 Carlos Alberto Nogueira-de-Almeida1*
Carlos Alberto Nogueira-de-Almeida1* Daniela Prozorovscaia2
Daniela Prozorovscaia2 Elaine M. Bento Mosquera3,4
Elaine M. Bento Mosquera3,4 Fábio da Veiga Ued5
Fábio da Veiga Ued5 Vanessa Caroline Campos2
Vanessa Caroline Campos2- 1Medical Department, Federal University of São Carlos, São Carlos, Brazil
- 2Nestlé Institute of Health Sciences, Nestlé Research, Lausanne, Switzerland
- 3Federal University of São Paulo, São Paulo, Brazil
- 4Medical, Scientific and Regulatory Affairs - Nestlé Nutrition/Nestlé Brazil Ltda, São Paulo, Brazil
- 5FMRP - Nutrition Department, University of São Paulo, São Paulo, São Paulo, Brazil
Background: Despite all efforts, iron deficiency anemia remains a serious public health problem among Brazilian children.
Objective: To evaluate dietary iron intake and dietary practices that interfere with the absorption of this nutrient from three regions of Brazil.
Methods: Brazil Kids Nutrition and Health Study is a cross-sectional dietary intake study in children aged 4–13.9 years old designed to investigate nutrient intakes and gaps of Brazilian children in a representative sample of households from Northeast, Southeast and South regions. Nutrient intake was assessed based on multiple-pass 24-h dietary recall and U.S. National Cancer Institute method was used to estimate usual micronutrients intakes and compliance with Dietary Reference Intakes.
Results: Five hundred sixteen individuals participated in the study (52.3% male). The top three most consumed food sources of iron were products of plant origin. Food sources of animal origin contributed with <20% of the total iron intake. Vitamin C intake was adequate, but the concomitant consumption of food sources of vitamin C with plant food sources of iron was not common. On the other hand, the concomitant intake of plant food sources of iron with food sources of iron chelators (e.g., coffee and teas) was frequent.
Conclusions: Adequate iron intake was observed in all three regions in Brazil. Children's diet showed low iron bioavailability and insufficient consumption of food sources of iron absorption stimulants. Frequent presence of iron chelators and inhibitors of iron absorption might help to explain the high prevalence of iron deficiency in the country.
Introduction
Anemia is a serious global public health problem particularly affecting young children and pregnant women (1). In Brazil, a recent nationwide meta-analysis observed a prevalence of anemia of 38, 36, 35, and 28% in the Northeast, Midwest, South and Southeast regions of Brazil, respectively, in children from 0 to 7 years old (2). Data obtained by the ENANI study showed prevalences of 10% for the country as a whole, but reaching 17% in the North and 19 % for children under 2 years of age (3). As worldwide (4), the most common cause of anemia in Brazil is iron deficiency mainly due a low consumption of dietary iron (3, 5–8). Since iron plays a fundamental role in child development, especially in the development of the central nervous system (9), iron deficiency anemia leads to important health issues as poor motor and cognitive development, growth problems and impaired immune system (10–12). There are several consequences of iron deficiency anemia in childhood, highlighting negative interference in the production and action of cytokines, in the phagocytic capacity of neutrophils and macrophages (13) and in the production of T lymphocytes (14), leading to lower immunity (15, 16), psychomotor changes (17), impairment of thyroid function at risk of affecting growth (18–21) and unsatisfactory cognitive development (9) with learning impairment (17, 22–25).
Understanding the causes underlying iron deficiency anemia is crucial and some of them have been listed to explain the high prevalence in Brazil: use of unmodified cow's milk after weaning (26) associated with the low use of fortified products in complementary feeding (27); low reserve accumulated by infants during pregnancy and lactation due to the high prevalence of iron deficiency among pregnant and lactating women (28); low bioavailability of dietary iron due to reduced intake of meat and fortified products (29); presence of iron sources mainly of plant origin, with low bioavailability, in addition to the abundance of phytates and other chelators (30, 31).
Brazilian publications evaluating food intake and nutritional factors that interfere with iron absorption in some age groups are rare, but necessary to understand the high rates of anemia in Brazilian children. For this reason, the present study aimed to evaluate dietary iron intake and dietary practices that interfere with the absorption of this nutrient in children aged 4–8 years old from three regions of Brazil.
Methods
Study design and population
The Brazil Kids Nutrition and Health Study (B-KNHS) is a cross-sectional dietary intake study in children aged 4–13.9 years old (n = 983) designed to investigate the nutrient intakes and gaps of Brazilian children in a representative sample of the three main geographic regions in Brazil (Northeast, Southeast, and South), among urban and rural households. Detailed methodology information of B-KNHS were published at a previous paper (32). The study was designed to obtain a representative sample within the three regions of interest. The sample size included four stages of selection (geographic region, state, sector, and household) to ensure maximum randomization. First, we stratified the population into nine geographical regions composed of groupings of states. We sampled a total of nine states, with at least one state in each region: Northeast, Southeast, and South. Next, population sectors were selected in proportion to the estimated the appropriate number of children. Population estimates were based on the 2008 National Household Sample Survey (PNAD), conducted by the Brazilian Institute of Geography and Statistics (IBGE). Within each selected sector, households were randomly recruited at a starting point and then field interviewers conducted a random walk through the sector, adhering to a set of rules that specified household selection according to the estimated number of children within the sector. Within eligible households, one child at the age range was randomly selected. Data from 516 children, restricting the age group to those aged between 4 and 8.9 years old, were analyzed: Northeast (n = 169), South (n = 162) and Southeast (n = 185). The number of subjects was proportional to the population in each region, with a study response rate of 70.4%. Regarding the 29.6% that did not agree to respond, we chose, for ethical reasons, not to ask why and these families were not included in the analyses.
The survey protocol and data collection instruments were approved by the institutional review boards of RTI International, Faculdade de Ciências Farmacêuticas from University of São Paulo and the National Commission for Research Ethics (Comissão Nacional de Ética em Pesquisa). Informed consent was obtained from each child's parent/guardian for participation in the study.
Data collection
In-person interviews were conducted with each child and caregiver in their house from September to December 2019. A structured questionnaire was used to collect information on socio-demographic characteristics of households and caregivers, child characteristics including anthropometric measurements, lifestyle parameters, dietary patterns, and food intakes. The Brazilian Economic Classification Criteria were used for the economic stratification of the population. The questionnaire for family economic status covered parents' schooling and the presence/absence and number of domestic appliances, vehicles, and rooms in the child's home. Families were classified into categories from A (highest) to E (lowest). All interviewers were trained on study procedures and interviewing techniques via standard protocol which was tested during a pilot study run with 60 subjects.
Dietary assessment
Nutrient intake was assessed by trained interviewers based on multiple-pass 24-h dietary recall to capture a detailed list of foods and beverages consumed by each child. Information included the quantity consumed, preparation method (e.g., boiled, fried, added sugar, salt, etc.); eating occasion (e.g., breakfast, lunch, dinner, snacks); and eating location (e.g., home, someone else's home, school, daycare, restaurant, party/event, traveling or other). A second 24-h recall was collected from a random 25% subsample to estimate within-person variance for estimating usual nutrient intakes. Parents or primary caregivers responded on behalf of children under 6 years of age. Primary caregivers were interviewed in the presence of children 6–8 years, so children could provide additional information, such as foods eaten at school. A booklet adapted for the study including food measurements guide was used to support interviewers in recording detailed information on type of food consumed and the quantity in household measurements. Intake data were entered into Nutrition Data System for Research software (NDSR, version 2018, University of Minnesota, Minneapolis, MN) to estimate energy and nutrient content of foods and beverages consumed. The data base was completed with local foods and recipes. Foods added were typically foods identified several times in the interviews or foods commonly consumed in a particular region that were not yet in the database.
Statistical analysis
All statistical analyses were performed with the use of SAS (version 9, SAS Institute Inc.) and SAS-callable SUDAAN® (version 11, RTI International) software. The U.S. National Cancer Institute method (33) was used to estimate usual micronutrients intakes and compliance with Dietary Reference Intakes (DRIs) assessing the probabilities of meeting the Estimated Average Requirement (EAR, % < EAR) and exceeding the Adequate Intake (AI, % >AI) or Tolerable Upper Intake Level (UL, % >UL). To investigate the food sources of nutrients, a food classification system was designed to group foods based on major and minor food categories. This system was based on the food classification system used in previous dietary intakes studies in young children in the USA (34), adjusted to incorporate local food culture of Brazilian children. The percentage of children consuming foods and food groups on a given day (%), amount consumed (g) and percent contribution to total energy intake (TEI) were calculated.
Results
A total of 516 individuals participated in the study (52.3% male). The distribution in social classes respects the proportion found in Brazil, in which the majority of the population is in the middle class (C1 and C2), followed by the lower classes (D and E) and a minority in the upper classes (A and B) (35). Almost 80% of the main caregivers have intermediate education, between elementary and high school. Most families have an income of more than $500 (equivalent to ~2.3 local minimum wages), and about 1/3 reported receiving financial support from the government to buy food (Table 1).
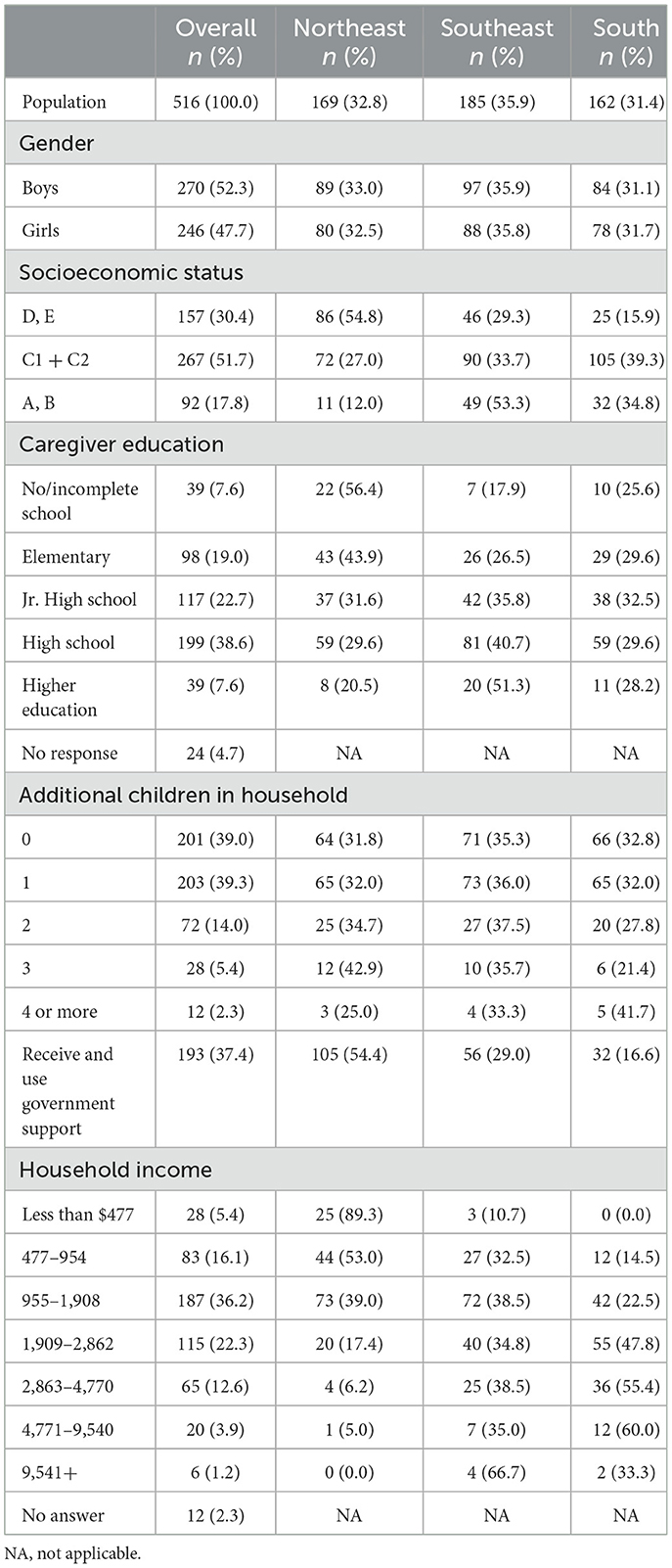
Table 1. Demographic characteristics of Brazilian children aged 4–8 years living in the Northeast, Southeast, and South regions of the country.
The inadequacy of micronutrient intake is shown in Table 2. The percentage of inadequate intake of magnesium, zinc, iron, phosphorus, niacin and folate was below 2%. Vitamins C (8%) and A (20%) also had low values of inadequate intake (Table 2). However, vitamins E, D, K and choline, as well as potassium and calcium had percentages of inadequacy above 67%. Although there is variability in the inadequacy of intake between different nutrients, higher prevalence of inadequate intakes was found among children of lower classes and for those from Northeast region.
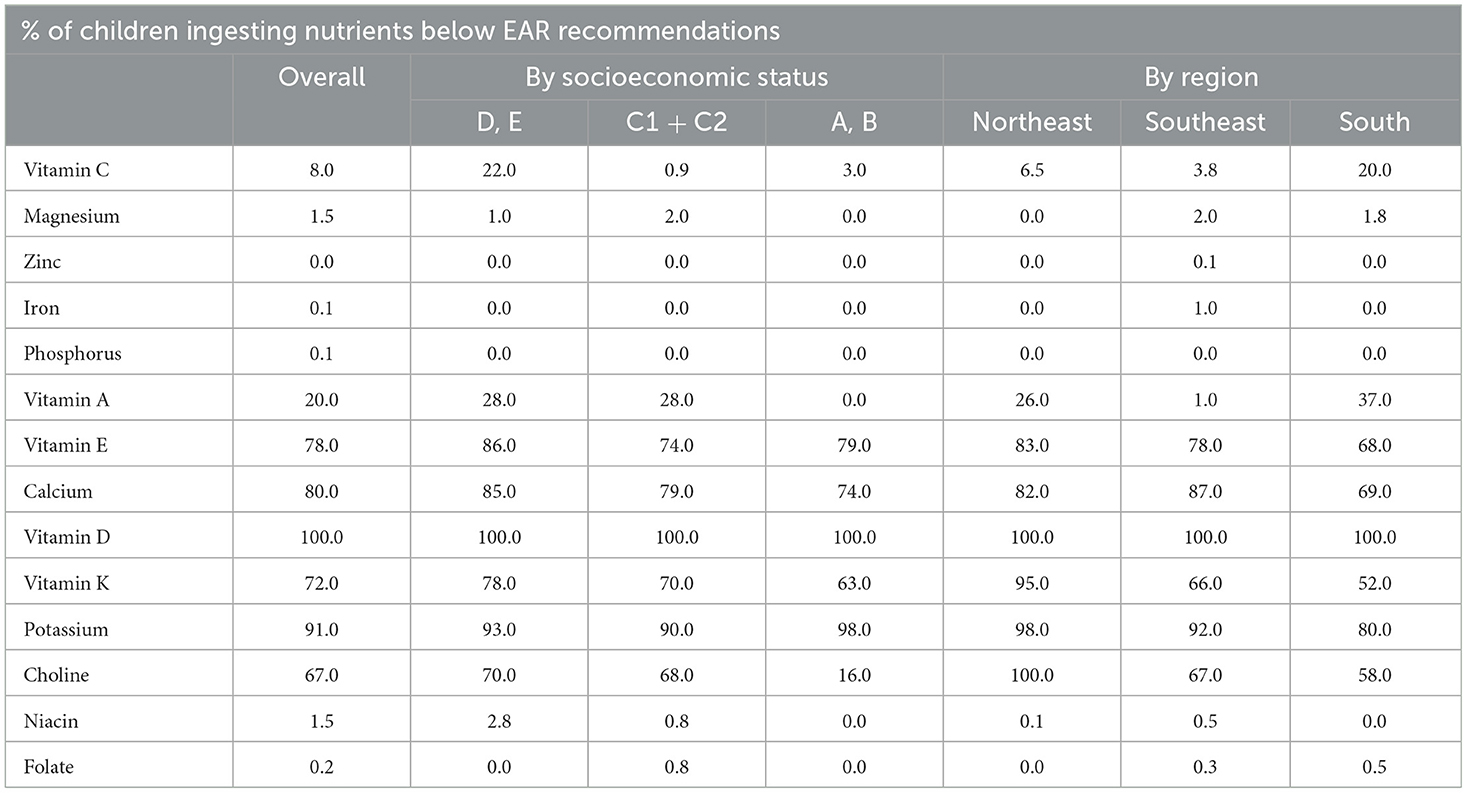
Table 2. Prevalence of inadequate intake of micronutrients by Brazilian children aged 4–8 years in the Northeast, Southeast, and South regions and according to socioeconomic status.
Regarding the consumption of food sources of iron (Table 3), for all regions, the first three most consumed food sources were products of plant origin, such as pulses, breads and sweet bakery products, which contributed with 38% of the iron daily ingested. Food sources of animal origin appeared from the fourth position and contributed with < 20% of the total iron intake, in the different regions, considering all meat and meat products together.
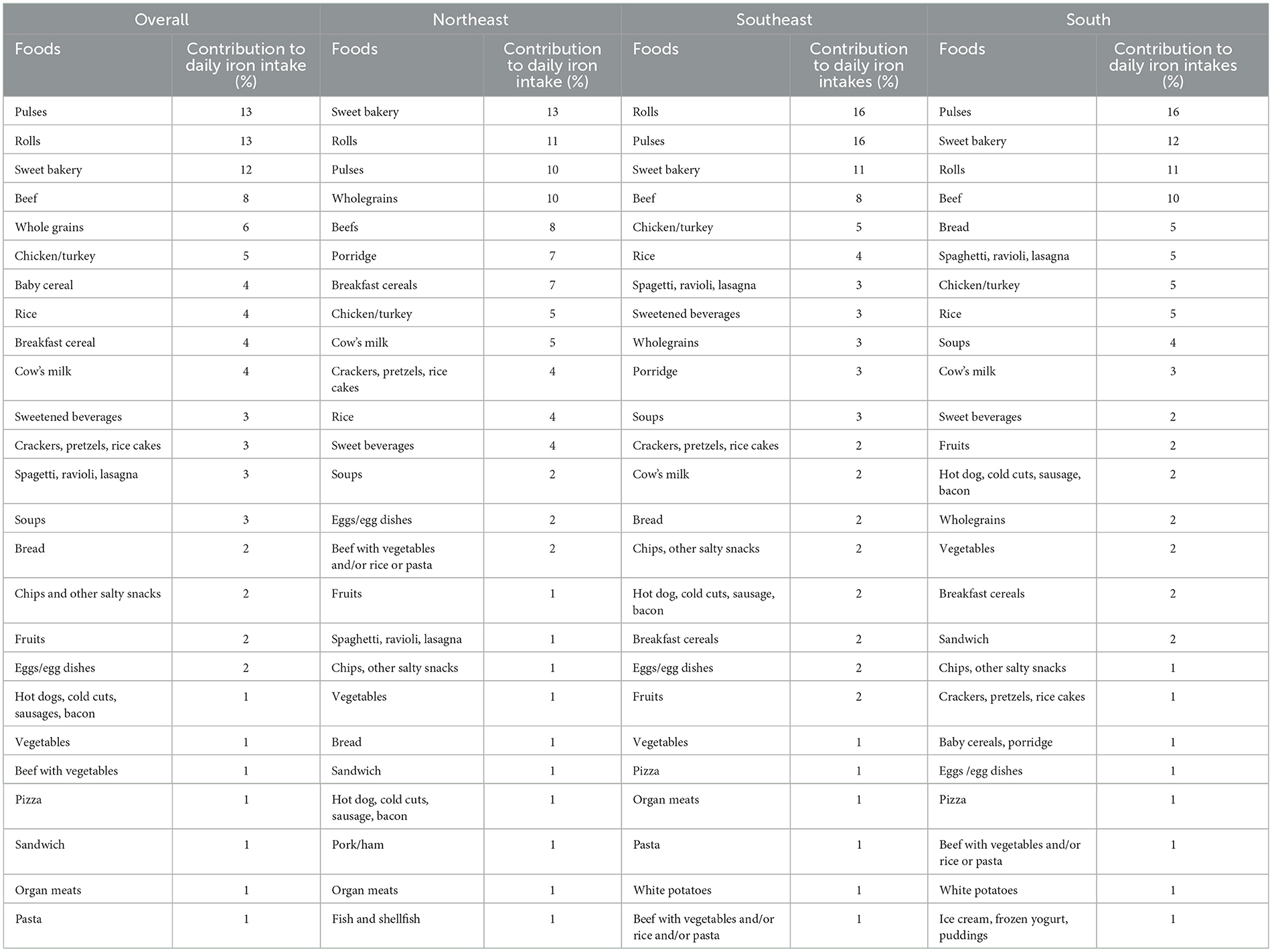
Table 3. Main dietary sources of iron consumed by Brazilian children aged 4–8 years in the Northeast, Southeast, and South regions of the country.
Almost half of Brazilian children did not consume animal food sources of iron such as beef and chicken/turkey (Figure 1). Figure 2 shows the daily per capita consumption of the five most relevant sources of iron for this sample, with 75 g/day for meat, in contrast to 112 g/day when adding up the other iron food sources. The main dietary sources of vitamin C, a stimulant of non-heme iron absorption, were artificial juices, fruits, vegetables, and 100% natural juices (Table 4).
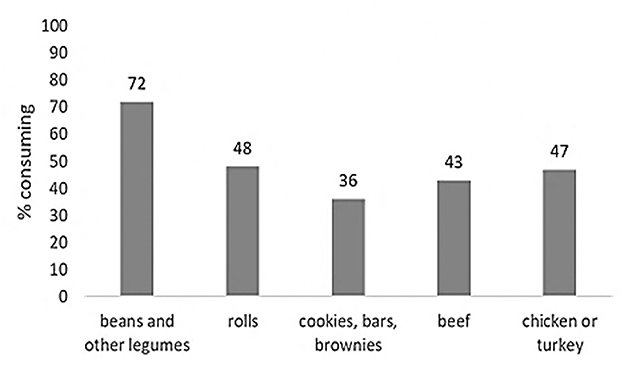
Figure 1. Percentage of Brazilian children aged 4–8 years who consume the five main dietary sources of iron.
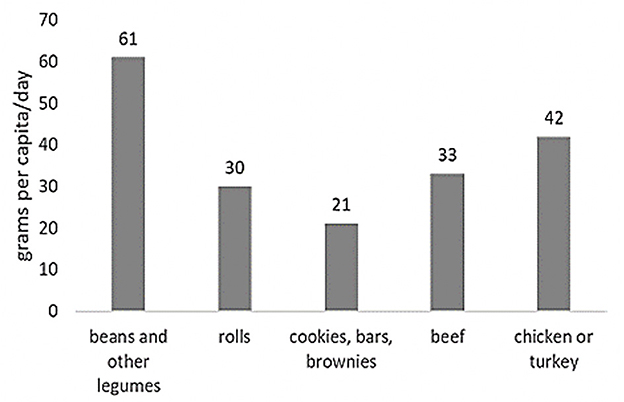
Figure 2. Per capita daily intake (g/day) of the five most relevant sources of iron in the diet of Brazilian children aged 4–8 years old.
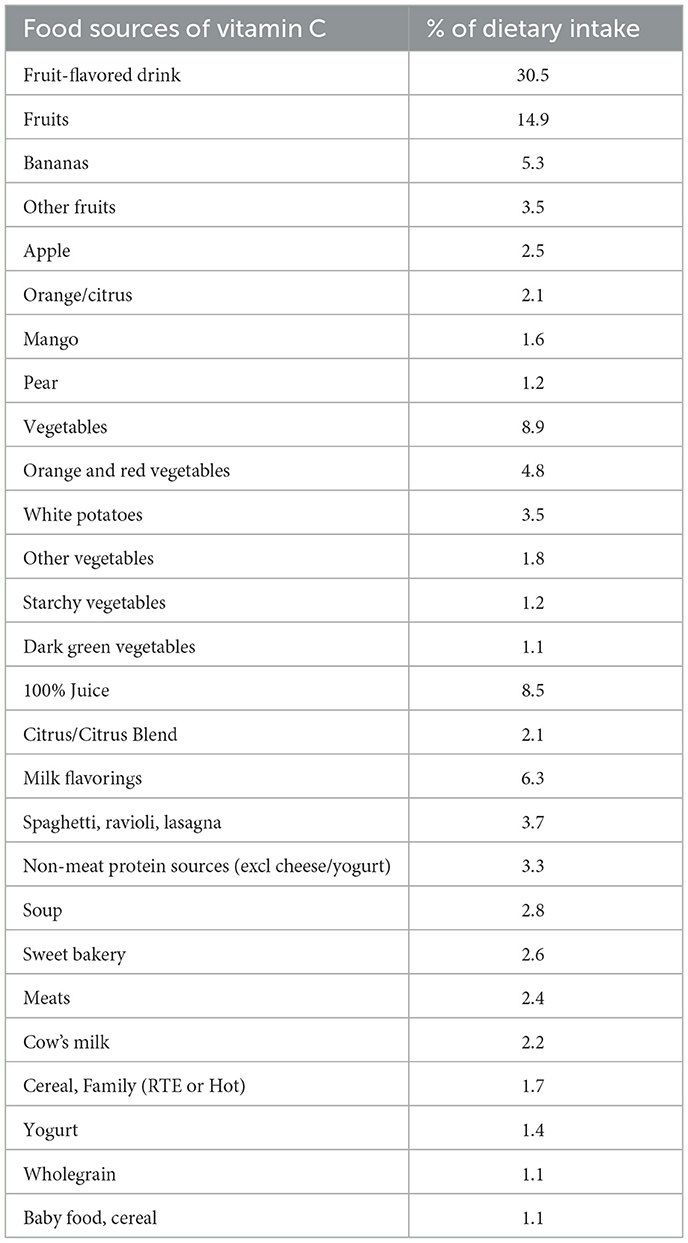
Table 4. Main dietary sources of vitamin C consumed by Brazilian children aged 4–8 years in the Northeast, Southeast, and South regions of the country.
Table 5 shows the concomitant presence of iron-rich plant foods and non-heme iron absorption stimulator/inhibitor substances in the three main daily meals (breakfast, lunch, and dinner). A breakfast, the five most consumed foods were milk, bakery products, tea, coffee, water, and milk flavoring, observing the concurrence of possible sources of iron via fortification (for example, milk and cereals) and inhibitors such as tea, coffee, and calcium. At lunch, rice, meat, breads, artificial juices, and water appear with a low prevalence of consumption of vegetable iron sources and vitamin C sources. At dinner there is a greater intake of meat, rice, water, beans, and desserts. Vegetable sources of iron are represented by beans (fourth position) associated with the consumption of vegetables and fruits that are sources of vitamin C present in the 10 first positions. However, it was also verified the presence of iron chelators in this meal, represented by tea and coffee.
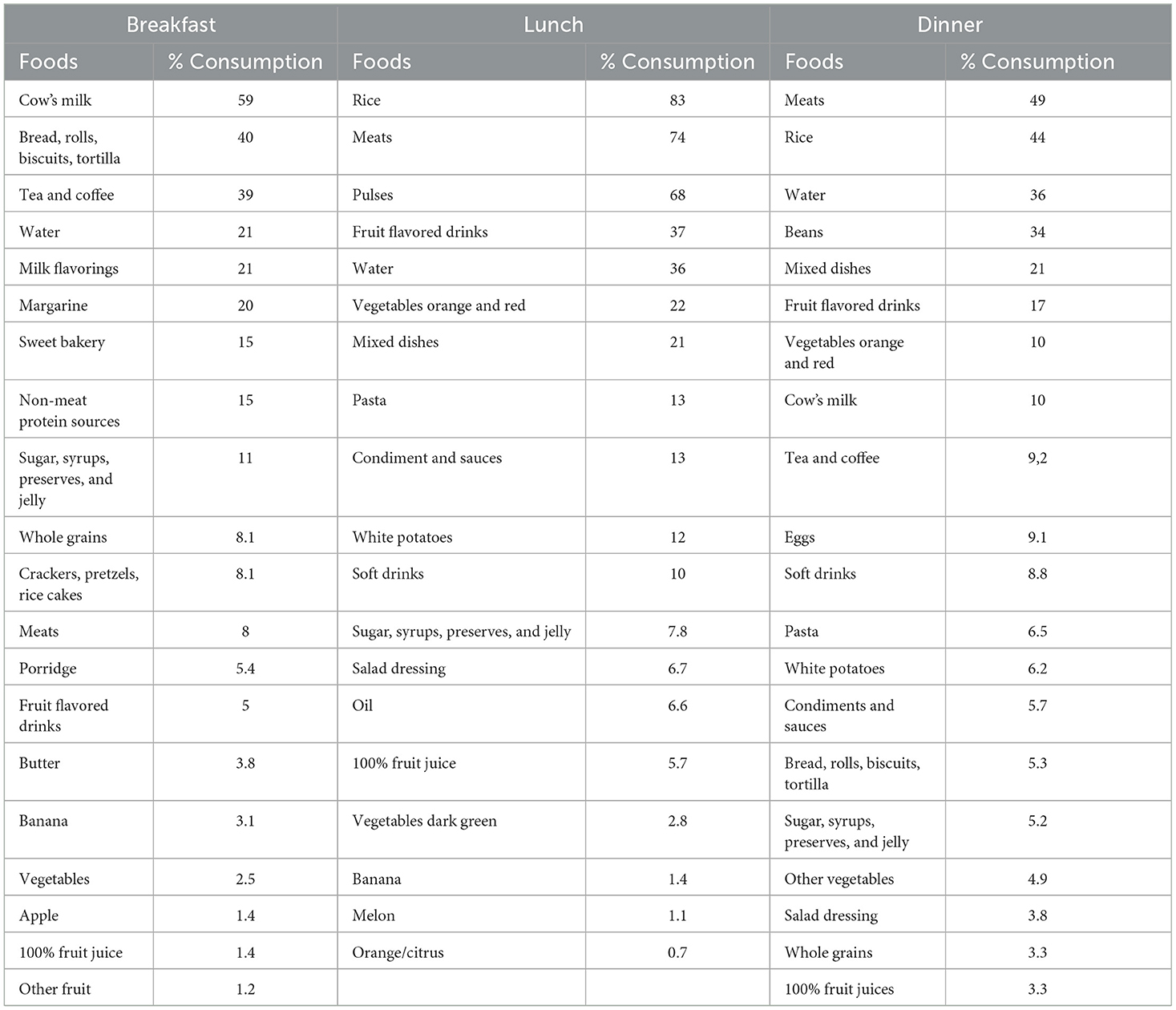
Table 5. Main foods and beverages consumed by Brazilian children aged 4–8 years in the Northeast, Southeast and South regions, for breakfast, lunch, and dinner.
Discussion
The prevalence of anemia in Brazil has shown a decline in recent years. Data from two meta-analyses (36, 37), published at 12-year intervals, show that the prevalence of anemia dropped by 23% among children aged ≤ 5 years. Despite this decrease, the numbers are still off concern due to the important impact on health. Children in the first year of life, might be at risk of not developing the necessary iron reserves and therefore, require, for the subsequent years of life, a higher intake of foods rich in high bioavailable iron, while limiting the concomitant intake of food sources of iron chelators (38).
The objectives of this study were to learn about the iron intakes, food sources of iron and dietary practices which may interfere with iron absorption of diets consumed by Brazilian children in the three most populated regions of the country. It was verified that only 30%−40% of children consumed beef or chicken in the 24 h prior to the interview. In contrast, 72% reported to consume legumes. Suggesting that the main sources of iron are of plant origin which, in addition to being of low bioavailability, they also contain iron chelators, such as phytates (30, 31). Unmodified cow's milk might also contribute to this process, especially because of the low iron content of this food and its low bioavailability (39). Although milk is often referred to as an iron chelator due to its calcium content, this fact has been questioned in other studies (40). Evidence indicates that this interference only exists when there is a concomitant intake of iron and calcium and especially when calcium intake is in amounts above the daily recommendations (DRI's) (41).
The data of the present study shows similar results to others already published, demonstrating several inadequacies of micronutrients intake (42). By the other hand, the prevalence of iron inadequate ingestion is extremely low contrasting with the high rates of anemia. This suggests that the iron requirements are covered by dietary iron, however its bioavailability might be inadequate (38). The top three food sources of iron consumed by Brazilian children were of plant origin, for all regions, representing more than 1/3 of all iron ingested. On the other hand, meat contributed with < 20% of the total iron intake and more than half of children did not consume meat in the 24 h prior to the interview. Similar results have already been observed by other authors and it is hypothesized that the intake of iron via plant sources (low bioavailability), the low intake of iron absorption stimulants (which could increase the bioavailability of non-heme iron) and the low meat consumption (high iron bioavailability) contribute significantly for iron deficiency establishment (6, 8, 10, 27, 30–32, 43).
In the study by Grillo et al. the consumption of fruits was considered insufficient in 48% of the children and vegetables in 80% (44). In the present study, similar results were found. More than 60% of children aged 4–8 years did not consume vegetables (excluding potatoes) in the 24 h prior to the interview and 58% of children did not consume fruit or fruit juices. Additionally, in the present study, it was found that the prevalence of inadequacies was more severe in the lower classes and most children from low-income families were from the Northeast (Table 1). Study by Borges et al. found a prevalence of anemia of 20.27% in children aged 7–9.9 years in Salvador, northeastern Brazil, where poverty and food intake with low iron bioavailability were the most relevant explanatory factors (6). Data from Manaus, in the North region of the country, showed a prevalence of anemia of 23.8% among 122 schoolchildren aged between 6 and 10 years; this study showed a relationship of anemia with low socioeconomic status and consumption of foods of low nutritional value and poor in iron of good bioavailability (45).
In the present study, amongst the most consumed food sources of iron were pulses and flour-based products. In Brazil, the fortification of wheat and corn flours with iron and folic acid is mandatory since 2004 (46). This may contribute to the total iron intake being adequate. However, a low impact of this fortification on the prevalence of anemia among children has already been demonstrated, possibly due to the small amount of farinaceous ingested in this age group, associated with the low bioavailability of iron added by mills (47). In addition, the consumption of foods such as beans, highly present at lunch and dinner in this sample, may not be the most viable strategy of achieving the daily recommendations of iron, considering that such group of foods presents in its composition factors that impair the absorption of iron, such as phytic acid and oxalic acid (48). It is estimated that only about 17% of the iron contained in cooked beans is used, while 34% of the iron present in the beef is available to the body (48).
The concomitant use of foods capable of stimulating the absorption of non-heme iron, especially vitamin C, could improve the utilization of iron from plant sources and fortified foods (43, 49, 50). In this context, fruits, natural juices, and even other foods fortified with ascorbic acid can help if ingested in a time close to the consumption of non-heme iron (43, 49). da Silva Ferreira et al. (51) evaluated the dietary practices of children leaving in Maceió (northeastern region of Brazil) and it was found a relationship between the presence of anemia and low consumption (< 2 portions per day) of fruits or fruit juices (51). In the present study, even though vitamin C intake was not low, temporal coincidence between the intake of food sources of iron and food sources of vitamin C was not observed in the three main meals. On the other hand, the concomitance of iron chelators, such as coffee and teas (52), was frequent.
Fortifying frequently consumed foods, such as milk, with highly available iron, can be an effective alternative to decrease iron deficiency (53), especially when fortification is based on sources of highly bioavailable iron (i.e., sulfate) or in combination with vit C (43, 53, 54), FAO/WHO considers that food fortification can be a quick and effective way to improve nutrient deficiency rates in populations (12). Furthermore, FAO/WHO recommends using highly bioavailable forms that do not alter the organoleptic characteristics of the food, and reinforces the fortification of common foods in infant feeding, such as milk, citing international experiences such as Chile, in which iron fortification in milk resulted in a rapid reduction in the rates of mineral deficiency (12). The success of this type of initiative may be in the fact that, when consumed regularly and frequently, fortified foods are able to maintain body iron stock, which is an advantage when compared to other types of initiatives, such as supplementation, which is intermittent (55).
The current study has some limitations. Food consumption in the 24 h prior to the interview does not represent the eating habits of the study population. In addition, data were collected in three Brazilian regions (Northeast, Southeast and South), leaving out two regions (North and Midwest). Despite this, it is possible to extend the data found to the entire population of Brazilian children, due to the North and Midwest regions having a human development index (HDI) and per capita income similar to the Northeast region, and due to the representative sample collected in the other regions. Finally, the questionnaire applied did not include information on the use of supplements (vitamins and minerals) that are frequently used by children and this eventual use has the potential to modify the nutritional status of micronutrients.
In conclusion, adequate iron intake was observed in all three regions of Brazil. On the other hand, the composition of the children's diet showed that the top food sources of iron were of plant origin. Moreover, within the same meal, an insufficient consumption of iron absorption stimulants, such as vitamin C, and a frequent presence of iron chelators and inhibitors of iron absorption was observed. Considering that the nutritional status of iron depends not only on the amount ingested but also on the ability of the human body to utilize the consumed iron, since the main mechanism for maintaining iron homeostasis in the human body is its absorbed amount (56), it is recommended that the bioavailability of the mineral in question be considered, to optimize its use by the human body and ensure greater fortification effectiveness. Similarly, two other factors should be considered, especially when referring to the time of consumption of foods sources of iron: the presence of other foods whose nutrients may increase their absorption (such as vitamin C), as well as the presence of chelating agents, which may negatively impact this process. Furthermore, we suggest that current dietary recommendations also include the minimum intake of highly bioavailable iron.
It is necessary to consider the use of iron-fortified foods as a viable vehicle to contribute to the intake of bioavailable iron, since several international public health interventions have already demonstrated the effectiveness of this type of action. Finally, national public campaigns are needed to inform the Brazilian parents and caregivers regarding the importance of adequate iron consumption in children and to bring awareness regarding the food practices that can help enhance the absorption of iron, taking in consideration the current diets of the Brazilian children.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The survey protocol and data collection instruments were approved by the institutional review boards of RTI International, Faculdade de Ciências Farmacêuticas from University of São Paulo and the National Commission for Research Ethics (Comissão Nacional de Ética em Pesquisa). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author contributions
CN-d-A: substantial contributions to the conception or design of the work, drafting the work or revising it critically for important intellectual content, final approval of the version to be published, figures, study design, data collection, data interpretation, and data analyses. DP: substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data for the work, drafting the work or revising it critically for important intellectual content, final approval of the version to be published, and data analyses. EM: substantial contributions to the conception of the work, final approval of the version to be published, and data interpretation. FU: substantial contributions to the conception or design of the work, or interpretation of data for the work, drafting the work, final approval of the version to be published, data collection, and data interpretation. VC: substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data for the work, drafting the work or revising it critically for important intellectual content, final approval of the version to be published, literature search, data analysis, and data interpretation. All authors contributed to the article and approved the submitted version.
Conflict of interest
Data collection was funded by the Nestlé Research Center - Switzerland. DP and VC work at Nestlé Institute of Health Sciences, Lausanne, Switzerland and EM is a post graduate student at UNIFESP and works at Nestlé Nutrition Brazil.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. WHO. WHO Global Anaemia Estimates, 2021 Edition. Geneva: WHO (2021). Available online at: https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children (accessed December 12, 2022).
2. Nogueira-de-Almeida CA, Ued FdV, Del Ciampo LA, Martinez EZ, Ferraz IS, Contini AA, et al. Prevalence of childhood anemia in Brazil: still a serious health problem. A systematic review and meta-analysis. Public Health Nutr. (2021) 24:6450–65. doi: 10.1017/S136898002100286X
3. UFRJ. Biomarkers of Micro- Nutrient Status: Prevalence of Deficiencies and Micronutrient Distribution Curves of Brazilian Children Under 5 Years of Age. Brazilian National Survey on Child Nutrition (ENANI-2019). Rio de Janeiro: Federal University of Rio de Janeiro – UFRJ (2021). Available online at: https://enani.nutricao.ufrj.br/index.php/relatorios (accessed December 10, 2022).
4. Wamer MJ, Kamran MT. Iron Deficiency Anemia. [Updated 2022 Aug 8]. Treasure Island, FL: StatPearls Publishing (2022).
5. Alves SPP, Simões MOS, Barros KNNO, da Silva RMP, Barros AMG, Medeiros CCM, et al. Fatores associados à anemia em adolescentes escolares: um estudo transversal. Res Soc Dev. (2021) 10:e3310514521. doi: 10.33448/rsd-v10i5.14521
6. Borges CQ, Silva Rde C, Assis AM, Pinto Ede J, Fiaccone RL, Pinheiro SM. [Factors associated with anemia in children and adolescents in public schools in Salvador, Bahia State, Brazil]. Cad Saude Publica. (2009) 25:877–88. doi: 10.1590/S0102-311X2009000400019
7. Hallberg L. Perspectives on nutritional iron deficiency. Annu Rev Nutr. (2001) 21:1–21. doi: 10.1146/annurev.nutr.21.1.1
8. Almeida CA, Ricco RG. Del Ciampo LA, de Souza AM, Dutra-de-Oliveira JE. Growth and hematological studies on Brazilian children of low socioeconomic level. Arch Latinoam Nutr. (2001) 51:230–5.
9. Vallée L. Iron and neurodevelopment. Arch Pediatr. (2017) 24(5s):5s18–15s22. doi: 10.1016/S0929-693X(17)24005-6
10. Allali S, Brousse V, Sacri AS, Chalumeau M, de Montalembert M. Anemia in children: prevalence, causes, diagnostic work-up, and long-term consequences. Expert Rev Hematol. (2017) 10:1023–8. doi: 10.1080/17474086.2017.1354696
11. Soliman A, Abu-Hamila N, El-Ebiary M. Assessment of Biodentine as an indirect pulp capping material in young permanent molars. Indian J Endocrinol Metab. (2014) 18:1–5. doi: 10.4103/tdj.tdj_16_18
12. WHO. Nutritional Anaemias: Tools for Effective Prevention and Control. Geneva: World Health Organization (2017). Report No.: 9241513063 Contract No.: CC BY-NC-SA 3.0 IGO.
13. Hassan TH, Badr MA, Karam NA, Zkaria M, El Saadany HF, Abdel Rahman DM, et al. Impact of iron deficiency anemia on the function of the immune system in children. Medicine. (2016) 95:e5395. doi: 10.1097/MD.0000000000005395
14. Gombart AF, Pierre A, Maggini S. A review of micronutrients and the immune system–working in harmony to reduce the risk of infection. Nutrients. (2020) 12:236. doi: 10.3390/nu12010236
15. de Pontual L. Fer et prédisposition aux infections. Arch Pédiatr. (2017) 24:5S14–15S17. doi: 10.1016/S0929-693X(17)24004-4
16. Martins AC, Almeida JI, Lima IS, Kapitão AS, Gozzelino R. Iron metabolism and the inflammatory response. IUBMB Life. (2017) 69:442–50. doi: 10.1002/iub.1635
17. Pivina L, Semenova Y, Doşa MD, Dauletyarova M, Bjørklund G. Iron deficiency, cognitive functions, and neurobehavioral disorders in children. J Mol Neurosci. (2019) 68:1–10. doi: 10.1007/s12031-019-01276-1
18. Borges CVD, Veiga APB., Barroso GdS, Jesus EFOd, Serpa RFB, Moreira S, et al. Associação entre concentrações séricas de minerais, índices antropométricos e ocorrência de diarréia entre crianças de baixa renda da região metropolitana do Rio de Janeiro. Rev Nutr. (2007) 20:159–69. doi: 10.1590/S1415-52732007000200005
19. Labib AG, El-Bana SM, Ahmed SM, Abolwafa NF. The effect of chronic anemia on physical growth and development among children under five years. Minia Sc Nur J. (2018) 4:11. doi: 10.21608/msnj.2018.187744
20. Pedraza DF, Rocha ACD, Sales MC. Deficiência de micronutrientes e crescimento linear: revisão sistemática de estudos observacionais. Ciênc Saúde Coletiva. (2013) 18:3333–47. doi: 10.1590/S1413-81232013001100023
21. Zimmermann MB. The influence of iron status on iodine utilization and thyroid function. Annu Rev Nutr. (2006) 26:367–89. doi: 10.1146/annurev.nutr.26.061505.111236
22. Christian P. Prenatal micronutrient supplementation and intellectual and motor function in early school-aged children in Nepal. JAMA. (2010) 304:2716–23. doi: 10.1001/jama.2010.1861
23. Lozoff B. Iron deficiency and child development. Food Nutr Bull. (2007) 28:S560–571. doi: 10.1177/15648265070284S409
24. Pala E, Erguven M, Guven S, Erdogan M, Balta T. Psychomotor development in children with iron deficiency and iron-deficiency anemia. Food Nutr Bull. (2010) 31:431–5. doi: 10.1177/156482651003100305
25. Tam E, Keats EC, Rind F, Das JK, Bhutta ZA. Micronutrient supplementation and fortification interventions on health and development outcomes among children under-five in low- and middle-income countries: a systematic review and meta-analysis. Nutrients. (2020) 12:289. doi: 10.3390/nu12020289
26. Bortolini GA, Vitolo MR, Gubert MB, Santos LMP. Early cow's milk consumption among Brazilian children: results of a national survey. J Pediatr. (2013) 89:608–13. doi: 10.1016/j.jped.2013.04.003
27. Bortolini GA, Vitolo MR. Importância das práticas alimentares no primeiro ano de vida na prevenção da deficiência de ferro. Rev Nutr. (2010) 23:1051–62. doi: 10.1590/S1415-52732010000600011
28. Bezerra AGN, Leal VS, Lira, Oliveira JS, Costa EC, Menezes RCE, et al. Anemia and associated factors in women at reproductive age in a Brazilian Northeastern municipality. Rev Bras Epidemiol. (2018) 21:e180001. doi: 10.1590/1980-549720180001
29. Siqueira MCG, Bezerra LS, Freitas CZG, Buchalla SCC, Lenquiste SA. Associação do estado nutricional com marcadores de anemia ferropriva em pré-escolares atendidos em umaesf de presidente prudente-Sp. Colloq Vitae. (2019) 12:8–19. doi: 10.5747/cv.2020.v12.n1.v278
30. Gaitán CD, Olivares GM, Arredondo OM, Pizarro AF. Biodisponibilidad de hierro en humanos. Rev Chil Nutr. (2006) 33:142–8. doi: 10.4067/S0717-75182006000200003
31. Mantadakis E, Chatzimichael E, Zikidou P. Iron deficiency anemia in children residing in high and low-income countries: risk factors, prevention, diagnosis and therapy. Mediterr J Hematol Infect Dis. (2020) 12:e2020041. doi: 10.4084/mjhid.2020.041
32. Anater AS, Hampton JC., Lopes TdVC, Giuntini EB, Campos VC, Harnack LJ, et al. Nutrient intakes among Brazilian children need improvement and show differences by region and socioeconomic level Nutrients. (2022) 14:485. doi: 10.3390/nu14030485
33. Dodd KW, Guenther PM, Freedman LS, Subar AF, Kipnis V, Midthune D, et al. Statistical methods for estimating usual intake of nutrients and foods: a review of the theory. J Am Diet Assoc. (2006) 106:1640–50. doi: 10.1016/j.jada.2006.07.011
34. Welker EB, Jacquier EF, Catellier DJ, Anater AS, Story MT. Room for improvement remains in food consumption patterns of young children aged 2–4 years. J Nutr. (2018) 148(suppl_3):1536S−46S. doi: 10.1093/jn/nxx053
35. Neri MC. Covid, Classes Econômicas e o Caminho do Meio: Crônica da Crise até Agosto de 2020. (2020), p. 30. Available online at: http://www.fgv.br/cps/CovidClasses (accessed December 08, 2022).
36. Ferreira HS, Vieira RCS, Livramento ARS, Dourado BLLFS, Silva GFA, Calheiros MSC. Prevalence of anaemia in Brazilian children in different epidemiological scenarios: an updated meta-analysis. Public Health Nutr. (2020) 24:2171–84. doi: 10.1017/S1368980019005287
37. Jordão RE, Bernardi JLD, Filho AAB. Prevalence of iron-deficiency anemia in Brazil: a systematic review. Rev Paul Pediatr. (2009) 27:9. doi: 10.1590/S0103-05822009000100014
38. López MA, Martos FC. Iron availability: an updated review. Int J Food Sci Nutr. (2004) 55:597–606. doi: 10.1080/09637480500085820
39. Oliveira MA, Osorio MM. Cow's milk consumption and iron deficiency anemia in children. J Pediatr. (2005) 81:361–7. doi: 10.2223/JPED.1386
40. Gaitán D, Flores S, Saavedra P, Miranda C, Olivares M, Arredondo M, et al. Calcium does not inhibit the absorption of 5 milligrams of nonheme or heme iron at doses less than 800 milligrams in nonpregnant women. J Nutr. (2011) 141:1652–6. doi: 10.3945/jn.111.138651
41. IOM. Dietary Reference Intakes for Calcium, and Vitamin D. Washington, DC: Institute of Medicine (2011). Available online at: http://www.nap.edu/iom (accessed December 10, 2022).
42. Fisberg M, Duarte Batista L. Nutrition Related-Practices in Brazilian Preschoolers: Identifying Challenges and Addressing Barriers. Building Future Health and Well-Being of Thriving Toddlers and Young Children. Nestlé Nutrition Institute Workshop Series, 6th ed. London: S. Karger AG (2020), p. 1–10.
43. Almeida CA, Ricco RG, Del Ciampo LA, Dutra-de-Oliveira JE, Cantolini A. Control of iron-deficiency anaemia in Brazilian preschool children using iron-fortified orange juice. Nutr Res. (2003) 23:27–33. doi: 10.1016/S0271-5317(02)00487-6
44. Grillo LP, Klitzke CA. Campos ICd, Mezadri T. Nutritional risks of low family income students residents in the coast of Santa Catarina, Brazil. Texto Contexto Enferm. (2005) 14:17–23. doi: 10.1590/S0104-07072005000500002
45. Souza DPM, Alencar FH, Lopes TM, Araújo SF, Araújo JS, Freire JL, editors. Ocorrência de Anemia Ferropriva em Escolares Residentes na Área Urbana de Manaus-AM. i-zona oeste XX Jornada de Iniciação Científica PIBIC INPA - CNPq/FAPEAM. Manaus, AM (2011).
46. Farinhas de trigo e/ou milho fortificadas com ferro 344 (2002). Available online at: http://189.28.128.100/nutricao/docs/ferro/resolucao_rdc344_2002.pdf
47. Assunção MCF, Santos IS, Barros AJD, Gigante DP, Victora CG. Efeito da fortificação de farinhas com ferro sobre anemia em pré-escolares, Pelotas, RS. Rev Saúde Pública. (2007) 41:539–48. doi: 10.1590/S0034-89102006005000031
48. Moura NC, Canniatti-Brazaca SG. Evaluation of iron availabilty of the common bean in comparson with bovine meat. Ciênc Tecnol Aliment. (2006) 26:270–6. doi: 10.1590/S0101-20612006000200007
49. Ballot D, Baynes RD, Bothwell TH, Gillooly M, MacFarlane BJ, MacPhail AP, et al. The effects of fruit juices and fruits on the absorption of iron from a rice meal. Br J Nutr. (1987) 57:331–43. doi: 10.1079/BJN19870041
50. Almeida CA, Baptista MEC., Crott GC, Cantolini A, Ricco RG, Ciampo LAD, et al. Monte Alto sem anemia, primeira fase: avaliação nutricional das crianças pré-escolares Rev paul pediatr. (2002) 20:275–9.
51. da Silva Ferreira H, de Assunção Bezerra MK, Lopes de. Assunção M, Egito de Menezes RC. Prevalence of and factors associated with anemia in school children from Maceió, Northeastern Brazil. BMC Public Health. (2016) 16:380. doi: 10.1186/s12889-016-3073-2
52. Zijp IM, Korver O, Tijburg LB. Effect of tea and other dietary factors on iron absorption. Crit Rev Food Sci Nutr. (2000) 40:371–98. doi: 10.1080/10408690091189194
53. da Silva Lopes K, Yamaji N, Rahman MO, Suto M, Takemoto Y, Garcia-Casal MN, et al. Nutrition-specific interventions for preventing and controlling anaemia throughout the life cycle: an overview of systematic reviews. Cochrane Database Syst Rev. (2021) 9:Cd013092. doi: 10.1002/14651858.CD013092.pub2
54. Mak T-N, Angeles-Agdeppa I, Tassy M, Capanzana MV, Offord EA. The nutritional impact of milk beverages in reducing nutrient inadequacy among children aged one to five years in the Philippines: a dietary modelling study. Nutrients. (2020) 12:1130. doi: 10.3390/nu12113330
55. Allen L, de Benoist B, Dary O, Hurrell R. Guidelines on Food Fortification with Micronutrients. Nations FaAOotU, editor. Geneva: World Health Organization (2006), p. 341.
Keywords: anemia, iron deficiency, bioavailability, ascorbic acid, chelating agents, Brazil
Citation: Nogueira-de-Almeida CA, Prozorovscaia D, Mosquera EMB, Ued FdV and Campos VC (2023) Low bioavailability of dietary iron among Brazilian children: Study in a representative sample from the Northeast, Southeast, and South regions. Front. Public Health 11:1122363. doi: 10.3389/fpubh.2023.1122363
Received: 12 December 2022; Accepted: 02 February 2023;
Published: 20 February 2023.
Edited by:
Juliana Souza Oliveira, Federal University of Pernambuco, BrazilReviewed by:
Elpis Mantadakis, Democritus University of Thrace, GreeceFernanda Martins, Unilever, Brazil
Cristiane Simões De Souza, Universidade Federal de Goiás, Brazil
Copyright © 2023 Nogueira-de-Almeida, Prozorovscaia, Mosquera, Ued and Campos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Alberto Nogueira-de-Almeida,  ZHIubm9ndWVpcmFAbWUuY29t
ZHIubm9ndWVpcmFAbWUuY29t