
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health , 15 May 2023
Sec. Aging and Public Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1113864
This article is part of the Research Topic Break the Mental Health Stigma: Loneliness View all 5 articles
 Basharat Hussain1*
Basharat Hussain1* Mahrukh Mirza1
Mahrukh Mirza1 Rebecca Baines1Lorna Burns1Sebastian Stevens2Sheena Asthana3,4,5
Rebecca Baines1Lorna Burns1Sebastian Stevens2Sheena Asthana3,4,5 Arunangsu Chatterjee4,6
Arunangsu Chatterjee4,6Introduction: Loneliness has significant impacts on the health of older adults. Social networks help to improve psychosocial and quality of life outcomes among older adults. A fifth of older adults live in rural communities, where geographic isolation poses challenges to health. The dynamics of social networks of older adults in rural communities has not been explored.
Objective: To synthesize the literature related to loneliness and social networks of older adults in rural settings.
Methods: A mixed-methods systematic review was conducted through searching six bibliographic databases to retrieve peer-reviewed literature with no time limits. We performed a methodological assessment of each study using a mixed method quality assessment tool. Findings are synthesized thematically.
Results: A total of 50 studies (32 quantitative, 15 qualitative, and 3 mixed methods) were included in this review. Studies were conducted in 17 different countries, the majority from China (n = 12), the UK (n = 9), and USA (n = 9). Findings revealed that social networks of older adults consist of family, friends and neighbors and continue to be developed through participation in various physical and social activities such as walking groups and participation in religious events. Social networks offer informational, functional, psychological and social support to older adults. Through their social networks, older adults feel socially connected and cared for. Successful interventions to improve social networks and address loneliness were those developed in groups or one-on-one with the older adults. The key ingredient to the positive impact of these interventions on reducing social isolation and loneliness was the formation of a social connection and regular engagement with the older adults. However, the review did not find any explicitly reported theory or model on which these interventions are based.
Conclusion: The prevalence of loneliness among older adults in rural areas needs urgent attention. Social network theory and methods can help in developing interventions to address social isolation and loneliness among older adults in rural communities.
Older adults living in rural communities experience challenges with their health and wellbeing. According to European Union, in 2018 there were 101 million older adults (aged 65 years or more) living in the EU and 20 % of these live in predominantly rural areas (1). The challenges for them are worse because of geographic and social isolation (2, 3).
Prevalence of loneliness among different population groups in the society is increasing to the extent that experts consider loneliness as a global public health epidemic (4, 5). A recent systematic review which is based on data from 113 countries found that a sizeable proportion of population experience loneliness globally (6). Surkalim et al. (6) review specifically noted that up to 6.5% of older adults in Northern European countries and upto 24.2% of older adults in Eastern European countries are experiencing loneliness. These findings are consistent with Bandari et al. (7) who noted that loneliness is more prevalence among older people. World Health Organization (WHO) identified that 20–34% older adults are lonely in some countries (8). Loneliness prevalence has exacerbated further during COVID-19 pandemic (9). A study based on 27 countries projected that the number of lonely adults aged ≥50 will increase from 105 million in 1990 to 333 million in 2050 in its sample countries alone (10). Abshire et al. (11) noted that owing to social isolation, ill health, and socioeconomic deprivation, older adults living in rural areas are at higher risk of experiencing loneliness.
Loneliness has adverse physical and mental health effects (6) compounded with social and economic implications. For example, loneliness is linked with feelings of deep sadness, disempowered and worthless (12). Loneliness is also negatively linked with self-esteem and sense of worth, increased vulnerability and risk for anxiety (13) and depressive symptoms (14). These aforementioned ill effects of loneliness further result in decline in cognitive functioning (15) which leads to poor quality of life (16) and may result in early mortality (17, 18). A systematic review conducted over a 25-year period reported loneliness in old age as a predictor of increased suicide ideations (19) which is supported by later studies (20, 21). Loneliness also effects physiological functioning (22) leading to increased risk of malnutrition (23).
It is reported that social networks play a pivotal role in health and wellbeing (24, 25) and perceptions of social isolation and loneliness (2, 25, 26). However, despite the importance of social networks to loneliness, limited research has examined these dynamics specifically in rural communities. Given the unique context of rural areas, both in terms of fostering social relationships and maintaining health and wellbeing, this mixed-method systematic review explored evidence of the impact of social networks on the loneliness of rural older adults. Key terms used in the review are explained in the literature as:
Loneliness is a perceived unpleasant feeling, which stems from a lack of desired social connections and inconsistency between expected and experienced strength of social relationships resulting in deficit of individual's social network (7). It is based on perceptions, evaluations and responses of one's interpersonal reality, and is expressed through the multifaceted interplay of behaviors, feelings and cognitions (27).
Social networks refer to the relationships, such as friendship and collaboration, between individuals and organizations (28). Social networks are composed of socially relevant nodes and ties. Nodes are network members (individuals and organizations) and ties are relations (family, friends, acquaintances, colleagues etc.) among them (29). A social network is a social structure depicting the connections that individuals and organizations form with one another.
It appears that social networks have been defined and studied in various ways, such as using the term social network (30) but also other related terms like social capital (31, 32), social connections (33), social support (34, 35) etc. However, core dimensions of these definitions convey meanings of social connectedness of an individual and receiving social and psychological support from these contacts. The number and types of contacts an individual has would reflect their social network size and structure. Perceived and received support (functional, psychological, and informational) determines the quality of any social network. Within the literature, social networks are also studied in terms of social isolation and loneliness (36, 37). For this review, social networks include all the aforementioned terms and aspects including any form of social connection, social support, social capital or inter-personal relationship of an older adult in rural areas.
Social connection is defined by structural (size of social network) and functional (intensity of social support) aspects of social life, and the quality of social relationships (satisfaction) (38). Social connection is the sense of belongingness, and of feeling connected, close, cared for and valued among family, friends and other social relations. It is an inherent human need and the basis of interpersonal relationships.
The United Nations defines older adults as persons over 60 years of age (39). In the UK, anyone over the age of 65 years is considered an older person (40). By convention, the stage of elderliness is defined according to chronological age. For example, people at age of 65 and above are referred as older adults; 65–74 years old as early older adult and those over 75 years as late older adult (41).
Categorization of areas as rural or urban is usually based on population density. For example, according to the UK Office for National Statistics (ONS) an area is referred as urban if it has a population of more than 10,000, land with a minimum area of 20 hectares (200,000 square meters), while settlements within 200 meters of each other are linked. All remaining areas are categorized as rural (42). The UN Statistical Commission distinguishes urban and rural areas based on population size and density. Rural areas consist of rural grid cells with a density below 300 inhabitants per km2. Rural areas have a population < 5,000 and at least 50% population living in rural grid cells (43). According to the US Census Bureau, an urban area has a population of at least 50,000 and a density of 500 people per square mile. All the remaining population, housing settlements and territory is defined as rural (44).
From these definitions it can be concluded that rural area has a population fewer than 5,000 and is less dense, has sparse population, low built in and is located at a distance from urban area.
Rural communities are small settlements which have a low population density with relative homogeneity and agriculture-related primary activities (45). People in rural communities are usually known to each other and generally have limited and poor access to social services like health, education and employment (46).
How do social networks impact the loneliness of older adults in rural communities?
From the identified literature on social networks and the loneliness of older adults in rural areas, the review also aims to address the following sub-questions:
• How older adults in rural areas form their social networks?
• What interventions are there, that address loneliness in older adults in rural communities?
• What social network theories or models have been used to develop social network interventions?
Ontologically, this review takes the stance of the existence of multiple perceptions and understandings about loneliness and social networks. In this view, feelings of loneliness and quality of social network are subjective realities and variable in different individual and cultural contexts.
Epistemologically, we take an interpretive position. We argue that loneliness and social networks are better understood through interpretive perspective rather than positivistic epistemology which has a narrow focus (47). Moreover, it is noted that healthcare practice is not just based on a positivistic view of the world, rather interpretation-based inquiry (such as narrative synthesis) could inform an holistic view of health, incorporating the feelings and experiences of individuals (48). We used a narrative approach which offers the flexibility of narrating evidence and insights from multiple types of studies (quantitative, qualitative and mixed methods). This is also helpful in building a holistic picture of the review topic, and answer what, how and why questions (49).
We developed a comprehensive search strategy and remained reflexive at all stages of the review. Reflexivity is helpful in identifying any biases and taking steps to address these.
This mixed methods review included quantitative and qualitative studies to answer the review questions. We used Daudt et al. (50) framework to select studies for this review. Following the database searches, two team members rigorously applied inclusion and exclusion criteria (BH, MM). For example, we only included studies clearly mentioning their setting (rural), focus (older adults) and studying loneliness and social network together. All included studies were analyzed at the same time and the findings were integrated. The findings of quantitative studies were narratively summarized and integrated with qualitative findings. In this way, the data were transformed according to the data-based convergent synthesis method described by Hong et al. (51) and manualised by the Joanna Briggs (52). The review team has expertise in undertaking various types of reviews and their reviews have been published in high ranked journals (e.g., BMJ Open, Vaccine). We also used team discussions and feedback meetings as a way to address reviewers bias during interpretations of findings from individual study as well as construction of themes.
The literature searches were conducted in January 2022 after an iterative development of the search strategy. We consulted an information specialist in development of the search strategy. The strategy comprised blocks of terms representing the concepts in the PICO and comprised subject headings and free text terms for each concept. PICO was structured as:
• Participants (P): older adults age 60 or over
• Phenomenon of Interest (I): social network and loneliness
• Context (CO): in rural community settings.
The following databases were searched: MEDLINE (Ovid), CINAHL (EBSCO), Embase (Ovid), PsycINFO, Scopus, SocINDEX (EBSCO). Full search histories are reported in Appendix A.
Studies were included if they reported primary research into social networks and loneliness of older adults, living in community in a rural setting. Older adults were defined as those aged 60 or over. Social networks included any form of social connection, social support, social capital, or inter-personal relationship. Any studies which described the setting as remote or rural were included even though these definitions differ by country. Studies from any country were included and we did not limit by date.
Studies were excluded if they did not report primary research, if the population was not older adults in a rural setting, and if they did not explore the relationship between social networks and loneliness. Studies were excluded if they were conducted on older adults in care settings (e.g., care home, hospital). Moreover, studies were excluded if they were not in the English language. Conference abstracts, dissertations, policy briefs or documents were excluded.
All references were exported into EndNote software and duplicates were removed. To reduce the risk of any bias influencing data extraction, as a pilot, two reviewers (BH and MM) independently reviewed the first 500 titles and abstracts. This was followed by a discussion to clarify the screening criteria and agree the decision making.
BH single screened all remaining references independently. Studies meeting the inclusion criteria mentioned above are included. Data were extracted on an Excel sheet for each included study. We extracted the following information from each study: authors, title, year, design, participants, setting, analysis, and findings (see Appendix B).
To report the quality of current evidence on the topic we undertook the quality assessment of the included studies. BH and MM assessed quality of studies using 2018 version of mixed methods appraisal tool (MMAT) for quality assessment of the studies (53). This tool was used because our systematic review included studies of mixed methods i.e., qualitative, quantitative and mixed methods. These reviewers independently assessed the quality of studies and any disagreement in the judgements of the two reviewers was addressed through discussion with the rest of the review team (see Appendix B). We decided not to exclude any study based on poor quality. This decision was taken because the evidence base on the topic is sparse. We did not undertake sensitivity analysis owing to mixed methods studies included in the review.
According to Hong et al. (51), there are two designs for synthesizing findings in narrative synthesis review: convergent and sequential. We used data-based convergent synthesis design and synthesized qualitative and quantitative evidence together. This helped us present insights on the topic together/coherently, rather in sequential way where qualitative and quantitative findings are presented separately. We used thematic narrative method to synthesize the findings. Firstly, findings from each study were inductively coded. Then, the resultant open codes and examples of excerpts were discussed with the review team before being collapsed into broader themes and synthesized narratively under each review theme (51).
The searches identified 36,156 records, which after de-duplication and title and abstract screening, left 79 records for full text retrieval. Following the full text eligibility screening, 29 reports were excluded, leaving 50 studies for inclusion in the synthesis (see Figure 1).
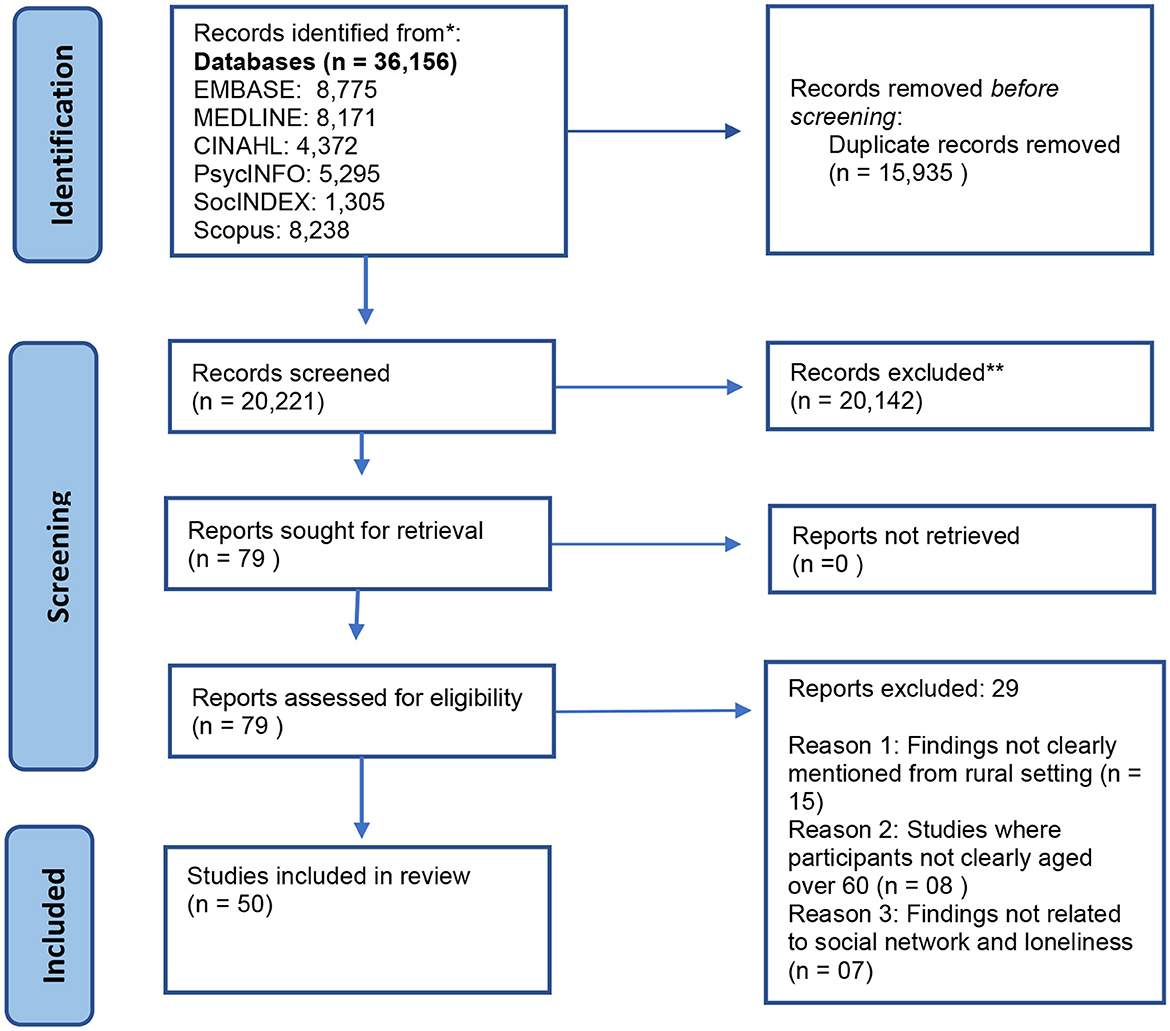
Figure 1. PRISMA flow chart.
In total this review identified 50 studies conducted across 17 countries as summarized in the chart below (Figure 2).

Figure 2. Number of studies from different countries.
Included studies used quantitative, qualitative, and mixed methods as summarized below:
- Quantitative n = 32
• Descriptive: n = 25
• Cross-sectional analytic study: n = 5
• Quantitative randomized trial: n = 1
• Quantitative non-randomized: n = 1
- Qualitative: n = 15
- Mixed Methods: n = 3
The majority of the studies included were of high quality, n = 25 studies were ranked as very good, n = 21 ranked as good while only n = 5 were of poor quality due to insufficient details about methods.
The review findings are reported into three main themes. These are explained below:
This theme is related to the development of social networks among older adults in rural areas. This theme is further divided into three sub-themes. Sub-themes are described below.
The review found that place is an important factor in determining social network of an older adult. Compared to urban areas, older adults in rural areas have more structural social support (35). The study measured structural social support for older adults on four items: (i) number of people who share similar interests and are known and have contact with? (ii) number of people known to an older adult to whom they meet or talk to during a week? (iii) How many friends do they have who can visit you in your home and feel “at home”? and (iv) How many people can you speak openly with?
The review found that older adults form primary social networks within their families (54). Spouses and adult children are important part of social networks and also sources of social support for the rural older adults (55, 56). Social interaction of older adults is mainly focused on family members (57), and in some cultures (such as Malays in Malaysia) along with immediate family members, relatives are also part of social network for older adults (56).
As with family contact, persons from rural areas are more likely to have social networks with the neighbors (56, 58). Such networks help to address the issue of loneliness in a better way because living on the same place can ignite a certain sense of belongingness with the place and the people. Neighborhood networks is especially common among older women living alone (59). This indicates that place is an important factor for determining the social network of an older adult. However, a study on social frailty among older adults found that older adults living in community setting in rural areas are lonelier than ones in assisted living facility (60).
Age is an important factor in developing or maintaining social network. It is found that older adults become lonelier with the increase in age (61, 62). Kivett (63) found that older rural adults are high risk for the loneliness according to a combination of physical and social losses that they had incurred. In China, depression and age were both significantly associated with loneliness in empty-nest older adults (64). Heenan (57) found that the majority (29) of their participants had experienced reduced social network and some degree of loneliness since becoming 65 years old.
Moreover, the marital status of a person is also an important factor in determining social network. It is found that single older adults have reduced social networks and feel lonelier (65, 66). As people age they loss valuable relations and contacts which make them more vulnerable. Arling (67) noted that widows living in rural areas have limited social network and are more prone to loneliness.
Having a spouse is the most long-term and strongest connection in family related social network in rural areas (55). However, when this connection is lost, widows suffer from loneliness (61, 63). Wenger (61) asserts that the widowed as a group in rural areas are lonelier than others because they do not overcome the trauma quickly and it becomes almost impossible to build new connections as they lose their interest in surroundings for a long period. These findings are confirmed by a more recent study by Jiang et al. (32) which measured Bonding Social Capital (BOC) and Bridging Social Capital (BRC) and evidenced that rural older adults widowed were significantly lower on BOC and BRC, and loneliness of rural participants was significantly associated with both BOC and BRC. Therefore, widows become more prone to loneliness as they get older.
For older adults in rural areas, expansion of social networks is achieved through participation in physical and social activities (68). These activities include participating in sports (31), community events and meetings (54). De Koning et al. (33) noted that physical activity can play role in developing new social contacts. In their study, older adult participants in the moderate-to-vigorous physical activity (MVPA) group reported several more sources of social contact compared to those with low physical activity group.
Expansion of social networks is hindered by various factors. These include decline in physical health (56) and disabilities (55, 69). Old age is another barrier that limits social participation as with older age people often experience onset of physical disabilities and chronic illnesses (69). Shergold (70) noted that older age and ill-health are barriers to weekly physical and social activity. These can both hinder the maintenance of an existing social network, and prevent it expanding further. This situation can result in experiencing loneliness, and loneliness itself reduces social participation (71), thus making quality of life for older adults even poorer. Participation in social and physical activities is also hampered by the lack of transportation (68), and fear of crimes (56). Shergold (70) noted that those with car access are up to three times more likely to participate in formal activity (OR 3.228; CI 1.656, 6.293), as compared to those without access to car. Limited access to a car means limited participation in social activities, thus reducing opportunities for expanding one's social network. These factors all contribute to the restriction of social interactions which would otherwise enhance the physical and mental health of older people.
One way to overcome physical disabilities and transport related barriers is the use of technology to get in touch with one's social contacts. Coffee et al. (34) noted that older adults use online socializing as a way to remain connected with their social networks, which was a useful means of communication during the COVID-19 pandemic. Berg et al. (72) support use of technology and consider information and communication technology as enabling connections between older adults and their social networks. Similarly, Willard et al. (73) regarded internet use as important for maintaining social contacts among older adults in rural areas. In using the internet, older adults can increase their online social contacts as well as maintain existing social networks (34, 73). Use of internet can also help the older adults to be exposed to new ideas and information which can help them to interact not only with the people from their age but also from other age groups.
This theme is related with the strength of social networks and their impact on loneliness of older adults in rural areas. It is further divided into two sub-themes: social impacts and, physio-psychological impacts.
Social networks play a vital role in establishing feelings of social connectedness among older adults, being able to talk and share thoughts, feel cared for, and supported, and creates a sense of belonging (68). Family is an important part of the social networks of an older adult, offering protection against loneliness (74). Family support also provides older adults with meaningful roles in their family, in turn contributing to their wellbeing, optimism and healthy behaviors (75). Older adults also rely upon family members to provide access to socializing opportunities (57). However, a lack, or absence of family support is significantly associated with loneliness, especially among “empty-nest” older adults in China (64). In addition, a lack of weekly activity with friends and family slightly increases the probability of the loneliness (OR 1.472; CI 0.877, 2.470) (70).
Besides family and friends related social networks, rural participants get support from their neighbors (56). Neighbors offer support in times of need (76), and support from neighbors had a significant positive effect on the older women living alone; as it helped to be able to maintain activities of daily living and brought an improvement in their health status (59). Social network with neighbors works as a coping strategy for loneliness too (34) as reiterated by Sánchez-Moreno et al. (77), where participation in neighborhood and religious groups reduced loneliness.
From the aformentioned studies, it is important to note that social networks offer different kinds of support to older adults. Li and Wang (35) study found that among different types of support, functional social support had a positive effect over loneliness. It is noted that engagement and participation of older adults is important in receiving social support. For example, relationships involving co-engagement were more likely to convey social support (i.e., emotional, instrumental, informational), companionship and social influence (encouragement of healthy behaviors) than relationships that do not involve co-engagement (30). One study (74) indicated that more social support offered protection against loneliness. Relatedly, the influence of living alone was negated by having a good social support system (78).
Moreover, frequent loneliness among older adults is found to be associated with their low participation in organized social activities (63). De Koning et al. (36) argue that volunteering, accompanying others and engaging in sports or exercise were associated with lower social isolation from neighbors, family, and friends. These findings are well-supported by a study conduted in Ireland (79) which noted the intersectionality between social relationships, place, work, health and quality of life among older women.
Similarly, social networks developed through modern technology such as the telephone also have an impact on the loneliness of older adults in rural areas. For example, participants in Hinck (80) study, described their typical day on how they made and received phone calls to deal with loneliness. Participants took an active role in communicating with others by telephoning (80), and a relatively new study by Evans et al. (56) suggested telephone use strengthens social support.
A decline in social relationships and social support led to a higher level of depressive symptoms and low level in quality-of-life scores (69, 81). It is also found that social support partially act as a mediator for depression (82), and those with self-reported depression had significantly higher levels of loneliness (83).
The perceived social support was positively correlated with psychological resilience (84). The study by Hinck (80) supports Yue et al. (84) reporting subjective life experiences of participants highlighting how positive memories of those past experiences strengthened their psychological resilience and have helped them in coping with loneliness (80). Along with memories, there are some other factors like self-confidence, self-worth, and perceived respect which may have an effect on an individual's psychological resilience (85). Van der Geest (85) propose that damage to one's notion of perceived respect toward themselves constitutes an experience of loneliness in older adults. With aging, people tend to become more sensitive about being listened to or given opportunity to impart wisdom and advice to younger people. However, in Van der Geest (85) study, the older adults reported feeling unheard, and a lack of respect. This affected their psychological state and the relationship between the social support they receive and their feelings of loneliness.
As people age, they have reduced social networks and consequently they feel loneliness (61, 63). Lack of social networks results in social isolation and detachment from society (54). A detached older person feels no attachment or lacks a sense of belongingness with the larger group; which results into lower emotional support and is correlated with depression and higher loneliness scores among older adults (86). Higher loneliness in turn results in lower engagement in activities particularly self-care, leisure, and socializing (83).
Coffee et al. (34) viewed increasing social networks in the community as a strategy to cope with loneliness of older adults in rural areas. From their study, De Koning et al. (33) posit that being socially active helps in staying mentally well. There is evidence that any opportunity for social interaction would help reduce loneliness among older adults (87).
Moreover, having poor social network and feeling socially isolated is linked with malnutrition among older adults (37). In another interesting study, it is found that poor social network and feelings of loneliness leads to admission in nursing homes for older adults in rural areas (88).
The review identified a variety of interventions to address loneliness among older people, based on their differing purpose, underlying mechanisms for action and expected outcomes. The purpose of the interventions included: increasing physical activity and social connectedness of older adults (68), enhancing social participation (89, 90), building social capital and friendship (31), mediating loneliness and perceived stress among older people (91), enhancing connectedness, informal care giving and local participation (73), improving general mental health, nutritional status, satisfaction with life, and social capital (92) tackling social isolation and loneliness (58, 93–95).
This theme is further divided in three sub-themes. The description of sub-themes is given below.
These interventions offered range of social and educational activities to the older adults. For example, in the UK, a village services project offered six community-based services and activities that provided help to meet the needs of older rural residents in three regions of England (95). The services include: (i). Warden service- Community wardens giving emotional and practical support to housebound/lonely, bereaved and convalescing older adults, (ii). Lunch club—A parish center lunch club, part of a county-wide initiative to grow community self-help networks, (iii). Welfare rights—A dedicated worker helping older residents of rural villages in former mining communities access benefit entitlements, (iv). Befriending—Two linked befriending services providing a regular social visit for lonely, isolated clients in their own homes, (v). Information and advice Service—offering information and advice on benefits and services to older adults in dispersed rural areas, including a dedicated worker to visit older adults in their homes to help clients access benefit entitlements, (vi) Lunch club/mobile care service—Transport to a regular social event/meal combined with the delivery of mobile hand, foot and hair care to older people living in remote rural settings.
Likewise, a befriending intervention (58) and the Young at Heart group (57) are both Ireland-based interventions. The befriending intervention administered a weekly home visiting service led by volunteer befrienders intending to facilitate social interaction as well as community-based social groups, activities and outings among the befrienders and befriendees (58). The Young at Heart group is a community-based initiative started in 2008 in Northern Ireland (57). The group aimed to identify needs of local older adults in a participatory way and meet the identified needs. The group identified that older adults need opportunities to socialize, develop skills and obtain information. The group organized various activities for older adults including tea-dances, whist-drives, health information, social security information, local history talks and events, storytelling, outings, information technology & transport, and opportunities for networking with other groups. Similarly, another intervention from China known as Community Canteen offered the opportunity for rural older adults to eat lunch and dinner together each day (92).
Furthermore, online assistance and interventions have also been tested. These interventions are beneficial in resolving major hindrance on the way of generating social support (68), and other physical disabilities (69). In Netherlands, an online community care platform called as “Grubbenvorst-Online” offered apps to older adults living in rural area of Grubbenvorst (73). These apps offered a matching tool for informal care where users could exchange informal help, a local calendar on local events and activities, and social services in which users could find information about available care services and organizations.
Apart from massive interventions, for two different interventions driven-game shooting (31) and Community Canteen Service (92) noted statistically significant, positive impact on mental health and wellbeing, and social capital of the participants where social capital of the Canteen Group was better than the Non-Canteen Group along with improvements in life satisfaction. Latham-Green et al. (31) claimed that the intervention created social impact via social capital creation and identity reinforcement.
The Educational Program for Social Participation in Iran delivered 5 weeks long weekly 60–80 min educational sessions to older adults for encouraging them to increase their social participation and activities in the society (89). This program noted significant improvement in loneliness feeling scores of the intervention group from 62.24 ± 0.7.53 to 28.86 ± 6.88 (P < 0.001), however, the control group experienced no significant changes in feelings of loneliness scores (89).
A variety of psychological interventions to tackle loneliness among older adults have been carried out. In China, Chinese Traditional Festival Activities based Group Reminiscence Therapy (CTFA-GRT) was a psychological health promotion program for older adults (91). This program integrated the situational memories of group reminiscence therapy into traditional Chinese festival activities, making it easier to help older adults living alone find a theme of common reminiscence. These are a series of days based on international celebrations and religious events such as International Women's Day (Enhance positive experience), Mother's Day (Recall maternal love), Chinese Valentine's Day (Let go and feel loved).
A social prescribing pilot project for older adults in rural area of South Korea during COVID-19 pandemic offered weekly 10 weeks interventions including music storytelling, a self-help group, gardening, and COVID-19 prevention in 2020 (90). These interventions contributed positively to psychological wellbeing of the older adults by increasing the social connections of older adults and reducing their loneliness.
Moreover, many of these activities were group-based and implemented in different societies across the globe. For example, Active Aging Program—a community health promotion program in British Columbia (Canada) offered walking groups, Garden Club activities, swim programs, Tai Chi, peer support, bee garden, meals, carpet bowling, language education, tea socials, outings by bus, community meals and mobility clinics (68). These activities were contextualized to meet the needs of local populations across British Columbia.
Three interventions: Social Prescribing Intervention, Education Program for Social Participation, and Active Aging Program all found that social participation scores increased for the sample that received these interventions. And it is noteworthy that these studies were conducted in different countries yet achieved the same outcomes such that, social participation scores increased as a result of these interventions (68, 89, 90). The social prescribing intervention resulted in an increase in the social participation attitude score. Although the average score of self-efficacy increased, it was not statistically significant (90). Pearce and Lillyman (94) found that self-worth levels increased with social connections. The Active Aging Program found that older adults through participation in different activities developed social connections, had opportunity to talk and share their thoughts, felt cared for and created a sense of belongingness (68).
Along with improved social participation scores, a positive effect on loneliness was also noted as a result of these interventions. The Social prescribing intervention provided positive outcomes in terms of loneliness (90) such that, loneliness was reduced significantly, while self-esteem increased significantly (94) and depression was also noted to get reduced considerably. The Chinese Traditional Festival Activities and based on Group Reminiscence Therapy (CTFA-GRT) also noted positive outcomes for the participants for the perceived stress and loneliness of rural older adults living alone in the intervention group (91). Combined with a simple effects test, the PSS and UCLA-LS of those in the intervention groups significantly decreased at 8 months after the baseline (91). In addition, the sustainable effect of this program lasted 3 months after the intervention (91). Therefore, it can be said that these interventions not only reduced loneliness in its participants, but reduced loneliness sustained for next 3 months outside the intervention (91).
Many interventions used different activities, hobbies, and sports for older adults to connect with each other during these social engagements (31, 58, 90). For example, Bantry-White et al. (58) promoted similarities between group members who shared the rural areas and called it a befriending intervention. By sharing a common history that they co-constructed by using local old photographs and poetry they created a sense of attachment among them that let befrienders and befriended developed friendships and connections through activities such as knitting, baking, bingo, dancing, and gardening. Similarly, Driven Game Shooting in England offered regular involvement of older adults in a rural and countryside sport (31).
Art is a stated means to promote expression and discourage feelings of loneliness (93, 94). MacLeod et al. (93) claimed intervening through arts is a quality effort. In the UK context, an art program implemented creative arts projects named “Extend,” “My Story,” “The Rural Pub Arts Hub” to reduce loneliness among older adults in rural part of Hertford (94). Extend—offered dance sessions involving gentle chair-based exercises to music and are aimed to teach techniques to prevent falls and improve mobility, balance, and independence. My Story was a reminiscence project that captures the stories of older adults on film. The films provided insights into the lives of those involved and enable deeper relationships to develop between the day care staff, families and older adults as conversations arise from the previously unknown stories and interests. The Rural Pub Arts Hub project held accessible beginners' art classes for the over-sixties in rural pubs. The sessions ran over 10 weeks and were led by local artists who introduce painting with watercolor, drawing with watercolor pencils and water-soluble fiber tip pens. Each class worked toward creating a mural, as well as working on collages, stitched imagery and mark-making, and each participant created their own artist's book.
A second art based intervention program from Canada called “Seniors Connecting with Seniors through Expressive Arts Making”—consisted of in-home volunteer-based expressive arts (93). In this intervention, older adult volunteers were matched one-to-one with eight socially isolated older adults to conduct in-home, individual, intermodal art making activities in their dyads over 10 sessions. Among others, these volunteers were retired artists, teachers, and nurses.
Our review finds that family, friends, and neighbors are important sources for developing social network for older adults in rural areas. These social networks are developed through living in a particular area as well as through participation in various physical and social activities. Older adults receive informational, functional, psychological, and social support from their social network. Having good social network generates feelings of being socially connected and valued among the older adults. Our review also found that loneliness of older adults in rural areas can be reduced through group as well as one to one interventions. These findings are similar to other systematic reviews (96–98). Characteristics of effective interventions included their adaptability to the local and individual context, a community development approach, and productive engagement with older adults (99). However, it is also important to remain cautious as there is no one-size-fits-all approach to address loneliness among older adults; therefore, it is important to tailor interventions in a way that suit the needs of individual older adults, specific population groups of older adults and the extent of loneliness being experienced (100). Although our review noted that video calls and online forums helped to reduce loneliness, a robust literature review suggested that there is uncertainty in the evidence to support that video calls are helpful in addressing loneliness among older adults (101).
Caution is also needed in making assumptions that older adults with weak social ties utilize more health services (including physician visits and community- or home-based services) than required by their actual needs (102).
Our review identified that causes of loneliness among older adults in rural areas are varied (103). Marital status, loss of spouse, health issues, limited social network and low level of physical and social activity can all cause loneliness among older adults in rural areas. These risk factors for loneliness are similar to a recent review undertaken to identify longitudinal risk factors for loneliness among older adults in the UK (104) and Europe broadly (105). In our review, we also identify that age is an important social variable associated with loneliness. We identified that loneliness can increase with age suggesting that older adults are more likely to feel lonely. These findings are similar to a 24 years longitudinal study conducted in the UK (106).
A number of theories have been proposed to explain the cause of loneliness (e.g., the existential, the cognitive, the psychodynamic and the interactionist) (107). However, to our knowledge none of the studies have used social network theory to explain causes of loneliness. In our view social network theory can be very helpful in explaining loneliness among older adults living in rural areas (108).
In addressing loneliness, our review suggests that the interventions that develop and/or strengthen existing social networks of the older adults are helpful (99). The exact mechanism through which social networks influence health (109) or specifically reduce loneliness is still unknown (31). However, the underlying mechanism relating to positive influence of social network on loneliness could be due to mainly two reasons:
Firstly, a social network offers opportunity for the older adults to participate in physical and social activities and remain engaged (110). This shifts the cognitive thinking process of older adults toward social activities, rather than their loneliness. The mind of older adults remains preoccupied in social activities and this prevents developing feelings of loneliness (110, 111). It is considered that regular engagement in physical activity, remaining in touch with family contacts and social participation decreases physiological distress among older adults (112).
Secondly, having social network gives feeling of social connectedness to older adults (113). It is identified that these feelings of connectedness with other and to a community or neighborhood contributes to wellbeing of older adults (114). Older adults trust their social surroundings and feel less anxious (115). This develops an environment of reciprocity and feelings of physical, psychological, and social security for the older adults. An older person can get information, emotional, and psychosocial support, and hope that in time of need, support from social connections would be available. Feeling secure and being in a reciprocal relationship reduces social isolation and loneliness (116). In parallel to a recent rigorous study on social network and mental health (117), our review also underlines the need to address the subjective factors of social isolation (such as feelings of loneliness) and objective factors of social isolation (such as social network size) in a complementary way to achieve the goal of improving mental health of the older adults.
Our review identified important evidence gaps in the topic of our interest. A range of terms were used in the reviewed literature to convey the meanings of social network (108). These terminologies include social connections, social support, social capital etc. The use of an agreed upon definition of social network in healthcare research would help in enhancing credibility of the evidence.
Methodologically, we observed that there is gap in the use of social network specific methods and techniques in healthcare research (118). If we intend to understand the concept of social networks in healthcare, Social network specific methods and techniques must be used in undertaking studies (119).
Loneliness among older adults can result in poor health and wellbeing including cognitive impairments such as dementia (120). Therefore, there is an urgent need to generate evidence regarding the mechanisms through which social networks reduce loneliness of older adults in rural areas (119). Studies on this topic need to be robust and conducted in different cultural contexts (121). Studies related to social network and loneliness of older adults from minority population groups such as minority ethnic background living in rural areas of developed world are also needed (122).
Our review included studies with different study designs including, quantitative qualitative and mixed methods, however most studies used different tools to assess social support, loneliness and sample sizes varied across different studies this made synthesize of the data challenge. We included few interventional studies to address loneliness and showed positive benefits of the intervention in reducing loneliness and promoting social participation, however, the sample sizes were very low in these studies. The majority of the studies included were of high and, very good.
Most of the studies were conducted in China, USA and UK with only two studies from other continents such as Africa. Therefore, the evidence from this review may not be generalisable to all countries.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This work was supported by the Healthy Ageing Through Innovation in Rural Europe project, which was partly funded by the Interreg 2 Seas Mers Zeeën (Project no. 2S07-004), European Regional Development Fund.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1113864/full#supplementary-material
1. Augere-Granier M-L, Mceldowney J. Older People in the European Union's Rural Areas: Issues and Challenges. Brussels: European Union (2020). doi: 10.2861/114962
2. Henning-Smith C, Evenson A, Kozhimannil K, Moscovice I. Geographic variation in transportation concerns and adaptations to travel-limiting health conditions in the United States. J Transport Health. (2018) 8:137–45. doi: 10.1016/j.jth.2017.11.146
3. Whitacre BE, Wheeler D, Landgraf C. What can the national broadband map tell us about the health care connectivity gap? J Rural Health. (2017) 33:284–9. doi: 10.1111/jrh.12177
4. Hunter D. Loneliness: a public health issue. Perspect Public Health. (2012) 132:153. doi: 10.1177/1757913912449564
6. Surkalim DL, Luo M, Eres R, Gebel K, van Buskirk J, Bauman A, et al. The prevalence of loneliness across 113 countries: systematic review and meta-analysis. BMJ. (2022) 376:e067068. doi: 10.1136/bmj-2021-067068
7. Bandari R, Khankeh HR, Shahboulaghi FM, Ebadi A, Keshtkar AA, Montazeri A. Defining loneliness in older adults: protocol for a systematic review. Syst Rev. (2019) 8:1–6. doi: 10.1186/s13643-018-0935-y
8. WHO. Social Isolation and Loneliness Among Older People: Advocacy Brief. (2021). Available online at: https://www.who.int/publications/i/item/9789240030749 (accessed April 09, 2023).
9. Su Y, Rao W, Li M, Caron G, D'Arcy C, Meng X. Prevalence of loneliness and social isolation among older adults during the COVID-19 pandemic: a systematic review and meta-analysis. Int Psychogeriatr. (2022) 24:1–13. doi: 10.1017/S1041610222000199
10. Newmyer L, Verdery AM, Wang H, Margolis R. Population aging, demographic metabolism, and the rising tide of late middle age to older adult loneliness around the world. Populat Develop Rev. (2022) 48:829–62. doi: 10.1111/padr
11. Abshire DA, Graves JM, Amiri S, Williams-Gilbert W. Differences in loneliness across the rural-urban continuum among adults living in Washington State. J Rural Health. (2022) 38:187–93. doi: 10.1111/jrh.12535
12. Moeyersons M, De Vliegher K, Huyghe B, De Groof S, Milisen K, de Casterlé BD. ‘Living in a shrinking world'—the experience of loneliness among community-dwelling older people with reduced mobility: a qualitative grounded theory approach. BMC Geriatr. (2022) 22:285. doi: 10.1186/s12877-022-02998-5
13. Sandu V, Zólyomi E, Leichsenring K. Addressing loneliness and social isolation among older people in Europe. Policy Brief. (2021) 1–16.
14. Van Beljouw IM, van Exel E, de Jong Gierveld J, Comijs HC, Heerings M, Stek ML, et al. “Being all alone makes me sad”: loneliness in older adults with depressive symptoms. Int Psychogeriatr. (2014) 26:1541–51. doi: 10.1017/S1041610214000581
15. Donovan NJ, Wu Q, Rentz DM, Sperling RA, Marshall GA, Glymour MM. Loneliness, depression and cognitive function in older US adults. Int J Geriatr Psychiatry. (2017) 32:564–73. doi: 10.1002/gps.4495
16. Musich S, Wang SS, Hawkins K, Yeh CS. The impact of loneliness on quality of life and patient satisfaction among older, sicker adults. Gerontol Geriatr Med. (2015) 1:1–9. doi: 10.1177/2333721415582119
17. Henriksen J, Larsen ER, Mattisson C, Andersson NW. Loneliness, health and mortality. Epidemiol Psychiatr Sci. (2019) 28:234–9. doi: 10.1017/S2045796017000580
18. Beller J. Loneliness and mortality: the moderating effect of positive affect. Appl Psychol Health Wellbeing. (2023) 15:49–65. doi: 10.1111/aphw.12354
19. Mezuk B, Rock A, Lohman MC, Choi M. Suicide risk in long-term care facilities: a systematic review. Int J Geriatr Psychiatry. (2014) 29:1198–211. doi: 10.1002/gps.4142
20. Chang Q, Chan CH, Yip PS. A meta-analytic review on social relationships and suicidal ideation among older adults. Soc Sci Med. (2017) 191:65–76. doi: 10.1016/j.socscimed.2017.09.003
21. Heuser C, Howe J. The relation between social isolation and increasing suicide rates in the elderly. Qual Ageing Older Adults. (2019) 20:2–9. doi: 10.1108/QAOA-06-2018-0026
22. Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med. (2010) 40:218–27. doi: 10.1007/s12160-010-9210-8
23. Ramic E, Pranjic N, Batic-Mujanovic O, Karic E, Alibasic E, Alic A. The effect of loneliness on malnutrition in elderly population. Med Arch. (2011) 65:92.
24. Montgomery SC, Donnelly M, Bhatnagar P, Carlin A, Kee F, Hunter RF. Peer social network processes and adolescent health behaviors: a systematic review. Prev Med. (2020) 130:105900. doi: 10.1016/j.ypmed.2019.105900
25. Latkin CA, Knowlton AR. Social network assessments and interventions for health behavior change: a critical review. Behav Med. (2015) 41:90–7. doi: 10.1080/08964289.2015.1034645
26. Harasemiw O, Newall N, Shooshtari S, Mackenzie C, Menec V. From social integration to social isolation: the relationship between social network types and perceived availability of social support in a national sample of older Canadians. Res Aging. (2018) 40:715–39. doi: 10.1177/0164027517734587
27. Motta V. Key concept: loneliness. Philos Psychiatry Psychol. (2021) 28:71–81. doi: 10.1353/ppp.2021.0012
28. Snijders TA. The statistical evaluation of social network dynamics. Sociol Methodol. (2001) 31:361–95. doi: 10.1111/0081-1750.00099
29. Marin A, Wellman B. Social network analysis: an introduction. SAGE Handb Soc Netw Anal. (2011) 11:25. doi: 10.4135/9781446294413.n2
30. Ashida S, Sewell DK, Schafer EJ, Schroer A, Friberg J. Social network members who engage in activities with older adults: do they bring more social benefits than other members? Ageing Soc. (2019) 39:1050–69. doi: 10.1017/S0144686X17001490
31. Latham-Green T, Hazenberg R, Denny S. Examining the role of driven-game shooting as a psycho-social resource for older adults in rural areas: a mixed-methods study. Ageing Soc. (2021) 43:902–28. doi: 10.1017/S0144686X2100091X
32. Jiang D, Hou Y, Hao J, Zhou J, Jiang J, Wang Q. Association between personal social capital and loneliness among widowed older people. Int J Environ Res Public Health. (2020) 17:1–11. doi: 10.3390/ijerph17165799
33. De Koning J, Richards SH, Wood GER, Stathi A. Profiles of loneliness and social isolation in physically active and inactive older adults in rural England. Int J Environ Res Public Health. (2021) 18:3971. doi: 10.3390/ijerph18083971
34. Coffee P, Ryde G, Swales B, Neely K, Connelly J, Kirkland A, et al. Loneliness, wellbeing, and social activity in scottish older adults resulting from social distancing during the COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:4517. doi: 10.3390/ijerph18094517
35. Li H, Wang C. The relationships among structural social support, functional social support, and loneliness in older adults: analysis of regional differences based on a multigroup structural equation model. Front Psychol. (2021) 12:732173. doi: 10.3389/fpsyg.2021.732173
36. De Koning J, Richards S, Stathi A. Loneliness, social isolation, and objectively measured physical activity in rural-living older adults. J Aging Phys Act. (2020) 28:467–77. doi: 10.1123/japa.2019-0027
37. Boulos C, Salameh P, Barberger-Gateau P. Social isolation and risk for malnutrition among older people. Geriatr Gerontol Int. (2017) 17:286–94. doi: 10.1111/ggi.12711
38. Holt-Lunstad J. The major health implications of social connection. Curr Dir Psychol Sci. (2021) 30:251–9. doi: 10.1177/0963721421999630
39. UNHCR UN Refugee Agency. Older Persons. (2023). Available online at: https://emergency.unhcr.org/entry/43935/older-persons#:~:text=An%20older%20person%20is%20defined,or%20age%2Drelated%20health%20conditions (accessed March 14, 2023).
40. ONS. Profile of older people living in England and Wales. (2021). Available online at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/ageing/articles/profileoftheolderpopulationlivinginenglandandwalesin2021andchangessince2011/2023-04-03#:~:text=The%20majority%20of%20people%20aged%2065%20years%20or%20over%20in,aged%2085%20years%20and%20over (accessed March 23, 2023).
41. Orimo H, Ito H, Suzuki T, Araki A, Hosoi T, Sawabe M. Reviewing the definition of “elderly”. Geriatr Gerontol Int. (2006) 6:149–58. doi: 10.1111/j.1447-0594.2006.00341.x
42. ONS. 2011 Rural/Urban Classification. (2016). Available online at: https://www.ons.gov.uk/methodology/geography/geographicalproducts/ruralurbanclassifications/2011ruralurbanclassification (accessed March 14, 2023).
43. UN Statistical Commission. A Recommendation on the Method to Delineate Cities, Urban Rural Areas for International Statistical Comparisons. (2020). Available online at: https://unstats.un.org/unsd/statcom/51st-session/documents/BG-Item3j-Recommendation-E.pdf (accessed March 14, 2023).
44. Ratcliffe M, Burd C, Holder K, Fields A. Defining rural at the US Census Bureau. Am Community Survey Geogr Brief. (2016) 1:1–8.
45. Scott J, Marshall G. (eds.). A Dictionary of Sociology. London: Oxford University Press. (2009). doi: 10.1093/acref/9780199533008.001.0001
46. Curtin L. Overview of Rural Communities: Context, Challenges Resilience. (2015). Available online at: https://www.apa.org/pi/aids/resources/exchange/2015/01/rural-communities (accessed March 16, 2023).
47. Greenhalgh T, Thorne S, Malterud K. Time to challenge the spurious hierarchy of systematic over narrative reviews? Eur J Clin Invest. (2018) 48:e12931. doi: 10.1111/eci.12931
48. Malterud K. The art and science of clinical knowledge: evidence beyond measures and numbers. Lancet. (2001) 358:397–400. doi: 10.1016/S0140-6736(01)05548-9
49. Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews. Product ESRC Methods Programme Version. (2006) 1:b92.
50. Daudt HM, van Mossel C, Scott SJ. Enhancing the scoping study methodology: a large, inter-professional team's experience with Arksey and O'Malley's framework. BMC Med Res Methodol. (2013) 13:48. doi: 10.1186/1471-2288-13-48
51. Hong QN, Pluye P, Bujold M, Wassef M. Convergent and sequential synthesis designs: implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst Rev. (2017) 6:1–14. doi: 10.1186/s13643-017-0454-2
52. Stern C, Lizarondo L, Carrier J, Godfrey C, Rieger K, Salmond S, et al. Methodological guidance for the conduct of mixed methods systematic reviews. JBI Evid Synth. (2020) 18:2108–18. doi: 10.11124/JBISRIR-D-19-00169
53. Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed methods appraisal tool (MMAT), version (2018). Registr Copyright. (2018) 34:285–91. doi: 10.3233/EFI-180221
54. Conkova N, Vullnetari J, King R, Fokkema T, Warren-Findlow J. “left Like Stones in the middle of the Road”: narratives of Aging Alone and Coping Strategies in Rural Albania and Bulgaria. J Gerontol Ser B Psychol Sci Soc Sci. (2019) 74:1492–500. doi: 10.1093/geronb/gby127
55. Wang G, Hu M, Xiao S-Y, Zhou L. Loneliness and depression among rural empty-nest elderly adults in Liuyang, China: a cross-sectional study. BMJ Open. (2017) 7:e016091. doi: 10.1136/bmjopen-2017-016091
56. Evans N, imelda JD, allotey P, Reidpath DD, Pool. R. Social support and care arrangements of older people living alone in rural Malaysia. Ageing Soc. (2018) 38:2061–81. doi: 10.1017/S0144686X17000472
57. Heenan D. How local interventions can build capacity to address social isolation in dispersed rural communities: a case study from Northern Ireland. Ageing Int. (2011) 36:475–91. doi: 10.1007/s12126-010-9095-7
58. Bantry-White E, O'sullivan S, O'connell C, Kenny L. The symbolic representation of community in social isolation and loneliness among older people: insights for intervention from a rural Irish case study. Health Soc Care Community. (2018) 26:e552–9. doi: 10.1111/hsc.12569
59. Saito E, Sagawa Y, Kanagawa K. Social support as a predictor of health status among older adults living alone in Japan. Nurs Health Sci. (2005) 7:29–36. doi: 10.1111/j.1442-2018.2005.00220.x
60. Bunt S, Steverink N, Douma L, Van Der Schans C, Hobbelen H, Meijering L. Experiences of social frailty among rural community-dwelling and assisted-living older adults: a qualitative study. Ageing Soc. (2021) 43:857–77. doi: 10.1017/S0144686X21000830
61. Wenger GC. Adapting to old age in rural Britain. Int J Aging Hum Dev. (1984) 19:287–99. doi: 10.2190/QXH5-Y7AU-9UVG-6AKN
62. Feng Z, Phillips DR, Jones K. A geographical multivariable multilevel analysis of social exclusion among older people in China: evidence from the China Longitudinal Aging Social Survey ageing study. Geogr J. (2018) 184:413–28. doi: 10.1111/geoj.12274
63. Kivett VR. Discriminators of loneliness among the rural elderly: implications for intervention. Gerontologist. (1979) 19:108–15. doi: 10.1093/geront/19.1.108
64. Cheng P, Jin Y, Sun H, Tang Z, Zhang C, Chen Y, et al. Disparities in prevalence and risk indicators of loneliness between rural empty nest and non-empty nest older adults in Chizhou, China. Geriatr Gerontol Int. (2015) 15:356–64. doi: 10.1111/ggi.12277
65. Liu L-J, Guo Q. Loneliness and health-related quality of life for the empty nest elderly in the rural area of a mountainous county in China. Qual Life Res. (2007) 16:1275–80. doi: 10.1007/s11136-007-9250-0
66. Wu ZQ, Sun L, Sun YH, Zhang XJ, Tao FB, Cui GH. Correlation between loneliness and social relationship among empty nest elderly in Anhui rural area, China. Aging Mental Health. (2010) 14:108–12. doi: 10.1080/13607860903228796
67. Arling G. Resistance to isolation among elderly widows. Int J Aging Hum Dev. (1976) 7:67–86. doi: 10.2190/EC9P-7E6B-3BHD-LVA7
68. Franke T, Sims-Gould J, Lusina-Furst S, Mckay H. “I didn't think i needed it. But I find I look forward to it very much”: social connectedness and physical health through the eyes of older adults. Activit Adapt Aging. (2020) 46:9–30. doi: 10.1080/01924788.2020.1845586
69. Cerhan JR, Wallace RB. Predictors of decline in social relationships in the rural elderly. Am J Epidemiol. (1993) 137:870–80. doi: 10.1093/oxfordjournals.aje.a116748
70. Shergold I. Taking part in activities, an exploration of the role of discretionary travel in older people's wellbeing. J Transport Health. (2019) 12:195–205. doi: 10.1016/j.jth.2019.01.005
71. Çam C, Atay E, Aygar H, Öcal EE, Önsüz MF, Işikli B, et al. Elderly people's quality of life in rural areas of turkey and its relationship with loneliness and sociodemographic characteristics. Psychogeriatrics. (2021) 21:795–804. doi: 10.1111/psyg.12741
72. Berg T, Winterton R, Warburton J, Petersen M. 'Although we're isolated, we're not really isolated': the value of information and communication technology for older people in rural Australia. Australas J Ageing. (2017) 36:313–7. doi: 10.1111/ajag.12449
73. Willard S, Van Rossum E, Spreeuwenberg M, De Witte L. Perceived impact of an online community care platform for Dutch older adults on local participation, informal caregiving, and feelings of connectedness: pretest-posttest observational study. J Med Internet Res. (2020) 22:e20304. doi: 10.2196/20304
74. Wang G, Wang K, Li Y, Zhang X, Shen Q, Ge X, et al. Loneliness among the rural older people in Anhui, China: prevalence and associated factors. Int J Geriatr Psychiatry. (2011) 26:1162–8. doi: 10.1002/gps.2656
75. Lewis J. The role of the social engagement in the definition of successful ageing among Alaska native elders in Bristol Bay, Alaska. Psychol Dev Soc J. (2014) 26:263–90. doi: 10.1177/0971333614549143
76. Buys L, Burton L, Cuthill M, Hogan A, Wilson B, Baker D. Establishing and maintaining social connectivity: an understanding of the lived experiences of older adults residing in regional and rural communities. Aust J Rural Health. (2015) 23:291–4. doi: 10.1111/ajr.12196
77. Sánchez-Moreno E, Gallardo-Peralta LP, Leyton C. The social gradient in mental health and well-being for indigenous older adults living in rural areas: a cross-sectional comparison with rural non-indigenous population in Chile. J Aging Health. (2021) 33:287–99. doi: 10.1177/0898264320979201
78. Fukunaga R, Koyama A, Fujise N, Ikeda M, Abe Y, Nakagawa Y. Living alone is associated with depression among the elderly in a rural community in Japan. Psychogeriatrics. (2012) 12:179–85. doi: 10.1111/j.1479-8301.2012.00402.x
79. Herbert A. How ageing and quality of life is influenced by social relationships: an exploration of Rural Midlife Women in Ireland. Soc Stud. (2018) 15:45–64. doi: 10.5817/SOC2018-1-45
80. Hinck SM. The Lived Experience of Oldest-Old Rural Adults. St. Louis, MO: Saint Louis University (2002).
81. Liu Y, Qu Z, Meng Z, Wang S. Relationship between loneliness and quality of life in elderly empty nesters from the Wolong Panda Nature Reserve in Sichuan province, China, from the perspective of Rural Population and Social Sustainability. Phys A Stat Mech Applic. (2020) 551:124154. doi: 10.1016/j.physa.2020.124154
82. Wan Mohd Azam WMY, Din NC, Ahmad M, Ghazali SE, Ibrahim N, Said Z, et al. Loneliness and depression among the elderly in an agricultural settlement: mediating effects of social support. Asia-Pac Psychiatry. (2013) 5:134–9. doi: 10.1111/appy.12061
83. Garabrant AA, Liu C-J. Loneliness and activity engagement among rural homebound older adults with and without self-reported depression. Am J Occup Ther. (2021) 75:1–9. doi: 10.5014/ajot.2021.043828
84. Yue L, Lin H, Qin L, Gui-Zhen Q, Huan Z, Shan Z. Moderating effect of psychological resilience on the perceived social support and loneliness in the left-behind elderly in rural areas. Front Nurs. (2021) 8:357–63. doi: 10.2478/fon-2021-0035
85. Van der Geest S. Dying peacefully: considering good death and bad death in Kwahu-Tafo, Ghana. Soc Sci Med. (2004) 58:899–911. doi: 10.1016/j.socscimed.2003.10.041
86. Theeke LA, Goins RT, Moore J, Campbell H. Loneliness, depression, social support, and quality of life in older chronically ill Appalachians. J Psychol Interdiscipl Appl. (2012) 146:155–71. doi: 10.1080/00223980.2011.609571
87. Roos V, Kahl C, Keating N. Loneliness of older black South African women subjected to forcible relocation. Glob Health Action. (2019) 12:1672329. doi: 10.1080/16549716.2019.1672329
88. Cutrona CE, de la Mora A, Wallace RB, Russell DW. Loneliness and nursing home admission among rural older adults. Psychol Aging. (1997) 12:574–89. doi: 10.1037/0882-7974.12.4.574
89. Nazari M, Jokar F, Fararooei M, Kaveh MH. The effectiveness of social participation educational program on the feeling of loneliness of elderly people in rural areas of Baiza City (South of Fars Province). J Health Sci Surveill Syst. (2021) 9:155–61. doi: 10.30476/jhsss.2020.88190.1136
90. Shin DE, Kim JE, Lee YL, Chung MA, Yoon HJ, Nam EW, et al. Effects of social prescribing pilot project for the elderly in rural area of South Korea during COVID-19 pandemic. Health Sci Rep. (2021) 4:e320. doi: 10.1002/hsr2.320
91. Li S, Dai Y, Zhou Y, Zhang J, Zhou C. Efficacy of group reminiscence therapy based on chinese traditional festival activities (ctfa-grt) on loneliness and perceived stress of rural older adults living alone in china: a randomized controlled trial. Aging Mental Health. (2021) 26:1377–84. doi: 10.1080/13607863.2021.1935457
92. Wang X, Li Y, Guo C, Liu M, Yeh CH. Community canteen services for the rural elderly: determining impacts on general mental health, nutritional status, satisfaction with life, and social capital. BMC Public Health. (2020) 20:230. doi: 10.1186/s12889-020-8305-9
93. Macleod A, Skinner MW, Wilkinson F, Reid H. Connecting socially isolated older rural adults with older volunteers through expressive arts. Can J Aging. (2016) 35:14–27. doi: 10.1017/S071498081500063X
94. Pearce R, Lillyman S. Reducing social isolation in a rural community through participation in creative arts projects. Nurs Older People. (2015) 27:33–8. doi: 10.7748/nop.27.10.33.s22
95. Dwyer P, Hardill I. Promoting social inclusion? The impact of village services on the lives of older people living in rural England. Ageing Soc. (2011) 31:243–64. doi: 10.1017/S0144686X10000851
96. Dickens AP, Richards SH, Greaves CJ, Campbell JL. Interventions targeting social isolation in older people: a systematic review. BMC Public Health. (2011) 11:647. doi: 10.1186/1471-2458-11-647
97. Findlay RA. Interventions to reduce social isolation amongst older people: where is the evidence? Ageing Soc. (2003) 23:647–58. doi: 10.1017/S0144686X03001296
98. Poscia A, Stojanovic J, La Milia DI, Duplaga M, Grysztar M, Moscato U, et al. Interventions targeting loneliness and social isolation among the older people: an update systematic review. Exp Gerontol. (2018) 102:133–44. doi: 10.1016/j.exger.2017.11.017
99. Gardiner C, Geldenhuys G, Gott M. Interventions to reduce social isolation and loneliness among older people: an integrative review. Health Soc Care Community. (2018) 26:147–57. doi: 10.1111/hsc.12367
100. Fakoya OA, Mccorry NK, donnelly M. Loneliness and social isolation interventions for older adults: a scoping review of reviews. BMC Public Health. (2020) 20:129. doi: 10.1186/s12889-020-8251-6
101. Noone C, Mcsharry J, Smalle M, Burns A, Dwan K, Devane D, et al. Video calls for reducing social isolation and loneliness in older people: a rapid review. Cochrane Database Syst Rev. (2020) 1–42. doi: 10.1002/14651858.CD013632
102. Valtorta NK, Moore DC, Barron L, Stow D, Hanratty B. Older adults' social relationships and health care utilization: a systematic review. Am J Public Health. (2018) 108:e1–e10. doi: 10.2105/AJPH.2017.304256
103. Litwin H, Levinsky M. Always alone? Network transitions among detached older Europeans and their effects. Ageing Soc. (2021) 41:2299–313. doi: 10.1017/S0144686X20000240
104. Dahlberg L, Mckee KJ, Frank A, Naseer M. A systematic review of longitudinal risk factors for loneliness in older adults. Aging Mental Health. (2022) 26:225–49. doi: 10.1080/13607863.2021.1876638
105. Hajek A, König H-H. Which factors contribute to loneliness among older Europeans? Findings from the survey of health, ageing and retirement in Europe: determinants of loneliness. Arch Gerontol Geriatr. (2020) 89:104080. doi: 10.1016/j.archger.2020.104080
106. Wenger GC, Burholt V. Changes in levels of social isolation and loneliness among older people in a rural area: a twenty–year longitudinal study. Can J Aging. (2004) 23:115–27. doi: 10.1353/cja.2004.0028
107. Donaldson JM, Watson R. Loneliness in elderly people: an important area for nursing research. J Adv Nurs. (1996) 24:952–9. doi: 10.1111/j.1365-2648.1996.tb02931.x
108. Wasserman S, Faust K. Social Network Analysis: Methods and Applications. London: Cambridge University Press (1994). doi: 10.1017/CBO9780511815478
109. Ehsan A, Klaas HS, Bastianen A, Spini D. Social capital and health: a systematic review of systematic reviews. SSM-Popul Health. (2019) 8:100425. doi: 10.1016/j.ssmph.2019.100425
110. Li T, Zhang Y. Social network types and the health of older adults: exploring reciprocal associations. Soc Sci Med. (2015) 130:59–68. doi: 10.1016/j.socscimed.2015.02.007
111. Hagan R, Manktelow R, Taylor BJ, Mallett J. Reducing loneliness amongst older people: a systematic search and narrative review. Aging Mental Health. (2014) 18:683–93. doi: 10.1080/13607863.2013.875122
112. Gyasi RM, Yeboah AA, Mensah CM, Ouedraogo R, Addae EA. Neighborhood, social isolation and mental health outcome among older people in Ghana. J Affect Disord. (2019) 259:154–63. doi: 10.1016/j.jad.2019.08.024
113. Cornwell B, Laumann EO, Schumm LP. The social connectedness of older adults: a national profile. Am Sociol Rev. (2008) 73:185–203. doi: 10.1177/000312240807300201
114. Ten Bruggencate T, Luijkx KG, Sturm J. Social needs of older people: a systematic literature review. Ageing Soc. (2018) 38:1745–70. doi: 10.1017/S0144686X17000150
115. Musalia J. Social capital and health in Kenya: a multilevel analysis. Soc Sci Med. (2016) 167:11–9. doi: 10.1016/j.socscimed.2016.08.043
116. Cattan M, White M, Bond J, Learmouth A. Preventing social isolation and loneliness among older people: a systematic review of health promotion interventions. Ageing Soc. (2005) 25:41–67. doi: 10.1017/S0144686X04002594
117. Domènech-Abella J, Mundó J, Haro JM, Rubio-Valera M. Anxiety, depression, loneliness and social network in the elderly: longitudinal associations from The Irish Longitudinal Study on Ageing (TILDA). J Affect Disord. (2019) 246:82–8. doi: 10.1016/j.jad.2018.12.043
118. Shelton RC, Lee M, Brotzman LE, Crookes DM, Jandorf L, Erwin D, et al. Use of social network analysis in the development, dissemination, implementation, and sustainability of health behavior interventions for adults: a systematic review. Soc Sci Med. (2019) 220:81–101. doi: 10.1016/j.socscimed.2018.10.013
119. Valente TW, Pitts SR. An appraisal of social network theory and analysis as applied to public health: challenges and opportunities. Annu Rev Public Health. (2017) 38:103–18. doi: 10.1146/annurev-publhealth-031816-044528
120. Lara E, Martín-María N, de la Torre-Luque A, Koyanagi A, Vancampfort D, Izquierdo A, Miret M. Does loneliness contribute to mild cognitive impairment and dementia? A systematic review and meta-analysis of longitudinal studies. Ageing Res Rev. (2019) 52:7–16. doi: 10.1016/j.arr.2019.03.002
121. Shen B, Guan T, Ma J, Yang L, Liu Y. Social network research hotspots and trends in public health: a bibliometric and visual analysis. Public Health Pract. (2021) 2:100155. doi: 10.1016/j.puhip.2021.100155
Keywords: loneliness, social network, social connections, older adults, rural area, rural communities, healthy aging, social isolation
Citation: Hussain B, Mirza M, Baines R, Burns L, Stevens S, Asthana S and Chatterjee A (2023) Loneliness and social networks of older adults in rural communities: a narrative synthesis systematic review. Front. Public Health 11:1113864. doi: 10.3389/fpubh.2023.1113864
Received: 01 December 2022; Accepted: 17 April 2023;
Published: 15 May 2023.
Edited by:
Wen-Hsu Lin, National Yang Ming Chiao Tung University, TaiwanReviewed by:
Carlo Lazzari, South West Yorkshire Partnership NHS Foundation Trust, United KingdomCopyright © 2023 Hussain, Mirza, Baines, Burns, Stevens, Asthana and Chatterjee. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Basharat Hussain, YmFzaGFyYXQuaHVzc2FpbkBwbHltb3V0aC5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.