 Matías Henríquez1
Matías Henríquez1 Rodrigo Ramirez-Campillo2
Rodrigo Ramirez-Campillo2 Carlos Cristi-Montero3
Carlos Cristi-Montero3 Raul Reina4
Raul Reina4 Cristián Alvarez2
Cristián Alvarez2 Gerson Ferrari5
Gerson Ferrari5 Nicolas Aguilar-Farias6
Nicolas Aguilar-Farias6 Kabir P. Sadarangani7,8*
Kabir P. Sadarangani7,8*- 1Escuela de Kinesiología, Facultad de Odontología y Ciencias de la Rehabilitación, Universidad San Sebastián, Providencia, Chile
- 2Faculty of Rehabilitation Sciences, School of Physical Therapy, Exercise and Rehabilitation Sciences Institute, Universidad Andres Bello, Santiago, Chile
- 3IRyS Group, Physical Education School, Pontificia Universidad Católica de Valparaíso, Valparaíso, Chile
- 4Sports Research Centre, Miguel Hernández University, Elche, Spain
- 5Universidad de Santiago de Chile (USACH), Escuela de Ciencias de la Actividad Física, el Deporte y la Salud, Santiago, Chile
- 6Department of Physical Education, Sports and Recreation, Universidad de La Frontera, Temuco, Chile
- 7Escuela de Kinesiología, Universidad Autónoma de Chile, Santiago, Chile
- 8Faculty of Health and Dentistry, School of Kinesiology, Universidad Diego Portales, Santiago, Chile
Background: People with disabilities usually face barriers to regularly engaging in physical activities. Estimating physical activity patterns are necessary to elaborate policies and strategies to facilitate active lifestyles, considering the particular access difficulties experienced by this population.
Purpose: This study aimed (i) to describe the prevalence of physical activity levels and (ii) to examine the associations of physical activity levels with socio-demographic variables and type of disability in the 2020 Chilean National Physical Activity and Sports Habits in Populations with Disabilities (CNPASHPwD) survey during the coronavirus disease 19 (COVID-19) pandemic.
Methods: Cross-sectional data from 3,150 adults (18–99 years old), 59.8% female, were analyzed from November to December 2020. Self-reported age, gender, type of disability (i.e., physical, visual, hearing, intellectual, or mixed), socio-economic status, area and zone of residence, and physical activity levels (0 min/week, < 150 min/week, ≥ 150 min/week) were obtained.
Results: 11.9% of the participants were classified as active (≥ 150 min/week), and 62.6% declared no involvement in physical activity. A larger proportion of females (61.7%) did not meet the current guidelines (≥ 150 min/week of physical activity) in comparison with males (p < 0.001). Participants with visual and hearing disabilities were more likely to be active than those with other types of disabilities. Those living in the central and southern regions of Chile were more likely to be physically active than those from the northern region. Also, older participants, women, and those from lower socio-economic statuses were less likely to meet the physical activity guidelines.
Conclusion: Alarmingly, nine out of ten participants were categorized as physically inactive, particularly women, older adults, and those with a low socioeconomic status. If the pandemic context moderated, the considerable prevalence of reduced physical activity levels deserves future exploration. Health promotion initiatives should consider these aspects, emphasizing inclusive environments and increasing opportunities to favor healthy behaviors, countering the COVID-19 effects.
1. Introduction
Inadequate physical activity (PA) levels and sedentary behaviors are linked to non-communicable diseases and all-cause mortality in the global population (1–4). Compared to the average population, people with different disabilities show even lower PA levels and increased risk of comorbidities (5). The benefits of being physically active reinforce the need for providing opportunity access to perform PA to everyone of all ages (6–8). Although people with disabilities face several barriers that limit their participation in PA and which differ from those without disabilities, challenging the possibilities to ensure participation and the benefits of regular practice in this group is imperative (9–11). Global efforts to promote PA in people living with disabilities resulted in the first World Health Organization (WHO) guidelines based on wide-ranging evidence and describing recommendations that could facilitate the practice and participation of overall society activities in this specific population (12).
Most population data to estimate or monitor PA patterns are conducted through national surveys, where the available data are mainly focused on high-income countries or northern regions (North America and Europe) (13). Thereby, a lack of evidence is appreciable in low-to-middle-income countries or Latin-American and African regions. For example, in Netherlands and Australia, adults living with disabilities had lower PA levels and were less likely to meet PA guidelines than those without disabilities (13, 14). These findings align with another study conducted in the United States, where half of the adults were physically inactive and more likely to have a chronic disease (15–17). According to Martin Ginis et al. (5), the significant disparities in participation rates and the near-absence of population-level data on PA in people with disabilities from low-income and middle-income countries represent a problem for healthcare systems and population quality of life. In this regard, more extraordinary global efforts towards international goals such as the United Nations (UN) Sustainable Development Goals (SDG) of healthy lives and well-being for all have been directed to face these challenges. In this sense, the Latin American region is an active member state responsible for covering and accomplishing the SDG (18). One study analyzed the participation in PA of people with chronic health physical conditions (e.g., chronic back pain, angina, arthritis, asthma, diabetes, hearing problems, tuberculosis, visual impairment, and edentulism) in a few South American countries (i.e., Brazil, Ecuador, Paraguay, and Uruguay) (19). Even though this study provides novel information about a multi-national scope, people with disabilities and different impairments (i.e., hearing, intellectual, or mixed-related disabilities) were not incorporated into the analysis.
The 2020 Chilean National Physical Activity and Sports Habits in Populations with Disabilities study (CNPASHPwD; Estudio Nacional de Hábitos de Actividad Física y Deporte en Población con Discapacidad in Spanish) (20), aims to collect information and epidemiological evidence through the application of a national survey about patterns of practice during coronavirus disease 19 (COVID-19) pandemic. However, to favor fewer infection rates during the pandemic, international organizations and governments imposed various preventive measures, such as restricted movement of the citizens, social/physical distancing, and banning social gatherings (21). It is essential to highlight that people with disabilities are especially exposed to the effects of the pandemic, where confinement strategies drastically decreased PA levels and increased sedentary lifestyles even more, which directly affected their health parameters (22, 23). Exploring the prevalence of PA levels considering participants with the mentioned health conditions and socio-demographic data from a country in the South American region may provide novel knowledge and bridge gaps in local factors that could facilitate intervention strategies targeting the population with a disability.
Therefore, this study aimed (i) to describe the prevalence of reported PA levels of Chilean adults with disabilities and (ii) to examine the associations of their PA levels with socio-demographic factors and type of disability participating in the 2020 CNPASHPwD during the COVID-19 pandemic.
2. Materials and methods
2.1. Study design and participants
The 2020 CNPASHPwD study used a cross-sectional design to identify PA levels and competitive sports practices in the national population with disabilities completed during the COVID-19 pandemic (20). A stratified cluster and multistage random sample from the Population and Housing Census of 2017 was selected, considering individuals aged ≥13 years with a disability, a valid home address from all socio-economic sectors, and geographical units in urban and rural sectors. Sample size was calculated for each region, according to estimating proportions formulae assuming p = 0.5, setting the statistical power at a 95% confidence interval and a sampling error of 5.9%. With this calculation, the sample size required in each region ranged between 269 and 276 participants (24). Data were collected by census track covering households using face-to-face questionnaires. The planned sample size was 4,393 surveys, but only a response rate of 87% was achieved, corresponding to 3,833 surveys (20). The surveys were completed in all the regions from November 21 to December 23, 2020. However, two southern regions were in partial restrictions, limiting the possibility of reaching the planned sample size. For participants whose disability prevented them from answering the surveys independently (e.g., intellectual disabilities), their parents/guardians were instructed to support their responses. For this study, only adult participants aged ≥18 were considered for the analysis (25), with a final sample of 3,150 participants. The study protocol was reviewed and approved by the ethics research committee of the Ministry of Sports and carried out following the guidelines of the World Medical Association’s Declaration of Helsinki. All participants gave consent to participate.
2.2. Variables
2.2.1. Socio-demographic
The survey includes questions to collect information about age, gender (male, female, or no answer), socio-economic status (i.e., five levels according to income per capita in quintiles), area of residence (urban or rural), and region of residence denominated according to the number of the administrative divisions (north: XV, I, II, III and IV; central: XIII, V, VI, VII, VIII; and south: XVI, IX, X, XI, XII, XIV).
2.2.2. Disability types
Respondents were categorized into five disability types according to their impairments, including physical, visual, hearing, intellectual, and mixed which generate activity limitations and restrict their daily participation according to the International Classification of Functioning, Disability, and Health framework, which is in line with the UN definition of disability (18, 26).
2.2.3. Physical activity
Physical activity was measured with the categorical option from the validated Swedish National Board of Health and Welfare, which has an acceptable correlation with objective devices among adult the population (27, 28). Duration of moderate or vigorous-intensity leisure-time PA was reported according to time intervals for all seven days of the week. Intervals included 0 min/day, < 15 min/day, 15–30 min/day, 31–45 min/day, 46–60 min/day and > 60 min/day. The average minutes of each interval were truncated to create categories of recommendations according to the WHO (29), into 0 min/week (nonphysical activity), 1–149 min/week (some but less than recommended), and ≥ 150 min/week (active).
2.3. Statistical analysis
Descriptive characteristics variables are presented with mean and standard deviation for continuous variables, while frequency and percentages for categorical variables. Bivariate associations using t-test, Chi-squared, or Fisher exact test assessed for differences among PA levels. Multivariable logistic regression was performed to analyze the association between PA recommendations (active ≥150 min/week or inactive <150 min/week) and disability type, gender, age, socio-economic status, area, and region of residence. The results from the logistic regression were expressed in odds ratios (ORs) and their 95% confidence intervals (95% CIs) for crude (disability type) and adjusted models (all covariates). All analyses were undertaken using Stata Version 15.1 (Stata Corp, College Station, Texas, United States), and a complex sample design was used. A p-value of <0.05 was considered statistically significant.
3. Results
In total, 3,150 participants were considered for this analysis. The participants’ socio-demographic characteristics and PA levels are described in Table 1. Of the participants, 59.8% were female, 52.9% reported visual impairments or disability, 50.8% belonged to the two lowest socio-economic quintiles, 44.3% resided in the central region, and 82.9% lived in urban settings. Regarding PA levels, only 11.9% of the participants were physically active.

Table 1. Socio-demographic characteristics of participants.
Table 2 illustrates the prevalence of PA according to the socio-demographic characteristics of the participants with disabilities. Those who reported meeting PA recommendations were younger than their counterparts (p < 0.001). According to gender, larger proportions of males were classified as active compared to female participants (p < 0.001). There was a particular higher prevalence of non-practice of PA among those participants with physical (23.6%), intellectual (4.1%), and mixed (16.2%) disabilities (p < 0.001). Physical inactivity prevalence increased in participants from the poorest quintiles (i.e., E: 20.8%), while most active participants were categorized in the wealthiest group (i.e., A: 12.5%). A lower prevalence of participants from the northern region achieved ≥150 min/week (27.1%) in comparison to participants from the central area (47.3%). Nearly 80% of participants from urban areas fulfilled the PA recommendations.
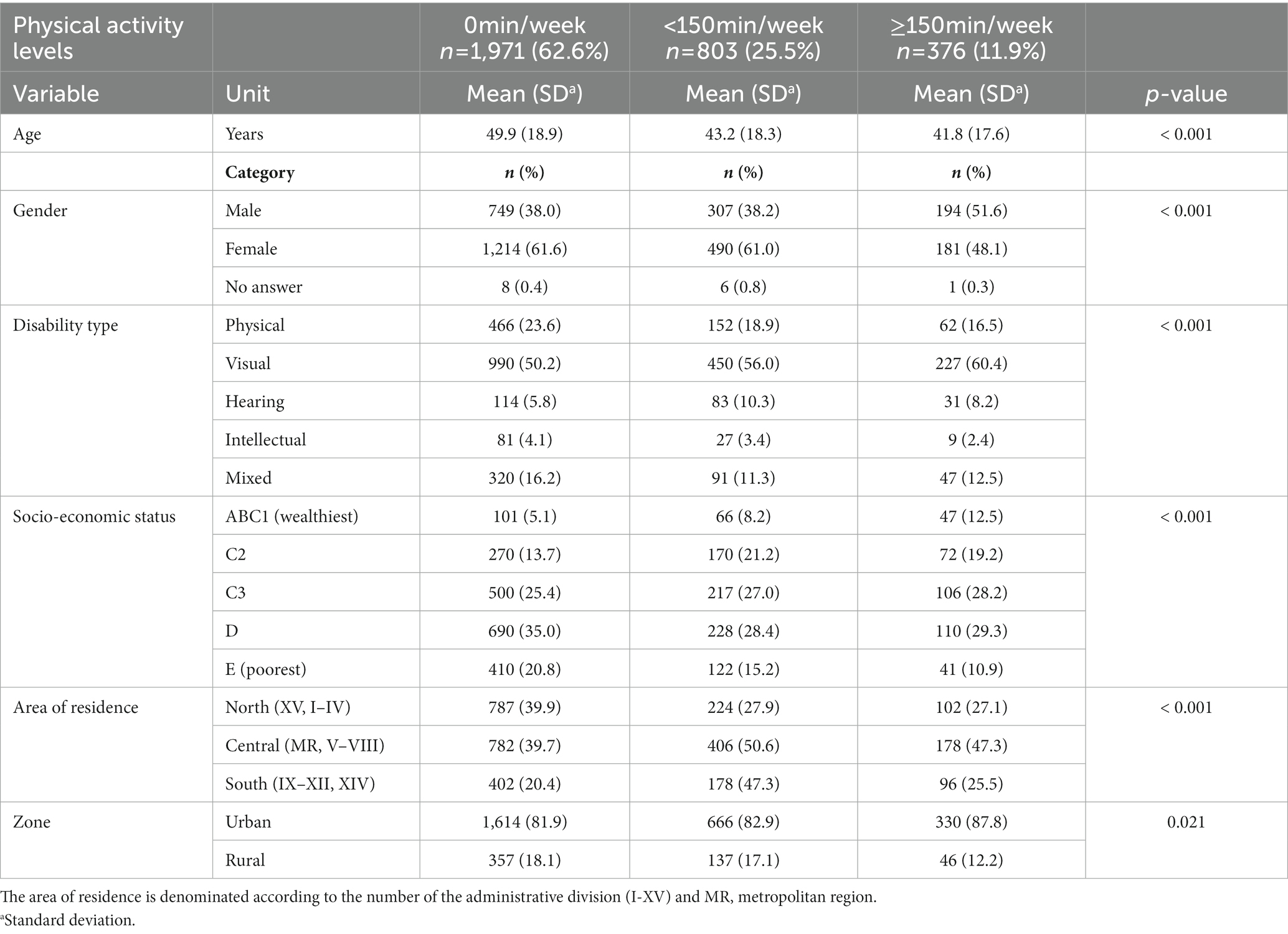
Table 2. Prevalence of physical activity levels in participants according to their socio-demographic characteristics.
The ORs and the 95% CI reported PA levels according to the socio-demographic characteristics of the participants can be found in Figure 1. Participants with visual and hearing impairment (OR = 1.30–2.16; 95% CI: 1.233; 2.957) were associated with higher odds of achieving international recommendations of PA than those with physical impairment. Also, older participants had fewer odds of being categorized as physically active (i.e., ≥ 150 min/week) compared to younger participants (OR = 0.98; 95% CI: 0.978; 0.987). In addition, female participants were less likely to be physically active than male participants (OR = 0.83; 95% CI: 0.709; 0.965). Moreover, participants who belong to the lowest quintiles were less likely to meet current PA recommendations (OR = 0.53–0.66; 95% CI: 0.371;0.901). Finally, participants living in the central or southern regions of the country were more likely to participate in adequate levels of PA than those living in the northern area (OR = 1.68–2.17; 95% CI: 1.355; 2.598).
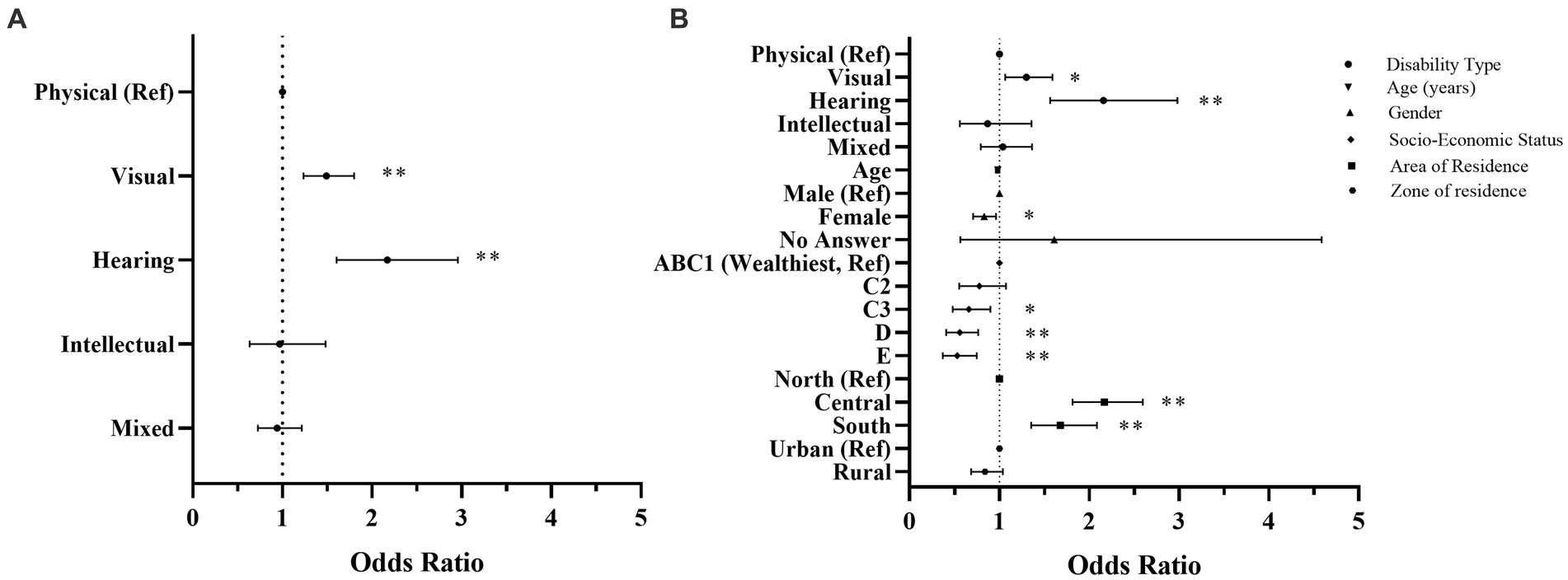
Figure 1. Forest plot of odds ratios and 95% confidence intervals. The plot represents the association between physical activity levels and the type of disability of the participants. (A) is adjusted for disability types and (B) is additionally adjusted for age, gender, socio-economic status, area of residence, and zone of residence. Results are interpreted as higher or lower odds of being physically active. Ref, reference; *p < 0.05; **p < 0.01.
4. Discussion
To the best of our knowledge, this is the first study to describe the prevalence of PA patterns and socio-demographic characteristics in a sample of Latin American adults with disabilities during the COVID-19 pandemic. The current study showed that 11.9% met the PA guidelines, and 62.6% declared non-physical activity. Moreover, males, younger, with visual or hearing disabilities from the wealthiest economic status and with residency in the central and southern zones of the country, were more likely to meet adequate levels of PA recommendations.
According to PA levels, these results align with previous studies, showing that people with disabilities reported lower levels than those without disabilities (14, 30). Furthermore, this can be seen in a recent work performed on South American adults during the COVID-19 pandemic lockdown showed that 56.9% of the participants were categorized as physically active, a higher prevalence compared to the reported in the present study (31). In addition, McGuire et al. (32) described that adults with disabilities were less likely to engage with recommended levels of PA in comparison to their counterparts, showing the health disparities which could be involved in this population and higher odds of developing chronic diseases (17, 33). Furthermore, previous reports showed that people with disabilities could also achieve health benefits by performing PA at levels even below international recommendations (5, 34), considering the particularities of the specific disability (35, 36). In this line, PA has been demonstrated as a feasible tool for improving and maintaining health in these groups, wherein every minute counts (29); however, compliance with PA recommendations is still low, corresponding to the reported by the participants. The update of the WHO guidelines on PA and sedentary behavior includes recommendations for adults living with a disability, facilitating the development and implementation of policies for participation in this population. However, considering the extensive range of health and functional profiles, a broader level of PA recommendation is needed according to each group’s characteristics as the evidence available increases (12). Additional challenges could be faced by people with disabilities during measures of social isolation, whereas previous studies reported that the use of assistive devices and environmental barriers limit PA participation (9, 11, 37), and the impact of the housing-built environment on the quality of life (38).
Some authors suggested that along with the natural aging process, adults with a disability could experience more difficulties associated with an accelerated musculoskeletal impairment-specific process, secondary health conditions, and lower levels of PA that affect overall health and quality of life (39–42). In this context, PA is critical to maintaining or improving physical functioning in people with chronic health conditions (43). According to age, the results indicated that lower PA levels were presented in major proportions among older adults. Previous studies have shown that older adults without disabilities are more likely to be inactive and present an increased cardiovascular risk than younger adults (44, 45). Moreover, higher amounts of sedentary behavior time could negatively impact the increased risk of premature mortality, especially in physically inactive individuals, reinforcing the importance of maintaining higher levels of total PA at any intensity (46, 47). The public health crisis increased the risk of death and severe outcomes due to COVID-19 in older people living with disabilities more than in people without disabilities, significantly impacting the disability community and probably affecting their levels of PA (48).
In terms of gender, female participants presented a higher prevalence of physical inactivity, in line with previous studies among women with disabilities (49–52). Women with disabilities are at higher risk of inactivity-related health consequences due to facing significant barriers in different spheres and difficulting participating in PA (5, 53). Especially in Latin America, data from people without disabilities described that women’s participation in PA had been identified as insufficient and lower than in other regions of the world. This concern reinforces the need to develop specific strategies for this population (53, 54).
Previous reports informed that people with multiple disabilities present the lowest PA levels probably due to the number of barriers at different levels (i.e., psychological, environmental factors, activity costs, and lack of support) and difficulties that are determinants of participation (49, 55). In addition, Lobenius-Palmér et al. (50) assessed the prevalence of PA in youths with multiple disabilities and reported that participants with hearing impairments were the most physically active. This finding is consistent with the results found in this study, where participants with hearing and visual impairments present higher levels of PA than those from the physical disability group. Probably, these results could be influenced due to the specific-local barriers that face people with physical and intellectual disabilities, limiting their possibilities to engage in different types of PA and achieve optimal health (15, 39, 40). Additionally, the disability itself, the requirement of support personnel, and the use of assistive-specific devices to facilitate the practice of PA could limit the chances of opportunities for participation (9). People with disabilities face complex challenges where government responses do not fully address the population’s basic needs in a health emergency scenario such as the COVID-19 pandemic, hindering even more, the possibility of being concerned about the practice of PA (23). The pandemic measures drastically impact the PA levels and the increment of sedentary behaviors in people living with disabilities (56) and able-bodied populations (57), a cautionary aspect that should be considered when interpreting the results.
People with disabilities experience higher living costs due to difficulties with functional autonomy, support requirements, and access to specific equipment, facing more significant inequalities than people without disabilities, summating in a considerable socio-economic disadvantage (58–60). It is remarkable to describe that the disability prevalence, on average, is higher in low-and lower-middle-income countries than in upper-middle-and high-income countries (59). Particularly, socio-economic status was identified as a relevant factor that influences the time engaging in PA and impacts the prevalence of sitting time, showing inequality patterns between the poorest and wealthy segments of the Chilean population (61). This study showed a higher prevalence of physical inactivity in the lowest quintiles. Similarly, previous research highlighted that the principal determinants in low socio-economic status communities to engage in PA participation involve the urban environment, financial constraints, work-life integration, community engagement, social support, and individual psychological factors (62). People living with disabilities are constantly constrained by barriers that difficult their involvement in PA and sports, where the economic factor could be relevant for accessing to sport, requiring specific equipment, or higher transport costs, among others (10, 11, 37, 63–65). Werneck et al. (65) described that socio-economic inequalities in South American populations without disabilities increased for total and leisure-time physical activity over the years. According to the author’s knowledge, there are no reports considering PA disparities according to the socio-economic characteristics of people living with disabilities in the Latin American region prior or during the COVID-19 pandemic.
The COVID-19 pandemic disproportionately affected the socio-economic lives, particularly the poorest and most vulnerable segments of society, such as women, the older adults, and people living with disabilities (48). The lack of adequate socio-economic support for the population with disabilities during the pandemic could have significant repercussions on daily life, considering the low levels of participation in the labor market and high levels of involvement in the informal economic employment in the region, constrained by health measures limiting all type of activities (66, 67). Our results demonstrated greater physical activity levels in people living in the central and southern regions of the country when compared to those from the northern regions. These results are probably conditioned by the country’s geographical diversity, where the Chilean population is exposed to high levels of urbanization, principally in the central zone (68). In particular, Sadarangani et al. (69) showed that in the Chilean non-impaired population, the same differences in PA level were presented according to the region of residence, reinforcing the particularities of each environment and the possible impact on health parameters. Moreover, local disability-specific policies and consistent actions promoting physical activity in people with disabilities are important to address greater participation levels advocating this aspect as a basic human right. Although Chile is a member of the UN, and there are some policies and actions oriented specifically to this population segment, the results of this study suggest relevant disparities due to the high prevalence of physical inactivity, remarking that these strategies are not enough (70). Furthermore, people with disabilities could experience more barriers and fewer opportunities to access services or infrastructure. Consequently, they participate less in PA in rural contexts, facing more challenges than their counterparts in urban residency zones (71). Lastly, cultural-specific characteristics could also constraint the participation of people with disabilities, considering that some local barriers may be relevant only in the study country and not in other regions, impacting in a unique form the complex relationship between barriers and facilitators for engagement in physical activity (72, 73).
4.1. Strengths and limitations
According to Martin Ginis (5), there is a need to develop research on PA in people with disabilities, focusing on data collection in middle and low-income countries where monitoring is required to measure the accomplishment of the UNs´2030 Agenda and SDGs. The novelty of this research relies on the analysis of a large random sample of participants living with disabilities, providing data on a population from the Latin American region, which could help to have a more profound understanding of the magnitude of the prevalence of PA levels in people with disabilities. Facilitating their participation in PA could be a challenge that requires multi-sectorial efforts considering the particularities of this population and investing in inclusive environments that benefit all the society (12). A more holistic approach is necessary for further studies addressing other aspects that could impact PA participation and patterns, such as sitting time, screen time exposure, active transport, gender differences, or nutritional behaviors.
This study is not free of limitations that should be addressed. First, the PA levels reported in this study are based on self-reported methods, which could include estimation problems due to potential self-reporting bias. Second, CNPASHPwD employed a cross-sectional design, precluding inferences about causality. Third, the number of participants in each disability group is limited (i.e., intellectual and hearing impairments), and the degree of disability is unavailable; thus, residual confounding remains as a possibility. Also, the health measures to contain the COVID-19 pandemic could influence the responses of the level of participation in PA; however, this novel information is of interest considering the absence of previous reports. Further studies should consider these limitations and explore possible barriers and facilitators impacting PA patterns. In addition, future studies could incorporate longitudinal analysis, neighborhood countries, transport modes or distance to sports facilities, considering the multiple barriers faced by people with disabilities.
In conclusion, 11.9% of the people living with disabilities in Chile during the COVID-19 pandemic were classified as physically active, in which especially males and those from the highest socio-economic segments, and those living in the central and southern regions of Chile were more likely to be active. These data could be helpful to potential strategies or local policies to promote PA in certain specific disability groups in collaboration with different sectors of Chilean society and in concordance with the SDGs.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Transparency law. Requests to access these datasets should be directed to https://www.portaltransparencia.cl/PortalPdT/.
Ethics statement
The studies involving human participants were reviewed and approved by Sports Ministry. The patients/participants provided their written informed consent to participate in this study.
Author contributions
KS and MH involved in conceptualization and roles or writing—original draft. KS involved in data curation, performed the formal analysis and has full access to all the data in the study and is responsible for the decision to submit for publication. KS, MH, RR-C, CC-M, RR, CA, GF, and NA-F were involved in writing—review and editing. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lee, IM, Shiroma, EJ, Lobelo, F, Puska, P, Blair, SN, Katzmarzyk, PT, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. (2012) 380:219–29. doi: 10.1016/S0140-6736(12)61031-9
2. Rezende, LFM, Sá, TH, Mielke, GI, Viscondi, JYK, Rey-López, JP, and Garcia, LMT. All-cause mortality attributable to sitting time: analysis of 54 countries worldwide. Am J Prev Med. (2016) 51:253–63. doi: 10.1016/j.amepre.2016.01.022
3. Lavie, CJ, Ozemek, C, Carbone, S, Katzmarzyk, PT, and Blair, SN. Sedentary behavior, exercise, and cardiovascular health. Circ Res. (2019) 124:799–815. doi: 10.1161/CIRCRESAHA.118.312669
4. Rezende, LFM, Ferrari, G, Lee, DH, Aune, D, Liao, B, Huang, W, et al. Lifestyle risk factors and all-cause and cause-specific mortality: assessing the influence of reverse causation in a prospective cohort of 457, 021 US adults. Eur J Epidemiol. (2022) 37:11–23. doi: 10.1007/s10654-021-00829-2
5. Martin Ginis, KA, van der Ploeg, HP, Foster, C, Lai, B, McBride, CB, Ng, K, et al. Participation of people living with disabilities in physical activity: a global perspective. Lancet. (2021) 398:443–55. doi: 10.1016/S0140-6736(21)01164-8
6. Lear, SA, Hu, W, Rangarajan, S, Gasevic, D, Leong, D, Iqbal, R, et al. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: the PURE study. Lancet. (2017) 390:2643–54. doi: 10.1016/S0140-6736(17)31634-3
7. Ekelund, U, Steene-Johannessen, J, Brown, WJ, Fagerland, MW, Owen, N, Powell, KE, et al. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet. (2016) 388:1302–10. doi: 10.1016/S0140-6736(16)30370-1
8. Reiner, M, Niermann, C, Jekauc, D, and Woll, A. Long-term health benefits of physical activity – a systematic review of longitudinal studies. BMC Public Health. (2013) 13:1–9. doi: 10.1186/1471-2458-13-813
9. Jaarsma, EA, Dijkstra, PU, Geertzen, JHB, and Dekker, R. Barriers to and facilitators of sports participation for people with physical disabilities: a systematic review. Scand J Med Sci Sports. (2014) 24:871–81. doi: 10.1111/sms.12218
10. Bossink, LWM, van der Putten, AA, and Vlaskamp, C. Understanding low levels of physical activity in people with intellectual disabilities: a systematic review to identify barriers and facilitators. Res Dev Disabil. (2017) 68:95–110. doi: 10.1016/j.ridd.2017.06.008
11. Jaarsma, EA, Dekker, R, Koopmans, SA, Dijkstra, PU, and Geertzen, JHB. Barriers and facilitators of sports participation in people with visual impairments. Adapt Phys Act Q. (2014) 31:240–64. doi: 10.1123/2013-0119
12. Carty, C, van der Ploeg, HP, Biddle, SJH, Bull, F, Willumsen, J, Lee, L, et al. The first global physical activity and sedentary behavior guidelines for people living with disability. J Phys Act Health. (2021) 18:86–93. doi: 10.1123/jpah.2020-0629
13. Hassett, L, Shields, N, Cole, J, Owen, K, and Sherrington, C. Comparisons of leisure-time physical activity participation by adults with and without a disability: results of an Australian cross-sectional national survey. BMJ Open Sport Exerc Med. (2021) 7:e000991. doi: 10.1136/bmjsem-2020-000991
14. de Hollander, EL, and Proper, KI. Physical activity levels of adults with various physical disabilities. Prev Med Rep. (2018) 10:370–6. doi: 10.1016/j.pmedr.2018.04.017
15. Hollis, ND, Zhang, QC, Cyrus, AC, Courtney-Long, E, Watson, K, and Carroll, DD. Physical activity types among US adults with mobility disability, behavioral risk factor surveillance system, 2017. Disabil Health J. (2020) 13:100888. doi: 10.1016/j.dhjo.2020.100888
16. Brown, DR, Carroll, DD, Workman, LM, Carlson, SA, and Brown, DW. Physical activity and health-related quality of life: US adults with and without limitations. Qual Life Res. (2014) 23:2673–80. doi: 10.1007/s11136-014-0739-z
17. Carroll, DD, Courtney-Long, EA, Stevens, AC, Sloan, ML, Lullo, C, Visser, SN, et al. Vital signs: disability and physical activity--United States, 2009-2012. MMWR Morb Mortal Wkly Rep. (2014) 63:407–13.
18. United Nations. (2006). Convention on the rights of persons with disabilities. Treaty Series (2006) 2515:3. doi: UN Doc. A/61/611.
19. Vancampfort, D, Koyanagi, A, Ward, PB, Rosenbaum, S, Schuch, FB, Mugisha, J, et al. Chronic physical conditions, multimorbidity and physical activity across 46 low and middle income countries. Int J Behav Nutr Phys Act. (2017) 14:1–13. doi: 10.1186/s12966-017-0463-5
20. Ministerio del Deporte. (2020). Estudio nacional de hábitos de actividad física y deporte en población con discapacidad.
21. Hossain, MM, Sultana, A, and Purohit, N. Mental health outcomes of quarantine and isolation for infection prevention: a systematic umbrella review of the global evidence. SSRN Electron J. (2020) 42:1–27. doi: 10.2139/ssrn.3561265
22. Narici, M, de Vito, G, Franchi, M, Paoli, A, Moro, T, Marcolin, G, et al. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur J Sport Sci. (2020) 21:614–35. doi: 10.1080/17461391.2020.1761076
23. Sakellariou, D, Malfitano, APS, and Rotarou, ES. Disability inclusiveness of government responses to COVID-19 in South America: a framework analysis study. Int J Equity Health. (2020) 19:1–11. doi: 10.1186/s12939-020-01244-x
24. Universidad de Concepción. (2020). Segundo estudio nacional de hábitos de actividad física y deportes en población con discapacidad, primer informe. Concepción. 4–78 pp.
25. World Health Organization. (2020). WHO guidelines on physical activity and sedentary behaviour. Available at: https://www.who.int/publications/i/item/9789240015128.
26. Kostanjsek, N. Use of the international classification of functioning, disability and health (ICF) as a conceptual framework and common language for disability statistics and health information systems. BMC Public Health. (2011) 11:S3. doi: 10.1186/1471-2458-11-S4-S3
27. Olsson, SJG, Ekblom, Ö, Andersson, E, Börjesson, M, and Kallings, LV. Categorical answer modes provide superior validity to open answers when asking for level of physical activity: a cross-sectional study. Scand J Public Health. (2016) 44:70–6. doi: 10.1177/1403494815602830
28. The Swedish National Board of Health and Welfare. (2011). Nationella riktlinjer för sjukdomsförebyggande metoder 2011 Tobaksbruk, riskbruk av alkohol, otillräcklig fysisk aktivitet och ohälsosamma matvanor Stöd för styrning och ledning. Västerås, Sweden.
29. Bull, FC, Al-Ansari, SS, Biddle, S, Borodulin, K, Buman, MP, Cardon, G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
30. Fernández-Verdejo, R, and Suárez-Reyes, M. Inactividad física versus sedentarismo: análisis de la Encuesta Nacional de Salud de Chile 2016-2017. Rev Med Chil. (2021) 149:103–9. doi: 10.4067/S0034-98872021000100103
31. Sadarangani, KP, de Roia, GF, Lobo, P, Chavez, R, Meyer, J, Cristi-Montero, C, et al. Changes in sitting time, screen exposure and physical activity during covid-19 lockdown in south American adults: a cross-sectional study. Int J Environ Res Public Health. (2021) 18:5239. doi: 10.3390/ijerph18105239
32. McGuire, LC, Strine, TW, Okoro, CA, Ahluwalia, IB, and Ford, ES. Healthy lifestyle behaviors among older U.S. adults with and without disabilities, behavioral risk factor surveillance system, 2003. Prev Chronic Dis. (2007) 4:A09.
33. Rimmer, JH, Rowland, JL, and Yamaki, K. Obesity and secondary conditions in adolescents with disabilities: addressing the needs of an underserved population. J Adolesc Health. (2007) 41:224–9. doi: 10.1016/j.jadohealth.2007.05.005
34. Martin Ginis, KA, Van Der Scheer, JW, Latimer-Cheung, AE, Barrow, A, Bourne, C, Carruthers, P, et al. Evidence-based scientific exercise guidelines for adults with spinal cord injury: an update and a new guideline. Spinal Cord. (2018) 56:308–21. doi: 10.1038/s41393-017-0017-3
35. Verschuren, O, Peterson, MD, Balemans, ACJ, and Hurvitz, EA. Exercise and physical activity recommendations for people with cerebral palsy. Dev Med Child Neurol. (2016) 58:798–808. doi: 10.1111/dmcn.13053
36. Bernhardt, J, Roth, EJ, Shaughnessy, M, Mac Kay-Lyons, M, Tang, A, Eng, JJ, et al. Physical activity and exercise recommendations for stroke survivors. Stroke. (2014) 45:2532–53. doi: 10.1161/str.0000000000000022
37. Jaarsma, EA, Dekker, R, Geertzen, JHB, and Dijkstra, PU. Sports participation after rehabilitation: barriers and facilitators. J Rehabil Med. (2016) 48:72–9. doi: 10.2340/16501977-2017
38. Amerio, A, Brambilla, A, Morganti, A, Aguglia, A, Bianchi, D, Santi, F, et al. COVID-19 lockdown: housing built environment’s effects on mental health. Int J Environ Res Public Health. (2020) 17:5973. doi: 10.3390/ijerph17165973
39. Sweeting, J, Merom, D, Astuti, PAS, Antoun, M, Edwards, K, and Ding, D. Physical activity interventions for adults who are visually impaired: a systematic review and meta-analysis. BMJ Open. (2020) 10:e034036. doi: 10.1136/bmjopen-2019-034036
40. Starkoff, BE, Lenz, EK, Lieberman, L, and Foley, J. Sedentary behavior in adults with visual impairments. Disabil Health J. (2016) 9:609–15. doi: 10.1016/j.dhjo.2016.05.005
41. Verschuren, O, Smorenburg, ARP, Luiking, Y, Bell, K, Barber, L, and Peterson, MD. Determinants of muscle preservation in individuals with cerebral palsy across the lifespan: a narrative review of the literature. J Cachexia Sarcopenia Muscle. (2018) 9:453–64. doi: 10.1002/jcsm.12287
42. Johansson, M, Björne, P, Runesson, I, and Ahlström, G. Healthy ageing in people with intellectual disabilities from managers’ perspective: a qualitative study. Healthcare (Switzerland). (2017) 5:45. doi: 10.3390/healthcare5030045
43. Rimmer, JH. Exercise and physical activity in persons aging with a physical disability. Phys Med Rehabil Clin N Am. (2005) 16:41–56. doi: 10.1016/j.pmr.2004.06.013
44. Hallal, PC, Andersen, LB, Bull, FC, Guthold, R, Haskell, W, Ekelund, U, et al. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. (2012) 380:247–57. doi: 10.1016/S0140-6736(12)60646-1
45. Wilby, ML. Physical mobility impairment and risk for cardiovascular disease. Health Equity. (2019) 3:527–31. doi: 10.1089/heq.2019.0065
46. Ekelund, U, Tarp, J, Steene-Johannessen, J, Hansen, BH, Jefferis, B, Fagerland, MW, et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: systematic review and harmonised meta-analysis. BMJ. (2019) 366:l4570. doi: 10.1136/bmj.l4570
47. Dunstan, DW, Dogra, S, Carter, SE, and Owen, N. Sit less and move more for cardiovascular health: emerging insights and opportunities. Nat Rev Cardiol. (2021) 18:637–48. doi: 10.1038/s41569-021-00547-y
48. Shakespeare, T, Ndagire, F, and Seketi, QE. Triple jeopardy: disabled people and the COVID-19 pandemic. Lancet. (2021) 397:1331–3. doi: 10.1016/S0140-6736(21)00625-5
49. Úbeda-Colomer, J, Monforte, J, and Devís-Devís, J. Physical activity of university students with disabilities: accomplishment of recommendations and differences by age, sex, disability and weight status. Public Health. (2019) 166:69–78. doi: 10.1016/j.puhe.2018.10.006
50. Lobenius-Palmér, K, Sjöqvist, B, Hurtig-Wennlöf, A, and Lundqvist, LO. Accelerometer-assessed physical activity and sedentary time in youth with disabilities. Adapt Phys Act Q. (2018) 35:1–19. doi: 10.1123/apaq.2015-0065
51. Phillips, AC, and Holland, AJ. Assessment of objectively measured physical activity levels in individuals with intellectual disabilities with and without down’s syndrome. PLoS One. (2011) 6:6–12. doi: 10.1371/journal.pone.0028618
52. Mitchell, LE, Ziviani, J, and Boyd, RN. Habitual physical activity of independently ambulant children and adolescents with cerebral palsy: are they doing enough? Phys Ther. (2015) 95:202–11. doi: 10.2522/ptj.20140031
53. Úbeda-Colomer, J, Devís-Devís, J, and Martin Ginis, KA. Gender differences in theory-based predictors of physical activity in university students with disabilities. Rev Latinoam Psicol. (2020) 52:141–8. doi: 10.14349/rlp.2020.v52.14
54. Guthold, R, Stevens, GAA, Riley, LMM, and Bull, FCC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. (2018) 6:e1077–86. doi: 10.1016/S2214-109X(18)30357-7
55. Simeonsson, RJ, Carlson, D, Huntington, GS, McMillen, JS, and Brent, JL. Students with disabilities: a national survey of participation in school activities. Disabil Rehabil. (2001) 23:49–63. doi: 10.1080/096382801750058134
56. de Boer, DR, Hoekstra, F, Huetink, KIM, Hoekstra, T, Krops, LA, and Hettinga, FJ. Physical activity, sedentary behavior and well-being of adults with physical disabilities and/or chronic diseases during the first wave of the COVID-19 pandemic: a rapid review. Int J Environ Res Public Health. (2021) 18:6342. doi: 10.3390/ijerph18126342
57. Stockwell, S, Trott, M, Tully, M, Shin, J, Barnett, Y, Butler, L, et al. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: a systematic review. BMJ Open Sport Exerc Med. (2021) 7:e000960–8. doi: 10.1136/bmjsem-2020-000960
58. Braithwaite, J, and Mont, D. Disability and poverty: a survey of World Bank poverty assessments and implications. Alternatives. (2009) 3:219–32. doi: 10.1016/j.alter.2008.10.002
59. Hosseinpoor, AR, Williams, JAS, Gautam, J, Posarac, A, Officer, A, Verdes, E, et al. Socioeconomic inequality in disability among adults: a multicountry study using the world health survey. Am J Public Health. (2013) 103:1278–86. doi: 10.2105/AJPH.2012.301115
60. Cullinan, J, Gannon, B, and Lyons, S. Estimating the extra cost of living for people with disabilities. Health Econ. (2011) 20:582–99. doi: 10.1002/hec.1619
61. Vega-Salas, MJ, Caro, P, Johnson, L, Armstrong, MEG, and Papadaki, A. Socioeconomic inequalities in physical activity and sedentary behaviour among the Chilean population: a systematic review of observational studies. Int J Environ Res Public Health. (2021) 18:9722. doi: 10.3390/ijerph18189722
62. Rawal, LB, Smith, BJ, Quach, H, and Renzaho, AMN. Physical activity among adults with low socioeconomic status living in industrialized countries: a meta-ethnographic approach to understanding socioecological complexities. J Environ Public Health. (2020) 2020:1–13. doi: 10.1155/2020/4283027
63. Buffart, LM, Westendorp, T, Van Den Berg-Emons, RJ, Stam, HJ, and Roebroeck, ME. Perceived barriers to and facilitators of physical activity in young adults with childhood-onset physical disabilities. J Rehabil Med. (2009) 41:881–5. doi: 10.2340/16501977-0420
64. Shields, N, Bruder, AM, and Cleary, SL. An exploratory content analysis of how physiotherapists perceive barriers and facilitators to participation in physical activity among adults with disability. Physiother Theory Pract. (2019) 37:149–57. doi: 10.1080/09593985.2019.1623957
65. Werneck, AO, Araujo, RHO, Aguilar-Farias, N, Ferrari, G, Brazo-Sayavera, J, García-Witulski, C, et al. Time trends and inequalities of physical activity domains and sitting time in South America. J Glob Health. (2022) 12:04027. doi: 10.7189/jogh.12.04027
66. Pinilla-Roncancio, M, and Caicedo, NR. Legislation on disability and employment: to what extent are employment rights guaranteed for persons with disabilities? Int J Environ Res Public Health. (2022) 19:5654. doi: 10.3390/ijerph19095654
67. Pinilla-Roncancio, M, and Gallardo, M. Inequality in labour market opportunities for people with disabilities: evidence for six Latin American countries. Glob Soc Policy. (2022) 23:67–91. doi: 10.1177/14680181211070201
68. Barrado, VJ, Suckel, JL, Olhabé, BT, and Cona, FC. Promoted urbanization of the countryside: the case of Santiago’s periphery, Chile (1980–2017). Land (Basel). (2020) 9:1–20. doi: 10.3390/land9100370
69. Sadarangani, KP, von Oetinger, A, Cristi-Montero, C, Cortínez-O’Ryan, A, Aguilar-Farías, N, and Martínez-Gómez, D. Beneficial association between active travel and metabolic syndrome in Latin-America: a cross-sectional analysis from the Chilean National Health Survey 2009–2010. Prev Med (Baltim). (2018) 107:8–13. doi: 10.1016/j.ypmed.2017.12.005
70. Sit, C, Aubert, S, Carty, C, Silva, DAS, López-Gil, JF, Asunta, P, et al. Promoting physical activity among children and adolescents with disabilities: the translation of policy to practice internationally. J Phys Act Health. (2022) 19:758–68. doi: 10.1123/jpah.2022-0351
71. Booyens, M, Van Pletzen, E, and Lorenzo, T. The complexity of rural contexts experienced by community disability workers in three southern African countries. Afr J Disabil. (2015) 4:1–9. doi: 10.4102/ajod.v4i1.167
72. Jaarsma, EA, Geertzen, JHB, de Jong, R, Dijkstra, PU, and Dekker, R. Barriers and facilitators of sports in Dutch Paralympic athletes: an explorative study. Scand J Med Sci Sports. (2014) 24:830–6. doi: 10.1111/sms.12071
Keywords: disabled persons, sports for persons with disabilities, COVID-19, Latin America, socioeconomic factors, physical activity
Citation: Henríquez M, Ramirez-Campillo R, Cristi-Montero C, Reina R, Alvarez C, Ferrari G, Aguilar-Farias N and Sadarangani KP (2023) Alarming low physical activity levels in Chilean adults with disabilities during COVID-19 pandemic: a representative national survey analysis. Front. Public Health. 11:1090050. doi: 10.3389/fpubh.2023.1090050
Edited by:
Jim Lusted, The Open University, United KingdomReviewed by:
Borja Suarez-villadat, Alfonso X el Sabio University, SpainEsmaeel Saemi, Shahid Chamran University of Ahvaz, Iran
Copyright © 2023 Henríquez, Ramirez-Campillo, Cristi-Montero, Reina, Alvarez, Ferrari, Aguilar-Farias and Sadarangani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kabir P. Sadarangani, a2FiaXIuc2FkYXJhbmdhbmlAY2xvdWQudWF1dG9ub21hLmNs