 Andrea Duarte-Díaz1,2,3,4
Andrea Duarte-Díaz1,2,3,4 Lilisbeth Perestelo-Pérez3,4,5*
Lilisbeth Perestelo-Pérez3,4,5* Amado Rivero-Santana1,3,4
Amado Rivero-Santana1,3,4 Wenceslao Peñate2Yolanda Álvarez-Pérez1,3,4Vanesa Ramos-García1,3,4Himar González-Pacheco1,3,4Libertad Goya-Arteaga6Miriam de Bonis-Braun6Silvia González-Martín6Yolanda Ramallo-Fariña1,3,4
Wenceslao Peñate2Yolanda Álvarez-Pérez1,3,4Vanesa Ramos-García1,3,4Himar González-Pacheco1,3,4Libertad Goya-Arteaga6Miriam de Bonis-Braun6Silvia González-Martín6Yolanda Ramallo-Fariña1,3,4 Carme Carrion3,7Pedro Serrano-Aguilar3,4,5
Carme Carrion3,7Pedro Serrano-Aguilar3,4,5- 1Canary Islands Health Research Institute Foundation (FIISC), Tenerife, Spain
- 2Department of Clinical Psychology, Psychobiology and Methodology, Universidad de La Laguna, (ULL), Tenerife, Spain
- 3Network for Research on Chronicity, Primary Care, and Health Promotion (RICAPPS), Madrid, Spain
- 4The Spanish Network of Agencies for Health Technology Assessment and Services of the National Health System (RedETS), Madrid, Spain
- 5Evaluation Unit (SESCS), Canary Islands Health Service (SCS), Tenerife, Spain
- 6Multiprofessional Unit of Family and Community Care of La Laguna-Norte, Tenerife, Spain
- 7eHealth Lab Research Group, School of Health Sciences, Universitat Oberta de Catalunya (UOC), Barcelona, Spain
Introduction: The aim of this systematic review is to assess the relationship between patient empowerment and other empowerment-related constructs, and affective symptoms and quality of life in patients with type 2 diabetes.
Methods: A systematic review of the literature was conducted, according to the PRISMA guidelines. Studies addressing adult patients with type 2 diabetes and reporting the association between empowerment-related constructs and subjective measures of anxiety, depression and distress, as well as self-reported quality of life were included. The following electronic databases were consulted from inception to July 2022: Medline, Embase, PsycINFO, and Cochrane Library. The methodological quality of the included studies was analyzed using validated tools adapted to each study design. Meta-analyses of correlations were performed using an inverse variance restricted maximum likelihood random-effects.
Results: The initial search yielded 2463 references and seventy-one studies were finally included. We found a weak-to-moderate inverse association between patient empowerment-related constructs and both anxiety (r = −0.22) and depression (r = −0.29). Moreover, empowerment-related constructs were moderately negatively correlated with distress (r = −0.31) and moderately positively correlated with general quality of life (r = 0.32). Small associations between empowerment-related constructs and both mental (r = 0.23) and physical quality of life (r = 0.13) were also reported.
Discussion: This evidence is mostly from cross-sectional studies. High-quality prospective studies are needed not only to better understand the role of patient empowerment but to assess causal associations. The results of the study highlight the importance of patient empowerment and other empowerment-related constructs such as self-efficacy or perceived control in diabetes care. Thus, they should be considered in the design, development and implementation of effective interventions and policies aimed at improving psychosocial outcomes in patients with type 2 diabetes.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020192429, identifier CRD42020192429.
1. Introduction
Diabetes Mellitus (DM) is a major public health problem with a high and increasing frequency (1). According to the IDF Diabetes Atlas for 2021, an estimated 536.6 million individuals between the ages of 20 and 79 were diagnosed with diabetes, and this number is projected to rise to 783.2 million by 2045 (2). Type 2 Diabetes Mellitus (T2DM), accounts for 90–95% of all diagnosed cases of DM (3, 4). T2DM imposes a considerable burden on patients' health and health-related quality of life (HRQOL), as well as on socioeconomic issues (5, 6).
Although there is no cure for T2DM, it is possible to improve disease control to delay clinical complications and mortality by means of personalized and complex therapeutic strategies including lifestyle modification (7). Adherence to self-care behaviors is not easy but it is needed to achieve sustained long-term control and improve health outcomes. Both psychological and psychosocial problems have been identified as common barriers to self-care in patients with T2DM (8).
Research studies have reported a higher incidence of T2DM in individuals with major depression compared to the general population (9). Nearly one in four patients with T2DM suffer from comorbid depression (10). Besides, compared to the general population, a higher incidence and prevalence of anxiety disorders have also been reported among people with T2DM (11, 12). According to a recent meta-analysis on the prevalence of T2DM in mental disorders, 14% of individuals with anxiety disorder and 9% of individuals with depression have been diagnosed with T2DM (13). It is reported that patients with T2DM and comorbid mental health problems are more likely to have diabetes complications (14) and are less likely to meet the guidelines for a healthy lifestyle and self-care recommendations (15–17), with greater difficulties in achieving and maintaining diabetes control. It has recently been pointed out that T2DM patients with comorbid anxiety or depressive disorders have a higher likelihood of visiting the emergency room when compared to diabetic patients without mental health problems (18). Furthermore, the risk of 4-year-all-cause mortality is 14% higher in those T2DM patients with comorbid depression (18). Depression and chronic psychological stress can trigger the activation of the hypothalamic-pituitary-adrenal axis, which in turn stimulates the sympathetic nervous system, increases platelet aggregation response, and inflammation while reducing insulin sensitivity (19, 20). These physiological changes may contribute to poor glycemic control and an increased risk of diabetes-related complications such as retinopathy, enteropathy, dermatopathy, diabetic foot, and neuropathy (21).
Understanding mental health issues in patients with T2DM has become a major concern. The American Diabetes Association highlight the need to integrate psychosocial care with person-centered medical care for people with diabetes to optimize health outcomes and promote HRQOL (22). Person-centered care (PCC) has a holistic view of patient care, focusing on the need of seeing people beyond the illness, valuing their needs and respecting their rights and dignity. One of the core elements of PCC is patient empowerment, defined as a process through which people can gain control over decisions and actions affecting their health (23). From this point of view, the aim of patient empowerment is to provide them with critical thinking, skills and tools to take responsibility for their health and wellbeing, develop autonomy and make informed autonomous decisions.
Despite the growing interest in PCC and the encouragement of patients to be actively involved in their care, defining and measuring empowerment is still challenging. Firstly, it has not only been conceptualized as a process but also as an outcome. It can be considered as the process through which patients gain control over their healthcare and it can be achieved through patient-centeredness. Accordingly, patient empowerment has been defined as a meta-paradigm that connects patient participation and patient-centeredness (24). From this point of view, patient participation may be considered a condition to achieve PCC, which in turn can promote patient empowerment (24). Moreover, it can also be considered as an outcome since patients are empowered when they have the necessary knowledge and skills to influence their own behavior to improve their quality of life (QoL) (25). Secondly, most definitions of patient empowerment include references to other theoretically-related constructs such as self-efficacy, patient activation or perceived control (26–28). Even when there have been attempts to clarify the boundaries between empowerment and these concepts, it may be difficult to fully differentiate one from the other (26). Bravo et al. (29) proposed a novel conceptual map of patient empowerment in 2015. According to the authors, patient empowerment can be conceived as a state ranging across a spectrum from low to high levels and depends on patient, provider and healthcare system factors. In addition, they suggested that this level of patient empowerment can be potentially measurable using a set of related constructs as indicators, including those referring to patients' capacities (e.g., self-efficacy, perceived control) and behaviors (e.g., patient activation) (29). Empowerment is an umbrella term, but the core of this concept is the idea of supporting patients to become more responsible for their own health (30). Patient empowerment is thus a more wide-ranging and multidimensional concept (31), but there's no universally accepted instrument that can be used to measure it (32).
Promoting the participation of people in their own healthcare is considered an ethical imperative included in the Declaration of Salzburg (33). Previous studies have shown that patients with Type 2 Diabetes Mellitus (T2DM) who report higher levels of patient empowerment tend to experience fewer affective symptoms (34, 35). Furthermore, in a secondary analysis of a randomized controlled trial it was found that an increase in patient empowerment is associated with improvements in both anxiety and depressive symptoms (36). This finding is particularly significant considering that affective and emotional disorders in T2DM have been associated with non-adherence to diet, physical activity and medication (16, 37, 38). Existing evidence suggests that empowering patients may not only improve affective symptoms but also enhance QoL (39, 40). Two systematic reviews (SR) have shown that empowerment-based strategies may improve clinical, behavioral and psychological outcomes in patients with T2DM (41, 42). Baldoni et al. (41) reported that programs based on collective empowerment strategies lead to an increase in confidence and DM knowledge, better attitudes toward the disease and more healthy eating patterns. Likewise, Aquino et al. (42) concluded that individual empowerment-based strategies have several psychosocial benefits such as more self-care behaviors, increased motivation, self-efficacy as well as DM knowledge and better QoL.
Even though previous SR have highlighted the effectiveness of empowerment-based interventions, to the best of our knowledge no previous reviews have synthesized data on the association between the level of patient empowerment or empowerment-related constructs and affective outcomes and QoL in patients with T2DM. This SR and meta-analysis (MA) address this gap and provide additional and relevant information on the relationship between patient empowerment itself and affective symptoms and QoL while also highlighting the importance of other empowerment-related constructs.
2. Methods
2.1. The protocol and registration
The results of this SR and MA were reported based on the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) 2020 statement (43) (Supplementary material 1). This SR was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the registration number CRD42020192429.
2.2. Eligibility criteria
2.2.1. Participants
Studies addressing patients with T2DM, aged 18 years or older were included. Studies involving children or adolescents, patients with type 1 DM, gestational DM or participants with pre-diabetes were excluded.
2.2.2. Outcomes
Studies analyzing the association between patient empowerment or empowerment-related constructs and both affective symptoms (i.e., anxiety, depression and distress) and QoL were included. Given the lack of consensus on the definition of patient empowerment, and in order to be exhaustive, this review included not only studies assessing patient empowerment itself, but also other empowerment-related constructs that might be potential indicators, such as self-efficacy, patient activation and perceived control. Outcomes related to self- or clinician-rated symptoms of anxiety, depression and distress, as well as self-reported QoL, using validated instruments, were included. Figure 1 shows the anticipated theoretical relationships among the variables evaluated in the present review.
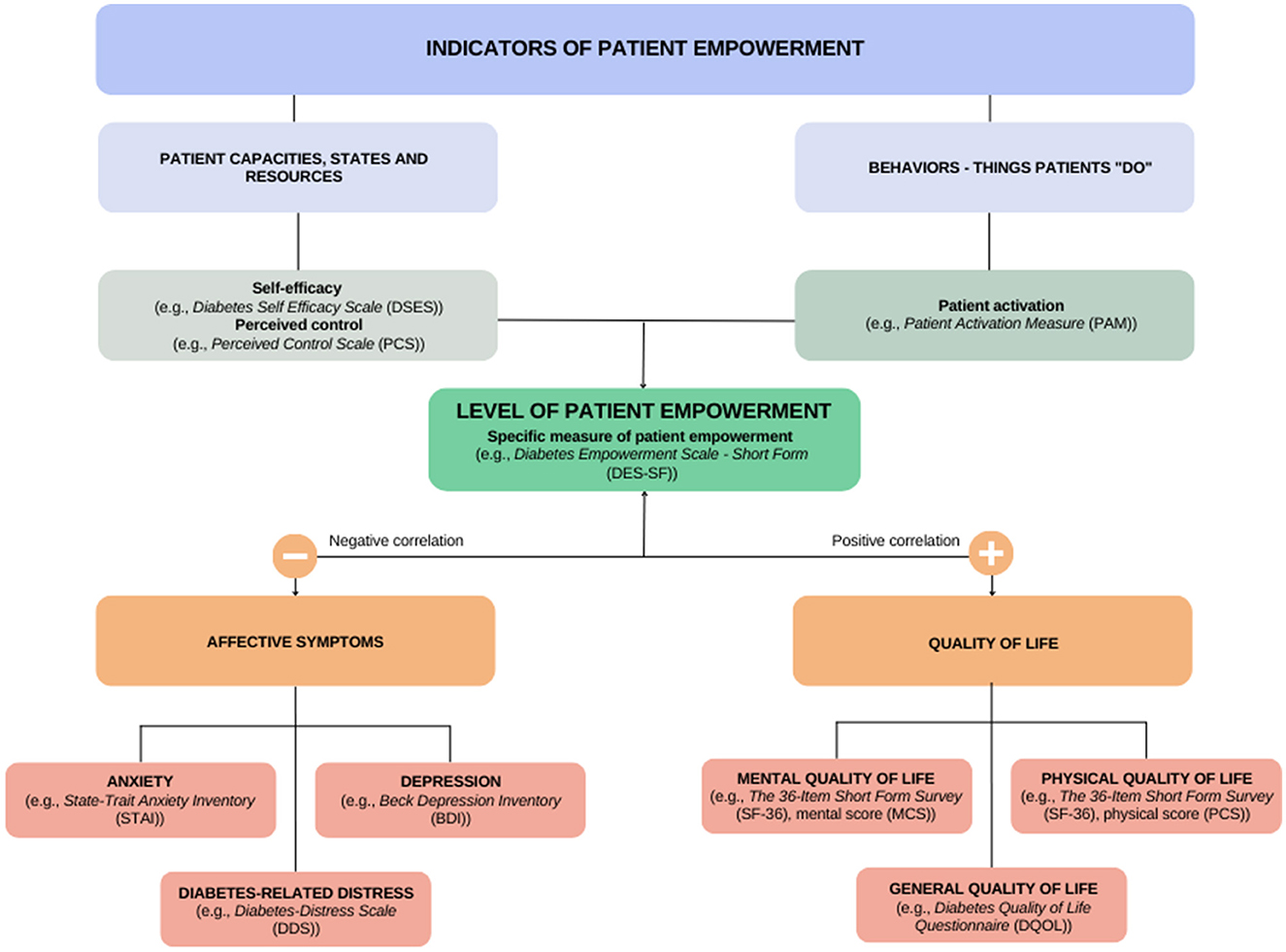
Figure 1. Diagram of patient empowerment and related-constructs in relation to affective symptoms and quality of life. Adapted with permission from Bravo et al. (29), licensed under CC BY 4.0.
2.2.3. Study design
Since terms of associations can be reported in various study designs, we included all study designs in the eligibility criteria. Clinical trials, pre-post intervention studies or observational studies addressing the association of patient empowerment or empowerment-related constructs on affective outcomes (i.e., anxiety, depression or distress) and QoL were subsequently included. Clinical trials not including a specific measure of patient empowerment, self-efficacy, patient activation or perceived control were excluded, even if the intervention was based on PCC principles. In anticipation of not finding much longitudinal evidence, cross-sectional studies were also considered to test the hypothesis of no association between the study variables. Conference abstracts, letters, commentaries, essays, book chapters, qualitative studies, protocols and reviews were also excluded.
2.3. Study selection and data extraction
The following electronic databases were consulted from inception to July 2022: Medline, Embase, PsycINFO and Cochrane Library. To ensure comprehensiveness, the search strategy included keywords related to patient empowerment as well as other related constructs that could serve as potential indicators of the level of patient empowerment. The following terms were used individually and combined according to the Medical Subject Heading (MeSH) terms: “diabetes,” “anxiety,” “depression,” “quality of life,” “empowerment,” “self-efficacy” and “patient activation” (Supplementary material 2). No language or publication year restrictions were applied to limit the search. Monthly Medline searches were conducted until the study submission. Additionally, the list of references of all eligible articles were screened and manual searches in Google Scholar were undertaken.
2.4. Study selection and data extraction
All citations extracted from the different electronic databases were imported into a standardized Microsoft Excel data sheet and duplicates were removed. Firstly, two members of the research team independently reviewed all titles and abstracts in order to pre-select those meeting the inclusion criteria. Secondly, the full-text of the potentially relevant studies was screened for eligibility by two reviewers. Any disagreement was solved by discussion and consensus and a third reviewer was consulted if needed. From each included study, two reviewers independently extracted data on the following variables according to a standardized data extraction form in Microsoft Excel: first author, year of publication, country, number of participants, mean age, study design, study population, outcomes, effect estimates for the main outcomes and main results.
2.5. Risk of bias assessment
The Joanna Briggs Institute critical appraisal checklist was used (112) was used to evaluate the quality of cross-sectional studies. Version 2 of the Cochrane risk-of-bias tool for randomized trials (113) was used to assess the risk of bias in randomized trials. The methodological quality of cohort and pre-post studies was assessed using the National Institute of Health quality assessment tools (114). Quality assessment was undertaken by two independent reviewers and disagreements were solved by discussion and consensus or after consulting a third reviewer.
2.6. Statistical analyses
Meta-analyses were performed using the transformation of r values into Fisher's z scores and then reconverting them to r values. The associations were classified as weak (r = 0.10 to 0.29), moderate (r = 0.30 to 0.49) or strong (≥50) (115). When effect sizes different to Pearson's correlation were reported, each was converted using the following formulas:
(1) Spearman's correlation to Pearson's correlation (116):
(2) Regression coefficient from multiple linear regression to Pearson's correlation (117):
(3) χ2 to Pearson's correlation (118):
Where n denotes sample size, λ = 1 if β is positive and λ = 0 if β is negative.
When multiple correlation coefficients were reported in a particular study (i.e., the association between different empowerment subscales and general QoL), an average effect size was calculated in order to preserve statistical independence between samples. Heterogeneity was calculated by means of the Cochran's Q test and quantified by Higgins I2 statistics (119). Correlation coefficients were pooled using an inverse variance restricted maximum likelihood random-effects MA (120), with 95% as confidence interval (95%CI) and visually displayed through forest-plots. The authors conducted subgroup analyses for categorical variables and bivariate meta-regression for continuous variables in addition to using random-effects models when significant heterogeneity was present. Additionally, a 'leave-one-out' sensitivity analysis was performed to evaluate the influence of potential outliers on the pooled effect estimate and to explore other sources of heterogeneity. The available data allowed the analysis of the influence of three moderating variables pre-specified in the study protocol: type of empowerment-related construct, mean age and Hba1c. Other subgroups and potential moderators were subsequently defined post-hoc: type of study (cross-sectional vs longitudinal), type of distress measure (diabetes-related distress vs. general distress), gender (defined as % of females) and years since diagnosis. Subgroup analyses were performed if at least two studies for each subgroup of interest were available. When at least ten correlation coefficients were included, the publication bias was evaluated using the Egger test (121) and the trim-and-fill method (122) was used to correct for possible funnel plot asymmetry. All the analyses were performed in Stata v17 (123) using the meta package (124).
3. Results
The initial search in the electronic databases yielded 2,463 references. After removing duplicates, 1557 records were screened by title and abstract and 191 full-text articles were assessed for eligibility. Five additional records were identified through manual searches (50, 80) and citation list (62, 104, 110). Seventy-one studies were finally included: sixty-one cross-sectional studies (34, 35, 44, 45, 47–69, 71–78, 80, 83–88, 91–97, 99–102, 104–111), five observational prospective studies (36, 70, 81, 82, 89), four randomized controlled trials (RCTs) (79, 90, 98, 103) and one pre-post intervention study (46). Figure 2 shows the flowchart of the selection process of the studies'.
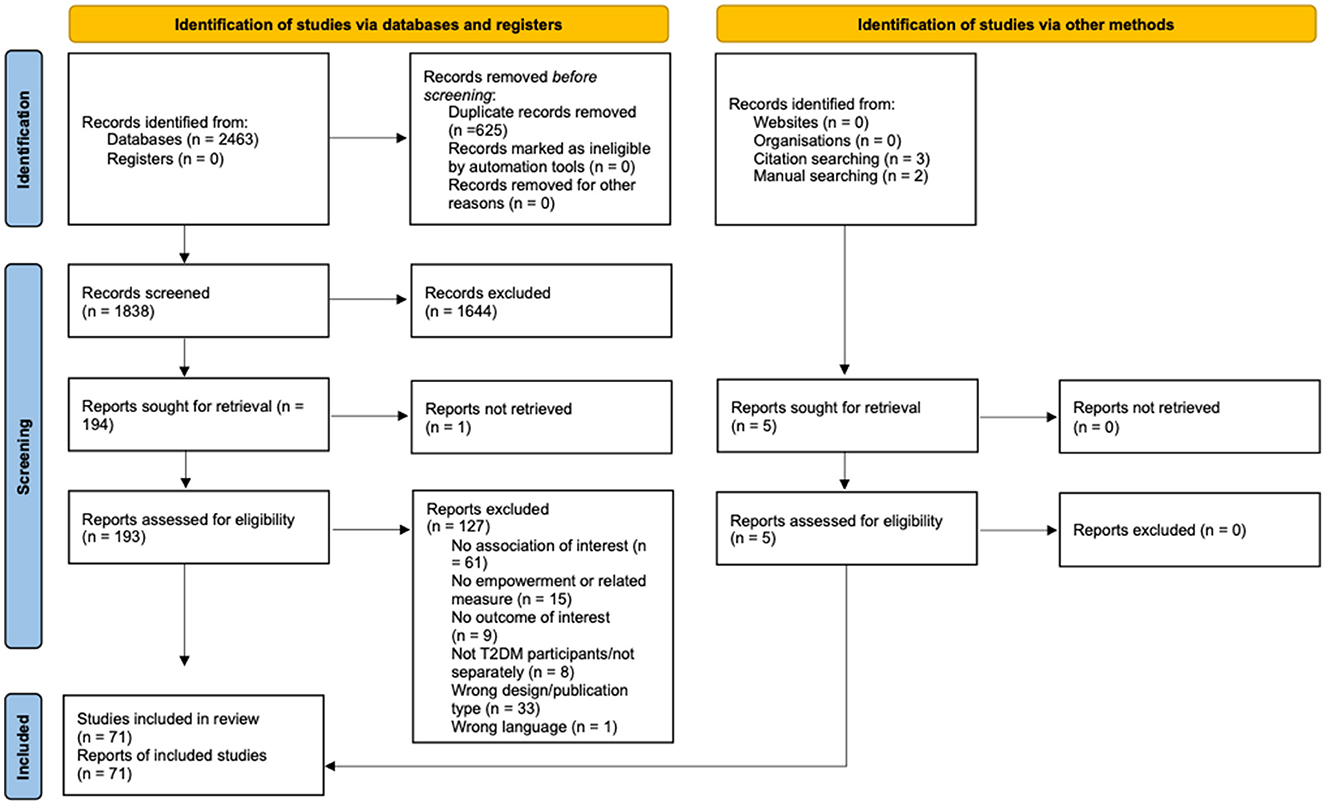
Figure 2. PRISMA flow-chart of the study selection process.
3.1. Characteristics of the included studies
The total sample was made up of 20,825 participants, mean age ranging from 46 to nearly 74 years of age and 57% were females. Thirty-two studies were carried out in Asia, twenty-three in North America, thirteen in Europe, two in Africa and the remaining two in South-America. Table 1 shows the studies' characteristics.
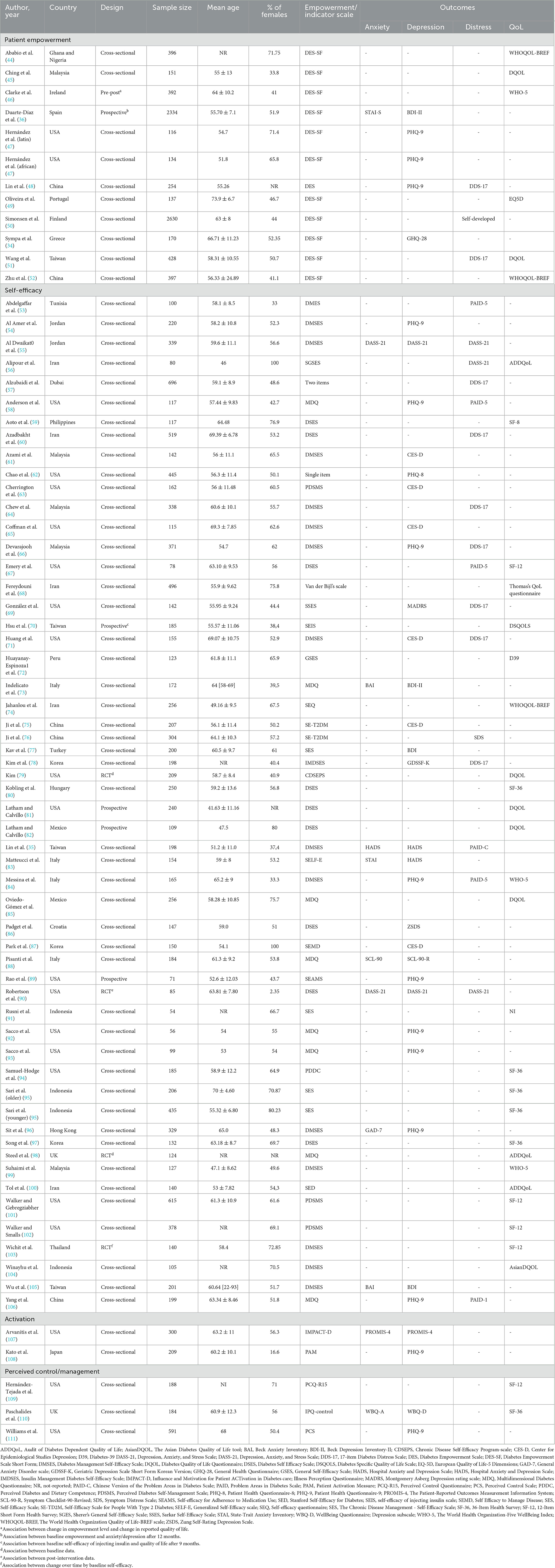
Table 1. Main characteristics of the included studies.
Eleven studies (n = 11) (34, 36, 44–52) specifically assessed patient empowerment using both long and short forms of the Diabetes Empowerment Scale. Moreover, the majority of the studies did not specifically investigate patient empowerment, but instead examined related constructs that may serve as indicators of the level of patient: self-efficacy (n = 54) (35, 53–75, 77–102), patient activation (n = 2) (107, 108) and perceived control (n = 3) (109–111). Overall, the quality of the studies included in the analyses ranged from low to moderate. Most cross-sectional studies clearly defined inclusion and exclusion criteria and all described subjects in detail. The main source of bias in these studies was the unclear identification of confounding factors. In prospective studies, the research question and objectives were clearly stated. However, none of them assessed the independent variable more than once over time. The overall bias in RCTs was high in two studies (79, 98) and unclear in another two (90, 103). The only pre-post study failed to clearly report information on different items and it was thus rated as being of poor quality (46). The full quality assessment can be found in Supplementary material 3.
3.2. The association between empowerment-related constructs and anxiety
Eleven studies (35, 36, 55, 73, 83, 88, 90, 96, 105, 107, 110) (n = 4,480) assessed the relation between three empowerment-related constructs and anxious symptoms. Eight studies used self-efficacy scales (35, 55, 73, 83, 88, 90, 96, 105) and three used empowerment (36), activation (107) and perceived control (110) measures, respectively. One study, not included in the MA due to the lack of numerical data (83), reported a negative association between self-efficacy and anxiety in their subsample of patients with T2DM.
The MA of the remaining ten studies (n = 4,326) (35, 36, 55, 73, 88, 90, 96, 105, 107, 110) showed a weak inverse correlation between patient empowerment and its indicators and anxious symptomatology (r = −0.22; 95%CI −0.28 to −0.15; I2 = 74.47%; k = 10) (Figure 3).
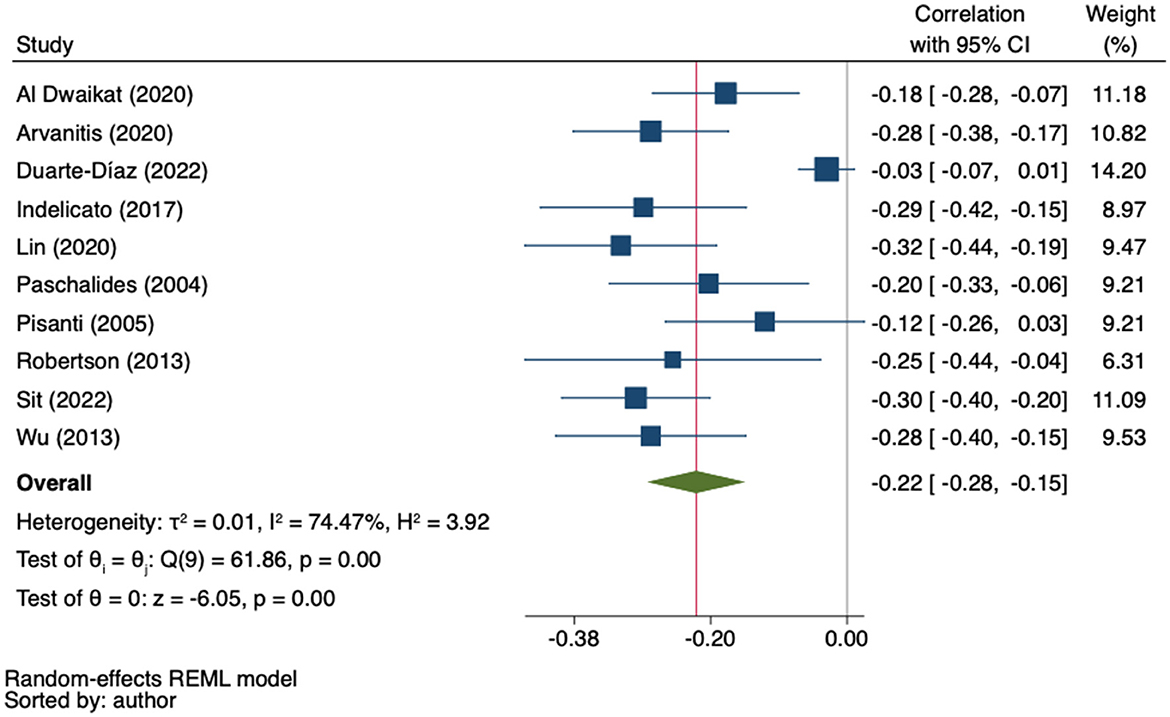
Figure 3. Random-effects meta-analysis on the association between empowerment and anxiety.
Sensitivity analysis using the leave-one-out approach identified one outlier study (36). When it was excluded, the heterogeneity decreased to 14.33% (Q = 8.72, p = 0.366) and the effect increased to −0.25 (95% CI from −0.29 to −0.20) (Supplementary material 4A). In the univariate meta-regression analyses, nor age (β = 0.00; 95%CI −0.01 to 0.01; k = 9); gender (β = 0.00; 95%CI −0.00 to 0.01; k = 9); HbA1C level (β = 0.08; 95%CI −0.01 to 0.16; k = 6) nor years since diagnosis (β = 0.02; 95%CI −0.01 to 0.05; k = 7) obtained significant results. The regression-based Egger's test showed evidence of small-study effects (p = 0.02) and the funnel-plot analysis was asymmetrical, indicating publication bias. Trim-and-fill analysis by the imputation of two studies on the right side resulted in a lower, but still statistically significant correlation coefficient (r = −0.20, 95%CI −0.26 to −0.13) (Figure 4).
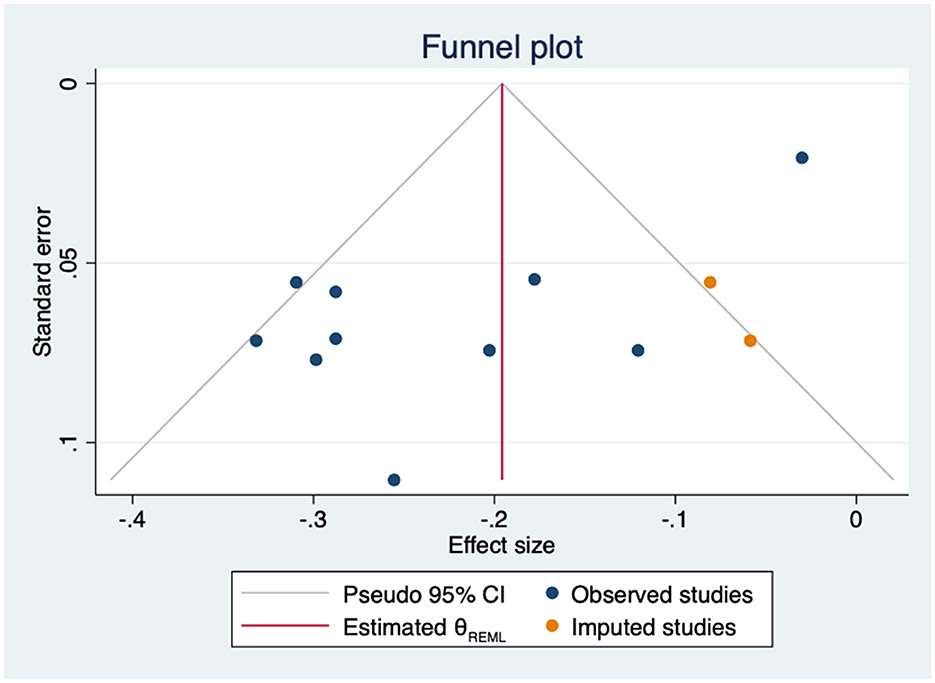
Figure 4. Funnel plot with trim-and-fill imputations for the association between empowerment and anxiety.
3.3. The association between empowerment-related constructs and depression
The relationship between empowerment-related constructs and depressive symptoms was reported in thirty-five studies (n = 9315) (34–36, 47, 48, 54, 55, 58, 61–63, 65, 66, 69, 71, 73, 75, 77, 78, 83, 84, 86–90, 92, 93, 96, 105–108, 110, 111). The most frequently used empowerment construct was self-efficacy (n = 27) (35, 54, 55, 58, 61–63, 65, 66, 69, 71, 73, 75, 77, 78, 80, 83, 84, 86–90, 92, 93, 96, 105, 106), followed by patient empowerment itself (n = 4) (34, 36, 47, 48), perceived control (n = 2) (110, 111) and patient activation (n = 2) (107, 108). Two studies were not included in the quantitative analysis due the lack of numerical data (65, 83) and Sacco et al. (92) was also excluded because its sample overlapped with Sacco et al. (93). Matteucci et al. (83) found a negative association between self-efficacy and depression, whereas in the study of Coffman et al. (65) the association between diabetes self-efficacy and depression was not significant.
Through a MA including thirty correlation coefficients from twenty-nine original studies (n = 8,990) (34–36, 47, 48, 54, 55, 58, 61–63, 66, 69, 71, 73, 75, 77, 78, 80, 84, 86–90, 93, 96, 105–108, 110, 111), a weak-to-moderate inverse correlation was found (r = −0.29; 95%CI −0.33 to −0.24; I2 = 78.08%; k = 32) (Figure 5).
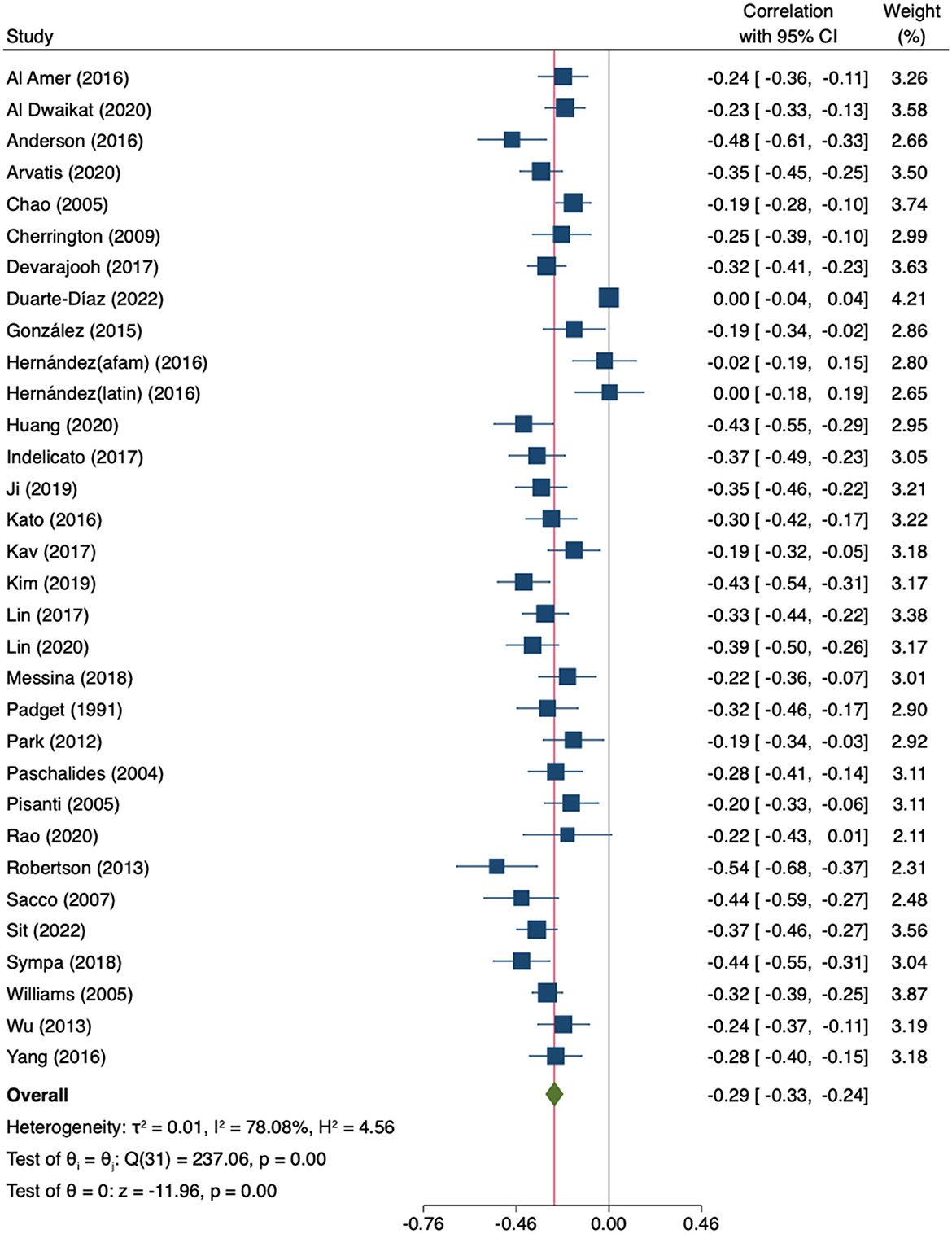
Figure 5. Random-effects meta-analysis on the association between empowerment and depression.
The leave-one-out MA showed that neither the direction nor significance of the pooled effect changed after the removal of any individual study (Supplementary material 4B). The estimates ranged from −0.28 to −0.30. There was significant heterogeneity across studies (Q = 237.06; p < 0.000). The subgroup analysis by empowerment-related construct showed no significant differences (p = 0.455), not even when comparing specific empowerment measures against the other combined empowerment-related constructs (p = 0.143) (Supplementary material 5A). However, in in the subgroup of studies using patient empowerment scales, heterogeneity was high and the association with depressive symptoms was not statistically significant. In the univariate meta-regression analyses, both age and female gender significantly moderated the association between patient empowerment-related constructs and depression (age: β = −0.01; 95%CI −0.02 to −0.00; k = 31; gender: β = 0.00; 95%CI 0.00 to 0.01; k = 31). Age accounted for 17% of heterogeneity and gender for 18%. In the multivariate analysis, only gender remained significant (β = 0.00; 95%CI 0.00 to 0.01; k = 30). Neither HbA1c levels (β = −0.07; 95%CI −0.17 to 0.03; k = 17) nor years since diagnosis (β = −0.00; 95%CI −0.03 to 0.02; k = 22) were found to be significant moderators. The regression-based Egger's test was not significant (p = 0.08), however Duval and Tweedie's trim-and-fill analysis suggested that four studies were missing on the right side of the mean effect (Figure 6). The imputation of these four studies did not substantially change the result (r = −0.27; 95%CI −0.32 to −0.22, k = 36).
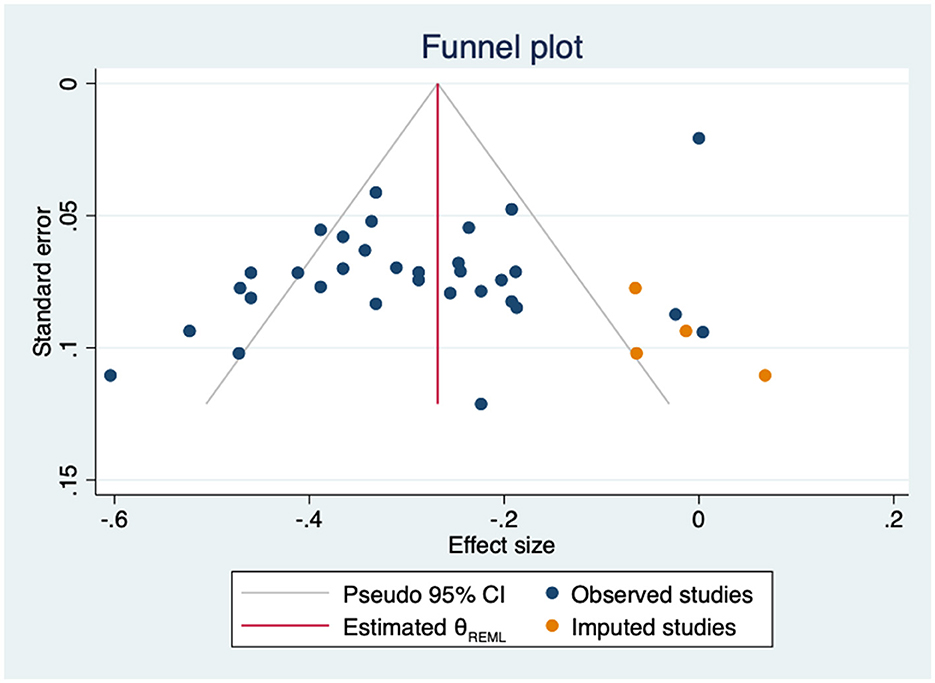
Figure 6. Funnel plot with trim-and-fill imputations for the association between empowerment and depression.
3.4. The association between empowerment-related constructs and distress
Twenty studies (n = 7,396) (35, 48, 50, 51, 53, 55–58, 60, 64, 66, 67, 69, 71, 76, 78, 84, 90, 106) reported the association between empowerment-related constructs and general or diabetes-related distress. Most of the studies used self-efficacy scales (n = 17) (35, 53, 55–58, 60, 64, 66, 67, 69, 71, 76, 78, 84, 90, 106) whereas a specific scale addressing diabetes patient empowerment was used in three studies (48, 50, 51). One study, not included in the MA due to the lack of numerical data (57), reported that distress levels were significantly lower among those T2DM patients who reported higher self-efficacy.
The MA of the remaining nineteen studies (n = 6,700) showed a moderate inverse correlation between empowerment-related constructs and distress (r = −0.31; 95%CI −0.38 to −0.25; I2 = 86%; k = 19) (Figure 7).
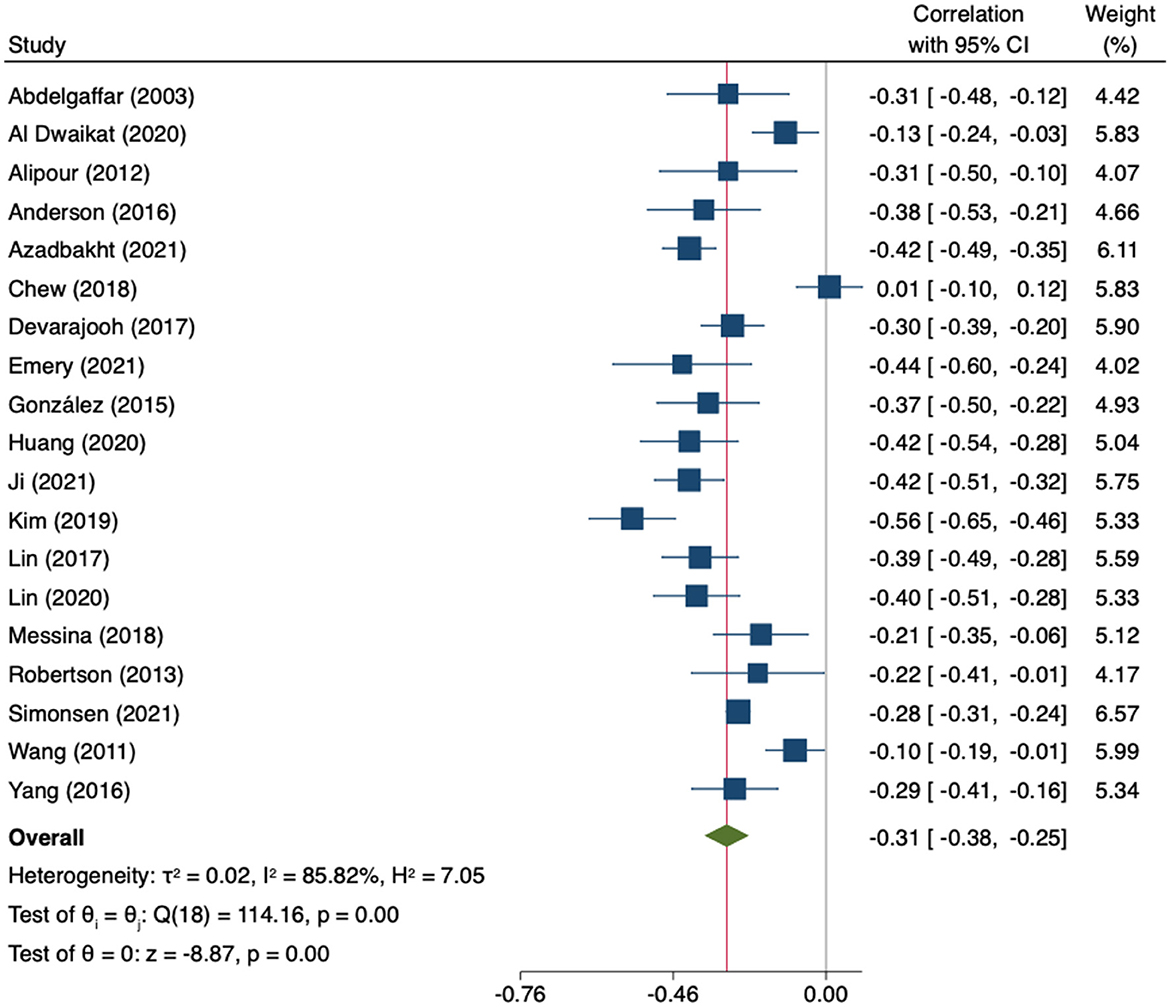
Figure 7. Random-effects meta-analysis on the association between empowerment and distress.
The leave-one-out analysis showed no relevant influence of any individual study. The estimates ranged from −0.30 to −0.33 (Supplementary material 4C). Heterogeneity was high and statistically significant (Q = 114.16, p = 0.000). In the subgroup analysis by type of empowerment construct, no statistically significant differences were found (p = 0.439). The correlation was stronger in studies using specific diabetes-related distress measures than in studies using general ones (p = 0.03) (Supplementary material 5B). Likewise, none of the sociodemographic or clinical variables significantly modified the association between empowerment-related constructs and distress (age: β = 0.01; 95%CI −0.01 to 0.01; k = 18; gender: β = 0.00; 95%CI −0.00 to 0.00; k = 18; HbA1c: β = 0.09; 95%CI −0.11 to 0.25; k = 8; and years since diagnosis: β = −0.02; 95%CI −0.05 to 0.01; k = 14). No evidence of small-study effects was identified by the Egger test (p = 0.348). Nevertheless, the imputation of three coefficients in the right side of the plot (Figure 8) slightly decreased the association (r = −0.29, 95%CI −0.37 to −0.22, k = 22).
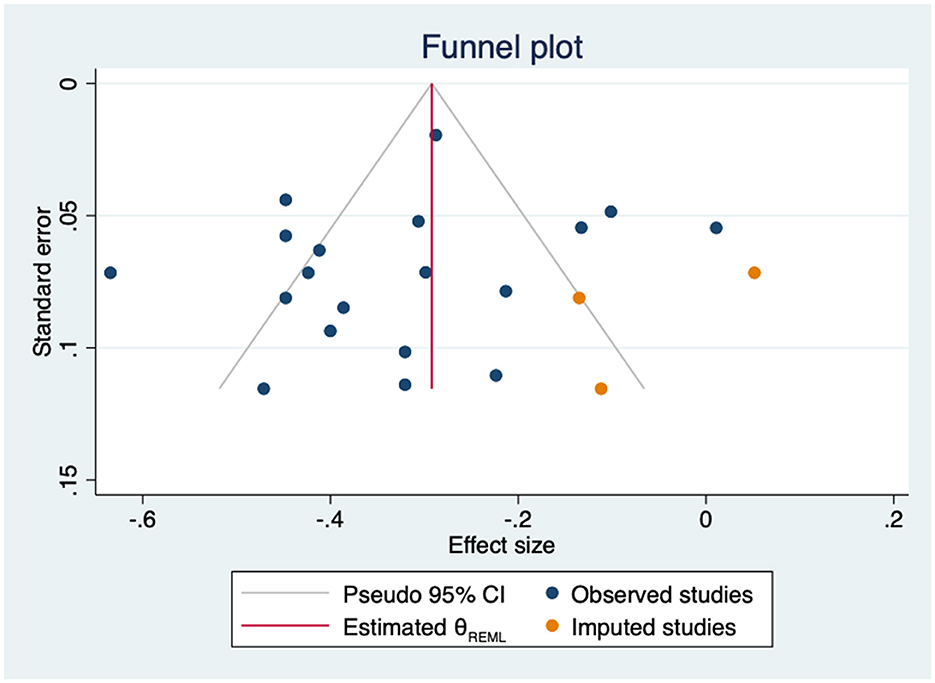
Figure 8. Funnel plot with trim-and-fill imputations for the association between empowerment and distress.
3.5. The association between empowerment-related constructs and quality of life
3.5.1. General quality of life
Twenty-two studies (n = 5,005) (44–46, 49, 51, 52, 56, 68, 70, 72, 74, 79, 81, 82, 84, 85, 91, 95, 98–100, 104) evaluated the relationship between empowerment-related constructs and general QoL in patients with T2DM. Specific patient empowerment scales were used in six studies (44–46, 49, 51, 52) while self-efficacy was used in the remaining sixteen studies (56, 68, 70, 72, 74, 79, 81, 82, 84, 85, 91, 95, 98–100, 104). One study (44) used ANOVA to quantify this association and was not included in the MA. The aim of this study was to identify predictors of good QoL among diabetic patients in Ghana and Nigeria, reporting that patient empowerment only significantly predicted QoL in Nigeria.
Twenty-two correlation coefficients from twenty-one studies (n = 4,609) were pooled. A moderate positive correlation was found but heterogeneity across studies was high (r = 0.32; 95%CI 0.25–0.38; I2 = 82.46%, k = 22) (Figure 9).
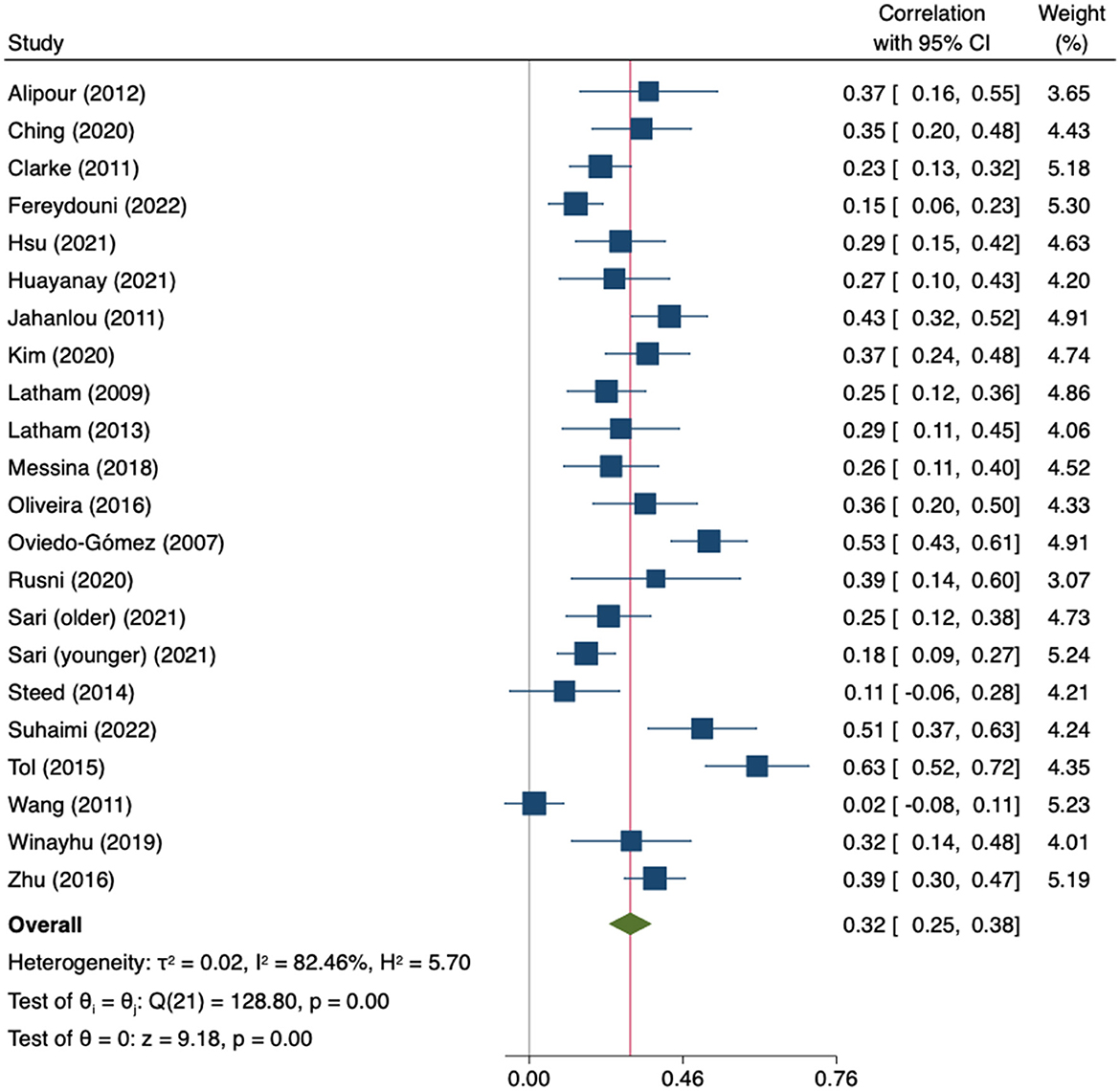
Figure 9. Random-effects meta-analysis on the association between empowerment and general QoL.
The leave-one-out sensitivity analysis did not identify any study whose exclusion substantially modified the result. The estimates ranged from 0.30 to 0.33 (Supplementary material 4D). Heterogeneity across studies was high and statistically significant (Q = 128.80, p = 0.000). The subgroup analyses by construct (empowerment vs. self-efficacy) and by type of study (cross-sectional vs. longitudinal) did not find statistically significant differences (Supplementary material 5C). Other sources of heterogeneity were analyzed through meta-regression, but neither age (β = −0.00; 95%CI −0.01 to 0.01; k = 19), gender (β = 0.00; 95%CI −0.00 to 0.00; k = 20), HbA1c (β = 0.04; 95%CI −0.17 to 0.24; k = 6), nor years since diagnosis (β = −0.02; 95%CI −0.06 to 0.02; k = 11) found significant results. The Egger tests showed no evidence of small-study effects (p = 0.121) and the trim-and-fill model suggested that no imputation or adjustment was needed (Figure 10).
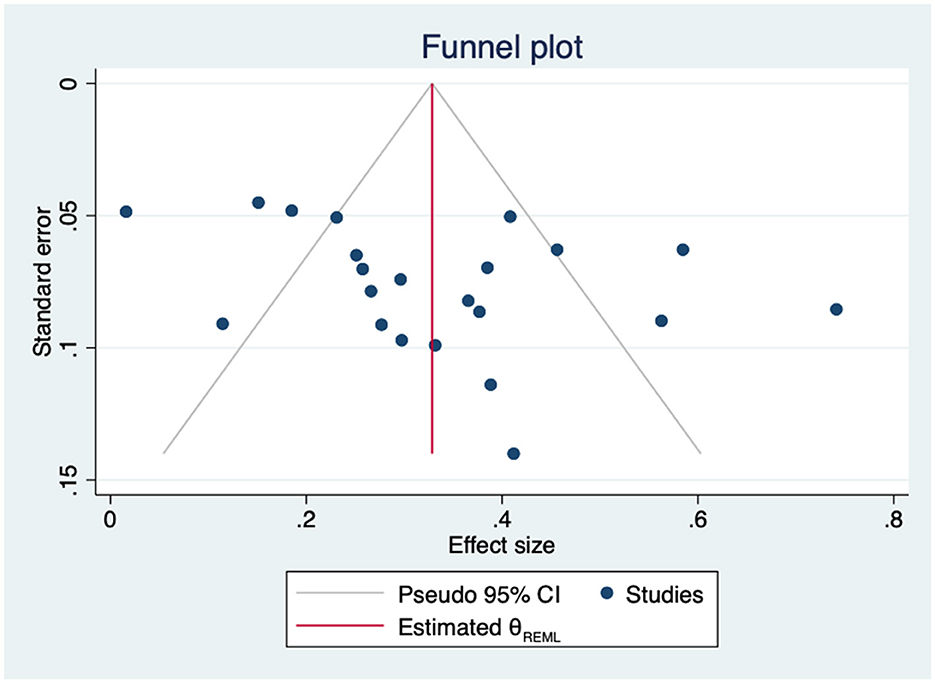
Figure 10. Funnel plot for the association between empowerment and general QoL.
3.5.2. Mental quality of life
Eight studies (n = 2,267) reported data on the association between self-efficacy and the mental component of QoL (59, 67, 80, 94, 97, 101–103) and two did so with perceived control (109, 110). The MA of these ten studies showed a significant positive correlation (r = 0.23; 95%CI 0.10 to 0.35; I2 = 90%; k = 10) (Figure 11).
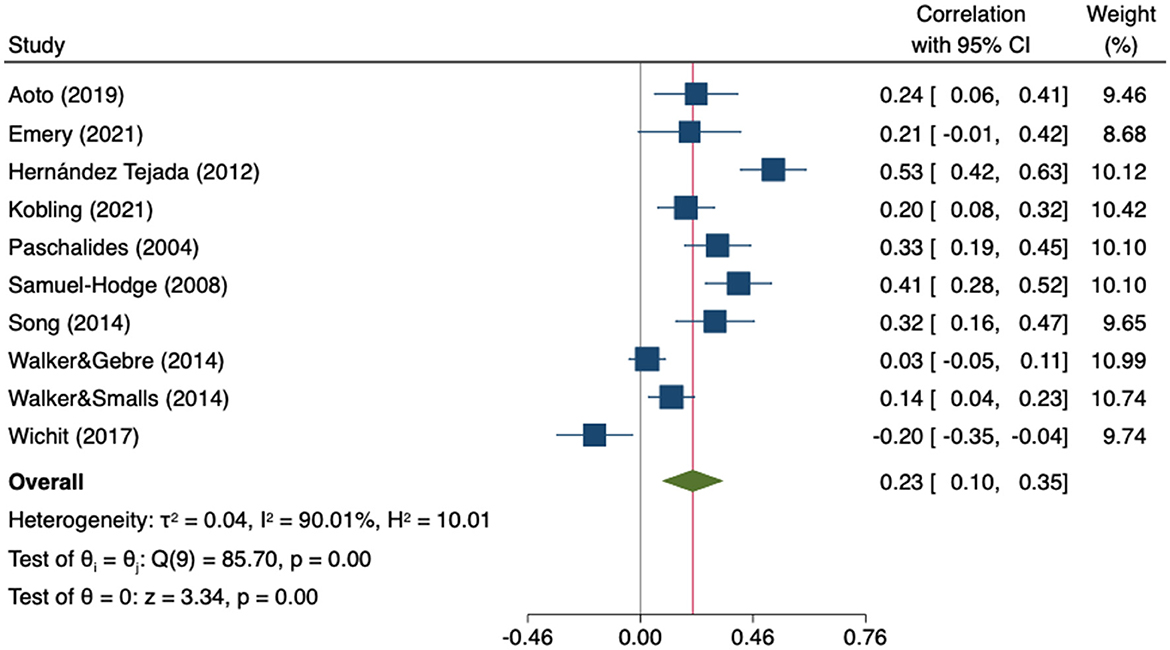
Figure 11. Random-effects meta-analysis on the association between empowerment and mental QoL.
The sensitivity analysis showed that neither the direction nor significance of the pooled effect changed after removing any individual study. The estimates ranged from 0.19 to 0.27 (Supplementary material 4E). Heterogeneity was high and statistically significant (Q = 85.70, p = 0.000). Subgroup analysis revealed that the correlation coefficient in studies using perceived control scales was significantly higher than in those using self-efficacy scales (p = 0.037) (Supplementary material 5D). The moderator analyses through meta-regression showed no statistical effect of age (β = 0.03; 95%CI −0.04 to 0.10; k = 8), gender (β = −0.00; 95%CI −0.02 to 0.02; k = 10), HbA1c (β = 0.21; 95%CI −0.04 to 0.46; k = 7) or years since diagnosis (β = 0.05; 95%CI −0.02 to 0.11; k = 6). The Egger tests showed no evidence of small-study effects (p = 0.675), however, Duval and Tweedie's trim-and-fill analysis suggested that three studies were missing on the left side of the mean effect (Figure 12). When these three studies were imputed, the association was no longer statistically significant (r = 0.13; 95%CI −0.01 to 0.28, k = 13).
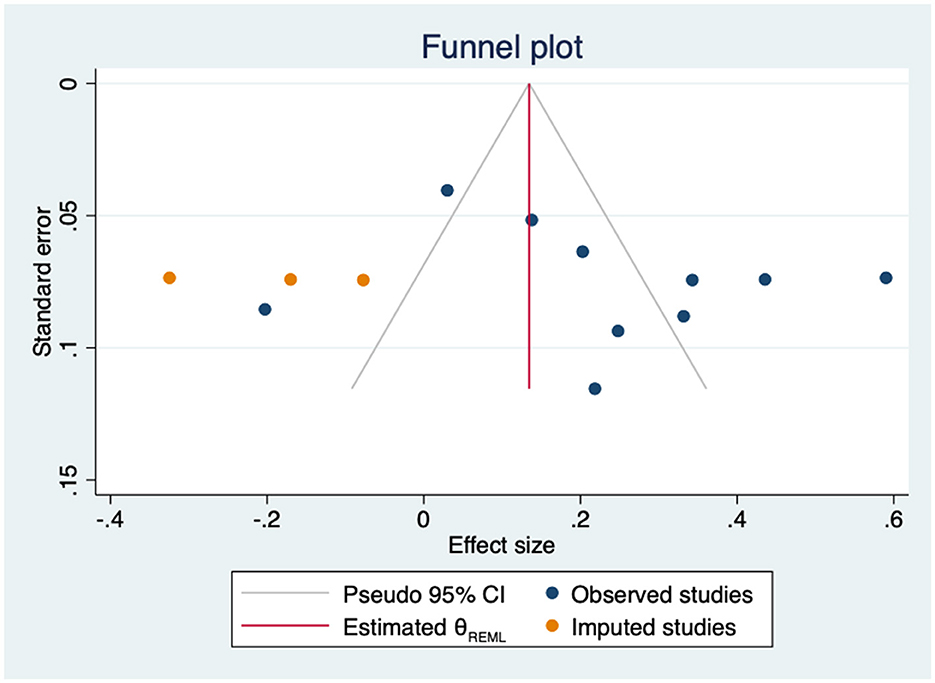
Figure 12. Funnel plot with trim-and-fill imputations for the association between empowerment and mental QoL.
3.5.3. Physical quality of life
Seven studies (n = 2,082) reported data on the association between self-efficacy and the physical component of QoL (59, 67, 80, 97, 101–103) and two did so with perceived control (109, 110). A weak positive significant correlation with physical QoL was observed (r = 0.13; 95%CI 0.04 to 0.22; I2 = 74.80%, k = 9) in the MA of the nine studies (Figure 13).
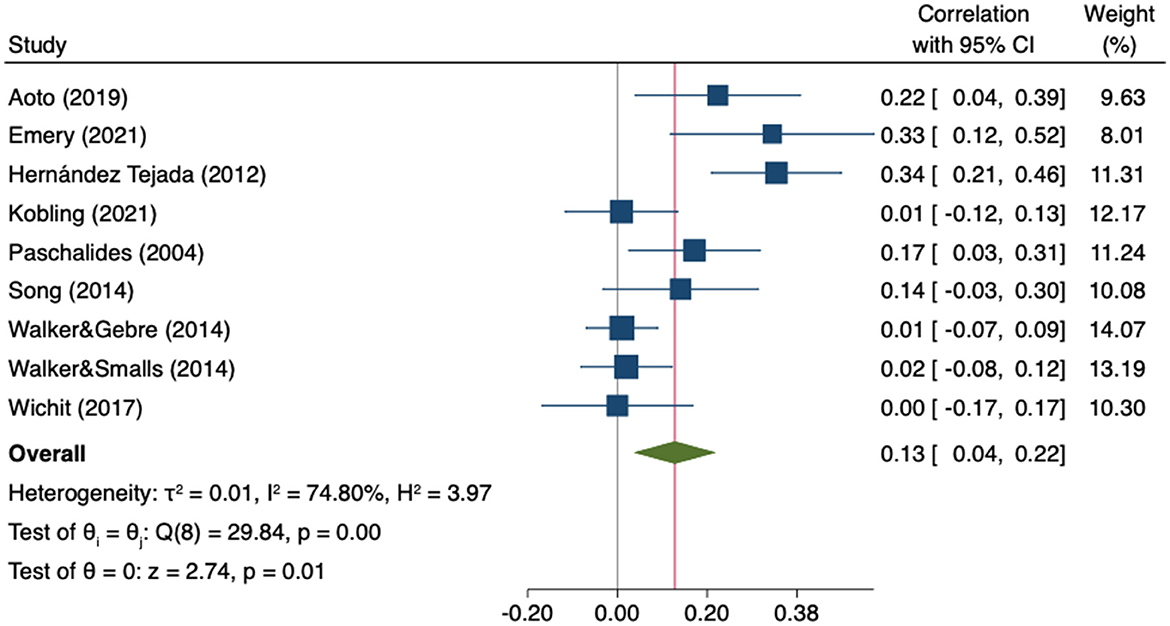
Figure 13. Random-effects meta-analysis on the association between empowerment and physical QoL.
The sensitivity analysis showed the consistency of the findings as neither direction or significance of the pooled effect changed after removing any individual study. The estimates ranged from 0.09 to 0.14 (Supplementary material 4F). Heterogeneity was high and statistically significant (Q = 29.84, p = 0.0002). No statistically significant differences were found in the subgroup analysis by type of empowerment indicator (self-efficacy vs. perceived control) (Supplementary material 5E). The visual inspection of the funnel plot suggested showed asymmetry (Figure 14).
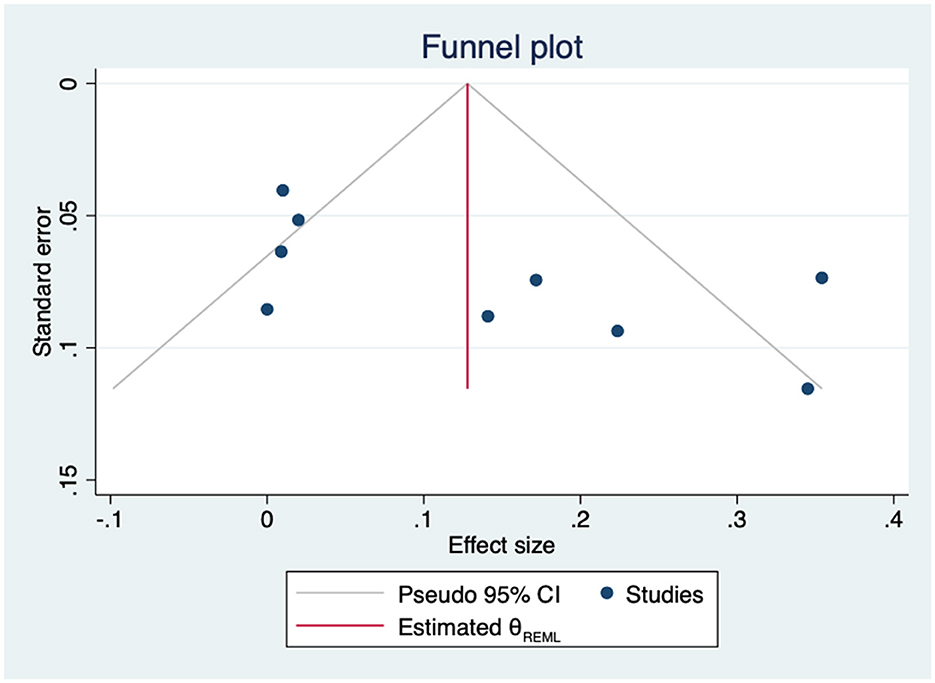
Figure 14. Funnel plot for the association between empowerment and physical QoL.
4. Discussion
To the best of our knowledge, this SR is the first synthesis of the available knowledge on the relationship between patient empowerment or related constructs with affective outcomes and QoL in patients with T2DM. Seventy-one studies were identified, including a large total sample of adults with T2DM. However, only a few studies have evaluated empowerment itself, with most of them relying on self-efficacy measures, since this construct has a longer tradition in psychology than patient empowerment. As a result, the results mainly refer to this specific component of empowerment, i.e., the self-perception of being able to execute behaviors necessary to resolve specific problems or tasks (the self-management of the disease in this case). As mentioned in the introduction, empowerment has a broader theoretical scope than constructs such as self-efficacy or perceived control. For instance, it includes not only the subjective perception of self-efficacy, but also the objective cognitive and emotional abilities required for adequate disease management (e.g., correct knowledge of self-care strategies, objective health literacy, adaptive coping styles or good communication skills when interacting with healthcare providers). However, the different theoretical models of empowerment agree that self-efficacy is one of its essential components, and it is not conceivable to have an empowered patient with a poor perception of their ability to correctly manage their health condition correctly. There is empirical evidence showing that empowerment and self-efficacy are different and not interchangeable concepts, but they are also significantly correlated (125–127). Our subgroup analyses based on the evaluated construct were inconclusive due to the small number of studies assessing empowerment. Nevertheless, the pooled results of these studies were also significant in the same direction as the association between self-efficacy and the outcomes, albeit the strength of the association may be weaker, especially for depression.
The results of the MA showed significant inverse relationships between these constructs and anxiety, depression and distress. Besides, there are significant positive associations with mental, physical and general QoL Nevertheless, the number of studies/patients is lower for the mental and physical components, as well as the strength of their correlations with the empowerment-related constructs. The effect sizes are small, between 0.13 and 0.32 in absolute values. Results on depression showed a significant moderator effect of gender. Specifically, when the percentage of females in the samples increased, so did the observed inverse correlation between empowerment and depressive symptoms (nonetheless, a significant proportion of the variance remained unexplained after controlling for gender). We do not know of other studies in diabetes that have analyzed this moderator effect of gender. In a study with family caregivers of elderly people, a lower self-efficacy was associated with depressive symptoms and this relationship was stronger in female caregivers (128).
Although publication bias cannot be ruled out, the pooled correlations did not change substantially and remained significant when potential missed studies were imputed. The main uncertainty relating to these results has to do with the high heterogeneity observed in all the analyses, which was mostly unexplained by the moderators studied (except by one outlier study causing most of the heterogeneity in the case of anxiety). The few subgroup analyses conducted with the available data are inconclusive because all of them are limited by the low number of studies in one of the subgroups. Another methodological limitation of the identified evidence is that most studies were cross-sectional, ruling out the possibility of investigating longitudinal associations. Only four prospective studies reported this association for QoL and could be included in a subgroup analysis, showing a slightly lower correlation than that observed in cross-sectional studies (0.25 vs. 0.33), although this difference was not significant. Duarte-Díaz et al. (36) found that baseline empowerment was not a significant predictor of anxiety and depression 1 and 2 years later, but the change in empowerment significantly correlated with an inverse change in affective outcomes. Future studies should try to overcome these limitations, including prospective designs, interaction analyses with gender or other sociodemographic or clinical variables, and also comparing the predictive capacity of the different empowerment-related constructs on glycemic control and acute complications.
The American Psychological Association defines psychological distress as “a set of painful mental and physical symptoms that are associated with normal fluctuations of mood in most people” (129). Likewise, diabetes-related distress implies significant negative emotional reactions to the diagnosis of diabetes, the threat of complications and self-management demands (130). According to the results here, lower levels of empowerment-related constructs, especially self-efficacy, are linked to both general and diabetes-related distress, but the strength of the association was higher with specific diabetes distress scales. Although this result is provisional due to the low number of studies in the subgroup of general distress, it seems reasonable to expect that patient empowerment, which includes knowledge, skills, attitudes and self-awareness to influence one's own health, is mainly related to the specific affective processes arising due to the difficulty of managing the demands of diabetes. The positive impact of empowerment and related constructs on psychological symptoms and distress results in a better mental and general quality of life; earlier SRs among patients with other health conditions such as cardiovascular disease (131), cancer (132) and rheumatoid arthritis (133) have shown significant positive associations between empowerment-related constructs and quality of life.
The correlation between self-efficacy about diabetes self-care and affective outcomes aligns with Bandura's postulates (134). Self-efficacy plays a pivotal role in regulating affective states (135). Patients with lower self-efficacy may harbor doubts about their abilities to cope with the daily demands of diabetes, resulting in increased stress, anxiety or depression. On the other side, the possibility of bidirectional associations cannot be ruled out and the patients' ability and willingness to be actively involved in their care may be affected by the presence of affective symptoms. Depressed patients may feel that they have less control over the disease, thus resulting in poorer self-care strategies (136). Likewise, anxiety can interfere on cognitive and motivational processes necessary for an adequate self-care and the emergence of empowerment (137). On the contrary, empowering patients may improve affective symptoms. A recent MA showed that interventions tailoring patient activation effectively improve anxiety and depression symptoms in several chronic conditions including diabetes (138). Similarly, Hernández-Jimenez et al. (39), found that a 2-years comprehensive program based on empowerment strategies had a noteworthy positive effect on both anxiety and depression symptoms in recently diagnosed T2DM patients.
The findings here have some relevant implications for clinical practice. Previous studies have emphasized the importance of managing emotional symptoms in patients with T2DM and that empowerment-related constructs might play a significant role. The association between affective symptoms and diabetes self-care and treatment adherence has been widely studied but what the influence of these pathways is has still not been fully explained. Affective symptoms are related to lower self-efficacy and low self-efficacy is equally associated with poor glycemic control and lower medication adherence (139). Moreover, several studies highlight empowerment-related constructs as potential mediators between affective outcomes and self-care and diabetes control. Specifically, there is evidence suggesting that both depression and diabetes distress are related to poorer treatment adherence, self-care behaviors and glycemic control while this association is partially mediated through perceived control or self-efficacy (48, 66, 69). In addition, a recent study including patients with type 1 DM and T2DM has shown that the association between self-efficacy and QoL was partially mediated by depressive symptoms (140). Accordingly, it is necessary to establish how these variables are related to each other to better understand the pathways through which patient empowerment is related to affective symptoms and QoL and how they jointly affect self-management and glycemic control in patients with T2DM.
The main methodological limitation of this SR is the possibility of missing studies not included in the databases used. Furthermore, gray literature was not included in the search strategy and this may have resulted in a loss of information. Other limitations concern to the identified studies and have been previously commented. Most of them are cross-sectional, precluding conclusions about longitudinal associations. A high statistically significant heterogeneity was obtained in all the analyses, mostly unexplained by the studied moderators. Subgroup analyses were limited by the low number of studies in one of the subgroups, and there could be non-considered confounding variables that potentially moderated the observed associations. Finally, despite the fact that publication bias was not identified, the Egger tests may lack the statistical power to detect bias due to the small number of included studies in the case of anxiety and both mental and physical QoL.
5. Conclusion
Current evidence suggests that empowerment-related constructs are negatively associated with affective symptoms and positively correlated with QoL in patients with T2DM. A wide range of variables can affect psychological outcomes and thus these associations are complex. In accordance, the correlation coefficients we reported are mostly small but not negligible. This evidence is mainly from cross-sectional studies and thus it is not possible to confirm the direction of the observed association. Consequently, high-quality prospective studies are warranted not only to better understand the role of patient empowerment and other indicators on affective symptoms and QoL but also to assess causal associations. Moreover, variables potentially modifying the association between empowerment-related constructs and affective outcomes and QoL remain unclear and require further investigation.
5.1. Practice implications
The findings of this SR provide valuable information to researchers, healthcare professionals and policy makers involved in the management of T2DM. The results highlight patient empowerment and related constructs as significant components of diabetes care linked to better mental health and increased QoL. Thus, this should be considered in the design, development and implementation of effective interventions and policies that seek to improve clinical and psychosocial outcomes in patients with T2DM.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
AD-D: conceptualization, methodology, formal analysis, investigation, and writing—original draft. LP-P: conceptualization, methodology, supervision, and writing—review and editing. AR-S: conceptualization, methodology, formal analysis, and writing—review and editing. WP: conceptualization, supervision, and writing—review and editing. YÁ-P, VR-G, LG-A, MB-B, and SG-M: investigation and writing—review and editing. HG-P, YR-F, and CC: writing—review and editing. PS-A: supervision and writing—review and editing. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to thank Leticia Rodríguez and Carlos González for their help with the database search and acquisition of the relevant papers. We also thank Patrick Dennis for copyediting services during preparation of the final manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1118324/full#supplementary-material
References
1. Al-Lawati JA. Diabetes mellitus: A local and global public health emergency! Vol. 32, Oman Medical Journal. Oman Medical Specialty Board (2017). p. 177–9. doi: 10.5001/omj.2017.34
2. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF diabetes atlas: global, regional, and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. (2022) 183:109119. doi: 10.1016/j.diabres.2021.109119
3. Moini J. Type 2 Diabetes. In: Epidemiology of Diabetes. Elsevier (2019). p. 91–114. doi: 10.1016/B978-0-12-816864-6.00007-9
4. American Diabetes Association. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care. (2020) 43:S14–31. doi: 10.2337/dc20-S002
5. Cannon A, Handelsman Y, Heile M, Shannon M. Burden of illness in type 2 diabetes mellitus. J Manag Care Spec Pharm. (2018) 24:S5–13. doi: 10.18553/jmcp.2018.24.9-a.s5
6. Liu J, Wang R, Ganz ML, Paprocki Y, Schneider D, Weatherall J. The burden of severe hypoglycemia in type 2 diabetes. Curr Med Res Opin. (2018) 34:179–86. doi: 10.1080/03007995.2017.1391080
7. Davies MJ, D'Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European association for the study of diabetes (EASD). Vol. 41, Diabetes Care. American Diabetes Association Inc. (2018). p. (2669–701. doi: 10.2337/dci18-0033
8. Sina M, Graffy J, Simmons D. Associations between barriers to self-care and diabetes complications among patients with type 2 diabetes. Diabetes Res Clin Pract. (2018) 141:126–31. doi: 10.1016/j.diabres.2018.04.031
9. Vancampfort D, Mitchell AJ, De Hert M, Sienaert P, Probst M, Buys R, et al. Type 2 diabetes in patients with major depressive disorder: a meta-analysis of prevalence estimates and predictors: review: depression and diabetes. Depress Anxiety. (2015) 32:763–73. doi: 10.1002/da.22387
10. Khaledi M, Haghighatdoost F, Feizi A, Aminorroaya A. The prevalence of comorbid depression in patients with type 2 diabetes: an updated systematic review and meta-analysis on huge number of observational studies. Acta Diabetol. (2019) 56:9. doi: 10.1007/s00592-019-01295-9
11. Chaturvedi SK, Manche Gowda S, Ahmed HU, Alosaimi FD, Andreone N, Bobrov A, et al. More anxious than depressed: prevalence and correlates in a 15-nation study of anxiety disorders in people with type 2 diabetes mellitus. Gen Psychiatry. (2019) 32:76. doi: 10.1136/gpsych-2019-100076
12. Chaudhary R, Kumar P, Chopra A, Chabbra S, Singh P. Comparative study of psychiatric manifestations among Type i and Type II diabetic patients. Indian J Psychol Med. (2017) 39:342–6. doi: 10.4103/IJPSYM.IJPSYM_35_17
13. Lindekilde N, Scheuer SH, Rutters F, Knudsen L, Lasgaard M, Rubin KH, et al. Prevalence of type 2 diabetes in psychiatric disorders: an umbrella review with meta-analysis of 245 observational studies from 32 systematic reviews. Diabetologia. (2022) 65:440–56. doi: 10.1007/s00125-021-05609-x
14. Lloyd CE, Sartorius N, Ahmed HU, Alvarez A, Bahendeka S, Bobrov AE, et al. Factors associated with the onset of major depressive disorder in adults with type 2 diabetes living in 12 different countries: Results from the INTERPRET-DD prospective study. Epidemiol Psychiatr Sci. (2020) 29:438. doi: 10.1017/S2045796020000438
15. Smith KJ, Pedneault M, Schmitz N. Investigation of anxiety and depression symptom co-morbidity in a community sample with type 2 diabetes: associations with indicators of self-care. Can J Public Health. (2015) 106:e496–501. doi: 10.17269/CJPH.106.5170
16. Nefs G, Hendrieckx C, Reddy P, Browne JL, Bot M, Dixon J, et al. Comorbid elevated symptoms of anxiety and depression in adults with type 1 or type 2 diabetes: results from the international diabetes miles study. J Diabetes Complications. (2019) 33:523–9. doi: 10.1016/j.jdiacomp.2019.04.013
17. Naicker K, Øverland S, Johnson JA, Manuel D, Skogen JC, Sivertsen B, et al. Symptoms of anxiety and depression in type 2 diabetes: associations with clinical diabetes measures and self-management outcomes in the Norwegian HUNT study. Psychoneuroendocrinology. (2017) 84:116–23. doi: 10.1016/j.psyneuen.2017.07.002
18. Guerrero Fernández de., Alba I, Gimeno-Miguel A, Poblador-Plou B, Gimeno-Feliu LA, Ioakeim-Skoufa I, Rojo-Martínez G, et al. Association between mental health comorbidity and health outcomes in type 2 diabetes mellitus patients. Sci Rep. (2020) 10:1–9. doi: 10.1038/s41598-020-76546-9
19. Danese A, Moffitt TE, Harrington H, Milne BJ, Polanczyk G, Pariante CM, et al. Adverse childhood experiences and adult risk factors for age-related disease: depression, inflammation, and clustering of metabolic risk markers. Arch Pediatr Adolesc Med. (2009) 3:214. doi: 10.1001/archpediatrics.2009.214
20. Vogelzangs N, Suthers K, Ferrucci L, Simonsick EM, Ble A, Schrager M, et al. Hypercortisolemic depression is associated with the metabolic syndrome in late-life. Psychoneuroendocrinology. (2007) 32:151–9. doi: 10.1016/j.psyneuen.2006.11.009
21. de Groot M, Anderson R, Freedland KE, Clouse RE, Lustman PJ. Association of depression and diabetes complications: a meta-analysis. Psychosom Med. (2001) 63:619–30. doi: 10.1097/00006842-200107000-00015
22. Young-Hyman D, De Groot M, Hill-Briggs F, Gonzalez JS, Hood K, Peyrot M. Psychosocial care for people with diabetes: a position statement of the American diabetes association. Diabetes Care. (2016) 39:2126–40. doi: 10.2337/dc16-2053
23. World Health Organization. Division of Health Promotion and Communication E. Health Promotion Glossary. Geneva PP - Geneva: World Health Organization (1998).
24. Castro EM, Van Regenmortel T, Vanhaecht K, Sermeus W, Van Hecke A. Patient empowerment, patient participation and patient-centeredness in hospital care: a concept analysis based on a literature review. Patient Educ Couns. (2016) 99:1923–39. doi: 10.1016/j.pec.2016.07.026
25. Funnell MM, Anderson RM. Empowerment and self-management of diabetes. Clin Diabetes. (2004) 22:123–7. doi: 10.2337/diaclin.22.3.123
26. Fumagalli LP, Radaelli G, Lettieri E. Bertele' P, Masella C. Patient Empowerment and its neighbours: clarifying the boundaries and their mutual relationships. Health Policy. (2015) 119:384–94. doi: 10.1016/j.healthpol.2014.10.017
27. Aujoulat I, D'Hoore W, Deccache A. Patient empowerment in theory and practice: polysemy or cacophony? Patient Educ Couns. (2007) 66:13–20. doi: 10.1016/j.pec.2006.09.008
28. McAllister M, Dunn G, Payne K, Davies L, Todd C. Patient empowerment: The need to consider it as a measurable patient-reported outcome for chronic conditions. BMC Health Serv Res. (2012) 12:1–8. doi: 10.1186/1472-6963-12-157
29. Bravo P, Edwards A, Barr PJ, Scholl I, Elwyn G, McAllister M. Conceptualising patient empowerment: a mixed methods study. BMC Health Serv Res. (2015) 15:252. doi: 10.1186/s12913-015-0907-z
30. Tilkin, De Winter, Ketterer, Etienne, Vanmeerbeek, Schoenaers. considering patients' empowerment in chronic care management: a cross-level approach. Eur J Investig Health Psychol Educ. (2019) 10:134–42. doi: 10.3390/ejihpe10010012
31. Pekonen A, Eloranta S, Stolt M, Virolainen P, Leino-Kilpi H. Measuring patient empowerment—A systematic review. Patient Educ Couns. (2020) 103:777–87. doi: 10.1016/j.pec.2019.10.019
32. Barr PJ, Scholl I, Bravo P, Faber MJ, Elwyn G, McAllister M. Assessment of patient empowerment—A systematic review of measures. PLoS ONE. (2015) 10:e0126553. doi: 10.1371/journal.pone.0126553
33. Salzburg Global Seminar. Salzburg statement on shared decision making. BMJ. (2011) 342:1745. doi: 10.1136/bmj.d1745
34. Sympa P, Vlachou E, Kazakos K, Govina O, Stamatiou G, Lavdaniti M. Depression and Self-efficacy in patients with type 2 diabetes in Northern Greece. Endocr Metab Immune Disord - Drug Targets. (2017) 18:371–8. doi: 10.2174/1871530317666171120154002
35. Lin YH, Chen DA, Lin C, Huang H. Type d personality is associated with glycemic control and socio-psychological factors on patients with type 2 diabetes mellitus: a cross-sectional study. Psychol Res Behav Manag. (2020) 13:373–81. doi: 10.2147/PRBM.S245226
36. Duarte-Díaz A, González-Pacheco H, Rivero-Santana A, Ramallo-Fariña Y, Perestelo-Pérez L, Álvarez-Pérez Y, et al. Increased patient empowerment is associated with improvement in anxiety and depression symptoms in type 2 diabetes mellitus: findings from the indica study. Int J Environ Res Public Health. (2022) 19:4818–4818. doi: 10.3390/ijerph19084818
37. Hoogendoorn CJ, Shapira A, Roy JF, Walker EA, Cohen HW, Gonzalez JS. Depressive symptom dimensions and medication non-adherence in suboptimally controlled type 2 diabetes. J Diabetes Complications. (2019) 33:217–22. doi: 10.1016/j.jdiacomp.2018.12.001
38. Brown SA, García AA, Brown A, Becker BJ, Conn VS, Ramírez G, et al. Biobehavioral determinants of glycemic control in type 2 diabetes: a systematic review and meta-analysis. Patient Educ Couns. (2016) 99:1558–67. doi: 10.1016/j.pec.2016.03.020
39. Hernández-Jiménez S, García-Ulloa AC, Bello-Chavolla OY, Aguilar-Salinas CA, Kershenobich-Stalnikowitz D. Long-term effectiveness of a type 2 diabetes comprehensive care program. The CAIPaDi model. Diabetes Res Clin Pract. (2019) 151:128–37. doi: 10.1016/j.diabres.2019.04.009
40. Cheng L, Sit JWH, Choi KC, Chair SY, Li X, Wu Y, et al. The effects of an empowerment-based self-management intervention on empowerment level, psychological distress, and quality of life in patients with poorly controlled type 2 diabetes: a randomized controlled trial. Int J Nurs Stud. (2019) 3:103407. doi: 10.1016/j.ijnurstu.2019.103407
41. Baldoni NR, Aquino JA, Sanches-Giraud C, Di Lorenzo Oliveira C, de Figueiredo RC, Cardoso CS, et al. Collective empowerment strategies for patients with diabetes mellitus: a systematic review and meta-analysis. Prim Care Diabetes. (2017) 11:201–11. doi: 10.1016/j.pcd.2016.09.006
42. Aquino JA, Baldoni NR, Flôr CR, Sanches C, Di Lorenzo Oliveira C, Alves GCS, et al. Effectiveness of individual strategies for the empowerment of patients with diabetes mellitus: a systematic review with meta-analysis. Prim Care Diabetes. (2018) 12:97–110. doi: 10.1016/j.pcd.2017.10.004
43. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. The BMJ. (2021) 54:372. doi: 10.1136/bmj.n71
44. Ababio GK, Bosomprah S, Olumide A, Aperkor N, Aimakhu C, Oteng-Yeboah A, et al. Predictors of quality of life in patients with diabetes mellitus in two tertiary health institutions in Ghana and Nigeria. Niger Postgrad Med J. (2017) 24:48–55. doi: 10.4103/npmj.npmj_3_17
45. Ching SM, Yee A, Lee PY, Ramachandran V, Shum KM, Ismael NFI, et al. Psychometric properties of the Malay version of the diabetes empowerment scale among hospital Serdang type 2 diabetes mellitus patients using exploratory factor analysis. Health Qual Life Outcomes. (2020) 18:1280. doi: 10.1186/s12955-020-1280-0
46. Clarke A. Effectiveness of a community orientated diabetes education (CODE) programme for people with type 2 diabetes. Eur Diabetes Nurs. (2011 S) 8:94–99a. doi: 10.1002/edn.188
47. Hernandez R, Ruggiero L, Prohaska TR, Chavez N, Boughton SW, Peacock N, et al. A cross-sectional study of depressive symptoms and diabetes self-care in African Americans and Hispanics/Latinos with diabetes: the role of self-efficacy. Diabetes Educ. (2016) 42:452–61. doi: 10.1177/0145721716654008
48. Lin K, Park C, Li M, Wang X, Li X, Li W, et al. Effects of depression, diabetes distress, diabetes self-efficacy, and diabetes self-management on glycemic control among Chinese population with type 2 diabetes mellitus. Diabetes Res Clin Pract. (2017) 131:179–86. doi: 10.1016/j.diabres.2017.03.013
49. Oliveira S, Morais C. Literacy promotion and empowerment of type 2 diabetics elderly in primary health care. Millenium. (2016) 5:175–82. Available online at: https://revistas.rcaap.pt/millenium/article/view/13940
50. Simonsen N, Koponen AM, Suominen S. Empowerment among adult patients with type 2 diabetes: age differentials in relation to person-centred primary care, community resources, social support and other life-contextual circumstances. BMC Public Health. (2021) 21:855. doi: 10.1186/s12889-021-10855-0
51. Wang RH, Wu LC, Hsu HY, A. path model of health-related quality of life in Type 2 diabetic patients: a cross-sectional study in Taiwan. J Adv Nurs. (2011) 67:2658–67. doi: 10.1111/j.1365-2648.2011.05701.x
52. Zhu Y, Fish AF Li F, Liu L, Lou Q. Psychosocial factors not metabolic control impact the quality of life among patients with type 2 diabetes in China. Acta Diabetol. (2016) 53:535–41. doi: 10.1007/s00592-015-0832-y
53. Abdelghaffar W, Amiri H, Zouari B. Self-care activities adherence in Tunisian patients with type 2 diabetes: role of diabetes-related distress and self-efficacy. Acta Diabetol. (2020) 57:631–3. doi: 10.1007/s00592-020-01476-x
54. Al-Amer R, Ramjan L, Glew P, Randall S, Salamonson Y. Self-efficacy, depression, and self-care activities in adult Jordanians with type 2 diabetes: the role of illness perception. Issues Ment Health Nurs. (2016) 37:744–55. doi: 10.1080/01612840.2016.1208692
55. Al-Dwaikat TN, Rababah JA, Al-Hammouri MM, Chlebowy DO. Social support, self-efficacy, and psychological wellbeing of adults with type 2 diabetes. West J Nurs Res. (2021) 43:288–97. doi: 10.1177/0193945920921101
56. Alipour A, Zare H, Poursharifi H, Aerab Sheibani K, Afkhami Ardekani M. The intermediary role of self-efficacy in relation with stress, glycosylated haemoglobin and health-related quality of life in patients with type2 diabetes. Iran J Public Health. (2012) 41:76–80. Available online at: http://ijph.tums.ac.ir
57. Alzubaidi H, Sulieman H, Mc Namara K, Samorinha C, Browning C. The relationship between diabetes distress, medication taking, glycaemic control and self-management. Int J Clin Pharm. (2022) 44:127–37. doi: 10.1007/s11096-021-01322-2
58. Anderson JR, Novak JR, Johnson MD, Deitz SL, Walker A, Wilcox A, et al. A dyadic multiple mediation model of patient and spouse stressors predicting patient dietary and exercise adherence via depression symptoms and diabetes self-efficacy. J Behav Med. (2016) 39:1020–32. doi: 10.1007/s10865-016-9796-9
59. Aoto H, Tanimura C, Majbauddin A, Kobayashi N, Morita T, Inoue K, et al. A conceptual model for quality of life among people with type 2 diabetes in the Philippines. Yonago Acta Med. (2019) 62:53–61. doi: 10.33160/yam.2019.03.008
60. Azadbakht M, Fadayevatan R, Tanjani PT, Foroughan M, Zanjari N. Prevalence and determinant factors of diabetes distress in community-dwelling elderly in Qom, Iran. Int J Prev Med. (2021) 12:145–145. doi: 10.4103/ijpvm.IJPVM_372_19
61. Azami G, Soh KL, Sazlina SG. Salmiah MdS, Khosravi A, Aazami S, et al. The effect of depression on poor glycemic control in adults with type 2 diabetes: the mediating roles of self-efficacy and self-management behaviors Dubai diabetes. Endocrinol J. (2019) 25:80–9. doi: 10.1159/000502126
62. Chao J, Nau DP, Aikens JE, Taylor SD. The mediating role of health beliefs in the relationship between depressive symptoms and medication adherence in persons with diabetes. Res Soc Adm Pharm. (2005) 1:508–25. doi: 10.1016/j.sapharm.2005.09.002
63. Cherrington A, Wallston KA, Rothman RL. Exploring the relationship between diabetes self-efficacy, depressive symptoms, and glycemic control among men and women with type 2 diabetes. J Behav Med. (2010) 33:81–9. doi: 10.1007/s10865-009-9233-4
64. Chew BH, Vos RC, Pouwer F, Rutten GEHM. The associations between diabetes distress and self-efficacy, medication adherence, self-care activities and disease control depend on the way diabetes distress is measured: comparing the DDS-17, DDS-2 and the PAID-5. Diabetes Res Clin Pract. (2018) 142:74–84. doi: 10.1016/j.diabres.2018.05.021
65. Coffman MJ. Effects of tangible social support and depression on diabetes self-efficacy. J Gerontol Nurs. (2008) 34:32–9. doi: 10.3928/00989134-20080401-02
66. Devarajooh C, Chinna K. Depression, distress and self-efficacy: the impact on diabetes self-care practices. PLoS ONE. (2017) 12:96. doi: 10.1371/journal.pone.0175096
67. Emery KA, Robins J, Salyer J, Thurby-Hay L, Djira G. Type 2 diabetes self-management variables and predictors. Clin Nurs Res. (2021) 5:105477382110673. doi: 10.1177/10547738211067322
68. Fereydouni F, Hajian-Tilaki K, Meftah N, Chehrazi M, A. path causal model in the association between self-efficacy and self-care with quality of life in patients with type 2 diabetes: an application of the structural equation model. Health Sci Rep. (2022) 5:e534–e534. doi: 10.1002/hsr2.534
69. Gonzalez JS, Shreck E, Psaros C, Safren SA. Distress and type 2 diabetes-treatment adherence: a mediating role for perceived control. Health Psychol. (2015) 34:505–13. doi: 10.1037/hea0000131
70. Hsu HC, Chen SY, Lee YJ, Chen WY, Wang RH. Pathways of diabetes distress, decisional balance, self-efficacy and resilience to quality of life in insulin-treated patients with type 2 diabetes: A 9-month prospective study. J Clin Nurs. (2021) 30:1070–8. doi: 10.1111/jocn.15652
71. Huang YC, Zuñiga J, García A. Illness perceptions as a mediator between emotional distress and management self-efficacy among Chinese Americans with type 2 diabetes. Ethn Health. (2020) 5:7339. doi: 10.1080/13557858.2020.1817339
72. Huayanay-Espinoza IE, Guerra-Castañon F, Reyes-Diaz M, Lazo-Porras M, de la Cruz-Luque C, Herrera DA, et al. Calidad de vida y autoeficacia en pacientes con diabetes mellitus tipo 2 en un hospital público peruano. Medwave. (2021) 21:e8133. doi: 10.5867/medwave.2021.02.8132
73. Indelicato L, Dauriz M, Santi L, Bonora F, Negri C, Cacciatori V, et al. Psychological distress, self-efficacy, and glycemic control in type 2 diabetes. Nutr Metab Cardiovasc Dis. (2017) 27:300–6. doi: 10.1016/j.numecd.2017.01.006
74. Jahanlou, Karami. The effect of literacy level on health related-quality of life, self-efficacy and self-management behaviors in diabetic patients - PubMed. Acta Med Iran. (2011) 5:153–8. Available online at: https://acta.tums.ac.ir/index.php/acta/article/view/3714
75. Ji M, Ren D, Dunbar-Jacob J, Gary-Webb TL, Erlen JA. Self-management behaviors, glycemic control, and metabolic syndrome in type 2 diabetes. Nurs Res. (2020) 69:E9–17. doi: 10.1097/NNR.0000000000000401
76. Ji M, Sereika SM, Dunbar-Jacob J, Erlen JA. Correlation of symptom distress, self-efficacy, and social support with problem-solving and glycemic control among patients with type 2 diabetes. Sci Diabetes Self-Manag Care. (2021) 47:85–93. doi: 10.1177/0145721720983222
77. Kav S, Yilmaz AA, Bulut Y, Dogan N. Self-efficacy, depression and self-care activities of people with type 2 diabetes in Turkey. Collegian. (2017) 24:27–35. doi: 10.1016/j.colegn.2015.09.005
78. Kim MY, Lee EJ. Factors affecting self-care behavior levels among elderly patients with type 2 diabetes: A quantile regression approach. Med Lith. (2019) 55:340. doi: 10.3390/medicina55070340
79. Kim MT, Kim KB, Ko J, Murry N, Xie B, Radhakrishnan K, et al. Health literacy and outcomes of a community-based self-help intervention: a case of Korean Americans with type 2 diabetes. Nurs Res. (2020) 69:210–8. doi: 10.1097/NNR.0000000000000409
80. Köbling T, Váradi Z, Katona É, Somodi S, Kempler P, Páll D, et al. Predictors of dietary self-efficacy in high glycosylated hemoglobin A1c type 2 diabetic patients. J Int Med Res. (2020) 48:1284. doi: 10.1177/0300060520931284
81. Latham CL, Calvillo E. Predictors of successful diabetes management in low-income Hispanic people. West J Nurs Res. (2009) 31:364–88. doi: 10.1177/0193945908328263
82. Latham CL, Calvillo E. Predictors of diabetes outcomes in Mexico: testing the hispanic health protection model. J Transcult Nurs. (2013) 24:271–81. doi: 10.1177/1043659613481626
83. Matteucci, Giampetro. Closing the gap between literature and practice: evaluation of a teaching programme (in the absence of a structured treatment) on both type 1 and type 2 diabetes - PubMed. Diabetes Nutr Metab. (2003) 5:298–305.
84. Messina R, Rucci P, Sturt J, Mancini T, Fantini MP. Assessing self-efficacy in type 2 diabetes management: validation of the italian version of the diabetes management self-efficacy scale (IT-DMSES). Health Qual Life Outcomes. (2018) 16(1). doi: 10.1186/s12955-018-0901-3
85. Oviedo-Gómez MT, Reidl-Martínez LM. Predictores psicológicos individuales de la calidad de vida en diabetes tipo 2. Revista Mexicana de Psicol. (2008) 54:31–42. Available online at: https://www.redalyc.org/articulo.oa?id=243020635005
86. Padgett DK. Correlates of self-efficacy beliefs among patients with non-insulin dependent diabetes mellitus in Zagreb, Yugoslavia. Patient Educ Couns. (1991) 18:139–47. doi: 10.1016/0738-3991(91)90006-Q
87. Park H, Kim MT. Impact of social role strain, depression, social support and age on diabetes self-efficacy in Korean women with type 2 diabetes. J Cardiovasc Nurs. (2012) 27:76–83. doi: 10.1097/JCN.0b013e318214d9d9
88. Pisanti R, Lzzari D. Il ruolo delle rappresentazioni della malattia e delle dimensioni socio cognitive nell'adattamento emotivo in un gruppo di pazienti affetti da diabete di tipo II. / The role of illness perception and the socio-cognitive dimension in emotional adjustment i. Psicoterapia Cognitive e Comportamentale. (2005) 25:235–48.
89. Rao D, Maurer M, Meyer J, Zhang J, Shiyanbola OO. Medication adherence changes in blacks with diabetes: a mixed methods study. Am J Health Behav. (2020) 44:257–70. doi: 10.5993/AJHB.44.2.13
90. Robertson SM, Amspoker AB, Cully JA, Ross EL, Naik AD. Affective symptoms and change in diabetes self-efficacy and glycaemic control. Diabet Med. (2013) 30:1216. doi: 10.1111/dme.12146
91. Rusni M, Amriati M, Askar M. The relation between self-efficacy and quality of life of patients with type 2 diabetes mellitus in Pelamonia hospital Makassar. Indian J Public Health Res Dev. (2020) 11:2346–50. doi: 10.37506/ijphrd.v11i3.2752
92. Sacco WP, Wells KJ, Vaughan CA, Friedman A, Perez S, Matthew R. Depression in adults with type 2 diabetes: the role of adherence, body mass index, and self-efficacy. Health Psychol. (2005) 24:630–4. doi: 10.1037/0278-6133.24.6.630
93. Sacco WP, Wells KJ, Friedman A, Matthew R, Perez S, Vaughan CA. Adherence, body mass index, and depression in adults with type 2 diabetes: the mediational role of diabetes symptoms and self-efficacy. Health Psychol. (2007) 26:693–700. doi: 10.1037/0278-6133.26.6.693
94. Samuel-Hodge CD, Watkins DC, Rowell KL, Hooten EG. Coping styles, well-being, and self-care behaviors among African Americans with type 2 diabetes. Diabetes Educ. (2008) 34:501–10. doi: 10.1177/0145721708316946
95. Sari Y, Isworo A, Upoyo AS, Taufik A, Setiyani R, Swasti KG, et al. The differences in health-related quality of life between younger and older adults and its associated factors in patients with type 2 diabetes mellitus in Indonesia. Health Qual Life Outcomes. (2021) 19:2. doi: 10.1186/s12955-021-01756-2
96. Sit RW, Wang B, Ng WS, Abullah A, Isamail IZ, Goh LH, et al. Prevalence and association of chronic musculoskeletal pain on self-management, glycemic control and quality of life among Chinese type 2 diabetes patients in primary care. Prim Care Diabetes. (2022) 3:4. doi: 10.1016/j.pcd.2022.04.004
97. Song R, Ahn S, Oh H, A. structural equation model of quality of life in adults with type 2 diabetes in Korea. Appl Nurs Res. (2013) 26:116–20. doi: 10.1016/j.apnr.2013.04.001
98. Steed L, Barnard M, Hurel S, Jenkins C, Newman S. How does change occur following a theoretically based self-management intervention for type 2 diabetes. Psychol Health Med. (2014) 19:536–46. doi: 10.1080/13548506.2013.845301
99. Suhaimi AF, Makki SM, Tan KA, Silim UA, Ibrahim N. Translation and validation of the malay version of the WHO-5 wellbeing index: reliability and validity evidence from a sample of type 2 diabetes mellitus patients. Int J Environ Res Public Health. (2022) 19:4415. doi: 10.3390/ijerph19074415
100. Tol A, Sharifirad G, Eslami A, Shojaeizadeh D, Alhani F, Tehrani MM. Analysis of some predictive factors of quality of life among type 2 diabetic patients. J Educ Health Promot. (2015) 4:9–9. doi: 10.4103/2277-9531.154022
101. Walker RJ, Gebregziabher M, Martin-Harris B, Egede LE. Independent effects of socioeconomic and psychological social determinants of health on self-care and outcomes in Type 2 diabetes. Gen Hosp Psychiatry. (2014) 36:662–8. doi: 10.1016/j.genhosppsych.2014.06.011
102. Walker R, Smalls B, Hernández-Tejada M, Campbell J, Egede L. Effect of diabetes self-efficacy on glycemic control, medication adherence, self-care behaviors, and quality of life in a predominantly low-income, minority population - PubMed. Ethn Dis. (2014) 45:349–55.
103. Wichit N, Mnatzaganian G, Courtney M, Schulz P, Johnson M. Randomized controlled trial of a family-oriented self-management program to improve self-efficacy, glycemic control and quality of life among Thai individuals with Type 2 diabetes. Diabetes Res Clin Pract. (2017) 123:37–48. doi: 10.1016/j.diabres.2016.11.013
104. Winahyu KM, Anggita R, Widakdo G. Characteristics of patients, self-efficacy and quality of life among patients with type 2 diabetes mellitus. J Keperawatan Padjadjaran. (2019) 7:1175. doi: 10.24198/jkp.v7i3.1175
105. Wu SFV, Huang YC, Lee MC, Wang TJ, Tung HH, Wu MP. Self-efficacy, self-care behavior, anxiety, and depression in Taiwanese with type 2 diabetes: A cross-sectional survey. Nurs Health Sci. (2013) 15:213–9. doi: 10.1111/nhs.12022
106. Yang F, Pang JS, Cheng WJY. Self-care adherence and psychological functioning of older patients with type 2 diabetes: effects of persuasion, social pressure, and self-efficacy. J Clin Psychol Med Settings. (2016) 23:389–401. doi: 10.1007/s10880-016-9470-y
107. Arvanitis M, Bailey SC, Wismer G, Griffith JW, Freeman E, Sims TJ, et al. Development of the influence, motivation, and patient activation in diabetes (IMPACT-DTM) measure. Diabetes Res Clin Pract. (2020) 159:7965. doi: 10.1016/j.diabres.2019.107965
108. Kato A, Fujimaki Y, Fujimori S, Isogawa A, Onishi Y, Suzuki R, et al. Association between self-stigma and self-care behaviors in patients with type 2 diabetes: a cross-sectional study. BMJ Open Diabetes Res Care. (2016) 4:1–7. doi: 10.1136/bmjdrc-2015-000156
109. Hernandez-Tejada MA, Lynch CP, Strom JL, Egede LE. Effect of perceived control on quality of life in indigent adults with type 2 diabetes. Diabetes Educ. (2012) 38:256–62. doi: 10.1177/0145721711436135
110. Paschalides C, Wearden AJ, Dunkerley R, Bundy C, Davies R, Dickens CM. The associations of anxiety, depression and personal illness representations with glycaemic control and health-related quality of life in patients with type 2 diabetes mellitus. J Psychosom Res. (2004) 57:557–64. doi: 10.1016/j.jpsychores.2004.03.006
111. Williams GC, McGregor HA, King D, Nelson CC, Glasgow RE. Variation in perceived competence, glycemic control, and patient satisfaction: relationship to autonomy support from physicians. Patient Educ Couns. (2005) 57:39–45. doi: 10.1016/j.pec.2004.04.001
112. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetc R, et al. Chapter 7: systematic reviews of etiology and risk. In: JBI Manual for Evidence Synthesis JBI. (2020). doi: 10.46658/JBIRM-17-06
113. Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomized trials. BMJ Online. (2011) 343:7829. doi: 10.1136/bmj.d5928
114. National Heart Lung and Blood institute. Study Quality Assessment Tools | NHLBI, NIH. Study Quality Assessment Tools. (2020). Available online at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed May 18, 2021).
115. Cohen J. Statistical power analysis for the behavioral sciences. Academic Press. (2013) 3:1587. doi: 10.4324/9780203771587
116. Rupinski MT, Dunlap WP. Approximating Pearson product-moment correlations from Kendall's tau and Spearman's rho. Educ Psychol Meas. (1996) 56:419–29. doi: 10.1177/0013164496056003004
117. Peterson RA, Brown SP. On the use of beta coefficients in meta-analysis. J Appl Psychol. (2005) 90:175–81. doi: 10.1037/0021-9010.90.1.175
118. Rosenthal R. Parametric measures of effect size. In:Cooper H, Hedges LV, , editors. The Handbook of Research Synthesis. Russell Sage Foundation (1994). p. (231–44.
119. Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
120. Viechtbauer W. Bias and efficiency of meta-analytic variance estimators in the random-effects model. J Educ Behav Stat. (2005) 30:261–93. doi: 10.3102/10769986030003261
121. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
122. Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. (2000) 56:455–63. doi: 10.1111/j.0006-341X.2000.00455.x
123. StataCorp. Stata: Release 17. Statisticacl Software. College Station, TX: StataCorp LLC (2021).
124. StataCorp. Stata Meta-Analysis Reference Manual - Release 17. A Stata Press Publication. TX: StataCorp LLC (2021).
125. Lee YJ, Shin SJ, Wang RH, Lin KD, Lee YL, Wang YH. Pathways of empowerment perceptions, health literacy, self-efficacy, and self-care behaviors to glycemic control in patients with type 2 diabetes mellitus. Patient Educ Couns. (2016) 99:287–94. doi: 10.1016/j.pec.2015.08.021
126. Garcimartín P, Comín-Colet J, Pardo-Cladellas Y, Badosa N, Linas A, Rosenfeld L, et al. Validation of the Spanish version of the questionnaire on patient empowerment in long-term conditions. Shiyanbola OO, editor. PLOS ONE. (2020) 15:e0233338. doi: 10.1371/journal.pone.0233338
127. Kärner Köhler A, Tingström P, Jaarsma T, Nilsson S. Patient empowerment and general self-efficacy in patients with coronary heart disease: a cross-sectional study. BMC Fam Pract. (2018) 19:76. doi: 10.1186/s12875-018-0749-y
128. Chang YP, Seo Y, Von Visger T. Family caregivers' self-efficacy and its relations to wellbeing: gender and age differences. Innov Aging. (2020) 4(Supplement_1):150–150. doi: 10.1093/geroni/igaa057.490
129. American Psychological Association. Psychological distress – APA Dictionary of Psychology. (2020). Available online at: https://dictionary.apa.org/psychological-distress (accessed May 30, 2021).
130. Gonzalez JS, Fisher L, Polonsky WH. Depression in diabetes: have we been missing something important? Diabetes Care. (2011) 34:236–9. doi: 10.2337/dc10-1970
131. Banik A, Schwarzer R, Knoll N, Czekierda K, Luszczynska A. Self-efficacy and quality of life among people with cardiovascular diseases: a meta-analysis. Rehabil Psychol. (2018) 63:295–312. doi: 10.1037/rep0000199
132. Chirico A, Lucidi F, Merluzzi T, Alivernini F, Laurentiis M De, Botti G, et al. A meta-analytic review of the relationship of cancer coping selfefficacy with distress and quality of life. Oncotarget Impact J LLC. (2017) 8:36800–11. doi: 10.18632/oncotarget.15758
133. Martinez-Calderon J, Meeus M, Struyf F, Luque-Suarez A. The role of self-efficacy in pain intensity, function, psychological factors, health behaviors, and quality of life in people with rheumatoid arthritis: a systematic review. Physiotherapy Theory Practice. Taylor and Francis Ltd (2020) 36:21–37. doi: 10.1080/09593985.2018.1482512
134. Bandura A. Social foundations of thought and action: A social cognitive theory. Soc Found Thought Action Soc Cogn Theory. (1986) xiii:617.
135. Bandura A. Regulation of cognitive processes through perceived self-efficacy. Dev Psychol. (1989) 25:729–35. doi: 10.1037/0012-1649.25.5.729
136. Egede LE, Ellis C. The effects of depression on diabetes knowledge, diabetes self-management, and perceived control in indigent patients with type 2 diabetes. Diabetes Technol Ther. (2008) 10:213–9. doi: 10.1089/dia.2007.0278
137. Bickett A, Tapp H. Anxiety and diabetes: Innovative approaches to management in primary care. Exp Biol Med. (2016) 241:1724–31. doi: 10.1177/1535370216657613
138. Lin MY, Weng WS, Apriliyasari RW, Van Truong P, Tsai PS. Effects of patient activation intervention on chronic diseases: a meta-analysis. J Nurs Res. (2020) 28:387. doi: 10.1097/jnr.0000000000000387
139. Náfrádi L, Nakamoto K, Schulz PJ. Is patient empowerment the key to promote adherence? A systematic review of the relationship between self-efficacy, health locus of control and medication adherence. PLoS ONE. (2017) 12:6458. doi: 10.1371/journal.pone.0186458
140. Knowles SR, Apputhurai P, O'Brien CL, Ski CF, Thompson DR, Castle DJ. Exploring the relationships between illness perceptions, self-efficacy, coping strategies, psychological distress and quality of life in a cohort of adults with diabetes mellitus. Psychol Health Med. (2020) 25:214–28. doi: 10.1080/13548506.2019.1695865
Keywords: empowerment, diabetes, affective outcomes, quality of life, systematic review and meta-analysis, self-efficacy
Citation: Duarte-Díaz A, Perestelo-Pérez L, Rivero-Santana A, Peñate W, Álvarez-Pérez Y, Ramos-García V, González-Pacheco H, Goya-Arteaga L, de Bonis-Braun M, González-Martín S, Ramallo-Fariña Y, Carrion C and Serrano-Aguilar P (2023) The relationship between patient empowerment and related constructs, affective symptoms and quality of life in patients with type 2 diabetes: a systematic review and meta-analysis. Front. Public Health 11:1118324. doi: 10.3389/fpubh.2023.1118324
Received: 09 December 2022; Accepted: 27 March 2023;
Published: 17 April 2023.
Edited by:
Muhammad Shahzad Aslam, Xiamen University, MalaysiaReviewed by:
Sultan Ayaz, JSI Research and Training Institute, PakistanNavin Kumar Loganadan, Hospital Putrajaya, Malaysia
Mathumalar Loganathan, Universiti Teknologi MARA, Malaysia
Copyright © 2023 Duarte-Díaz, Perestelo-Pérez, Rivero-Santana, Peñate, Álvarez-Pérez, Ramos-García, González-Pacheco, Goya-Arteaga, de Bonis-Braun, González-Martín, Ramallo-Fariña, Carrion and Serrano-Aguilar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lilisbeth Perestelo-Pérez, bGlsaXNiZXRoLnBlcmVzdGVsb3BlcmV6QHNlc2NzLmVz