
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Public Health, 04 August 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1079042
This article is part of the Research TopicVector-borne diseases and consequences on human health: a multidisciplinary approachView all 12 articles
 Manuel Calvopiña1*
Manuel Calvopiña1* María Montesdeoca-Andrade2
María Montesdeoca-Andrade2 Carlos Bastidas-Caldes3,4Sandra Enriquez5
Carlos Bastidas-Caldes3,4Sandra Enriquez5 Richar Rodríguez-Hidalgo5,6Dayana Aguilar-Rodríguez7Philip Cooper7,8
Richar Rodríguez-Hidalgo5,6Dayana Aguilar-Rodríguez7Philip Cooper7,8Babesiosis is a protozoan disease acquired by the bite of different species of ticks. More than 100 Babesia spp. infect wild and domestic animals worldwide, but only a few have been documented to infect humans. Generally, babesiosis is asymptomatic in immunocompetent persons; however, in immunocompromised can be life-threatening. A 13-year-old boy from the Amazon region presented with a 3-month evolution of fever, chills, general malaise, and arthralgia accompanied by anemia and jaundice. In the last 4 years was diagnosed with chronic kidney failure. By nested-PCR using 18S RNA ribosomal gene as target and DNA sequencing, the phylogenetic analysis showed Babesia bigemina as the causative agent in the blood. Treatment with oral quinine plus clindamycin for six continuous weeks was effective with no relapse occurring during 12 months of follow-up. This is the second human case in Ecuador but the first caused by the zoonotic B. bigemina which confirms the existence of active transmission that should alert public health decision-making authorities on the emergence of this zoonosis and the need for research to determine strategies to reduce tick exposure.
Babesiosis is an emerging tick-borne zoonosis with a worldwide distribution. The number of reported human cases in the literature has increased over recent years, indicating an extension of risk areas (1). Human infections are caused by some species of Babesia, that include but are not limited to B. microti, B. divergens, B. duncani, B. motasi, B. crassa, and two Babesia strains, i.e., Babesia spp. KO1 and Babesia spp. CN1; the latter two may represent a new Babesia species (1, 2). The predominant species causing human infections in the North America is B. microti, in Europe it is B. divergens, while in Asia several cases with B. microti, B. venatorum, and B. crassa-like have been reported (3). Other species, such as B. microti Kobe-type, B. microti-like, and some B. divergens–like parasites, have also been implicated in human infections (1, 2, 4). There are rare cases where Babesia spp. that normally infect cattle and other animals, cause disease in humans especially if they are asplenic or immunocompromised (5).
Few human cases have been diagnosed from South America. There were two from Brazil without molecular identification of the Babesia spp. (6). In Colombia in 2003, the first parasitological confirmed case was reported by B. bovis, along with three serological positive cases for B. bovis and one for B. bigemina (7). In a subsequent study, using PCR, four asymptomatic cases due to B. bovis and two of B. bigemina were detected (8). However, both reports have been disputed given a lack of more definitive evidence from DNA sequencing (9). In a study in Bolivia, 3.3% of persons were positive for B. microti by microscopy and PCR, while seroprevalence was 45.7% (2). A traveler from Uruguay to Spain presented mild symptoms due to B. microti infection (10). The only symptomatic case reported to have originated in Ecuador and diagnosed in USA was caused by B. microti (11).
Ecuador, located in the northwest of South America, is crossed by the Andes belt that divide into three ecoregions: the Andean temperate region, the Pacific Coast tropical region, and the interior tropical Amazon basin. Non-continental Ecuador includes the Galápagos Islands at 1,369 km from the Pacific coast. Babesiosis in cattle is considered endemic and is a national veterinary public health problem where the main tick vector is the Rhipicephalus microplus, a species widely distributed in the tropics, subtropics and Andes, between 0 and 2,600 m altitude (12–14). Furthermore, Rh. microplus collected from tropical regions resulted positive for B. bovis, B. bigemina and co-infections (12, 13). At least 41 Ixodid tick species, 32 species of hard ticks (Ixodidae) and 9 species of soft ticks (Argasidae), belonging to Amblyomma, Dermacentor, Haemaphysalis, Ixodes, and Rhipicephalus genera have been documented in Ecuador, including Galapagos Islands (15, 16), with additional species recorded in the Andes region (17).
The clinical manifestations of babesiosis in immunocompetent persons range from asymptomatic to a mild illness. In contrast, severe illness requiring hospital admission is common in persons who are immunosuppressed or splenectomised; or who have cancer, human immunodeficiency virus infection, haemoglobinopathy, or chronic heart, lung, kidney, or liver disease. The severity of babesiosis depends primarily on the immune status of the patient and may cause death (18). With an infection by B. divergens, B. duncani and B. venatorum, there seems to be a higher probability of severe disease (19). After a gradual onset of malaise and fatigue, the most common clinical sign is fever, sometimes as high as 40.9°C (105.6°F), with chills and sweats accompanied by headache, myalgia, anorexia, arthralgia, and nausea. In severe infections, fever may be accompanied by splenomegaly, hepatomegaly, jaundice, and acute respiratory failure (18). Babesiosis is a protozoal infection like malaria, confusing both clinical and laboratory diagnosis, and more so in areas where the two diseases are overlapping (11).
The diagnosis of babesiosis is based on epidemiology and clinical presentation (4). Laboratory findings that are consistent with hemolytic anemia include a low hematocrit, hemoglobin, and haptoglobin levels, but elevated reticulocyte count and lactate dehydrogenase level; thrombocytopenia is commonly observed (18). Because of difficulties in the laboratory identification of Babesia species that have a similar morphology and because of antigenic cross-reactivity, molecular techniques such as PCR and DNA sequencing are often required for species identification (1). DNA sequencing for the phylogenetic analysis of Babesia provides data on nucleotide sequences present in an amplified target gene sequence while PCR generates a large number of copies of a specific DNA fragment, represented as a single band (20). PCR is more sensitive and specific than blood smear (19). Among DNA-based assays, nested-PCR based on 18S RNA small subunit fragment for Babesia species have been used extensively for the diagnosis of babesiosis, and is highly sensitive, even at low levels of parasitemia (21).
Patients with mild to moderate babesiosis are treated with combination therapy of atovaquone and azithromycin, and severe cases with clindamycin plus quinine. Based on multiple case reports, a 7-to-10-day course of clindamycin-quinine combination is often used to treat severe babesiosis (3). A minimum of 6 weeks for highly immunocompromised patients is recommended (21).
Here we report a severe case of babesiosis caused by B. bigemina in an immunocompromised Ecuadorian child from the Amazon basin region who was treated successfully with the combination of clindamycin plus quinine.
A 13-year-old boy, Amerindian of the Shuar ethnic group, was born and raised on a farm located in Guayusa (Lat = −0.24837, Long = −77.06041), province of Orellana, northern part of the Ecuadorian Amazon, 8 hours from Quito, the capital of Ecuador. An important antecedent was that he had suffered from stage 3 chronic kidney disease for the previous 4 years (glomerular filtration rate of 49 mL/min), secondary to an anatomical malformation of the urinary tract. He had never received a blood transfusion. Clinical history revealed that for 3 months the child had presented a clinical picture characterized by a fever of 38 to 39.4°C, accompanied by chills, sweating, anorexia, general malaise, and arthralgia. One month prior to hospital admission, the fever was accompanied by jaundice, initially affecting the sclera and later became generalized, with pain of moderate intensity in the right flank. The child had always resided in the Amazon region where the presence of numerous wild animals including deer (Mazama americana), rodents, and insects such as mosquitoes, sandflies, and ticks are abundant. He was first medically managed with antipyretics and antibiotics in a local health center and provincial hospital. Since the fever did not subside and the clinical picture of kidney failure worsened, he was transferred to a referral hospital in Quito. Upon admission, he had a fever of 38°C, heart rate of 114 beats/min, respiratory rate of 22/min, oxygen saturation of 97%, blood pressure 129/65 mm Hg, weight 35.4 Kg, height 136.5 cm, abdominal pain, arthralgia, myalgia, and urinary incontinence with dark urine. On physical examination, pale skin and mucous membranes were observed, as were multiple scratching excoriations on the lower extremities.
The blood tests revealed a white blood cell count of 19,500 mm3 with 67% neutrophils, 19% lymphocytes, 11% eosinophils, 2% basophils, and 1% monocytes. Hemoglobin 6.3 mg/dL, hematocrit 19.7%, platelets 139,000 mm3, urea 145 mg/dL (12–54 mg/dL), creatinine 3.5 mg/dL (0.7 to 1.2 mg/dL for men), blood urea nitrogen (BUN) 29 mg/dL (7–20 mg/dL), alanine-aminotransferase 64 U/L (4 to 36 U/L) and aspartate aminotransferase 61 U/L (8 to 33 U/L). The direct Coombs test was positive, and lactate dehydrogenase (LDH) was 295 U/L (140 to 280 U/L). Serological studies for human immunodeficiency virus (HIV), viral hepatitis and immunological tests for malaria, Chagas, leptospirosis, and Lyme disease were all negative. Peripheral thick and thin blood smears for Plasmodium spp. and Trypanosoma cruzi were negative. No intraerythrocytic structures compatible with Babesia spp. were observed.
In imaging studies with sonography, hydroureteronephrosis of the right kidney was observed, while the left one was decreased in size with a loss of corticomedullary relationship and ectasia. The right kidney showed the presence of two ureters that ended together ipsilaterally. A bilobed bladder separated by a septum with a paravesical diverticulum was also observed.
Genomic DNA of whole-blood samples was isolated using commercial Qiagen DNA™-blood MiniPrep kit. A nested PCR for the long fragment of 18S rRNA gene for detection of Babesia species were performed. The first PCR step was amplified using the primer set PiroF (5’-GCCAGTAGTC ATATGCTTGTGTTA-3′) and Piro6R (5’-CTCCTTCCTYTAAG TGATAAGGTTCAC-3′). Another pair of primers, Piro1F (5′- CCATGCAGTTCTWAGTAYAARCTTTTA-3′) and Piro5.5R (5’-CCTYTAAGTGATAAGGTTCACAAAACTT-3′) were used in the second PCR (22). In a 2% agarose gel, a clear band of approximately 1,670 bp was observed. The amplicon was sequenced using the Sanger sequencing by an external provider (Macrogen-South Korea). The chromatogram sequence of the gene, obtained with forward and reverse primers, were assembled and consensus sequence was edited using MEGA XI software. The Nucleotide Blast, for the final sequence of 1,546 bp, show a query coverage of 100% and identity of 99.87% for B. bigemina using the NCBI resources and a GenBank accession number was obtained (OQ607820.1). The sequences were aligned and compared using the MEGA XI. A phylogenetic tree was constructed through Neighbor Joining method with a Bootstrap of 500 replicates, comparing eleven NCBI sequences from GenBank (Figure 1). Purified DNA of B. bovis and B. bigemina, kindly supplied by Instituto de Genética de la Universidad Nacional de Colombia, were used as positive controls.
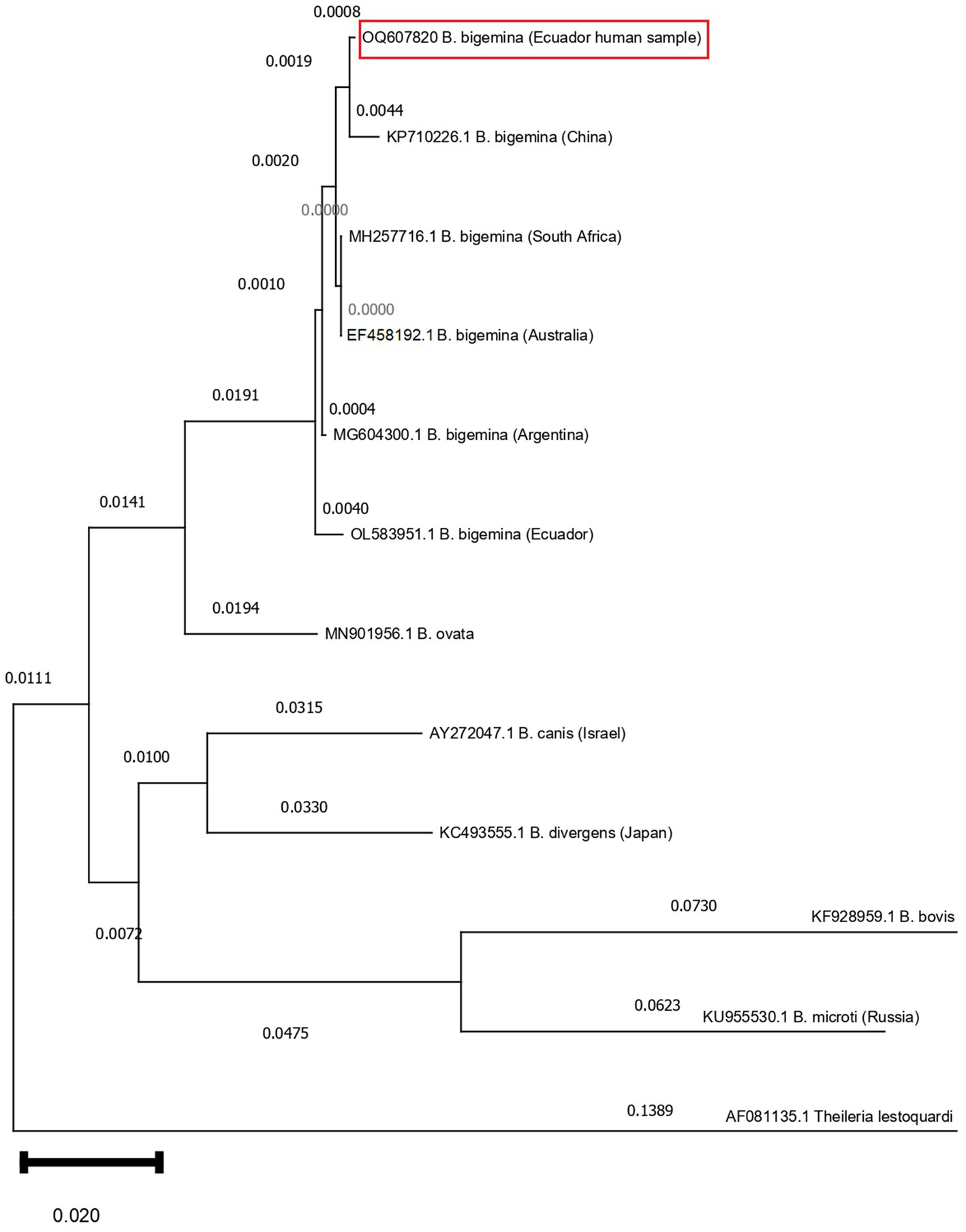
Figure 1. Phylogenetic tree based on the 1,670 nucleotides of the 18S rRNA gene of Babesia bigemina. The optimal tree was inferred using the Neighbor-Joining method. The confidence probability (multiplied by 500) that the interior branch length is greater than 0, as estimated using the bootstrap test (1,000 replicates is shown next to the branches). The evolutionary distances were computed using the Tamura Nei model (distribution of 48 parameters). Patient (Ecuador human sample, GenBank accession number OQ607820) showed identities of 99.35% when compared with published B. bigemina sequences (KP710226.1, MH257716.1, EF458192.1, MG604300.1, OL583951.1). Theileria lestoquardi (AF081135.1) compared as outgroup.
After 32 days of clinical management in the nephrology unit, BUN and creatinine values decreased to 118 mg/dL and 2.2 mg/dL, respectively. Whereas hemoglobin and hematocrit rose to 12.8 mg/dL and 38.8%, respectively. The leukocyte count decreased to 13,400 mm3. Anti-Babesia treatment was started with oral quinine 300 mg every 8 hours plus clindamycin 300 mg every 12 h, which was continued as an outpatient treatment for 6 continuous weeks. No adverse effects were reported to any of the drugs. Symptoms subsided after 7 days of treatment. No symptomatology was reported at 3-, 6- and 12-month controls and no parasitic forms compatible with Babesia were observed in peripheral blood smears. His mother signed the consent for the publication of the case.
Reports of symptomatic cases of human babesiosis worldwide are rare, although in recent years the increased numbers have led experts to consider it as an emerging disease, especially in tropical and subtropical regions (1). The report of this case with severe symptoms in an immunosuppressed boy with the identification of the Babesia specie is important in documenting the geographic distribution of human disease in South America and particularly in Ecuador. This is the second symptomatic case in Ecuador, but the first in the Amazon region with B. bigemina identified as the causative agent using molecular methods (e.g., n-PCR and DNA sequencing). The first case, which came from the tropical Pacific coastal region and diagnosed in the USA, was caused by B. microti (11). This shows that human Babesia infection is present in the two tropical ecoregions of the country.
Most human infections are caused by B. microti and B. divergens and rarely by other species (1, 2, 4, 9). Few human cases by B. bigemina have been reported from Colombia and Ecuador in asymptomatic persons residing in the Amazon (7, 8). However, these cases were not confirmed by DNA sequencing: the use of PCR and or serology cannot confirm the Babesia species with certainty (1, 9, 20, 23). Babesia bigemina is widely distributed geographically and, together with B. bovis, is highly infective in livestock (12, 14). In Ecuador, B. bigemina has been reported to infect cattle and ticks from the tropical regions, as well as the Andean region (12, 13). Therefore, it is imperative to consider B. bigemina as a potential infectious agent which causes severe disease in immunosuppressed patients, as occurred in the present case. We believe that there is underdiagnosis of human babesiosis in Ecuador due to the lack of information among physicians and laboratory technicians, unavailability of sensitive diagnostic tests, and lack of epidemiological studies. Furthermore, there could be a misinterpretation of intra-erythrocytic microorganisms on blood smear with Plasmodium spp. (11) since malaria is endemic in Ecuador (24). There is a report of other febrile illnesses transmitted by ticks in the Amazon such as Rickettsia (25). Therefore, the presence of Babesia infections should be investigated in febrile patients.
The Babesia species that infect cattle and livestock in South America are B. bigemina and B. bovis (2, 26). Using PCR targeting the 18S ribosomal gene in cattle from the Coast and Andes identified both B. bigemina and B. bovis (12). This information indicates that active transmission in domestic animals is occurring with a permanent risk of infection to humans. The main vectors of B. bigemina and B. bovis in cattle are ticks of the genus Rhipicephalus, Rh. sanguineus but mainly Rh. microplus, species widely distributed in the tropics and subtropics of South America (13, 26). Although few studies on ticks exist in the country, several tick species of different genera that could act as potential vectors of B. bigemina and others, have been documented (12, 14, 15, 17).
The severe clinical symptoms of the present case are a consequence of the child being immunosuppressed due to his chronic kidney failure and delay in the diagnosis (18, 19, 21). In the hematological profile, the observed decrease in hemoglobin and hematocrit was most probably due to the hemolytic anemia. Associated laboratory findings, such as thrombocytopenia, elevation of liver and kidney enzyme levels, jaundice, and dark urine a month before hospitalization, are consistent with a Babesia infection confirmed later by nested-PCR and DNA sequencing. In addition, the history of exposure to ticks also supports the diagnosis. No intraerythrocytic forms of Babesia spp. were observed, probably due to it being a chronic infection with 3 months of evolution. In chronic cases, parasites may be undetectable by microscopy, so it is important to use the molecular-based techniques, which detects a specific sequence of the nucleic acids of the parasite (20, 23). Along with the progress in molecular techniques, the knowledge of Babesia is further expanding and more species will probably be discovered.
Because the boy was with severe and chronic infection was treated using the combination of quinine plus clindamycin for 6 weeks, as recommended by the Infectious Diseases Society of America (IDSA) guidelines (3). Clinical symptoms and parasites may relapse in immunocompromised patients despite 7 to 10 days of antimicrobial therapy and may persist for more than a year if the infection is not adequately treated (18, 19, 21). He recovered completely clinical and did not present any adverse reactions during the 12 months of follow-up.
The report of this human case confirms the existence of the disease and active transmission in Ecuador, as well as its wide geographical distribution, should alert human and veterinary physicians and decision-making authorities of the importance of this emerging zoonosis and the needed research to determine preventive and control strategies. Information on the distribution of Babesia species is essential for the diagnosis and prevention of the disease. Unfortunately, surveillance of ticks and tick-borne pathogens do not exist in the country. We recommend strengthening the research capacity in a One Health context in order to develop control strategies that reduce the direct and indirect health and economic burden caused by ticks and tick-borne diseases.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
MC: overall coordination, writing, editing, and revision of manuscript. MM-A: diagnosis and management of patient, writing, and editing of manuscript. CB-C, RR-H, and SE: parasitological and molecular diagnosis, writing, and editing of manuscript. PC and DA-R: molecular diagnosis and editing of the manuscript. All authors read and approved the final manuscript.
This study was supported by Universidad de las Américas (UDLA), Quito, Ecuador.
We greatly thank the mother for consenting to publication of this case report.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Yang, Y, Christie, J, Köster, L, Du, A, and Yao, C. Emerging human Babesiosis with “ground zero” in North America. Microorganisms. (2021) 9:440. doi: 10.3390/microorganisms9020440
2. Gabrielli, S, Totino, V, Macchioni, F, Zuñiga, F, Rojas, P, Lara, Y, et al. Human Babesiosis, Bolivia, 2013. Emerg Infect Dis. (2016) 22:1445–7. doi: 10.3201/eid2208.150195
3. Krause, PJ, Auwaerter, PG, Bannuru, RR, Branda, JA, Falck-Ytter, YT, Lantos, PM, et al. Clinical practice guidelines by the Infectious Diseases Society of America (IDSA): 2020 guideline on diagnosis and Management of Babesiosis. Clin Infect Dis. (2021) 72:185–9. doi: 10.1093/cid/ciab050
4. Kumar, A, O'Bryan, J, and Krause, PJ. The global emergence of human Babesiosis. Pathogens. (2021) 10:1447. doi: 10.3390/pathogens10111447. Erratum in: Pathogens. 2022 May 23;11(5): Erratum in: Pathogens. 2022 Aug 17;11(8)
5. Hunfeld, K, Hildebrandt, A, and Gray, J. Babesiosis: recent insights into an ancient disease. Int J Parasitol. (2008) 38:1219–37. doi: 10.1016/j.ijpara.2008.03.001
6. Rech, A, Bittar, CM, de Castro, CG, Azevedo, KR, dos Santos, RP, Machado, ARL, et al. Asymptomatic Babesiosis in a child with Hepatoblastoma. J Pediatr Hematol Oncol. (2004) 26:213. doi: 10.1097/00043426-200403000-00015
7. Ríos, L, Alvarez, G, and Blair, S. Serological and parasitological study and report of the first case of human babesiosis in Colombia. Rev Soc Bras Med Trop. (2003) 36:493–8. doi: 10.1590/S0037-86822003000400010
8. Gonzalez, J, Echaide, I, Pabón, A, Gabriel Piñeros, JJ, Blair, S, and Tobón-Castaño, A. Babesiosis prevalence in malaria-endemic regions of Colombia. J Vector Borne Dis. (2018) 55:222. doi: 10.4103/0972-9062.249480
9. Silva-Ramos, CR, and Faccini-Martínez, ÁA. Call for Caution to Consider Babesia bovis and Babesia bigemina as Anthropozoonotic Agents in Colombia. Comment on Kumar et al. The Global Emergence of Human Babesiosis. Pathogens 2021, 10, 1447. Pathogens. (2022) 11:263. doi: 10.3390/pathogens11020263
10. Arsuaga, M, Gonzalez, LM, Lobo, CA, de la Calle, F, Bautista, JM, Azcárate, IG, et al. First report of Babesia microti -caused Babesiosis in Spain. Vector-Borne Zoonotic Dis. (2016) 16:677–9. doi: 10.1089/vbz.2016.1946
11. Al Zoubi, M, Kwak, T, Patel, J, Kulkarni, M, and Kallal, CA. Atypical challenging and first case report of babesiosis in Ecuador. IDCases. (2016) 4:15–7. doi: 10.1016/j.idcr.2016.02.003
12. Chávez-Larrea, MA, Cholota-Iza, C, Medina-Naranjo, V, Yugcha-Díaz, M, Ron-Román, J, Martin-Solano, S, et al. Detection of Babesia spp. in high altitude cattle in Ecuador, possible evidence of the adaptation of vectors and diseases to new climatic conditions. Pathogens. (2021) 10:1593. doi: 10.3390/pathogens10121593
13. OIE . (2023). Organización Mundial de Sanidad Animal. Capitulo 3.4.2. Babesiosis bovina. Manual de las Pruebas de Diagnóstico y de las Vacunas para los Animales Terrestres para los Animales Terrestres 2021. Actualizacion. Available at: https://www.oie.int/es/que-hacemos/normas/codigos-y-manuales/acceso-en-linea-al-manual-terrestre/ (Accessed February 10, 2023).
14. Rodríguez-Hidalgo, R, Pérez-Otáñez, X, Garcés-Carrera, S, Vanwambeke, SO, Madder, M, and Benítez-Ortiz, W. The current status of resistance to alpha-cypermethrin, ivermectin, and amitraz of the cattle tick (Rhipicephalus microplus) in Ecuador. PLoS One. (2017) 12:652. doi: 10.1371/journal.pone.0174652
15. Enríquez, S, Guerrero, R, Arrivillaga-Henríquez, J, Araujo, P, Villacrés, E, Enríquez, A, et al. New Records of Ticks of genus Amblyomma Koch, 1844 (Acari: Ixodidae) for Ecuador. Acta Parasitol. (2020) 65:430–40. doi: 10.2478/s11686-020-00173-7
16. Dusbábek, FAA, Guglielmone, A, Estrada-Peña, JE, and Keirans, RG. Robbins: ticks (Acari: Ixodida) of the Neotropical zoogeographic region. Folia Parasitol (Praha). (2004) 51:375–5. doi: 10.14411/fp.2004.048
17. Pesquera, C, Portillo, A, Palomar, AM, and Oteo, JA. Investigation of tick-borne bacteria (Rickettsia spp., Anaplasma spp., Ehrlichia spp. and Borrelia spp.) in ticks collected from Andean tapirs, cattle and vegetation from a protected area in Ecuador. Parasit Vectors. (2015) 8:46. doi: 10.1186/s13071-015-0662-3
18. Vannier, E, and Krause, PJ. Human Babesiosis. N Engl J Med. (2012) 366:2397–407. doi: 10.1056/NEJMra1202018
19. Anettová, L, and Kazimírová, M. Human Babesiosis: Ecoepidemiology, diagnosis and treatment. In: Vector-Borne Diseases & Treatment. eds. A Alberti, L Falsone G Faviav (Cambridge: Open Access Book). (2019). 29.
20. Criado-Fornelio, A, Martinez-Marcos, A, Buling-Saraña, A, and Barba-Carretero, JC. Molecular studies on Babesia, Theileria and Hepatozoon in southern Europe. Part II. Phylogenetic analysis and evolutionary history. Vet Parasitol. (2003) 114:173–94. doi: 10.1016/S0304-4017(03)00141-9
21. Sanchez, E, Vannier, E, Wormser, GP, and Hu, LT. Diagnosis, treatment, and prevention of Lyme disease, human granulocytic Anaplasmosis, and Babesiosis. JAMA. (2016) 315:1767. doi: 10.1001/jama.2016.2884
22. Liu, J, Guan, G, Li, Y, Liu, A, Luo, J, and Yin, H. A molecular survey of Babesia species and detection of a new Babesia species by DNA related to B. venatorum from white yaks in Tianzhu, China. Front Microbiol. (2017) 8:419. doi: 10.3389/fmicb.2017.00419
23. Mtshali, MS, and Mtshali, PS. Molecular diagnosis and phylogenetic analysis of Babesia bigemina and Babesia bovis hemoparasites from cattle in South Africa. BMC Vet Res. (2013) 9:154. doi: 10.1186/1746-6148-9-154
24. MSP . (2019). Diagnóstico y Tratamiento de Malaria Acuerdo 0346–2019. Available at: https://www.salud.gob.ec/catalogo-de-normas-politicas-reglamentos-protocolos-manuales-planes-guias-y-otros-del-msp/ (Accessed January 18, 2023).
25. de Bravo, NB, Smalligan, RD, Russell, KL, Manock, SR, Espín, JF, Jacobsen, KH, et al. Etiology of acute undifferentiated febrile illness in the Amazon basin of Ecuador. Am J Trop Med Hyg. (2009) 81:146–51. doi: 10.4269/ajtmh.2009.81.146
Keywords: babesiosis, Babesia bigemina , case report, zoonosis, tick-borne, Ecuador, Amazon
Citation: Calvopiña M, Montesdeoca-Andrade M, Bastidas-Caldes C, Enriquez S, Rodríguez-Hidalgo R, Aguilar-Rodríguez D and Cooper P (2023) Case report: First report on human infection by tick-borne Babesia bigemina in the Amazon region of Ecuador. Front. Public Health. 11:1079042. doi: 10.3389/fpubh.2023.1079042
Edited by:
Abdulaziz Alouffi, King Abdulaziz City for Science and Technology, Saudi ArabiaReviewed by:
Hayley Danielle Yaglom, Translational Genomics Research Institute, United StatesCopyright © 2023 Calvopiña, Montesdeoca-Andrade, Bastidas-Caldes, Enriquez, Rodríguez-Hidalgo, Aguilar-Rodríguez and Cooper. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manuel Calvopiña, bWFudWVsLmNhbHZvcGluYUB1ZGxhLmVkdS5lYw==; bWFudWVsY2Fsdm9waW5hQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.