
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 02 March 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1087044
This article is part of the Research TopicSoil-Transmitted Helminth Infections from a One Health PerspectiveView all 5 articles
 Muhammed O. Afolabi1*
Muhammed O. Afolabi1* Doudou Sow2
Doudou Sow2 Ibrahima Mbaye3
Ibrahima Mbaye3 Marie Pierre Diouf3
Marie Pierre Diouf3 Mor Absa Loum4Elhadji Babacar Fall4Amadou Seck3Isaac A. Manga4Cheikh Cissé3
Mor Absa Loum4Elhadji Babacar Fall4Amadou Seck3Isaac A. Manga4Cheikh Cissé3 Baba Camara5Awa Diouf3Ndéye Aida Gaye3Aminata Colle Lo4
Baba Camara5Awa Diouf3Ndéye Aida Gaye3Aminata Colle Lo4 Brian Greenwood1Jean Louis A. Ndiaye3
Brian Greenwood1Jean Louis A. Ndiaye3Background: Concurrent infections of Plasmodium falciparum with Soil Transmitted Helminths (STH) and Schistosoma spp are still a major public health problem among children living in Sub-Saharan Africa. We conducted two prospective studies among children living in urban and rural settings of Senegal, where control programmes for malaria, STH and schistosomiasis have been sustained, to determine the prevalence of malaria-helminth co-infection.
Methods: We enrolled 910 children aged 1–14 years from Saraya and Diourbel districts of Senegal in June and November 2021, respectively. We collected finger-prick blood samples from the children for malaria parasite detection using microscopy and PCR methods. Stool samples were also collected and Kato-Katz and PCR methods were used to detect STH and S. mansoni; and Merthiolate-iodine-formalin (MIF) test for other intestinal protozoans. Urine samples were analyzed using a filtration test, Point of Care Circulating Cathodic Antigens (POC-CCA) and PCR methods for detection of S. haematobium. Statistical analyses were performed to compare the continuous and categorical variables across the two study sites and age groups, as well as using the adjusted Odds ratios (aOR) to explore risk factors for malaria-helminth co-infections.
Results: The overall prevalence of polyparasitism with P. falciparum, STH, S. haematobium and S. mansoni among children in the two study sites was 2.2% (20/910) while prevalence of P. falciparum-S. haematobium co-infection was 1.1% (10/910); P. falciparum-S. mansoni 0.7% (6/910) and P. falciparum with any intestinal protozoan 2.4% (22/910). Co-infection was slightly higher among 5–14 year old children (17/629, 2.7%; 95% CI: 1.43–3.97) than 1–4 years (3/281, 1.1%; 95% CI: −0.12–2.32) and, in boys (13/567, 2.3%; 95% CI: 1.27–3.96) than girls (7/343, 2.1%; 95% CI: 0.52–3.48). Children aged 5–14 years (aOR = 3.37; 95% CI: 0.82–13.77, p = 0.09), who were boys (aOR = 1.44; 95% CI: 0.48–4.36, p = 0.51) and lived in Saraya (aOR = 1.27; 95% CI: 0.24–6.69, p = 0.77) had a higher risk of malaria-helminth co-infection than other age group, in girls and those who lived in Diourbel. Living in houses with spaces between the walls and roofs as well as frequent contacts with water during swimming were statistically significant risk factors for malaria-helminth co-infection.
Conclusions: The prevalence of malaria-helminth co-infection is low in two districts in Senegal, possibly due to sustained implementation of effective control measures for malaria and NTDs. These findings could help to develop and implement strategies that would lead to elimination of malaria and helminths in the study areas.
Co-existence of two or more parasitic infections in a human host has been described in the literature as “polyparasitism” or “multiparasitism” (1, 2). This concept of concomitant infections with multiple species of parasites is well documented in children living in low-and middle-income countries (LMIC) (3, 4). Apart from the high burden of single parasitic infections and their associated health consequences, concurrent infections with Plasmodium falciparum, soil transmitted helminths (STH) and/or Schistosomes impact child growth and development (5, 6). Climatic factors and poor socio-economic conditions that support the persistence of the malaria parasite vectors and the infective larval stages of STHs and Schistosoma spp have been widely reported to favor the geographic overlap of these multiple parasitic infections, especially in Sub-Saharan Africa (SSA) (4). Despite the devastating impact of both malaria and helminth infections on child survival, vertical control programmes targeting single parasitic infection are still being implemented in most co-endemic settings in SSA. Historical data have shown that coverage of these control programmes fluctuates and their effectiveness varies depending on the preventive chemotherapy used and the duration between cycles (7). In addition, variations in uptake of chemotherapy have contributed to the survival of parasites in certain areas and age groups, mainly among children (8).
Although a reduction in the prevalence of mono-infection with Plasmodium spp (9, 10), and STH (11, 12) has been reported in many African communities as a result of sustained implementation of various control strategies, concurrent infections with malaria, STH and schistosomiasis still remain a significant public health threat. In such co-endemic settings, vertical control measures that target a single parasitic infection may not be the optimum control strategy to interrupt the transmission cycle of the parasites.
Monitoring the prevalence of parasitic infections is recommended before and after the implementation of a control campaign in order to understand the transmission dynamics of the targeted parasite at the population level. However, in many countries with co-endemic parasitic infections, control programmes are often implemented without comprehensive baseline data, mainly because of financial challenges and logistical factors related to undocumented channels of accessing the control medications (13). In addition, most impact assessment studies deploy traditional diagnostic methods which tend to underestimate the prevalence of parasitic infections, especially in low transmission settings. Given that accurate diagnostic tools play a pivotal role in monitoring of treatment efficacies in mass drug administration (MDA) programmes, there is a need for the deployment of improved, yet simple and cost-effective diagnostic tool to detect mixed infections in a single reaction (14). This approach will provide reliable estimates of the prevalence of co-existing parasitic infections, in line with the goals of the new WHO 2030 NTD road map which now focuses on eliminating STH and schistosomiasis as a public health problem (11). The WHO Global technical strategy for malaria 2016–2030, which sets the target of reducing global malaria incidence and mortality rates by at least 90% by 2030 and accelerate progress toward malaria elimination is consistent with the 2030 NTD road map (15).
Given the changing landscape of transmission of malaria, STH and schistosomiasis in SSA, integrated approaches to tackle multiply-related infectious diseases are key WHO recommendations to achieve the 2030 targets. In 2022, the Kigali Declaration pledged USD 4.25 billion to support an end to malaria and NTDs by 2030 (16). Given this development, obtaining reliable data on the prevalence of co-infection with malaria, STH and schistosomiasis across endemic areas becomes an increasingly important prerequisite to developing locally appropriate control strategies that could interrupt transmission of these infections. We designed the studies reported in this paper to measure the co-prevalence of helminths and malaria in two areas of Senegal as a prelude to the design of an integrated control strategy.
We conducted two prospective, population-based studies among pre-school and school-aged children in Saraya and Diourbel districts of Senegal in June and November 2021, respectively. The study period did not correspond to a peak of malaria transmission in the two study sites. Further details about the settings and population for these study areas have been described elsewhere (17). Briefly, Saraya is a rural settlement in the south-eastern region of Senegal while Diourbel, in the western region of the country is largely sub-urban. Saraya and Diourbel are about 740 km south and 134 km east of Dakar, the capital of Senegal, respectively (Figure 1). The two communities share similar epidemiological profiles. Saraya and Diourbel districts have a tropical Sudano-Sahelian climate with well-defined dry and humid seasons that result from northeast winter winds and southwest summer winds. There are two seasons: a dry season from November to May and a rainy season from May to November in Saraya and in Diourbel, rains starts in July. Mean daily temperatures range from 14 to 36°C from July to February and 21–40°C from March to June. While malaria, STH and schistosomiasis have almost been eliminated in most districts in Senegal, Diourbel and Saraya were parts of communities that had a persistent, high burden of malaria (18) and helminths (19). In both districts, control programmes for STH and schistosomiasis have been implemented annually since 2014 (20). Also, Seasonal Malaria Chemoprevention (SMC) was introduced in 2013 in Saraya district and from 2019 in Diourbel district, with high levels of coverage achieved in both districts (20).
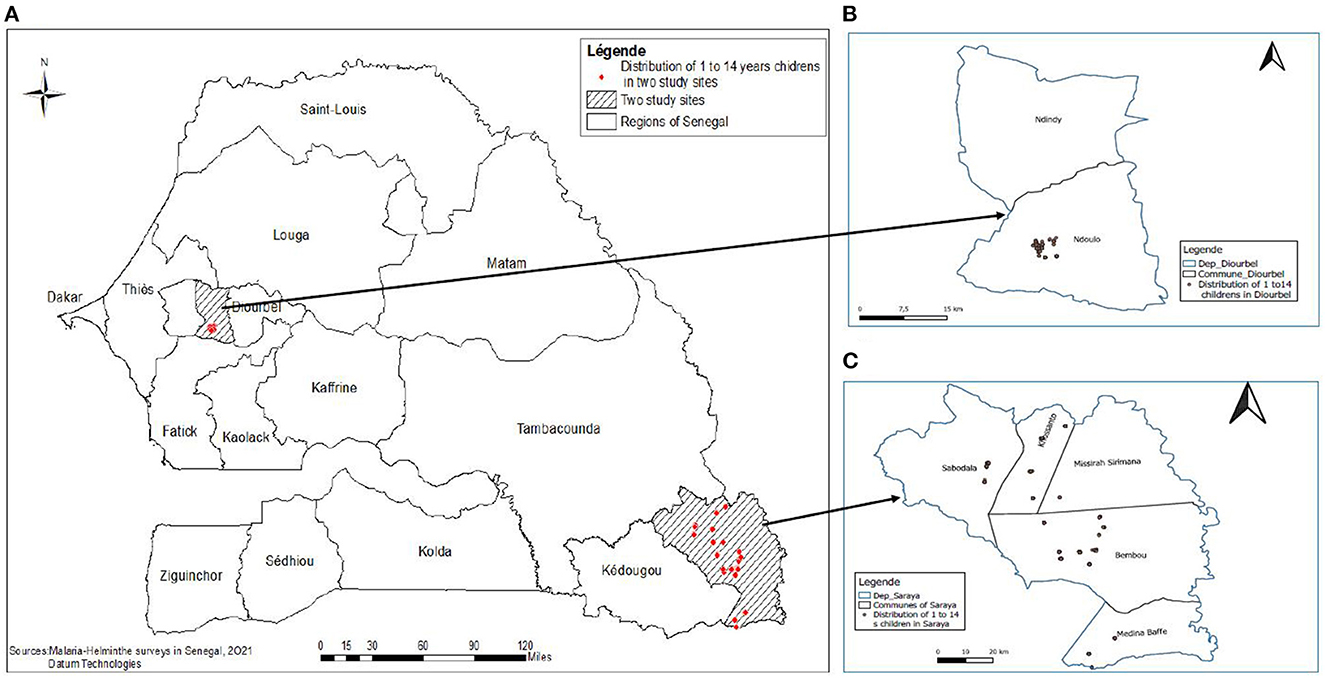
Figure 1. (A–C) Map of Senegal showing the two study sites in Saraya and Diuorbel districts.
This study was conducted among pre-school and school-aged children (1–14 years) of either gender, who had been resident in the study areas for at least 6 months and whose parents or primary caregivers consented to their participation in the study. In Saraya site, the primary caregivers were the parents and guardians of these children. In Diourbel site, pre-school and school aged children lived as full boarders in Koranic schools (also called “dahras”) where they received Arabic education. The primary caregivers of the children in these schools were Koranic teachers, heads of Koranic schools and their wives.
Given that the prevalence of malaria-helminth co-infections was reported to be 13–25% among West African children (21–24), a minimum total sample size of 500 male and female children was needed to show that the variation of true prevalence was not more than 5% when improved diagnostic tools were used to detect the co-infection. Using multi-stage sampling, we selected representative households in Saraya district and Koranic schools in Diourbel district. We subsequently collected household information and the number of male and female children by age group (1–4 and 5–14 years) in the selected households and schools in the two sites. Next, we selected randomly the households or schools in the enumeration databases. To ensure a fair representation of households in the study sites, the Lot Quality Assurance Sampling technique (25) was used to recruit study participants. For example, a total of 15 children, with a roughly even mix of boys and girls, ranging in ages from 1–4 and 5–14 years, was randomly selected in each household within the selected village or Koranic school (Figure 2).
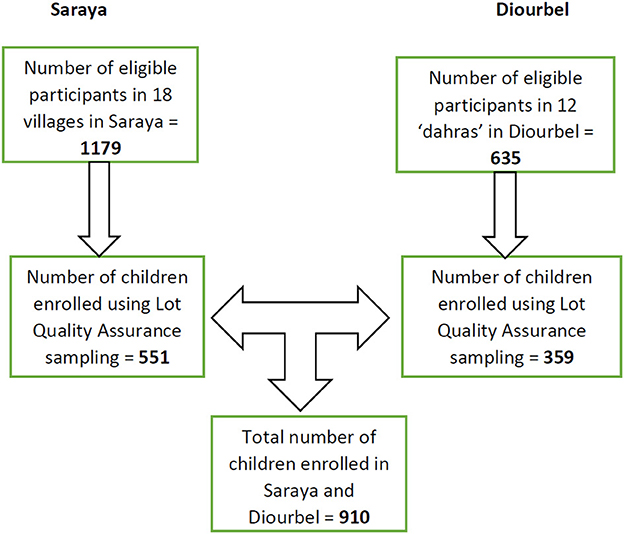
Figure 2. Flow chart showing enrolment process of study participants in Saraya and Diourbel, 2021.
The studies were conducted in collaboration with the SMC and NTD programmes of the Senegal Ministry of Health and Social Action, which provided strategic support that facilitated community acceptance and mobilization. Prior to the commencement of the studies, engagement meetings with the community leaders, heads of households and parents/care-givers of potentially eligible children were undertaken to explain the study, using a simple picture depicting the burden and impact of concomitant infections with malaria and helminth in children, its rationale and the informed consent procedure, including risk and benefits of allowing children to participate in the study. After each meeting, trained research assistants identified parents/caregivers of potential study participants to explain the study further to them on an individual basis. Parents/caregivers who considered that the study was appropriate for their child/ward were visited at home at a mutually agreed time for further engagements and a formal consent procedure was completed. After obtaining written informed consent from a parent/primary care-giver, the research staff who were native speakers of a local language spoken widely in the community, administered a purpose-designed electronic questionnaire to the parents/care-givers using the local language of preference. The questionnaire covered information on socio-demographic features, health and residence characteristics, household wealth, bed net use, history of deworming and malaria treatment, environmental and behavioral factors predisposing children to co-infections with malaria and helminths. Finger-prick blood samples were collected from each participant for thick and thin smear microscopy, and filter paper blots were collected for Plasmodium DNA isolation and PCR amplification for species determination. Also, freshly voided urine and stool samples were collected for microscopic detection of Schistosoma spp and STH eggs.
To comply with COVID-19 public health measures that were in place at the time of the studies, body temperature was measured using a digital, non-contact, infra-red thermometer. A study participant was considered febrile, if the temperature was ≥ 37.5 °C. Height was measured to the nearest 0.1 cm using a wall-mounted stadiometer; weight was measured to the nearest 0.5 kg using a digital weighing scale, and mid-upper arm circumference (MUAC) was measured using a graduated, color-coded tape recommended by UNICEF. These measurements were used to estimate anthropometric indices including weight-for-age; height for-age and weight-for height. Anthropometric indices were computed as z-scores based on the WHO growth reference curves using the WHO AnthroPlus 1.0.4 for personal computers manual. Underweight was defined as a weight-for-age (WA) z score of < – 2, wasting as a weight-for-height (WH) z score of < – 2 and stunting as height-for-age (HA) z score of < – 2. A child was categorized as being malnourished, if they scored < – 2 in one of the anthropometric indices of WA, HA and WH indices (26).
Blood was collected by finger-prick for malaria parasite detection. Thick and thin blood films were prepared following standard operational procedures. Thin blood films were fixed in methanol and thick blood films were de-hemoglobinised in water before Giemsa staining. The blood films were examined microscopically following standard procedures (27). Slides were considered positive when asexual forms and/or gametocytes of any Plasmodium species were observed on the blood film. Two experienced microscopists read all slides independently. Malaria parasite density per μl of blood was determined by counting the number of parasites per 200 leukocytes and multiplying by an average value of white blood cell count, considered to be 8,000/ul. Parasitaemia was classified as low (≤ 500 parasite/μl of blood), moderate (501–5000 parasites/μl of blood) and high (> 5000 parasites/μl of blood).
A freshly voided urine sample was collected from each study participant into a pre-labeled plastic container with a screw cap. The urine sample was drawn from the plastic container using a syringe and filtered through a polycarbonate membrane filter (STERLITECH Corporation, Washington, USA). The filter membrane was examined microscopically for the presence of schistosome eggs (27). Ten percent of negative samples and all positive samples were re-read by a senior laboratory staff member immediately after the first reading to validate the results. Schistosome egg density was expressed as the number of eggs in 10 ml urine (eggs/10 ml) and the intensity of infection was categorized as either light (< 50 eggs/10 ml) or heavy infection (≥ 50 eggs/10 ml) (28).
In addition, parallel testing for schistosome circulating cathodic antigens (CCA) in urine was undertaken (29). The urine CCA dipstick test has been extensively used in SSA and has sensitivity and specificity values ranging from 52.5 to 63.2% and 57.7 to 75.6%, respectively (30, 31). Two drops of urine were added to the circular well of the test cassette. Following 20 min of incubation, results were determined by visual reading (Schisto POC-CCA cassette based test; Rapid Medical Diagnostics, Pretoria, South Africa).
Fresh stool samples were collected, smears were prepared, and examined using the Kato-Katz thick smear method (27). Duplicate smears were prepared for each specimen using a 41.7 mg Kato-Katz template. Each slide was allowed to clear for 30 min, and then examined at 100 × total magnification within 1 h of preparation to avoid missing hookworm eggs. The number of eggs counted per slide was multiplied by 24 to obtain the egg count per gram (epg) of feces. As a quality control measure, all positive slides and 50% of randomly selected negative smears were re-examined independently by a third parasitologist. An average of the counts was utilized. For A. lumbricoides, participants with 1–4 999 epgs were classified as having light infection, those with 5 000–49 999 epg as moderate, and ≥ 50 000 as heavy infections. For T. trichuria, participants with 1–999 epg was light infection; 1 000–9 999 epg as moderate, and ≥ 10 000 as heavy infection. The intensity of infections was classified according to WHO guidelines for S. mansoni infection into light (1–99 eggs/g of stool (epg), moderate (100–399 epg) and heavy infections (≥400 epg) (28).
The traditional fixation method, MIF technique (32), was used to further examine the stool samples. The 2 × 24 Copro-Duo Kit (RAL Diagnostics, France) was used to highlight protozoan cysts, schistosome eggs and unfertilized Ascaris eggs. Stool samples were added to cryotubes to which Mercurothiolate, Iodine and Formalin (MIF) solution (4 drops of Lugol in 15 microliters of MIF) was added. The samples were stored at +4°C, smears prepared and examined for parasite eggs using 10x and 40x microscope objectives.
Dried blood spot, urine and stool samples were analyzed using PCR methods described in the Supplementary file S1.
Descriptive analyses including median and interquartile range (IQR), geometric means, frequencies, and proportions were undertaken to summarize the data. Means and proportions were constructed for continuous and categorical variables, respectively. The study participants were categorized into pre-school (1–4 years) and school aged (5–14 years) children. Co-infection was defined as infection involving Plasmodium spp with at least one helminth parasite. Differences in the proportions between the two study sites were compared using Pearson's Chi-squared (χ2) and Fisher Exact tests. Correlation coefficient (r) was used to establish the relationship between the different parasite densities. Uni-variable regression analyses were used to explore risk factors for malaria-helminth co-infections. Odds ratios and 95% confidence intervals were obtained for each explanatory variable and malaria-helminth co-infection in the respective logistic models. The adjusted odds ratio (aOR) in the multivariate analysis was used to establish the strength of the association of the risk factors with the co-infection. Variables with p-values < 0.05 were considered indicative of statistical significance. All data were analyzed using R 4.1.1 software.
Ethical approvals for this study were obtained from the Research Ethics Committee of the London School of Hygiene and Tropical Medicine and the Comité National d'Ethique pour la Recherche en Santé (CNERS) in Senegal. Written informed consent was obtained from parents/caregivers whose children participated in the study after explaining the purpose and benefits of their participation. Participation was voluntary, and personal data collected about the study children were anonymised, kept confidential and held in compliance with international data privacy protection laws and regulations. Participants who had positive results for P. falciparum were treated with a complete course of the first line treatment recommended by the Senegal national treatment guideline policy for uncomplicated malaria (artesunate-amodiaquine), participants with an STH were treated with a single dose of albendazole; and praziquantel was used to treat children who had positive results for schistosomiasis (33).
From 14 to 21 June 2021, we enrolled 551 children from 18 villages of Saraya district, and 359 children in 12 randomly selected Koranic schools in Diourbel district from 3 to 6 November 2021. The median ages (IQR) for children aged 1–4 years were 3.3 (2.5–4) and 4 (3–4) in Saraya and Diourbel sites respectively. Among the 5–14 years age group, the median ages (IQR) were 8.1 (7, 8.5) and 9.3 (8, 11) in Saraya and Diourbel, respectively. An almost equal number of boys and girls were enrolled in Saraya (275/551, 49.9%) and Diourbel (276/551, 50.1%), respectively. However, 297 boys (297/359, 82.7%) and only 62 girls (62/359, 17.3%) were enrolled in Diourbel. A similar proportion of children were found to be malnourished in Saraya and Diourbel: 98/551 (17.8%) and (68/359, 18.9%), respectively. A majority of children in Saraya lived in houses owned by their parents/caregivers (506/551, 91.8%), while about three-fifths of the children (231/359, 64.3%) in Diourbel lived in the houses owned by their primary caregivers. Majority of houses where the children in Diourbel lived were made of block and cement 247/359 (68.8%) while in Saraya the majority lived in houses built from wood (233/258, 42.1%), or mud (135, 24.4%). Similar proportions of children in Diourbel and Saraya lived in houses which had no net on their doors (349/351, 97.2% vs. 542/551, 98.3%) or windows (349/359, 97.2% vs. 540/551, 98%). More than 80% of the children in Diourbel, compared to about 65% of the children in Saraya had bed nets in their houses: (302/359, 84.1% vs. 360/551, 65.3%) respectively and more than three-fifth of the children in Diourbel slept under a bed net every night (224/359, 62.4%) compared to slightly over half of the children in Saraya (312/551, 56.6%) (Table 1).
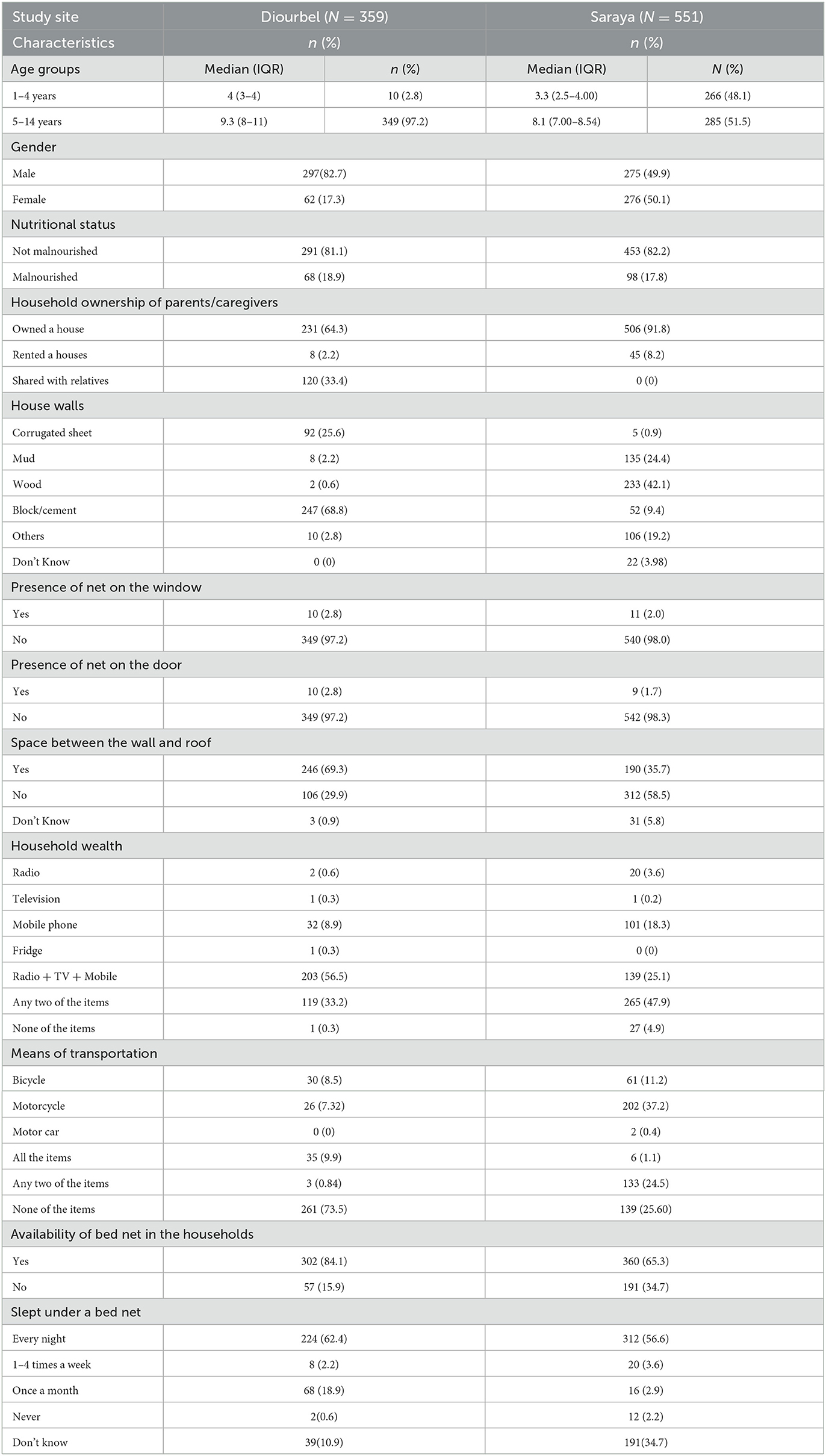
Table 1. Socio-demographic characteristics of study participants, Saraya and Diourbel, 2021.
More than half of the children in Diourbel lived in houses where toilet facilities were shared among many family members; this proportion was higher among children in Saraya (190/359, 52.9% vs. 423/551, 76.8%). Almost all children in Diourbel and Saraya used water to clean their anus following defaecation (355/359, 98.9% and 550 /551, 99.8%), respectively. However, only about two-fifth of the children in Diourbel and one-third of Saraya children washed their hands with soap and water after defaecation (149/359, 41.5% and 157/551, 28.5%), respectively. The source of drinking water in more than 60% of children in Diourbel was from a public tap water (241/351, 67.1%) while the most common source of drinking among Saraya children was from a public borehole (237/551, 42.9%). While about 13% of children in Saraya had daily exposure to river water through activities such as swimming (76/551, 13.7%), this was reported in only two children in Diourbel (2/359, 0.6%). Playing in sandy areas was practiced by a majority of the children in both study sites (353/359, 98.3% and 488/551, 88.6%, respectively); walking barefooted was reported in 11.3% of Saraya children (61/551, 11.3%) and in six children from Diourbel (6/359, 1.7%). Slightly more than 10% of the children in Saraya reported fever in the 28 days prior to this study (72/551, 13.1%) while this was reported in only one child in Diourbel (1/359, 0.3%). Nearly half of the children in Diourbel and a quarter of the children in Saraya had received deworming drugs in the 12 months preceding the study (173/359, 48.2% and 140/551, 25.5%). Similarly, above half of Diourbel and Saraya children received antimalarial treatment more than 8 weeks before the studies (202/359, 56.4% and 391/551, 71%, respectively) (Table 2).

Table 2. Social and behavioral practices of study participants, Saraya and Diourbel districts, 2021.
Across the two study sites, the combined prevalence of P. falciparum and P. malariae detected by microscopy was 4.2% (38/908) and 7.1% (26/364) by PCR. The combined methods yielded a total prevalence of 5.9% (54/908). A mixed infection with P. falciparum and P. malariae was seen in only one child. P. faciparum was detected in 29 children aged 5–14 years (29/630, 3.2%) and in 24 boys (24/569, 4.2%).
The overall prevalence of STH spp detected by microscopy in both sites was 1.4% (11/778) and 1.2% (9/767) by PCR. The combined methods showed a prevalence of 2.4% (19/787). T. trichiura was detected in six children (6/778, 0.8%), a mixed infection with A. lumbricoides and T. trichiura was detected in only one child. and A. duodenale was detected by PCR in one child. T. trichiura was slightly more common among children aged 5–14 years (10/577, 2.9%) than in 1–4 years old (2/208, 1.0%) and, in boys (9/515, 1.8%) than girls (3/270, 1.1%). A similar pattern of distribution was observed in the overall prevalence of any STH spp.
Fifty-one children had S. haematobium detected by the urine filtration test (51/857, 6%), 29 of whom had light and 22 had heavy infections. Eighteen children were detected to have S. mansoni by Kato-Katz method (18/857, 2.1%), all of whom had light infections. Utilizing PCR, 84 children had S. haematobium (84/868, 9.7%) and 41 children had a S. mansoni infection (41/868, 4.7%), giving an overall prevalence of 14.4%. The rapid POC-CCA test showed that 154 children had Schistosoma spp (154/874, 28.6%). S. haematobium infection was more common among 1–4 years old (37/254, 14.6%) and boys (69/558, 12.4%) than in 5–14 year old (65/618, 10.5%) or in girls (33/314, 10.5%). S. mansoni was also more common among 1–4 year olds (17/254, 6.7%) and in girls (24/314, 7.6%) than in 5–14 years (27/618, 4.4%) or boys (20/558, 3.6 %). The prevalence of mixed infection with S. haematobium and S. mansoni was 29% (253/874); with a higher prevalence observed in children aged 1–4 years (115/254, 45.3%) than in 5–14 year olds (138/618, 22.3 %) and in girls (111/314, 35.4%) compared with boys (141/558, 25.3%). More than half of the children had at least one intestinal protozoa (394/771, 51.1%). The prevalence of Giardia intestinalis, Blastocytis hominis and Entamoeba coli were 27.7, 22.2 and 18.9%, respectively. Intestinal protozoas were more common among children aged 5–14 years (279/569, 49%) than in 1–4 year olds (115/276, 56.9%) and in girls (138/338, 52.7 %) than in boys (253/507, 50.1%). The prevalence of polyparasitism with P. falciparum, STH, S. haematobium and S. mansoni among the children was 2.2% (20/910) while the prevalence of P. falciparum-S. haematobium co-infection was 1.1% (10/910), that of P. falciparum-S. mansoni 0.7% (6/910) and of P. falciparum with any intestinal protozoa 2.4% (22/910). Co-infection was higher among 5–14 year old children (17/629, 2.7%) than in 1–4 year olds (3/281, 1.1%) and in boys (13/567, 2.3%) than in girls (7/343, 2.1%) (Table 3).

Table 3. Prevalence of malaria, STH, schistosomiasis, intestinal protozoa and malaria-helminth co-infection by diagnostic methods, age group, and gender of study participants, Saraya and Diourbel, 2021.
Table 4 summarizes the correlation of malaria parasite density with age group, gender and intensity of S. haematobium infection. The mean malaria parasite density was higher among participants aged 1–4 years than in children aged 5–14 years and in those who were girls and had light S. haematobium infection.
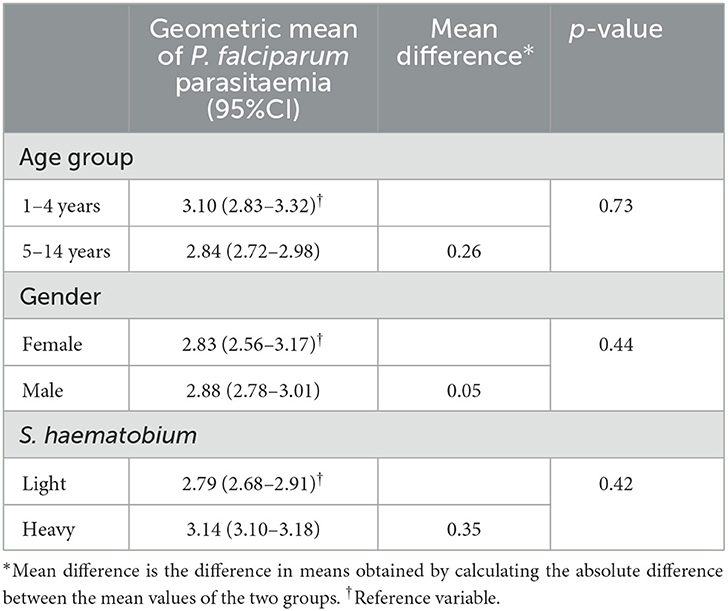
Table 4. Intensity of malaria parasitaemia (per μl of blood) in relation to age group, gender, and helminth infection status of study participants, Saraya and Diourbel, 2021.
Univariate analysis showed that participants aged 5–14 years, who were boys and lived in Saraya had a higher risk of malaria-helminth co-infection than their counterparts but this association did not a reach statistical significance. On the other hand, living in houses with spaces between the walls and roofs as well as frequent contacts with water during swimming were statistically significant risk factors for malaria-helminth co-infection. When adjusted for confounding factors, living in houses with spaces between the walls and roofs remained the only statistically significant risk factor for malaria-helminth co-infection (Table 5).
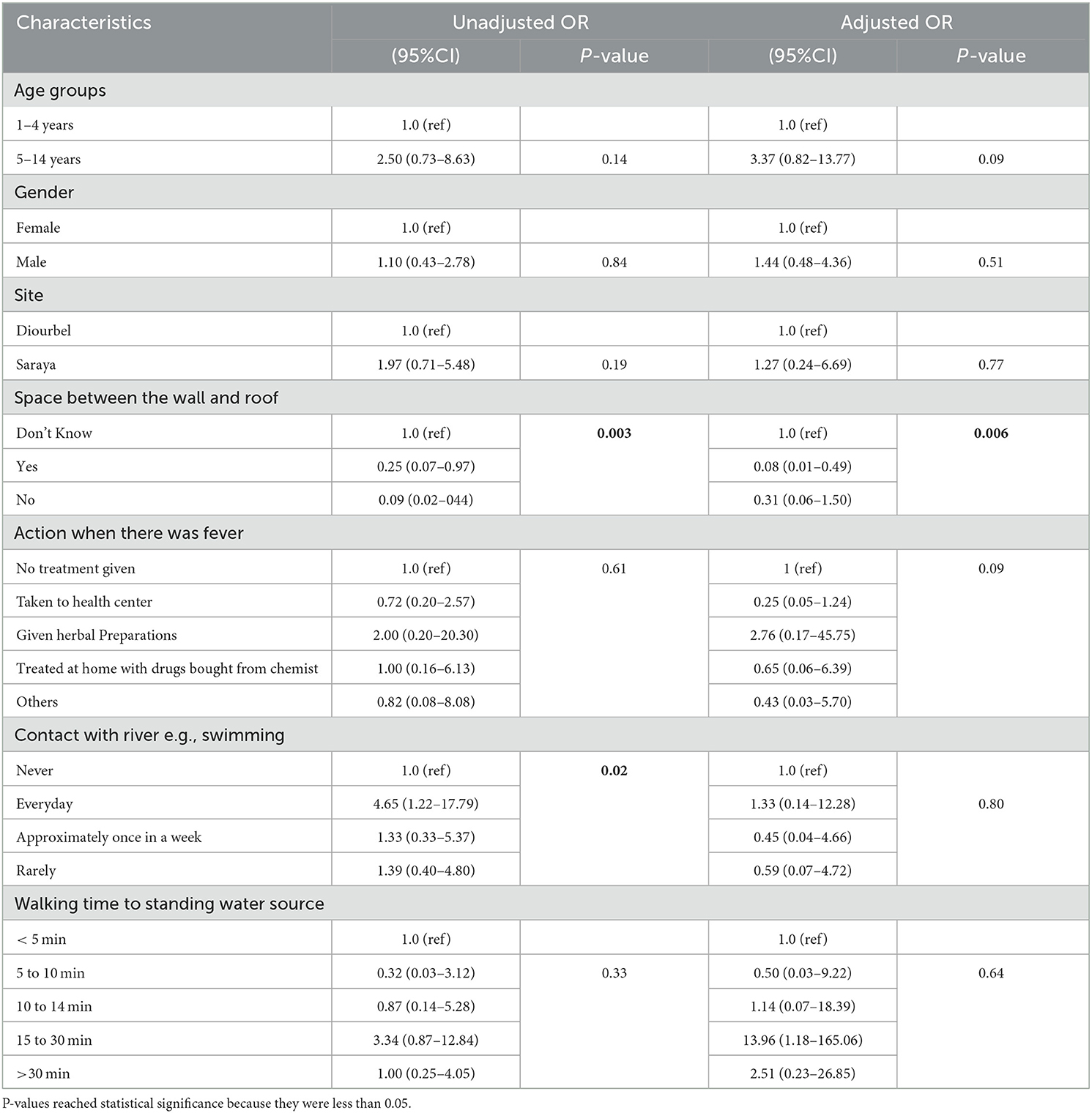
Table 5. Risk factors for malaria-helminth co-infections among study participants, Saraya and Diourbel combined, 2021.
Comprehensive monitoring of control programmes targeting malaria and NTDs are crucial to assess the impact of the interventions, and align them toward achieving the new WHO road maps that now focus on elimination of these diseases by 2030. We conducted the studies in two epidemiological distinct yet similar settings in Senegal where malaria and NTD control programmes have been consistently implemented. Despite the rural and sub-urban locations of the two study sites, the socio-demographic features of the study participants were largely similar. However, disparities were observed in the fewer girls and relatively low number of children aged 1–4 years enrolled in Diourbel compared to Saraya where equal numbers of boys and girls were enrolled. One of the reasons for these differences is that the house-to-house recruitment approach adopted in the rural communities of Saraya was not logistically feasible in the sub-urban setting of Diourbel because of its cosmopolitan nature and relatively high population density. Hence, the recruitment of study participants was done through the Koranic school platform which enjoys a very high enrolment for pre-school and school-aged children in Senegal.
Also, despite the striking differences in the house structures in the two study sites, a similar proportion of children in Diourbel and Saraya lived in houses which had no net on the doors or windows. However, household ownership of, and sleeping under, a treated bed net was higher among Diourbel children than their counterparts in Saraya. A similar trend was observed in hand hygiene following defaecation where a relatively higher proportion of children in Diourbel practiced hand washing with soap and water.
Our findings showed that the prevalence of polyparasitism with P. falciparum, STH, S. haematobium and S. mansoni among the children was very low at 2.2%, despite the use of conventional and improved diagnostic methods such as PCR. Similar low trends were observed for co-infections with P. falciparum-S. haematobium, P. falciparum-S. mansoni and P. falciparum with any intestinal protozoa. These results contrast sharply with the findings of similar studies conducted in co-endemic communities in SSA (34–39). A plausible reason for the striking differences may be due to the fact that our studies were conducted in 2021 while previous studies reporting higher prevalence of Plasmodium-helminth co-infection were conducted between 2010 and 2015 when control programmes for malaria and NTDs were sub-optimal in many countries. The findings of a very low prevalence of the polyparasitism in our studies are likely to be a direct consequence of the impact of effective malaria and NTD control measures which included case-management with drug treatment, application of indoor residual spraying (IRS), distribution of insecticide-treated nets (ITN) and integrated vector management measures that were consistently implemented on a yearly basis in Senegal (20, 40). Similar findings have been reported in the neighboring Gambia where malaria (41, 42), and NTD (43) have also reached pre-elimination stages. However, a few recently conducted studies in other West African countries (44, 45) and in many other Sub-Saharan countries have shown that the prevalence of malaria is still very high, especially among pre-school and school aged children (46) Though not as high as the burden of malaria in these African countries, the epidemiological profile of STH and schistosomiasis are also higher than the findings of our studies. For example, a recently conducted study in a co-endemic community in Sierra Leone reported a malaria prevalence of about 30% among children aged 1–11 years and 12.5% for STH (44). Despite sharing similar epidemiological and environmental features, the findings from Sierra Leone differ remarkably from an overall prevalence of 3.5% obtained for Plasmodium spp across our two study sites. In the same vein, the overall prevalence of STH spp in our studies was about 1%, making our study areas a strong candidate for STH elimination as a public health problem (EPHP), as defined by the WHO NTD road map of attaining a prevalence of < 2% of moderate-to-heavy intensity infections (11). Although effective implementation of malaria and NTD control programmes have been widely cited as the major reason for the disparities in the burden of malaria and STH in our study areas and other African countries (9, 10, 12), more empirical studies are needed to unravel other contributing factors that may be responsible for the wide differences obtained in our study areas and other African countries where the burden of malaria-helminth co-infection is still high.
Unexpectedly, the prevalence of schistosomiasis in our studies did not follow a similar trend observed for malaria and STH. Given that mass drug administration of preventive chemotherapy for STH and schistosomiasis are implemented concurrently during national campaigns in Senegal, an overall prevalence of 28.6% by POC-CCA test suggested that schistosomiasis control is not as effective as for STH. Although, a prevalence of schistosome infection of 8% was obtained with the Kato-Katz method while PCR gave a prevalence of 14%, we did not observe in our study the limitations in diagnostic accuracy surrounding the use of POC-CCA rapid test in low endemic settings where low parasite burden is common (47). The Kato-Katz method is known to be less sensitive in low transmission settings, hence, its use yielded the lowest prevalence for detection of Schistosomes in our studies. The relatively high prevalence of schistosomiasis identified by PCR and POC-CCA tests in our studies might be explained from poor uptake of praziquantel among children. Due to its unpleasant taste, many children have been reported to spit or vomit praziquantel within few minutes of administration. A pediatric formulation of praziquantel has recently been developed and evaluated in clinical trials to overcome this limitation, but it will not be ready for deployment until 2024 (48).
Although, the prevalence of co-infection involving P. falciparum and intestinal protozoa was low in our studies, more than half of the children had at least one intestinal protozoa, with the prevalence of 27.7, 22.2 and 18.9% for Giardia intestinalis, Blastocystis hominis and Entamoeba coli, respectively. Despite Kato-Katz technique being the gold standard method recommended for detection of intestinal helminths, it did not identify any of these protozoas. This confirms the superiority of the MIF technique deployed in our studies, despite being a simpler and less expensive technique that performs competitively with Kato-Katz in both laboratory and field work on intestinal helminths, particularly in resource-limited settings (49). Although STH appears to be moving toward elimination stage in our study areas, the burden of multiple intestinal protozoa was still very high. Various factors in the biology of the intestinal protozoans, including the high excretion rate, low infectious dose, and the robustness of the cyst transmission stage, are particularly suited for transmission in our study sites. Most NTD control programmes deploy the WHO recommended albendazole or mebendazole as the preventive chemotherapy of choice for STH control, (50) which however is not effective against the intestinal protozoas. Given the need to tackle this silent burden of high intestinal protozoans by a cross-disciplinary and collaborative approach, an addition of a single-dose of tinidazole to the current NTD preventive chemotherapy may be justified, due to the challenges of poor compliance with multiple doses of metronidazole.
The distribution pattern of polyparasitism involving P. falciparum, STH, S. haematobium and S. mansoni in our studies showed a higher preponderance among 5–14 years old children and boys. The same patterns were also observed for co-infections with P. falciparum-STH, P. falciparum- S. haematobium, and P. falciparum-S. mansoni. These findings agree with the results of some other studies conducted in co-endemic settings in SSA (1, 51, 52), while a few other studies reported different distribution patterns (39, 53, 54). A main reason for the similarities of our findings with other studies is the high prevalence among male school-aged children which increased their risk to co-infection with P. falciparum and multiple helminths. Different socio-cultural practices which placed some activities such as fetching water on young girls, thereby exposing them frequently to contaminated water and increased their risk for the co-infection accounted for the different findings reported in other studies (39, 53, 54). Univariate analysis in our studies showed that living in houses with spaces in the roofs and walls as well as frequent contacts with contaminated water were the risk factors for malaria-helminth co-infection. However, when this was adjusted for confounding variables, living in houses with spaces in the roofs and walls remained the only predictor of malaria-helminth co-infection. These findings require further confirmation because the children might also be exposed to other environmental risk factors and/or risky sanitation and hygiene practices which were not investigated.
The major limitation of our studies was the different timing of the implementation of the two studies as the first study was conducted in Saraya at the beginning of malaria transmission season in June 2021, whilst the second study was conducted at the end of malaria transmission in Diourbel. These timings might have impacted on our findings but these times were selected to avoid the overlap with the implementation of SMC campaigns which run from June to September and the MDA campaigns for STH and schistosomiasis which are held annually around October in the study sites. To ensure that we obtained reliable estimates of the epidemiological profile of malaria-helminth co-infection, we deployed both conventional and improved diagnostic methods which strengthened our findings. We will also conduct further analysis using Luminex multiplex assays (55) to understand the exposure history of the children and the transmission dynamics of Plasmodium and helminth co-infection in our study areas.
We found a very low prevalence of malaria-helminth co-infection in two diverse settings in Senegal, but the prevalence of mono-infection with schistosomiasis and intestinal protozoans was high among the pre-school and school-aged children. The incidence of co-infection was bound to be low because of the low prevalence of malaria. Low parasite loads could represent chronic parasite infections which may play a major role in multiple morbidities, the impact of which are often sub-clinical acting as reservoirs that make interruptions of cycles of infection transmission impossible. Therefore, more studies are needed to obtain reliable estimates of malaria-helminth co-morbidity in high and low transmission settings. This will provide country-specific evidence to guide the development of cross-cutting approaches that would address the critical gaps in implementation of strategies that may help achieve the WHO targets of eliminating malaria and NTD by 2030.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the London School of Hygiene and Tropical Medicine and the Comité National d'Ethique pour la Recherche en Santé (CNERS) in Senegal. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
MOA conceptualized the study and developed the first draft of the manuscript. MOA, BG, JLAN, and DS developed the study protocol. MOA, JLAN, and DS supervised the data collection. IM, EBF, and IAM coordinated the field work. ACL, MPD, NAG, and AD performed the laboratory analysis. MAL analyzed the data. BG, JLAN, and DS reviewed the manuscript critically for important intellectual contents. All authors reviewed and approved the final draft of the manuscript.
This study is implemented as part of a career development fellowship awarded to MOA, which is funded under the UK Research and Innovation Future Leaders Fellowship scheme (MR/S03286X/1). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
We appreciate Dr. Babacar Gueye, Dr. Doudou Sene, Dr. Ndeye M'Backé Kane, Dr. Boubacar Diop and the entire management at the Senegal National Malaria Control Programme, NTD Control Programme, SMC Programme and the Ministry of Health and Social Action for supporting the implementation of this study. We also thank the Medical Directors and staff of Saraya and Diourbel Health Centers as well as all child-participants and their parents/caregivers.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1087044/full#supplementary-material
1. Sumbele IUN, Otia OV, Bopda OSM, Ebai CB, Kimbi HK, Nkuo-Akenji T. Polyparasitism with Schistosoma haematobium, Plasmodium and soil-transmitted helminths in school-aged children in Muyuka-Cameroon following implementation of control measures: a cross sectional study. Inf Dis Poverty. (2021) 10:14. doi: 10.1186/s40249-021-00802-x
2. Pullan R, Brooke S. The health impact of polyparasitism in humans: are we underestimating the burden of parasitic diseases? Parasitology. (2008) 135:783–94. doi: 10.1017/S0031182008000346
3. Courtin D, Djilali-Saïah A, Milet J, Soulard V, Gaye O, Migot-Nabias F, et al. Schistosoma haematobium infection affects Plasmodium falciparum-specific IgG responses associated with protection against malaria. Parasite Immunol. (2011) 33:124–31. doi: 10.1111/j.1365-3024.2010.01267.x
4. Brooker S, Akhwale W, Pullan R, Estambale B, Clarke SE, Snow RW, et al. Epidemiology of plasmodium-helminth co-infection in Africa: populations at risk, potential impact on anemia, and prospects for combining control. Am J Trop Med Hyg. (2007) 77:88–98. doi: 10.4269/ajtmh.2007.77.88
5. Ezeamama AE, McGarvey ST, Acosta LP, Zierler S, Manalo DL, Wu HW, et al. The synergistic effect of concomitant schistosomiasis, hookworm, and trichuris infections on children's anemia burden. PLoS Negl Trop Dis. (2008) 2:e245. doi: 10.1371/journal.pntd.0000245
6. Degarege A, Legesse M, Medhin G, Animut A, Erko B. Malaria and related outcomes in patients with intestinal helminths: a cross-sectional study. BMC Infect Dis. (2012) 12:291. doi: 10.1186/1471-2334-12-291
7. Steinmann P, Utzinger J, Du ZW, Zhou XN. Multiparasitism a neglected reality on global, regional and local scale. Adv Parasitol. (2010) 73:21–50. doi: 10.1016/S0065-308X(10)73002-5
8. Dye C, Mertens T, Hirnschall G, Mpanju-Shumbusho W, Newman RD, Raviglione MC, et al. WHO and the future of disease control programmes. Lancet. (2013) 381:413–8. doi: 10.1016/S0140-6736(12)61812-1
9. Pabalan N, Singian E, Tabangay L, Jarjanazi H, Boivin MJ, Ezeamama AE. Soil-transmitted helminth infection, loss of education and cognitive impairment in school-aged children: a systematic review and meta-analysis. PLoS Negl Trop Dis. (2018) 12:e0005523. doi: 10.1371/journal.pntd.0005523
10. Kamau A, Mogeni P, Okiro EA. A systematic review of changing malaria disease burden in sub-Saharan Africa since 2000: comparing model predictions and empirical observations. BMC Med. (2020) 18: 94. doi: 10.1186/s12916-020-01559-0
11. WHO. Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030. Geneva: World Health Organization (2020).
12. Alemu A, Shiferaw Y, Ambachew A, Hamid H. Malaria helminth co-infections and their contribution for aneamia in febrile patients attending Azzezo health center, Gondar, Northwest Ethiopia: a cross sectional study. Asian Pac J Trop Med. (2012) 5:803–9. doi: 10.1016/S1995-7645(12)60147-3
13. Sartorius B, Cano J, Simpson H, Tusting LS, Marczak LB, Miller-Petrie MK, et al. Prevalence and intensity of soil-transmitted helminth infections of children in sub-Saharan Africa, 2000-18: a geospatial analysis. Lancet Glob Health. (2021) 9:e52–60. doi: 10.1016/S2214-109X(20)30398-3
14. Winkler S, Willheim M, Baier K, Schmid D, Aichelburg A, Graninger W, et al. Reciprocal regulation of Th1- and Th2-cytokine-producing T cells during clearance of parasitemia in Plasmodium falciparum malaria. Infect Immun. (1998) 66:6040–4. doi: 10.1128/IAI.66.12.6040-6044.1998
15. WHO/UNICEF/UNU. Iron Deficiency Anemia: Assessment, prevention and Control: A Guide for Programme Managers. World Health Organization, Geneva. (2011). Available online at: https://www.who.int/nutrition/publications/en/ida_assessment_prevention_control.pdf (accessed July 21, 2020).
16. Basic Laboratory Methods in Medical Parasitology. (2020). Available online at: https://www.who.int/malaria/publications/atoz/9241544104_part1/en/ (accessed July 21, 2020).
17. Le Hesran JY, Akiana J. Ndiaye el HM, Dia M, Senghor P, Konate L. Severe malaria attack is associated with high prevalence of Ascaris lumbricoides infection among children in rural. Senegal Trans R Soc Trop Med Hyg. (2004) 98:397–9. doi: 10.1016/j.trstmh.2003.10.009
18. Malaria in Senegal: Statistics Facts. (2022) Available online at: https://www.severemalaria.org/countries/senegal-0 (accessed March 10, 2022).
19. Senegal ESPEN - World Health Organization. (2022) Available online at: https://espen.afro.who.int/countries/senegal (accessed March 10, 2022).
20. Expanded Special Project for Elimination of Neglected Tropical Diseases (ESPEN). (2020) Available online at: https://espen.afro.who.int/ (accessed June 12, 2020).
21. Ademowo GO, Rabiu O, Kosoko A. Dada-adegbola H, Arinola G, Falade C. Prevalence and interaction of malaria and helminth co-infections among symptomatic and asymptomatic children in Southwest Nigeria. Int J Inf Diseases. (2014) 21:297. doi: 10.1016/j.ijid.2014.03.1035
22. Babamale OA, Ugbomoiko US, Heukelbach J. High prevalence of Plasmodium falciparum and soil-transmitted helminth co-infections in a periurban community in Kwara State, Nigeria. J Infect Public Health. (2018) 11:48–53. doi: 10.1016/j.jiph.2017.03.002
23. Yapi RB, Hürlimann E, Houngbedji CA, Ndri PB, Silué KD, Soro G, et al. Infection and co-infection with helminths and plasmodium among school children in côte d'ivoire: results from a national cross-sectional survey. PLoS Negl Trop Dis. (2014) 8:e2913. doi: 10.1371/journal.pntd.0002913
24. Sokhna C, Le Hesran J-Y, Mbaye PA, Akiana J, Camara P, Diop M, et al. Increase of malaria attacks among children presenting concomitant infection by Schistosoma mansoni in Senegal. Malar J. (2004) 3:43. doi: 10.1186/1475-2875-3-43
25. Brooker S, Kabatereine NB, Myatt M, Russell Stothard J, Fenwick A. Rapid assessment of Schistosoma mansoni: the validity, applicability and cost-effectiveness of the lot quality assurance sampling method in Uganda. Tropical Med Int Health. (2005) 10:647–58 doi: 10.1111/j.1365-3156.2005.01446.x
26. Abanyie FA, McCracken C, Kirwan P, Molloy SF, Asaolu SO, Holland CV, et al. Ascaris co-infection does not alter malaria-induced anaemia in a cohort of Nigerian preschool children. Malar J. (2013) 12:1. doi: 10.1186/1475-2875-12-1
27. Cheesbrough M. District Laboratory Practice in Tropical Countries: Part1 and 2. Cambridge: Cambridge University Press. (2014).
28. Montresor A, Crompton DWT, Hall A, Bundy DAP, Savioli L. Guidelines for the Evaluation of Soil-Transmitted Helminthiasis and Schistosomiasis at Community Level. Geneva: World Health Organization (1998).
29. Van Lieshout L, De Jonge N. el Masry NA, Mansour MM, Krijger FW, Deelder AM. Improved diagnostic performance of the circulating antigen assay in human schistosomiasis by parallel testing for circulating anodic and cathodic antigens in serum and urine. Am J Trop Med Hyg. (1992) 47:463–9. doi: 10.4269/ajtmh.1992.47.463
30. Sousa-Figueiredo JC, Betson M, Kabatereine NB, Stothard JR. The urine circulating cathodic antigen (CCA) dipstick: a valid substitute for microscopy for mapping and point-of-care diagnosis of intestinal schistosomiasis. PLoS Negl Trop Dis. (2013) 7:e2008. doi: 10.1371/journal.pntd.0002008
31. Mazigo HD, Kepha S. Kinung'hi SM. Sensitivity and specificity of point-of-care circulating Cathodic antigen test before and after praziquantel treatment in diagnosing Schistosoma mansoni infection in adult population co-infected with human immunodeficiency virus-1, North-Western Tanzania. Arch Pub Health. (2018) 76:29. doi: 10.1186/s13690-018-0274-4
32. Sapero JJ, Lawless DK. The MIF stain-preservation technic for the identification of intestinal protozoa. Am J Trop Med Hyg. (1953) 2:613–9. doi: 10.4269/ajtmh.1953.2.613
33. Prevention control of schistosomiasis soil-transmitted helminthiasis. World Health Organ Tech Rep Ser. (2002) 912:1–57. Available online at: https://pubmed.ncbi.nlm.nih.gov/12592987/
34. Ayeh-Kumi PF, Addo-Osafo K, Attah SK, Tetteh-Quarcoo PB, Obeng-Nkrumah N, Awuah-Mensah G, et al. Malaria, helminths and malnutrition: a cross-sectional survey of school children in the South-Tongu district of Ghana. BMC Res Notes. (2016) 9:242. doi: 10.1186/s13104-016-2025-3
35. Bisanzio D, Mutuku F, Bustinduy AL, Mungai PL, Muchiri EM, King CH, et al. Cross-sectional study of the burden of vector-borne and soil-transmitted polyparasitism in rural communities of Coast Province, Kenya. PLoS Negl Trop Dis. (2014) 8:e2992. doi: 10.1371/journal.pntd.0002992
36. Kepha S, Nuwaha F, Nikolay B, Gichuki P, Edwards T, Allen E, et al. Epidemiology of coinfection with soil transmitted helminths and Plasmodium falciparum among school children in Bumula District in western Kenya. Parasit Vectors. (2015) 8:314. doi: 10.1186/s13071-015-0891-5
37. Mazigo HD, Waihenya R, Lwambo NJ, Mnyone LL, Mahande AM, Seni J, et al. Co-infections with Plasmodium falciparum, Schistosoma mansoni and intestinal helminths among school children in endemic areas of northwestern Tanzania. Parasit Vectors. (2010) 3:44. doi: 10.1186/1756-3305-3-44
38. Mekachie Sandie S, Sumbele IUN, Tasah MM, Kimbi HK. Malaria and intestinal parasite co-infection and its association with anaemia among people living with HIV in Buea, Southwest cameroon: a community-based retrospective cohort study. PLoS ONE. (2021) 16:e0245743. doi: 10.1371/journal.pone.0245743
39. Salim N, Knopp S, Lweno O, Abdul U, Mohamed A, Schindler T, et al. Distribution and risk factors for Plasmodium and helminth co-infections: a cross-sectional survey among children in Bagamoyo district, coastal region of Tanzania. PLoS Negl Trop Dis. (2015) 9:e0003660. doi: 10.1371/journal.pntd.0003660
40. The Malaria Atlas Project. (2020). Available online at: https://malariaatlas.org/ (accessed June 12, 2020).
41. Ceesay SJ, Casals-Pascual C, Nwakanma DC, Walther M, Gomez-Escobar N, Fulford AJ, et al. Continued decline of malaria in the gambia with implications for elimination. PLoS ONE. (2010) 5:e12242. doi: 10.1371/journal.pone.0012242
42. Adedoja A, Tijani BD, Akanbi AA, Ojurongbe TA, Adeyeba OA, Ojurongbe O. Co-endemicity of Plasmodium falciparum and intestinal helminths infection in school age children in rural communities of kwara state Nigeria. PLoS Neglected Tropical Diseases. (2015) 9:e0003940. doi: 10.1371/journal.pntd.0003940
43. Ajayi IO, Afonne C, Dada-Adegbola H, Falade CO. Prevalence of asymptomatic malaria and intestinal helminthiasis co-infection among children living in selected rural communities in ibadan Nigeria. Am J Epidemiol Inf Dis. (2015) 3:15–20.
44. Baiden F, Fleck S, Leigh B, Ayieko P, Tindanbil D, Otieno T, et al. Prevalence of malaria and helminth infections in rural communities in northern Sierra Leone, a baseline study to inform Ebola vaccine study protocols. PLoS ONE. (2022) 17:e0270968. doi: 10.1371/journal.pone.0270968
45. Carmona-Fonseca J, Uscátegui Peñuela RM, Correa Botero AM. Parasitosis intestinal en niños de zonas palúdicas de Antioquia (Colombia). Iatreia. (2009) 22:27–46.
46. Mawili-Mboumba DP, Koumba Lengongo JV, Offouga Mbouoronde C, Nkoghe D, et al. Prevalence of and risk factors for malaria, filariasis, and intestinal parasites as single infections or co-infections in different settlements of Gabon. Inf Dis Poverty. (2018) 7:6. doi: 10.1186/s40249-017-0381-4
47. Peralta JM, Cavalcanti MG. Is POC-CCA a truly reliable test for schistosomiasis diagnosis in low endemic areas? The trace results controversy. PLoS Neglected Tropical Dis. (2018) 12:e0006813. doi: 10.1371/journal.pntd.0006813
48. Kinung'hi SM, Magnussen P, Kaatano GM, Kishamawe C, Vennervald BJ. Malaria and helminth co-infections in school and preschool children: a cross-sectional study in Magu district, north-western Tanzania. PloS One. (2014) 9:e86510. doi: 10.1371/journal.pone.0086510
49. Incani RN, Homan T, Pinelli E, Mughini-Gras L, Guevara H, Jesus J. Comparison between merthiolate-iodine-formalin and Kato-Katz methods for the diagnosis of human helminth infections in resource-limited settings. J Helminthol. (2017) 91:657–64. doi: 10.1017/S0022149X16000766
50. Lo NC, Addiss DG, Hotez PJ, King CH, Stothard JR, Evans DS, et al. A call to strengthen the global strategy against schistosomiasis and soil-transmitted helminthiasis: the time is now. Lancet Infect Dis. (2017) 17:e64–e9. doi: 10.1016/S1473-3099(16)30535-7
51. Sumbele IU, Nkemnji GB, Kimbi HK. Soil-transmitted helminths and Plasmodium falciparum malaria among individuals living in different agroecosystems in two rural communities in the mount Cameroon area: a cross-sectional study. Inf Dis Poverty. (2017) 6:67. doi: 10.1186/s40249-017-0266-6
52. Sumbele IUN, Otia OV, Francis L, Bopda OSM, Ebai CB, Ning TR, et al. Confounding influences of malnutrition and Plasmodium falciparum and Schistosoma haematobium infections on haematological parameters in school children in Muyuka, Cameroon. BMC Infect Dis. (2021) 21:477. doi: 10.1186/s12879-021-06201-9
53. Ojo OE, Adebayo AS, Awobode HO, Nguewa P, Anumudu CI. Schistosoma haematobium and Plasmodium falciparum co-infection in Nigeria 2001–2018: a systematic review and meta-analysis. Sci Afr. (2019) 3:e000186. doi: 10.1016/j.sciaf.2019.e00186
54. Tuasha N, Hailemeskel E, Erko B, Petros B. Comorbidity of intestinal helminthiases among malaria outpatients of Wondo Genet health centers, southern Ethiopia: implications for integrated control. BMC Infect Dis. (2019) 19:659. doi: 10.1186/s12879-019-4290-y
55. Wu L, Hall T, Ssewanyana I, Oulton T, Patterson C, Vasileva H, et al. Optimisation and standardisation of a multiplex immunoassay of diverse Plasmodium falciparum antigens to assess changes in malaria transmission using sero-epidemiology. Wellcome Open Res. (2019) 4:26. doi: 10.12688/wellcomeopenres.14950.1
Keywords: burden, co-endemicity, geohelminths, malaria, bilharzia (schistosomiasis), Sub-Saharan Africa
Citation: Afolabi MO, Sow D, Mbaye I, Diouf MP, Loum MA, Fall EB, Seck A, Manga IA, Cissé C, Camara B, Diouf A, Gaye NA, Colle Lo A, Greenwood B and Ndiaye JLA (2023) Prevalence of malaria-helminth co-infections among children living in a setting of high coverage of standard interventions for malaria and helminths: Two population-based studies in Senegal. Front. Public Health 11:1087044. doi: 10.3389/fpubh.2023.1087044
Received: 01 November 2022; Accepted: 14 February 2023;
Published: 02 March 2023.
Edited by:
Mathieu Nacher, INSERM CIC1424 Centre d'Investigation Clinique Antilles Guyane, French GuianaReviewed by:
Nirianne Querijero Palacpac, Osaka University, JapanCopyright © 2023 Afolabi, Sow, Mbaye, Diouf, Loum, Fall, Seck, Manga, Cissé, Camara, Diouf, Gaye, Colle Lo, Greenwood and Ndiaye. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Muhammed O. Afolabi, bXVoYW1tZWQuYWZvbGFiaUBsc2h0bS5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.