
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 07 February 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1078023
 Md. Ashraful Islam1*
Md. Ashraful Islam1* Dhfer Mahdi Alshayban1
Dhfer Mahdi Alshayban1 Atta Abbas Naqvi2
Atta Abbas Naqvi2 Muhammad Bilal Maqsood3
Muhammad Bilal Maqsood3 Azfar Athar Ishaqui4Muhammad Kashif5Majid Ali6
Azfar Athar Ishaqui4Muhammad Kashif5Majid Ali6 Abdul Haseeb7
Abdul Haseeb7Aim: The study aimed to document the anxiety attributed to COVID-19, disease knowledge, and intention to vaccinate against the disease in general public. Moreover, the interplay among these three outcomes was also investigated.
Methods: A cross-sectional study was conducted for 2 months in three cities of Dammam Region of Saudi Arabia. The target segment was the adult population of Saudi Arabia. Convenience sampling was used and all adults aged ≥18 were invited to participate. The questionnaire used in the study was available in both Arabic and English languages. It included a demographic section, a section dedicated to vaccination intention and, a section containing coronavirus anxiety scale (CAS). The data analysis was carried out using IBM SPSS version 23. The study was approved by an ethics committee (IRB-2021-05-297).
Results: A total of 542 responses were analyzed. Most respondents had no anxiety attributed to COVID-19 (92.1%), self-reported good knowledge of COVID-19 (79.7%) and intended to administer a vaccine (57.4%). Age groups 18–29 years and 30–45 years, and having a chronic medical condition, were found to be determinants of having COVID-19 anxiety (p < 0.05). The variables of self-rated good knowledge of disease, never contracted COVID-19, and incomes of SAR 5,000 (i.e., USD 1333), and SAR 7,500–10,000 (i.e., USD 1999.5–2666), were found to be determinants of having positive intention toward vaccination (p < 0.05).
Conclusion: The anxiety due to COVID-19 was present in a few participants. Besides, self-reported knowledge about COVID-19 and intention to administer a vaccine, were positively linked to each other. However, both variables had no effect on COVID-19 anxiety. It is important to review and address the determinants of positive intention to further increase vaccine acceptance rate.
Since March 2020, the world is in the midst of COVID-19 pandemic (1). Since then the virus has been evolving and several new variants of the virus that have high transmission and capability to spread have been reported (2–4). Besides, the daily reporting of new cases and deaths due attributable to COVID-19 was a common occurrence in the news media (5). Such news reports and emotive information propagated a sense of fear and anxiety among the general masses, and it may be linked to anxiety and psychological distress (5, 6). It was also reported that the disease had an effect on social relationships (7).
A study mentions that an individual may respond to fear either rationally or irrationally. A person may respond to the fear of COVID-19 by understanding the threat and preventing the risk (6). However, an irrational response to the fear would be to panic. This may limit the ability of an individual to understand the threat. Moreover, providing more information about the scientifically authentic threat may trigger more panic which would reduce the benefits of the information to the individual (6). As this impact of media information on mental health is observed in this crisis, the WHO has termed this phenomenon as “infodemic.” The term implies that there might be an over-profusion of some reliable and anecdotal information available to the public that makes it difficult to find reliable information at the time of need (5, 8). It was reported that media coverage of the COVID-19 crisis also resulted in stress in the public (5). This sense of fear and panic is detrimental to the mental health of an individual which was already affected due to the containment strategy of lockdowns (9).
During the COVID-19 pandemic, fear of job insecurity was a significant reason for financial anxiety regardless of the employment sector and income among employees in Saudi Arabia (10).
A possible way to reduce occurrence of new COVID-19 infections is through vaccination. This would instigate an immune response in the body and may significantly reduce the likelihood of spread (11). It offers a potential solution to exiting the current crisis (12). A large-scale vaccination drive against COVID-19 is considered as a successful response by the public health authorities in the UK, to address the spread of this viral infection in future (13). A number of vaccine candidates have shown efficacy in clinical trials and have been approved for use in public recently (11, 14, 15).
Saudi health authority approved the first vaccine for the disease as early as December 2020 and started administering vaccines in January 2021. Later in February 2021, the second vaccine was approved for use (16). Initially, large urban centers such as provincial capitals were prioritized for the delivery of vaccines. The vaccine-eligible population was divided into three strata. The first stratum comprised of the healthcare practitioners, geriatrics, military personnel, immune-compromised, obese individuals, and patients with certain chronic diseases. The second stratum comprised of individuals who worked in essential services along with patients with chronic diseases. Both strata had individuals with high risk of COVID-19 and its complications and therefore, were prioritized to receive a vaccine by July 2021. The general public was in the third stratum and was prioritized to be vaccinated by September 2021 (17).
However, how anxious the general public is due to COVID-19 infection, their level of awareness and the intention to vaccinate against the viral infection needs to be seen. In addition, it is worthwhile documenting how these three factors affect each other and the overall vaccination intention.
The study aimed to report the anxiety attributed to COVID-19, self-rated disease knowledge, and intention to vaccinate against the disease among general public. Moreover, the interplay among these three outcomes was also investigated.
This study was designed as a cross-sectional survey and was conducted for 2 months, i.e., September–October 2021 in three cities of the Dammam Region of Saudi Arabia.
The target segment was the adult population. Adult male and female participants who aged 18 and above and eligible for a vaccine, were invited to participate in this study. Incomplete responses were excluded from study.
The data was collected using a convenient sampling method. Participants who could be conveniently approached were contacted. The mode of survey was physical as well as online. Both forms were available as per the convenience of participants. The online survey was conducted using an electronic tablet, while the hardcopies were handed to participants and later collected. The venues selected were mostly open public spaces such as public parks and open areas of shopping malls. The data was collected once per participant and there was no follow-up.
The sample size was calculated using an online sample size calculator. Dammam Region consists of several cities. Our study included cities namely Dammam, Dhahran, and Khobar. According to available estimates at the time of this writing, the population of Dammam city was 7,68,602 while Dhahran and Khobar had a population of 99,540 and 1,65,799 respectively (18). Since there was no description of numbers related to the vaccine eligible population, the sum of all three figures, i.e., population of 1,033,941 individuals, was considered the total population of these cities and thus, our target population.
The sample size was calculated using a margin of error of 5% and a confidence interval of 97.5%. From the initial calculation, the number of samples obtained was 503 (19). Later, the sample size was adjusted for non-response/missing error rate which was considered at 20%. Finally, the required sample size turned to 629.
The research questionnaire consisted of a demographic section, a section dedicated to vaccination intention and, a section containing Coronavirus Anxiety Scale (CAS) (20). The demographic section contained questions related to the age, sex, nationality, education level, marital status, occupation, residence, and income. The second section contained items related to the participants' medical history, any exposure to COVID-19, self-rated knowledge about COVID-19, level of compliance to recommendations aimed at preventing COVID-19 spread, and vaccination intention. The third section was CAS itself, a validated scale to measure anxiety related to the disease. The scale contained 4 items related to the COVID-19 anxiety on a person's daily life in last 14 days. The scale was Likert-format, and each item had 5 possible options. Each options awarded a score. A cumulative score of ≥ 9 indicated COVID-19 anxiety (20).
A formal permission was obtained from the developer of the scale through email. The questionnaire was formulated in native Arabic and English languages. The CAS scale was already available in both English and Arabic languages at the time of study. The survey was piloted in few participants before actual study.
Data were checked for incomplete and missing responses. At the beginning 558 responses were received and 71 samples of incomplete responses were excluded from the data set. Of 23 partially incomplete responses, 16 were excluded due to untreatable nature, whereas 7 (seven) responses were treated using the “last observation carried forward” statistical method. Finally, a total of 542 complete responses were analyzed. The potential sources of bias considered during this study were selection bias due to the convenient sampling, and information bias attributed to the self-reporting format of this study. The study outcomes were the intention to vaccinate and COVID-19 anxiety. A secondary outcome considered was COVID-19 self-reported knowledge.
The data were coded and entered for analysis in IBM SPSS version 23. The demographic data was reported using sample counts (N) and percentages (%) for descriptive data. Simple and multiple logistic regression methods were used to report the determinants of the outcomes. Only the significant variables were included in the multiple regression model. The significance of those variables was determined by simple regression analysis and necessary model fitness parameters were checked by required statistics that are mentioned in footnotes of Tables 4–6.
The participants were briefed about the study and their consent was sought. The participation was voluntary. An electronic informed consent was designed and was shown at the front page of the online survey, and it was also available in hardcopy. The participants in the online survey could only access the survey if they consent to participate while those who preferred the hardcopy were asked to provide their consent before accessing the survey. The nature of consent was implied, i.e., participants were not required to provide their personal identifiable details. The study was approved by the Institutional Review Board of Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia (IRB -2021-05-297).
A total of 542 responses were analyzed.
Most respondents were female (N = 352, 64.9%) and aged between 18 and 29 years (N = 306, 56.5%). Most of them were Saudi nationals (N = 513, 94.6%), students (N = 219, 40.4%), resided in urban area (N = 457, 84.3%) and had postgraduate qualification (N = 230, 42.4%). Slightly less than half (N = 237, 43.7%) had a monthly family income above Saudi Arabian Riyal (SAR) 10,000, i.e., > United States Dollar (USD) 2666, (Table 1).
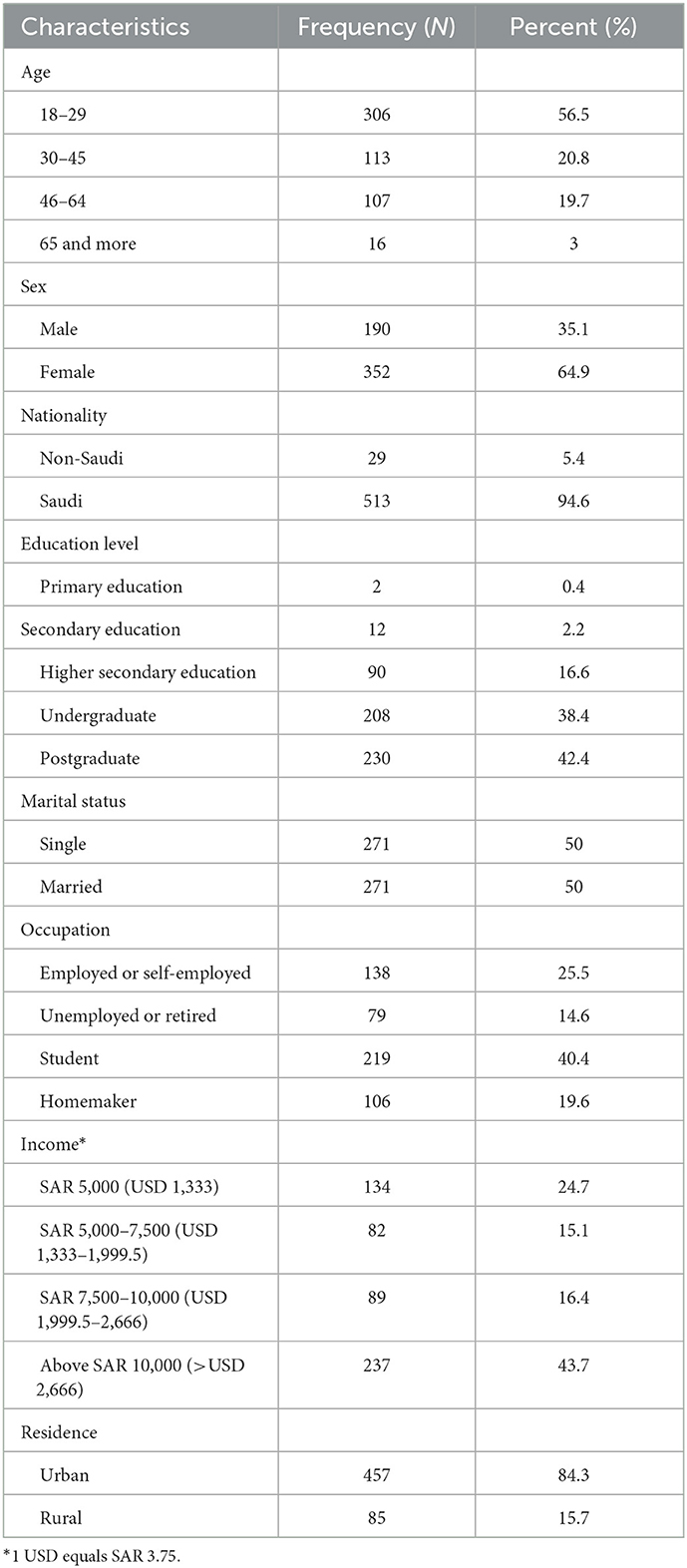
Table 1. Background characteristics of participants (N = 542).
Most participants did not have any chronic illnesses (N = 449, 82.8%) and mental illnesses (N = 492, 90.8%). More than half of participants rated their knowledge of COVID-19 as good (N = 304, 56.1%). The majority did not suffer from COVID-19 (N = 458, 84.5%) however, had COVID-19 patients in their family (N = 469, 86.5%). Most of the participants never missed a doctor recommended vaccine (N = 508, 93.7%) and intended to vaccinate against COVID-19 (N = 311, 57.4%) (Table 2).
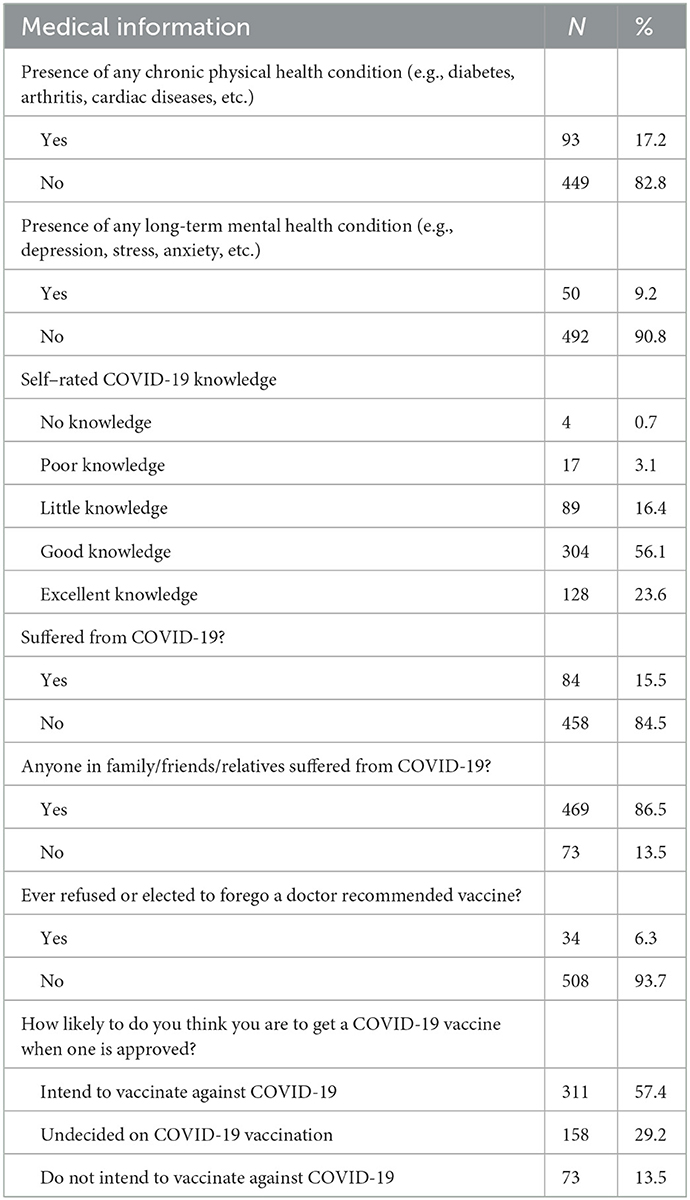
Table 2. Medical information of participants (N = 542).
Slightly less than half of the participants mentioned that they follow the recommendations from authorities regarding COVID-19 prevention at most times (Figure 1).
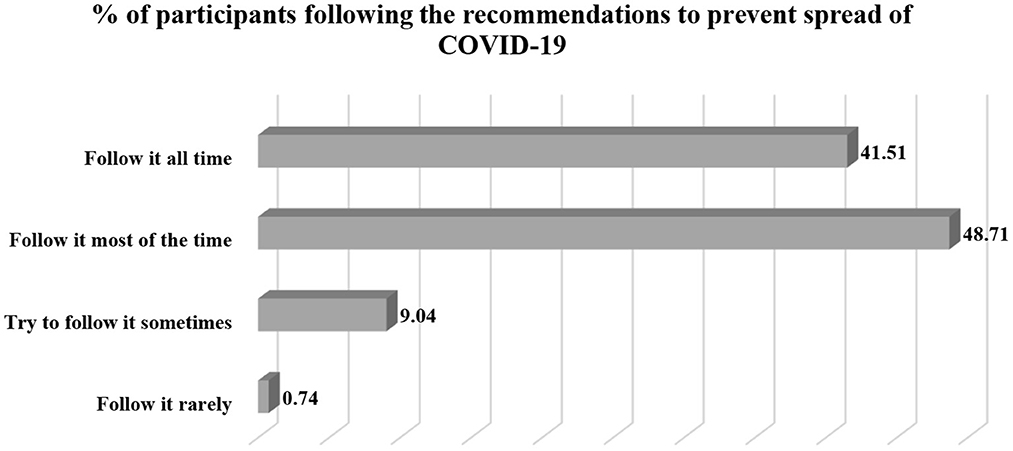
Figure 1. Percentage distribution of participants regarding compliance to COVID-19 prevention guidelines.
The majority reported an acceptable level of knowledge of COVID-19 viral infection (N = 432, 79.7%). More than half of the participants had positive intent regarding COVID-19 vaccination (N = 311, 57.4%). Most of them had no anxiety attributed to COVID-19 (N = 499, 92.1%). The reliability of the Coronavirus Anxiety Scale (CAS) was 0.845, i.e., Cronbach's alpha value (Table 3).
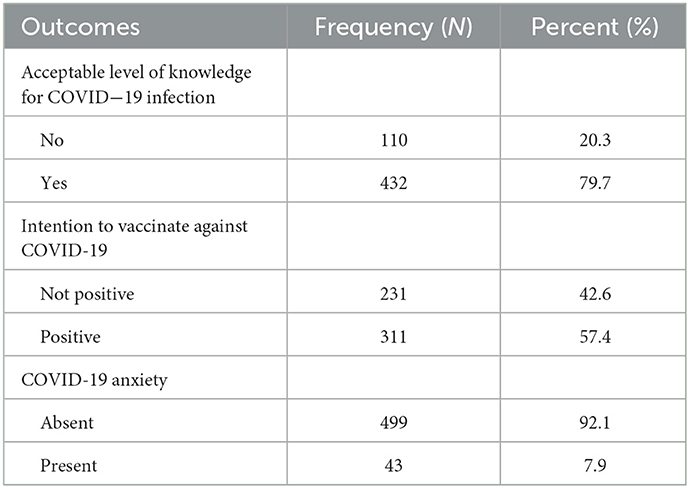
Table 3. Characteristics of outcome variables (N = 542).
The model for COVID-19 anxiety highlighted those individuals in age groups 18–29 and 30–45 years were more likely to have COVID-19 anxiety, i.e., (AOR 5.33) and (AOR 6.48), respectively, compared to individuals aged 46 years and above, when adjusted for other demographics (p < 0.05). Besides, individuals who mentioned having any long-term mental health condition were roughly three times more likely to have COVID-19 anxiety (AOR 2.66) compared to those without any mental illness when other demographics are considered (p < 0.05). Some of the variables were significant determinants of COVID-19 anxiety alone and became non-significant when adjusted for all different demographics (Table 4).
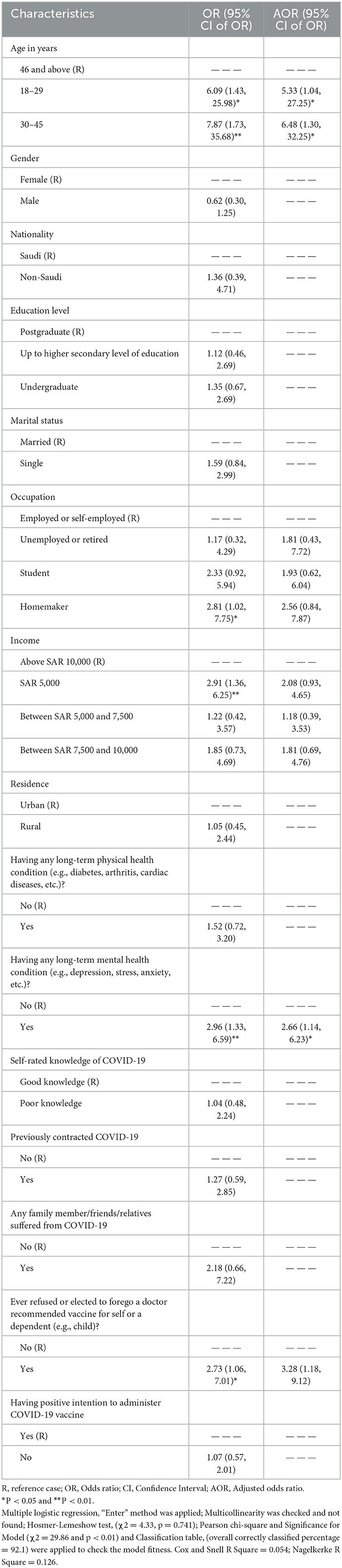
Table 4. Determinants of COVID-19 anxiety.
The model for a positive intention toward COVID-19 vaccination reported that compared to the females, the male respondents had a higher likelihood of positive intention (AOR 2.27) after adjusting for all demographic characteristics (p < 0.001). Besides, those who were single (AOR 1.77) had a higher likelihood of positive intention (p < 0.01). Further, compared to those individuals having a monthly income above SAR 10,000, those with an income of SAR 5,000 (AOR 0.59) and SAR 7,500–10,000 (AOR 0.57), had negative intention when adjusted for other demographics (p < 0.05). Individuals who rated their knowledge of COVID-19 as good were more likely to vaccinate (AOR 1.78), while those who never contracted the disease showed positive intention (1.74) toward vaccination when adjusted for all other demographics (p < 0.05). Some of the variables were significant determinants of positive intention alone and become non-significant when adjusted for all other demographics (Table 5).
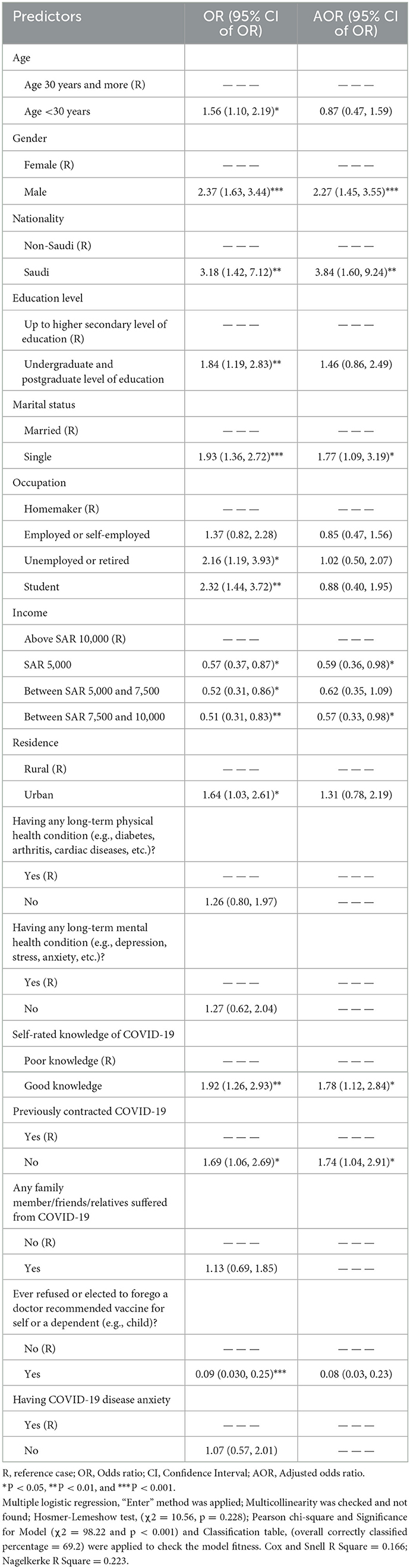
Table 5. Determinants of positive intention toward COVID-19 vaccination.
The model for self-rated good knowledge of COVID-19 disease revealed that compared to individuals who lived in rural localities, individuals living in urban areas were more likely to rate their knowledge as good (AOR 1.71) when other demographics were considered (p < 0.05). Besides, individuals who did not have any long-term mental health condition were three times more likely to rate their knowledge of COVID-19 as good (AOR 2.74) when adjusting other demographics (p < 0.01). Moreover, individuals who intended to receive COVID-19 vaccine were more likely to rate their knowledge of the disease as good (AOR 1.75) when other variables were considered (p < 0.05). Some of the variables were significant determinants of positive intention alone and become non-significant when adjusted for all other demographics (Table 6).
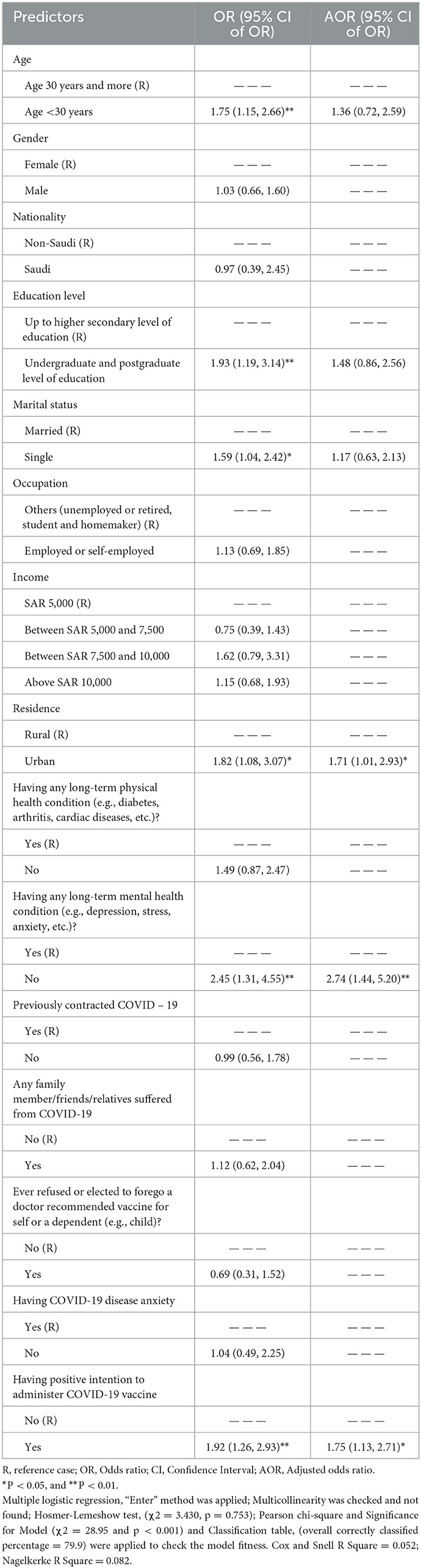
Table 6. Determinants of good knowledge of COVID-19 disease.
The interplay of COVID-19 disease anxiety, self-rated disease knowledge, and vaccine intention has not been investigated so far among general public in Saudi Arabia. Although, studies have documented knowledge, vaccination acceptance, and fear of the disease as standalone concepts (21–25). However, how these entities affect each other remains undocumented. The findings of this study highlighted that the COVID-19 anxiety appeared independent of the disease knowledge and vaccine acceptance. However, the latter two appeared to influence each other as both were reported as significant determinants for each other. There is logic in this finding as knowledge of COVID-19 has the potential to improve the understanding about vaccines for the same. The COVID-19 knowledge had a positive impact on vaccination intention. However, it does not affect the COVID-19 anxiety which appeared to be influenced by the mental health of respondent.
Our findings highlight that the self-rated knowledge of COVID-19 among most participants was at an acceptable level. This confirmed the findings of previous studies which reported that public in Saudi Arabia is quite aware of the infection (26–28). However, one of the study reported that it may be higher among individuals with higher education and income (28). In our study, most participants had higher education and income. To this end, this study adds to the existing body of literature by carrying out the analysis to report the determinants of self-rated good knowledge of COVID-19. The residence may impact an individual's life. People living in urban areas may have more opportunities for obtaining education and finding better work as most educational institutes and work related opportunities are usually concentrated in urban areas. Our findings reveal that individuals who resided in urban localities were more likely to rate their knowledge as good compared to those living in rural areas. Besides, individuals with a higher degree such as bachelor or a postgraduate qualification were more likely to rate their knowledge as good compared to others. However, the variable of higher education was only a significant determinant when other demographics were not considered. Further, our data could not establish the aspect of income as a significant determinant of self-rated good knowledge of the infection. In another study, it was reported that older participants were more knowledgeable (26). However, in our study we found that participants aged 30 years or younger were more likely to rate their knowledge as good. Though, the variable of age was only significant when other variables were not considered.
Our findings highlight that individuals who did not suffer from any long-term mental health condition were more likely to rate their knowledge of COVID-19 as good. This aspect of viewing mental health issues alongside knowledge of disease was not reported from this population. This finding also raises the question of evaluating the impact of mental health on disease knowledge. In this context, an interesting finding was reported by Al Dhaheri et al. (29) that the disease had some level of psychological impact. It was also observed in our study that the individuals who intended to receive a vaccine for the disease were roughly two times more likely to rate their knowledge as good.
In regards to the intention to receive a vaccine for COVID-19, more than half of the target segment, i.e., 57.4% had a positive intention to receive a vaccine. This was similar to the results reported by previous studies (30, 31). In addition, the data highlights that the male respondents and those who never contracted the disease before, had a higher likelihood of positive intention as compared to female respondents and individuals with a history of COVID-19 infection, respectively. Being male and having no history of COVID-19 infection were previously reported as predictors of positive intention in this population (31). In addition, our data highlighted that individuals who rated their knowledge of COVID-19 as good were more likely to vaccinate. A possible explanation for this occurrence could be that better understanding about the disease may prompt an individual to seek a positive change, i.e., treatment. Hence, patients who rated their knowledge as good understood the disease and its treatment. Therefore, they indicated their acceptance for vaccination.
It was also observed that most respondents had no anxiety owing to the viral infection. Individuals with long-term mental illnesses appeared prone to having COVID-19 anxiety. This was in line with results of a previous study where it was reported that the disease had a psychological impact (29). Therefore, it is likely that respondents in our study who suffered from mental illness were more anxious. Our study reported that younger individuals were more likely to have anxiety as compared to the older ones. To this end, a previous study reported a high level of anxiety in young adults between 18 and 29 years during COVID-19 resultant lockdown in Saudi Arabia (32). Thus, our findings highlight the presence of continued anxiety in this age group. This age group usually contains individuals who are either involved in their studies or are working. COVID-19 has caused disruptions in education and work sectors such as switching to online education (33). It has also resulted in switching to work from home (34). This coupled with new outbreaks and emergence of new variants of the virus may continuously bother such individuals. It is extremely important to address the mental issues pertaining to individuals in this age group.
The study has some limitations, due to the convenient nature of data collection, there may be a selection bias as the researchers gather data from individuals who could be easily approached. Although the study gathered data from a large number of participants with reasonable demographic diversity, the findings should be interpreted with caution. This also affects the generalizability of the findings. However, since it was carried out in several sites at different times of day. This would have offered a considerable level of random data collection within the convenient realm. Therefore, it is expected that the findings may be limited to local settings and may not be generalized.
Secondly, there may an element of information bias attributed to the self-reporting format of this study particularly with answers related to the COVID-19 disease anxiety, disease knowledge, compliance to social distancing protocols provided by the health authority. We believe that there may be a slight overestimation by respondents as they may have tended to select a socially acceptable response. Although, they were informed that the data was collected without any personal identifier, and they cannot be identified once the response has been submitted. Besides, it was explicitly requested to provide an honest response for this exact purpose. Moreover, some of the findings of this study were similar to the ones reported previously. Lastly, study gathered data from a small number of non-Saudi respondents and therefore, all comparisons made based on nationality must be interpreted with caution.
The findings of this study highlight that COVID-19 knowledge had a positive impact on vaccination intention however, it does not affect COVID-19 anxiety. It is recommended to initiate more disease awareness campaigns in small towns and rural communities as individuals hailing from those localities had low knowledge and subsequently less positive intent. Secondly, mental conditioning sessions may be required for students and employees at universities and workplaces respectively as these groups had a higher likelihood of COVID-19 anxiety.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Institutional Review Board of Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia (IRB−2021-05-297). The patients/participants provided their written informed consent to participate in this study.
MI: conceptualization, methodology, questionnaire design, ethical clearance, formal analysis, writing–original draft, correspondence, revision of manuscript, and preparing response to reviewers' comments. DA: methodology, questionnaire design, writing–original draft, revision of manuscript, preparing response to reviewers' comments, and supervision of process. AN: conceptualization, methodology, questionnaire design, writing–original draft, revision of manuscript, and preparing response to reviewers' comments. MM and AI: methodology, questionnaire design, data collection, revision of manuscript, and preparing response to reviewers' comments. MK: questionnaire design, data collection, and revision of manuscript. MA: methodology, questionnaire design, revision of manuscript, and preparing response to reviewers' comments. AH: methodology, questionnaire design, revision of manuscript, funding acknowledgment, and supervision of process.
The authors would like to thank the Deanship of Scientific Research at the Umm Al-Qura University for supporting this work by grant code 22UQU4290073DSR10.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1078023/full#supplementary-material
1. Cucinotta D, Vanelli M. WHO Declares COVID-19 a pandemic. Acta bio-medica Atenei Parmensis. (2020) 91:157–60. doi: 10.23750/abm.v91i1.9397
2. Conti P, Caraffa A, Gallenga CE, Kritas SK, Frydas I, Younes A, et al. The British variant of the new coronavirus-19 (SARS-CoV-2) should not create a vaccine problem. J Biol Regul Homeost Agents. (2020) 35:1–4. doi: 10.23812/21-3-E
3. Lauring AS, Hodcroft EB. Genetic variants of SARS-CoV-2—what do they mean? JAMA. (2021) 325:529–31. doi: 10.1001/jama.2020.27124
4. Thomson H. Two years of the coronavirus. New Sci. (2022) 253:10–13. doi: 10.1016/S0262-4079(22)00003-3
5. Bendau A, Petzold MB, Pyrkosch L, Mascarell Maricic L, Betzler F, Rogoll J, et al. Associations between COVID-19 related media consumption and symptoms of anxiety, depression and COVID-19 related fear in the general population in Germany. Eur Arch Psychiatry Clin Neurosci. (2021) 271:283–91. doi: 10.1007/s00406-020-01171-6
6. Hoong NK, Kemp R. Understanding and reducing the fear of COVID-19. J Zhejiang Univ Sci B. (2020) 21:752–4. doi: 10.1631/jzus.B2000228
7. Naser AY, Al-Hadithi HT, Dahmash EZ, Alwafi H, Alwan SS, Abdullah ZA. The effect of the 2019 Coronavirus disease outbreak on social relationships: a cross-sectional study in Jordan. Int J Soc Psychiatry. (2021) 67:664–71. doi: 10.1177/0020764020966631
8. World Health Organization. Novel Coronavirus (2019-nCoV). Situation Report-13 (2020). Available online at: https://apps.who.int/iris/handle/10665/330778 (accessed August, 2022).
9. Singh S, Roy D, Sinha K, Parveen S, Sharma G, Joshi G. Impact of COVID-19 and lockdown on mental health of children and adolescents: a narrative review with recommendations. Psychiatry Res. (2020) 293:113429. doi: 10.1016/j.psychres.2020.113429
10. Basyouni SS, El Keshky MES. Job insecurity, work-related flow, and financial anxiety in the midst of COVID-19 pandemic and economic downturn. Front Psychol. (2021) 12:632265. doi: 10.3389/fpsyg.2021.632265
11. Teijaro JR, Farber DL. COVID-19 vaccines: modes of immune activation and future challenges. Nat Rev Immunol. (2021) 21:195–7. doi: 10.1038/s41577-021-00526-x
12. Moore S, Hill EM, Tildesley MJ, Dyson L, Keeling MK. Vaccination and non-pharmaceutical interventions for COVID-19: a mathematical modelling study. Lancet Infect Dis. (2021) 21:793–802. doi: 10.1016/S1473-3099(21)00143-2
13. GOV.UK. Guidance. COVID-19 Response: Living with COVID-19 (2022). Available online at: https://www.gov.uk/government/publications/covid-19-response-living-with-covid-19/covid-19-response-living-with-covid-19 (accessed June 5, 2022).
14. Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N Engl J Med. (2020) 383:2603–15. doi: 10.1056/NEJMoa2034577
15. Voysey M, Clemens SAC, Madhi SA, Weckx LY, Folegatti PM, Aley PK, et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet. (2021) 397:99–111. doi: 10.1016/S0140-6736(20)32661-1
16. Al-Qahtani MS, Afifi IK. COVID-19 vaccine and its impacts on dental practice in Saudi Arabia. J Umm Al-Qura Univ Med Sci. (2022) 8:29–33. doi: 10.54940/ms60940175
17. Assiri A, Al-Tawfiq JA, Alkhalifa M, Duhailan HA, Qahtani SA, Abu Dawas R, et al. Launching COVID-19 vaccination in Saudi Arabia: lessons learned, and the way forward. Travel Med Infect Dis. (2021) 43:102119. doi: 10.1016/j.tmaid.2021.102119
18. World Population Review. Population of Cities in Saudi Arabia (2022). Available online at: https://worldpopulationreview.com/countries/cities/saudi-arabia (accessed August, 2022).
19. Raosoft Sample Size Calculator (2022). Available online at: http://www.raosoft.com/samplesize.html (accessed August, 2022).
20. Lee SA. Coronavirus anxiety scale: a brief mental health screener for COVID-19 related anxiety. Death Stud. (2020) 44:393–401. doi: 10.1080/07481187.2020.1748481
21. Al-Rahimi JS, Nass NM, Hassoubah SA, Wazqar DY, Alamoudi SA. Levels and predictors of fear and health anxiety during the current outbreak of COVID-19 in immunocompromised and chronic disease patients in Saudi Arabia: a cross-sectional correlational study. PLoS ONE. (2021) 16:e0250554. doi: 10.1371/journal.pone.0250554
22. Narapureddy BR, Muzammil K, Alshahrani MY, Alkhathami AG, Alsabaani A, AlShahrani AM, et al. COVID-19 vaccine acceptance: beliefs and barriers associated with vaccination among the residents of KSA. J Multidiscip Healthc. (2021) 14:3243–52. doi: 10.2147/JMDH.S340431
23. Mohsin SF, Agwan MA, Shaikh S, Alsuwaydani ZA, AlSuwaydani SA. COVID-19: fear and anxiety among healthcare workers in Saudi Arabia. A cross-sectional study. Inquiry. (2021) 58:00469580211025225. doi: 10.1177/00469580211025225
24. Shaikhain T, Al-Husayni F, Bukhari G, Alhawsa B, Shalabi N, Munshi A, et al. Knowledge and attitude toward coronavirus disease 19 pandemic among Saudi Arabia population: a cross-sectional study. SAGE Open Med. (2021). doi: 10.1177/20503121211052421
25. Mohammed Z, Arafa A, Atlam ES, El-Qerafi N, El-Shazly M, Al-Hazazi O, et al. Psychological problems among the university students in Saudi Arabia during the COVID-19 pandemic Int J Clin Pract. (2021) 75:e14853. doi: 10.1111/ijcp.14853
26. Al-Hanawi MK, Angawi K, Alshareef N, Qattan AMN, Helmy HZ, Abudawood Y, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front. Public. Health. (2020) 27:217. doi: 10.3389/fpubh.2020.00217
27. Almofada SK, Alherbisch RJ, Almuhraj NA, Almeshary BN, Alrabiah B, Saffan AA, et al. Knowledge, attitudes, and practices toward COVID-19 in a Saudi Arabian population: a cross-sectional study. Cureus. (2020) 12:e8905. doi: 10.7759/cureus.8905
28. Alsharqi OZ, Qattan A, Alshareef N, Chirwa GC, Al-Hanawi MK. Inequalities in knowledge about COVID-19 in the Kingdom of Saudi Arabia. Front Public Health. (2021) 9:743520. doi: 10.3389/fpubh.2021.743520
29. Dhaheri ASA, Bataineh MF, Mohamad MN, Ajab A, Marzouqi AA, Jarrar AH, et al. Impact of COVID-19 on mental health and quality of life: is there any effect? A cross-sectional study of the MENA region. PLoS One. (2021) 16:e02491. doi: 10.1371/journal.pone.0249107
30. Fayed AA, Shahrani ASA, Almanea LT, Alsweed NI, Almarzoug LM, Almuwallad RI, et al. Willingness to receive the COVID-19 and seasonal influenza vaccines among the Saudi population and vaccine uptake during the initial stage of the national vaccination campaign: a cross-sectional survey. Vaccines. (2021) 9:765. doi: 10.3390/vaccines9070765
31. Noushad M, Nassani MZ, Koppolu P, Alsalhani AB, Samran A, Alqerban A, et al. Predictors of COVID-19 vaccine intention among the saudi arabian population: a cross-sectional survey. Vaccines. (2021) 8:892. doi: 10.3390/vaccines9080892
32. Albagmi FM, AlNujaidi HY, Al Shawan DS. Anxiety levels amid the COVID-19 lockdown in Saudi Arabia. Int J Gen Med. (2021) 14:2161–70. doi: 10.2147/IJGM.S312465
33. Al-Shahrani AM. Students' Anxiety during the COVID-19 pandemic in Saudi Arabia. J Family Med Primary Care. (2021) 10:3192–7. doi: 10.4103/jfmpc.jfmpc_46_21
Keywords: COVID-19, pandemic, COVID-19 vaccine acceptance, vaccine, Saudi Arabia
Citation: Islam MA, Alshayban DM, Naqvi AA, Maqsood MB, Ishaqui AA, Kashif M, Ali M and Haseeb A (2023) How anxiety attributed to COVID-19, disease knowledge, and intention to vaccinate against SARS-CoV-2 viral infection prevail in general public of Saudi Arabia? Front. Public Health 11:1078023. doi: 10.3389/fpubh.2023.1078023
Received: 23 October 2022; Accepted: 18 January 2023;
Published: 07 February 2023.
Edited by:
Guodong Ding, Shanghai Jiao Tong University, ChinaReviewed by:
Wibke Bayer, Essen University Hospital, GermanyCopyright © 2023 Islam, Alshayban, Naqvi, Maqsood, Ishaqui, Kashif, Ali and Haseeb. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Md. Ashraful Islam,  bWFpc2xhbUBpYXUuZWR1LnNh
bWFpc2xhbUBpYXUuZWR1LnNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.