
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health , 27 March 2023
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1081518
This article is part of the Research Topic Insights in Life-course Epidemiology and Social Inequalities in Health: 2022 View all 5 articles
 Javier Álvarez-Gálvez1,2
Javier Álvarez-Gálvez1,2 Esther Ortega-Martín1*
Esther Ortega-Martín1* Jesús Carretero-Bravo1
Jesús Carretero-Bravo1 Celia Pérez-Muñoz3
Celia Pérez-Muñoz3 Víctor Suárez-Lledó1
Víctor Suárez-Lledó1 Begoña Ramos-Fiol1
Begoña Ramos-Fiol1Social determinants of multimorbidity are poorly understood in clinical practice. This review aims to characterize the different multimorbidity patterns described in the literature while identifying the social and behavioral determinants that may affect their emergence and subsequent evolution. We searched PubMed, Embase, Scopus, Web of Science, Ovid MEDLINE, CINAHL Complete, PsycINFO and Google Scholar. In total, 97 studies were chosen from the 48,044 identified. Cardiometabolic, musculoskeletal, mental, and respiratory patterns were the most prevalent. Cardiometabolic multimorbidity profiles were common among men with low socioeconomic status, while musculoskeletal, mental and complex patterns were found to be more prevalent among women. Alcohol consumption and smoking increased the risk of multimorbidity, especially in men. While the association of multimorbidity with lower socioeconomic status is evident, patterns of mild multimorbidity, mental and respiratory related to middle and high socioeconomic status are also observed. The findings of the present review point to the need for further studies addressing the impact of multimorbidity and its social determinants in population groups where this problem remains invisible (e.g., women, children, adolescents and young adults, ethnic groups, disabled population, older people living alone and/or with few social relations), as well as further work with more heterogeneous samples (i.e., not only focusing on older people) and using more robust methodologies for better classification and subsequent understanding of multimorbidity patterns. Besides, more studies focusing on the social determinants of multimorbidity and its inequalities are urgently needed in low- and middle-income countries, where this problem is currently understudied.
Multimorbidity can be defined as the co-occurrence of two or more chronic diseases or long-term medical conditions in an individual (1–4). This condition is associated with increased disability and functional impairment, lower quality of life, increased health services utilization, fragmentation of care, polypharmacy, complex treatment, and increased mortality (5–7), particularly among older people. The progressive increase in the number of patients with multimorbidity represents a major global challenge for daily clinical practice, as well as for health systems, governments, and epidemiological research (8–11). Recent evidence has highlighted the limitations of current healthcare systems for addressing the complex needs of patients with comorbidity and multimorbidity due to inadequate or absent attention to coexisting chronic conditions (12–15).
The prevalence of chronic conditions among older populations, such as obesity, hypertension, diabetes, heart disease, chronic obstructive pulmonary disease, musculoskeletal disease, mental disorders, or cancer is growing due to the progressive increase in life expectancy. However, the increase in multimorbidity is only partially explained by population aging (11, 16). Multimorbidity also affects the young population in Western countries, particularly those living in low- and middle-income countries (LMIC) (17). According to the World Health Survey, the average prevalence of multimorbidity is 7.8% in 28 LMICs (11). Similarly, the WHO Study on global AGEing and adult health (SAGE) indicates that more than one-fifth of participants in six LMICs had multimorbidity (18). Recent studies show that social determinants play an essential role in these differences, showing an advance of 10–15 years in the age of onset of multimorbidity among populations with fewer socioeconomic resources (19–21).
Social determinants shape the distribution of health inequalities and chronicity (22). In the same way as communicable diseases, non-communicable diseases are also determined by social and economic differences between populations (socioeconomic status, educational level, economic hardship, lifestyles, and risk behaviors, among others) (23–25). Although the impact of social inequalities on health is clearly identified in the specialized literature, the pattern of association of the different chronic conditions that make up multimorbidity and their respective social and behavioral determinants are not so well-defined (1, 15, 26–29), even though these are the factors that social and health policies could most easily address. Recent work shows that multimorbidity is strongly associated with social and economic factors that condition the early onset of chronicity and subsequent multimorbidity in disadvantaged social groups (1, 19). Indeed, those of low socioeconomic status experience the most negative effects of multimorbidity (30). However, to date, there is little evidence that provides us with information on other types of social and behavioral determinants (such as ethnic characteristics, lifestyles, income, living area, among others) that could be fundamental in the emergence and evolution of multimorbidity patterns that are less prevalent than cardiovascular and musculoskeletal ones, which are the most studied in the literature (for example, multimorbidity among younger groups, mental health patterns, and combined or complex patterns). Therefore, further research is needed to improve our current knowledge of multimorbidity patterns and the social and behavioral determinants that may characterize the different multimorbidity profiles, which is a fundamental step for policy planning and the future sustainability of health systems (31–33).
Current clinical guidelines do not cover all the needs of patients with multimorbidity due to health care that is not tailored to the needs of people with multimorbidity (10). In fact, understanding the different pathological processes of chronicity could improve treatment by focusing on the disease cluster rather than treating individual diseases separately (34). Since there is consistent evidence that chronic diseases tend to accumulate according to certain patterns (15, 19), the identification of specific multimorbidity classes and the social and behavioral factors that give rise to them could help healthcare providers to predict the probability of the occurrence of co-joint chronic conditions, and thus be able to control the appearance of future comorbidities while improving patients' quality of life (15, 35, 36).
Some of these early studies have addressed the social determinants of certain multimorbidity patterns (35). The multimorbidity profiles described in these studies range from well-known chronic disease combinations that conform the most prevalent patterns (e.g., cardiovascular, musculoskeletal, or mental disorders) to more complex disease conglomerates that are usually appear in older age groups (15, 19). The great diversity in the occurrence of these groups of conditions leads to a lack of studies that provide a complete description of the wide range of different multimorbidity patterns (i.e., understood in this context as the specific combination of co-joint chronic conditions) identified through different classification methods, nor do we find studies that comprehensively address the association with the social and behavioral determinants that could affect the different chronicity profiles (34, 38). While some studies have been commonly focused on determinants such as gender and/or age, other studies have been particularly oriented toward the global indicators of multimorbidity (i.e., commonly counting the number of chronic conditions) without taking into account the specific aggregation pattern of chronic diseases (15, 19, 37–39). In this regard, to the best of our knowledge, to date there is no study that provides a comprehensive characterization of the social and behavioral determinants of multimorbidity patterns that have been discovered using diverse methods.
The present systematic review aims to fill this knowledge gap. Specifically, with this work, we aim to (1) characterize the different multimorbidity patterns described in specialized literature; (2) identify the social and behavioral determinants of these multimorbidity profiles (or classes); and (3) describe and compare the different methods used for the classification of multimorbidity profiles, their advantages, and possible limitations. Thus, studies analyzing multimorbidity patterns related to social and behavioral determinants were systematically reviewed.
This systematic review was registered on 10 May 2022 in the PROSPERO database (CRD4202232328140). This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (40).
Our inclusion criteria were as follow:
• Studies with defined patterns of physical and/or mental multimorbidity. Following the World Health Organization definition, we used a broad concept of multimorbidity as the coexistence of two or more chronic conditions in the same individual.
• In addition, we selected studies that associate multimorbidity patterns to social determinants. Specifically, we considered sociodemographic (age, gender, marital status), socioeconomic (education, income, working status, among other) and behavioral (lifestyles) determinants.
• We only reviewed studies written in English and Spanish.
• Finally, we selected articles published from January 1, 2011 to December 31, 2021. We consider this 10-year time frame broad enough to ensure comparability of studies. In fact, although there are earlier studies on multimorbidity it is not until 2012–2014 that the literature begins to focus specifically on multimorbidity patterns (15).
Our exclusion criteria were:
• Studies that were not research articles published in scientific journals (i.e., abstracts, doctoral theses, editorials, press articles, commentaries, journal letters, books and all types of reviews).
• We excluded studies with multimorbidity patterns with a specific underlying disease (i.e., patterns in people with diabetes, with dementia, or similar).
• Moreover, multimorbidity studies with communicable and non-chronic diseases were excluded.
The search was performed by B.R.-F in the databases PubMed/MedLine, Embase, Ovid MEDLINE, PsycINFO, Web of Science, Scopus, and CINAHL Complete on January, 2022. Google Scholar was used to supplement the main databases. This search was repeated in July 2022. The search strategy for this review was performed by combining three sets of keywords (multimorbidity, social-behavioral determinants, and patterns) to search for relevant literature using Boolean operators. The search strategy, which can be found in Supplementary Table 1, was adapted to each database. The references obtained from the search strategy were exported to Microsoft Excel 2019 for deduplication of the results and screening.
The quality of the studies was evaluated using Axis Tool quality assessment (41), a critical appraisal tool to systematically assess the methodological quality of selected studies. This tool consists of 20 questions with expanded explanations that are assessed with yes/no/don't know (for more information see the Supplementary Table 2). These questions evaluate general aspects of the research and reporting, such as the introduction, methodology, and quality of the discussion. The purpose of these questions is to guarantee the quality of the selected studies. The tool was implemented by two reviewers (BR-F, EO-M) that, in the case of disagreement, solved the possible discrepancies using the scores of a third reviewer. The three reviewers jointly analyzed the articles with the lowest methodological score (in our case, two articles with a score of 16/20). After a full evaluation, these articles were retained by the agreement of the reviewers.
First, titles and abstracts were examined by four reviewers (JC-B, EO-M, CP-M, BR-F). Subsequently, the full texts of the retrieved articles were reviewed according to the eligibility criteria. For data extraction from the selected articles, tables created for their organization were used. The information extracted from each publication was: author, title, year of publication, abstract, objective, conclusions, method of pattern extraction, multimorbidity patterns, social-behavioral factors, and population characteristics. Due to the breadth and variety of results the data were divided into different tables. The first table contained the identifying data of the articles (title, authors, and year) (Supplementary Table 3) as well as the summarized content of the article (objectives, topics, and conclusions). The second table compiled the pattern extraction methods and the results obtained, such as multimorbidity patterns, associated social-behavioral factors and the characteristics of the population studied (Supplementary Table 4). The third table combined the articles presenting each social-behavioral determinant according to the pattern extraction method (Supplementary Table 5). For the data analysis, a narrative synthesis and summary of the different methods of identifying patterns and their association with different social determinants were described in order the identify the work done so far and knowledge gaps in this field.
A total of 135,665 articles were identified, of which 48,044 remained after removing duplicates. After screening titles and abstracts, 946 articles were examined for full text. Finally, a total of 97 articles were selected for review after full-text reading and review of methodological quality (Figure 1).
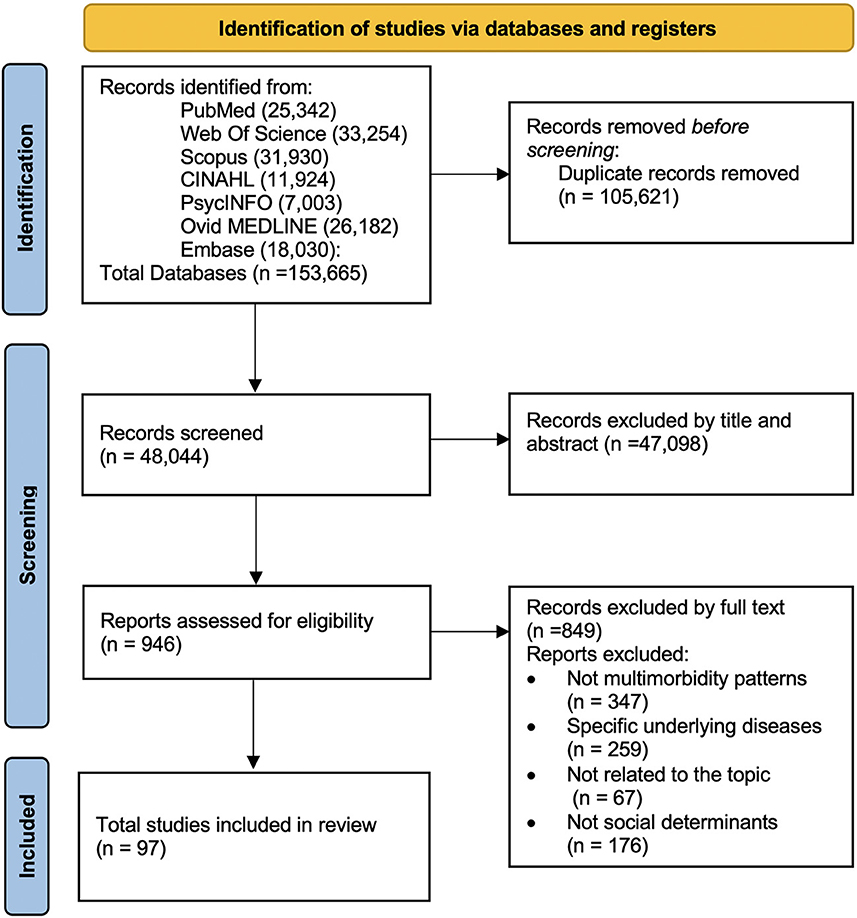
Figure 1. PRISMA flow diagram (40).
Among the selected studies, five main groups of classification techniques for the identification of multimorbidity patterns were found: (1) latent class analysis (42–78); (2) cluster analysis techniques (79–100); (3) factor analysis (101–119); (4) machine learning methods (120–129); and (5) based on expert knowledge (130–137), from the most to the least frequent. The cluster technique included studies using k-means, fuzzy c-means and hierarchical clustering. Factor analysis comprised exploratory factor analysis and principal component analysis. Finally, machine learning tools comprised methods based on network techniques, self-organizing maps, and non-negative matrix factorization.
In total, 41 social and behavioral determinants were found, which were grouped and subsequently analyzed around six principal domains: (1) sociodemographics (including sex, age, and marital status); (2) socioeconomic status (education, poverty, deprivation index, income management, household wealth, occupation, socioeconomic level, occupational status, index of relative socioeconomic disadvantage, financial wealth, skin color/race, and migrate status); (3) lifestyle (smoke, physical activity, drink, sleep quality, substance use, body mass index (BMI), lifestyle risk factor, diet and waist circumference); (4) social networks and social relationships (degree of social relationships, size of social network, and loneliness); (5) living area characteristics (residence place, violence area, area deprivation, area level-income, area level education, area infrastructure); and (6) health service use (type of health insurance, visits, etc.). Table 1 summarizes the main social determinants associated with multimorbidity according to the identified methods for multimorbidity pattern extraction. As we can observe, sociodemographic, socioeconomic and behavioral determinants have been the factors more commonly studied through methods such as latent class analysis, cluster and factor analysis techniques and, recently, through machine learning tools.
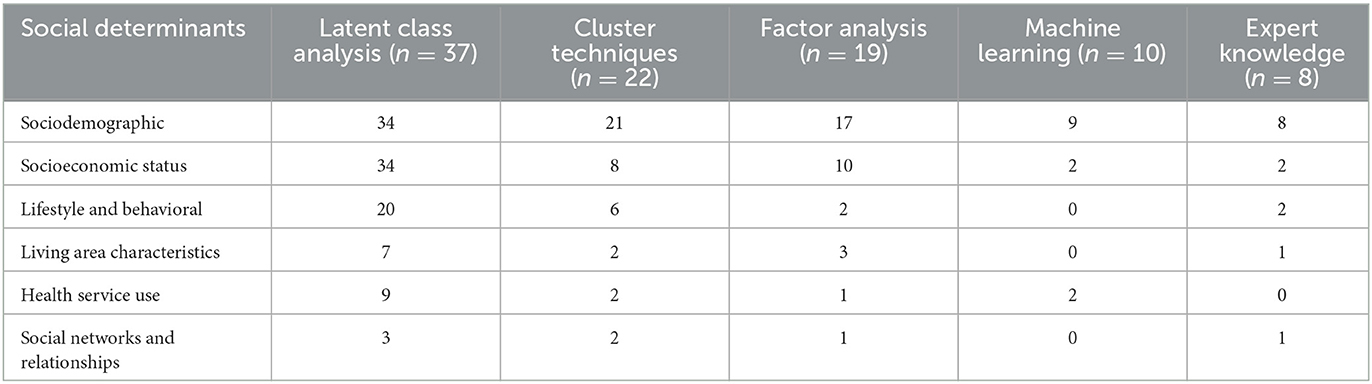
Table 1. Social determinants by multimorbidity pattern extraction method.
A broad set studies detected a stronger association of mental and musculoskeletal multimorbidity with female sex, including neurological diseases (64, 130), musculoskeletal and osteoarticular (42, 64, 67, 71, 93, 102, 126, 130, 131); and common mental disorders (42, 132), like anxiety (44, 67, 86, 93, 114) depression (43, 67, 86, 93, 114, 119), dementia (85) and emotional disorders (47). While cardiometabolic patterns (53, 71, 73, 78, 82, 90, 94, 114, 123), musculoskeletal (53, 96), digestive and genitourinary patterns (99, 110, 124, 131) were more frequent in men. As expected, a positive association between multimorbidity and age was found (67, 74, 105, 110, 132, 133). Although it was also possible to find multimorbidity among the young population, this group was usually classified in patterns called “relatively healthy” (44, 50, 60, 70, 78, 90, 125). The more prevalent multimorbidity patterns in older population were: cardiovascular (44, 58, 60, 71, 72, 81, 86), cardiometabolic (61, 73, 76, 94), musculoskeletal (81, 86, 94), cognitive impairment or dementia-related (60, 86), arthritis-cataracts (53, 58, 72, 87) and respiratory-mental-articular (56, 61). Mental health patterns linked to anxiety and depression were more frequent in younger people (44, 47, 50, 58, 86). However, multimorbidity patterns linked to dementia and cognitive impairment increase significantly with age (111, 128).
In several studies, being married was a protective factor against multimorbidity. In fact, those married were commonly classified in the relatively healthy class (55, 60, 66, 70, 72, 78, 97), while being divorced, separated, or cohabiting couples were more likely to be linked to mental health multimorbidity patterns such as the denominated “depression cluster” (66) and divorced people were more likely to be in the “psychiatric class” (97). In contrast, single people were more likely to belong to the complex multimorbidity pattern (42, 59). Widowers were more likely to belong to dementia, geriatric or neurodegenerative disease classes (78, 128), depression (66) and cardiorespiratory or musculoskeletal patterns (56).
Positive associations were found between household income and multimorbidity (107, 133). In particular, people with lower income presented a higher risk of being in the depression-arthritis (58), depression-chronic pain (48), respiratory (107), and mental health patterns (138). Overall, they were relatively healthy (52, 74) even though having multimorbidity. Conversely, having a low income was associated with a higher probability of belonging to the cardiometabolic pattern (53, 60, 65, 76), suffering musculoskeletal disease (sometimes combined with mental health conditions) (53, 107), and respiratory patterns (53, 76). The proportion of patients with multimorbidity who had physical-mental comorbidities increased substantially with greater socioeconomic deprivation (132, 138). In particular, high-income groups were less likely to present comorbidities such as depression-arthritis (58), depression-chronic pain (48), rhinitis-allergies (107), heart-related diseases or belonging to severe (or complex) multimorbidity classes (44). In general, the higher their income, the more likely they were to belong to the “relatively healthy” class (52, 74). Conversely, having a low income was found to be associated with a higher likelihood of belonging to the cardiometabolic pattern (60), depression-insomnia and musculoskeletal-mental-functional (107), cardiopulmonary and cerebrovascular (65), arthritis, asthma, allergy, depression, and thyroid-related diseases (76), cardiorespiratory-arthritis-cataracts and metabolic classes (63). They were also associated with classes linked to alcohol and substance abuse problems (43). In general, having a low income increased the likelihood of belonging to the classes with the highest rate of disease and mortality (44, 48, 49). In parallel, chronic disease in adulthood tended to increase the risk of poverty (104). Material deprivation was a risk factor for all multimorbidity patterns (59).
Different studies show that low educational levels increase the risk of suffering multimorbidity (42, 70, 75). Low education is associated with cardiometabolic (42, 60), musculoskeletal (75), respiratory (42) and mental health multimorbidity patterns (58), which are commonly organized around depressive disorders. On the other hand, high education was found to be a protective factor among the severely impaired population, metabolic and joint-COPD-ulcer patterns in the study by Zacarías-Pons et al. (59). However, a high educational level also presented a positive association with mental health patterns (specifically, psychiatric disorders and depression) (58). Similarly, being a woman with good education and high income was mainly related to the anxiety-related classes (44). Patterns were also found to be associated with low socioeconomic status (i.e., low education level and low income), such as cardiometabolic (76, 104), metabolic (74), or respiratory-mental-musculoskeletal ones (103). Low educational level and difficulty managing income were also significantly associated with a higher likelihood of having psychosomatic and musculoskeletal patterns (108).
Concerning occupational status, never working increased the risk of belonging to the cardiometabolic class (108) and being unemployed of being classified in multimorbidity patterns linked to substance use (i.e., alcohol, tobacco, and other drugs) (77). Similarly, non-working (42), being unemployed, or pre-retired (70) increased the odds of belonging to any multimorbidity class except the respiratory ones (i.e., characterized by asthma-allergy conditions). Civil servants presented a higher prevalence of musculoskeletal patterns (75) similar to manual workers, which even had a higher probability of belonging to the cognitive and sensory impairment-related classes (97). Also, the vascular-inflammatory class was associated with a low educational level and unemployment (74).
In terms of ethnicity, most studies assessed were focused on Caucasian population (44, 47, 48, 52, 60, 86, 123, 128). Race or ethnicity was found to be associated with certain chronic diseases. Van Cleave et al. (65) found a higher prevalence of cardiopulmonary and cerebrovascular patterns among black men, while Bisquera et al. (86) found that pain and liver disease conditions were also most probably linked with this population group. On the other hand, Janssen et al. (128) found associations with liver patterns and other physical injuries among Native Americans. Kalgotra et al. (123) found associations between endocrine, nutritional, immune, injury, and poisoning-related diseases. The Asian population was linked to cerebrovascular patterns and gastrointestinal cancer (128), and the Caucasian population was commonly associated with mental and musculoskeletal patterns (123).
Regarding migration status, Diaz et al. (109) found that the patterns among Norwegians and immigrants from Western Europe and North America were similar. However, multimorbidity patterns were not the same when compared with other immigrant groups. Janssen et al. (128) found that cardiovascular, cancer and geriatric patterns were more prevalent among local US residents, while urological, gastrointestinal, or respiratory disease patterns were more frequent among non-residents.
Risk behaviors such as alcohol consumption or smoking increased the risk of belonging to all multimorbidity classes, especially in men (54, 79, 108), and also in complex mental health patterns in young men (138). However, several articles report that smoking is also a risk factor for the cardiometabolic class (60, 73), which is associated with other determinants such as less education, lower income and related overweight (60) or higher waist circumference, physical activity, and a history of asthma or heart attack (73). In the study by Barile et al. (68), the mental health class was the most likely to smoke currently. In fact, 46% of people aged 18–44 in the depression class were regular smokers (43). Smoking was a risk factor only for the respiratory-mental-articular class (61). Other studies found that smoking increased the risk for the musculoskeletal class (75, 108). And, as expected, being a current or former smoker also increases the risk of belonging to respiratory multimorbidity patterns (108). Simoes et al. (67) found a direct association between smoking and obesity in the respiratory class. In the cardiorespiratory-arthritis-cataract pattern, the probability of membership increased with increasing age and being a smoker (53).
The relationship between alcohol consumption and multimorbidity was mediated by the age groups and related chronic conditions. Hernández et al. (49) found variations by the country for the relationship between alcohol and multimorbidity patterns. In the USA, the association was negative for all patterns. In contrast, in Canada and England, it was harmful to the patterns of high disease probability and metabolic and arthritis. Finally, positive associations were found in certain patterns such as osteoporosis, arthritis, hypertension, and metabolic in Ireland. According to the study by Jackson et al. (108), people who did not drink alcohol were more likely to belong to the cardiometabolic pattern. Specifically, 50% of people with complex cardiometabolic and cognitive impairment patterns were abstainers. This figure increased in the respiratory patterns where the number of moderate-strong drinkers was highest, while the younger heaviest drinking group were also the healthy subjects (60).
Physical activity was a protective factor for the respiratory-mental-articular class (61). However, physical activity significantly decreased in several groups having certain chronic conditions such as diabetes (75), respiratory and vascular-inflammatory (74). Likewise, some studies (58, 59) found more frequent intense physical activity among relatively healthy classes. On the contrary, lower physical activity was more characteristic in population groups with cardiovascular, musculoskeletal and mental health conditions (68, 97).
Although we did not find studies that analyzed the impact and/or relationship of diet with multimorbidity patterns, a clear association was observed between BMI and the subsequent occurrence of chronic comorbidities. For this reason, we used this indicator as a proxy variable for diet. In particular, obesity increases the risk of belonging to all multimorbidity classes (67, 75). Overweight and obesity were found to be risk factors for musculoskeletal or severe impairment (44) and cardiometabolic (108). Similarly, patterns of physical and mental conditions (68), complex metabolic, respiratory, and age-related conditions (60) were also associated with an increased risk of obesity. Depression was strongly associated with overweight or obesity among females (67).
Regarding the type of area of residence, we found that multimorbidity was more prevalent in urban areas (98). For instance, the cardiometabolic burden was lower in rural areas. Territorial characteristics such as the level of crime and violence in the area were also found to be associated with a pattern of chronic pain and respiratory diseases in men (101). In these areas of higher economic deprivation and lower socioeconomic status (i.e., lower household income and lower education levels), cardiometabolic, respiratory, mental and musculoskeletal patterns were more prevalent (104). Consequently, the possible effect of the area of residence over multimorbidity patterns was linked to specific socioeconomic conditions of the groups. In any case, the existing literature does not provide a clear characterization of either the social mechanisms or the ecological effects involved in the association between the local area of residence and multimorbidity patterns.
Being insured at the medical level presented important variations depending on the different countries and the respective health systems, so no clear association pattern was detected (74, 125). For instance, in the US, people with Medicaid and an additional private insurance were more likely to be found in the oncology and neurological patterns (45). Regarding the use of health services, in the study by Craig et al. (74), all classes of multimorbidity were significantly associated with higher use of health services. Similarly, patterns associated with cardiometabolic complications in pregnancy, vascular and cancer were directly related to unplanned readmissions (121). More specifically, Buja et al. (57) found that patterns such as cardiac, metabolic-ischaemic, cardiorespiratory, or cancer impairment were more at risk of hospitalization than the neurological class. Patterns linked to substance use were also associated with having more than three emergency department visits (77). Egan et al. (79) associated more hospitalizations in congestive heart failure (35%), neurological (27%), and chronic kidney-related disease patterns (24%).
In the study of 2020 by Marengoni et al. (97), the patterns of cognitive and sensory impairment had the highest percentage of people with a poor (or reduced) social network and inadequate physical activity levels. In addition, a large network of friends and having social support were found to reduce the risk of presenting patterns of degenerative-digestive diseases while increasing adherence to medications (62). Moreover, in the same way that social support has been identified as a protective factor against chronicity, the suicide of a family member has also been identified as a risk factor in the development and consolidation of severe patterns of mental multimorbidity (138). On the other hand, the cardiometabolic and respiratory-mental-articular patterns between the ages of 50 and 64 years were associated with a greater presence of feelings of loneliness, limitations in activities of daily living, and a worse state of health (61). On the other hand, the probability of suffering from degenerative-digestive diseases seemed to increase in patients with poor sleep quality and an unbalanced diet, despite having a large family network and a medium-high income (62).
Poor quality of life was associated with belonging to the complex cardiometabolic and respiratory classes (42), and activities of daily living were also affected to a greater extent by specific patterns such as cardiovascular, respiratory, mental and articular (56, 61).
With the intention of reducing the diversity of multimorbidity patterns that we have found in the different studies analyzed up to this point, the most prevalent and relevant profiles were synthesize around nine global classes (in decreasing order): (1) Cardiovascular; (2) Musculoskeletal; (3) Mental; (4) Respiratory; (5) Complex (characterized by many simultaneous chronic diseases or complicated multimorbidity); (6) Cancer; (7) Metabolic; (8) Neurological; and (9) Relatively Healthy (i.e., those who present minor or less serious chronic conditions). Figure 2 describes the number of relationships identified between the most frequent patterns and the respective social determinants (negative values denote that an inverse statistical association was identified).
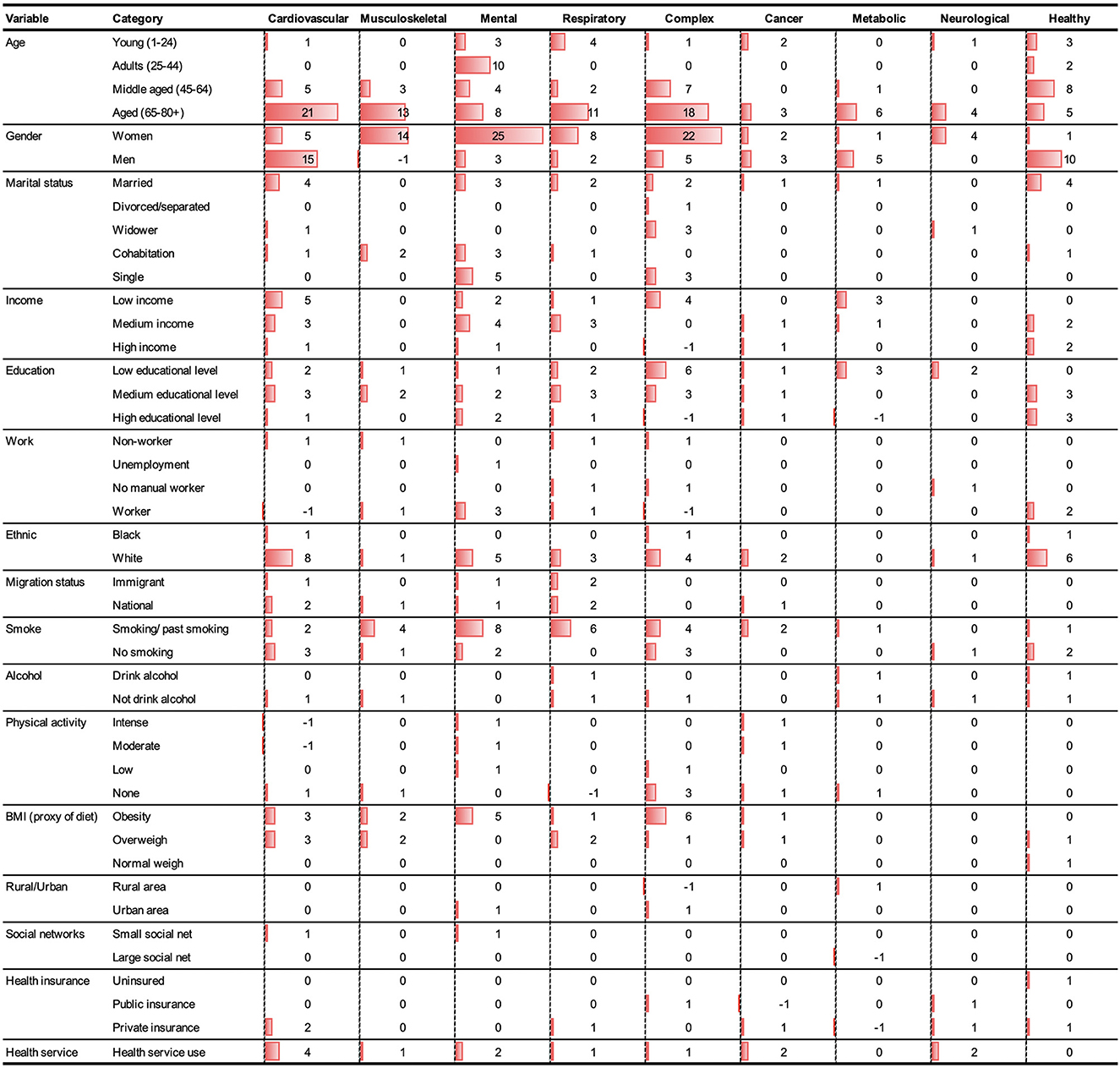
Figure 2. Number of associations identified between different social determinants and the main multimorbidity patterns.
To the best of our knowledge, this is the first systematic review to perform a comprehensive study of the association between multimorbidity and its social and behavioral determinants while considering the statistical methods employed to extract multimorbidity patterns. However, it is possible to find other review papers that separately address multimorbidity patterns (17, 35, 139, 140) or their association (141–143) with specific patterns. Until now, no work has integrated the wide diversity of multimorbidity patterns, social determinants and classification methods. The results yielded 97 publications from which 41 different social determinants (i.e., including sociodemographics, socioeconomic and individual behavioral ones) and the nine most prevalent multimorbidity patterns described in the literature were synthesized. The articles were very diverse regarding extraction methods, determinants studied and the resulting multimorbidity patterns. Nevertheless, some interesting findings were identified.
Although in the present study, we have considered the “relatively healthy” class to characterize individuals with less severe conditions of this problem (e.g., allergies related), the most commonly observed patterns have been the following: cardiovascular, musculoskeletal, mental; respiratory, complex, cancer, metabolic, and neurological. Among these global multimorbidity domains, the three most prevalent patterns identified were generally characterized by musculoskeletal, mental and cardiovascular conditions (17). However, recent studies have identified a fourth highly prevalent pattern characterized by the presence of different allergy related diseases (i.e., seasonal allergies, asthma, digestive or skin problems) (144–146), which in our search is mainly diluted in the respiratory (20, 73, 101, 108) and complex (44, 69) patterns.
From a sociodemographic point of view, our study reveals important differences in the multimorbidity patterns of men and women, which, according to the results described, seem to be linked to avoidable social inequalities that can be linked to the social and economic conditions of these groups. Thus, while musculoskeletal (42, 64, 67, 71, 93, 102, 126, 130, 131) and mental patterns (43, 67, 86, 93, 114, 119) are more typical of women, cardiovascular patterns are more prevalent in men (24, 53, 71, 73, 78, 82, 90, 94, 123), which leads us to believe that behind these results there are also important differences in the individual behaviors and lifestyles of these groups (e.g., considering the differences among married and individuals living alone) (55, 60, 66, 70, 72, 78, 97). Likewise, in the case of age, the present results show that multimorbidity is not only a matter of older people (although it is more visible in these age groups) (89, 104, 105, 137) since certain types of multimorbidity are also observed in young and middle age people, such as mental and allergy multimorbidity patterns (42, 95). In addition, we must consider that most of the studies were focused on the older population. Hence, multimorbidity patterns in children and young are clearly under-represented and under-studied (45, 46).
Similarly, with a few exceptions (51, 65), most studies did not consider ethnic or racial differences. In fact, most reviewed works were oriented to Western countries' populations and mainly applied to white Caucasians groups, even though specific multimorbidity patterns have been found to be more prevalent in African Americans (147). Therefore, multimorbidity patterns described in many of the studies and their association with specific social determinants may be biased in terms of race and ethnicity. Therefore, studies with a more heterogeneous population would be needed to provide a better characterization and measurement of this problem.
Most of the studies in this review demonstrate that a lower socioeconomic status commonly increases the risk of suffering severe multimorbidity (e.g., musculoskeletal, cardiovascular, complex patterns) (44, 48, 49, 53, 59, 60, 63, 65, 76, 107, 132, 133). Multimorbidity patterns can also be linked to social and living conditions and individual lifestyles. For instance, low educational attainment and living in a deprived area were associated with a higher risk of multimorbidity (40, 42, 58, 70, 74–76, 103, 104, 108). People with a low level of education may have a higher risk of health illiteracy and difficulties in finding, understanding and applying health care information (148). In addition, our results show that the behaviors and lifestyles associated with morbidity patterns are in parallel mediated by population socioeconomic conditions. The results show that alcohol and tobacco consumption can substantially impact the appearance of cardiometabolic, musculoskeletal, mental and respiratory multimorbidity patterns (43, 49, 53, 54, 60, 61, 67, 68, 77, 108). At the same time, healthy behaviors such as physical activity seem to slow down the early appearance of these multimorbidity patterns or, at least, lessen their impact on the patient's quality of life (58, 59, 61, 68, 74, 75, 97). Likewise, although no studies have been found that specifically address the impact of diet on multimorbidity, the findings highlight the strong relationship between obesity and overweight with the appearance of the most prevalent patterns (cardiovascular and musculoskeletal) and subsequent mortality in the population (44, 60, 67, 68, 75, 108). In this sense, the need for specific studies to address the relationship between nutrition and multimorbidity (particularly with cancer-related patterns), as well as identifying preventive strategies to intervene in the problem of multimorbidity from an early age, is evident.
Although we have not found many studies that analyse the impact of social networks and personal relationships on multimorbidity, we have identified some works indicating the relevance of social connections in multimorbidity (61, 62, 97). On the other hand, although the impact of multimorbidity on the use of services is clearly reflected in the literature (149), no evidence has been found that points to the possible positive and/or adverse effects that the use of health services can have on specific patterns of multimorbidity. In this sense, we believe this line of work should be addressed in future research.
Although one of our initial objectives was to be able to concisely compare the multimorbidity patterns identified in each investigation, the high heterogeneity of the data and classification techniques used, in addition to the fact that there is no general nomenclature to define the patterns, has not allowed us to synthesize the findings in a generic way, nor to estimate the prevalence of the different patterns. Due to the diversity of articles on multimorbidity and the variety of ways of measuring this health condition and its associated terms, it was difficult to identify an integrative definition of the concept that covered the full spectrum and complexity of mental and physical chronic conditions. Consequently, the pattern extraction methodology was diverse among the selected articles. In the grouping into five categories, the most frequent method was the LCA technique, and the least frequent was expert opinion, which seems to be a classification criterion that is progressively disappearing as new machine learning methods appear that enable the use of different levels of variable measurement, the use of data with high dimensionality and, consequently, facilitate the classification of complex multimorbidity patterns (139). In any case, despite this limitation, we consider this finding to be beneficial, since it highlights the need to work on future research that will make it possible to create a clear conceptual framework and an interoperable taxonomy of multimorbidity patterns in the field, as well as new methods that will allow us to better measure and compare chronicity profiles (146).
The present review has some advantages over previous work. On the one hand, this is the first time that a comprehensive review has been carried out that synthesizes the different classification methods used for the extraction of co-joint chronic disease patterns, together with a detailed description of the different typologies of multimorbidity described in the literature and their respective social and behavioral determinants (including individual sociodemographic and socioeconomic factors, lifestyles and risk behaviors, ethnic group, as well as contextual aspects such as social connectivity, place of residence, or use of health services). On the other hand, despite the difficulties in synthesizing the results of studies based on different populations, chronic pathologies and classification methods, the breadth of our work has allowed us to identify gaps in knowledge on topics that may be fundamental for future approaches to multimorbidity, such as chronicity patterns in children and young people or, for example, the influence of relationships and social networks on the emergence and evolution of chronic pluri-pathology.
The findings of the present review evidence the need for further studies addressing the impact of multimorbidity and its social determinants in population groups where this problem remains invisible (e.g., women, children, adolescents and young adults, ethnic groups, disabled population, older people living alone and/or with few social relations), as well as further work with more heterogeneous samples (i.e., not only focusing on older people) and using more robust methodologies for better classification and subsequent understanding of multimorbidity patterns. In addition, more studies focusing on the social determinants of multimorbidity and its inequalities are urgently needed in LMIC, where this problem is currently understudied. Finally, our results point to the need for the development of multidisciplinary multimorbidity research and new social and health policies tailored to address social inequalities in population groups with different needs, in order to improve health outcomes and increase the efficiency of health services at the local level.
JÁ-G lead the DEMMOCAD project, conceived the study, interpreted the results, and developed the final version of the manuscript. JC-B, EO-M, CP-M, BR-F, and VS-L searched the different databases, extracted the data, assessed the results, and develop the first draft of the document. The manuscript, figures, and final tables were read and approved by all authors.
This publication was supported by public funds the ITI call (integrated territorial investment), developed by the Health Department of the Andalusian Government. The DEMMOCAD project has been 80% co-financed by funds from the FEDER operational program of Andalusia 2014–2020. This publication and research has been partially granted by INDESS (Instituto Universitario de Investigación para el Desarrollo Social Sostenible), University of Cadiz, Jerez de la Frontera, Spain.
We would like to acknowledge the support of the University Research Institute for Sustainable Social Development, the University of Cadiz, the Ramon y Cajal program run by the Spanish Ministry of Science and Innovation, and also, to the Doctoral Programme in Clinical Medicine and Public Health, University of Granada, Spain.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1081518/full#supplementary-material
1. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. (2012) 380:37–43. doi: 10.1016/S0140-6736(12)60240-2
2. World Health Organization. The World Health Report 2008: Primary Health Care Now More Than Ever. World Health Organization (2008). Available online at: https://apps.who.int/iris/handle/10665/43949 (accessed June 24, 2022).
3. Fortin M. Prevalence of multimorbidity among adults seen in family practice. Ann Fam Med. (2005) 3:223–8. doi: 10.1370/afm.272
4. van den Akker M, Buntinx F, Metsemakers JFM, Roos S, Knottnerus JA. Multimorbidity in general practice: prevalence, incidence, and determinants of co-occurring chronic and recurrent diseases. J Clin Epidemiol. (1998) 51:367–75. doi: 10.1016/S0895-4356(97)00306-5
5. Gallacher KI, Batty GD, McLean G, Mercer SW, Guthrie B, May CR, et al. Stroke, multimorbidity and polypharmacy in a nationally representative sample of 1,424,378 patients in Scotland: implications for treatment burden. BMC Med. (2014) 12:151. doi: 10.1186/s12916-014-0151-0
6. Gijsen R, Hoeymans N, Schellevis FG, Ruwaard D, Satariano WA. Causes and consequences of comorbidity: a review. J Clin Epidemiol. (2001) 54:661–74. doi: 10.1016/S0895-4356(00)00363-2
7. Vetrano DL, Roso-Llorach A, Fernández S, Guisado-Clavero M, Violán C, Onder G, et al. Twelve-year clinical trajectories of multimorbidity in a population of older adults. Nat Commun. (2020) 11:3223. doi: 10.1038/s41467-020-16780-x
8. Fortin M, Soubhi H, Hudon C, Bayliss EA, van den Akker M. Multimorbidity's many challenges. BMJ. (2007) 334:1016–7. doi: 10.1136/bmj.39201.463819.2C
9. Fortin M, Lapointe L, Hudon C, Vanasse A. Multimorbidity is common to family practice: Is it commonly researched? Can Fam Physician. (2005) 51:244–5.
10. Moffat K, Mercer SW. Challenges of managing people with multimorbidity in today's healthcare systems. BMC Fam Pract. (2015) 16:129. doi: 10.1186/s12875-015-0344-4
11. Afshar S, Roderick PJ, Kowal P, Dimitrov BD, Hill AG. Multimorbidity and the inequalities of global ageing: a cross-sectional study of 28 countries using the World Health Surveys. BMC Public Health. (2015) 15:776. doi: 10.1186/s12889-015-2008-7
12. Starfield B, Lemke KW, Bernhardt T, Foldes SS, Forrest CB, Weiner JP. Comorbidity: implications for the importance of primary care in ‘case’ management. Ann Fam Med. (2003) 1:8–14. doi: 10.1370/afm.1
13. Tinetti ME, Bogardus ST, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med. (2004) 351:2870–4. doi: 10.1056/NEJMsb042458
14. Redelmeier DA, Tan SH, Booth GL. The treatment of unrelated disorders in patients with chronic medical diseases. N Engl J Med. (1998) 338:1516–20. doi: 10.1056/NEJM199805213382106
15. Prados-Torres A, Calderón-Larrañaga A, Hancco-Saavedra J, Poblador-Plou B, van den Akker M. Multimorbidity patterns: a systematic review. J Clin Epidemiol. (2014) 67:254–66. doi: 10.1016/j.jclinepi.2013.09.021
16. Prados-Torres A, Del Cura-González I, Prados-Torres J, Leiva-Fernández F, López-Rodríguez J, Calderón-Larrañaga A, et al. Multimorbidity in general practice and the Ariadne principles. A person-centred approach. Aten Primaria. (2017) 49:300–7. doi: 10.1016/j.aprim.2016.11.013
17. Hay SI, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. (2017) 390:1260–344. doi: 10.1016/S0140-6736(17)32130-X
18. Arokiasamy P, Uttamacharya U, Jain K, Biritwum RB, Yawson AE, Wu F, et al. The impact of multimorbidity on adult physical and mental health in low- and middle-income countries: what does the study on global ageing and adult health (SAGE) reveal? BMC Med. (2015) 13:178. doi: 10.1186/s12916-015-0402-8
19. Violan C, Foguet-Boreu Q, Flores-Mateo G, Salisbury C, Blom J, Freitag M, et al. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS ONE. (2014) 9:e102149. doi: 10.1371/journal.pone.0102149
20. van Oostrom SH, Gijsen R, Stirbu I, Korevaar JC, Schellevis FG, Picavet HSJ, et al. Time trends in prevalence of chronic diseases and multimorbidity not only due to aging: data from general practices and health surveys. PLoS ONE. (2016) 11:e0160264. doi: 10.1371/journal.pone.0160264
21. Beaglehole R, Epping-Jordan J, Patel V, Chopra M, Ebrahim S, Kidd M, et al. Improving the prevention and management of chronic disease in low-income and middle-income countries: a priority for primary health care. Lancet Lond Engl. (2008) 372:940–9. doi: 10.1016/S0140-6736(08)61404-X
22. Vogeli C, Shields AE, Lee TA, Gibson TB, Marder WD, Weiss KB, et al. Multiple chronic conditions: prevalence, health consequences, and implications for quality, care management, and costs. J Gen Intern Med. (2007) 22:391–5. doi: 10.1007/s11606-007-0322-1
23. Schäfer I, Leitner EC von, Schön G, Koller D, Hansen H, Kolonko T, et al. Multimorbidity patterns in the elderly: a new approach of disease clustering identifies complex interrelations between chronic conditions. PLoS ONE. (2010) 5:e15941. doi: 10.1371/journal.pone.0015941
24. Lappenschaar M, Hommersom A, Lucas PJF. Probabilistic causal models of multimorbidity concepts. AMIA Annu Symp Proc. (2012) 2012:475–84.
25. Andrade LH, Benseñor IM, Viana MC, Andreoni S, Wang YP. Clustering of psychiatric and somatic illnesses in the general population: multimorbidity and socioeconomic correlates. Braz J Med Biol Res Rev Bras Pesqui Medicas E Biol. (2010) 43:483–91. doi: 10.1590/S0100-879X2010007500024
26. Rzewuska M, de Azevedo-Marques JM, Coxon D, Zanetti ML, Zanetti ACG, Franco LJ, et al. Epidemiology of multimorbidity within the Brazilian adult general population: evidence from the 2013 National Health Survey (PNS 2013). PLoS ONE. (2017) 12:e0171813. doi: 10.1371/journal.pone.0171813
27. Banerjee S. Multimorbidity–older adults need health care that can count past one. Lancet Lond Engl. (2015) 385:587–9. doi: 10.1016/S0140-6736(14)61596-8
28. Muth C, Beyer M, Fortin M, Rochon J, Oswald F, Valderas JM, et al. Multimorbidity's research challenges and priorities from a clinical perspective: the case of ‘Mr Curran’. Eur J Gen Pract. (2014) 20:139–47. doi: 10.3109/13814788.2013.839651
29. Weiss CO, Varadhan R, Puhan MA, Vickers A, Bandeen-Roche K, Boyd CM, et al. Multimorbidity and evidence generation. J Gen Intern Med. (2014) 29:653–60. doi: 10.1007/s11606-013-2660-5
30. Vetrano DL, Calderón-Larrañaga A, Marengoni A, Onder G, Bauer JM, Cesari M, et al. An international perspective on chronic multimorbidity: approaching the elephant in the room. J Gerontol Ser A. (2018) 73:1350–6. doi: 10.1093/gerona/glx178
31. Álvarez-Gálvez J, Rodero-Cosano ML, Salinas-Pérez JA, Gómez-Baya D. Exploring the complex associations among social determinants of health in andalusia after the 2008 financial crisis. Soc Indic Res. (2019) 141:873–93. doi: 10.1007/s11205-018-1845-z
32. Alvarez-Galvez J. Discovering complex interrelationships between socioeconomic status and health in Europe: a case study applying Bayesian Networks. Soc Sci Res. (2016) 56:133–43. doi: 10.1016/j.ssresearch.2015.12.011
33. Alvarez-Galvez J. Multidimensionality of health inequalities: a cross-country identification of health clusters through multivariate classification techniques. Int J Environ Res Public Health. (2018) 15:E1900. doi: 10.3390/ijerph15091900
34. Busija L, Lim K, Szoeke C, Sanders KM, McCabe MP. Do replicable profiles of multimorbidity exist? Systematic review and synthesis. Eur J Epidemiol. (2019) 34:1025–53. doi: 10.1007/s10654-019-00568-5
35. Hernández B, Reilly RB, Kenny RA. Investigation of multimorbidity and prevalent disease combinations in older Irish adults using network analysis and association rules. Sci Rep. (2019) 9:14567. doi: 10.1038/s41598-019-51135-7
36. Mondor L, Cohen D, Khan AI, Wodchis WP. Income inequalities in multimorbidity prevalence in Ontario, Canada: a decomposition analysis of linked survey and health administrative data. Int J Equity Health. (2018) 17:90. doi: 10.1186/s12939-018-0800-6
37. Huntley AL, Johnson R, Purdy S, Valderas JM, Salisbury C. Measures of multimorbidity and morbidity burden for use in primary care and community settings: a systematic review and guide. Ann Fam Med. (2012) 10:134–41. doi: 10.1370/afm.1363
38. France EF, Wyke S, Gunn JM, Mair FS, McLean G, Mercer SW. Multimorbidity in primary care: a systematic review of prospective cohort studies. Br J Gen Pract J R Coll Gen Pract. (2012) 62:e297–307. doi: 10.3399/bjgp12X636146
39. Pathirana TI, Jackson CA. Socioeconomic status and multimorbidity: a systematic review and meta-analysis. Aust N Z J Public Health. (2018) 42:186–94. doi: 10.1111/1753-6405.12762
40. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:89. doi: 10.1136/bmj.n71
41. Downes M, Brennan M, Williams H, Dean R. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open. (2016) 6:e011458. doi: 10.1136/bmjopen-2016-011458
42. Larsen FB, Pedersen MH, Friis K, Glümer C, Lasgaard M. A latent class analysis of multimorbidity and the relationship to socio-demographic factors and health-related quality of life. A national population-based study of 162,283 Danish adults. PLoS ONE. (2017) 12:e0169426. doi: 10.1371/journal.pone.0169426
43. Zhu Y, Edwards D, Mant J, Payne RA, Kiddle S. Characteristics, service use and mortality of clusters of multimorbid patients in England: a population-based study. BMC Med. (2020) 18:78. doi: 10.1186/s12916-020-01543-8
44. Zheng DD, McCollister KE, Christ SL, Lam BL, Feaster DJ, Lee DJ. Chronic condition patterns in the US population and their association with health related quality of life. Prev Med. (2020) 136:106102. doi: 10.1016/j.ypmed.2020.106102
45. Lindley LC, Mack JW, Bruce DJ. Clusters of multiple complex chronic conditions: a latent class analysis of children at end of life. J Pain Symptom Manage. (2016) 51:868–74. doi: 10.1016/j.jpainsymman.2015.12.310
46. Carrilero N, Dalmau-Bueno A, García-Altés A. Comorbidity patterns and socioeconomic inequalities in children under 15 with medical complexity: a population-based study. BMC Pediatr. (2020) 20:358. doi: 10.1186/s12887-020-02253-z
47. Essau CA, de la Torre-Luque A. Comorbidity profile of mental disorders among adolescents: a latent class analysis. Psychiatry Res. (2019) 278:228–34. doi: 10.1016/j.psychres.2019.06.007
48. Morin RT, Li Y, Mackin RS, Whooley M, Byers AL, Francisco S, et al. Comorbidity profiles identified in older primary care patients who attempt suicide. J Am Geriatr Soc. (2019) 67:2553–9. doi: 10.1111/jgs.16126
49. Hernández B, Voll S, Lewis NA, McCrory C, White A, Stirland L, et al. Comparisons of disease cluster patterns, prevalence and health factors in the USA, Canada, England and Ireland. BMC Public Health. (2021) 21:1674. doi: 10.1186/s12889-021-11706-8
50. Pugh MJV, Finley EP, Copeland LA, Wang CP, Noel PH, Amuan ME, et al. Complex comorbidity clusters in OEF/OIF veterans: the polytrauma clinical triad and beyond. Med Care. (2014) 52:172–81. doi: 10.1097/MLR.0000000000000059
51. Smith CM, Feigal J, Sloane R, Biederman DJ. Differences in clinical outcomes of adults referred to a homeless transitional care program based on multimorbid health profiles: a latent class analysis. Front Psychiatry. (2021) 12:780366. doi: 10.3389/fpsyt.2021.780366
52. Gebregziabher M, Ward RC, Taber DJ, Walker RJ, Ozieh M, Dismuke CE, et al. Ethnic and geographic variations in multimorbidty: evidence from three large cohorts. Soc Sci Med. (2018) 211:198–206. doi: 10.1016/j.socscimed.2018.06.020
53. Nguyen H, Chua KC, Dregan A, Vitoratou S, Bayes-Marin I, Olaya B, et al. Factors associated with multimorbidity patterns in older adults in england: findings from the English Longitudinal Study of Aging (ELSA). J Aging Health. (2020) 32:1120–32. doi: 10.1177/0898264319891026
54. Chidumwa G, Maposa I, Corso B, Minicuci N, Kowal P, Micklesfield LK, et al. Identifying co-occurrence and clustering of chronic diseases using latent class analysis: cross-sectional findings from SAGE South Africa Wave 2. BMJ Open. (2021) 11:e041604. doi: 10.1136/bmjopen-2020-041604
55. Whitson HE, Johnson KS, Sloane R, Cigolle CT, Pieper CF, Landerman L, et al. Identifying patterns of multimorbidity in older americans: application of latent class analysis. J Am Geriatr Soc. (2016) 64:1668–73. doi: 10.1111/jgs.14201
56. Olaya B, Moneta MV, Caballero FF, Tyrovolas S, Bayes I, Ayuso-Mateos JL, et al. Latent class analysis of multimorbidity patterns and associated outcomes in Spanish older adults: a prospective cohort study. BMC Geriatr. (2017) 17:186. doi: 10.1186/s12877-017-0586-1
57. Buja A, Rivera M, De Battisti E, Corti MC, Avossa F, Schievano E, et al. Multimorbidity and hospital admissions in high-need, high-cost elderly patients. J Aging Health. (2020) 32:259–68. doi: 10.1177/0898264318817091
58. Bendayan R, Zhu Y, Federman AD, Dobson RJB. Multimorbidity patterns and memory trajectories in older adults: evidence from the english longitudinal study of aging. J Gerontol Ser Biol Sci Med Sci. (2021) 76:867–75. doi: 10.1093/gerona/glab009
59. Zacarías-Pons L, Vilalta-Franch J, Turró-Garriga O, Saez M, Garre-Olmo J. Multimorbidity patterns and their related characteristics in European older adults: a longitudinal perspective. Arch Gerontol Geriatr. (2021) 95:104428. doi: 10.1016/j.archger.2021.104428
60. Zheng DD, Loewenstein DA, Christ SL, Feaster DJ, Lam BL, McCollister KE, et al. Multimorbidity patterns and their relationship to mortality in the US older adult population. PLoS ONE. (2021) 16:e0245053. doi: 10.1371/journal.pone.0245053
61. Bayes-Marin I, Sanchez-Niubo A, Egea-Cortés L, Nguyen H, Prina M, Fernández D, et al. Multimorbidity patterns in low-middle and high income regions: a multiregion latent class analysis using ATHLOS harmonised cohorts. BMJ Open. (2020) 10:e034441. doi: 10.1136/bmjopen-2019-034441
62. Lu J, Wang Y, Hou L, Zuo Z, Zhang N, Wei A. Multimorbidity patterns in old adults and their associated multi-layered factors: a cross-sectional study. BMC Geriatr. (2021) 21:372. doi: 10.1186/s12877-021-02292-w
63. Nguyen H, Wu YT, Dregan A, Vitoratou S, Chua KC, Prina AM. Multimorbidity patterns, all-cause mortality and healthy aging in older English adults: results from the English Longitudinal Study of Aging. Geriatr Gerontol Int. (2020) 20:1126–32. doi: 10.1111/ggi.14051
64. Nguyen QD, Wu C, Odden MC, Kim DH. Multimorbidity patterns, frailty, and survival in community-dwelling older adults. J Gerontol Ser Biol Sci Med Sci. (2019) 74:1265–70. doi: 10.1093/gerona/gly205
65. Van Cleave JH, Egleston BL, Abbott KM, Hirschman KB, Rao A, Naylor MD. Multiple chronic conditions and hospitalizations among recipients of long-term services and supports. Nurs Res. (2016) 65:425–34. doi: 10.1097/NNR.0000000000000185
66. Bratzke L, Carlson B, Moon C, Brown R, Koscik R, Johnson S. Multiple Chronic Conditions: implications for cognition - findings from the Wisconsin Registry for Alzheimer's Prevention (WRAP). Physiol Behav. (2018) 42:56–61. doi: 10.1016/j.apnr.2018.06.004
67. Simões D, Araújo FA, Severo M, Monjardino T, Cruz I, Carmona L, et al. Patterns and consequences of multimorbidity in the general population: there is no chronic disease management without rheumatic disease management. Arthritis Care Res. (2017) 69:12–20. doi: 10.1002/acr.22996
68. Barile JP, Mitchell SA, Thompson WW, Zack MM, Reeve BB, Cella D, et al. Patterns of chronic conditions and their associations with behaviors and quality of life, 2010. Prev Chronic Dis. (2015) 12:150179. doi: 10.5888/pcd12.150179
69. Filipčić I, Šimunović Filipčić I, Grošić V, Bakija I, Šago D, Benjak T, et al. Patterns of chronic physical multimorbidity in psychiatric and general population. J Psychosom Res. (2018) 114:72–80. doi: 10.1016/j.jpsychores.2018.09.011
70. Møller SP, Laursen B, Johannesen CK, Tolstrup JS, Schramm S. Patterns of multimorbidity and demographic profile of latent classes in a Danish population-A register-based study. PLoS ONE. (2020) 15:e0237375. doi: 10.1371/journal.pone.0237375
71. Tan XW, Xie Y, Lew JK, Lee PSS, Lee ES. Patterns of patients with multiple chronic conditions in primary care: a cross-sectional study. PLoS ONE. (2020) 15:e0238353. doi: 10.1371/journal.pone.0238353
72. Ronaldson A, Arias de la Torre J, Bendayan R, Yadegarfar ME, Rhead R, Douiri A, et al. Physical multimorbidity, depressive symptoms, and social participation in adults over 50 years of age: findings from the English Longitudinal Study of Ageing. Aging Ment Health. (2021) 27:43–53. doi: 10.1080/13607863.2021.2017847
73. Hunter ML, Knuiman MW, Musk B, Hui J, Murray K, Beilby JP, et al. Prevalence and patterns of multimorbidity in Australian baby boomers: the Busselton healthy ageing study. BMC Public Health. (2021) 21:1539. doi: 10.1186/s12889-021-11578-y
74. Craig LS, Cunningham-Myrie CA, Hotchkiss DR, Hernandez JH, Gustat J, Theall KP. Social determinants of multimorbidity in Jamaica: application of latent class analysis in a cross-sectional study. BMC Public Health. (2021) 21:1197. doi: 10.1186/s12889-021-11225-6
75. Khorrami Z, Rezapour M, Etemad K, Yarahmadi S, Khodakarim S, Mahdavi Hezaveh A, et al. The patterns of non-communicable disease multimorbidity in iran: a multilevel analysis. Sci Rep. (2020) 10:3034. doi: 10.1038/s41598-020-59668-y
76. Park B, Lee HA, Park H. Use of latent class analysis to identify multimorbidity patterns and associated factors in Korean adults aged 50 years and older. PLoS ONE. (2019) 14:e0216259. doi: 10.1371/journal.pone.0216259
77. Prenovost KM, Fihn SD, Maciejewski ML, Nelson K, Vijan S, Rosland AM. Using item response theory with health system data to identify latent groups of patients with multiple health conditions. PLoS ONE. (2018) 13:e0206915. doi: 10.1371/journal.pone.0206915
78. Tazzeo C, Rizzuto D, Calderón-Larrañaga A, Roso-Llorach A, Marengoni A, Welmer AK, et al. Multimorbidity patterns and risk of frailty in older community-dwelling adults: A population-based cohort study. Age Ageing. (2021) 50:2183–91. doi: 10.1093/ageing/afab138
79. Egan BM, Sutherland SE, Tilkemeier PL, Davis RA, Rutledge V, Sinopoli A. A cluster-based approach for integrating clinical management of Medicare beneficiaries with multiple chronic conditions. PLoS ONE. (2019) 14:e0217696. doi: 10.1371/journal.pone.0217696
80. Alhasoun F, Aleissa F, Alhazzani M, Moyano LG, Pinhanez C, González MC. Age density patterns in patients medical conditions: a clustering approach. PLoS Comput Biol. (2018) 14:e1006115. doi: 10.1371/journal.pcbi.1006115
81. Bekić S, Babič F, Filipčić I, Majnarić LT. Clustering of mental and physical comorbidity and the risk of frailty in patients aged 60 years or more in primary care. Med Sci Monit. (2019) 25:6820–35. doi: 10.12659/MSM.915063
82. Roso-Llorach A, Violán C, Foguet-Boreu Q, Rodriguez-Blanco T, Pons-Vigués M, Pujol-Ribera E, et al. Comparative analysis of methods for identifying multimorbidity patterns: a study of ‘real-world' data. BMJ Open. (2018) 8:e01898. doi: 10.1136/bmjopen-2017-018986
83. Lai FTT, Beeler PE, Yip BHK, Cheetham M, Chau PYK, Chung RY, et al. Comparing multimorbidity patterns among discharged middle-aged and older inpatients between hong kong and zurich: a hierarchical agglomerative clustering analysis of routine hospital records. Front Med. (2021) 8:651925. doi: 10.3389/fmed.2021.651925
84. Collerton J, Jagger C, Yadegarfar ME, Davies K, Parker SG, Robinson L, et al. Deconstructing complex multimorbidity in the very old: findings from the newcastle 85+ study. BioMed Res Int. (2016) 2016:8745670. doi: 10.1155/2016/8745670
85. Matesanz-Fernández M, Seoane-Pillado T, Iñiguez-Vázquez I, Suárez-Gil R, Pértega-Díaz S, Casariego-Vales E. Description of multimorbidity clusters of admitted patients in medical departments of a general hospital. Postgrad Med J. (2021) 98:294–9 doi: 10.1136/postgradmedj-2020-139361
86. Bisquera A, Gulliford M, Dodhia H, Ledwaba-Chapman L, Durbaba S, Soley-Bori M, et al. Identifying longitudinal clusters of multimorbidity in an urban setting: a population-based cross-sectional study. Lancet Reg Health Eur. (2021) 3:100047. doi: 10.1016/j.lanepe.2021.100047
87. Wang X, Yao S, Wang M, Cao G, Chen Z, Huang Z, et al. Multimorbidity among two million adults in China. Int J Environ Res Public Health. (2020) 17:3395. doi: 10.3390/ijerph17103395
88. Machón M, Mateo-Abad M, Clerencia-Sierra M, Güell C, Poblador-Pou B, Vrotsou K, et al. Multimorbidity and functional status in older people: a cluster analysis. Eur Geriatr Med. (2020) 11:321–32. doi: 10.1007/s41999-020-00291-5
89. Wang L, Palmer AJM and health related quality of life (HRQoL) in a nationally representative population sample: I of count versus cluster method for defining multimorbidity on Hrq, Cocker F, Sanderson K. Multimorbidity and health-related quality of life (HRQoL) in a nationally representative population sample: implications of count versus cluster method for defining multimorbidity on HRQoL. Health Qual Life Outcomes. (2017) 15:7–7. doi: 10.1186/s12955-016-0580-x
90. Marengoni A, Tazzeo C, Calderón-Larrañaga A, Roso-Llorach A, Onder G, Zucchelli A, et al. Multimorbidity Patterns and 6-year risk of institutionalization in older persons: the role of social formal and informal care. J Am Med Dir Assoc. (2021) 22:2184–9. doi: 10.1016/j.jamda.2020.12.040
91. Foguet-Boreu Q, Violán C, Rodriguez-Blanco T, Roso-Llorach A, Pons-Vigués M, Pujol-Ribera E, et al. Multimorbidity patterns in elderly primary health care patients in a South Mediterranean European region: a cluster analysis. PLoS ONE. (2015) 10:e0141155. doi: 10.1371/journal.pone.0141155
92. Guisado-Clavero M, Roso-Llorach A, López-Jimenez T, Pons-Vigués M, Foguet-Boreu Q, Muñoz MA, et al. Multimorbidity patterns in the elderly: a prospective cohort study with cluster analysis. BMC Geriatr. (2018) 18:16. doi: 10.1186/s12877-018-0705-7
93. Baré M, Herranz S, Roso-Llorach A, Jordana R, Violán C, Lleal M, et al. Multimorbidity patterns of chronic conditions and geriatric syndromes in older patients from the MoPIM multicentre cohort study. BMJ Open. (2021) 11:e049334. doi: 10.1136/bmjopen-2021-049334
94. Violán C, Roso-Llorach A, Foguet-Boreu Q, Guisado-Clavero M, Pons-Vigués M, Pujol-Ribera E, et al. Multimorbidity patterns with K-means nonhierarchical cluster analysis. BMC Fam Pract. (2018) 19:108. doi: 10.1186/s12875-018-0790-x
95. Violán C, Foguet-Boreu Q, Roso-Llorach A, Rodriguez-Blanco T, Pons-Vigués M, Pujol-Ribera E, et al. Patrones de multimorbilidad en adultos jóvenes en Cataluña: un análisis de clústeres. Aten Primaria. (2016) 48:479–92. doi: 10.1016/j.aprim.2015.10.006
96. Teh RO, Menzies OH, Connolly MJ, Doughty RN, Wilkinson TJ, Pillai A, et al. Patterns of multi-morbidity and prediction of hospitalisation and all-cause mortality in advanced age. Age Ageing. (2018) 47:261–8. doi: 10.1093/ageing/afx184
97. Marengoni A, Roso-Llorach A, Vetrano DL, Fernández-Bertolín S, Guisado-Clavero M, Violán C, et al. Patterns of multimorbidity in a population-based cohort of older people: sociodemographic, lifestyle, clinical, and functional differences. J Gerontol A Biol Sci Med Sci. (2020) 75:798–805. doi: 10.1093/gerona/glz137
98. Yao SS, Cao GY, Han L, Chen ZS, Huang ZT, Gong P, et al. Prevalence and patterns of multimorbidity in a nationally representative sample of older Chinese: results from the china health and retirement longitudinal study. J Gerontol Ser Biol Sci Med Sci. (2020) 75:1974–80. doi: 10.1093/gerona/glz185
99. Violán C, Foguet-Boreu Q, Fernández-Bertolín S, Guisado-Clavero M, Cabrera-Bean M, Formiga F, et al. Soft clustering using real-world data for the identification of multimorbidity patterns in an elderly population: cross-sectional study in a Mediterranean population. BMJ Open. (2019) 9:e029594. doi: 10.1136/bmjopen-2019-029594
100. Ibarra-Castillo C, Guisado-Clavero M, Violan-Fors C, Pons-Vigués M, López-Jiménez T, Roso-Llorach A. Survival in relation to multimorbidity patterns in older adults in primary care in Barcelona, Spain (2010-2014): a longitudinal study based on electronic health records. J Epidemiol Community Health. (2018) 72:185–92. doi: 10.1136/jech-2017-209984
101. Wang YP, Nunes BP, Coêlho BM, Santana GL, do Nascimento CF, Viana MC, et al. Multilevel analysis of the patterns of physical-mental multimorbidity in general population of São Paulo Metropolitan Area, Brazil. Sci Rep. (2019) 9:2390. doi: 10.1038/s41598-019-39326-8
102. Prados-Torres A, Poblador-Plou B, Calderón-Larrañaga A, Gimeno-Feliu LA, González-Rubio F, Poncel-Falcó A, et al. Multimorbidity patterns in primary care: interactions among chronic diseases using factor analysis. PLoS ONE. (2012) 7:e32190. doi: 10.1371/journal.pone.0032190
103. Eaton NR, Keyes KM, Krueger RF, Noordhof A, Skodol AE, Markon KE, et al. Ethnicity and psychiatric comorbidity in a national sample: evidence for latent comorbidity factor invariance and connections with disorder prevalence. Soc Psychiatry Psychiatr Epidemiol. (2013) 48:701–10. doi: 10.1007/s00127-012-0595-5
104. Nunes BP, Chiavegatto Filho ADP, Pati S, Cruz Teixeira DS, Flores TR, Camargo-Figuera FA, et al. Contextual and individual inequalities of multimorbidity in Brazilian adults: a cross-sectional national-based study. BMJ Open. (2017) 7:e015885. doi: 10.1136/bmjopen-2017-015885
105. Walker V, Perret-Guillaume C, Kesse-Guyot E, Agrinier N, Hercberg S, Galan P, et al. Effect of multimorbidity on health-related quality of life in adults aged 55 years or older: results from the SU.VI.MAX 2 Cohort. PLoS ONE. (2016) 11:e0169282. doi: 10.1371/journal.pone.0169282
106. Garin N, Koyanagi A, Chatterji S, Tyrovolas S, Olaya B, Leonardi M, et al. Global multimorbidity patterns: a cross-sectional, population-based, multi-country study. J Gerontol Ser Biol Sci Med Sci. (2016) 71:205–14. doi: 10.1093/gerona/glv128
107. dos Santos Costa C, Flores TR, Wendt A, Neves RG, Tomasi E, Cesar JA, et al. Inequalities in multimorbidity among elderly: a population-based study in a city in Southern Brazil. Cad Saude Publica. (2018) 34:e00040718. doi: 10.1590/0102-311x00040718
108. Jackson CA, Dobson AJ, Tooth LR, Mishra GD. Lifestyle and socioeconomic determinants of multimorbidity patterns among mid-aged women: a longitudinal study. PLoS ONE. (2016) 11:e0156804. doi: 10.1371/journal.pone.0156804
109. Diaz E, Poblador-Pou B, Gimeno-Feliu LA, Calderón-Larrañaga A, Kumar BN, Prados-Torres A. Multimorbidity and its patterns according to immigrant origin. A nationwide register-based study in norway. PLoS ONE. (2015) 10:e0145233. doi: 10.1371/journal.pone.0145233
110. Ioakeim-Skoufa I, Poblador-Plou B, Carmona-Pírez J, Díez-Manglano J, Navickas R, Gimeno-Feliu LA, et al. Multimorbidity patterns in the general population: results from the epichron cohort study. Int J Environ Res Public Health. (2020) 17:4242. doi: 10.3390/ijerph17124242
111. Piotrowicz K, Pac A, Skalska A, Mossakowska M, Chudek J, Zdrojewski T, et al. Patterns of multimorbidity in 4588 older adults: implications for a nongeriatrician specialist. Pol Arch Intern Med. (2021) 131:16128. doi: 10.20452/pamw.16128
112. Kirchberger I, Meisinger C, Heier M, Zimmermann AK, Thorand B, Autenrieth CS, et al. Patterns of multimorbidity in the aged population. Results from the KORA-Age study. PLoS ONE. (2012) 7:e30556. doi: 10.1371/journal.pone.0030556
113. Jovic D, Vukovic D, Marinkovic J. Prevalence and patterns of multi-morbidity in Serbian adults: a cross-sectional study. PLoS ONE. (2016) 11:e0148646. doi: 10.1371/journal.pone.0148646
114. Schäfer I, Hansen H, Schön G, Höfels S, Altiner A, Dahlhaus A, et al. The influence of age, gender and socio-economic status on multimorbidity patterns in primary care. First results from the multicare cohort study. BMC Health Serv Res. (2012) 12:89. doi: 10.1186/1472-6963-12-89
115. Rivera-Almaraz A, Manrique-Espinoza B, Ávila-Funes JA, Chatterji S, Naidoo N, Kowal P, et al. Disability, quality of life and all-cause mortality in older Mexican adults: association with multimorbidity and frailty. BMC Geriatr. (2018) 18:236. doi: 10.1186/s12877-018-0928-7
116. Seeley JR, Kosty DB, Farmer RF, Lewinsohn PM. The modeling of internalizing disorders on the basis of patterns of lifetime comorbidity: associations with psychosocial functioning and psychiatric disorders among first-degree relatives. J Abnorm Psychol. (2011) 120:308–21. doi: 10.1037/a0022621
117. Lenzi J, Avaldi VM, Rucci P, Pieri G, Fantini MP. Burden of multimorbidity in relation to age, gender and immigrant status: a cross-sectional study based on administrative data. BMJ Open. (2016) 6:e012812. doi: 10.1136/bmjopen-2016-012812
118. Gu J, Chao J, Chen W, Xu H, Wu Z, Chen H, et al. Multimorbidity in the community-dwelling elderly in urban China. Arch Gerontol Geriatr. (2017) 68:62–7. doi: 10.1016/j.archger.2016.09.001
119. Poblador-Plou B, Van Den Akker M, Vos R, Calderón-Larrañaga A, Metsemakers J, Prados-Torres A. Similar multimorbidity patterns in primary care patients from two European regions: results of a factor analysis. PLoS ONE. (2014) 9:e100375. doi: 10.1371/journal.pone.0100375
120. Yu J, Li Y, Zheng Z, Jia H, Cao P, Qiangba Y, et al. Analysis of multimorbidity networks associated with different factors in Northeast China: a cross-sectional analysis. BMJ Open. (2021) 11:e051050. doi: 10.1136/bmjopen-2021-051050
121. Roth JA, Sakoparnig T, Gerber M, Hug BL, Abshagen C, Fucile G, et al. Bayesian networks to identify potential high-risk multimorbidity and intervention clusters in inpatients: an explorative data mining study. Swiss Med Wkly. (2020) 150:w20299. doi: 10.4414/smw.2020.20299
122. Kalgotra P, Sharda R, Croff JM. Examining health disparities by gender: a multimorbidity network analysis of electronic medical record. Int J Med Inf . (2017) 108:22–8. doi: 10.1016/j.ijmedinf.2017.09.014
123. Kalgotra P, Sharda R, Croff JM. Examining multimorbidity differences across racial groups: a network analysis of electronic medical records. Sci Rep. (2020) 10:13538. doi: 10.1038/s41598-020-70470-8
124. Cavallo P, Pagano S, De Santis M, capobianco E. General practitioners records are epidemiological predictors of comorbidities: an analytical cross-sectional 10-year retrospective study. J Clin Med. (2018) 7:184. doi: 10.3390/jcm7080184
125. Yu J, Song F, Li Y, Zheng Z, Jia H, Sun Y, et al. Multimorbidity analysis of 13 systemic diseases in northeast China. Int J Environ Res Public Health. (2020) 17:1817. doi: 10.3390/ijerph17061817
126. Lee Y, Kim H, Jeong H, Noh Y. Patterns of multimorbidity in adults: an association rules analysis using the Korea health panel. Int J Environ Res Public Health. (2020) 17:2618. doi: 10.3390/ijerph17082618
127. Chmiel A, Klimek P, Thurner S. Spreading of diseases through comorbidity networks across life and gender. New J Phys. (2014) 16:115013. doi: 10.1088/1367-2630/16/11/115013
128. Janssen DJA, Rechberger S, Wouters EFM, Schols JMGA, Johnson MJ, Currow DC, et al. Clustering of 27,525,663 death records from the united states based on health conditions associated with death: an example of big health data exploration. J Clin Med. (2019) 8:922. doi: 10.3390/jcm8070922
129. Hassaine A, Canoy D, Solares JRA, Zhu Y, Rao S, Li Y, et al. Learning multimorbidity patterns from electronic health records using non-negative matrix factorisation. J Biomed Inform. (2020) 112:103606. doi: 10.1016/j.jbi.2020.103606
130. Almagro P, Ponce A, Komal S, De La Asunción Villaverde M, Castrillo C, Grau G, et al. Multimorbidity gender patterns in hospitalized elderly patients. PLoS ONE. (2020) 15:e0227252. doi: 10.1371/journal.pone.0227252
131. Chen N, Zhou L, Huang J, Yu W, Chen C, Jin H, et al. Identifying multimorbidity patterns of non-communicable diseases in paediatric inpatients: a cross-sectional study in Shanghai, China. BMJ Open. (2021) 11:e042679. doi: 10.1136/bmjopen-2020-042679
132. Cassell A, Edwards D, Harshfield A, Rhodes K, Brimicombe J, Payne R, et al. The epidemiology of multimorbidity in primary care: a retrospective cohort study. Br J Gen Pract. (2018) 68:e245–51. doi: 10.3399/bjgp18X695465
133. Wister A. Social determinants and health behaviours among older adults experiencing multimorbidity using the canadian longitudinal study on aging. Can J Aging / La Rev Can du Vieil. (2022) 41:327–47. doi: 10.3389/fpubh.2022.896312
134. Hsu CW, Wang LJ, Lin PY, Hung CF, Yang YH, Chen YM, et al. Differences in psychiatric comorbidities and gender distribution among three clusters of personality disorders: a nationwide population-based study. J Clin Med. (2021) 10:3294. doi: 10.3390/jcm10153294
135. Violán C, Bejarano-Rivera N, Foguet-Boreu Q, Roso-Llorach A, Pons-Vigués M, Martin Mateo M, et al. The burden of cardiovascular morbidity in a European Mediterranean population with multimorbidity: a cross-sectional study. BMC Fam Pract. (2016) 17:150. doi: 10.1186/s12875-016-0546-4
136. Souza DLB, Oliveras-Fabregas A, Minobes-Molina E, de Camargo Cancela M, Galbany-Estragués P, Jerez-Roig J. Trends of multimorbidity in 15 European countries: a population-based study in community-dwelling adults aged 50 and over. BMC Public Health. (2021) 21:76. doi: 10.1186/s12889-020-10084-x
137. Excoffier S, Herzig L, N'Goran AA, Déruaz-Luyet A, Haller DM. Prevalence of multimorbidity in general practice: a cross-sectional study within the Swiss Sentinel Surveillance System (Sentinella). BMJ Open. (2018) 8:e019616. doi: 10.1136/bmjopen-2017-019616
138. Rosellini AJ, Szentkúti P, Horváth-Puhó E, SmithML, Galatzer-Levy I, Lash TL, et al. Latent classes of posttraumatic psychiatric comorbidity in the general population. J Psychiatr Res. (2021) 136:334–2. doi: 10.1016/j.jpsychires.2021.02.013
139. Ng SK, Tawiah R, Sawyer M, Scuffham P. Patterns of multimorbid health conditions: a systematic review of analytical methods and comparison analysis. Int J Epidemiol. (2018) 47:1687–704. doi: 10.1093/ije/dyy134
140. Rajoo SS, Wee ZJ, Lee PSS, Wong FY, Lee ES. A systematic review of the patterns of associative multimorbidity in Asia. BioMed Res Int. (2021) 2021:6621785. doi: 10.1155/2021/6621785
141. Makovski TT, Schmitz S, Zeegers MP, Stranges S, van den Akker M. Multimorbidity and quality of life: systematic literature review and meta-analysis. Ageing Res Rev. (2019) 53:100903. doi: 10.1016/j.arr.2019.04.005
142. McGilton KS, Vellani S, Yeung L, Chishtie J, Commisso E, Ploeg J, et al. Identifying and understanding the health and social care needs of older adults with multiple chronic conditions and their caregivers: a scoping review. BMC Geriatr. (2018) 18:231. doi: 10.1186/s12877-018-0925-x
143. Feng X, Kelly M, Sarma H. The association between educational level and multimorbidity among adults in Southeast Asia: a systematic review. PLoS ONE. (2021) 16:e0261584. doi: 10.1371/journal.pone.0261584
144. Wang Z, Peng W, Li M, Li X, Yang T, Li C, et al. Association between multimorbidity patterns and disability among older people covered by long-term care insurance in Shanghai, China. BMC Public Health. (2021) 21:418. doi: 10.1186/s12889-021-10463-y
145. Alvarez-Galvez J, Carretero-Bravo J, Suarez-Lledo V, Ortega-Martin E, Ramos-Fiol B et al. Social inequalities in multimorbidity patterns in Europe: a multilevel latent class analysis using the European Social Survey (ESS). SSM Popul Health. (2022) 20:101268. doi: 10.1016/j.ssmph.2022.101268
146. Alvarez-Galvez J, Vegas-Lozano E. Discovery and classification of complex multimorbidity patterns: unravelling chronicity networks and their social profiles. Sci Rep. (2022) 12:20004. doi: 10.1038/s41598-022-23617-8
147. Alshakhs M, Jackson B, Ikponmwosa D, Reynolds R, Madlock-Brown C. Multimorbidity patterns across race/ethnicity as stratified by age and obesity. Sci Rep. (2022) 12:9716. doi: 10.1038/s41598-022-13733-w
148. Noordman J, van Vliet L, Kaunang M, van den Muijsenbergh M, Boland G, van Dulmen S. Towards appropriate information provision for and decision-making with patients with limited health literacy in hospital-based palliative care in Western countries: a scoping review into available communication strategies and tools for healthcare providers. BMC Palliat Care. (2019) 18:37. doi: 10.1186/s12904-019-0421-x
Keywords: multimorbidity, comorbidity, chronic conditions, chronicity, social determinants, behavioral determinants
Citation: Álvarez-Gálvez J, Ortega-Martín E, Carretero-Bravo J, Pérez-Muñoz C, Suárez-Lledó V and Ramos-Fiol B (2023) Social determinants of multimorbidity patterns: A systematic review. Front. Public Health 11:1081518. doi: 10.3389/fpubh.2023.1081518
Received: 27 October 2022; Accepted: 02 March 2023;
Published: 27 March 2023.
Edited by:
Cyrille Delpierre, INSERM U1027 Epidémiologie et analyses en santé publique: Risques, Maladies Chroniques et Handicap, FranceReviewed by:
Rubén López-Bueno, University of Zaragoza, SpainCopyright © 2023 Álvarez-Gálvez, Ortega-Martín, Carretero-Bravo, Pérez-Muñoz, Suárez-Lledó and Ramos-Fiol. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Esther Ortega-Martín, ZXN0aGVyLm9ydGVnYUB1Y2EuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.