quantity and quality, and was found to be higher in Chinese mothers than in a diverse USA sample, it has been identified as a detrimental factor in appetite regulation among children (57). Restrictive feeding is associated with poorer self-regulation of appetite and limited consumption of fruits and vegetables (58). Fruit and vegetable consumption is related to obesity prevention, but restrictive feeding may result in later preference for restricted foods and increased consumption of these restricted foods when the restriction is removed, potentially increasing the risk of obesity over time (59). Restrictive feeding shows a positive association with food responsiveness behavior and a negative association with satiety responsiveness behavior, the findings in this study consistent with Western developed countries (20). Restrictive feeding was positively correlated with food responsiveness (23), which may increase childhood desire to eat forbidden food (17). Restricting access to a palatable food has been found to increase energy intake in children (60), children may learn to respond to food cues rather than internal cues of hunger and satiety, and parents who adopt highly restrictive feeding may be associated with a higher risk of childhood OW/OB (61). This study showed restrictive feeding was not associated with food fussiness behavior in children, which is not in line with a UK study (62). Previous studies either did not found that higher restrictive feeding was associated with higher childhood OW/OB (63), or that higher restrictive feeding reduced the risk of weight gain (64). In this study, restrictive feeding was directly associated with higher childhood OW/OB, positively predicted childhood OW/OB through the sequential mediation of lower effortful control and satiety responsiveness, and the sequential mediation of lower effortful control and higher food responsiveness, respectively.
Pressuring feeding has been associated with lower intuitive eating and higher disordered eating behaviors in children (65). Previous studies either did not report an association between pressuring feeding and childhood OW/OB (66), or report the association of pressuring feeding with poorer diet quality (67), lower weight status (68), and lower childhood OW/OB (10). This study revealed that food avoidant behaviors, e.g., slowness in eating and food fussiness were mediators in the association between pressuring feeding and childhood OW/OB. These findings are consistent with studies in the UK and Nigeria, which found that pressuring feeding was associated with slowness in eating and satiety responsiveness behaviors (69). However, an Australian study did not report any relationship between pressuring feeding and food fussiness behavior (23). A Norwegian study showed that higher pressuring feeding, e.g., using food as a reward, predicted increased food approach behaviors, e.g., enjoyment of food (70). However, a Ethiopian study did not report an association between pressuring feeding and food approach behaviors, e.g., food responsiveness and enjoyment of food (17). In LMICs, where food scarcity and undernutrition were major threats to childhood survival in the past, feeding practices have evolved in response to these threats (71). Pressuring feeding, e.g., encouraging children to finish food is customary in LMICs cultures, this area has not received enough research and social attention, which may be why Chinese mothers in this study did not report their children engaging in emotional overeating behavior, as they may not distinguish emotional overeating from “big appetite” (17).
Laissez-faire feeding can be conceptualized as the opposite of monitoring (72), previous studies either report that higher monitoring was associated with less childhood overweight (73), or did not report this association (74). In this study, no pathways were identified from pressuring and laissez-faire feeding to childhood OW/OB through the sequential mediation of childhood eating behaviors and temperament. Indulgent feeding is significantly associated with higher consumption of unhealthy foods and lower nutrient intake in children (7), and higher childhood OW/OB (75). Children with indulgent parents were found to gain excess weight (76), Chinese mothers with lower indulgent feeding positively restricted the amount of unhealthy foods for their children (7), this study showed that Chinese mothers engaged in lower indulgent feeding, positively predicted childhood OW/OB through lower food fussiness. In a USA study, children with higher negative affectivity significantly experienced pressuring feeding, and food fussiness behavior (77).
Few studies have focused on the mediators of childhood temperament and eating behaviors in the relationship between feeding practices and childhood OW/OB. Previous studies reported that temperament was associated with feeding practices (78), childhood eating behaviors (79), and childhood OW/OB (9). The combination of feeding practices and temperament has been identified as important predictor in predicting childhood eating behaviors and the risk of OW/OB (4). In similar environments, inherent characteristic of children can be influenced differently, e.g., infants with a highly negative temperament may respond distinctively to parental soothing, potentially impacting early childhood development depending on feeding practices (4). In the development of childhood temperament related to eating behaviors, the process may occur within feeding practices where parents who tend to one type of feeding practices, e.g., restrictive feeding interacts with emotionally reactive children, may forgo restriction in favor of calming emotional children (4). This study did not report any effect of restriction feeding on negative affectivity and surgency. Feeding practices may be based on childhood temperament, e.g., parents adapted the restriction feeding to soothe or reward foods to children with negative temperament; and inhibited children were more likely to develop food neophobia, especially when their parents reported pressuring feeding (80). However, this study did not report any effect of restrictive feeding on negative affectivity. Parents may also soothe infants using food with higher surgency (higher activity and approach to novelty or reward) (9). This study did not report the sequential mediation from pressuring feeding to childhood eating behaviors and OW/OB.
Infants exhibit effortful control, characterized by the ability to initiate, maintain, and cease activities and awareness of rules (4). Attentional behaviors, e.g., focusing and sustained attention, form the foundation of effortful control (81), and the emergence of temperament-based effortful control (82) is significantly associated with the development of childhood OW/OB (83). In this study, responsive and restrictive feedings negatively predicted childhood OW/OB through effortful control, food responsiveness and satiety responsiveness. Negative affectivity of temperament was significantly associated with neophobic eating behaviors (80), and the risk of obesity (84). Difficult temperament is reliable measure of negative emotionality (4), and indulgent feeding is directly related to childhood food fussiness, mediated by negative affectivity (35). Anger reactivity is the emotion responsible for the relationship with overeating, while fear reactivity is highly related to undereating (4). Higher negative affectivity was related to higher pressuring feeding and childhood food fussiness (77). Fear reactivity is significantly related to food neophobia (4), and reactivity and regulation affects childhood OW/OB (85). Thus, temperament is indirectly associated with feeding practices, childhood eating behaviors and OW/OB (4). Negative affectivity predicts food approach behaviors, e.g., emotional overeating, and food avoidant behaviors, e.g., food fussiness and emotional undereating (86). This study reported that responsive feeding negatively predicted childhood OW/OB through the sequential mediation of negative affectivity and enjoyment of food. The frequency of consumption of sugar-rich foods and drinks (SFD) depended on childhood negative affectivity, children with higher negative affectivity consumed higher SFD when plenty of these foods were available (87). Children with effortful control were positively associated with self-regulated satiety responsiveness, and negatively associated with childhood OW/OB (86). This study reported that only responsive feeding was directly associated with the effect of childhood negative affectivity behaviors on OW/OB through food responsiveness behavior. This study did not report surgency behavior as a mediator in the pathways from feeding practices to childhood behaviors and OW/OB.
To the best of our knowledge, this is the first study in a LMIC to identify the pathways from maternal feeding practices to childhood OW/OB through the mediators of childhood temperament and eating behaviors. The SEM combines confirmatory factor analysis (CFA) and path analysis estimating latent variables, attributes the relationship among variables. The SEM approach including sociodemographic variables as covariates is valuable in providing methodological challenges in estimating direct and indirect effects through multiple pathways to propose targeted interventions. This study provides relevant evidence regarding maternal feeding practices, and the mediators of childhood temperament and eating behaviors, can guide intervention strategies aimed at preventing childhood OW/OB. The research design provided a varied sample including lower socioeconomic status (SES) families, e.g., mothers with lower education. The study sample primarily consisted of unemployed mothers (55%) who did not regularly take their children for health checkups, which indicates inadequate data collection on infant and young child aged 0–3 years and their families, particularly in LMICs, allowing governments to avoid the responsibilities for progressing of infant and young child feeding. The participants were sampled from a population not studied well in the same field. This sudy combined physical measurements of BMIz to determine the childhood OW/OB status. Policymakers in LMICs should prioritize improving maternal feeding practices through childhood temperament and eating behaviors to prevent childhood OW/OB. Such action is required to adopt new or enhanced national data collections and analytical approaches, e.g., incorporating infant and young child feeding practices into national health systems, a healthcare professional training on infant and young child feeding. Recommendations for using fiscal policy to make larger investments in maternal, infant, and young child health and nutrition are warranted. Longitudinal studies with large and representative population samples are essential to further fully elucidate the pathways linking maternal feeding practices and childhood OW/OB regrading childhood eating behaviors and temperament when designing mitigation intervention strategies.
This cross-sectional study is limited for the interpretation of the causality, and maternal feeding practices, childhood eating behaviors and temperament are dynamic and changing landscapes. Feeding practices, childhood temperament, and eating behaviors were measured using primarily maternal report data, which are of particular concern (4), but the maternal feeding practices may well reflect maternal concern about the infant and young child being over-or underweight. There is one measurement of BMIz, the conclusions maybe shallow and overstated. This study did not collect other factors that can be the participation in the feeding activity as confounding effects, e.g., grandparents’ involvement in feeding practices. This study had a unidirectional perspective, maternal feeding is a dynamic process to which both child and mother contribute (88), further studies of bidirectional relationships between maternal feeding practices and childhood temperament, eating behaviors and OW/OB are required.
Feeding practices negatively predicted childhood OW/OB through the mediators of childhood temperament and eating behaviors in children aged 6–23 month, which may be beneficial to identify early interventions of healthy weight trajectories. This study could help governments agencies, policymakers, and healthcare workers to establish optimal intervention programs targeting maternal feeding practices through childhood eating behaviors and temperament to prevent childhood OW/OB in LMICs.
The data analyzed in this study is subject to the following licenses/restrictions: availability of data and materials. The datasets generated and analyzed during the current study are not publicly available due to original consent, but are available from the corresponding author upon reasonable request. Requests to access these datasets should be directed to XZ, eGlhb25pbmcuemhhbmcyMkBvdXRsb29rLmNvbQ==.
The studies involving humans were approved by Xuzhou Medical University ethics committee. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
XZ designed and supervised the study, prepared the manuscript, developed the conceptual framework, analyzed the data, interpreted the results, and wrote the original and final manuscript. QZ developed the conceptual framework, collected, analyzed, and interpreted the results. WL and SW aided in interpreting the results. NV drafted the final manuscript. JC managed and supervised the study. All authors have read and agreed to the published version of the manuscript.
This study was funded by the Key Research Development project of Xuzhou (KC22295), and Hangzhou Normal University. This project was also supported by the Scientific Research Fund of Zhejiang Provincial Education Department (y202351682). The funding bodies were not involved in the study design, data collection, or data analysis, or in the writing of the manuscript.
The authors thank all the participants volunteered in this study. We also thank the editors and reviewers for their invaluable comments to improve the quality of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1122645/full#supplementary-material
1. Savage, JS, Birch, LL, Marini, M, Anzman-Frasca, S, and Paul, IM. Effect of the INSIGHT responsive parenting intervention on rapid infant weight gain and overweight status at age 1 year: a randomized clinical trial. JAMA Pediatr. (2016) 170:742–9. doi: 10.1001/jamapediatrics.2016.0445
2. Pang, WW, and McCrickerd, K. The impact of feeding experiences during infancy on later child eating behaviours. Curr Opin Clin Nutr Metab Care. (2021) 24:246–51. doi: 10.1097/MCO.0000000000000744
3. Zhang, X, Rosenthal, DM, Benton, L, and Lakhanpaul, M. Cultural influences on complementary feeding beliefs amongst new Chinese immigrant mothers in England: a mixed methods study. Int J Environ Res Public Health. (2020) 17:5468. doi: 10.3390/ijerph17155468
4. Stifter, CA, and Moding, KJ. Temperament in obesity-related research: concepts, challenges, and considerations for future research. Appetite. (2019) 141:104308. doi: 10.1016/j.appet.2019.05.039
5. Hughes, SO, Power, TG, O’Connor, TM, Fisher, JO, Micheli, NE, and Papaioannou, MA. Maternal feeding style and child weight status among Hispanic families with low-income levels: a longitudinal study of the direction of effects. Int J Behav Nutr Phys Act. (2021) 18:30. doi: 10.1186/s12966-021-01094-y
6. Vaughn, AE, Ward, DS, Fisher, JO, Faith, MS, Hughes, SO, Kremers, SPJ, et al. Fundamental constructs in food parenting practices: a content map to guide future research. Nutr Rev. (2016) 74:98–117. doi: 10.1093/nutrit/nuv061
7. Zhang, X, and Benton, L. The Association of Acculturation and Complementary Infant and young child feeding practices among new Chinese immigrant mothers in England: a mixed methods study. Int J Environ Res Public Health. (2019) 16:3282. doi: 10.3390/ijerph16183282
8. Hughes, SO, Power, TG, Papaioannou, MA, Cross, MB, Nicklas, TA, Hall, SK, et al. Emotional climate, feeding practices, and feeding styles: an observational analysis of the dinner meal in head start families. Int J Behav Nutr Phys Act. (2011) 8:60. doi: 10.1186/1479-5868-8-60
9. Stifter, CA, and Moding, KJ. Infant temperament and parent use of food to soothe predict change in weight-for-length across infancy: early risk factors for childhood obesity. Int J Obes. (2018) 42:1631–8. doi: 10.1038/s41366-018-0006-4
10. Shloim, N, Edelson, LR, Martin, N, and Hetherington, MM. Parenting styles, feeding styles, feeding practices, and weight status in 4-12 year-old children: a systematic review of the literature. Front Psychol. (2015) 6:1849. doi: 10.3389/fpsyg.2015.01849
11. Putnam, SP, Helbig, AL, Gartstein, MA, Rothbart, MK, and Leerkes, E. Development and assessment of short and very short forms of the infant behavior questionnaire-revised. J Pers Assess. (2014) 96:445–58. doi: 10.1080/00223891.2013.841171
12. Wittig, SMO, and Rodriguez, CM. Emerging behavior problems: bidirectional relations between maternal and paternal parenting styles with infant temperament. Dev Psychol. (2019) 55:1199–210. doi: 10.1037/dev0000707
13. Saudino, KJ. Behavioral genetics and child temperament. J Dev Behav Pediatr. (2005) 26:214–23. doi: 10.1097/00004703-200506000-00010
14. Silva Garcia, K, Power, TG, Beck, AD, Fisher, JO, Goodell, LS, Johnson, SL, et al. Stability in the feeding practices and styles of low-income mothers: questionnaire and observational analyses. Int J Behav Nutr Phys Act. (2018) 15:28. doi: 10.1186/s12966-018-0656-6
15. Faith, MS, Hittner, JB, Hurston, SR, Yin, J, Greenspan, LC, Quesenberry, CP Jr, et al. Association of Infant Temperament with Subsequent Obesity in young children of mothers with gestational diabetes mellitus. JAMA Pediatr. (2019) 173:424–33. doi: 10.1001/jamapediatrics.2018.5199
16. Herle, M, Fildes, A, van Jaarsveld, C, Rijsdijk, F, and Llewellyn, CH. Parental reports of infant and child eating behaviors are not affected by their beliefs about their Twins' Zygosity. Behav Genet. (2016) 46:763–71. doi: 10.1007/s10519-016-9798-y
17. Gebru, NW, Gebreyesus, SH, Yirgu, R, Habtemariam, E, and Abebe, DS. The relationship between caregivers' feeding practices and children's eating behaviours among preschool children in Ethiopia. Appetite. (2021) 157:104992. doi: 10.1016/j.appet.2020.104992
18. Roy, S, Bandyopadhyay, S, Bandyopadhyay, L, Dasgupta, A, Paul, B, and Mandal, S. Nutritional status and eating behavior of children: a study among primary school children in a rural area of West Bengal. J Family Med Prim Care. (2020) 9:844–9. doi: 10.4103/jfmpc.jfmpc_965_19
19. Kwon, KM, Shim, J, Kang, M, and Paik, HY. Association between picky eating behaviors and nutritional status in early childhood: performance of a picky eating behavior questionnaire. Nutrients. (2017) 9:463. doi: 10.3390/nu9050463
20. Jansen, PW, Roza, SJ, Jaddoe, VWV, Mackenbach, JD, Raat, H, Hofman, A, et al. Children's eating behavior, feeding practices of parents and weight problems in early childhood: results from the population-based generation R study. Int J Behav Nutr Phys Act. (2012) 9:130. doi: 10.1186/1479-5868-9-130
21. Webber, L, Cooke, L, Hill, C, and Wardle, J. Associations between children's appetitive traits and maternal feeding practices. J Am Diet Assoc. (2010) 110:1718–22. doi: 10.1016/j.jada.2010.08.007
22. Warkentin, S, Mais, LA, Latorre, MRDO, Carnell, S, and de Aguiar CarrazedoTaddei, JA. Relationships between parent feeding behaviors and parent and child characteristics in Brazilian preschoolers: a cross-sectional study. BMC Public Health. (2018) 18:704. doi: 10.1186/s12889-018-5593-4
23. Gregory, JE, Paxton, SJ, and Brozovic, AM. Maternal feeding practices, child eating behaviour and body mass index in preschool-aged children: a prospective analysis. Int J Behav Nutr Phys Act. (2010) 7:55. doi: 10.1186/1479-5868-7-55
24. Rodgers, RF, Paxton, SJ, Massey, R, Campbell, KJ, Wertheim, EH, Skouteris, H, et al. Maternal feeding practices predict weight gain and obesogenic eating behaviors in young children: a prospective study. Int J Behav Nutr Phys Act. (2013) 10:24. doi: 10.1186/1479-5868-10-24
25. Hoffmann, DA, Marx, JM, Kiefner-Burmeister, A, and Musher-Eizenman, DR. Influence of maternal feeding goals and practices on children's eating behaviors. Appetite. (2016) 107:21–7. doi: 10.1016/j.appet.2016.07.014
26. Yee, AZ, Lwin, MO, and Ho, SS. The influence of parental practices on child promotive and preventive food consumption behaviors: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. (2017) 14:47. doi: 10.1186/s12966-017-0501-3
27. McCrickerd, K, and Forde, CG. Consistency of eating rate, Oral processing Behaviours and energy intake across meals. Nutrients. (2017) 9:891. doi: 10.3390/nu9080891
28. Moding, KJ, and Stifter, CA. Does temperament underlie infant novel food responses?: continuity of approach-withdrawal from 6 to 18 months. Child Dev. (2018) 89:e444–58. doi: 10.1111/cdev.12902
29. Haycraft, E, Farrow, C, Meyer, C, Powell, F, and Blissett, J. Relationships between temperament and eating behaviours in young children. Appetite. (2011) 56:689–92. doi: 10.1016/j.appet.2011.02.005
30. Zandian, M, Bergh, C, Ioakimidis, I, Esfandiari, M, Shield, J, Lightman, S, et al. Control of body weight by eating behavior in children. Front Pediatr. (2015) 3:89. doi: 10.3389/fped.2015.00089
31. Savage, JS, Fisher, JO, and Birch, LL. Parental influence on eating behavior: conception to adolescence. J Law Med Ethics. (2007) 35:22–34. doi: 10.1111/j.1748-720X.2007.00111.x
32. Holley, CE, Haycraft, E, and Farrow, C. Unpacking the relationships between positive feeding practices and children's eating behaviours: the moderating role of child temperament. Appetite. (2020) 147:104548. doi: 10.1016/j.appet.2019.104548
33. Russell, CG, and Russell, A. Biological and psychosocial processes in the development of Children's appetitive traits: insights from developmental theory and research. Nutrients. (2018) 10:692. doi: 10.3390/nu10060692
34. Thompson, AL, Wasser, H, Nulty, A, and Bentley, ME. Feeding style profiles are associated with maternal and infant characteristics and infant feeding practices and weight outcomes in African American mothers and infants. Appetite. (2021) 160:105084. doi: 10.1016/j.appet.2020.105084
35. Innella, N, McNaughton, D, Schoeny, M, Tangney, C, Breitenstein, S, Reed, M, et al. Child temperament, maternal feeding practices, and parenting styles and their influence on obesogenic behaviors in Hispanic preschool children. J Sch Nurs. (2019) 35:287–98. doi: 10.1177/1059840518771485
36. Kerkhoff, D, and Nussbeck, FW. The Influence of Sample Size on Parameter Estimates in Three-Level Random-Effects Models. Front. Psychol. (2019) 10:1067. doi: 10.3389/fpsyg.2019.0106742
37. Thompson, AL, Mendez, MA, Borja, JB, Adair, LS, Zimmer, CR, and Bentley, ME. Development and validation of the infant feeding style questionnaire. Appetite. (2009) 53:210–21. doi: 10.1016/j.appet.2009.06.010
38. Aminabadi, NA, Ghoreishizadeh, A, Ghoreishizadeh, M, Oskouei, SG, and Ghojazadeh, M. Can child temperament be related to early childhood caries? Caries Res. (2014) 48:3–12. doi: 10.1159/000351636
39. Hahn-Holbrook, J, Fish, A, and Glynn, LM. Human Milk Omega-3 fatty acid composition is associated with infant temperament. Nutrients. (2019) 11:2964. doi: 10.3390/nu11122964
40. de Onis, M, Onyango, AW, van den Broeck, J, Chumlea, WC, and Martorell, R. Measurement and standardization protocols for anthropometry used in the construction of a new international growth reference. Food Nutr Bull. (2004) 25:S27–36. doi: 10.1177/15648265040251S104
41. WHO Multicentre Growth Reference Study Group. WHO child growth standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: Methods and development. Geneva: World Health Organization (2006).
42. Hu, L, and Bentler, PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model Multidiscip J. (1999) 6:1–55. doi: 10.1080/10705519909540118
43. Kline, RB ed. Principles and practice of structural equation modeling. 3rd ed. New York, NY: Guilford Press (2011).
44. Mackinnon, DP. Integrating mediators and moderators in research design. Res Soc Work Pract. (2011) 21:675–81. doi: 10.1177/1049731511414148
45. Preacher, KJ, and Hayes, AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. (2008) 40:879–91. doi: 10.3758/BRM.40.3.879
46. VanderWeele, TJ. Mediation analysis: a Practitioner's guide. Annu Rev Public Health. (2016) 37:17–32. doi: 10.1146/annurev-publhealth-032315-021402
47. Fritz, MS, and Mackinnon, DP. Required sample size to detect the mediated effect. Psychol Sci. (2007) 18:233–9. doi: 10.1111/j.1467-9280.2007.01882.x
48. McNally, J, Hugh-Jones, S, Caton, S, Vereijken, C, Weenen, H, and Hetherington, M. Communicating hunger and satiation in the first 2 years of life: a systematic review. Matern Child Nutr. (2016) 12:205–28. doi: 10.1111/mcn.12230
49. Daniels, LA, Mallan, KM, Nicholson, JM, Battistutta, D, and Magarey, A. Outcomes of an early feeding practices intervention to prevent childhood obesity. Pediatrics. (2013) 132:e109–18. doi: 10.1542/peds.2012-2882
50. Savage, JS, Hohman, EE, Marini, ME, Shelly, A, Paul, IM, and Birch, LL. INSIGHT responsive parenting intervention and infant feeding practices: randomized clinical trial. Int J Behav Nutr Phys Act. (2018) 15:64. doi: 10.1186/s12966-018-0700-6
51. Hurley, KM, Cross, MB, and Hughes, SO. A systematic review of responsive feeding and child obesity in high-income countries. J Nutr. (2011) 141:495–501. doi: 10.3945/jn.110.130047
52. DiSantis, KI, Hodges, EA, Johnson, SL, and Fisher, JO. The role of responsive feeding in overweight during infancy and toddlerhood: a systematic review. Int J Obes. (2011) 35:480–92. doi: 10.1038/ijo.2011.3
53. Patrick, H, and Nicklas, TA. A review of family and social determinants of children's eating patterns and diet quality. J Am Coll Nutr. (2005) 24:83–92. doi: 10.1080/07315724.2005.10719448
54. Paul, IM, Savage, JS, Anzman-Frasca, S, Marini, ME, Beiler, JS, Hess, LB, et al. Effect of a responsive parenting educational intervention on childhood weight outcomes at 3 years of age: the INSIGHT randomized clinical trial. JAMA. (2018) 320:461–8. doi: 10.1001/jama.2018.9432
55. Harris, HA, Anzman-Frasca, S, Marini, ME, Paul, IM, Birch, LL, and Savage, JS. Effect of a responsive parenting intervention on child emotional overeating is mediated by reduced maternal use of food to soothe: the INSIGHT RCT. Pediatr Obes. (2020) 15:e12645. doi: 10.1111/ijpo.12645
56. Vollmer, RL, and Mobley, AR. Parenting styles, feeding styles, and their influence on child obesogenic behaviors and body weight. A review. Appetite. (2013) 71:232–41. doi: 10.1016/j.appet.2013.08.015
57. DiSantis, KI, Hodges, EA, and Fisher, JO. The association of breastfeeding duration with later maternal feeding styles in infancy and toddlerhood: a cross-sectional analysis. Int J Behav Nutr Phys Act. (2013) 10:53. doi: 10.1186/1479-5868-10-53
58. Gerards, SM, and Kremers, SP. The role of food parenting skills and the home food environment in Children's weight gain and obesity. Curr Obes Rep. (2015) 4:30–6. doi: 10.1007/s13679-015-0139-x
59. Rhee, KE, Lumeng, JC, Appugliese, DP, Kaciroti, N, and Bradley, RH. Parenting styles and overweight status in first grade. Pediatrics. (2006) 117:2047–54. doi: 10.1542/peds.2005-2259
60. Rollins, BY, Loken, E, Savage, JS, and Birch, LL. Effects of restriction on children's intake differ by child temperament, food reinforcement, and parent's chronic use of restriction. Appetite. (2014) 73:31–9. doi: 10.1016/j.appet.2013.10.005
61. Berhane, HY, Jirström, M, Abdelmenan, S, Berhane, Y, Alsanius, B, Trenholm, J, et al. Social stratification, diet diversity and malnutrition among preschoolers: a survey of Addis Ababa, Ethiopia. Nutrients. (2020) 12:712. doi: 10.3390/nu12030712
62. Harris, HA, Fildes, A, Mallan, KM, and Llewellyn, CH. Maternal feeding practices and fussy eating in toddlerhood: a discordant twin analysis. Int J Behav Nutr Phys Act. (2016) 13:81. doi: 10.1186/s12966-016-0408-4
63. Spill, MK, Callahan, EH, Shapiro, MJ, Spahn, JM, Wong, YP, Benjamin-Neelon, SE, et al. Caregiver feeding practices and child weight outcomes: a systematic review. Am J Clin Nutr. (2019) 109:990S–1002S. doi: 10.1093/ajcn/nqy276
64. Panagiotakos, DB, Chrysohoou, C, Pitsavos, C, and Stefanadis, C. Association between the prevalence of obesity and adherence to the Mediterranean diet: the ATTICA study. Nutrition. (2006) 22:449–56. doi: 10.1016/j.nut.2005.11.004
65. Ellis, JM, Galloway, AT, Webb, RM, Martz, DM, and Farrow, CV. Recollections of pressure to eat during childhood, but not picky eating, predict young adult eating behavior. Appetite. (2016) 97:58–63. doi: 10.1016/j.appet.2015.11.020
66. Lumeng, JC, Ozbeki, TN, Appugliese, DP, Kaciroti, N, Corwyn, RF, and Bradley, RH. Observed assertive and intrusive maternal feeding behaviors increase child adiposity. Am J Clin Nutr. (2012) 95:640–7. doi: 10.3945/ajcn.111.024851
67. Thompson, AL, Adair, LS, and Bentley, ME. Pressuring and restrictive feeding styles influence infant feeding and size among a low-income African-American sample. Obesity (Silver Spring). (2013) 21:562–71. doi: 10.1002/oby.20091
68. Dinkevich, E, Leid, L, Pryor, K, Wei, Y, Huberman, H, and Carnell, S. Mothers' feeding behaviors in infancy: do they predict child weight trajectories? Obesity (Silver Spring). (2015) 23:2470–6. doi: 10.1002/oby.21320
69. Powell, FC, Farrow, CV, and Meyer, C. Food avoidance in children. The influence of maternal feeding practices and behaviours. Appetite. (2011) 57:683–92. doi: 10.1016/j.appet.2011.08.011
70. Steinsbekk, S, Belsky, J, and Wichstrom, L. Parental feeding and child eating: an investigation of reciprocal effects. Child Dev. (2016) 87:1538–49. doi: 10.1111/cdev.12546
71. Birch, L, Savage, JS, and Ventura, A. Influences on the development of Children's eating Behaviours: from infancy to adolescence. Can J Diet Pract Res. (2007) 68:s1–s56.
72. Lumeng, JC, Kaciroti, N, Retzloff, L, Rosenblum, K, and Miller, AL. Longitudinal associations between maternal feeding and overweight in low-income toddlers. Appetite. (2017) 113:23–9. doi: 10.1016/j.appet.2017.02.016
73. Afonso, L, Lopes, C, Severo, M, Santos, S, Real, H, Durão, C, et al. Bidirectional association between parental child-feeding practices and body mass index at 4 and 7 y of age. Am J Clin Nutr. (2016) 103:861–7. doi: 10.3945/ajcn.115.120824
74. Tschann, JM, Gregorich, SE, Penilla, C, Pasch, LA, de Groat, CL, Flores, E, et al. Parental feeding practices in Mexican American families: initial test of an expanded measure. Int J Behav Nutr Phys Act. (2013) 10:6. doi: 10.1186/1479-5868-10-6
75. Tovar, A, Choumenkovitch, SF, Hennessy, E, Boulos, R, Must, A, Hughes, SO, et al. Low demanding parental feeding style is associated with low consumption of whole grains among children of recent immigrants. Appetite. (2015) 95:211–8. doi: 10.1016/j.appet.2015.06.006
76. Hennessy, E, Hughes, SO, Goldberg, JP, Hyatt, RR, and Economos, CD. Permissive parental feeding behavior is associated with an increase in intake of low-nutrient-dense foods among American children living in rural communities. J Acad Nutr Diet. (2012) 112:142–8. doi: 10.1016/j.jada.2011.08.030
77. Kidwell, KM, Kozikowski, C, Roth, T, Lundahl, A, and Nelson, TD. Concurrent and longitudinal associations among temperament, parental feeding styles, and selective eating in a preschool sample. J Pediatr Psychol. (2018) 43:572–83. doi: 10.1093/jpepsy/jsx148
78. McMeekin, S, Jansen, E, Mallan, K, Nicholson, J, Magarey, A, and Daniels, L. Associations between infant temperament and early feeding practices. A cross-sectional study of Australian mother-infant dyads from the NOURISH randomised controlled trial. Appetite. (2013) 60:239–45. doi: 10.1016/j.appet.2012.10.005
79. Godefroy, V, Trinchera, L, Darcel, N, and Rigal, N. Behavioural measures of child's eating temperament and their link with BMI. Appetite. (2017) 110:6–14. doi: 10.1016/j.appet.2016.12.005
80. Moding, KJ, and Stifter, CA. Temperamental approach/withdrawal and food neophobia in early childhood: concurrent and longitudinal associations. Appetite. (2016) 107:654–62. doi: 10.1016/j.appet.2016.09.013
81. Garon, N, Bryson, SE, and Smith, IM. Executive function in preschoolers: a review using an integrative framework. Psychol Bull. (2008) 134:31–60. doi: 10.1037/0033-2909.134.1.31
82. Blair, C, Zelazo, PD, and Greenberg, MT. The measurement of executive function in early childhood. Dev Neuropsychol. (2005) 28:561–71. doi: 10.1207/s15326942dn2802_1
83. Miller, AL, Rosenblum, KL, Retzloff, LB, and Lumeng, JC. Observed self-regulation is associated with weight in low-income toddlers. Appetite. (2016) 105:705–12. doi: 10.1016/j.appet.2016.07.007
84. Anzman-Frasca, S, Stifter, CA, and Birch, LL. Temperament and childhood obesity risk: a review of the literature. J Dev Behav Pediatr. (2012) 33:732–45. doi: 10.1097/DBP.0b013e31826a119f
85. Hughes, SO, Frankel, LA, Beltran, A, Hodges, E, Hoerr, S, Lumeng, J, et al. Food parenting measurement issues: working group consensus report. Child Obes. (2013) 9:S-95–S-102. doi: 10.1089/chi.2013.0032
86. Steinsbekk, S, Bjørklund, O, Llewellyn, C, and Wichstrøm, L. Temperament as a predictor of eating behavior in middle childhood – a fixed effects approach. Appetite. (2020) 150:104640. doi: 10.1016/j.appet.2020.104640
87. Pajulahti, R, Salmela-Aro, K, Lehto, R, Vepsäläinen, H, Lehto, E, Nissinen, K, et al. Does temperament make children differently susceptible to their home physical food environment? A cross-sectional DAGIS study on 3-6 year old Finnish children's food consumption. Appetite. (2021) 161:105140. doi: 10.1016/j.appet.2021.105140
88. Zohar, AH, Lev-Ari, L, and Bachner-Melman, R. Two to tango? The dance of maternal authority and feeding practices with child eating behavior. Int J Environ Res Public Health. (2021) 18:1650. doi: 10.3390/ijerph18041650

Keywords: feeding practices, temperament, eating behaviors, overweight and obesity, infant and young child
Citation: Zhang X, Zhou Q, Vivor NK, Liu W, Cao J and Wang S (2023) Sequential mediation of early temperament and eating behaviors in the pathways from feeding practices to childhood overweight and obesity. Front. Public Health. 11:1122645. doi: 10.3389/fpubh.2023.1122645
Edited by:
Rossella Alfano, University of Hasselt, BelgiumReviewed by:
Ada H. Zohar, Ruppin Academic Center, IsraelCopyright © 2023 Zhang, Zhou, Vivor, Liu, Cao and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoning Zhang, eGlhb25pbmcuemhhbmcyMkBvdXRsb29rLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.