
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Public Health, 25 January 2023
Sec. Public Mental Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1100546
 Marianna Purgato1Giulia Turrini1
Marianna Purgato1Giulia Turrini1 Federico Tedeschi1Riccardo Serra1,2
Federico Tedeschi1Riccardo Serra1,2 Lorenzo Tarsitani2Beatrice Compri1Giulia Muriago1Camilla Cadorin1
Lorenzo Tarsitani2Beatrice Compri1Giulia Muriago1Camilla Cadorin1 Giovanni Ostuzzi1
Giovanni Ostuzzi1 Pablo Nicaise3
Pablo Nicaise3 Vincent Lorant3
Vincent Lorant3 Marit Sijbrandij4Anke B. Witteveen4
Marit Sijbrandij4Anke B. Witteveen4 José Luis Ayuso-Mateos5,6,7
José Luis Ayuso-Mateos5,6,7 Roberto Mediavilla5,6,8Josep Maria Haro6,9Mireia Felez-Nobrega6,9Natasha Figueiredo10Giulia Pollice10
Roberto Mediavilla5,6,8Josep Maria Haro6,9Mireia Felez-Nobrega6,9Natasha Figueiredo10Giulia Pollice10 David McDaid11
David McDaid11 A-La Park11Raffael Kalisch12,13Papoula Petri-Romão13James Underhill14
A-La Park11Raffael Kalisch12,13Papoula Petri-Romão13James Underhill14 Richard A. Bryant15Michela Nosè1
Richard A. Bryant15Michela Nosè1 Corrado Barbui1* on behalf of the RESPOND Consortium
Corrado Barbui1* on behalf of the RESPOND ConsortiumIntroduction: Migrant populations, including workers, undocumented migrants, asylum seekers, refugees, internationally displaced persons, and other populations on the move, are exposed to a variety of stressors and potentially traumatic events before, during, and after the migration process. In recent years, the COVID-19 pandemic has represented an additional stressor, especially for migrants on the move. As a consequence, migration may increase vulnerability of individuals toward a worsening of subjective wellbeing, quality of life, and mental health, which, in turn, may increase the risk of developing mental health conditions. Against this background, we designed a stepped-care programme consisting of two scalable psychological interventions developed by the World Health Organization and locally adapted for migrant populations. The effectiveness and cost-effectiveness of this stepped-care programme will be assessed in terms of mental health outcomes, resilience, wellbeing, and costs to healthcare systems.
Methods and analysis: We present the study protocol for a pragmatic randomized study with a parallel-group design that will enroll participants with a migrant background and elevated level of psychological distress. Participants will be randomized to care as usual only or to care a usual plus a guided self-help stress management guide (Doing What Matters in Times of Stress, DWM) and a five-session cognitive behavioral intervention (Problem Management Plus, PM+). Participants will self-report all measures at baseline before random allocation, 2 weeks after DWM delivery, 1 week after PM+ delivery and 2 months after PM+ delivery. All participants will receive a single-session of a support intervention, namely Psychological First Aid. We will include 212 participants. An intention-to-treat analysis using linear mixed models will be conducted to explore the programme's effect on anxiety and depression symptoms, as measured by the Patient Health Questionnaire—Anxiety and Depression Scale summary score 2 months after PM+ delivery. Secondary outcomes include post-traumatic stress disorder symptoms, resilience, quality of life, resource utilization, cost, and cost-effectiveness.
Discussion: This study is the first randomized controlled trial that combines two World Health Organization psychological interventions tailored for migrant populations with an elevated level of psychological distress. The present study will make available DWM/PM+ packages adapted for remote delivery following a task-shifting approach, and will generate evidence to inform policy responses based on a more efficient use of resources for improving resilience, wellbeing and mental health.
Clinical trial registration: ClinicalTrials.gov, identifier: NCT04993534.
The concept of migration refers to the process of moving from one country, region, or place to another one (1). As part of this concept, migration may occur within a country or across an international border, temporarily or permanently, and for a variety of reasons (2). The European Psychiatric Association guidance on mental health care of migrants has grouped reasons for migration in pull and push factors (1). Pull factors include educational or economic growth or personal factors, while push factors include political, poverty, terrorism, displacement, war or religious factors. Migrant is therefore an umbrella term, without any formal recognition under international laws, that generally includes a variety of different populations such as migrant workers, undocumented migrants, asylum seekers, refugees, internally displaced persons, and other populations on the move (1, 3).
Italy represents one of the first countries reached by migrants in the attempt to arrive in Europe. Over the last decades migration figures have fluctuated, with a peak in arrivals in 2016 (4). The number of arrivals reached 34 thousand in 2020 and almost 60 thousand in 2021 (4). UNHCR data indicates that, at the end of 2021, Italy hosted over 165 thousand forced migrants with a refugee status or requesting asylum (5). Most migrants arrived from Nigeria, Pakistan, Afghanistan, Mali, Somalia, and Gambia (4). According to the Italian reception system, after arrival, migrants are included in reception programmes that include food, housing, legal, and social guidance and support, and the development of individual interventions to promote socioeconomic inclusion and integration (6, 7).
During the migration process there may be factors that increase the vulnerability of individuals toward a worsening of subjective wellbeing, quality of life, and mental health, which, in turn, may increase the risk of developing mental health conditions. A discrepancy between expectations and achievements, poor support networks, difficulties in the processes of adjustment and acculturation, financial, administrative and legal issues, are commonly experienced stressors and living difficulties occurring during and after the migration process. Forcibly displaced migrants may additionally experience the loss of homes, hopes, possessions, and may be exposed to potentially traumatic events such as bombings, threats, captivity, torture, injury, and witnessing the death or injury of loved ones (8–11). After arrival in host countries major threats may include discrimination, economic problems, language barriers, loss of family and community support, poor access to social, educational and health services, and uncertain asylum application procedures (12). Notably, the COVID-19 pandemic has represented an additional stressor for migrant populations (13).
Epidemiological studies have documented that pre, during, and post migration stressors and potentially traumatic events are responsible for a high prevalence of psychological distress and mental health conditions in migrant populations, with differences related to reasons for migration, number and type of traumatic events, and time since resettlement (14–18).
In recent years, a growing number of randomized studies, and subsequently systematic reviews and meta-analyses, have documented the efficacy of psychological and psychosocial interventions on mental health outcomes in migrant populations, especially refugees and asylum seekers (19–21). However, these interventions require extensive training and considerable time to be delivered, staff with a mental health background, a monitoring and supervision infrastructure, and a face-to-face individual delivery modality in most cases. As these characteristics make them unlikely to be highly implemented, and unsuitable to address the needs of many people in a way that maximizes the use of resources, the World Health Organization (WHO) has developed a number of scalable psychological interventions for populations affected by adversity (22). A core feature of these interventions is that they can be trained and delivered by non-professional helpers, such as a trained peer, or helper at the workplace, or a psychosocial worker, following a task-shifting approach where tasks are moved from highly qualified health workers to health workers who have fewer qualifications in order to make more efficient use of the available resources (23). They are generally short in duration and highly protocolized, which makes them easy to be delivered by non-professional helpers. They have also been designed to be widely applicable to a variety of mental health problems irrespective of the presence of a mental health diagnosis, and easily adaptable to different populations, cultures and languages. Finally, the interventions and their implementation materials are open access, and they can be delivered through a variety of delivery modalities, including the use of digital technologies such as mobile phone or laptop or other.
In the present study, we designed a stepped-care programme of two scalable psychological interventions developed by the WHO and locally adapted for migrant populations. The first step consists of a mobile-supported website with a guided self-help programme, adapted from Self Help Plus (SH+), called Doing What matters in times of Stress (DWM) (24, 25). The second step is Problem Management Plus (PM+), an individual intervention based on problem-solving and cognitive behavioral therapy techniques delivered individually through video calls and offered only to participants who continue to show elevated levels of psychological distress after step 1 (26, 27). Both interventions have proved effective in humanitarian settings (28–35), but they have not been integrated into an online stepped-care programme.
The study aim is to evaluate the effectiveness and cost-effectiveness of the culturally and contextually adapted DWM/PM+ stepped-care programme among migrants resettled in Italy during the COVID-19 pandemic in terms of mental health outcomes (depression, anxiety and PTSD), resilience, wellbeing, self-identified problems, quality of life, and socio-economic impacts. We hypothesize a stronger decrease in anxiety and depression symptoms in the experimental arm, receiving the adapted DWM/PM+ stepped-care programme, as compared with the control arm, receiving care-as-usual (CAU).
The study is part of an EU-funded project named “Improving the Preparedness of Health Systems to Reduce Mental health and Psychosocial Concerns resulting from the COVID-19 Pandemic” (RESPOND) (www.respond-project.eu). Participants will be randomized to the adapted stepped-care DWM/PM+ intervention together with psychological first aid (PFA) or to PFA and CAU alone. Participants will self-report all measures at baseline before random allocation, 2 weeks after DWM delivery, 1 week after PM+ delivery and 2 months after PM+ delivery.
The present trial focuses on participants with a migrant background and elevated level of psychological distress, and it is coordinated by the WHO Collaborating Center of the University of Verona. We are currently recruiting participants through (a) key stakeholders such as non-governmental organizations (NGOs) located in Italy, (b) other community-based organizations offering legal and/or social and/or psychosocial support to this vulnerable group, or (c) targeted social media recruitment. Investigators proactively approached local organizations providing social, health, and/or legal support to migrant populations including refugees and asylum seekers to identify potentially eligible participants.
An Ethics and Data Advisory Board (EDAB) will monitor and provide expert advice on data management and all ethical, legal and societal issues that arise within the project, promoting integrity and a better alignment of RESPOND with social needs and expectations that may arise within or as a result of RESPOND. The study will be reported in accordance with the Consolidated Standards of Reporting Trials statement (36).
Participants will be eligible to participate in the study if they meet the following criteria:
• 18 years or older;
• Being a migrant resettled in Italy temporarily or permanently (including migrant workers, undocumented migrants, asylum seekers, refugees, internationally displaced persons, or other persons on the move);
• Having elevated levels of psychological distress [Kessler Psychological Distress Scale (K10) >15.9] (37);
• Sufficient mastery (written and spoken) of one of the languages the DWM/PM+ intervention is being delivered in (English, Italian, French);
• Oral and written informed consent before entering the study.
Potential participants who meet the inclusion criteria will be excluded from participation in this study if they meet any of the following criteria:
• Acute medical conditions that require hospitalization;
• Imminent suicide risk, or expressed acute needs or protection risks that require immediate follow-up;
• Severe mental disorder (e.g., psychotic disorder);
• Severe cognitive impairment (e.g., severe intellectual disability or dementia);
• Initiated, stopped, or significantly modified psychiatric drug treatment over the previous 2 months;
• Currently receiving specialized psychological treatment (e.g., Cognitive Behavioral treatment, Eye Movement Desensitization and Reprocessing);
• Planning to permanently move back to their home country before the last quantitative follow-up assessment (2 months after PM+).
Before being enrolled in the study, people who are interested will be informed using easily accessible language and terminology about the nature and scope of the study in a form understandable to them. A research assistant will explain the research and will provide the study materials. People agreeing to participate will be asked to complete a written consent form, offering a minimum consideration time of 1 week, before screening for inclusion and exclusion criteria. Participants meeting the inclusion criteria will be included in the randomized study. We will inform participants of the reasons why they can or cannot be included in the study. Participants will be asked to sign a second informed consent form, covering the optional recording of PM+ sessions, in case of PM+ administration. However, giving consent for the audio recordings will not be a condition for participating in the study. Audio recordings will only be used for fidelity assessments and supervisions.
Eligible participants will be randomly assigned with an equal probability of assignment to one of the two groups (allocation ratio 1:1). The randomization schedule will be generated using the web-based software Castor Electronic Data Capture (38). This electronic tool employs a variable block randomization method, in order to allocate groups randomly permuted in blocks of unequal size. The site investigators will not know the block size and will not be able to access the randomization list. In addition, the web-based software will allow random allocation only after the main information on the enrolled participant is entered, on verification of the inclusion criteria.
Psychological distress will be measures using the K10 (37). The K10 is a ten-item self-report questionnaire to screen broadly for psychological distress (e.g., anxiety and depression related distress) experienced in the past 30 days. Items are rated on a five-point Likert scale ranging from none of the time to all of the time. The sum of the ten items gives a total score ranging from 10 to 50. Higher scores represent higher levels of distress. The K10 has strong psychometric properties and has strong discriminatory power to distinguish DSM-IV cases from non-cases (37).
Suicidality will be explored with the ‘assessment of suicidal thoughts' risk tool from PM+ (26). Similarly, suspicion of a severe mental disorder and cognitive impairment will be assessed using the PM+ tool “Impairments possibly due to severe mental, neurological or substance use disorders” (26). This is a tool which is to be filled in by the assessor based on their observations and judgment of the client's behaviors. A judgment on four yes/no items that investigate the possibility of symptoms of severe mental, neurological, or substance use disorder is required. No questions are asked to the participant. The tool does not allow to make any diagnosis, but only indicates suspicion of a disorder.
Participants in the intervention arm will be offered a stepped care programme consisting of two scalable psychological interventions: DWM and PM+. All participants, both in the intervention and control group, will be offered a short counseling session, namely PFA, and will also maintain their care as usual.
The delivery of DWM, PM+ and PFA will be facilitated by peer helpers with at least primary school level literacy as well as good knowledge and skills in providing psychosocial support. Helpers will speak the same language as the participants (as well as being able to communicate in English). It is not necessary for helpers to have a psychosocial or mental health background in order to be able to offer these interventions. Necessary skills include foundational helping skills, such as effective community and rapport-building skills, and experience supporting people in distress. Helpers will receive training in delivering PFA, DWM, and PM+ by registered clinical psychologists trained by the WHO, and will receive continuous supervision throughout the study period.
Before randomization, all participants will be offered individual Psychological First Aid (PFA) through a phone call or teleconferencing meeting with a research assistant (39). PFA is a WHO developed support strategy that involves humane, supportive and practical help for individuals who have been affected by serious humanitarian crises. PFA does not necessarily involve a discussion of the event(s) that cause the distress but aims particularly at five basic elements that are crucial to promote in the aftermath of crises, i.e., a sense of safety, calm, self- and community efficacy, connectedness, and hope. PFA consists of a conversation (up to 30–45 min) on various themes; in PFA, the helper provides non-intruding practical care and support, assesses needs and concerns, helps people to address basic needs (e.g., information), listens to people without pressuring them to talk, comforts and helps them to feel calm, as well as helping them to connect to information, services, and social support, and protects them from further harm.
In addition to PFA, both the intervention and control group will receive care-as-usual (CAU). CAU may include community care, social/legal support, psychoeducation, information about locally available referral options and about specific resources that might be helpful (e.g., hotlines for people in distress or experiencing loneliness, or support for women who might be experiencing gender-based violence).
Participants randomized to the intervention group will be offered DWM (24, 25). DWM is a booklet, adapted into a mobile website, divided into five monographic chapters covering five acceptance- and mindfulness-based strategies for managing stress. Chapters include audio recordings with different practices and exercises that help participants identify barriers and facilitators for practicing or triggers that exacerbate stress responses. During the local adaptation process undertaken in RESPOND, we adapted exercises to reflect barriers or stress triggers that might affect migrants resettled in Italy.
After allocation, DWM users will be assigned to a helper who will offer ongoing support with practical exercises and key concepts over the phone. An initial call will be arranged 2–5 days after entering the study. After that call, the participant receives a message with login details. The course is spread over 5 weeks, and new modules are released every week. Helpers also schedule weekly ongoing support calls. Support calls will take no longer than 15 min per call. The aim of the calls is to provide motivation and support in using the intervention. Participants who do not want to receive phone calls might contact their helpers using the messaging system included in the website. We will keep track of every helper-participant contact and use website metadata on participants' activity.
PM+ will be offered to participants reporting significant levels of psychological distress after DWM, as measured by a K10 score higher than 15.9. PM+ is a brief five-session psychological intervention based on cognitive behavioral therapy techniques (26, 27). Helpers will schedule 5 weekly sessions covering each strategy. As a result of the local adaptation process, we have adapted PM+ to be delivered online using teleconferencing tools, and shortened sessions from 90 to 60 min. Helpers will record the calls to monitor fidelity and go through identified barriers during practice over the week.
Participants will be asked to complete online questionnaires at the following assessments: T0: screening for eligibility including psychological distress (before random allocation); T1: baseline assessment (before random allocation and PFA provision); T2: 2 weeks after DWM delivery; T3: 1 week after PM+ delivery; T4: 2 months after PM+ delivery. The primary outcome will be the change in symptoms of depression and anxiety from baseline to 2 months after the PM+ intervention, measured through the combined sum score of the Patient Health Questionnaire-9 (PHQ-9) (40, 41) and Generalized Anxiety Disorder (GAD-7) (42), previously validated as the PHQ-ADS (43).
In addition, the following measures will be considered secondary outcomes: depression (PHQ-9); anxiety (GAD-7); posttraumatic stress disorder (PCL-5) (44); self-identified problems (PSYCHLOPS) (45); resilience, operationalised as mental health after stressor exposure (46); quality of life (EQ-5D-5L) (47); resource use and economic outcomes, collected using a modified version of the Client Service Receipt Inventory (CSRI) (48). The CSRI includes information on the use of healthcare and other services, time out of employment and other usual activities and the need for informal care.
Additional study parameters include the following: demographic data; COVID-19 exposure questionnaire; Positive Appraisal Style Scale, content focused (PASS-content) (46); exposure to adverse life-events (BTQ questionnaire) (49); treatment fidelity (DWM: tracking app usage based on meta-data, PM+: audio records, checklists); satisfaction (qualitative assessment); acceptability of the programme (qualitative assessment); adverse events; implementation indicators: reach, dose, resource use, costs of recruiting, training and retaining staff delivering the stepped-care programme, programme costs, adaptation, and quality. An overview of measures and the time periods when they are collected is presented in Table 1.
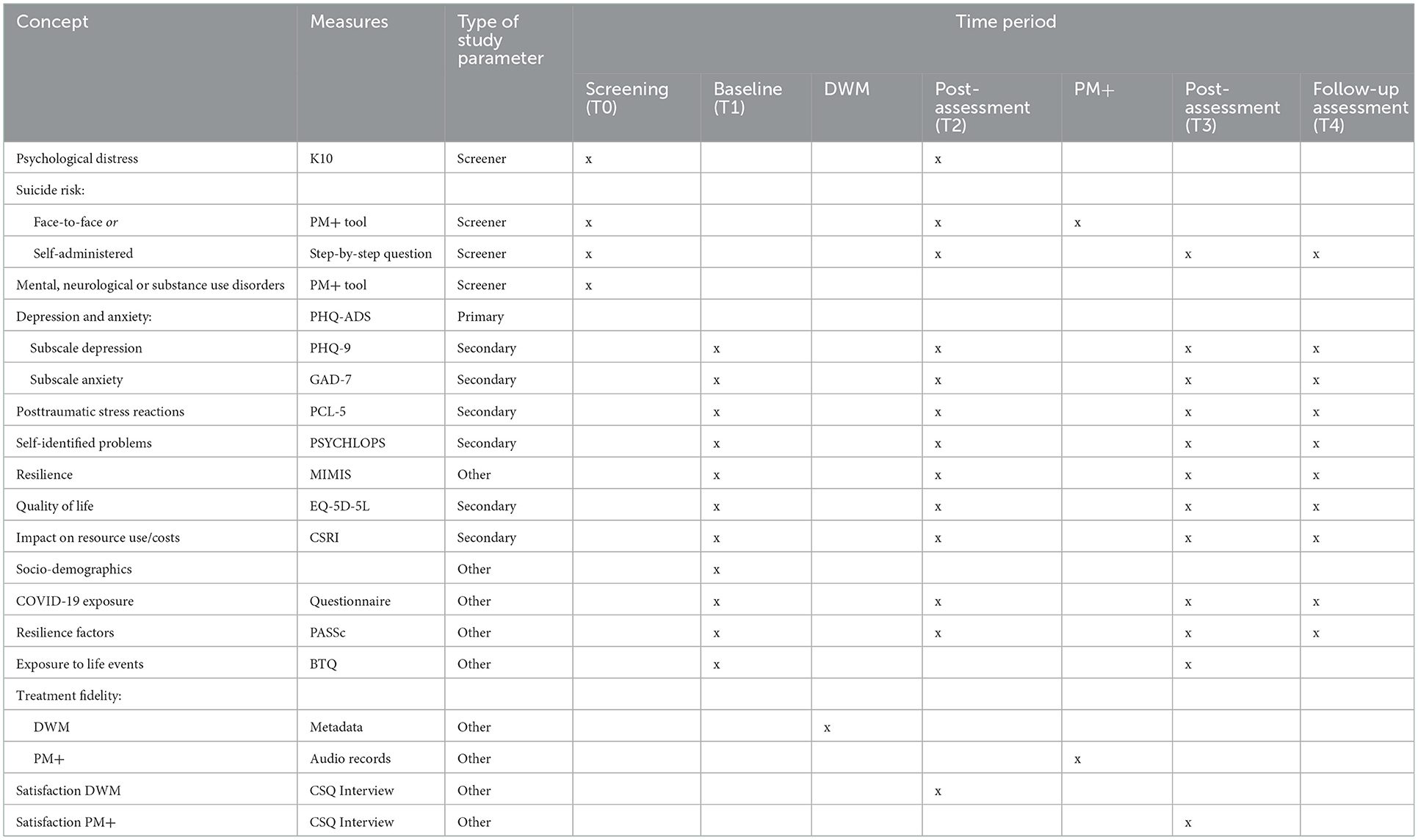
Table 1. Overview of concepts, measures, type of study parameter and time periods when they are collected.
The PHQ-ADS is a 16-item self-reported instrument that combines the nine-item Patient Health Questionnaire depression scale (PHQ-9) and seven-item Generalized Anxiety Disorder scale (GAD-7) into a composite measure of depression and anxiety (43). Respondents are asked about how much each symptom has bothered them over the past 2 weeks, with response options of “not at all,” “several days,” “more than half the days,” and “nearly every day,” scored as 0, 1, 2, and 3. The scale can range from 0 to 48, with higher scores indicating higher levels of depression and anxiety symptoms.
The eight-item PCL-5 is a self-reported instrument that measures PTSD symptoms (44). Respondents are asked how much each symptom has bothered them over the past 4 weeks, with response options of “not at all,” “a little bit,” “moderately,” “quite a bit,” and “extremely.” Items are rated on a 0–4 scale. The scale can range from 0 to 32 for the 8-item version, with higher scores indicating higher levels of PTSD symptoms.
The Psychological Outcomes Profiles (PSYCHLOPS) scale is a patient-generated outcome measure as an indicator of change after therapy (45). PSYCHLOPS consists of three domains: problems (two questions), function (one question), and wellbeing (one question). Participants are asked to give free text responses to the problem and function domains. Responses are scored on an ordinal six-point scale producing a maximum score of 18 (six points per domain).
Resilience can be defined as maintaining or recovering good mental health after facing adversity (46), which requires collecting information on mental health symptoms and exposure to stressors. To this end, a new measure of stressor exposure was developed, aimed to assess stressors particular to the study population. This measure was based on an adaptation of the Mainz Inventory of Micro stressors (MIMIS) (50), an objective measure of micro-stressors or daily hassles. After the COVID-19 outbreak, a shorter version, including pandemic-related stressors, was developed (51). In RESPOND qualitative interviews of the target population further informed which stressors participants were likely to encounter. The resulting measure consists of 22-item adaptation that includes: three general life events (e.g., recent break-up); six everyday stressors (e.g., excessive workload, financial problems); five COVID-19-specific stressors (e.g., being forced to quarantine); and eight refugee and migrant population specific stressors [e.g., Lack of access to services (for example: health services, etc.)]. Participants are asked to rate general life events that occurred in the past 2 months on a 5-point Likert scale, ranging from 0 (“never happened”) to 4 (“it had a major impact on me”). The remaining 19 items are rated on a 4-point Likert scale, ranging from 0 (“did not happen/almost never”) to 3 (“every day or nearly every day”). These items ask about the last 14 days.
The EQ-5D-5L consists of the EQ-5D and the EQ-Visual Analog Scale (VAS) (47). It rates the level of impairment across five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has five levels: none, slight, moderate, severe, and extreme problems. The labels for the 5L followed the format “no problems,” “slight problems,” “moderate problems,” “severe problems,” and “unable to”/“extreme problems” for all dimensions. The EQ-VAS, is measured from 0 (the worst imaginable health, not necessarily death) to 100 (the best imaginable health state). The endpoints of the scale are called “The best health you can imagine” and “The worst health you can imagine,” and the current health status of that day needs to be indicated, after which the number checked on the scale also needs to be written down. Higher scores indicate better quality of life.
An adapted version of the CSRI in Italian will be used to estimate changes in resource use. Appropriate unit costs will be used to estimate the costs of this resource used estimate. The RESPOND-adapted version used in Italy consists of a 13-item self-reported instrument that asks about the number and duration of contacts with healthcare professionals (physicians, mental health specialists, and nurses) in the past 2 months. It collects data on service utilization (e.g., use of health care and other services, time out of employment and other usual activities, need for informal care) and related characteristics of people with mental health problems.
The COVID-19 exposure questionnaire includes 11 questions related to the impact of COVID-19. The questionnaire is based on other COVID-19 questionnaires. It will be administered at each time-point.
The PASS-content is a measure of a person's general tendency of how they appraise stressors that they encounter; their positive appraisal style (PAS) (46). The 12-item questionnaire, asks the participant to report how frequently they have specific thoughts when facing adversity on a 4-point Likert scale from 1 = never to 4 = (almost) always (e.g., “I think that the situation also has its positive sides”). This measure was included at each time-point.
The Brief Trauma Questionnaire (BTQ) is a brief self- report questionnaire that is derived from the Brief Trauma Interview (49). The BTQ was originally designed to assess traumatic exposure according to DSM-IV but specifically asked only about Criterion A.1 (life threat/serious injury) because of the difficulty of accurately assessing A.2 (subjective response) in a brief self-report format. Criterion A.2 has been eliminated from the PTSD diagnostic criteria in DSM-5, so the BTQ provides a complete assessment of Criterion A. The questionnaire may be used to determine whether an individual has had an event that meets the A Criterion, or to determine the different types of Criterion A events an individual has experienced.
Adverse events are defined as any undesirable experience occurring to a participant during the study, whether or not considered related to the trial procedure or the stepped-care DWM/PM+ intervention. All adverse events reported spontaneously by study participants or observed by the investigators will be recorded and reported to the EDAB.
We will conduct in-depth interviews with key informants to assess the feasibility of programme implementation. We will select informants among completers and non-completers of DWM and PM+ interventions. We will also conduct interviews and focus group interviews with participants' relatives.
Masking participants and helpers about the intervention status will be impossible, due to the nature of the intervention. In addition, as the study does not include any observer-reported outcomes, it cannot include any masked outcome assessor. However, the statistician performing the analyses will be masked to the participants' allocation.
Based on prior studies on PM+ (32, 52), we aim to detect a small to medium Cohen's d effect size of 0.3 in the PM+ group at 2 months post-intervention based on the primary composite outcome PHQ-ADS. A power calculation for a repeated measurement design suggests a minimum sample size of N = 74 per group (power = 0.95, alpha = 0.05, two-sided, rho = 0.9) to identify an effect at the time of interest. Assuming an attrition rate of 30%, we aim to include a total number of 212 participants [106 in the stepped-care DWM/PM+ intervention group (with PFA and CAU) and 106 in the PFA and CAU comparison group].
All primary and secondary analyses will be performed on an intention-to-treat (ITT) basis. The ITT population will consist of all participants randomly assigned to the competitive intervention strategies and with at least data on the baseline assessment available. In order to check the robustness of results, all outcomes will be additionally analyzed using a per protocol (PP) approach, that will include only DWM participants clicking through all of the content of at least 3 modules (regardless of whether or not they engage in phone calls/messages with the helper) and PM+ participants attending at least 4 sessions. The analysis of the PP population will be used for confirmatory purposes only. If < 5% of participants do not receive the allocated intervention according to the study protocol, the PP analysis will not be performed.
The primary outcome will be summarized using number of subjects (n), minimum and maximum; and means, standard deviations (SD) for normally distributed data, or medians and inter-quartile ranges for non-normally distributed data. To compare the two treatment groups at baseline, standardized mean differences will be calculated. The primary analysis will simultaneously assess treatment effect on the average PHQ-ADS score at each time-point in the ITT population. The main conclusion of the trial will be based on the ITT analysis of the primary outcome (i.e., the effect on PHQ-ADS score at the 2-month follow-up). To estimate the treatment effect for the time-points T2, T3, and T4, a linear mixed model will be employed for the analysis on PHQ-ADS, which will have time as a fixed effect, baseline measurement of PHQ-ADS as covariate, and subject as random effects. Our model will be re-parametrized by constraining the treatment fixed-effect to be 0, and by including a time*treatment interaction at T2 as well. In this way, in each time-point, the treatment effect will be measured as the interaction between time (as a categorical variable) and treatment, with its value at T4 being our outcome of interest. The mean difference between two treatment arms at each visit/time together with its 95% confidence interval will be derived from the mixed model. In addition, a covariate-adjusted mixed model of primary outcome will be performed by adding covariates showing imbalance at baseline (as measured by a Standardized Mean Difference above 0.1 in absolute value). Robust standard errors will be used in all models.
A secondary analysis of the effect of treatment on PHQ-ADS score will be conducted using the per protocol (PP) population, using the same approach as reported above. In addition, a covariate-adjusted mixed model of primary outcome will be performed using the PP population by adding pre-specified covariates at baseline (gender, age, education, prior trauma, COVID-19 related events and the stressor exposure).
Missing data will be treated as missing at random (MAR). No imputations of missing values will be made, as multilevel models can deal with missing data (53). In the case only some items are missing for a specific scale, we will perform the Corrected Item mean Substitution method (i.e., the item mean across participants weighted by the subject's mean of completed items) (54), using information from subjects belonging to the same treatment arm for the same follow-up time (estimated values above the maximum or below the minimum admissible value will be set to maximum/minimum).
A linear mixed model with robust standard errors, as mentioned for the primary analysis, will be carried out to analyse the following secondary outcomes: depressive symptoms (PHQ-9), generalized anxiety (GAD-7); posttraumatic stress reactions (PCL-5), self-identified problems (PSYCHLOPS), and quality of life (EQ-5D-5L), as well as outcome-based resilience, operationalised as the PHQ-ADS total score against stressor exposure count (55). The secondary outcomes will be analyzed on the ITT population only. Further, mediation analyses including positive appraisal style (PASS-content) and the primary and secondary outcomes will be conducted.
Health economic analysis will be conducted from both a health care and societal perspective. It will determine the cost effectiveness of intervention compared to care as usual over the study period. The primary outcome measure for the economic analysis will be incremental cost per QALY gained at 2-month follow-up. This involves synthesis of data on quality of life using an Italian specific valuation of health states, as well as data on the costs of interventions and subsequent resource utilization in the two trials. Between-group comparison of mean costs will be completed using appropriate statistical tests depending on the type and distribution of data. Univariate sensitivity analyses, using non-parametric bootstrapping to account for uncertainty around cost and effectiveness in trial parameters, will be performed by varying the costs of interventions. Cost effectiveness planes and cost effectiveness acceptability curves will be presented.
The results of this randomized trial will be considered together with the results of three other trials that are being conducted using the same study design, but focussing on different vulnerable groups, as part of the RESPOND programme. While the present study has a focus on migrants including refugees and asylum seekers resettled in Italy, health-care workers is the target population of a study conducted in Spain (56), people living in social adversity conditions are being recruited in France, and in the Netherlands labor migrants are the target population. Taken together, these studies will quantify the beneficial effects of stepped-care psychological interventions in a wide range of populations exposed to COVID-19 related psychological distress or other types of stressors, and will make available DWM/PM+ packages adapted for remote delivery following a task-shifting approach. Through wide dissemination of the results of these studies, we aim to suggest policy responses based on a more efficient use of resources for improving resilience, wellbeing and poor mental health. Our vision is that these stepped care psychological interventions could be integrated into holistic response to future COVID-19 waves or future epidemics or health crises related to war or other humanitarian or economic emergencies.
As part of the RESPOND programme, studies conducted across vulnerable groups will be combined to reliably detect predictors and moderators for the effects of the DWM/PM+ programme. This is expected to generate unique information for future personalized delivery of mental health care.
The protocol, informed consent form, procedure to obtain consent, and the procedure to protect confidentiality of personal data of this trial was approved the Comitato Etico per la Sperimentazione Clinica delle province di Verona e Rovigo, Approval ID 46725 of 10/08/2021, and are registered in Clinicaltrial.gov (ClinicalTrials.gov Identifier: NCT04993534). Any amendments on the protocol will be communicated though updating in the public webpage of the Trial Registry. The funder has no role in study design; collection, management, analysis, and interpretation of data; writing of the report; and the decision to submit the report for publication. The results of this trial will be published in peer-reviewed journal articles and the final trial dataset will be made available after de-identification of the participants.
All data will be handled confidentially and will be coded by a code known only by the research team. Processing of personal data will comply to the General Data Regulation (“GDPR”) on the protection of individuals regarding the processing of personal data and the free movement of such data. Data including personal information will be stored in a locked record at the WHO Collaborating Center of the University of Verona to ensure the confidentiality of the study participants. Only authorized research personnel will have access to this data. According to the data management rules of RESPOND, all partners acknowledge and agree that no personal data, as defined in Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation) (“GDPR”), will be exchanged between the Parties. Moreover, all partners in RESPOND acknowledge and agree that each partner is considered independent controller, as defined in GDPR, for its processing of personal data and will act in accordance with applicable data protection laws (including but not limited to GDPR).
The study protocol was approved by the Comitato Etico per la Sperimentazione Clinica delle province di Verona e Rovigo, Approval ID 46725 of 10/08/2021. The patients/participants provided their written informed consent to participate in this study.
CB and MP drafted this manuscript, and all authors contributed to review and editing. All authors contributed to conceptualization, methodology, data curation, and protocol development. All authors approved the final version.
The RESPOND project is funded under Horizon 2020—the Framework Programme for Research and Innovation (2014–2020) (Grant number: 101016127—RESPOND). The content of this article reflects only the authors' views and the European Community is not liable for any use that may be made of the information contained therein.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1100546/full#supplementary-material
1. Bhugra D, Gupta S, Schouler-Ocak M, Graeff-Calliess I, Deakin NA, Qureshi A, et al. EPA guidance mental health care of migrants. Eur Psychiatry. (2014) 29:107–15. doi: 10.1016/j.eurpsy.2014.01.003
2. Abubakar I, Aldridge RW, Devakumar D, Orcutt M, Burns R, Barreto ML, et al. The UCL-lancet commission on migration and health: the health of a world on the move. Lancet. (2018) 392:2606–54. doi: 10.1016/S0140-6736(18)32114-7
3. Bhugra D, Gupta S, Bhui K, Craig T, Dogra N, Ingleby JD, et al. WPA guidance on mental health and mental health care in migrants. World Psychiatry. (2011) 10:2–10. doi: 10.1002/j.2051-5545.2011.tb00002.x
4. Statista. Migration to Italy—Statistics and Facts. Hamburg: Statista (2021). Available online at: https://www.statista.com/topics/5899/migration-to-italy/#topicHeader__wrapper (accessed December 15, 2022).
5. UNHCR. Refugee Data Finder. Washington, DC: UNHCR (2022). Available online at: https://www.unhcr.org/refugee-statistics/ (accessed December 15, 2022).
6. Cristofalo D, Bonetto C, Ballarin M, Amaddeo F, Ruggeri M, Nose M, et al. Access to and use of psychiatric services by migrants resettled in Northern Italy. J Immigr Minor Health. (2018) 20:1309–16. doi: 10.1007/s10903-018-0703-z
7. Nose M, Tarsitani L, Tedeschi F, Lotito C, Massetti P, Purgato M, et al. Association of traumatic events with levels of psychological distress and depressive symptoms in male asylum seekers and refugees resettled in Italy. BMC Psychiatry. (2020) 20:576. doi: 10.1186/s12888-020-02988-0
8. Inter-Agency Standing Committee,. IASC Guidelines on Mental Health Psychosocial Support in Emergency Settings. New York, NY: Inter-Agency Standing Committee (2007). Available online at: https://interagencystandingcommittee.org/system/files/Checklist%2520for%2520field%2520use%2520IASC%2520MHPSS.pdf (accessed December 15, 2022).
9. Jannesari S, Hatch S, Oram S. Seeking sanctuary: rethinking asylum and mental health. Epidemiol Psychiatr Sci. (2020) 29:e154. doi: 10.1017/S2045796020000669
10. Ceccarelli C, Prina E, Muneghina O, Jordans M, Barker E, Miller K, et al. Adverse childhood experiences and global mental health: avenues to reduce the burden of child and adolescent mental disorders. Epidemiol Psychiatr Sci. (2022) 31:e75. doi: 10.1017/S2045796022000580
11. Barbui C, Purgato M, Acarturk C, Churchill R, Cuijpers P, Koesters M, et al. Preventing the mental health consequences of war in refugee populations. Epidemiol Psychiatr Sci. (2022) 31:e24. doi: 10.1017/S2045796022000154
12. Sijbrandij M. Expanding the evidence: key priorities for research on mental health interventions for refugees in high-income countries. Epidemiol Psychiatr Sci. (2018) 27:105–8. doi: 10.1017/S2045796017000713
13. Inter-Agency Standing Committee,. IASC Guidance on Operational Considerations for Multisectoral Mental Health Psychosocial Support Programmes During the COVID-19 Pandemic. New York, NY: Inter-Agency Standing Committee (2020). Available online at: https://interagencystandingcommittee.org/system/files/2020-06/IASC%20Guidance%20on%20Operational%20considerations%20for%20Multisectoral%20MHPSS%20Programmes%20during%20the%20COVID-19%20Pandemic.pdf (accessed December 15, 2022).
14. Hasan SI, Yee A, Rinaldi A, Azham AA, Mohd Hairi F, Amer Nordin AS. Prevalence of common mental health issues among migrant workers: a systematic review and meta-analysis. PLoS ONE. (2021) 16:e0260221. doi: 10.1371/journal.pone.0260221
15. Martin F, Sashidharan SP. The mental health of adult irregular migrants to Europe: a systematic review. J Immigr Minor Health. (2022) 15:1–9. doi: 10.1007/s10903-022-01379-9
16. Blackmore R, Boyle JA, Fazel M, Ranasinha S, Gray KM, Fitzgerald G, et al. The prevalence of mental illness in refugees and asylum seekers: a systematic review and meta-analysis. PLoS Med. (2020) 17:e1003337. doi: 10.1371/journal.pmed.1003337
17. Henkelmann JR, de Best S, Deckers C, Jensen K, Shahab M, Elzinga B, et al. Anxiety, depression and post-traumatic stress disorder in refugees resettling in high-income countries: systematic review and meta-analysis. BJPsych Open. (2020) 6:e68. doi: 10.1192/bjo.2020.54
18. Mesa-Vieira C, Haas AD, Buitrago-Garcia D, Roa-Diaz ZM, Minder B, Gamba M, et al. Mental health of migrants with pre-migration exposure to armed conflict: a systematic review and meta-analysis. Lancet Public Health. (2022) 7:e469–e81. doi: 10.1016/S2468-2667(22)00061-5
19. Turrini G, Tedeschi F, Cuijpers P, Del Giovane C, Kip A, Morina N, et al. A network meta-analysis of psychosocial interventions for refugees and asylum seekers with PTSD. BMJ Glob Health. (2021) 6:29. doi: 10.1136/bmjgh-2021-005029
20. Uphoff E, Robertson L, Cabieses B, Villalon FJ, Purgato M, Churchill R, et al. An overview of systematic reviews on mental health promotion, prevention, and treatment of common mental disorders for refugees, asylum seekers, and internally displaced persons. Cochrane Database Syst Rev. (2020) 9:CD013458. doi: 10.1002/14651858.CD013458.pub2
21. Turrini G, Purgato M, Acarturk C, Anttila M, Au T, Ballette F, et al. Efficacy and acceptability of psychosocial interventions in asylum seekers and refugees: systematic review and meta-analysis. Epidemiol Psychiatr Sci. (2019) 28:376–88. doi: 10.1017/S2045796019000027
22. World Health Organization. Scalable Psychological Interventions for People in Communities Affected by Adversity. Geneva: World Health Organziation (2017). Available online at: https://apps.who.int/iris/bitstream/handle/10665/254581/WHO-MSD-MER-17.1-eng.pdf (accessed December 15, 2022).
23. World Health Organization. Task Shifting. Global Recommendations and Guidelines. Geneva: World Health Organziation (2008). Available online at: https://apps.who.int/iris/bitstream/handle/10665/43821/9789241596312_eng.pdf (accessed December 15, 2022).
24. World Health Organization. Doing What Matters in Times of Stress. Geneva: World Health Organziation (2021). Available online at: https://apps.who.int/iris/bitstream/handle/10665/331901/9789240003910-eng.pdf (accessed December 15, 2022).
25. Epping-Jordan JE, Harris R, Brown FL, Carswell K, Foley C, Garcia-Moreno C, et al. Self-help plus (SH+): a new WHO stress management package. World Psychiatry. (2016) 15:295–6. doi: 10.1002/wps.20355
26. World Health Organization. Problem Management Plus (PM+): Individual Psychological Help for Adults Impaired by Distress in Communities Exposed to Adversity. Geneva: World Health Organziation (2018). Available online at: https://apps.who.int/iris/bitstream/handle/10665/206417/WHO_MSD_MER_16.2_eng.pdf?sequence=1 (accessed December 15, 2022).
27. Dawson KS, Bryant RA, Harper M, Kuowei Tay A, Rahman A, Schafer A, et al. Problem management plus (PM+): a WHO transdiagnostic psychological intervention for common mental health problems. World Psychiatry. (2015) 14:354–7. doi: 10.1002/wps.20255
28. Tol WA, Leku MR, Lakin DP, Carswell K, Augustinavicius J, Adaku A, et al. Guided self-help to reduce psychological distress in South Sudanese female refugees in Uganda: a cluster randomized trial. Lancet Glob Health. (2020) 8:e254–e63. doi: 10.1016/S2214-109X(19)30504-2
29. Purgato M, Carswell K, Tedeschi F, Acarturk C, Anttila M, Au T, et al. Effectiveness of self-help plus in preventing mental disorders in refugees and asylum seekers in western Europe: a multinational randomized controlled trial. Psychother Psychosom. (2021) 90:403–14. doi: 10.1159/000517504
30. Acarturk C, Uygun E, Ilkkursun Z, Carswell K, Tedeschi F, Batu M, et al. Effectiveness of a WHO self-help psychological intervention for preventing mental disorders among Syrian refugees in Turkey: a randomized controlled trial. World Psychiatry. (2022) 21:88–95. doi: 10.1002/wps.20939
31. Acarturk C, Uygun E, Ilkkursun Z, Yurtbakan T, Kurt G, Adam-Troian J, et al. Group problem management plus (PM+) to decrease psychological distress among Syrian refugees in Turkey: a pilot randomised controlled trial. BMC Psychiatry. (2022) 22:8. doi: 10.1186/s12888-021-03645-w
32. Rahman A, Riaz N, Dawson KS, Usman Hamdani S, Chiumento A, Sijbrandij M, et al. Problem management plus (PM+): pilot trial of a WHO transdiagnostic psychological intervention in conflict-affected Pakistan. World Psychiatry. (2016) 15:182–3. doi: 10.1002/wps.20312
33. Spaaij J, Kiselev N, Berger C, Bryant RA, Cuijpers P, de Graaff AM, et al. Feasibility and acceptability of problem management plus (PM+) among Syrian refugees and asylum seekers in Switzerland: a mixed-method pilot randomized controlled trial. Eur J Psychotraumatol. (2022) 13:2002027. doi: 10.1080/20008198.2021.2002027
34. Bryant RA, Bawaneh A, Awwad M, Al-Hayek H, Giardinelli L, Whitney C, et al. Effectiveness of a brief group behavioral intervention for common mental disorders in Syrian refugees in Jordan: a randomized controlled trial. PLoS Med. (2022) 19:e1003949. doi: 10.1371/journal.pmed.1003949
35. de Graaff AM, Cuijpers P, Acarturk C, Bryant R, Burchert S, Fuhr DC, et al. Effectiveness of a peer-refugee delivered psychological intervention to reduce psychological distress among adult Syrian refugees in the Netherlands: study protocol. Eur J Psychotraumatol. (2020) 11:1694347. doi: 10.1080/20008198.2019.1694347
36. Moher D, Hopewell S, Schulz KF, Montori V, Gotzsche PC, Devereaux PJ, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. (2010) 340:c869. doi: 10.1136/bmj.c869
37. Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczek DK, Normand SL, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. (2002) 32:959–76. doi: 10.1017/S0033291702006074
38. Castor. Electronic Data Capture (EDC). Washington, DC: Castor (2017). Available online at: https://www.castoredc.com/electronic-data-capture-system/ (accessed December 15, 2022).
39. World Health Organization. Psychological First Aid: Facilitator's Manual for Orienting Field Workers. Geneva: World Health Organization (2013). Available online at: https://apps.who.int/iris/handle/10665/102380
40. Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary care evaluation of mental disorders Patient health questionnaire. JAMA. (1999) 282:1737–44. doi: 10.1001/jama.282.18.1737
41. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
42. Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
43. Kroenke K, Wu J, Yu Z, Bair MJ, Kean J, Stump T, et al. Patient health questionnaire anxiety and depression scale: initial validation in three clinical trials. Psychosom Med. (2016) 78:716–27. doi: 10.1097/PSY.0000000000000322
44. Weathers F, Litz B, Keane T, Palmieri P, Marx B, Schnurr P. The PTSD Checklist for DSM-5 (PCL-5). (2013). Available online at: https://www.ptsd.va.gov/professional/assessment/documents/PCL5_Standard_form.PDF (accessed December 15, 2022)
45. Ashworth M, Shepherd M, Christey J. A client-generated psychometric instrument: The development of ‘PSYCHLOPS. Counsel Psychother Res. (2004) 4:27–31. doi: 10.1080/14733140412331383913
46. Kalisch R, Muller MB, Tuscher O. A conceptual framework for the neurobiological study of resilience. Behav Brain Sci. (2015) 38:e92. doi: 10.1017/S0140525X1400082X
47. Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. (2011) 20:1727–36. doi: 10.1007/s11136-011-9903-x
48. Chisholm D, Knapp MR, Knudsen HC, Amaddeo F, Gaite L, Van WB. Client socio-demographic and service receipt inventory: European version—development of an instrument for international research. EPSILON study 5 European psychiatric services: inputs linked to outcome domains and needs. Br J Psychiatry Suppl. (2000) 39:s28–33. doi: 10.1192/bjp.177.39.s28
49. Schnurr PS, Vielhauer MJ, Findler MN, Hamblen JL. Trauma in the lives of older men: findings from the normative aging study. J Clin Geropsychol. (2002) 8:175–87. doi: 10.79-9362/02/0700-0175/0
50. Chmitorz A, Kurth K, Mey LK, Wenzel M, Lieb K, Tuscher O, et al. Assessment of microstressors in adults: questionnaire development and ecological validation of the mainz inventory of microstressors. JMIR Ment Health. (2020) 7:e14566. doi: 10.2196/14566
51. Veer IM, Riepenhausen A, Zerban M, Wackerhagen C, Puhlmann LMC, Engen H, et al. Psycho-social factors associated with mental resilience in the Corona lockdown. Transl Psychiatry. (2021) 11:67. doi: 10.1038/s41398-020-01150-4
52. Bryant RA, Schafer A, Dawson KS, Anjuri D, Mulili C, Ndogoni L, et al. Effectiveness of a brief behavioural intervention on psychological distress among women with a history of gender-based violence in urban Kenya: a randomised clinical trial. PLoS Med. (2017) 14:e1002371. doi: 10.1371/journal.pmed.1002371
53. Singer JDW, Willett JB. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence. Oxford: Oxford University Press (2003). doi: 10.1093/acprof:oso/9780195152968.001.0001
54. Huisman M. Item Nonresponse: Occurrence, Causes, and Imputation of Missing Answers to Test Item. London: Dswo Press (2020).
55. Kalisch R, Kober G, Binder H, Ahrens KF, Basten U, Chmitorz A, et al. The frequent stressor and mental health monitoring-paradigm: a proposal for the operationalization and measurement of resilience and the identification of resilience processes in longitudinal observational studies. Front Psychol. (2021) 12:710493. doi: 10.3389/fpsyg.2021.710493
56. Mediavilla R, McGreevy KR, Felez-Nobrega M, Monistrol-Mula A, Bravo-Ortiz MF, Bayon C, et al. Effectiveness of a stepped-care programme of internet-based psychological interventions for healthcare workers with psychological distress: study protocol for the RESPOND healthcare workers randomised controlled trial. Dig Health. (2022) 8:20552076221129084. doi: 10.1177/20552076221129084
Keywords: migrants, asylum seeker, refugee, psychological distress, COVID-19, resilience
Citation: Purgato M, Turrini G, Tedeschi F, Serra R, Tarsitani L, Compri B, Muriago G, Cadorin C, Ostuzzi G, Nicaise P, Lorant V, Sijbrandij M, Witteveen AB, Ayuso-Mateos JL, Mediavilla R, Haro JM, Felez-Nobrega M, Figueiredo N, Pollice G, McDaid D, Park AL, Kalisch R, Petri-Romão P, Underhill J, Bryant RA, Nosè M and Barbui C (2023) Effectiveness of a stepped-care programme of WHO psychological interventions in migrant populations resettled in Italy: Study protocol for the RESPOND randomized controlled trial. Front. Public Health 11:1100546. doi: 10.3389/fpubh.2023.1100546
Received: 16 November 2022; Accepted: 06 January 2023;
Published: 25 January 2023.
Edited by:
Wulf Rössler, Charité Universitätsmedizin Berlin, GermanyReviewed by:
Matthias Schützwohl, Technical University Dresden, GermanyCopyright © 2023 Purgato, Turrini, Tedeschi, Serra, Tarsitani, Compri, Muriago, Cadorin, Ostuzzi, Nicaise, Lorant, Sijbrandij, Witteveen, Ayuso-Mateos, Mediavilla, Haro, Felez-Nobrega, Figueiredo, Pollice, McDaid, Park, Kalisch, Petri-Romão, Underhill, Bryant, Nosè and Barbui. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Corrado Barbui,  Y29ycmFkby5iYXJidWlAdW5pdnIuaXQ=
Y29ycmFkby5iYXJidWlAdW5pdnIuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.