 Christine Fahim
Christine Fahim Jeanette Cooper
Jeanette Cooper Suvabna Theivendrampillai
Suvabna Theivendrampillai- Knowledge Translation Program, Li Ka Shing Knowledge Institute, Unity Health Toronto, Toronto, ON, Canada
Background: The COVID-19 pandemic has led to stigmatization of individuals based on race/ethnicity, age, gender, and occupation, among other factors. We canvassed Canadian residents to explore perceptions of and experiences with stigma during the COVID-19 pandemic.
Methods: We conducted an online survey between June 10 and December 31 2020. The survey was rooted in the Health Stigma and Discrimination Framework and included multiple choice, Likert and open-ended questions related to perceived and experienced stigma. Residents of Ontario, Canada were eligible to participate and we aimed to recruit a sample that was diverse by race/ethnicity and age.
Results: A total of 1,823 individuals participated in the survey (54% women, 39% men; 54% 18–40 years old, 28% 41–60 years old, 12% 61+ years old; 33% White, 26% East/SouthEast Asian, 14% Black, 12% South Asian). Fifty-one percent of participants agreed/strongly agreed that racist views had increased toward certain racial/ethnic groups in Canada during the pandemic. Participants perceived that people in Canada were stigmatized during the pandemic because of race/ethnicity (37%), political beliefs (26%), older age (24%), being a healthcare worker (23%), younger age (22%), being an essential worker (21%), and gender (11%). Thirty-nine percent of respondents feared experiencing and 37% experienced stigmatization during the pandemic. Men, individuals aged 18–40, and racialized participants were more likely to fear or experience stigma. With respect to health behaviors, 74, 68, and 59% of respondents were comfortable masking in public, seeking medical care if they became ill, and getting tested for COVID-19, respectively. Men were less likely to indicate comfort with mask wearing or seeking medical care. Participants aged 18–40 and Black participants were less likely to indicate comfort with all three behaviors compared to those over age 41 and White participants, respectively. South Asian participants were less likely to be comfortable seeking medical care compared to White Participants.
Discussion: Participants feared or experienced stigmatization towards various demographic characteristics during the COVID-19 pandemic. It is critical that the factors driving stigma during health emergencies in Canada be better understood in order to develop effective public health messaging and interventions.
Introduction
The COVID-19 pandemic led to rises in hate speech, racism, and stigmatization of certain populations (1–3). At the onset of the pandemic, this stigma was particularly directed toward people of Chinese (4–6) or East-Asian decent (4–6). However, as the pandemic evolved, other groups in Canada were stigmatized including those who had COVID-19, healthcare workers, individuals from communities perceived to have experienced outbreaks (particularly racialized communities), and individuals who did or did not participate in public health recommendations such as masking (7–9). Intersecting factors and ongoing structural inequities further resulted in the disproportionate impact of the pandemic on women, racialized persons, and frontline and healthcare workers (7).
Stigma can be driven by fears and a lack of knowledge (10). As the evidence on COVID-19 evolved, so did public health policies aimed at curbing its spread (11). These changing policies coupled with a perceived lack of transparency and limited public health information left individuals feeling a sense of distrust and confusion surrounding the pandemic (12). This created a climate for an “infodemic”, where public fear and desire for knowledge coupled with widespread misinformation facilitated the spread of stigmatization and discrimination (13–17).
Stigmatization can create a barrier to accessing health services and participating in public health behaviors (e.g., masking). Stangl et al., developers of the Health Stigma and Discrimination Framework (HSDF) outline that stigma “influences public health outcomes by worsening, undermining, or impeding a number of processes including social relationships, resource availability, stress, and psychological and behavioral responses, [thereby] exacerbating poor health” (10). The framework developers emphasize the importance of moving away from framing stigma as experiences between the individual “stigmatizer” vs. the “stigmatized” and rather, giving attention to narratives that drive stigma within broader organizational, community and historical systems that shape public opinion.
The purpose of this study was to use the HSDF to explore perceptions and experiences of stigma during the COVID-19 pandemic in Canada. Specifically, we aimed to explore perceptions and experiences of stigma among Ontario residents by gender, age, and race/ethnicity.
Materials and methods
The study was approved by the Toronto Academic Health Science Network REB (REB#20-092).
Study design
Survey study
The conduct and reporting of our survey study adhered to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) (18, 19). We aimed to recruit a convenience sample of participants who were residents of Ontario, Canada and reflected diversity with respect to age, gender and race/ethnicity.
Survey development
The survey was rooted in the HSDF which describes health stigmatization across a socio-ecological spectrum and considers how intersecting characteristics (such as race, sex, gender, age) interact within organizations, communities and public policy (18). The HSDF distinguishes between stigmatized experiences that impact outcomes (e.g., emotional health, social exclusion, access to treatment) and stigma practices (e.g., fear/misinformation that perpetuate stereotypes and discrimination), thus categorizing stigma as perceived and experienced.
The survey included 11 demographic questions and 36 questions on stigma. Survey questions included multiple choice, 5 point Likert scale, and open-ended responses (see Appendix A for survey). The survey was developed by the research team; team members piloted the survey for clarity prior to dissemination.
Recruitment
We aimed to generate a sample that was evenly distributed by male and female gender (although we were inclusive of all gender categories) and evenly distributed by age ranges (>18 years). With respect to race/ethnicity, we aimed to generate a sample that included a minimum of 25% of respondents who self-identified as East Asian or Black, respectively. We also aimed to include representation by other races/ethnicities.
We conducted an open survey with multiple recruitment channels. Survey links were distributed via our community partners including the Chinese Canadian National Council for Social Justice and the Chinese Canadian National Council Toronto Chapter, which are advocacy organizations for social justice. Study recruitment ads were also posted to our websites (Knowledge Translation Program, SPOR Evidence Alliance, KT Canada, Unity Health Toronto) and to Twitter, LinkedIn, Kijiji, and Reddit. Additionally, we sent study invitations via email to community and student organizations representing Black, Indigenous, and racialized (BIPOC) populations. We also enlisted a market organization, Canadian Viewpoint (20), to disseminate our survey and support recruitment of a diverse Ontario population. Canadian Viewpoint distributed the survey using an email invitation to their email listservs, which were composed of individuals who previously agreed to receiving email communications from Canadian Viewpoint. Survey participants had the option of entering into a draw for the chance to win a Visa gift card.
Informed consent
Participants who clicked on the survey link were directed to the survey landing page, which provided an overview of the study purpose, a description of how to complete the survey, and consent information. We provided a statement that consent would be implied by accessing the survey. All participation was voluntary; participants who did not wish to participate were directed to close the webpage. Responses were anonymous and were not mandatory.
Data collection
Surveys were posted using Qualtrics on our program website and distributed by Canadian Viewpoint. Data were collected between June 10th 2020–December 31st 2020.
Data analysis
Questionnaires with <5% data completion, completed by non-Ontario residents and duplicates were excluded from analysis. Quantitative data were summarized using descriptive statistics; textual responses were analyzed using content analysis by a team member experienced in qualitative analysis. Responses to the stigma questions were analyzed using ordinal regression to explore the association between stigma perceptions and experiences and demographic characteristics. We grouped responses to the 5-point Likert scale questions into three categories (Strongly disagree and Disagree; Neither Agree/Disagree; and Strongly Agree and Agree). We also combined groups by age and race/ethnicity to facilitate regression analyses. We excluded gender-diverse persons from the regression analysis by gender given insufficient sample size (<1% of the overall sample).
We used ordinal regression analysis conducted using the R statistical software (21), the R packages “polyr”, “foreign”, “ggplot2”, “MASS”, “Hmisc” and “reshape2” and RStudio (22). Statistical analysis was led by a statistician (BP).
Results
Participant demographics
A total of 1,823 individuals participated in the survey (Table 1). A total of 54.31% of participants identified their gender as female, 38.56% as male, 0.49% identified as genderfluid, transgender, gender variant, trans male, or non-binary and 6.64% did not respond. 53.87% of participants were between 18 and 40 years old, 28.41% were 41–60 years old and 11.79% were 61 years or older. With respect to race/ethnicity, 32.69% identified as White, 26% as East Asian or Southeast Asian, 14.21% as Black, and 11.68% as South Asian. 9.05% identified as LatinX, Middle Eastern, South American, Multiple Ethnicities, or Other and 5.48% of the sample identified as Indigenous. Approximately fifty percent of the sample were college/university educated, 13.55% had some college/university, and 18.43% had a post-graduate degree. Over half (52.06%) of participants worked full-time. The majority of the participants (82.99%) were Canadian citizens. Participants most commonly resided in Central Ontario (35.38%) and in the Toronto region (33.85%) (Table 1).
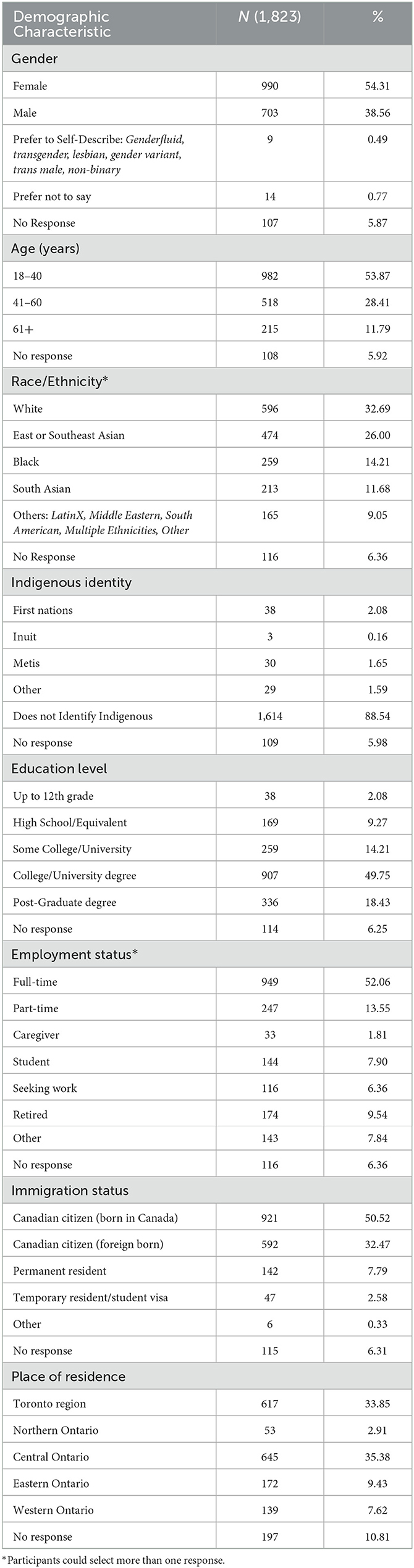
Table 1. Participant demographics.
Perceptions of blame
In response to the question “Do you think there is someone to blame for COVID-19”, 54.91% of participants answered not at all/a little, 22.60% answered somewhat, and 18.98% answered a lot/quite a lot. In the open-ended responses, participants (n = 1,155) assigned blame to the following entities: China/Chinese government/health officials (36.36%), governments (general) and public health officials (16.62%), people who do not follow public health advice (e.g., anti-masking, not following social distancing; 9.52%), Donald Trump/the US government (4.16%), wet markets (4.16%), and people who consume animals (3.98). Other responses (<4% each) included: the World Health Organization, laboratories in which the virus may have originated, media, travelers, and scientists.
Perceptions of stigma and racist views in Canada
51.45% of participants agreed/strongly agreed that racist views had increased toward certain racial/ethnic groups in Canada during the pandemic; 41.19% believed Canadians were speaking out against discrimination and stigmatization (Table 2). Men had slightly lower odds of agreeing with this statement compared to women participants (Table 3). East/South Asian and other non-White, non-Black, and non-East/South East Asian participants (grouped as “other”) were more likely to agree compared to White participants (OR 1.71, 1.85, respectively, Table 3).
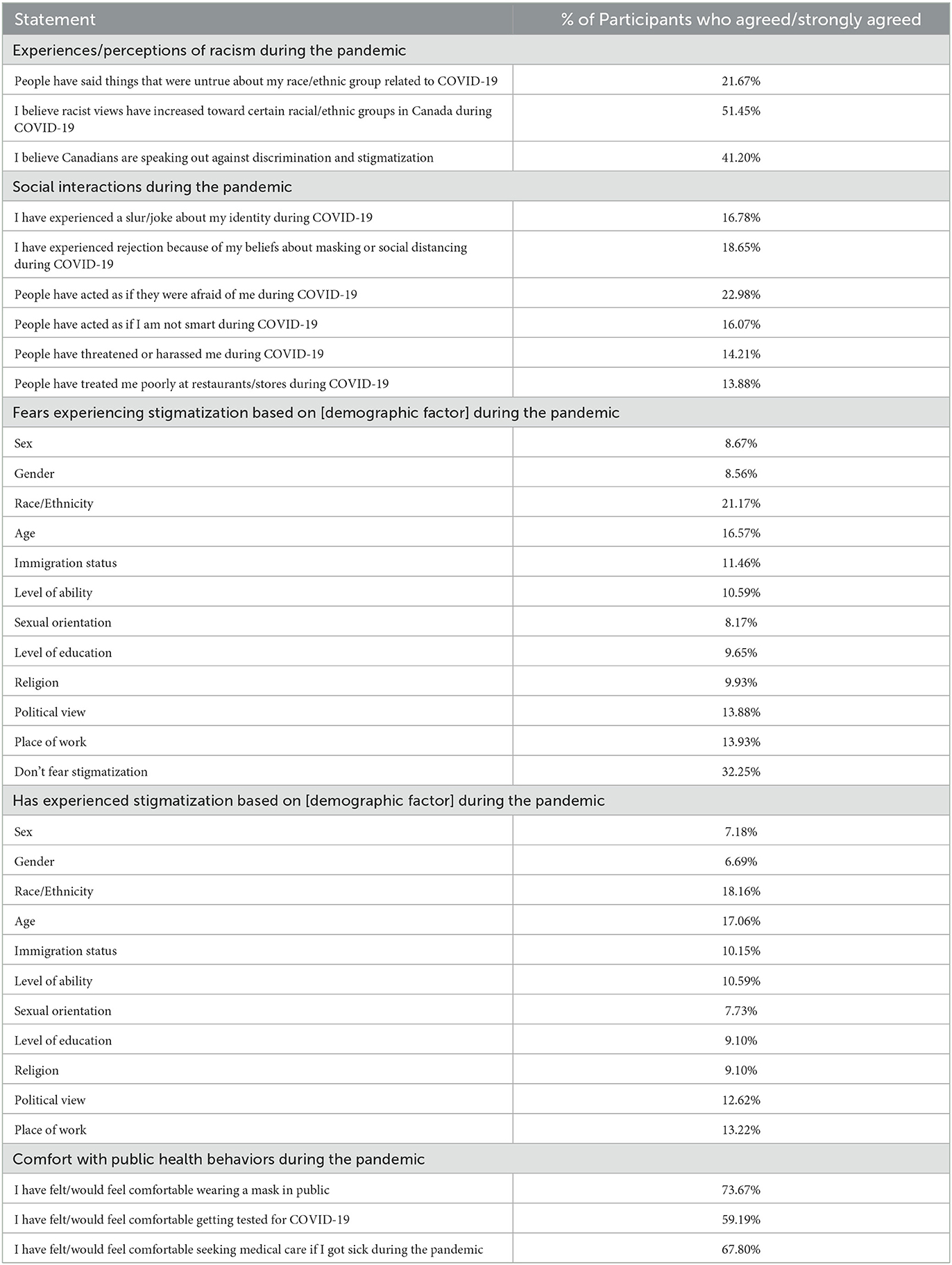
Table 2. Proportion of participants that agreed/strongly agreed with statements.
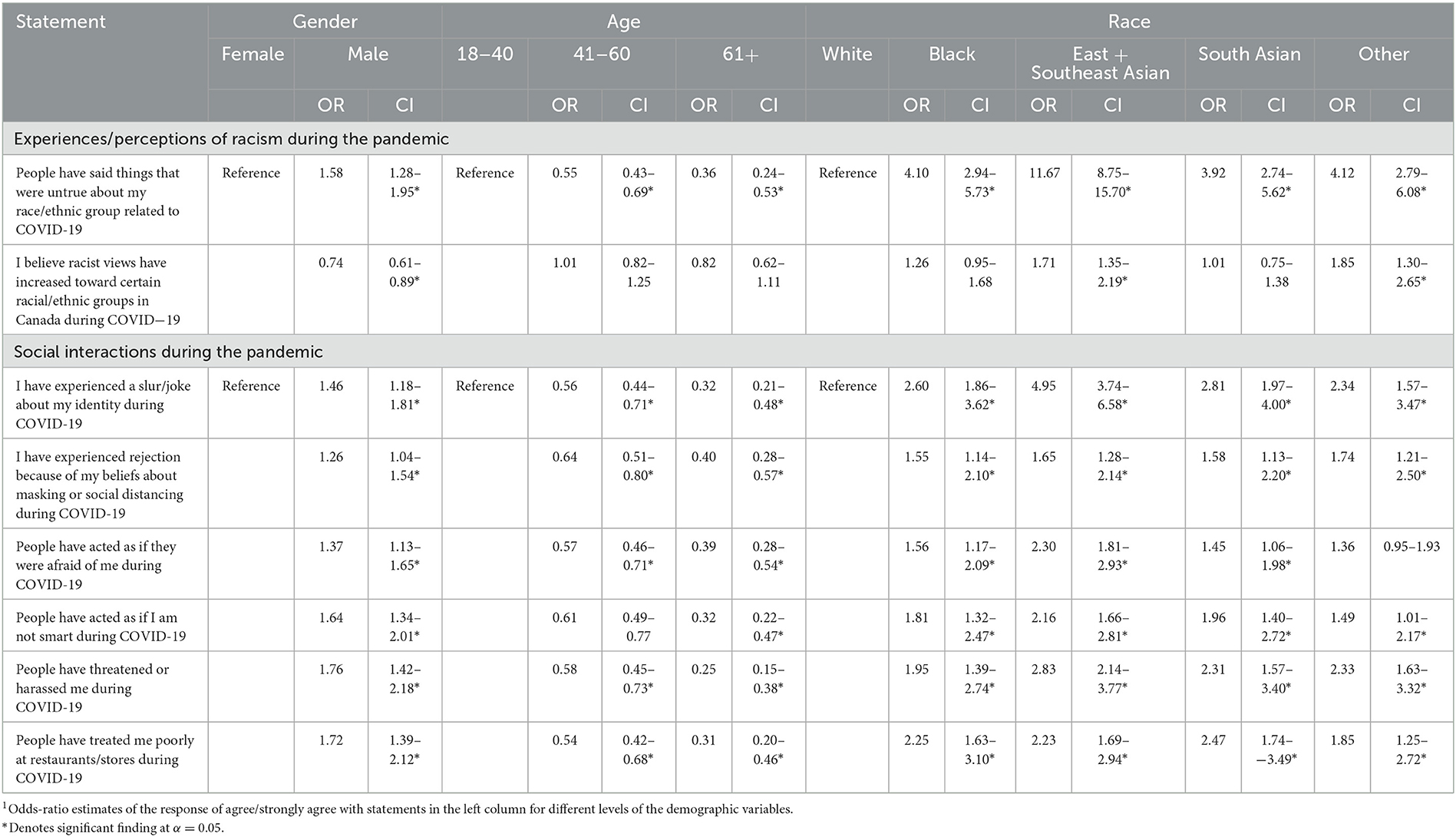
Table 3. Associations between experiences with social interactions during the COVID-19 pandemic and demographic characteristics1.
Participants believed individuals in Canada had been stigmatized “a lot/quite a lot” during the pandemic due to: race/ethnicity (37.46%), political beliefs (25.78%), older age (23.53%), being a healthcare worker (22.65%), younger age (21.94%), being an essential worker (21.39%), and gender (10.75%).
Fear of stigma
A total of 25.34% of participants said they were very afraid/concerned of experiencing stigma or racism, 32.86% were a little afraid/concerned and 28.96% were not afraid/concerned (4.06% were unsure, 5.16% selected N/A, and 3.62% did not respond). 21.67% of participants agreed that people had said untrue things about their race/ethnic group related to COVID-19; men were more likely to agree with this statement compared to women and racialized participants [particularly East or Southeast Asian participants (OR 11.67, Table 3)] were significantly more likely to agree compared to White participants.
40.10% percent of participants feared being stigmatized during the pandemic; 32.25% did not fear stigmatization (Table 2). Participants reported fearing stigmatization during the pandemic based on: race/ethnicity (21.17%), age (16.57%), political view (13.88%), place of work (13.93%), immigration status (11.46%), religion (9.93%), level of education (9.65%), level of ability (10.58%), sex (8.67%), gender (8.56%), and sexual orientation (8.17%).
Men were more likely to fear being stigmatized due to sex, gender, immigration status, level of ability, sexual orientation, level of education, religion, political view compared to Women (Table 4). Participants aged 18–40 were more likely to fear stigmatization on almost all assessed demographic factors compared to those over the age of 40 (Table 4). Racialized participants were more likely to report fear of stigmatization during the pandemic on all assessed demographic factors compared to White participants. Notably, East and Southeast Asian, Black, South Asian, and Other participants had an OR of 18.73, OR 6.28, OR 5.29, and OR 4.51 of fearing being stigmatized by race/ethnicity compared to White participants (see Table 4).
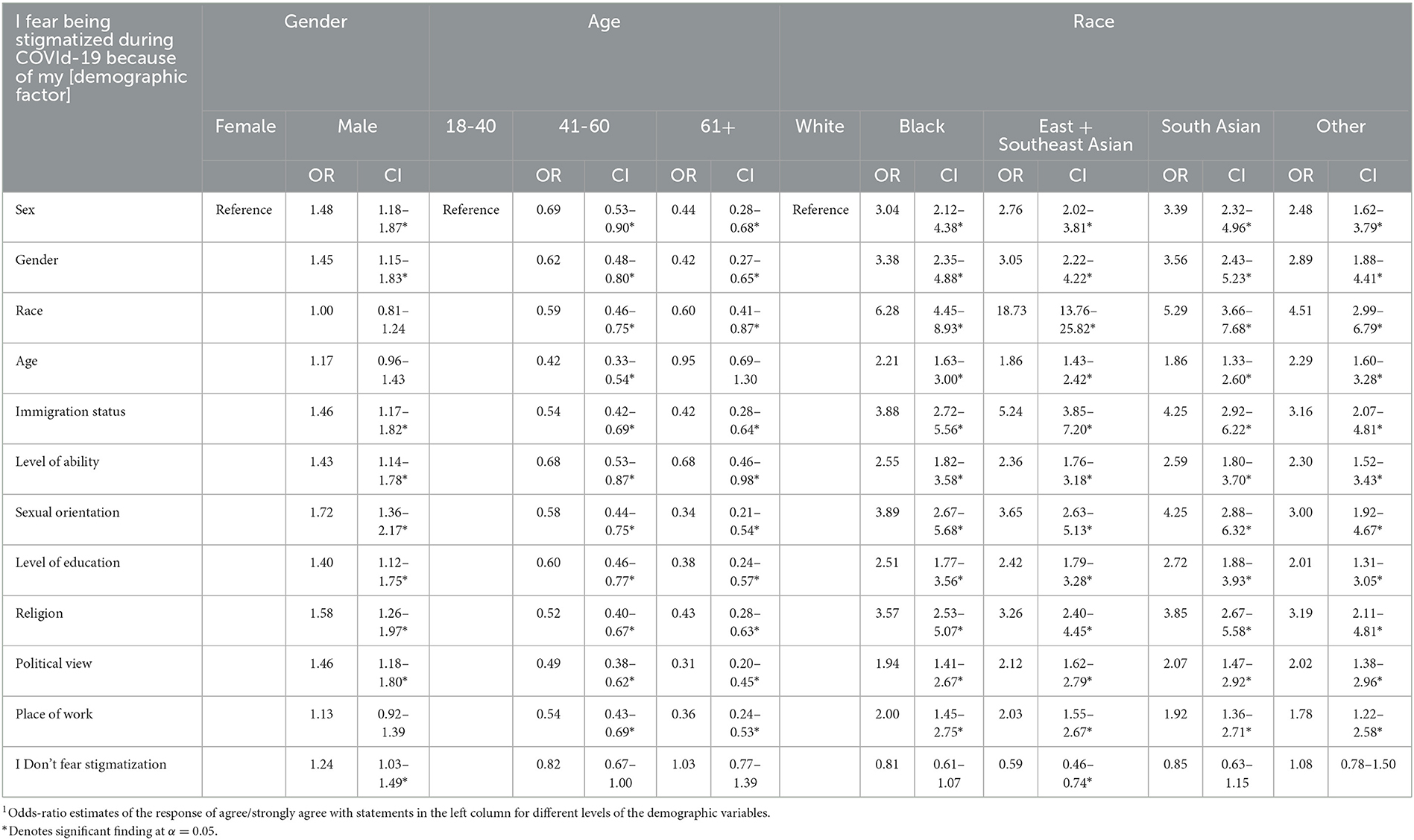
Table 4. Association between fear of being stigmatized based on demographic factors and demographic characteristics1.
Experiences of stigma
Table 2 highlights participants' experiences during the pandemic. Men and racialized participants were more likely to report experiencing negative social interactions during the pandemic compared to Women and White participants, respectively. Participants aged 18–40 were more likely to report negative social interactions compared to those over age 40, with one exception—Participants aged 40+ were more likely to report that people have acted afraid of them during the pandemic, compared to those 18–40 (Table 3).
Men were more likely to fear being stigmatized due to sex, gender, immigration status, level of ability, sexual orientation, level of education, religion, political view, and place of work compared to Women (Table 5). Participants aged 18–40 were more likely to fear stigmatization on all assessed demographic factors compared to those over the age of 40, with the exception of experiences of stigma based on age compared to those 61+ (OR 1.01, CI 0.74–1.38, Table 5). Similar to fear of stigma, racialized participants were more likely to report stigma experiences based on all assessed demographic factors compared to White participants.
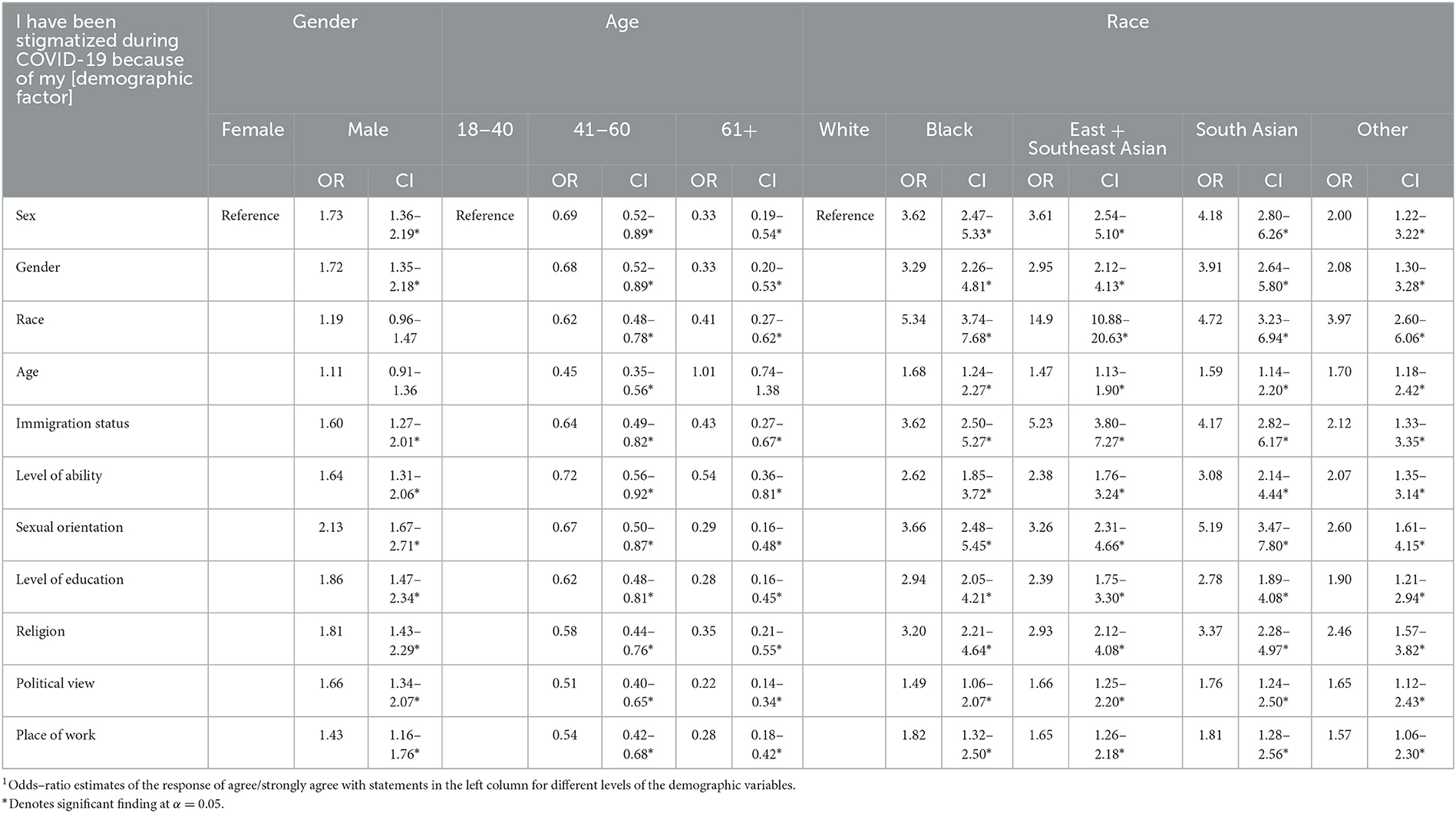
Table 5. Association between experiences of being stigmatized based on demographic factors and demographic characteristics1.
Health behaviors
The majority of participants reported being comfortable with three common health behaviors of the COVID-19 pandemic; 73.67% felt comfortable wearing a mask in public, 67.80% were comfortable seeking medical care if they became ill during the pandemic, and 59.19% were comfortable getting tested for COVID-19 (Table 2). Men were less likely to indicate comfort with mask wearing or seeking medical care. Participants aged 18–40 and Black participants were less likely to indicate comfort with all three behaviors compared to those over age 41 and White participants, respectively. South Asian participants were less likely to be comfortable seeking medical care compared to White Participants (Table 6).
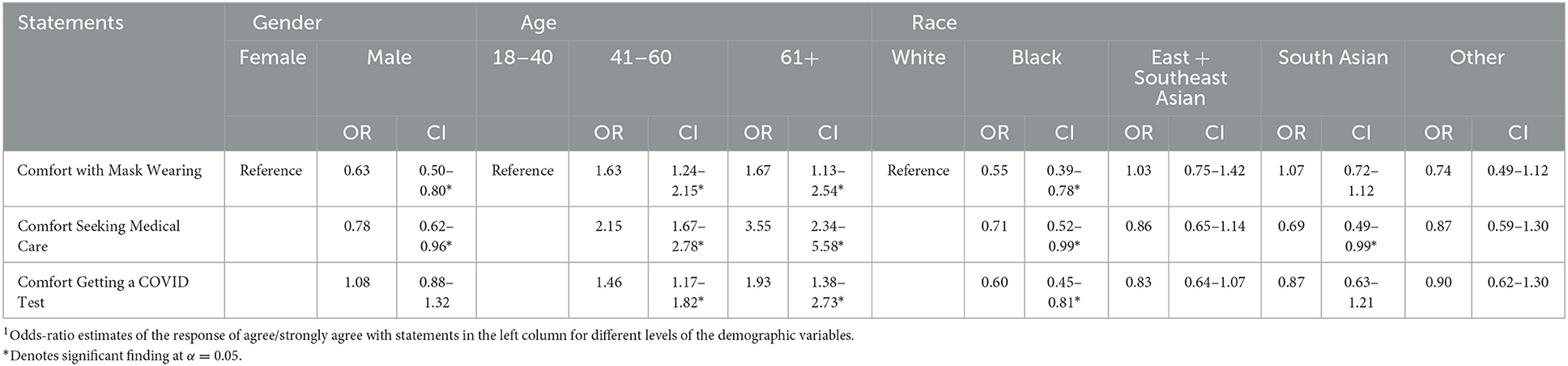
Table 6. Association of reported comfort with public health behaviors and demographic characteristics1.
Discussion
We surveyed over 1,800 residents of Ontario, Canada between June–December 2020 to canvass perceptions and experiences of stigma during the COVID-19 pandemic. Thirty-nine percent of participants feared being stigmatized during the pandemic and 37% experienced stigmatization or racism during the pandemic. Moreover, 51% of respondents believed that racism had increased in Canada during the pandemic. Our findings should be viewed within the following context: the time period represents the end of the first and start of the second waves of COVID-19 in the province (20). Ontario remained in a state of emergency until July 29th 2020 following the first wave of COVID-19 in the country. In July 2020, mandatory public health measures, such as masking in public spaces, became widespread (23). September 2020 saw an increase in COVID-19 cases which led to new restrictions across the province, particularly in regions with higher case volumes (24, 25). At the end of our study period (December 2020), the province had broken the record for daily new infections and was entering a province-wide shutdown beginning December 26th (25, 26). To provide further context to the study period, Summer 2020 was referred to as the “summer of racial reckoning” (27, 28). Black Lives Matter marches, media reports reporting anti-Asian racism in Ontario cities, and calls for anti-racist strategies highlighted deep-rooted systemic inequities in Canada and worldwide (29–31).
The HSDF indicates that stigma drivers (e.g., fears, blame, stereotypes) and facilitators (cultural norms, policies) interact to result in stigma “marking” based on health conditions and/or demographic factors (18). In our survey, we observed stigma marking based on race/ethnicity (with significantly greater odds reported for East Asian participants), age (for both older and younger adults), and profession. Individuals who were racialized, aged 18–40, and Men were more likely to fear and report experiencing stigma compared to White individuals, individuals over 40, and Women, respectively.
Among the 22% of participants who experienced stigma because of their race/ethnicity, 58% were East or South East Asian, 15% were Black and 12% were South Asian as compared to 5% of White participants. Notably, East and Southeast Asian participants were 14.9 times more likely to report experiencing racial stigma as compared to White participants. Our results are consistent with the 2020 Statistics Canada Canadian Perspective Survey Series, which is a longitudinal survey study assessing Canadians' perceptions during the pandemic (9). The June 2020 survey revealed that 20% of Canadians surveyed feared being the target of unwanted acts or behaviors because of perceived exposure risk to COVID-19 (9). Of this 20%, 1 in 5 feared being stigmatized because of their race and 1 in 10 feared being stigmatized because they worked in healthcare. Further, 13% of those who feared stigmatization attributed it to their older age.
During the initial pandemic wave, individuals of Asian descent, specifically those of Chinese ethnicity, experienced significant stigmatization, racism and marginalization (32). The CCNC Toronto Chapter, a Chinese Canadian advocacy group and partner on this study, reported 1,150 cases of racist attacks submitted to their web platforms from March 2020 to February 2021 (33). Individuals reporting these attacks were predominantly adolescents and of East Asian descent (under 18 years); adults over 55 years were more likely to report being physically assaulted. Their study identified the impact of intersecting characteristics on racist attacks, with individuals who reported the attacks in Chinese (versus English) being 34% more likely to experience emotional distress and 100% more likely to be physically assaulted (33). Similar incidents have been observed in the United States. Gardner et al. reported that 23% of Asians living in the US experienced COVID-19-related discrimination due to perceptions of blame toward China for the pandemic (25). In turn, these sentiments led to workplace discrimination and hiring biases toward Asian Americans during the pandemic (34). Similar to the findings of the CCNC Toronto Chapter, a US coalition of Asian American advocacy groups reported over 1,500 instances of racism, hate speech, or attacks against Asians and Asian Americans attributed to stigmatizing language and statements by prominent politicians and on social media (35).
Of the 39% of participants in our study who feared being stigmatized during the pandemic, 24% were White and 60% were Women. Although White participants were less likely than racialized participants to fear being stigmatized based on race/ethnicity, other reported fears of stigmatization were attributed to age, political views, and place of work. In our study, participants did not perceive gender to be a significant factor that led to increased stigma, however, Men were more likely than Women to report fear and experiences of stigma based on sex, gender, immigration status, level of ability, sexual orientation, level of education, religion, place of work and political views. Reports from the CCNC also suggest that Men were more likely than Women to be physically assaulted during the pandemic (24). Intersectional analysis may provide further context to these results. For instance, one qualitative Brazilian study suggests Men who typically experience class or gender privileges were surprised by stigmatization they experienced after contracting COVID-19 (36). The authors suggested this subset of the population is not used to being treated impolitely or being discriminated against as compared to other groups and therefore may have a heightened awareness of COVID-related stigma (36). Additionally, emerging data suggest significant gender differences in perceptions of COVID-19. In a survey of over 20,000 participants between March–April 2020 from eight high-income countries, Galasso et al. identified Women as more likely to perceive COVID-19 as a serious public health threat and to comply with preventive public health measures (37). Similarly, the Statistics Canada Survey reports that among those who feared stigmatization, 50% said it was because they do not wear a mask or did not intend to wear a mask (notably, data were gathered prior to mandatory mask mandates). This sentiment was proportionally higher among Men, younger adults, and Canadian-born individuals (9). Additional research to explore the mechanisms by which gender differences (particularly in consideration of other intersecting factors) manifest into fear of stigmatization or willingness to participate in public health behaviors are warranted.
The impact of stigma on health behaviors, and subsequently health outcomes, has been widely reported (38–40). For instance, a recent meta-analysis pooled the prevalence of stigma in infectious disease epidemics (e.g., SARS, H1N1, Zika, COVID-19) and identified 34% prevalence across all populations (40). In our study, 74, 68, and 59% of participants were comfortable masking, seeking medical care if exposed to/sick with COVID-19, and getting tested for COVID-19, respectively. However, Men and participants 18–40 were less likely to report comfort masking and seeking medical care compared to Women and participants 40+ years, respectively. Black participants were less comfortable with all three behaviors and South Asian participants were less comfortable seeking medical care as compared to White participants. Longstanding, systemic inequities and mistreatment leading to a lack of trust in the healthcare system may explain these observed patterns by race/ethnicity (41–43). The HDSF may further provide insights on how intersecting stigma experiences, when coupled with stigma practices, can manifest into health behaviors, access, and subsequently, health related outcomes (10).
Finally, another important and perhaps unique factor experienced during the COVID-19 pandemic was the global public's demand for information (e.g., how is COVID-19 transmitted, treated) contrasted against the scientific community's limited knowledge of the disease, particularly in the early days of the pandemic. The gap between the public's desire for knowledge coupled with the scientific community's efforts to generate evidence led to waves of infodemics, which included stigmatizing messages as well as conspiracy theories that give direct rise to stigma (44, 45). Stigmatizing information was widespread on social and mainstream media. Editorial cartoons consistently “othered” groups of people, (particularly people of Chinese origin or descent), racist and exclusionary hashtags trended on Twitter, derogatory comments toward prominent Asian-Canadians circulated widely, and trending tweets to ban Chinese immigration and boycott Chinese-owned businesses in Spring 2020 impacted entire neighborhoods in Canadian cities (30, 31, 46, 47). This stigmatizing information led to misinformation which was often shared widely. In fact, a Statistics Canada study estimated that over half of Canadians share misinformation/ unverified information online without first confirming its accuracy (48). Additional research exploring the intersection between stigma and misinformation in the Canadian context is both warranted and underway (49).
Strengths of our study include use of an integrated knowledge translation approach, meaning the project was designed and conducted in partnership with advocacy organizations. Use of this approach ensured our data explored questions and concepts that were important to community partners and will further the Canadian discourse on the impact of stigmatization during the COVID-19 pandemic. Second, we aimed to recruit a sample that reflected the diversity of Ontario's population; this approach allowed us to conduct secondary analyses to explore perceptions by age, race/ethnicity, and gender and contributes to the emerging literature on the use of an intersectionality lens in the conduct of health services research. Finally, this study is part of a research program that explored fear, stigma and misinformation in Canada during the COVID-19 pandemic; our studies will aim to provide actionable recommendations to improve communication and messaging in future public health emergencies.
This study has limitations. Our survey was limited to residents of Ontario and may not be representative of experiences of individuals residing in other Canadian provinces and territories. Study participants' demographics were skewed toward Women (54%) and individuals aged 18–40 (54%). Fifty-percent of the sample was college educated, which is reflective of the Canadian population (50). Our survey was limited to the first and second waves of the pandemic; it is likely that experiences and perceptions of stigmatization continued to evolve throughout the pandemic. For instance, in 2021, sentiments towards vaccinations stigmatized both those who were and were not in support of mandatory vaccination policies (51–53). Additionally, our study did not explore the impact of health related stigmas; for example, we did not evaluate whether individuals with pre-existing health conditions (e.g., HIV), individuals with disabilities, and individuals with comorbidities experienced intersecting health-related stigmas. Our study did not comprehensively explore the impact of COVID-19 on individual or social characteristics and certain groups may have been overlooked in our research. For instance, studies have highlighted the disproportionate impact of the pandemic on gender-diverse individuals (who were underrepresented in our sample) or the impact of political ideologies on attitudes toward COVID-19 (53, 54). Finally, we did not perform interaction analyses to determine the impact of intersecting categories (e.g., age x gender x race/ethnicity) on stigma perceptions and experiences. Our survey contained ordinal scale questions, which challenged our ability to interpret odds-ratio estimates for our independent variables. Additionally, our approach to demographic data collection (e.g., age ranges rather than specific ages) did not allow for linear analyses. In future, similar studies can design survey questions in a manner that will facilitate such analyses (55).
Conclusion
Our study describes fear and experiences of stigmatization during the COVID-19 pandemic among residents of Ontario, Canada. Racialized individuals, individuals aged 18–40 and Men were more likely to report fear and experiences of stigmatization during the pandemic. Understanding the factors that drive stigmatization during a health emergency and developing strategies to mitigate these sentiments are essential. Additional research on the impact of stigmatization during COVID-19 in Canada and whether it impacted health outcomes is needed.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study received ethics approval from the Toronto Academic Health Science Network REB (REB#20-092). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
CF and SS were responsible for data conceptualization and methodology. CF, JC, and ST facilitated data collection. JC and BP conducted the statistical analyses. CF and JC drafted the manuscript. All authors read, edited, and approved the final manuscript.
Funding
This study was funded via a Canadian Institutes of Health Research grant (Application #440278 awarded March 2020, PI: Dr. CF).
Acknowledgments
The authors thank Tom Lee, Christine Marquez, and Jyoti Prashad for their support administering this study and Negin Pak for supporting manuscript preparation and submission.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1068268/full#supplementary-material
References
1. Logie CH. Lessons learned from HIV can inform our approach to COVID-19 stigma. J Int AIDS Soc. (2020) 23:e25504. doi: 10.1002/jia2.25504
2. Miconi D, Li ZY, Frounfelker RL, Santavicca T, Cénat JM, Venkatesh V, et al. Ethno-cultural disparities in mental health during the COVID-19 pandemic: a cross-sectional study on the impact of exposure to the virus and COVID-19-related discrimination and stigma on mental health across ethno-cultural groups in Quebec (Canada). BJPsych Open. (2021) 7:e14. doi: 10.1192/bjo.2020.146
3. Wu C, Wilkes R, Qian Y, Kennedy EB. Acute discrimination and East Asian-white mental health gap during COVID-19 in Canada. Available SSRN 3626460. 2020; doi: 10.2139/ssrn.3626460
4. Smith LE, Potts HW, Aml?t R, Fear NT, Michie S, Rubin GJ. Holding a stigmatizing attitude at the start of the COVID-19 outbreak: a cross-sectional survey. Br J Health Psychol. (2022) 27:588–604. doi: 10.1111/bjhp.12564
5. Stechemesser A, Wenz L, Levermann A. Corona crisis fuels racially profiled hate in social media networks. EClinicalMedicine. (2020) 23. doi: 10.1016/j.eclinm.2020.100372
6. Croucher SM, Nguyen T, Rahmani D. Prejudice toward Asian Americans in the COVID-19 pandemic: the effects of social media use in the United States. Front Commun. (2020) 5:39. doi: 10.3389/fcomm.2020.00039
7. Ma Y, Zhan N. To mask or not to mask amid the COVID-19 pandemic: How Chinese students in America experience and cope with stigma. Chin Sociol Rev. (2022) 54:1–26. doi: 10.1080/21620555.2020.1833712
8. Kwon S. Mask wearing and perceived discrimination associated with COVID-19 in the United States from march 2020 to may 2021: three-level longitudinal analyses. Health Educ Behav. (2022) 49:200–9. doi: 10.1177/10901981221076396
9. Hango D,. Fear of COVID-19 related stigmatization. (2020). Available online at: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00051-eng.htm (accessed September 28, 2022).
10. Borenstein J. Stigma, Prejudice Discrimination Against People with Mental Illness Learn about Stigma, Prejudice Discrimination Against People with Mental Illness. (2020). Available online at: https://www.psychiatry.org/patients-families/stigma-and-discrimination (accessed February 22, 2023).
11. Hornik, R, Kikut, A, Jesch, E, Woko, C, Siegel, L, Kim, K. Association of COVID-19 Misinformation with Face Mask Wearing and Social Distancing in a Nationally Representative US Sample. Available online at: https://www.tandfonline.com/doi/full/10.1080/10410236.2020.1847437 (accessed February 22, 2023).
12. Person B, Sy F, Holton K, Govert B, Liang A, Garza B, et al. Fear and Stigma: The Epidemic within the SARS Outbreak.
13. Bridgman, A, Merkley, E, Loewen, PJ, Owen, T, Ruths, D, Teichmann, L, et al. The causes and consequences of COVID-19 misperceptions: Understanding the role of news and social media. Available online at: https://misinforeview.hks.harvard.edu/article/the-causes-and-consequences-of-covid-19-misperceptions-understanding-the-role-of-news-and-social-media/ (accessed February 22, 2023).
14. Fridman I, Lucas, N, Henke, D, Zigler, CK,. Association Between Public Knowledge About COVID-19, Trust in Information Sources, Adherence to Social Distancing: Cross-Sectional Survey. (2020). Available online at: https://publichealth.jmir.org/2020/3/e22060/authors doi: 10.2196/22060 (accessed February 22, 2023).
15. Schmidt T, Cloete A, Davids A, Makola L, Zondi N, Jantjies M. Myths, misconceptions, othering and stigmatizing responses to Covid-19 in South Africa: A rapid qualitative assessment.
16. Devakumar D, Shannon G, Bhopal SS, Abubakar I. Lancet. (2020). 395:1194. doi: 10.1016/S0140-673630792-3
17. Prooijen JW van, Douglas KM. Conspiracy theories as part of history: The role of societal crisis situations. 10. doi: 10.1177/1750698017701615
18. Stangl AL, Earnshaw VA, Logie CH, van Brakel WC, Simbayi L, Barré I, et al. The Health Stigma and Discrimination Framework: a global, crosscutting framework to inform research, intervention development, and policy on health-related stigmas. BMC Med. (2019) 17:1–13. doi: 10.1186/s12916-019-1271-3
19. Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. (2004) 6:e132. doi: 10.2196/jmir.6.3.e34
20. Detsky AS, Bogoch II. COVID-19 in Canada: experience and response to waves 2 and 3. JAMA. (2021) 326:1145–6. doi: 10.1001/jama.2021.14797
21. R, Core Team. R: A language environment for statistical computing. R Foundation for Statistical Computing, [Internet]. Vienna, Austria (2020). Available online at: https://www.R-project.org/ (accessed October 4, 2022).
22. RStudio Team. R: A language environment for statistical computing. R Foundation for Statistical Computing, [Internet]. Boston, MA: RStudio, PBC (2022). Available online at: http://www.rstudio.com (accessed October 5, 2022).
23. Reopening Ontario (A Flexible Response to COVID-19) Act,. (2020). Available online at: https://www.ontario.ca/laws/statute/20r17 (accessed February 22, 2023).
24. Ministry of Health. Update on COVID-19 Preparations and Actions [Internet]. (2020). Available online at: https://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/memos/DM_OH_CMOH_memo_COVID19_update_Sept_9.pdf (accessed September 28, 2022).
25. Public Health Ontario. Enhanced Epidemiological Summary: Trends of COVID-19 Incidence in Ontario [Internet]. (2021). Available online at: https://www.publichealthontario.ca/-/media/documents/ncov/epi/covid-19-epi-trends-incidence-ontario.pdf?la=en (accessed September 28, 2022).
26. Yelich I, Hilkene, A,. Ontario Announces Provincewide Shutdown to Stop Spread of COVID-19 Save Lives. (2020). Available online at: https://news.ontario.ca/en/release/59790/ontario-announces-provincewide-shutdown-to-stop-spread-of-covid-19-and-save-lives (accessed February 22, 2023).
27. Manning KD. A reckoning of racial reckoning. Lancet. (2022) 399:784–5. doi: 10.1016/S0140-6736(22)00317-8
28. Logan N. “Public relations and the racial reckoning: Exploring race, activism, and Black Lives Matter,” In: The Routledge Companion to Public Relations. Routledge (2023). p. 46–60. doi: 10.4324/9781003131700-5
29. Government Canada,. Building a Foundation for Change: Canada's Anti-Racism Strategy 2019–2022. (2019). Available online at: https://www.canada.ca/en/canadian-heritage/campaigns/anti-racism-engagement/anti-racism-strategy.html (accessed September 28, 2022).
30. Heng L,. Chinese Canadians facing hate, racism for coronavirus outbreak—much like the SARS outbreak in 2003. National Post. (2020). Available online at: https://nationalpost.com/news/chinese-canadians-facing-hate-racism-for-coronavirus-outbreak-much-like-the-sars-outbreak-in-2003 (accessed February 17, 2020).
31. Jeffords S,. Ministers, mayor push back against coronavirus stigma in Toronto's Chinatown neighbourhood. The Canadian Press. The Canadian Press. (2020). Available online at: https://globalnews.ca/news/6535457/toronto-mayor-provincial-federal-health-ministers-coronavirus/ (accessed February 11, 2020).
32. Mamuji AA, Lee C, Rozdilsky J, D'Souza J, Chu T. Anti-Chinese stigma in the Greater Toronto Area during COVID-19: aiming the spotlight towards community capacity. Soc Sci Humanit Open. (2021) 4:100232. doi: 10.1016/j.ssaho.2021.100232
33. A Year of Racist Attacks: Anti-Asian Racism across Canada One Year into the COVID-19 Pandemic. Available online at: https://drive.google.com/file/d/193CdlC8uq623VRlAzoO3ShfDTEutXQi2/view (accessed September 28, 2022).
34. Gardner DM, Briggs CQ, Ryan AM. It is your fault: workplace consequences of anti-Asian stigma during COVID-19. Equal Divers Incl Int J. (2021) 41:3–18. doi: 10.1108/EDI-08-2020-0252
35. Turner-Musa J, Ajayi O, Kemp L. Examining social determinants of health, stigma, and COVID-19 disparities. in MDPI. (2020). p. 168. doi: 10.3390/healthcare8020168
36. Sousa AR de, Cerqueira SSB, Santana T da S, Suto CSS, Almeida ES, Brito LS, et al. Stigma experienced by men diagnosed with COVID-19. Rev Bras Enferm. (2021) 75:221. doi: 10.1590/0034-7167-2021-0038
37. Galasso V, Pons V, Profeta P, Becher M, Brouard S, Foucault M. Gender differences in COVID-19 attitudes and behavior: panel evidence from eight countries. Proc Natl Acad Sci. (2020) 117:27285–91. doi: 10.1073/pnas.2012520117
38. Rueda S, Mitra S, Chen S, Gogolishvili D, Globerman J, Chambers L, et al. Examining the associations between HIV-related stigma and health outcomes in people living with HIV/AIDS: a series of meta-analyses. BMJ Open. (2016) 6:e011453. doi: 10.1136/bmjopen-2016-011453
39. Nyblade L, Stangl A, Weiss E, Ashburn K. Combating HIV stigma in health care settings: what works? J Int AIDS Soc. (2009) 12:1–7. doi: 10.1186/1758-2652-12-15
40. Yuan K, Huang XL, Yan W, Zhang YX, Gong YM, Su SZ, et al. A systematic review and meta-analysis on the prevalence of stigma in infectious diseases, including COVID-19: a call to action. Mol Psychiatry. (2022) 27:19–33. doi: 10.1038/s41380-021-01295-8
41. Batelaan K. ‘It's not the science we distrust; it's the scientists': Reframing the anti-vaccination movement within Black communities. Glob Public Health. (2022) 17:1099–112. doi: 10.1080/17441692.2021.1912809
42. Egede LE, Walker RJ. Structural racism, social risk factors, and Covid-19—a dangerous convergence for Black Americans. N Engl J Med. (2020) 383:e77. doi: 10.1056/NEJMp2023616
43. Marcelin JR, Swartz TH, Bernice F, Berthaud V, Christian R, Da Costa C, et al. Addressing and Inspiring Vaccine Confidence in Black, Indigenous, and People of Color During the Coronavirus Disease 2019 pandemic. Oxford: Oxford University Press US (2021). p. ofab417. doi: 10.1093/ofid/ofab417
44. Understanding the infodemic misinformation in the fight against COVID-19. Pan American Health Organization (PAHO). Available online at: https://iris.paho.org/bitstream/handle/10665.2/52052/Factsheet-infodemic_eng.pdf
45. Islam MS, Sarkar T, Khan SH, Mostofa Kamal AH, Murshid Hasan SM, Alamgir Kabir, et al. COVID-19–Related Infodemic and Its Impact on Public Health: A Global Social Media Analysis.
46. Labbé, F, Pelletier, C, Bettinger, JA, Curran, J, Graham, JE, Greyson, D, et al. Stigma and Blame Related to COVID-19 Pandemic: A Case-Study of Editorial Cartoons in Canada. Available online at: https://www.sciencedirect.com/science/article/pii/S0277953622001095 (accessed February 22, 2023).
47. Rodriguez J. “We need to support our Chinatowns”: Urgent calls for feds to revitalize hard-hit areas. Available online at: https://www.ctvnews.ca/health/coronavirus/we-need-to-support-our-chinatowns-urgent-calls-for-feds-to-revitalize-hard-hit-areas-1.5384148 (accessed February 22, 2023).
48. Garneau, K, Zossou, C,. Misinformation during the COVID-19 pandemic [Internet]. Available online at: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2021001/article/00003-eng.htm (accessed February 22, 2023).
49. Theivendrampillai S, Cooper J, Marquez C, Straus S, Fahim C. Canadian public perceptions and experiences with information during the COVID-19 pandemic. Poster Presented at the Academy Health 15th annual conference on the science of dissemination and implementation. (2022).
50. Education in Canada,. Key results from the 2016 Census [Internet]. (2017). Available online at: https://www150.statcan.gc.ca/n1/daily-quotidien/171129/dq171129a-eng.htm (accessed September 28, 2022).
51. Choi J, Lieff SA, Meltzer GY, Grivel MM, Chang VW, Yang LH, et al. Anti-vaccine attitudes among adults in the US during the COVID-19 pandemic after vaccine rollout. Vaccines. (2022) 10:933. doi: 10.3390/vaccines10060933
52. Monheim CL, Himmelstein MS. Public health noncompliance: Targets with COVID-19 are stigmatized when they fail to follow public health protocols. Stigma Health. (2022) 7:491–500. doi: 10.1037/sah0000388
53. Benham JL, Atabati O, Oxoby RJ, Mourali M, Shaffer B, Sheikh H, et al. COVID-19 vaccine–related attitudes and beliefs in Canada: National cross-sectional survey and cluster analysis. JMIR Public Health Surveill. (2021) 7:e30424. doi: 10.2196/30424
54. Gravelle TB, Phillips JB, Reifler J, Scotto TJ. Estimating the size of “anti-vax” and vaccine hesitant populations in the US, UK, and Canada: comparative latent class modeling of vaccine attitudes. Hum Vaccines Immunother. (2022) 18:2008214. doi: 10.1080/21645515.2021.2008214
Keywords: COVID-19, stigma, misinformation, health behaviors, Canada, discrimination
Citation: Fahim C, Cooper J, Theivendrampillai S, Pham B and Straus SE (2023) Exploring Canadian perceptions and experiences of stigma during the COVID-19 pandemic. Front. Public Health 11:1068268. doi: 10.3389/fpubh.2023.1068268
Received: 13 October 2022; Accepted: 13 February 2023;
Published: 07 March 2023.
Edited by:
Wulf Rössler, Charité Universitätsmedizin Berlin, GermanyReviewed by:
Yu Ren, Zhejiang Taizhou Hospital, ChinaAnissa Rizkianti, National Research and Innovation Agency (BRIN), Indonesia
Copyright © 2023 Fahim, Cooper, Theivendrampillai, Pham and Straus. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christine Fahim, Y2hyaXN0aW5lLmZhaGltQHVuaXR5aGVhbHRoLnRv