
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 15 June 2023
Sec. Health Economics
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1112072
 Seyyed-Hadi Ghamari1†
Seyyed-Hadi Ghamari1† Farnam Mohebi2†
Farnam Mohebi2† Mohsen Abbasi-Kangevari1
Mohsen Abbasi-Kangevari1 Soheil Peiman1Besharat Rahimi3
Soheil Peiman1Besharat Rahimi3 Naser Ahmadi1
Naser Ahmadi1 Yousef Farzi1
Yousef Farzi1 Shahedeh Seyfi1Nazila Shahbal1
Shahedeh Seyfi1Nazila Shahbal1 Mitra Modirian1
Mitra Modirian1 Mehrdad Azmin1Hossein Zokaei1Maryam Khezrian1Roya Sherafat4
Mehrdad Azmin1Hossein Zokaei1Maryam Khezrian1Roya Sherafat4 Mohammad-Reza Malekpour1
Mohammad-Reza Malekpour1 Shahin Roshani5
Shahin Roshani5 Negar Rezaei1,6Mohammad Javad Fallahi7,8Maryam Haddadzadeh Shoushtari9Zahra Akbaripour10
Negar Rezaei1,6Mohammad Javad Fallahi7,8Maryam Haddadzadeh Shoushtari9Zahra Akbaripour10 Shahab Khatibzadeh4
Shahab Khatibzadeh4 Saeid Shahraz11*
Saeid Shahraz11*Introduction: Due to insufficient data on patient experience with healthcare system among patients with chronic obstructive pulmonary disease (COPD), particularly in developing countries, this study attempted to investigate the journey of patients with COPD in the healthcare system using nationally representative data in Iran.
Methods: This nationally representative demonstration study was conducted from 2016 to 2018 using a novel machine-learning based sampling method based on different districts’ healthcare structures and outcome data. Pulmonologists confirmed eligible participants and nurses recruited and followed them up for 3 months/in 4 visits. Utilization of various healthcare services, direct and indirect costs (including non-health, absenteeism, loss of productivity, and time waste), and quality of healthcare services (using quality indicators) were assessed.
Results: This study constituted of a final sample of 235 patients with COPD, among whom 154 (65.5%) were male. Pharmacy and outpatient services were mostly utilized healthcare services, however, participants utilized outpatient services less than four times a year. The annual average direct cost of a patient with COPD was 1,605.5 USDs. Some 855, 359, 2,680, and 933 USDs were imposed annually on patients with COPD due to non-medical costs, absenteeism, loss of productivity, and time waste, respectively. Based on the quality indicators assessed during the study, the focus of healthcare providers has been the management of the acute phases of COPD as the blood oxygen levels of more than 80% of participants were documented by pulse oximetry devices. However, chronic phase management was mainly missed as less than a third of participants were referred to smoking and tobacco quit centers and got vaccinated. In addition, less than 10% of participants were considered for rehabilitation services, and only 2% completed four-session rehabilitation services.
Conclusion: COPD services have focused on inpatient care, where patients experience exacerbation of the condition. Upon discharge, patients do not receive appropriate follow-up services targeting on preventive care for optimal controlling of pulmonary function and preventing exacerbation.
Chronic obstructive pulmonary disease (COPD) is a progressive, debilitating lung disease contributing to 926.1 disability-adjusted life-years (DALYs) per 100,000 population in 2019, worldwide (1). The World Health Organization deduced that unless proper measures are taken, COPD will turn the disease to the third most leading cause of death by 2030 (2). On the other hand, COPD is a chronic disease with catastrophic aftermaths, which imposes high hospitalizations, healthcare utilization, and direct and indirect costs on patients and healthcare systems (3–5). The total economic cost of COPD according to American Lung Association report in 2019 is close to $50 billion each year, including $29.5 billion for direct health care expenditures, $12.4 billion for indirect mortality costs, and $8.0 billion for indirect morbidity costs (6).
Commensurate with the global scale, COPD has yet remained as a significant public health concern in Iran, as roughly 380,000 DALYs were attributed to COPD from 1990 to 2019 in Iran (7). In addition, it has been estimated that the annual hospitalization cost per patient with COPD was 865 US dollars in Iran (8). Therefore, assessing the trends in healthcare quality and costs for COPD as a globally high-volume and high-cost disease would shed light on the current disease status. This would potentially empower policymakers to seize any opportunities to lower the costs and increase the quality of care (9).
Investigating utilization, quality, and healthcare costs at national level often requires relatively high budgets and expenditures, limiting investigators’ capabilities, especially regarding sampling methods. Addressing the limitations of previous sampling methods, we established a cohort study with a novel machine-learning based sampling method for evaluating the medical care. Iran Quality of Care Medicine Program (IQCAMP) is series of longitudinal surveys focusing on the patient-experience with healthcare services, which measure multiple patient-centered variables of healthcare utilization, quality, and costs at periodic time intervals (10) for seven high-prevalence and high-cost diseases, including diabetes mellitus (11), COPD, myocardial infarction, congestive heart failure, stroke, major depressive disorder, and end-stage renal failure.
The aim of this study was to evaluate the utilization, quality, and costs of healthcare services used by patients with COPD in Iran, using data from IQCAMP. Our study provides direction on how to assess COPD care on a national level, particularly in countries that share similar healthcare systems to Iran. We also believe that this study can offer insight into the typical scenarios experienced by COPD patients within the Iranian healthcare architecture.
This study is a part of the IQCAMP study, a national study aimed to affordably evaluate the quality and costs of healthcare across the country for seven high-prevalence and high-cost diseases in Iran from 2016 to 2018, including diabetes mellitus (11), COPD, myocardial infarction, congestive heart failure, stroke, major depressive disorder, and end-stage renal failure. This study reports first-hand data on patient experience regarding healthcare utilization, costs, and quality of care for each disease among a limited but representative patient sample. In the current study, we reported the utilization, quality and costs of healthcare for COPD across the country.
The patients in the IQCAMP study were selected using a novel sampling method. A machine-learning-based sampling method was used to divide 31 provinces into eight clusters considering their similarity in healthcare structure and outcome data. One province from each cluster was selected for data collection. Simulation analysis of the sampling revealed an efficiency of up to 70% (10). One province per district was systematically selected for data gathering, and the decision tree machine learning method was applied for an accurate description of the features of selected clusters (Supplementary Figure S1 and Supplementary Table S1). More details are provided in depth elsewhere (10). Using the method, the sample size is calculated approximately 300 participants. In the selected clusters, eligible patients were identified by pulmonologists and were approached by trained study nurses to attract study participation.
COPD is medically defined and confirmed by spirometry via the forced expiratory volume (FEV1) to forced vital volume (FVC) ratio of below 0.7 (12). However, considering the paucity of spirometers and diagnostic equipment in scores of provinces in Iran, the study’s medical experts decided to use to use the physician confirmation of COPD cases instead of using the FEV1 measures. Notably, in case of availability, we also recorded spirometry results (12). Due to low service utilization of low severity cases, the IQCAMP team decided to fundamentally survey on patients with moderate-to-severe COPD, who were hospitalized at least once due to COPD exacerbation during the past 3 months. Disease severity was defined based on the pulmonologists’ expert opinion.
A group of nurses in each clusters called the participants and gave them detailed instruction about the study objectives and their right to leave the study at any time. The initial interview included participants’ past and current medical history. Then, three monthly follow-up interviews were held by the nurses to collect data on service utilization, quality indicators, and the cost of healthcare services received. The ethics committee of the Tehran University of Medical Sciences and the National Institute of Medical Research Development (NIMAD) approved the patient recruitment protocol.
In this study, we aimed to gather three types of data: (1) the frequency of the utilization of healthcare services including inpatient and outpatient medical visits, medications, paraclinical services, and imaging, (2) quality of healthcare using quality indicators, and (3) direct and indirect costs of services provided by the patient, health insurance and government. A panel of medical experts for COPD, health economists, and epidemiologists designed the questionnaire based on their experience and literature review.
The questionnaire was face-validated and then updated after a pilot study with the participation of ten individuals. Finally, the study questionnaire was hosted on an android provisioned device and then underwent usability testing for the study nurses. The questionnaire included five main domains: (1) sociodemographics, (2) medical status, (3) healthcare utilization, (4) healthcare quality, and (5) healthcare costs.
The sociodemographic questionnaire consisted of questions about the gender, age, literacy, occupational status, and wealth index. The wealth index was used to divide the population into quintiles, whereby the first and fifth quintiles present the least fortunate and wealthiest households, respectively. Principal component analysis (PCA) was applied to derive the household wealth index based on questions on key dwelling characteristics and household ownership, as described in the study protocol (13). The health status questionnaire included questions regarding the current health condition of participants, their awareness about the medical condition, complications, and aftermaths of their disease, and smoking status.
Three major categories of services, including therapeutic, diagnostic, and patient support services, were included in the healthcare utilization questionnaire. Therapeutic services consisted of inpatient and outpatient visits; diagnostic services consisted of laboratory, testing, and imaging services; and patient support services included rehabilitation, home care, medical equipment utilization, and pharmacy services. In addition, all medications that were available in the Iranian Pharmacopoeia and were used to treat COPD were included in the survey.
To assess the quality of healthcare services, an expert panel of individuals involved in managing patients with COPD including primary care physician, internist, pulmonologist, and sub-specialist in COPD were gathered. The panel initially extracted the quality indicators for healthcare services from resources provided by the Ministry of Health and Medical Services of Iran, frameworks utilized in developing countries, and National Qualification Framework (NQF) developed for the United States (US) (14). Then, the panel conducted an extensive literature review and included other indices that were deemed essential based on their own experience in assessing the quality of care, but not considered in the guidelines mentioned earlier. Finally, a set of indicators with the highest rates of agreement upon were included as quality-of-care assessment indicators in this study. The quality indicators included 14 questions: seven questions for chronic phase of COPD, and seven questions for exacerbation episodes (acute phase). Smoking cessation advice, referral to smoking and tobacco quit centers, assessing the accuracy of inhaler utilization at the first visit and during the past year, vaccination against seasonal influenza and pneumococcal pneumonia, and considering spirometry during the past 12 months were indicators of chronic phase. Quality of care for exacerbation episodes was assessed by patient education about first measures during an exacerbation, oxygen therapy at the emergency department, assessment of the accuracy of inhaler usage after exacerbation episode, usage of glucocorticoids after discharge, referral to and completion of 4 week rehabilitation services after discharge, and pulse-oximetry during hospitalization. A list of all indicators assessed by medical experts to be included in the study is presented in Supplementary Table S2.
Two categories of healthcare costs included direct medical and indirect costs. The direct costs section included questions regarding healthcare diagnostic and therapeutic services costs, hospitalization costs, and costs attributable to medication, rehabilitation, and home services. The indirect costs section included direct non-medical costs (i.e., transportation, accommodation, and childcare costs during the hospitalization), absenteeism, loss of productivity, and wasted time during the doctor-patient visits. Considering the disparate sources of healthcare costs including out-of-pocket costs, health insurance share and the governmental support, direct medical costs were gathered via hospital invoices and self-declarative questionnaire.
Data were collected through patients’ medical records, health insurance details, and interviews of patients via structured questionnaires. Provisioned devices were used for the electronic migration of the structured questionnaire.
The unit of analysis was defined as patient-month. Therefore, a 3 month follow-up of one patient was equal to three patient-month visits. Healthcare utilization data were reported by the number of events per month that resulted in healthcare services and the average number of monthly utilization of services per patient visit. To present the average annual costs of COPD, the average cost of each month was calculated and multiplied by 12. Purchasing Power Parity (PPP) was applied to convert Iranian Rials to US Dollars (USDs), where 1,000 USD equaled 16,773,000 Iranian Rials (15). Considering the importance of converting indirect costs to interpretable measures, firstly, the number of absent days from work due to their underlying disease multiplied in minimum daily wage to calculate absenteeism. Secondly, loss of productivity was calculated by asking the patients how much less they could earn due to their current illness. Quality of healthcare for COPD was assessed by reporting the number (%) of participants utilizing quality-of-care indices. All quantitative data were reported by central tendency (mean and median), and dispersion indices including standard deviation (SD) and interquartile range (IQR).
From 300 participants selected from eight clusters of Iran, a total of 235 (78.3%) patients with COPD completed the study, of which 154 (65.5%) were male. All patients have monthly been followed up for 3 months, which was interpreted as 705 patient visits. Sociodemographic characteristics of participants are presented in Table 1.
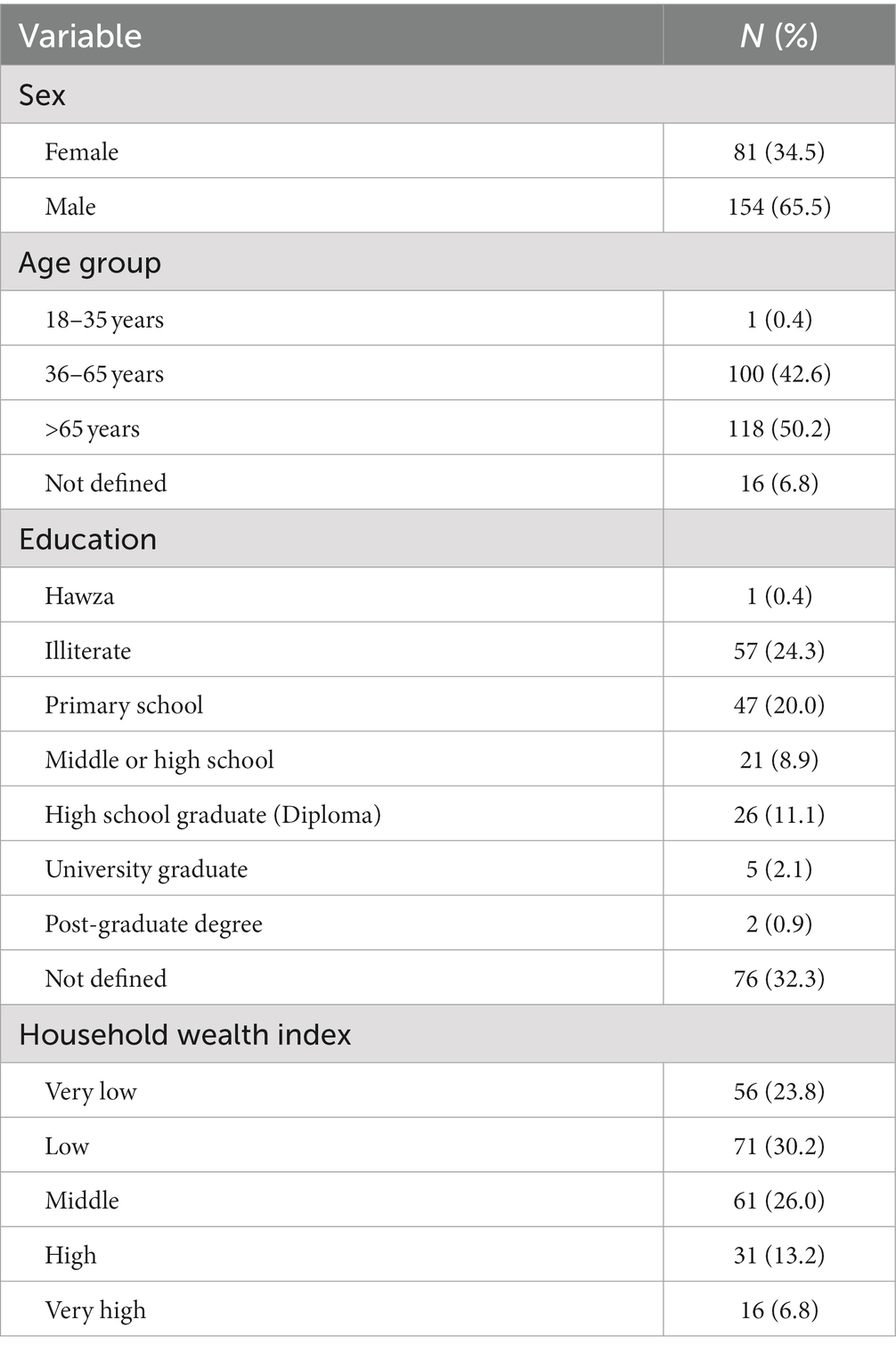
Table 1. Sociodemographic characteristics of participants.
Of all participants, 217 (92.3%) were aware of their disease, and 182 (83.9%) participants have been diagnosed with COPD for more than a year. Some 118 (50.0%) of participants declared they have a history of smoking, with 21 (17.8%) among women and 97 (82.2%) among men. Of participants with a history of smoking, 61 (51.7%) had not yet quit smoking [6 (10.0%) among women and 54 (88.5%) among men]. The mean (SD) and median (IQR) daily number of cigarette stubs were 21.1 (14.0) and 15.0 (20.0), respectively. The mean (SD) daily number of cigarette stubs among men was significantly higher than women: 21.0 (13.5) vs. 14.8 (16.1); p-value <0.001. The mean (SD) years of smoking was 31.9 (15.2) years, with 31.9 (15.1) and 22.8 (14.9) among women.
Table 2 presents the monthly utilization of various COPD services among 705 patient-visits. The most utilized services were pharmacy services with monthly use of 258 times (189 times for males and 69 times for females), followed by outpatient services with 142 times per month (99 times for males and 43 times for females). The most prescribed medications among patients with COPD were salbutamol inhaler [173 (73.6%)], tiotropium inhaler [98 (41.7%)] and ipratropium inhaler [95 (40.4%)]. The outpatient services were utilized less than four times a year. Almost none of the participants utilized the rehabilitation services.
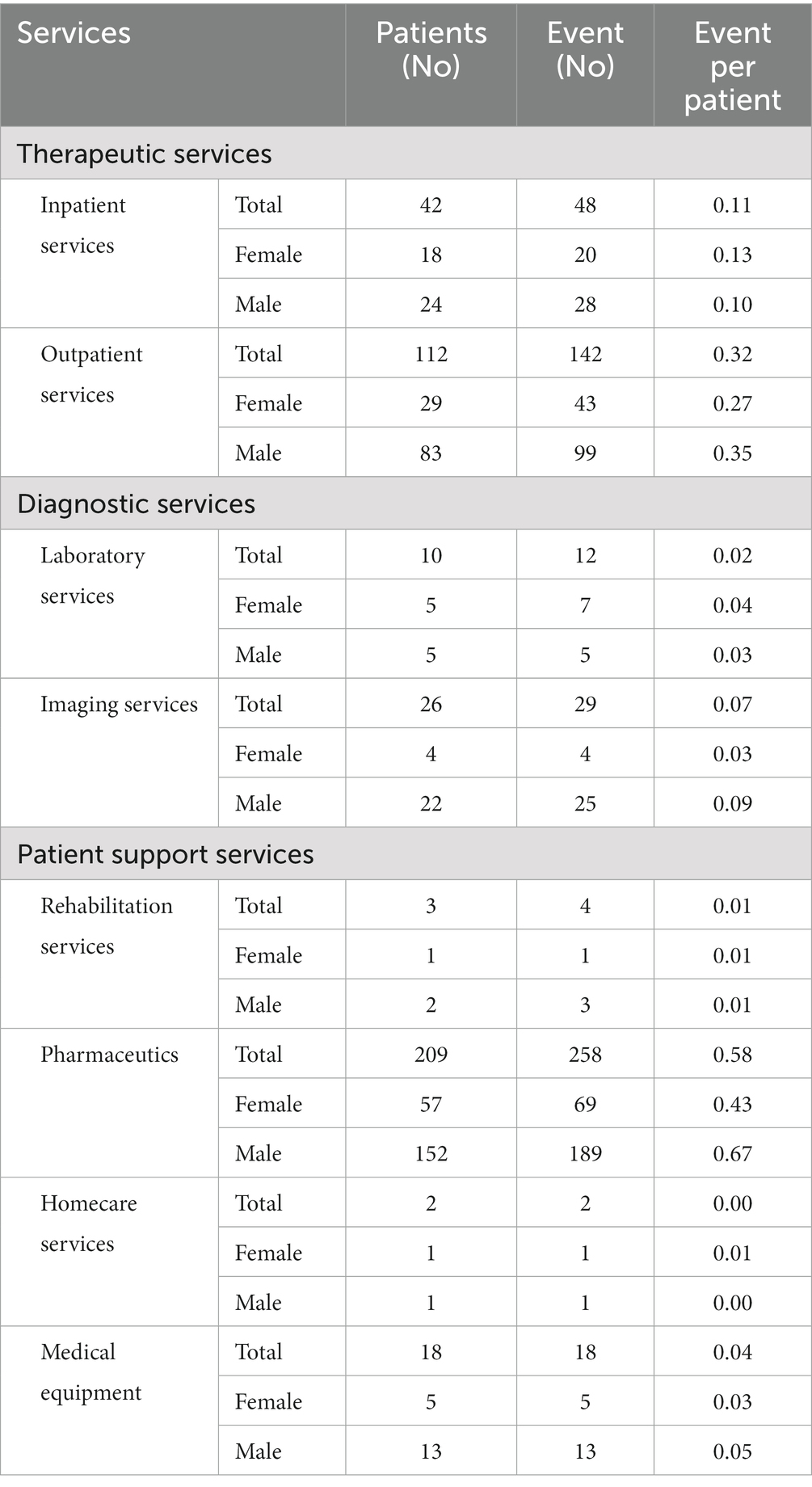
Table 2. Monthly utilization of various services among 705 patient visits of COPD.
During the exacerbation phase of COPD, the blood oxygen levels of more than 80% of participants with exacerbated COPD were measured by pulse oximetry devices and documented, which was between 80 to 93% among the majority of hospitalized participants. In addition, more than 80% of eligible participants harmonically received oxygen therapy during hospitalization in the emergency departments. However, less than half of participants were educated about essential first measures during COPD exacerbation, which was much lower among female participants. Less than 70% of participants were evaluated for the precision of inhaler usage after the COPD exacerbation episode.
Considering the chronic phase of COPD, some 60% of participants have been monitored by respiratory function tests and spirometry during the past year. Although the physician assessed the accuracy of inhaler usage among more than 75% of participants at the first patient-physician visit, only 67% of participants declared that the physician reassessed the accuracy during the past year. Most eligible participants were advised to quit smoking by their physicians. However, less than a third of participants were referred to smoking and tobacco quit centers and vaccinated against pneumococcus/Influenza. In addition, barely any participants were able to follow-up with rehabilitation services, and only 2% of participants have completed four-session rehabilitation services (Figure 1).
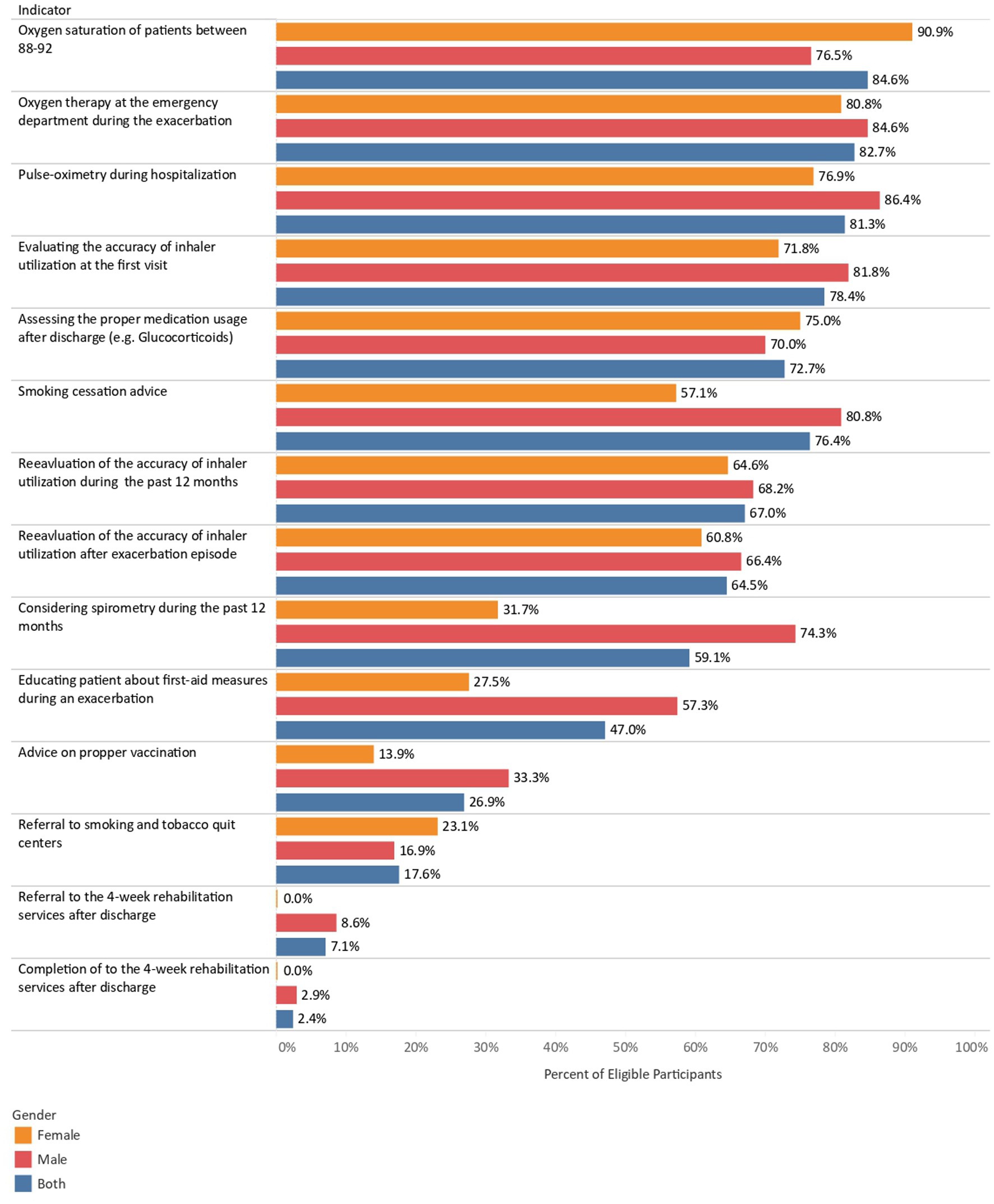
Figure 1. The quality indicators of COPD diagnosis and management among men and women.
The annual average direct cost of a patient with COPD was 1,605.5 USDs. Average out-of-pocket share of direct costs calculated 181.8 USD. While more than 85% of direct costs were due to hospitalization and inpatient services, most out-of-pocket costs were due to pharmacy services. Direct and indirect costs of COPD are presented in Table 3.
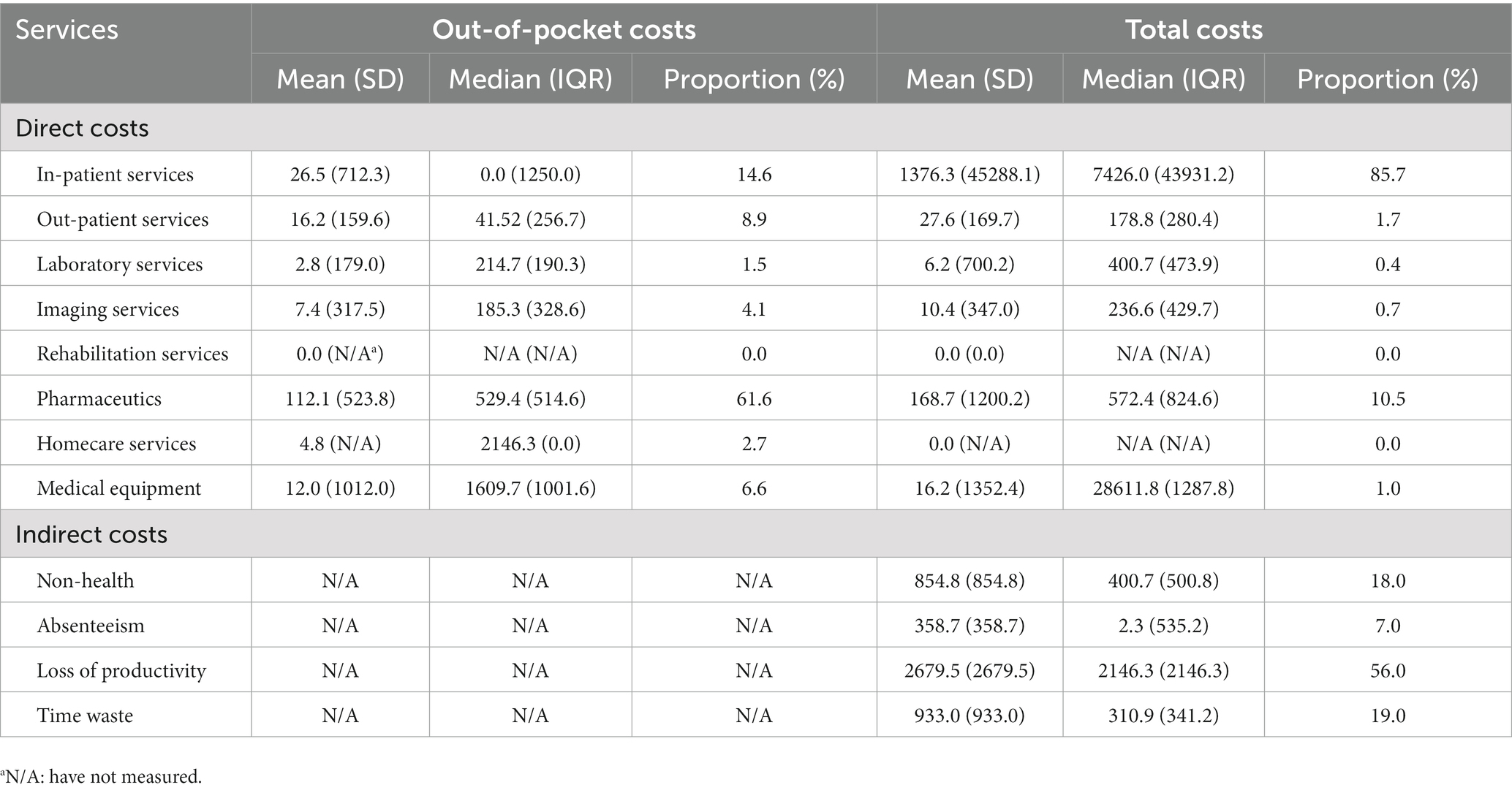
Table 3. Annual costs of various medical services for patients with COPD.
In this cohort study, we assessed the utilization, quality and costs of healthcare services for COPD in Iran using an affordable machine-learning based sampling method, which would pave the way for investigating such trends for high-volume and high-cost diseases on global scales and other nations. We found that pharmacy and outpatient medical services were the highest utilized healthcare services among patients with COPD. While medications imposed most of the out-of-pocket costs, the greatest portion of the direct costs were due to hospitalization and inpatient services. Healthcare quality provided for patients with COPD was higher in the exacerbation phases of the disease, and healthcare services revolved much less around chronic care for COPD.
Some 85% of the direct costs of COPD were due to hospitalization and inpatient services. Out-of-pocket costs were primarily due to pharmacy services. Enhanced availability of generic inhaled medication options could reduce cost and improve patients’ compliance (16). While COPD exacerbations generally result in healthcare resource use via increased physician visits, emergency department visits, hospitalizations, and pharmacy use (17), increased exacerbation frequency and severity impose higher costs, with the costs culminating among patients who require mechanical ventilation (18).
Healthcare providers measured patients’ blood oxygen levels in the emergency rooms and initiated oxygen therapy in most cases. Nevertheless, less than half of patients had been educated about the measures during COPD exacerbation including calling emergency services, administering oxygen supply, and maintaining in their most comfortable position. There is evidence that after the healthcare professionals have managed a COPD exacerbation episode of a patient, they have a golden opportunity to educate the patient about the necessary measures to prevent the following episode (19). Thus, patients need to receive appropriate maintenance therapy and attend appointments focusing on a medication regimen, proper inhaler technique, and assessment of symptoms to reduce exacerbation frequency and prevent the disease progression (18).
For further improvement in COPD course, it is recommended that pulmonary rehabilitation be started within 3 weeks of hospital discharge (20). Pulmonary rehabilitation is considered highly effective in improving dyspnea, exercise tolerance, and health-related quality of life. Some 60% of patients with COPD in England and Wales were enrolled into and completed a pulmonary rehabilitation program (21). Nevertheless, access to such services remains challenging for many patients, especially those living in limited resource settings (22). We found that only 7% of patients were advised by their physicians to attend rehabilitation programs within a month of referral. This might be partially due to scarcity of respiratory rehabilitating centers in Iran in addition to underestimation of the effectiveness of rehabilitation programs on COPD course. Unexpectedly, some 2% of patients reported completing on course of rehabilitation programs. In a study on Iranian patients with COPD, the barriers for pulmonary rehabilitation were partly due to patients lack of knowledge and the complexity and chronicity of COPD, which hinders patients from appropriate care. Another compelling reason regarding lower attendance of pulmonary rehabilitation services in Iran might be due to high costs of the service, inadequate insurance coverage, and inadequate professional competence of rehabilitation staff (23).
While spirometry remains the gold standard for diagnosis and monitoring COPD (24), less than 60% of the patients in this study were monitored by spirometry during the past year. In addition, we found that there was a significant two-fold gender gap between men and women in spirometry utilization. The underutilization of spirometry for COPD progression monitoring raises concerns, especially among women, who experience COPD exacerbations episodes more than men (25). COPD is mythically perceived as a male-dominated disease; however, it affects women and men almost equally (26). While smoking is traditionally considered the cause of COPD, household air pollution exposure and second-hand smoking are neglected risk factor for COPD, affecting women more than men (27). In addition, there is evidence that fear of stigmatization and improper knowledge about COPD cause could alter felt needs and healthcare-seeking behavior among women with COPD (28). On the other hand, primary care physicians play a central role in overseeing the multidisciplinary care of women with COPD (25). Thus, it is of paramount importance that physicians significantly improve awareness and encourage women with COPD to promptly seek medical advice. Primary care physicians play a central role in overseeing the multidisciplinary care of women with chronic obstructive pulmonary disease.
Smoking cessation is known to decrease mortality among patients with COPD via slowing the decline in lung function over time and limiting exacerbations (29). While physicians advised most patients to quit smoking, less than a third of participants were referred to professional centers for smoking cessation. Understandably, nearly half of the patients with a smoking history had not quit smoking at the study time. The accessibility to tobacco cessation centers is known to be a determinant of patients’ smoking cessation behavior (30). Iran’s Comprehensive National Tobacco Control Act has been in place since 2005. However, tobacco cessation programs in Iran have demonstrated no remarkable impacts. Notably, the prevalence of tobacco smoking has stagnated since 2004, when the STEPwise approach to chronic disease risk-factor surveillance (STEPS) survey was first conducted in the country (31). While the act also stated that smoking cessation counseling services ought to be provided in all health centers, the establishment of the national tobacco cessation helpline and tobacco cessation service clinics was announced in 2021 (32). Thus, the political will to lessen the burden of tobacco smoking needs to be strengthen, strict legislations need to be provided by the parliament and the government to discourage smoking, and more comprehensive solutions need to be employed to help quit smoking.
Less than a third of patients reported being vaccinated for pneumococcal and influenza during the last year, although vaccines are strongly recommended for patients with COPD for preventing poor outcomes (33). Reasons for low utilization of vaccines among patients could be improper knowledge (34), lack of vaccine recommendation by physicians, mistrust of vaccine safety, inconvenience of vaccination procedure, supply, and accessibility (35).
Patients with COPD often do not use their inhalers correctly, associated with an increased risk of disease exacerbation and hospitalization. Thus, periodic reinforcement of patient education on proper inhaler use is considered critical for COPD management (36). In our study, the accuracy of inhaler use was assessed by physicians for 75% of patients in the first visit and 70% after the last COPD exacerbation episode. This might partly be due to paucity of physician’s knowledge in addition to their negligence because of high workload in emergency rooms (37).
Overall, based on the quality indicators assessed during the study, the focus of healthcare providers has been the management of the acute phases of COPD and missed the management of the chronic phase. This might be due to several reasons as follows.
Firstly, Iran has undergone significant changes in the burden of diseases pattern from communicable diseases to non-communicable diseases. Nevertheless, the healthcare system has not yet been aligned commensurate with such dramatic changes. After the Declaration of Alma-Ata on Primary Healthcare in 1978, rural and urban health centers were established with preventive practices. Considering that most of the Iranian population resided in rural areas at that time, most of the investment was allocated to rural areas (38). Notwithstanding, the rural primary healthcare system with trained community healthcare workers and well-established guidelines was effective in modifiable risk factors, including high systolic blood pressure and high plasma glucose (39). Nevertheless, the population distribution pattern in Iran changed dramatically in the preceding decades (40), while the network of urban health centers did not develop along with the growing demand due to civilization.
In the absence of a functional central healthcare system in urban areas, the primary healthcare services are decentralized and solo-practice. To establish an integrated healthcare system, the family physician program was launched in rural areas in 2005 with less than 20,000 population. The program introduced general practitioners to act as the focal point in the referral system. In 2012, the program was piloted in urban areas of two provinces (41). Although the family physician program could have had the capacity to provide the infrastructure required for the management of chronic non-communicable diseases, it failed due to improper design and mismanagement.
Thus, the current healthcare system lacks the integrated network of healthcare providers as needed for the long-term management of chronic non-communicable diseases.
Concurrently, the attitudes of insurance companies towards lessening the burden of diseases are still set for communicable diseases, the main characteristic of which is their acute onset. This has resulted in a narrow spectrum of the diversity of services and medications covered by insurance programs (38), which remains an obstacle to properly managing chronic diseases. Previous evidence suggests that limited insurance coverage for chronic disease management is ill-suited for the needs of patients with COPD and is associated with adverse clinical outcomes such as cost-related medication nonadherence, reports of foregone specialist and follow-up care, higher emergency room admission, and hospitalizations (42). Medication costs could be a contributing factor affecting patients’ adherence to prescribed medications. This is not confined to COPD and has also been witnessed in other diseases such as cancer (43) and cardiovascular disease (44). The potential inequities in quality of care across various income groups also need to be assessed in future studies.
Neglecting the long-term management of COPD could result in a higher frequency of COPD exacerbations. Frequent moderate-to-severe COPD exacerbation episodes are known to fuel the rate of lung function (45) and adversely affect the patients’ health-related quality of life. Holistic approaches towards COPD management could consist of multidisciplinary teams (18), close follow-ups, regular home visits (46), medication review, proper inhaler technique training, and education. Subsequently, COPD-related or all-cause hospital readmission rates (47) could be reduced, patients’ quality of care would improve, and direct or indirect costs would be reduced (18). Education should become an essential part of COPD management to empower patients to take control of their disease. Novel approaches could be employed to enhance the utilization of pulmonary rehabilitation among patients with COPD, such as using home-based nursing (48). Telehealth technology (49) could also be used to deliver pulmonary rehabilitation or even remote monitoring of proper inhaler usage (50). Such approaches could make rehabilitation more cost-effective and accessible, which need to be assessed in future studies.
IQCAMP provided a patient-centered disease-specific vision on healthcare utilization, quality, and costs for seven high-volume, high-cost diseases in Iran. Studies indicating national quality and costs of healthcare are mainly performed in countries with a well-established economy. In such settings, the real-world data to help understand patient experience usually come from claims, electronic medical records, electronic health records, and established data registries. Such surveys are usually limited to small samples collected by non-representative sampling methods in developing countries. In the meantime, large-sample studies could be extravagant for developing countries. IQCAMP is a cohort study that generates real-world data that provides first-hand information on patient experience for seven medical conditions that consume more than 50% of healthcare costs. Therefore, the sampling method in IQCAMP could empower policymakers to conduct small sample size surveys with celerity and at a low cost.
We also acknowledge the limitations of the study. Although the data collection method of the study is more advantageous than the convenience sampling method, it is not as representative as simple random sampling at a national level. This could call for further research to investigate the optimum sampling method in health systems research to address the healthcare utilization, quality, and costs for COPD, as studied in the present research. It is worth mentioning that planning, conducting, and implementing the current survey are too tedious and have many complexities, hindering the study’s repetition. Nevertheless, the study design was deemed rational in Iran’s lack of an integrated health data system. As data on healthcare utilization was partly based on self-report, it could be subject to recall bias. In addition, the medication count in patients’ prescriptions was used as a proxy of medication utilization, which could not reflect the patients’ adherence to treatment. We were also eager to investigate the sub-national inequities in quality of care and utilization; however, the study did not have enough power for subgroup analysis and determination of geographical distribution due to a limited number of cases.
Although COPD is a high-cost and high-volume disease in Iran, healthcare quality provided for patients with COPD was solely high in the exacerbation phases of the disease, and healthcare services revolved much less around chronic care for COPD. Iran’s healthcare system is in transition from communicable diseases to non-communicable diseases. More concentration on post-acute phases of NCDs is required to contain NCDs pandemic.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, upon request.
The current study is a joint product of two grants, IranMHS and IQCAMP, that were approved by the Ethics Committee of Tehran University of Medical Sciences in Iran (no. IR.TUMS.REC.1394.1900) and the ethics committee of Iran National Institute for Medical Research Development, Tehran, Iran (Ethics code: IR.NIMAD.REC.1395.003), respectively. The patients/participants provided their written informed consent to participate in this study.
SK and SaS: conceptualization. FM, MM, NS, YF, ShS, SK, and SaS: data curation. MA-K, S-HG, NA, YF, MA, SR, ShS, and SaS: formal analysis. SaS: funding acquisition. MA-K, YF, ShS, NR, SK, and SaS: investigation. FM, YF, MA, ShS, NR, SK, and SaS: methodology. FM, YF, ShS, NR, and SaS: project administration. NR and SaS: resources. YF, MA, HZ, MK: software. YF, NR, and SaS: supervision. YF, NR, SK, and SaS: validation. S-HG, MA-K, and SaS: writing—original draft preparation. S-HG, FM, MA-K, SP, BR, NA, YF, ShS, NS, MM, MA, HZ, MK, RS, M-RM, SR, NR, MF, MS, ZA, SK, and SaS: writing—review and editing. All authors contributed to the article and approved the submitted version.
The authors would like to sincerely thank the IQCAMP COPD module interviewers, Roya Hamedi, Alireza Javaheri, Fatemeh Tolideh, Gita Ahmadizadeh, Maryam Abdolalizadeh, Mohammad Ghasem Abedinpour, Fatemeh Asghari Kachlam, Habib Kerchi, Zahra Keshtvarzi, Fariba Khademi, Masoumeh Rabieepour, Hanieh Mirbolouki, Azadeh Zahedifar, Mohammadreza Kaveh, and Ali Amiri.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1112072/full#supplementary-material
1. Momtazmanesh, S, Moghaddam, SS, Ghamari, SH, Rad, EM, Rezaei, N, Shobeiri, P, et al. Global burden of chronic respiratory diseases and risk factors, 1990–2019: an update from the Global Burden of Disease Study 2019. eClinical Medicine (2023) 59:101936.
2. Portegies, MLP, Lahousse, L, Joos, GF, Hofman, A, Koudstaal, PJ, Stricker, BH, et al. Chronic obstructive pulmonary disease and the risk of stroke the Rotterdam study. Am J Respir Crit Care Med. (2016) 193:251–8. doi: 10.1164/rccm.201505-0962OC
3. Byng, D, Lutter, JI, Wacker, ME, Jörres, RA, Liu, X, Karrasch, S, et al. Determinants of healthcare utilization and costs in COPD patients: first longitudinal results from the German COPD cohort COSYCONET. Int J COPD. (2019) 14:1423–39. doi: 10.2147/COPD.S201899
4. Wacker, ME, Hunger, M, Karrasch, S, Heinrich, J, Peters, A, Schulz, H, et al. Health-related quality of life and chronic obstructive pulmonary disease in early stages—longitudinal results from the population-based KORA cohort in a working age population. BMC Pulm Med. (2014) 14:134. doi: 10.1186/1471-2466-14-134
5. Wacker, ME, Jörres, RA, Karch, A, Wilke, S, Heinrich, J, Karrasch, S, et al. Assessing health-related quality of life in COPD: comparing generic and disease-specific instruments with focus on comorbidities. BMC Pulm Med. (2016) 16:70. doi: 10.1186/s12890-016-0238-9
6. Association AL. (2023) COPD trends brief—burden. Available at: https://www.lung.org/research/trends-in-lung-disease/copd-trends-brief/copd-burden. (Accessed April 29, 2023)
7. Heidari-Foroozan, M, Aryan, A, Esfahani, z, Shahrbaf, MA, Moghaddam, SS, Keykhaei, M, et al. National, subnational and risk attributed burden of chronic respiratory diseases in Iran from 1990 to 2019. Respir Res. (2023) 24. doi: 10.1186/s12931-023-02353-1
8. Rehman, AU, Ahmad Hassali, MA, Muhammad, SA, Shah, S, Abbas, S, IAB, HA, et al. The economic burden of chronic obstructive pulmonary disease (COPD) in the USA, Europe, and Asia: results from a systematic review of the literature. Expert Rev Pharmacoecon Outcomes Res. (2020) 20:661–72. doi: 10.1080/14737167.2020.1678385
9. van der Schans, S, Goossens, LMA, Boland, MRS, Kocks, JWH, Postma, MJ, van Boven, JFM, et al. Systematic review and quality appraisal of cost-effectiveness analyses of pharmacologic maintenance treatment for chronic obstructive pulmonary disease: methodological considerations and recommendations. Pharmacoeconomics. (2017) 35:43–63. doi: 10.1007/s40273-016-0448-2
10. Parsaeian, M, Mahdavi, M, Saadati, M, Mehdipour, P, Sheidaei, A, Khatibzadeh, S, et al. Introducing an efficient sampling method for national surveys with limited sample sizes: Application to a national study to determine quality and cost of healthcare. BMC Public Health. (2020) 21:1414. doi: 10.21203/rs.3.rs-20263/v1
11. Abbasi-Kangevari, M, Mohebi, F, Ghamari, SH, Modirian, M, Shahbal, N, Ahmadi, N, et al. Quality and cost of healthcare services in patients with diabetes in Iran: results of a nationwide short-term longitudinal survey. Front Endocrinol. (2023) 14:1099464. doi: 10.3389/fendo.2023.1099464
13. Rencher, AC, and Schimek, MG. Methods of multivariate analysis. Comput. Statistics. (1997) 12:422.
14. NQF: Measures, reports & tools. Available at: https://www.qualityforum.org/Measures_Reports_Tools.aspx
15. (2023)PPP conversion factor, GDP (LCU per international $)—Iran, Islamic rep.|data. Available at: https://data.worldbank.org/indicator/PA.NUS.PPP?locations=IR. (Accessed April 29, 2023)
16. Patel, MR, Press, VG, Gerald, LB, Barnes, T, Blake, K, Brown, LK, et al. Improving the affordability of prescription medications for people with chronic respiratory disease an official American thoracic society policy statement. Am J Respir Crit Care Med. (2018) 198:1367–74. doi: 10.1164/rccm.201810-1865ST
17. Dhamane, AD, Moretz, C, Zhou, Y, Burslem, K, Saverno, K, Jain, G, et al. COPD exacerbation frequency and its association with health care resource utilization and costs. Int J COPD. (2015) 10:2609–18. doi: 10.2147/COPD.S90148
18. Bollmeier, SG, and Hartmann, AP. Management of chronic obstructive pulmonary disease: A review focusing on exacerbations. Am J Health Syst Pharm. (2020) 77:259–68. doi: 10.1093/ajhp/zxz306
19. Hurst, JR, Donaldson, GC, Quint, JK, Goldring, JJP, Baghai-Ravary, R, and Wedzicha, JA. Temporal clustering of exacerbations in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. (2009) 179:369–74. doi: 10.1164/rccm.200807-1067OC
20. Wedzicha, JA, Calverley, PMA, Albert, RK, Anzueto, A, Criner, GJ, Hurst, JR, et al. Management of COPD exacerbations: A European Respiratory Society/American Thoracic Society guideline. Eur Respir J. (2017) 50:1602265. doi: 10.1183/13993003.02265-2016
21. None, TL. UK COPD treatment: failing to progress. Lancet. (2018) 391, 391:1550. doi: 10.1016/S0140-6736(18)30904-8
22. Halpin, DMG, Criner, GJ, Papi, A, Singh, D, Anzueto, A, Martinez, FJ, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. Am J Respir Crit Care Med. (2021) 203:24–36. doi: 10.1164/rccm.202009-3533SO
23. Sami, R, Salehi, K, Hashemi, M, and Atashi, V (2023). Exploring the barriers to pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: a qualitative study. BMC Health Serv. Res, 21:828, Doi: doi: 10.1186/s12913-021-06814-5
24. Hoesterey, D, das, N, Janssens, W, Buhr, RG, Martinez, FJ, Cooper, CB, et al. Spirometric indices of early airflow impairment in individuals at risk of developing COPD: Spirometry beyond FEV1/FVC. Respir Med. (2019) 156:58–68. doi: 10.1016/j.rmed.2019.08.004
25. Tsiligianni, I, Rodríguez, MR, Lisspers, K, Lee Tan, T, and Infantino, A. Call to action: improving primary care for women with COPD. NPJ Prim Care Respir Med. (2017) 27:1–6. doi: 10.1038/s41533-017-0013-2
26. Ancochea, J, Miravitlles, M, García-Río, F, Muñoz, L, Sánchez, G, Sobradillo, V, et al. Infradiagnóstico de la enfermedad pulmonar obstructiva crónica en mujeres: Cuantificación del problema, determinantes y propuestas de acción. Arch Bronconeumol. (2013) 49:223–9. doi: 10.1016/j.arbres.2012.11.010
27. Siddharthan, T, Grigsby, MR, Goodman, D, Chowdhury, M, Rubinstein, A, Irazola, V, et al. Association between household air pollution exposure and chronic obstructive pulmonary disease outcomes in 13 low-and middle-income country settings. Am J Respir Crit Care Med. (2018) 197:611–20. doi: 10.1164/rccm.201709-1861OC
28. Johnson, JL, Campbell, AC, Bowers, M, and Nichol, AM. Understanding the social consequences of chronic obstructive pulmonary disease: the effects of stigma and gender. Proc Am Thorac Soc. (2007) 4:680–2. doi: 10.1513/pats.200706-084SD
29. Wu, J, and Sin, DD. Improved patient outcome with smoking cessation: when is it too late? Int J COPD. (2011) 6:259–67. doi: 10.2147/COPD.S10771
30. Twyman, L, Bonevski, B, Paul, C, and Bryant, J. Perceived barriers to smoking cessation in selected vulnerable groups: a systematic review of the qualitative and quantitative literature. BMJ Open. (2014) 4:e006414–5. doi: 10.1136/bmjopen-2014-006414
31. Sohrabi, MR, Abbasi-Kangevari, M, and Kolahi, AA. Current tobacco smoking prevalence among Iranian population: a closer look at the STEPS surveys. Front Public Health. (2020) 8:571062. doi: 10.3389/fpubh.2020.571062
32. WHO EMRO. (2023). WHO supports establishment of national tobacco cessation hotline|news|Iran site. Available from: https://www.emro.who.int/fr/iran/news/who-supports-establishment-of-national-tobacco-cessation-hotline.html. (Accessed April 29, 2023)
33. Wedzicha, JA, and Seemungal, TA. COPD exacerbations: defining their cause and prevention. Lancet. (2007) 370:786–96. doi: 10.1016/S0140-6736(07)61382-8
34. Ye, C, Zhu, W, Yu, J, Li, Z, Hu, W, Hao, L, et al. Low coverage rate and awareness of influenza vaccine among older people in Shanghai, China: a cross-sectional study. Hum Vaccines Immunother. (2018) 14:2715–21. doi: 10.1080/21645515.2018.1491246
35. Wang, Y, Cheng, M, Wang, S, Wu, F, Yan, Q, Yang, Q, et al. Vaccination coverage with the pneumococcal and influenza vaccine among persons with chronic diseases in Shanghai, China, 2017. BMC Public Health. (2020) 20:1–9. doi: 10.1186/s12889-020-8388-3
36. Melani, AS, Bonavia, M, Cilenti, V, Cinti, C, Lodi, M, Martucci, P, et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. (2011) 105:930–8. doi: 10.1016/j.rmed.2011.01.005
37. Skowron, N, Wilke, P, Bernhard, M, Hegerl, U, and Gries, A. Workload in emergency departments: a problem for personnel and patients? Anaesthesist. (2019) 68:762–9. doi: 10.1007/s00101-019-00686-5
38. Danaei, G, Farzadfar, F, Kelishadi, R, Rashidian, A, Rouhani, OM, Ahmadnia, S, et al. Iran in transition. Lancet. (2019) 393:1984–2005. doi: 10.1016/S0140-6736(18)33197-0
39. Farzadfar, F, Murray, CJL, Gakidou, E, Bossert, T, Namdaritabar, H, Alikhani, S, et al. Effectiveness of diabetes and hypertension management by rural primary healthcare workers (Behvarz workers) in Iran: a nationally representative observational study. Lancet. (2012) 379:47–54. doi: 10.1016/S0140-6736(11)61349-4
40. Pilehvar, A. Spatial-geographical analysis of urbanization in Iran. Humanit Soc Sci Commun. (2021) 81:1–12. doi: 10.1057/s41599-021-00741-w
41. Bayati, M, Keshavarz, K, Lotfi, F, Barati, O, Zareian, S, Amiri, A, et al. Effect of two major health reforms on health care cost and utilization in Fars Province of Iran: family physician program and health transformation plan. BMC Health Serv Res. (2020) 201:63. doi: 10.1186/s12913-020-05257-8
42. Gaffney, A, White, A, Hawks, L, Himmelstein, D, Woolhandler, S, Christiani, DC, et al. High-deductible health plans and healthcare access, use, and financial strain in those with chronic obstructive pulmonary disease. Ann Am Thorac Soc. (2019) 17:49–56. doi: 10.1513/AnnalsATS.201905-400OC
43. Zafar, SY, Peppercorn, JM, Schrag, D, Taylor, DH, Goetzinger, AM, Zhong, X, et al. The financial toxicity of cancer treatment: a pilot study assessing out-of-pocket expenses and the insured cancer patient’s experience. Oncologist. (2013) 18:381–90. doi: 10.1634/theoncologist.2012-0279
44. Valero-Elizondo, J, Khera, R, Saxena, A, Grandhi, GR, Virani, SS, Butler, J, et al. Financial hardship from medical bills among nonelderly U.S. adults with atherosclerotic cardiovascular disease. J Am Coll Cardiol. (2019) 73:727–32. doi: 10.1016/j.jacc.2018.12.004
45. Halpin, DMG, Decramer, M, Celli, BR, Mueller, A, Metzdorf, N, and Tashkin, DP. Effect of a single exacerbation on decline in lung function in COPD. Respir Med. (2017) 128:85–91. doi: 10.1016/j.rmed.2017.04.013
46. Shah, T, Churpek, MM, Perraillon, MC, and Konetzka, RT. Understanding why patients with COPD get readmitted: a large national study to delineate the medicare population for the readmissions penalty expansion. Chest. (2015) 147:1219–26. doi: 10.1378/chest.14-2181
47. Alshabanat, A, Otterstatter, M, Sin, D, Road, J, Rempel, C, Burns, J, et al. Impact of a COPD comprehensive case management program on hospital length of stay and readmission rates. Int J COPD. (2017) 12:961–71. doi: 10.2147/COPD.S124385
48. Mohammadi, F, Jowkar, Z, Khankeh, HR, and Tafti, SF. Effect of home-based nursing pulmonary rehabilitation on patients with chronic obstructive pulmonary disease: A randomised clinical trial. Br J Community Nurs. (2013) 18:398–403. doi: 10.12968/bjcn.2013.18.8.398
49. Stickland, MK, Jourdain, T, Wong, EYL, Rodgers, WM, Jendzjowsky, NG, and MacDonald, GF. Using Telehealth technology to deliver pulmonary rehabilitation to patients with chronic obstructive pulmonary disease. Can Respir J. (2011) 18:216–20. doi: 10.1155/2011/640865
Keywords: COPD, continuity of patient care, healthcare utilization, patient journey, quality of care, standard of care
Citation: Ghamari S-H, Mohebi F, Abbasi-Kangevari M, Peiman S, Rahimi B, Ahmadi N, Farzi Y, Seyfi S, Shahbal N, Modirian M, Azmin M, Zokaei H, Khezrian M, Sherafat R, Malekpour M-R, Roshani S, Rezaei N, Fallahi MJ, Shoushtari MH, Akbaripour Z, Khatibzadeh S and Shahraz S (2023) Patient experience with chronic obstructive pulmonary disease: a nationally representative demonstration study on quality and cost of healthcare services. Front. Public Health 11:1112072. doi: 10.3389/fpubh.2023.1112072
Edited by:
Samuele Ceruti, Sant’Anna Clinic, SwitzerlandReviewed by:
Andrea Glotta, Ospedale Regionale di Lugano, SwitzerlandCopyright © 2023 Ghamari, Mohebi, Abbasi-Kangevari, Peiman, Rahimi, Ahmadi, Farzi, Seyfi, Shahbal, Modirian, Azmin, Zokaei, Khezrian, Sherafat, Malekpour, Roshani, Rezaei, Fallahi, Shoushtari, Akbaripour, Khatibzadeh and Shahraz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Saeid Shahraz, c2hhaHJhekBnbWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.