 Hamid Sharif Nia1
Hamid Sharif Nia1 Kelly-Ann Allen2
Kelly-Ann Allen2 Gökmen Arslan3,4
Gökmen Arslan3,4 Harpaljit Kaur5
Harpaljit Kaur5 Long She6
Long She6 Fatemeh Khoshnavay Fomani7*
Fatemeh Khoshnavay Fomani7* Ozkan Gorgulu8
Ozkan Gorgulu8 Erika Sivarajan Froelicher9,10
Erika Sivarajan Froelicher9,10- 1Traditional and Complementary Medicine Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran
- 2School of Educational Psychology and Counselling, Faculty of Education, Monash University, Melbourne, VIC, Australia
- 3Department of Psychological Counselling and Guidance, Mehmet Akif Ersoy University, Burdur, Türkiye
- 4Centre for Wellbeing Science, University of Melbourne, Melbourne, VIC, Australia
- 5School of Management and Marketing, Faculty of Business and Law, Taylor's University, Subang Jaya, Malaysia
- 6Faculty of Business, Design and Arts, Swinburne University of Technology, Kuching, Sarawak, Malaysia
- 7School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
- 8Department of Biostatistics and Medical Informatics, Kirşehir Ahi Evran University Faculty of Medicine, Kırşehir, Türkiye
- 9Department of Physiological Nursing, School of Nursing, University of California, San Francisco, San Francisco, CA, United States
- 10Department of Epidemiology and Biostatistics, School of Medicine, University of California, San Francisco, San Francisco, CA, United States
Background and purpose: Recent new mutations and increases in transmission of COVID-19 among adolescents and children highlight the importance of identifying which factors influence parental decisions regarding vaccinating their children. The current study aims to explore whether child vulnerability and parents' attitudes toward vaccines mediate the association between perceived financial well-being and vaccine hesitancy among parents.
Method: A predictive, cross-sectional, multi-country online questionnaire was administered with a convenience sample of 6,073 parents (Australia, 2,734; Iran, 2,447; China, 523; Turkey, 369). Participants completed the Parent Attitude About Child Vaccines (PACV), the Child Vulnerability Scale (CVS), a Financial Well-being (FWB) measure, and Parental Vaccine Hesitancy (PVH) questionnaire.
Results: The current study revealed that perceived financial well-being had significant and negative associations with parents' attitudes toward COVID-19 vaccines and child vulnerability among the Australian sample. Contrary to the Australian findings, results from Chinese participants indicated that financial well-being had significant and positive predictive effects on parent attitudes toward vaccines, child vulnerability, and parental vaccine hesitancy. The results of the Iranian sample revealed that parents' attitudes toward vaccines and child vulnerability significantly and negatively predicted parental vaccine hesitancy.
Conclusion: The current study revealed that a parents' perceived financial well-being had a significant and negative relationship with parental attitudes about vaccines and child vulnerability; however, it did not significantly predict parental vaccine hesitancy among Turkish parents as it did for parents in Australia, Iran, and China. Findings of the study have policy implications for how certain countries may tailor their vaccine-related health messages to parents with low financial wellbeing and parents with vulnerable children.
Introduction
Nowadays, some countries are preparing to announce the end of the COVID-19 pandemic. However, immunization remains a unique measure for protecting the population against this disease. The increasing number of COVID-19 cases and deaths has led governments worldwide to launch preventive strategies to control the pandemic (1–3) which assisted in flattening the pandemic curve, but there has been a resurgence in cases reported since the economies reopened (4, 5) and new variants emerged (6, 7). One of the strategies to curb the spread of the disease is the development of the COVID-19 vaccines which stimulate the immune system to produce antibodies against the virus (8). Promoting vaccination is crucial, especially among children and adolescents. However, due to the unprecedented speed and scale the vaccines were developed in some countries and settings (1, 9, 10), concerns regarding its effectiveness and safety have emerged (11–13), prompting vaccine hesitancy among healthcare workers (9, 14, 15), parents (16, 17), university students (18, 19), expectant mothers (20), and the general public (21–23).
Vaccine hesitancy is defined as the “delay in acceptance or refusal of vaccination despite availability of vaccination services” (24); p. 4,163. Previous research has linked vaccine hesitancy to age (9, 14, 25), education (26), occupation (9, 14, 27), trust (28–30), religious practices and beliefs (31, 32), vaccine misinformation (33–35), social media (36), miscalculation of risk and lack of knowledge (37), and gender (25, 38). Even though the number of cases of COVID-19 is increasing, vaccine hesitancy seems to be high across countries ranging from 10 to 50% (New Zealand 30%, Portugal 65%, Japan 43.9%, US 22%, and Singapore 33%) (39–43). The lowest rates of vaccine acceptance have been reported in the Middle East, Russia, Africa and several European countries (44).
One of the most significant public health challenges globally is addressing parental vaccine hesitancy, which has been identified previously for polio immunizations (45), measles, mumps and rubella (MMR) (46, 47), routine childhood vaccinations (48), and now for COVID-19 vaccines (26, 49). The acceptance of vaccination for children is highly influenced by parents' attitudes and feelings over the decision to vaccinate which varies from total acceptance to complete refusal (50, 51). Parents often worry about a combination of potential side effects of the vaccine (52–54), fear of compromising their children's immune systems (55), religious beliefs (56), and the fear of autism (57). This is linked to a lack of trust in the government (58, 59), the pharmaceutical industries (60, 61), and health providers (62, 63) as many presume there are motives behind promoting vaccinations (63, 64). These are often associated with newer vaccines (17) or the dissemination of vaccine misinformation from health care providers (59, 65) and the media (66, 67). Interestingly, studies have indicated that fathers, parents who are not vaccinated (68, 69), and negative vaccination experiences (70) play major roles in parents being hesitant about vaccinating their children. Resolving doubts on vaccination to provide higher immunization coverage for children is a critical concern for policymakers. There is a consensus that safe COVID-19 vaccines can end the current pandemic, and vaccine acceptance is as crucial as vaccine safety and effectiveness in the successful pandemic control (44).
Vaccine hesitancy
While vaccine hesitancy can present the individuals' adherence and acceptance of recommended vaccines for themselves (71), parental vaccine hesitancy may indicate that parents accept to vaccinate their children but are concerned about the vaccine's efficacy and safety (72). Vaccine-hesitant individuals may agree to some vaccines while refusing the other recommended vaccine for themselves or their children (73). Several individual, social, and cultural factors can determine the individual and parental willingness to get vaccines for themselves or their children (72). Although personal vaccine hesitancy does not necessarily lead to parental vaccine hesitancy, existing knowledge suggests a significant positive correlation between these two variables (74). Vaccine hesitancy has been identified as a public health challenge during the COVID-19 pandemic. The common personal reasons for refusing COVID-19 vaccines include concerns about safety and effectiveness, as well as the lack of trust in the vaccine's origin. People believe that the vaccines produced in a rush may be very dangerous or useless against COVID-19 (75). Similar to the other vaccines, parental hesitancy to the COVID-19 vaccines is a global public health concern and many studies focused on the factors that determine parents' willingness and intention to vaccinate their children against COVID-19 (76–78). Parental vaccine hesitancy hinders the immunization efforts for children against COVID-19 that aim to protect their health, as well as that of their community. Although some factors such as trust, attitude toward the COVID-19 vaccine safety and effectiveness, the perceived COVID-19 risk by parents, and parental satisfaction with social relations have been identified to be correlated with parental COVID-19 vaccine hesitancy (74, 79), further studies are recommended to investigate the factors affecting parental COVID-19 vaccine hesitancy.
Child vulnerability
Parental hesitancy over vaccination is closely linked to child vulnerability. Child vulnerability is defined as a parent's belief that a child is vulnerable to developmental or behavioral problems, and illness, or death (80). Considering Green and Solnit (81) and Forsyth et al. (80) suggest two underlying concepts that determine parents' perception of their child's vulnerability. These two concepts include the instance in which the child is medically vulnerable because of an existing health condition and the second concept include the instance in which the parents fear that their child may die (80). Past studies have found inconclusive relationship between vaccine hesitancy and child vulnerability variables (82, 83). However, parents of children with asthma, obesity, and other comorbid conditions were more hesitant in vaccinating their children (16) due to the risk of infection and vaccine side effects (70). Some parents who refuse vaccination for their children feel that their children are healthy and less vulnerable to the disease (70). On the contrary, with the increasing awareness on the need for immunization as COVID-19 severity increases and affects the health of vulnerable children, some parents approve vaccination (16).
Perceived financial well-being
Perceived financial well-being or the perception that an individual can fully meet their financial obligations now and in the future, has been found to negatively impact the hesitancy of parents toward vaccination (54, 83, 84). Parents who have low financial well-being tend to have diminished access to healthcare (80) and they are concerned about the cost of vaccinations, or potential medical costs if child experience an adverse reaction. Some studies suggest that parents experiencing financial pressures and stress are more likely to question the necessity and safety of vaccines than parents who have fewer financial concerns and high financial well-being (85). Generally, existing literature indicated that both low (85) and high financial status (86) can be considered as determinant factors of vaccine hesitancy among parents. Vaccination has been highly effective at decreasing the spread of some communicable diseases (87), thus mitigating childhood morbidity and mortality (88). With the new mutations and increased transmission of COVID-19 among young populations (89), it is important for this age group to be vaccinated to prevent further viral spread. In addition, to ensure that the vaccination efforts are at satisfactory levels, there is a need to overcome barriers related to parents' perceptions of low financial well-being and child vulnerability. Considering that research on this area is limited, the current study aims to investigate the relationships between financial well-being and vaccine hesitancy among parents by determining the drivers of hesitancy (83, 90). This study also aims to further explore whether child vulnerability and parent attitudes about vaccines mediate the association between financial well-being and vaccine hesitancy among parents.
Conceptual framework
Based on Roger's protection motivation theory (PMT) (1975, 1983), it is hypothesized that parental vaccine hesitancy is shaped by financial well-being (FWB), parent attitude about child vaccines (PACV), and child vulnerability (CVS). This theory justifies one's motivation to participate in protective behaviors, which are encouraged by threat stimulus (91). Based on PMT, a parent's decision of whether to participate in protective behaviors depends on two cognitive processes: coping and threat appraisal (92). Threat appraisal refers to one's adaptive actions which consist of threat severity, maladaptive rewards, and threat vulnerability (93) whereas coping appraisal indicates the ability of the individual to engage in protective behaviors in the presence of threat, (94) whereas threat appraisal refers to one's adaptive actions consist of threat severity, maladaptive rewards, and threat vulnerability. The uncertainties surrounding the side effects of the COVID-19 vaccine in children have caused increasing levels of fear among parents and may motivate parents to adopt protective behaviors as they may feel that there is no definitive treatment for the disease (95). The fear is further exacerbated by the vulnerability of the children, thus increasing the hesitancy of the vaccine among parents. In order to improve protection motivation, identifying and addressing the causes of reluctance through coping and threat appraisal procedures are needed.
Study hypotheses
In the light of the proposed conceptual research model and literature, the following hypotheses were developed:
Hypothesis 1: Financial well-being (FWB) is positively related to parent attitude about child vaccines (PACV).
Hypothesis 2: Financial well-being (FWB) is negatively related to child vulnerability (CVS).
Hypothesis 3: Financial well-being (FWB) is negatively related to parental vaccine hesitancy (PVH).
Hypothesis 4: Parent attitude about child vaccines (PACV) is negatively related to parental vaccine hesitancy (PVH).
Hypothesis 5: Child vulnerability (CVS) is related to parental vaccine hesitancy (PVH).
Hypothesis 6: Parent attitude about child vaccines (PACV) and child vulnerability (CVS) mediate the negative relationship between financial well-being (FWB) and parental vaccine hesitancy (PVH).
Method
Study design and participants
A cross-sectional, multi-country online study design was used to investigate the relationships between perceived financial wellbeing and parental vaccine hesitancy due to the pandemic, as well as the mediating role of the parents' attitudes toward COVID-19 vaccines and child vulnerability in these relationships (Figure 1). Data were collected over eight weeks, between 8 August 2021 and 1 October 2021. Parental vaccine hesitancy can be determined by a variety of individual and social factors identified in different study settings (44, 96). In this study, data were gathered from Australia, China, Turkey, and Iran which have almost similar COVID-19 vaccine hesitancy ranges (between 30 and 45%) among the general population despite their different socio-economic status (97–100).
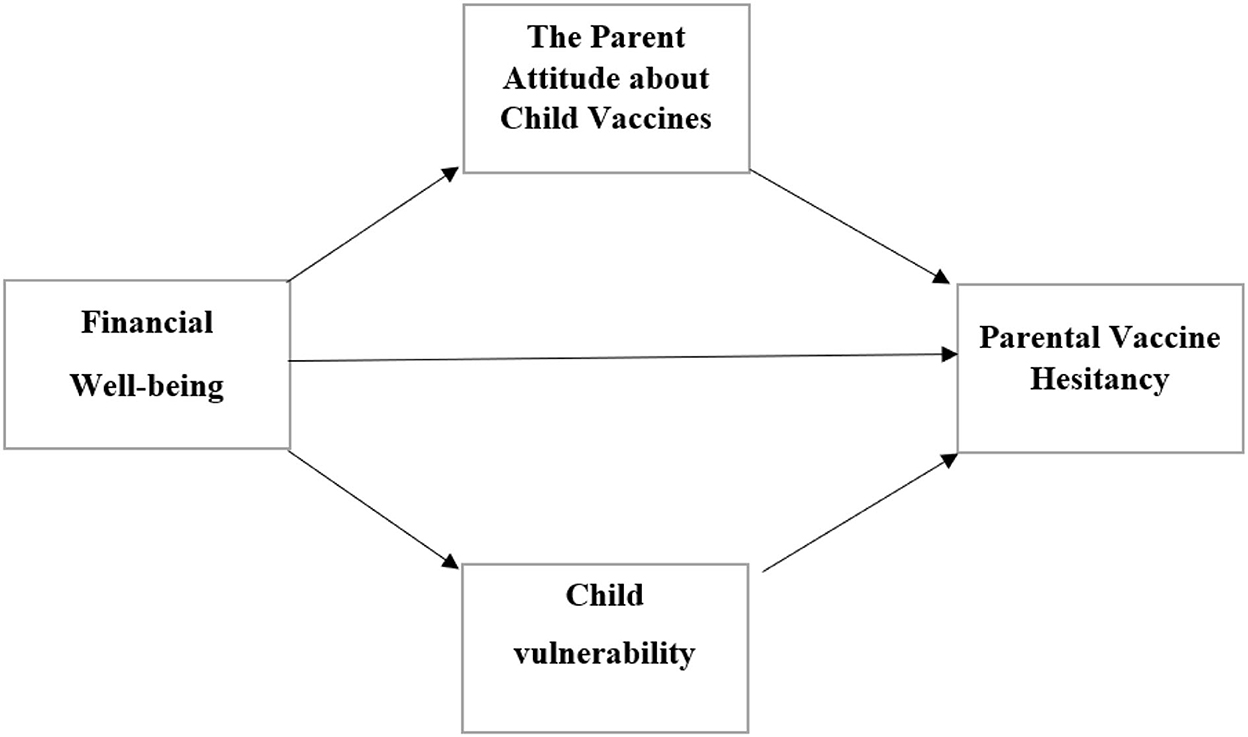
Figure 1. The proposed mediating model.
Inclusion criteria were: being a parent/caregiver of at least one child, having accessibility to a smartphone or another digital device to answer the web-based questionnaire, and having the ability to read the questionnaire items. The participants were recruited from Australia, Iran, China, and Turkey.
Data were gathered using a convenience sampling method along with probability sampling to reduce bias. The online questionnaire was prepared using Google form and a cover letter was included to provide the research aims and relevant information about the study. The questionnaire link was shared via popular messaging apps (e.g., WhatsApp, LinkedIn, Instagram, and Telegram) and in different virtual groups such as work groups, scientific groups, the newsgroup, and other popular groups. The questionnaire cover letter was prepared to introduce the research aims and provide any related information regarding the study. A total of 6,073 parents (Australia, 2,734; Iran, 2,447; China, 523; Turkey, 369) filled out the online questionnaire. The Iranian data were gathered in two phases: 1,187 parents participated in the study during the pre-5th waves of the COVID-19 outbreak, and 1,260 respondents contributed during the post-5th waves. The study participants' characteristics are presented in Table 1.
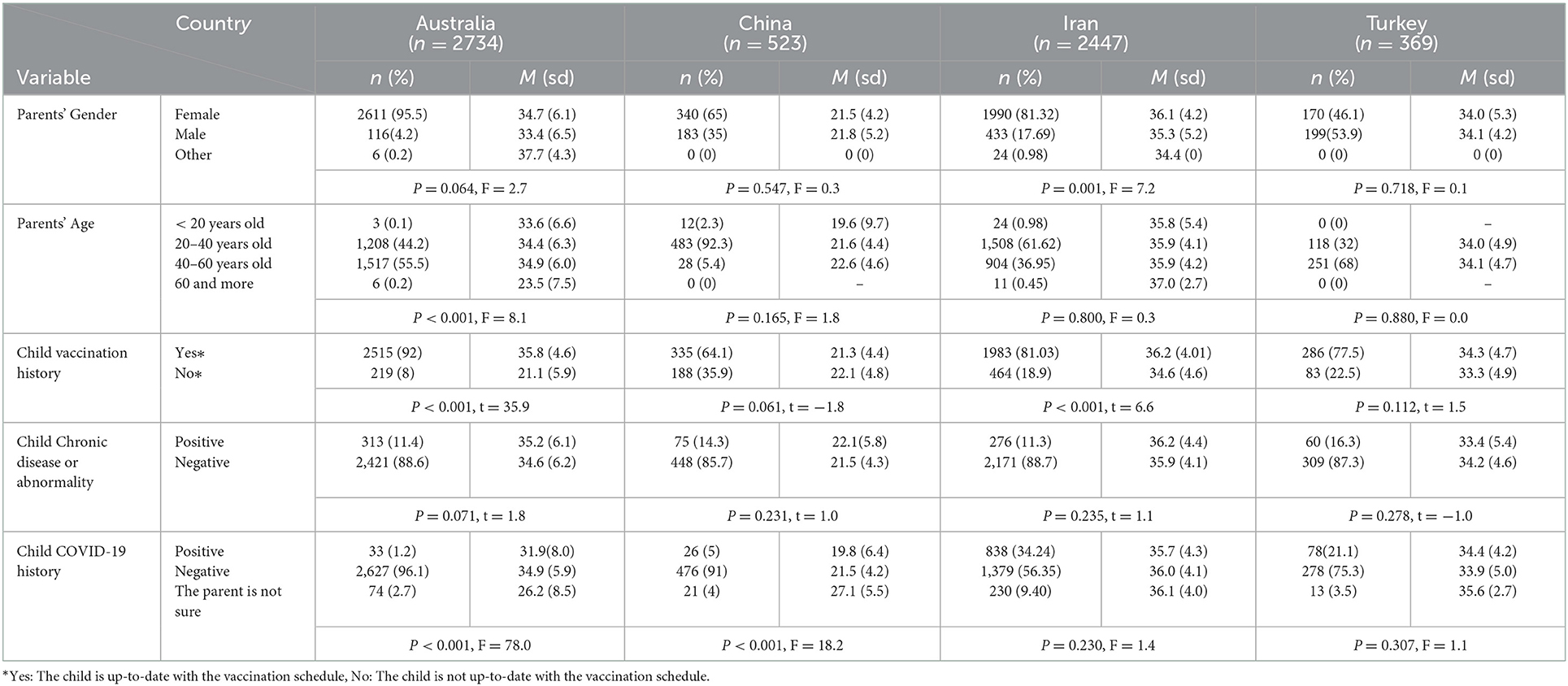
Table 1. Demographic characteristics of respondents and mean (SD) of COVID-19 vaccine hesitancy among parents.
Measurements
Sociodemographic characteristics
The respondents' sociodemographic variables which included age, gender, level of education, living area, child vaccination history, and child COVID-19 history were collected.
Translation procedures
The survey questionnaire contained sociodemographic information, Parent Attitudes about Child Vaccines (PACV), the Child Vulnerability Scale (CVS), Financial Well-being (FWB), and Parental Vaccine Hesitancy (PVH). Beaton et al.'s (101) instruction was used for translation and back-translation procedure. For countries where the first language was not English, all questionnaires were translated into the languages of the countries (Chinese, Persian, and Turkish). All translators were bilingual individuals. Two translators independently translated the questionnaires into the study setting language. The research team then assessed the translated versions and selected the best item translation. Following this step, two other bilingual translators who were “blinded” to the original version of the questionnaire conducted the back-translation procedure independently. The expert committee (consisting of research team members, two nurses, one physician in social medicine, and a methodologist) then checked the back-translated version to ensure the accuracy and equivalence between it and the original questionnaire version. Also, the committee assessed the cross-cultural equivalence and appropriateness of the questionnaire to the study population, as well as the semantic equivalence of the items. No item was changed during the procedure.
The parent attitude about child vaccines (PACV)
To investigate parental perceptions of vaccine safety, the sub-scale of safety and efficiency of the PACV questionnaire was used. The questionnaire consists of 15-item, 3-factor measures (two items on vaccine behavior, four items on beliefs about vaccine safety and efficiency, and nine items on general attitudes). A five-points Likert-scale questionnaire ranging from “strongly agree (5 scores)” to “strongly disagree (1 score)” was used to gather the data. Higher scores indicate more negative attitudes toward the vaccine (102).
The child vulnerability scale (CVS)
In order to investigate the parental perception of child vulnerability. The CVS is an 8-item self-report measure with 2 factors including “child medical condition” and “prior fears that child might die”. Participants were asked to rate their perception on their child's vulnerability using a five-points Likert-scale questionnaire ranging from “strongly agree (5 scores)” to “strongly disagree (1 score).” Higher scores indicated more perceived vulnerability (80).
Financial well-being (FWB)
Perceived financial well-being was measured by five items adapted from the CFPB's Financial Well-Being Scale (103). The CFPB's scale included the concepts of “financial situation” and “capability” and uses a 5-point Likert scale from “strongly agree (1 scores)” to “strongly disagree (5 score)”. Higher scores indicated more perceived financial well-being. A reverse scoring was used for item number 4 (I have money left over at the end of the month)”.
Parental vaccine hesitancy (PVH)
A 10-item, 2-factor measure consisting of “lack of confidence” and “risk” categories was used. The scale is measured on a five-point Likert-type rating scale ranging from “strongly disagree (1 score)” to “strongly agree (5 scores)”. Higher scores indicate more hesitancy (104).
Ethical consideration
The Ethics Committee of Mazandaran University of Medical Sciences, Iran approved the Ethical Considerations of this study (Reference No: IR.MAZUMS.REC.1400.189). In addition, all participants were informed of the purpose of the data collection, and questionnaires were distributed to the respondents only after they provided their consent to participate in the survey. Moreover, the respondents were ensured that their participation was on a voluntary basis and the confidentiality of all collected data was guaranteed.
Data analyses
A series of path analyses were used to explore the direct and indirect associations between parent attitudes about vaccines, child vulnerability, financial well-being, and parental vaccine hesitancy. Observed scale characteristics for all samples in the study were first examined. As recommended by Hair et al. (105), skewness and kurtosis scores were utilized to evaluate the assumption of normality for the study variables. Pearson correlation analysis was then performed to examine the relationships between the variables. In addition, the reliability of the measures was examined utilizing internal reliability (α) estimates. Finally, structural equation modeling was conducted to test the mediating role of parent attitudes about vaccines and child vulnerability in the link between financial well-being and parental vaccine hesitancy. Some model fit statistics, with their decision points, were examined to interoperate the results of path models: comparative fit index (CFI) and Tucker-Lewis index (TLI) scores ≥0.90 = an adequate data–model fit; and the root mean square error of approximation scores (RMSEA; with 90% confidence interval) ≤ 0.10 = an acceptable model fit (106). Before testing the mediation analyses, a series of measurement models were also carried out. Similar to structural modeling, data-model fit statistics were used to evaluate the results of this analysis. Additionally, multiple group analyses were performed to compare the direct and indirect associations between the variables of the study in the samples from different cultures. All study analyses were conducted utilizing SPSS v25 and AMOS v24.
Results
Observed scale characteristics results are presented in Table 2. Skewness and kurtosis scores were at an acceptable range suggesting that all measures in the study had relatively normal distribution. Further, correlation results were examined for each sample of the study, as seen in Table 3.
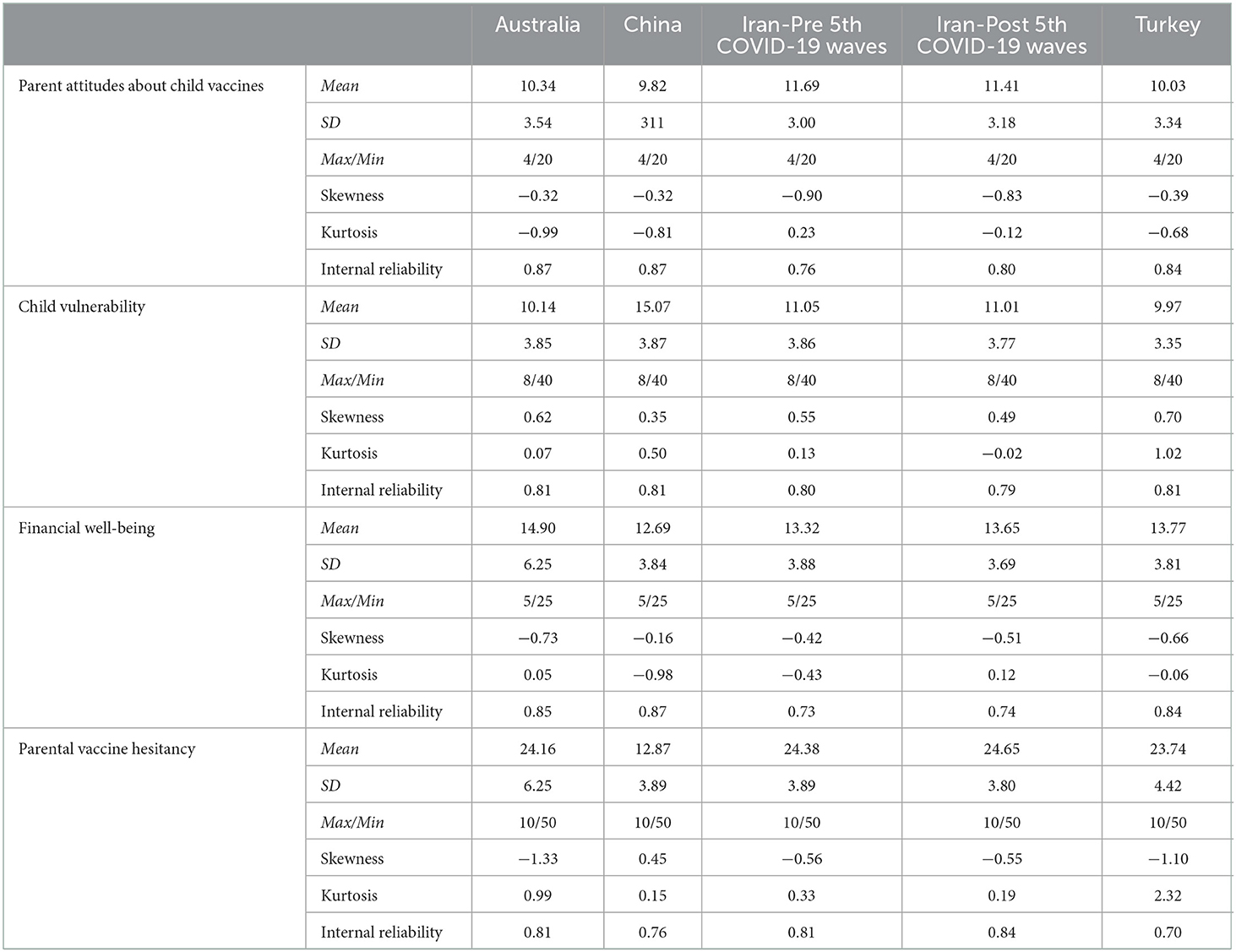
Table 2. Observed scale characteristics.
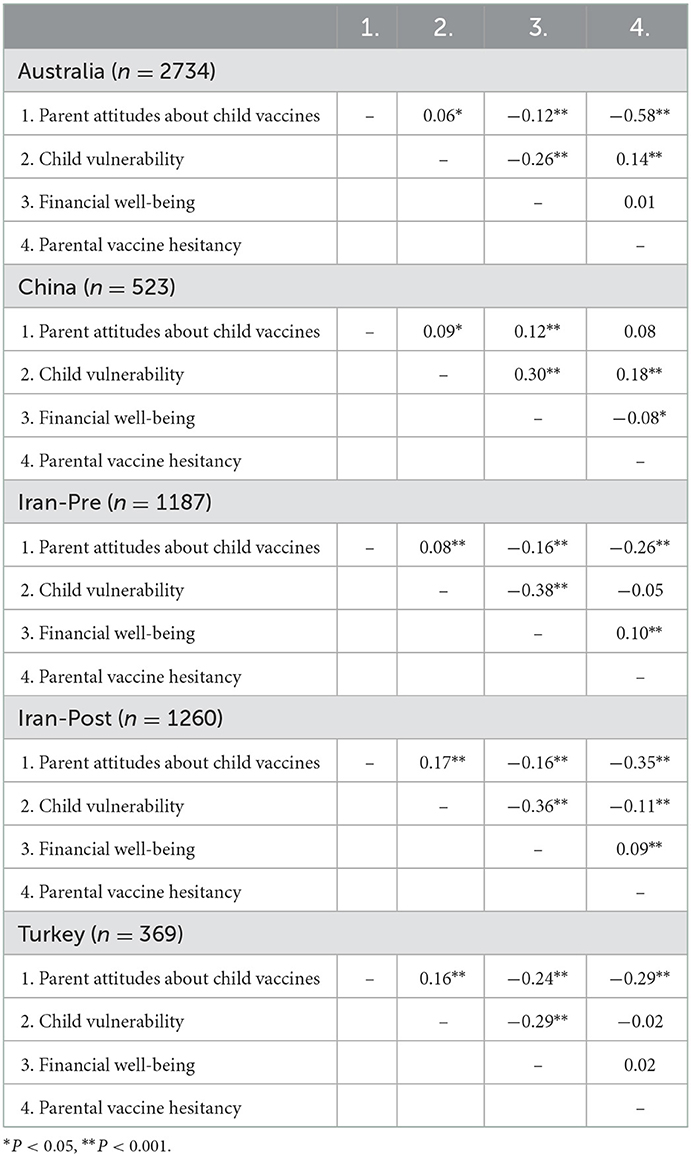
Table 3. Correlation results for the study variables.
The measurement models were then examined for the latent variables included in the mediation model using confirmatory factor analysis. The results indicated poor-to-adequate data-model fit statistics for each measure included in the study; therefore, modification indices, factor loadings (i.e., regression weights), and residual variances were examined in terms of countries to improve the measurement models. After excluding low loading items, which had regression weights <0.40 (107, 108), the measurement models were rerun. The modified measurement models provided better data-model fit statistics, as shown in Table 4.
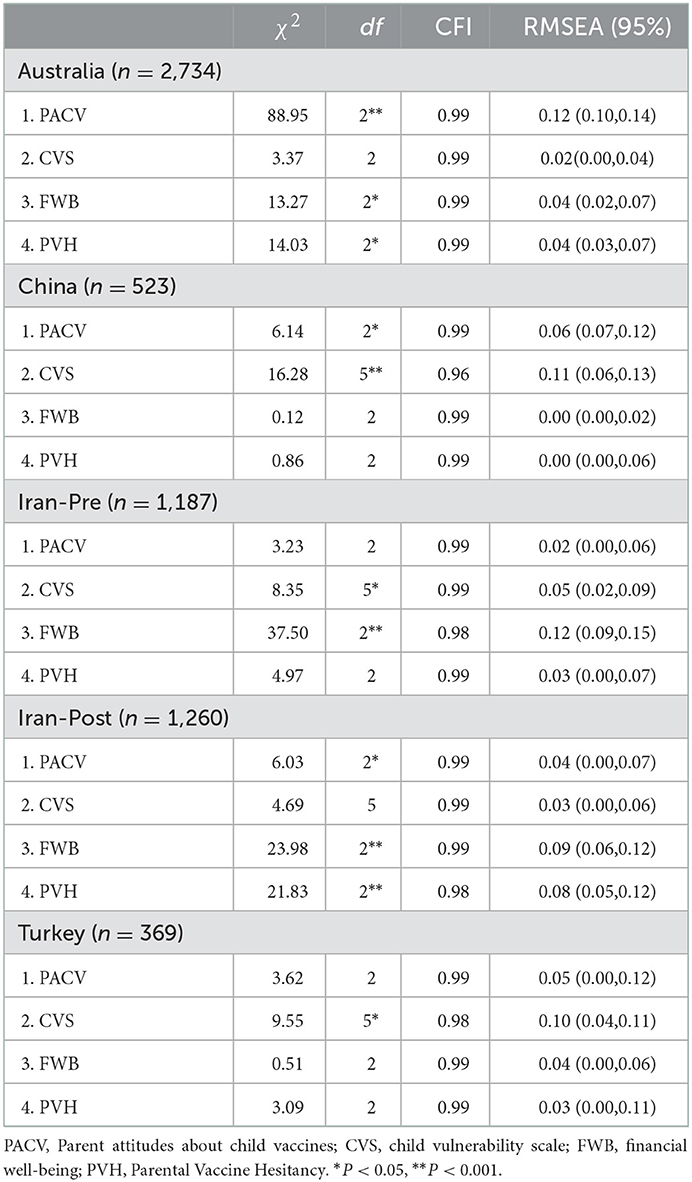
Table 4. Model fit statistics for the confirmatory factor analyses.
Measurement invariance were established across countries for the latent variables included in the model (109). Measurement invariance was utilized to examine configural, metric, and scalar invariance for countries using multiple-groups confirmatory factor analysis. Findings from these analyses were interpreted utilizing the ΔCFI and ΔRMSEA scores, with scores < 0.01 accepted as evidence of invariance across counties (110). Results from multi-group analyses indicated that measurement models, which were comprised of configural, metric, and scalar invariance, provided good-data model fit statistics across countries, as seen in Table 5. Given the change in the values of the CFI (ΔCFI < 0.01), although measurement invariance was observed at the configural invariance for all measures, it was not observed at the metric and scalar invariance levels for the PACV, FWB, and PVH. Measurement invariance of the CVS was also observed at the configural, metric, and scalar level.
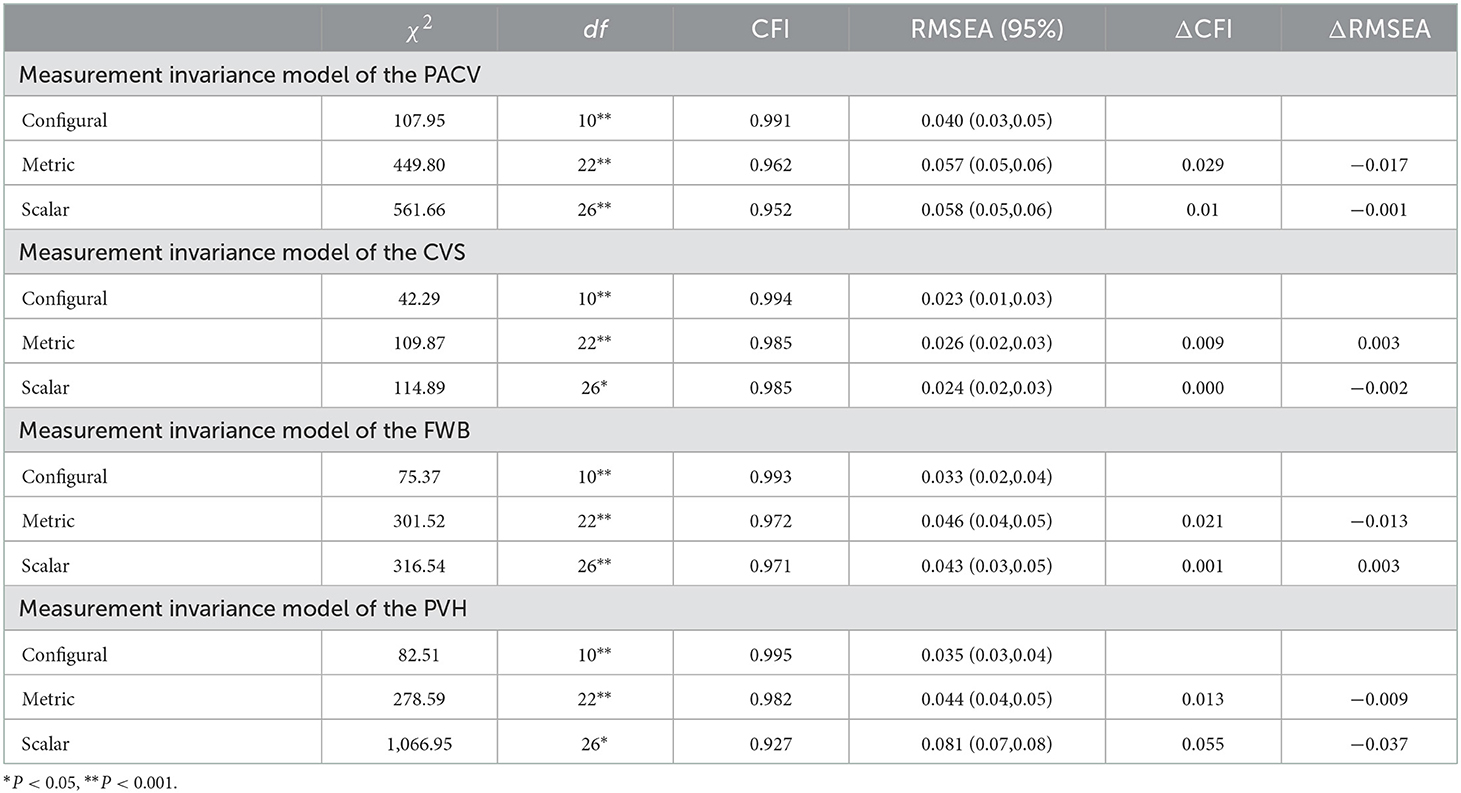
Table 5. Model fit statistics for the multi-group confirmatory factor analyses.
Finally, the mediating role of parent attitudes toward vaccines and child vulnerability in the link between financial wellbeing and parental vaccine hesitancy was tested. The results of the proposed model provided good-data model fit statistics (χ2= 14.52, df = 5, p = 0.01, CFI = 0.99, TLI = 0.98, RMSEA [95% CI] = 0.02 [0.01, 0.03]). In Australia, standardized regression estimates revealed that financial well-being had significant and negative associations with parent attitudes about vaccines and child vulnerability, but was not a significant predictor of parental vaccine hesitancy. Parental vaccine hesitancy was also predicted by parent attitudes about vaccines and child vulnerability. The indirect link of financial well-being with parental vaccine hesitancy through parent attitudes about vaccines and child vulnerability is significant, as shown in Table 6.
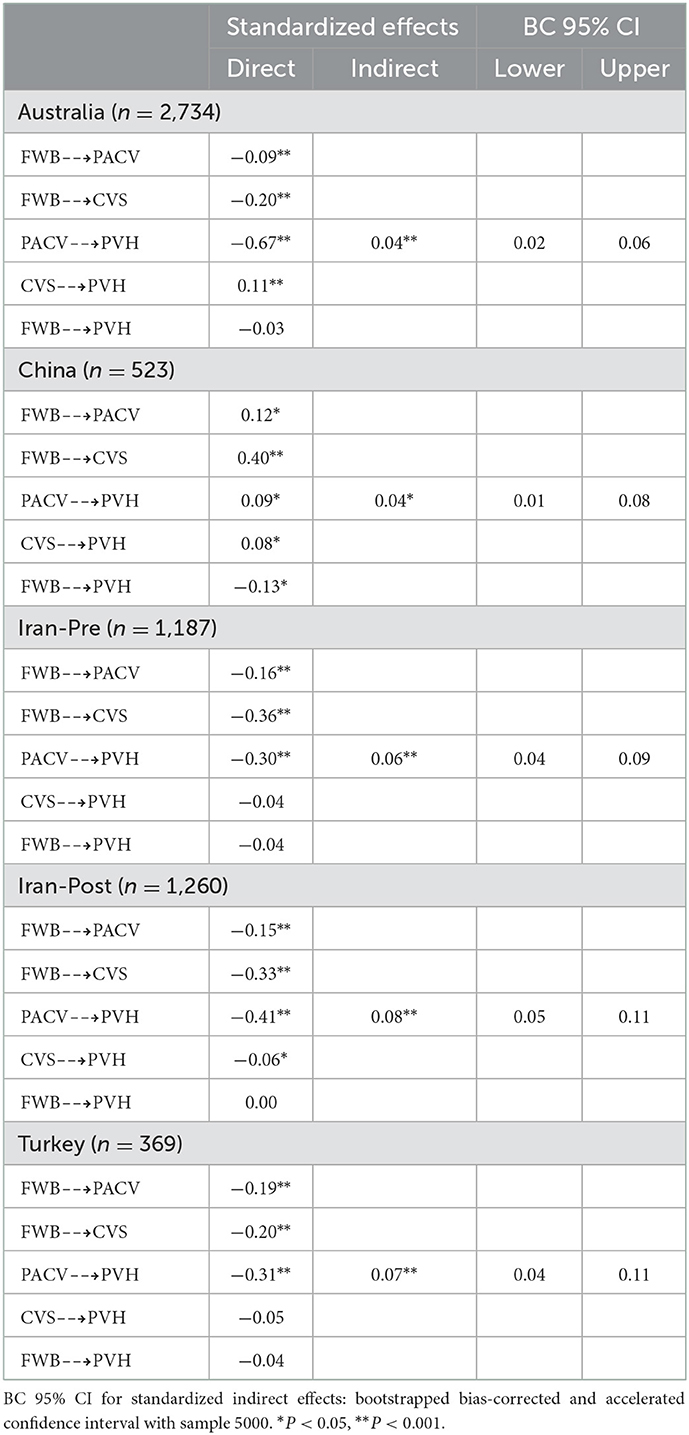
Table 6. Model paths indicating the direct and indirect associations between the variables of the study.
The results from Chinese participants indicated that financial well-being had significant and positive predictive effects on parent attitudes about vaccines, child vulnerability, and parental vaccine hesitancy. Additionally, parental vaccine hesitancy was predicted by parent attitudes about vaccines and child vulnerability, and these variables mediated the association between financial well-being and parental vaccine hesitancy. The model was then examined with Iranian participants. In the first sample, the model showed that financial well-being had significant and negative associations with parent attitudes about vaccines and child vulnerability, but was not a significant predictor of parental vaccine hesitancy. Although parental vaccine hesitancy was significantly predicted by parent attitudes about vaccines, it did not predict child vulnerability. The indirect link of financial well-being with parental vaccine hesitancy through parent attitudes about vaccines is significant.
The results of the second Iranian sample revealed that financial well-being had significant and negative associations with parent attitudes about vaccines and child vulnerability, but was not a significant predictor of parental vaccine hesitancy. Parent attitudes about vaccines and child vulnerability also significantly and negatively predicted parental vaccine hesitancy. Financial well-being had a significant association with parental vaccine hesitancy through parent attitudes about vaccines and child vulnerability.
Turkish parents' financial well-being had significant and negative relationships with parent attitudes about vaccines and child vulnerability; however, it did not significantly predict parental vaccine hesitancy. Parental vaccine hesitancy, on the other hand, then was significantly predicted by parent attitudes about vaccines. The indirect link of financial well-being with parental vaccine hesitancy through parent attitudes about vaccines is significant, as seen in Table 6.
Discussion
In the present study, we aimed to investigate the mediating role of parent attitudes toward COVID-19 vaccines and child vulnerability in the link between perceived financial well-being and parental vaccine hesitancy.
The current study indicated the mediating role of parent attitudes toward vaccines and child vulnerability in the link between financial well-being and parental vaccine hesitancy as a model in four countries including Australia, China, Iran, and Turkey. The COVID-19 vaccine hesitancy among parents is a worldwide health concern that has been investigated in different countries (17, 83). A wide range of factors that influence parents' vaccine hesitancy have been identified including ethnicity, family income, type of insurance, social media use (83), and uncertainty about vaccines (17, 111). It has been suggested that vaccine safety and effectiveness are two main concerns regarding the COVID-19 vaccine (26, 112). The current study support the findings from previous research. Studies have indicated that an individual's financial comfort can be considered as a predictor factor of vaccine hesitancy (113). Furthermore, attitudes toward vaccine safety and effectiveness predict the willingness of parents to get their children vaccinated against COVID-19 (114). The current study indicated the mediating role of parents' perception of their child's vulnerability in the relationship between financial well-being and vaccine hesitancy. This means that the degree to which the parents perceive their child as vulnerable to infection by COVID-19 can predict their willingness to get their children vaccinated regardless of their financial status. The theory of protection motivation (PMT) can help to explain the current findings. Accordingly, individual fear appraisal can make attitudes change (91). When individuals perceive the susceptibility and the severity of a situation, their knowledge, attitude, and performance may change (115, 116).
The current study revealed that financial well-being had significant and negative associations with parents' attitudes toward the COVID-19 vaccine and child vulnerability among the Australian participants. Generally, Australia has a high vaccine uptake in comparison with other high-income countries such as the US and Canada (117). However, some studies have indicated public concerns over the safety of existing COVID-19 vaccines (118, 119) that can raise parents' concerns regarding the safety and effectiveness of the vaccine for their children. Studies have determined several factors affecting parents' decision on childhood vaccination in Australia that include concerns such as potential side effects and vaccine safety (120). The current findings related to perceived financial well-being and parental vaccine hesitancy in Australia can be explained through past research. For instance, Swaney and Burns (86) found that Australian parents with self-reported higher-socioeconomic status were more likely to be vaccine-hesitant because they perceived themselves as educated and not wanting to control their children's health decisions. Also, they believed their families were safe from disease and vaccines posed a greater risk. Furthermore, they reported a belief that their lifestyle factors can protect them from vaccine-preventable diseases (86).
This study also revealed that parental vaccine hesitancy was predicted by Australian parents' attitudes toward the COVID-19 vaccine and perception of their child's level of vulnerability. One study (121) indicated that although parents expressed a strong desire for protecting their children, almost half of parents did not intend to vaccinate their children because they had concerns about the vaccine's long-term effects on child health and development.
Contrary to the Australian findings, the results of the Chinese participants indicated that perceived financial well-being had significant and positive predictive effects on parent attitudes toward vaccines, child vulnerability, and parental vaccine hesitancy. The findings of a population-based study (n = 2,463) indicated that more than 50% of Chinese parents were hesitant about the COVID-19 vaccine. While mothers were more hesitant, factors like the child's age (under 18 years old), knowledge deficit regarding the COVID-19 vaccinations, and lower awareness of the permission of vaccinating children were the determinants of parental vaccine hesitancy (77). The findings of Lu et al. (26) indicated that out of 3,673 parents more than 87.5% accepted the COVID-19 vaccine for their children. They believed that new vaccines, such as the COVID-19 vaccine, carry more risks than older vaccines. They also found that the parents' income was significantly related to vaccine hesitancy among Chinese parents. Parents with less than average income had lower hesitancy. This finding is supported by the result of the current study which showed that families with higher well-being perception have negative attitude toward the COVID-19 vaccine. The current study also revealed that financial well-being can predict Chinese parents' perceptions of their children's vulnerability. In general, children were considered as a vulnerable group and (122) living in a low-income family makes a child more vulnerable during the COVID-19 pandemic. The findings of a large survey (n = 20,632) conducted in China indicated that individuals with higher socioeconomic status worried less about COVID-19 as they had better education, higher income, and more resources in coping with COVID-19 (123) and therefore, may experience less stress. Published studies have addressed parental stress during the COVID-19 pandemic due to sociodemographic factors (124), their mental health (125), the children's distance education (126), the child's health status (127), and a variety of different factors. Contrary to this, the current study showed that Chinese parents who had the highest level of socioeconomic status perceived their children as more vulnerable to COVID-19.
Data from the Iranian participants revealed that parent' attitudes toward vaccines and child vulnerability significantly and negatively predicted parental vaccine hesitancy. Also, the study indicated that financial well-being had a significant association with parental vaccine hesitancy through parent attitudes about vaccines and child vulnerability. Some studies have investigated Iranian population's COVID-19 vaccination intent and have reported the importance of the role of trust in the healthcare systems (28), believing in COVID-19 vaccine effectiveness, low concern about vaccine safety, greater exposure to cues to vaccinate (128), as well as attitudes and subjective norms about the importance of COVID-19 vaccination, and using social media (129). Furthermore, Iranian intent to get COVID-19 vaccinated has been predicted by their attitudes, perceived COVID-19 infectability, and perceived behavioral control (130). Studies addressed that Iranian parents experienced fear during the COVID-19 outbreak and perceived their children as susceptible to infection (131). The children's vulnerability during the COVID-19 pandemic and following protective behavior was highlighted if the child had a chronic disease (132) or when individuals experienced economic issues (133). Iran has experienced more than five COVID-19 waves to date, and for children under 18 years old, vaccinations have only recently begun in Iran.
The current study revealed that financial well-being had significant and negative relationships with parent attitudes about vaccines and child vulnerability. However, it did not significantly predict parental vaccine hesitancy among Turkish parents. Parental vaccine hesitancy was significantly predictive of parents' attitudes about vaccines, but it did not predict the child's vulnerability. The findings of Ikiisik et al. (99) indicated that almost 90% of parents were hesitant about vaccinating their children with the COVID-19 vaccines. Age and risk perception were the identified factors that influence vaccine hesitancy. Another study indicated that only 36.3% of Turkish parents were willing to have their children receive the COVID-19 vaccine. Advising others to receive the vaccine was a significant predictor of parents' willingness to get the COVID-19 vaccine for their children (78). The correlation between attitude toward the COVID-19 vaccine and vaccine acceptance has been identified among the Turkish population (114). Kilic et al. (134) indicated that increasing fear of the COVID-19 contagion, having relatives infected with COVID-19, increasing perceived health status and life satisfaction, older age, being a male and not being a worker-tradesman increase the probability of having a positive attitude toward COVID-19 vaccine. Another study found that anxiety about the vaccine side effects, uncertainty of the vaccine effectiveness, and distrust of vaccines originating from abroad influence parental COVID-19 vaccine hesitancy (111).
Parental vaccine hesitancy, may also be predicted by the vaccine type and origin (75, 135). Parents may prefer conventional vaccines over mRNA vaccines due to lack of confidence in the mRNA technology and fear of its unknown side effects. Another concern among parents is the possible existence of microchips in some COVID-19 vaccines (135). Some studies showed that the general population trust COVID-19 vaccines manufactured by their government (75) while others may trust vaccines produced by the international, well-known, and specialized drug and vaccine companies. In general, vaccine acceptance is dynamic and time-dependent, and it can be influenced by different potential factors such as vaccine effectiveness, trust, vaccine safety, information, vaccine mandate, and fear (136).
Study limitations
One of the limitations of this study is the use of online data gathering wherein only parents with access to a smartphone or other digital device were not included in the study. Hence, the findings of the current study may not be generalized. Furthermore, the Iranian data were gathered before and during the 5th pandemic wave and now Iran is in its 6th COVID-19 pandemic wave, therefore some findings may not be current. Additionally, the data were gathered between 8 August 2021 and 1 October 2021 and considering the nature of the COVID-19 pandemic and the occurrence of subsequent waves of the disease, the current study variables may have been affected. The COVID-19 vaccine has now been used for a large number of children, hence the phenomenon of parental COVID-19 vaccine hesitancy may have also changed. It is therefore recommended that more studies be conducted to investigate the validity of the proposed model.
Conclusion
Children around the world are considered as a vulnerable group as their health is dependent on parents' or guardians' decisions. With the existence of the COVID-19 virus, vaccination of children is one of the best ways to protect them from the virus and prevent further spread of the disease. Despite the fact that COVID-19 vaccines are considered safe, vaccine hesitancy is common among parents. Vaccine hesitancy in the COVID-19 era is imbued in social, cultural, and historical contexts (137). The current study revealed that parental COVID-19 vaccine hesitancy could be predicted by parental perceptions of their child's vulnerability and their attitudes toward vaccines. Additionally, this study addressed the relationship between financial well-being and vaccine hesitancy, and suggests that consideration should be given to the type of vaccine messaging directed toward parents of varying economic groups regardless of what country they are located. Assessing the parents' vaccine hesitancy is recommended in public education campaigns to promote COVID-19 vaccination for children. Although the hospitalization and mortality rate of children due to COVID-19 infection has not been reported highly in various studies, COVID-19 infection among unvaccinated children can lead to more serious health consequences. In addition, contracting COVID-19 can deprive children of attending school and subsequently cause parents to be absent from work. On a macro scale, this would have adverse impact on the macro-economy.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was reviewed and approved by the Ethics Committee of Mazandaran University of Medical Sciences, Iran. Reference No: IR.MAZUMS.REC.1400.189. The participants provided their written informed consent to participate in this study.
Author contributions
Study conception and design: HS and FK. Data collection: FK, HS, K-AA, LS, and OG. Analysis and interpretation of results: GA and HS. Draft manuscript preparation: FK, HK, K-AA, and ES. All authors reviewed the results and approved the final version of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Poon LL. A Push for Real Normal: Mass Screening for COVID-19. Oxford, UK: Oxford University Press (2022). p. 4–6.
2. Allen H, Vusirikala A, Flannagan J, Twohig KA, Zaidi A, Chudasama D, et al. Household transmission of COVID-19 cases associated with SARS-CoV-2 delta variant (B. 1617 2): national case-control study. Lancet Reg Health Eur (2022) 12:100252. doi: 10.1016/j.lanepe.2021.100252
3. Kadri S, Mattoo S, Brady AH, Petkovic M. Innovative Solutions to the Clinical Challenges of COVID-19. Healthcare Informatics for Fighting COVID-19 and Future Epidemics. Berlin, Germany: Springer (2022). p. 337–51.
4. Devi SJL. COVID-19 resurgence in Iran. Lancet. (2020) 395:1896. doi: 10.1016/S0140-6736(20)31407-0
5. Shimizu K, Wharton G, Sakamoto H, Mossialos EJb. Resurgence of COVID-19 in Japan. UK: British Medical Journal Publishing Group (2020).
6. Eng G. Modeling the USA Winter 2021 Resurgence. medRxiv. (2022). doi: 10.1101/2022.01.06.22268868
7. He D, Fan G, Wang X, Li Y, Peng ZJm. The new SARS-CoV-2 variant and reinfection in the resurgence of COVID-19 outbreaks in Manaus, Brazil. MedRxiv. (2021). doi: 10.1101/2021.03.25.21254281
8. Depar U. How Do I Find a COVID-19 Vaccine or Booster? (2021) Available online at: www.cdcgov/coronavirus/vaccines (accessed on September 15, 2022).
9. Wiysonge CS, Alobwede SM, de Marie C Katoto P, Kidzeru EB, Lumngwena EN, Cooper S, et al. COVID-19 vaccine acceptance and hesitancy among healthcare workers in South Africa. Expert Rev Vaccines. (2022) 2022:1–11. doi: 10.12688/f1000research.123332.1
10. Ndwandwe D. Wiysonge CS. COVID-19 vaccines. Curr Opin Immunol. (2021) 71:111–6. doi: 10.1016/j.coi.2021.07.003
11. Liu Q, Qin C, Liu M. Liu J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: a systematic review and meta-analysis. Infect Dis Poverty. (2021) 10:1–15. doi: 10.1186/s40249-021-00915-3
12. Kaplan RM, Milstein A. Influence of a COVID-19 vaccine's effectiveness and safety profile on vaccination acceptance. Proc Natl Acad Sci U S A. (2021) 118:e2021726118. doi: 10.1073/pnas.2021726118
13. Wagner AL, Sheinfeld Gorin S, Boulton ML, Glover BA, Morenoff JD. Immunotherapeutics Effect of vaccine effectiveness and safety on COVID-19 vaccine acceptance in Detroit, Michigan. Hum Vaccin Immunother. (2020) 2021:1–6. doi: 10.1080/21645515.2021.1917233
14. Yasmin F, Najeeb H, Moeed A, Naeem U, Asghar MS, Chughtai NU, et al. COVID-19 vaccine hesitancy in the United States: a systematic review. Front Public Health. (2021) 9:770985. doi: 10.3389/fpubh.2021.770985
15. Kukreti S, Lu M-Y, Lin Y-H, Strong C, Lin C-Y, Ko N-Y, et al. Willingness of Taiwan's healthcare workers and outpatients to vaccinate against COVID-19 during a period without community outbreaks. Vaccines (Basel). (2021) 9:246. doi: 10.3390/vaccines9030246
16. Musa S, Dergaa I, Abdulmalik MA, Ammar A, Chamari K, Saad HB. BNT162b2 COVID-19 Vaccine hesitancy among parents of 4023 young adolescents (12–15 Years) in Qatar. Vaccines (Basel). (2021) 9:981. doi: 10.3390/vaccines9090981
17. Bagateli LE, Saeki EY, Fadda M, Agostoni C, Marchisio P. Milani GPJV. COVID-19 vaccine hesitancy among parents of children and adolescents living in Brazil. Vaccines (Basel). (2021) 9:1115. doi: 10.3390/vaccines9101115
18. Lucia VC, Kelekar A., Afonso NM. COVID-19 vaccine hesitancy among medical students. J Public Health (Oxf). (2021) 43:445–9. doi: 10.1093/pubmed/fdaa230
19. Riad A, Pokorná A, Antalová N, Krobot M, Zviadadze N, Serdiuk I, et al. Prevalence and drivers of COVID-19 vaccine hesitancy among Czech University students: national cross-sectional study. Vaccines (Basel). (2021) 9:948. doi: 10.3390/vaccines9090948
20. Ogbuabor DC. Chime AC. Prevalence and predictors of vaccine hesitancy among expectant mothers in Enugu metropolis, South-east Nigeria. J Public Health Policy. (2021) 42:222–35. doi: 10.1057/s41271-020-00273-8
21. Saluja S, Lam CN, Wishart D, McMorris A, Cousineau MR. Kaplan CM. Disparities in COVID-19 vaccine hesitancy among Los Angeles County adults after vaccine authorization. Prev Med Rep. (2021) 24:101544. doi: 10.1016/j.pmedr.2021.101544
22. Qunaibi EA, Helmy M, Basheti I, Sultan IJm. A high rate of COVID-19 vaccine hesitancy among arabs: results of a large-scale survey. Elife. (2021) 10:e68038. doi: 10.1101/2021.03.09.21252764
23. Almaghaslah D, Alsayari A, Kandasamy G, Vasudevan R. COVID-19 vaccine hesitancy among young adults in Saudi Arabia: a cross-sectional web-based study. Vaccines (Basel). (2021) 9:330. doi: 10.3390/vaccines9040330
24. MacDonald NE. Vaccine hesitancy: Definition, scope and determinants. Vaccines (Basel). (2015) 33:4161–4. doi: 10.1016/j.vaccine.2015.04.036
25. Alqudeimat Y, Alenezi D, AlHajri B, Alfouzan H, Almokhaizeem Z, Altamimi S, et al. Acceptance of a COVID-19 vaccine and its related determinants among the general adult population in Kuwait. Med Princ Pract. (2021) 30:262–71. doi: 10.1159/000514636
26. Lu J, Wen X, Guo Q, Ji M, Zhang F, Wagner AL, et al. Sensitivity to COVID-19 Vaccine Effectiveness and Safety in Shanghai, China. Vaccines (Basel). (2021) 9:472. doi: 10.3390/vaccines9050472
27. Paris C, Bénézit F, Geslin M, Polard E, Baldeyrou M, Turmel V, et al. COVID-19 vaccine hesitancy among healthcare workers. Infect Dis Now. (2021) 51:484–7. doi: 10.1016/j.idnow.2021.04.001
28. Ahorsu DK, Lin C-Y, Yahaghai R, Alimoradi Z, Broström A, Griffiths MD, et al. The mediational role of trust in the healthcare system in the association between generalized trust and willingness to get COVID-19 vaccination in Iran. Hum Vaccin Immunother. (2021) 18:1–8. doi: 10.1080/21645515.2021.1993689
29. Warren RC, Forrow L, Hodge Sr DA, Truog RD. Trustworthiness before trust—COVID-19 vaccine trials and the Black community. N Engl J Med. (2020) 383:e121. doi: 10.1056/NEJMp2030033
30. Willis DE, Andersen JA, Bryant-Moore K, Selig JP, Long CR, Felix HC, et al. COVID-19 vaccine hesitancy: Race/ethnicity, trust, and fear. (2021) 14:2200–7. doi: 10.1111/cts.13077
31. Quinn SC, Jamison A. Freimuth VJ. Measles outbreaks and public attitudes towards vaccine exemptions: some cautions and strategies for addressing vaccine hesitancy. Hum Vaccin Immunother. (2020) 16:1050–4. doi: 10.1080/21645515.2019.1646578
32. De Figueiredo A, Simas C, Karafillakis E, Paterson P, Larson HJ. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: a large-scale retrospective temporal modelling study. Lancet. (2020) 396:898–908. doi: 10.1016/S0140-6736(20)31558-0
33. Cornwall W. Officials gird for a war on vaccine misinformation. Science. (2020) 369:14–5. doi: 10.1126/science.369.6499.14
34. Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. (2021) 27:225–8. doi: 10.1038/s41591-020-1124-9
35. Rhodes ME, Sundstrom B, Ritter E, McKeever BW, McKeever RJ. Preparing for A COVID-19 vaccine: A mixed methods study of vaccine hesitant parents. J Health Commun. (2020) 25:831–7. doi: 10.1080/10810730.2021.1871986
36. Wilson SL, Wiysonge CJ. Social media and vaccine hesitancy. BMJ Glob Health. (2020) 5:e004206. doi: 10.1136/bmjgh-2020-004206
37. Reuben R, Aitken D, Freedman JL, Einstein G. Mistrust of the medical profession and higher disgust sensitivity predict parental vaccine hesitancy. PLoS ONE. (2020) 15:e0237755. doi: 10.1371/journal.pone.0237755
38. Wong LP, Alias H, Wong P-F, Lee HY, AbuBakar SJ. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum Vaccin Immunothe. (2020) 16:2204–14. doi: 10.1080/21645515.2020.1790279
39. Prickett K, Habibi H, Carr PA. COVID-19 vaccine hesitancy and acceptance in a cohort of diverse New Zealanders. Lancet Reg Health West Pac. (2021) 14:100241. doi: 10.26686/wgtn.14658885
40. Soares P, Rocha JV, Moniz M, Gama A, Laires PA, Pedro AR, et al. Factors associated with COVID-19 vaccine hesitancy. Vaccines (Basel). (2021) 9:300. doi: 10.3390/vaccines9030300
41. Nomura S, Eguchi A, Yoneoka D, Kawashima T, Tanoue Y, Murakami M, et al. Reasons for being unsure or unwilling regarding intention to take COVID-19 vaccine among Japanese people: A large cross-sectional national survey. Lancet Reg Health West Pac. (2021) 14:100223. doi: 10.1016/j.lanwpc.2021.100223
42. Khubchandani J, Sharma S, Price JH, Wiblishauser MJ, Sharma M, Webb FJ. COVID-19 vaccination hesitancy in the United States: a rapid national assessment. J Community Health. (2021) 46:270–7. doi: 10.1007/s10900-020-00958-x
43. Lim VW, Lim RL, Tan YR, Soh AS, Tan MX, Othman NB, et al. Government trust, perceptions of COVID-19 and behaviour change: cohort surveys, Singapore. Bull World Health Organ. (2021) 99:92. doi: 10.2471/BLT.20.269142
44. Sallam M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines. (2021) 9:160. doi: 10.3390/vaccines9020160
45. Ghinai I, Willott C, Dadari I, Larson HJ. Listening to the rumours: what the northern Nigeria polio vaccine boycott can tell us ten years on. Glob Public Health. (2013) 8:1138–50. doi: 10.1080/17441692.2013.859720
46. Hviid A, Hansen JV, Frisch M, Melbye MJ. Measles, mumps, rubella vaccination and autism: a nationwide cohort study Ann Intern Med. (2019) 170:513–20. doi: 10.7326/M18-2101
47. Phadke VK, Bednarczyk RA, Salmon DA, Omer SB. Association between vaccine refusal and vaccine-preventable diseases in the United States: a review of measles and pertussis. JAMA. (2016) 315:1149–58. doi: 10.1001/jama.2016.1353
48. Kempe A, Saville AW, Albertin C, Zimet G, Breck A, Helmkamp L, et al. Parental hesitancy about routine childhood and influenza vaccinations: a national survey. Pediatrics. (2020) 146:e20193852. doi: 10.1542/peds.2019-3852
49. Wang Q, Xiu S, Zhao S, Wang J, Han Y, Dong S, et al. Vaccine Hesitancy: COVID-19 and Influenza Vaccine Willingness among Parents in Wuxi, China—A Cross-Sectional Study. Vaccines. (2021) 9:342. doi: 10.3390/vaccines9040342
50. Dubé E, Laberge C, Guay M, Bramadat P, Roy R, Bettinger JA, et al. Vaccine hesitancy: an overview. Vaccines. (2013) 9:1763–73. doi: 10.4161/hv.24657
51. Larson HJ, Jarrett C, Eckersberger E, Smith DM, Paterson PJV. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007–2012. Vaccines. (2014) 32:2150–9. doi: 10.1016/j.vaccine.2014.01.081
52. Blaisdell LL, Gutheil C, Hootsmans NA. Han PKJM. Unknown risks: parental hesitation about vaccination. Med Decis Making. (2016) 36:479–89. doi: 10.1177/0272989X15607855
53. Burghouts J, Del Nogal B, Uriepero A, Hermans PW, de Waard JH, Verhagen LM. Childhood vaccine acceptance and refusal among Warao Amerindian Caregivers in Venezuela; A qualitative approach. PLoS ONE. (2017) 12:e0170227. doi: 10.1371/journal.pone.0170227
54. Nguyen KH, Santibanez TA, Stokley S, Lindley MC, Fisher A, Kim D, et al. Parental vaccine hesitancy and its association with adolescent HPV vaccination. Vaccines. (2021) 39:2416. doi: 10.1016/j.vaccine.2021.03.048
55. Geoghegan S, O'Callaghan KP, Offit PAJFim. Vaccine safety: myths and misinformation. Front Microbiol. (2020) 11:372. doi: 10.3389/fmicb.2020.00372
56. Paterson P, Chantler T, Larson HJ. Reasons for non-vaccination: Parental vaccine hesitancy and the childhood influenza vaccination school pilot programme in England. (2018) 36:5397–401. doi: 10.1016/j.vaccine.2017.08.016
57. Gabis LV, Attia OL, Goldman M, Barak N, Tefera P, Shefer S, et al. The myth of vaccination and autism spectrum. Eur J Paediatr Neurol. (2021) 36:151–8. doi: 10.1016/j.ejpn.2021.12.011
58. Tang L, Douglas S, Laila AJ. Among sheeples and antivaxxers: Social media responses to COVID-19 vaccine news posted by Canadian news organizations, and recommendations to counter vaccine hesitancy. Can Commun Dis Rep. (2021) 47:524–33. doi: 10.14745/ccdr.v47i12a03
59. Hudson A. Montelpare WJJIJoER, Health P. Predictors of vaccine hesitancy: Implications for COVID-19 public health messaging. Int J Environ Res Public Health. (2021) 18:8054. doi: 10.3390/ijerph18158054
60. Afolabi AA, Ilesanmi OS. Dealing with vaccine hesitancy in Africa: the prospective COVID-19 vaccine context Pan Afr Med J. (2021) 38:3. doi: 10.11604/pamj.2021.38.3.27401
61. Bauer A, Tiefengraber D, Wiedermann U. Towards understanding vaccine hesitancy and vaccination refusal in Austria. Wien Klin Wochenschr. (2021) 133:703–13. doi: 10.1007/s00508-020-01777-9
62. Olusanya OA, Bednarczyk RA, Davis RL, Shaban-Nejad A. Addressing Parental Vaccine Hesitancy and Other Barriers to Childhood/Adolescent Vaccination Uptake During the Coronavirus (COVID-19) Pandemic. Front Immunol. (2021) 12:855. doi: 10.3389/fimmu.2021.663074
63. Dubé E, Vivion M, Sauvageau C, Gagneur A, Gagnon R, Guay MJ. “Nature does things well, why should we interfere?” Vaccine hesitancy among mothers. Qual Health Res. (2016) 26:411–25. doi: 10.1177/1049732315573207
64. Attwell K, Leask J, Meyer SB, Rokkas P. Ward PJJoBI. Vaccine rejecting parents' engagement with expert systems that inform vaccination programs. J Bioeth Inq. (2017) 14:65–76. doi: 10.1007/s11673-016-9756-7
65. Colón-López V, Medina-Laabes DT, Abreu RS, Díaz Miranda OL, Ortiz AP, Fernández ME, et al. Understanding parents' views toward the newly enacted HPV vaccine school entry policy in Puerto Rico: a qualitative study. BMC Public Health. (2021) 21:1–9. doi: 10.1186/s12889-021-11952-w
66. Sun R, Wang X, Lin L, Zhang N, Li L, Zhou XJ, et al. The impact of negative emotional reactions on parental vaccine hesitancy after the vaccine event in China: A cross-sectional survey. Hum Vaccin Immunother. (2018) 2021:1–10. doi: 10.1080/21645515.2021.1907149
67. Volkman JE, Hokeness KL, Morse CR, Viens A, Dickie AJ. Information source's influence on vaccine perceptions: an exploration into perceptions of knowledge, risk and safety. J Commun Healthcare. (2021) 14:50–60. doi: 10.1080/17538068.2020.1793288
68. Napolitano F, D'Alessandro A. Angelillo IF. Investigating Italian parents' vaccine hesitancy: A cross-sectional survey. Human Vaccines Immunother. (2018) 14:1558–65. doi: 10.1080/21645515.2018.1463943
69. Wang J, Zhang Y, Long S, Fu X, Zhang X, Zhao S, et al. Non-epi vaccine hesitancy among chinese adults: A cross-sectional study. Vaccines. (2021) 9:772. doi: 10.3390/vaccines9070772
70. Forster AS, Rockliffe L, Chorley AJ, Marlow LA, Bedford H, Smith SG, et al. A qualitative systematic review of factors influencing parents' vaccination decision-making in the United Kingdom. SSM Popul Health. (2016) 2:603–12. doi: 10.1016/j.ssmph.2016.07.005
71. Domek GJ, O'Leary ST, Bull S, Bronsert M, Contreras-Roldan IL, Bolaños Ventura GA, et al. Measuring vaccine hesitancy: Field testing the WHO SAGE Working Group on Vaccine Hesitancy survey tool in Guatemala. Vaccine. (2018) 36:5273–81. doi: 10.1016/j.vaccine.2018.07.046
72. Cataldi JR, O'Leary ST. Parental vaccine hesitancy: scope, causes, and potential responses. Curr Opin Infect Dis. (2021) 34:519–26. doi: 10.1097/QCO.0000000000000774
73. Benin AL, Wisler-Scher DJ, Colson E, Shapiro ED, Holmboe ES. Qualitative Analysis of Mothers' Decision-Making About Vaccines for Infants: The Importance of Trust. Pediatrics. (2006) 117:1532–41. doi: 10.1542/peds.2005-1728
74. Horiuchi S, Sakamoto H, Abe SK, Shinohara R, Kushima M, Otawa S, et al. Factors of parental COVID-19 vaccine hesitancy: a cross sectional study in Japan. PLoS ONE. (2021) 16:e0261121. doi: 10.1371/journal.pone.0261121
75. Troiano G, Nardi A. Vaccine hesitancy in the era of COVID-19. Public Health. (2021) 194:245–51. doi: 10.1016/j.puhe.2021.02.025
76. Zheng M, Zhong W, Chen X, Wang N, Liu Y, Zhang Q, et al. Factors influencing parents' willingness to vaccinate their preschool children against COVID-19: Results from the mixed-method study in China. Human Vaccines Immunother. (2022) 18:2090776. doi: 10.1080/21645515.2022.2090776
77. Zhang M-X, Lin X-Q, Chen Y, Tung T-H, Zhu J-S. Determinants of parental hesitancy to vaccinate their children against COVID-19 in China. Expert Rev Vaccines. (2021) 20:1339–49. doi: 10.1080/14760584.2021.1967147
78. Yilmaz M, Sahin MK. Parents' willingness and attitudes concerning the COVID-19 vaccine: A cross-sectional study. Int J Clin Pract. (2021) 75:e14364. doi: 10.1111/ijcp.14364
79. He K, Mack WJ, Neely M, Lewis L, Anand V. Parental perspectives on immunizations: impact of the COVID-19 pandemic on childhood vaccine hesitancy. J Community Health. (2022) 47:39–52. doi: 10.1007/s10900-021-01017-9
80. Forsyth BWC, Horwitz SM, Leventhal JM, Bruger J, Leaf PJ. The child vulnerability scale: an instrument to measure parental perceptions of child vulnerability1. J Pediatr Psychol. (1996) 21:89–101. doi: 10.1093/jpepsy/21.1.89
81. Green M, Solnit AJ. Reactions to the threatened loss of a child: A vulnerable child syndrome pediatric management of the dying child, part III. Pediatrics. (1964) 34:58–66.
82. Schmid P, Rauber D, Betsch C, Lidolt G, Denker M-L. Barriers of influenza vaccination intention and behavior–a systematic review of influenza vaccine hesitancy, 2005–2016. PLoS ONE. (2017) 12:e0170550. doi: 10.1371/journal.pone.0170550
83. Alfieri NL, Kusma JD, Heard-Garris N, Davis MM, Golbeck E, Barrera L, et al. Parental COVID-19 vaccine hesitancy for children: vulnerability in an urban hotspot. BMC Public Health. (2021) 21:1–9. doi: 10.1186/s12889-021-11725-5
84. Zona S, Partesotti S, Bergomi A, Rosafio C, Antodaro F. Esposito SJ. Anti-COVID vaccination for adolescents: a survey on determinants of vaccine parental hesitancy. Vaccines. (2021) 9:1309. doi: 10.3390/vaccines9111309
85. Simas C, Larson HJ. Overcoming vaccine hesitancy in low-income and middle-income regions. Nat Rev Dis Prim. (2021) 7:41. doi: 10.1038/s41572-021-00279-w
86. Swaney SE, Burns S. Exploring reasons for vaccine-hesitancy among higher-SES parents in Perth, Western Australia. Health Promotion J Austr. (2019) 30:143–52. doi: 10.1002/hpja.190
87. Ashfield S. Donelle LJ. Parental online information access and childhood vaccination decisions in North America: scoping review. J Med Internet Res. (2020) 22:e20002. doi: 10.2196/20002
88. Ngo NV, Pemunta NV, Muluh NE, Adedze M, Basil N., Agwale SJHv, et al. Armed conflict, a neglected determinant of childhood vaccination: some children are left behind. Hum Vaccin Immunother. (2020) 16:1454–63. doi: 10.1080/21645515.2019.1688043
89. Rudan I, Adeloye D, Katikireddi V, Murray J, Simpson C, Shah SA, et al. The COVID-19 pandemic in children and young people during 2020-2021: A complex discussion on vaccination. J Glob Health. (2021) 11:01011. doi: 10.7189/jogh.11.01011
90. Goldman RD, Yan TD, Seiler M, Cotanda CP, Brown JC, Klein EJ, et al. Caregiver willingness to vaccinate their children against COVID-19: Cross sectional survey. Vaccine. (2020) 38:7668–73. doi: 10.1016/j.vaccine.2020.09.084
91. Rogers RW, A. Protection motivation theory of fear appeals and attitude change1. J Psychol. (1975) 91:93–114. doi: 10.1080/00223980.1975.9915803
92. Rogers RW. Cognitive and psychological processes in fear appeals and attitude change: A revised theory of protection motivation. Soc psychophysiol Sourcebook. (1983) 153–76.
93. Rippetoe PA, Rogers RW. Effects of components of protection-motivation theory on adaptive and maladaptive coping with a health threat. J Pers Soc Psychol. (1987) 52:596. doi: 10.1037/0022-3514.52.3.596
94. Janmaimool P. Application of protection motivation theory to investigate sustainable waste management behaviors. Sustainability. (2017) 9:1079. doi: 10.3390/su9071079
95. Ezati Rad R, Mohseni S, Kamalzadeh Takhti H, Hassani Azad M, Shahabi N, Aghamolaei T, et al. Application of the protection motivation theory for predicting COVID-19 preventive behaviors in Hormozgan, Iran: a cross-sectional study. BMC Public Health. (2021) 21:466. doi: 10.1186/s12889-021-10500-w
96. Agrawal A, Kolhapure S, Di Pasquale A, Rai J, Mathur A. Vaccine Hesitancy as a Challenge or Vaccine Confidence as an Opportunity for Childhood Immunisation in India. Infect Dis Ther. (2020) 9:421–32. doi: 10.1007/s40121-020-00302-9
97. Edwards B, Biddle N, Gray M, Sollis K. COVID-19 vaccine hesitancy and resistance: Correlates in a nationally representative longitudinal survey of the Australian population. PLoS ONE. (2021) 16:e0248892. doi: 10.1371/journal.pone.0248892
98. Wang C, Han B, Zhao T, Liu H, Liu B, Chen L, et al. Vaccination willingness, vaccine hesitancy, and estimated coverage at the first round of COVID-19 vaccination in China: A national cross-sectional study. Vaccine. (2021) 39:2833–42. doi: 10.1016/j.vaccine.2021.04.020
99. Ikiişik H, Akif Sezerol M, Taşçi Y, Maral I. COVID-19 vaccine hesitancy: A community-based research in Turkey. Int J Clin Pract. (2021) 75:e14336. doi: 10.1111/ijcp.14336
100. Omidvar S, Firouzbakht M. Acceptance of COVID-19 vaccine and determinant factors in the Iranian population: a web-based study. BMC Health Serv Res. (2022) 22:652. doi: 10.1186/s12913-022-07948-w
101. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. (2000) 25:3186–91. doi: 10.1097/00007632-200012150-00014
102. Opel DJ, Taylor JA, Mangione-Smith R, Solomon C, Zhao C, Catz S, et al. Validity and reliability of a survey to identify vaccine-hesitant parents. Vaccine. (2011) 29:6598–605. doi: 10.1016/j.vaccine.2011.06.115
103. Adam AM, Frimpong S, Boadu MO. Financial literacy and financial planning: Implication for financial well-being of retirees. Bus Econ Horizons. (2017) 13. doi: 10.15208/beh.2017.17
104. Shapiro GK, Tatar O, Dube E, Amsel R, Knauper B, Naz A, et al. The vaccine hesitancy scale: Psychometric properties and validation. Vaccine. (2018) 36:660–7. doi: 10.1016/j.vaccine.2017.12.043
105. Hair JF, Gabriel M, Patel V. AMOS covariance-based structural equation modeling (CB-SEM): Guidelines on its application as a marketing research tool. Braz J Mark. (2014) 13:44–55. doi: 10.5585/remark.v13i2.2718
106. Hooper D, Coughlan J, Mullen M. Evaluating model fit: a synthesis of the structural equation modelling literature. 7th European Conference on Research Methodology for Business and Management Studies. (2008).
108. Stevens JP. Applied multivariate statistics for the social sciences. London, United Kingdom: Routledge (2012).
109. Fischer R, Karl JA. A primer to (cross-cultural) multi-group invariance testing possibilities in R. Front Psychol. (2019) 2019:1507. doi: 10.3389/fpsyg.2019.01507
110. Drasgow F, Kanfer R. Equivalence of psychological measurement in heterogeneous populations. J Appl Psychol. (1985) 70:662. doi: 10.1037/0021-9010.70.4.662
111. Yigit M, Ozkaya-Parlakay A, Senel E. Evaluation of COVID-19 Vaccine Refusal in Parents. Pediatr Infect Dis J. (2021) 40:e134–6. doi: 10.1097/INF.0000000000003042
112. Wagner AL, Huang Z, Ren J, Laffoon M, Ji M, Pinckney LC, et al. Vaccine hesitancy and concerns about vaccine safety and effectiveness in Shanghai, China. Am J Prevent Med. (2021) 60:S77–86. doi: 10.1016/j.amepre.2020.09.003
113. Valckx S, Crèvecoeur J, Verelst F, Vranckx M, Hendrickx G, Hens N, et al. Individual factors influencing COVID-19 vaccine acceptance in between and during pandemic waves (July–December 2020). Vaccine. (2022) 40:151–61. doi: 10.1016/j.vaccine.2021.10.073
114. Çag Y, Bektemür G, Karabela S, Öztürk-Engin D, Çag Y, Aktaş S, et al. Parents' Attitudes Toward COVID-19 Vaccination and Childhood Vaccines During the COVID-19 Pandemic. Asia Pac J Public Health. (2021) 2021:10105395211058291. doi: 10.1177/10105395211058291
115. Tannenbaum MB, Hepler J, Zimmerman RS, Saul L, Jacobs S, Wilson K, et al. Appealing to fear: A meta-analysis of fear appeal effectiveness and theories. Psychol Bull. (2015) 141:1178–204. doi: 10.1037/a0039729
116. Ruiter RA, Kessels LT, Peters GJ, Kok G. Sixty years of fear appeal research: current state of the evidence. Int J Psychol. (2014) 49:63–70. doi: 10.1002/ijop.12042
117. Enticott J, Gill JS, Bacon SL, Lavoie KL, Epstein DS, Dawadi S, et al. Attitudes towards vaccines and intention to vaccinate against COVID-19: a cross-sectional analysis—implications for public health communications in Australia. BMJ Open. (2022) 12:e057127. doi: 10.1136/bmjopen-2021-057127
118. Kenyon G. Australia's struggle with the delta variant. Lancet Infect Dis. (2021) 21:1358. doi: 10.1016/S1473-3099(21)00579-X
119. Borriello A, Master D, Pellegrini A, Rose JM. Preferences for a COVID-19 vaccine in Australia. Vaccine. (2021) 39:473–9. doi: 10.1016/j.vaccine.2020.12.032
120. Enkel SL, Attwell K, Snelling TL, Christian HE. ‘Hesitant compliers': Qualitative analysis of concerned fully-vaccinating parents. Vaccine. (2018) 36:6459–63. doi: 10.1016/j.vaccine.2017.09.088
121. Evans S, Klas A, Mikocka-Walus A, German B, Rogers GD, Ling M, et al. “Poison” or “protection”? A mixed methods exploration of Australian parents' COVID-19 vaccination intentions. J Psychos Res. (2021) 150:110626. doi: 10.1016/j.jpsychores.2021.110626
122. Tso WWY, Wong RS, Tung KTS, Rao N, Fu KW, Yam JCS, et al. Vulnerability and resilience in children during the COVID-19 pandemic. Eur Child Adolesc Psychiatry. (2022) 31:161–76. doi: 10.1007/s00787-020-01680-8
123. Zhou M, Guo W. Social factors and worry associated with COVID-19: Evidence from a large survey in China. Soc Sci Med. (2021) 277:113934. doi: 10.1016/j.socscimed.2021.113934
124. Taubman-Ben-Ari O, Ben-Yaakov O, Chasson M. Parenting stress among new parents before and during the COVID-19 pandemic. Child Abuse & Neglect. (2021) 117:105080. doi: 10.1016/j.chiabu.2021.105080
125. Giannotti M, Mazzoni N, Bentenuto A, Venuti P, de Falco S. Family adjustment to COVID-19 lockdown in Italy: Parental stress, coparenting, and child externalizing behavior. Family Process. (2021) 61:745–63. doi: 10.1111/famp.12686
126. Moscardino U, Dicataldo R, Roch M, Carbone M, Mammarella IC. Parental stress during COVID-19: A brief report on the role of distance education and family resources in an Italian sample. Curr Psychol. (2021) 40:5749–52. doi: 10.1007/s12144-021-01454-8
127. Alhuzimi T. Stress and emotional wellbeing of parents due to change in routine for children with Autism Spectrum Disorder (ASD) at home during COVID-19 pandemic in Saudi Arabia. Res Dev Disabil. (2021) 108:103822. doi: 10.1016/j.ridd.2020.103822
128. Askarian M, Fu L, Taghrir MH, Borazjani R, Shayan Z, Taherifard E, et al. Factors Affecting COVID-19 Vaccination Intent Among Iranians: COVID-19 Vaccination Acceptance. (2020).
129. Ezati Rad R, Kahnouji K, Mohseni S, Shahabi N, Noruziyan F, Farshidi H, et al. Predicting the COVID-19 vaccine receive intention based on the theory of reasoned action in the south of Iran. BMC Public Health. (2022) 22:229. doi: 10.1186/s12889-022-12517-1
130. Yahaghi R, Ahmadizade S, Fotuhi R, Taherkhani E, Ranjbaran M, Buchali Z, et al. Fear of COVID-19 and Perceived COVID-19 Infectability Supplement Theory of Planned Behavior to Explain Iranians' Intention to Get COVID-19 Vaccinated. Vaccines. (2021) 9:684. doi: 10.3390/vaccines9070684
131. Bagherzadeh M, Salehi L, Mahmoodi Z. Investigating preventive health behaviors against COVID-19 in elementary school students' parents: A cross-sectional study from Tehran—Capital of Iran. J Educ Health Promot. (2021) 10:435. doi: 10.4103/jehp.jehp_58_21
132. Samadi SA, Bakhshalizadeh-Moradi S, Khandani F, Foladgar M, Poursaid-Mohammad M, McConkey R. Using hybrid telepractice for supporting parents of children with ASD during the COVID-19 lockdown: a feasibility study in Iran. Brain Sci. (2020) 10:892. doi: 10.3390/brainsci10110892
133. Heidari M, Jafari H. Challenges of COVID-19 vaccination in iran: in the fourth wave of pandemic spread. Prehosp Disaster Med. (2021) 36:659–60. doi: 10.1017/S1049023X21000777
134. Kilic M, Ustundag Ocal N, Uslukilic G. The relationship of COVID-19 vaccine attitude with life satisfaction, religious attitude and COVID-19 avoidance in Turkey. Hum Vaccin Immunother. (2021) 17:3384–93. doi: 10.1080/21645515.2021.1938493
135. Wong L-P, Lee H-Y, Alias H, AbuBakar S. Malaysian parents' willingness to vaccinate their children against COVID-19 infection and their perception of mRNA COVID-19 vaccines. Vaccines. (2022) 10:1790. doi: 10.3390/vaccines10111790
136. Roy DN, Biswas M, Islam E, Azam MS. Potential factors influencing COVID-19 vaccine acceptance and hesitancy: A systematic review. PLoS ONE. (2022) 17:e0265496. doi: 10.1371/journal.pone.0265496
Keywords: parental attitudes toward COVID-19 vaccines, child vulnerability, parental vaccine hesitancy, financial well-being, mediation study
Citation: Sharif Nia H, Allen K-A, Arslan G, Kaur H, She L, Khoshnavay Fomani F, Gorgulu O and Sivarajan Froelicher E (2023) The predictive role of parental attitudes toward COVID-19 vaccines and child vulnerability: A multi-country study on the relationship between parental vaccine hesitancy and financial well-being. Front. Public Health 11:1085197. doi: 10.3389/fpubh.2023.1085197
Received: 31 October 2022; Accepted: 03 January 2023;
Published: 16 February 2023.
Edited by:
Silvio Tafuri, University of Bari Aldo Moro, ItalyReviewed by:
Dumilah Ayuningtyas, University of Indonesia, IndonesiaCharles J. Vukotich, University of Pittsburgh, United States
Copyright © 2023 Sharif Nia, Allen, Arslan, Kaur, She, Khoshnavay Fomani, Gorgulu and Sivarajan Froelicher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fatemeh Khoshnavay Fomani,  Zi5raG9zaG5hdmFAZ21haWwuY29t
Zi5raG9zaG5hdmFAZ21haWwuY29t