
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 02 May 2023
Sec. Aging and Public Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1067243
This article is part of the Research Topic Personalized Care in Neurological Diseases View all 5 articles
 Mafalda Pernes1
Mafalda Pernes1 Inês Agostinho1
Inês Agostinho1 Rafael A. Bernardes2
Rafael A. Bernardes2 Júlio Belo Fernandes3,4
Júlio Belo Fernandes3,4 Cristina Lavareda Baixinho1,5*
Cristina Lavareda Baixinho1,5*Documentation is an important measure for the management of fall risk because it concentrates the attention of professionals, raises awareness of the existence of fall risk factors, and promotes action to eliminate or minimize them. This study aimed to map the evidence on information to document episodes of falls in older adults. We opted for a scoping review, which followed the Joanna Briggs Institute protocol for this kind of study. The research question that guided the research strategy was “What recommendations emerge from the research on the documentation of falls of the older person?” The inclusion criteria defined were older adults who had at least one fall; nursing documentation after a fall has occurred; and nursing homes, hospitals, community, and long-term care. The search was performed on the following platforms: MEDLINE, CINAHL, Scopus, and Cochrane Database of Systematic Reviews in January 2022 and allowed the identification of 854 articles, which after analysis resulted in a final sample of six articles. The documentation of fall episodes should answer the following questions: Who? What? When? Where? How? Doing what? What was said? What were the consequences? and What has been done? Despite the recommendations for the documentation of fall episodes as a preventive measure for their recurrence, there are no studies evaluating the cost-effectiveness of this measure. Future studies should explore the association between fall documentation, fall recurrence prevention programs, and their impact on the prevalence rate of the second and subsequent falls, as well as the severity of injuries and fear of falling.
Falls are a public health problem for older adults, not only because of their high prevalence in this age group (1–19) but also because of the negative impact they have on functionality, increasing the number of emergency room visits, hospitalizations, co-morbidity, decreased average life expectancy, and mortality rate above 65 years (1–6). Being a transversal accident in the entire context of the life of older adults is more than three times more common in institutionalized older adults (10–16, 18). Other studies have shown that 50.2% of residents suffered at least one fall in the previous year (10, 14), with an average of 1.3 ± 0.48 falls (12) per 1.57 ± 2.78 residents (9).
The cumulative effect of fear of falls, post-fall syndrome, and secondary injuries in a society with an exponential increase in people with neurological disorders and older adults may become epidemic and lead to a consumption of health resources (14). This takes authors to consider falls as a geriatric syndrome not only for people who suffer fractures and who do not regain the functionality they had before falling but also because ptophobia, or fear of falling, leads patients or their caregivers to make some restrictions on activity that conditionate the independence in self-care, over protecting their relative, and making them progressively more dependent on the execution of daily living activities (7–9, 14).
It is unanimous that a cost-effective measure for the prevention of falls is risk identification but also the association of preventive measures appropriate to the individual risk of each person (6–8, 15, 16). A literature review that aimed at identifying the tools used to assess fall risk in institutionalized older adults concludes that the tools with higher predictive value include scales, functional assessment tests, and the question “Did you fall in the last 12 months?” (8). It should be enhanced that this issue has a strong predictive value for the occurrence of new episodes (8), given that the recurrent fall has a variable incidence between 13 and 66.3% (7, 17, 18).
Thus, identifying people who have fallen is crucial because falling is a significant risk for the recurrence of this accident and determining its pattern. In addition, this identification will allow for targeted preventive measures to modifiable risk factors and adopt safety behaviors (14, 19). International recommendations observe that the determination of older adults at greater risk of falling is the first step toward the prevention and, even in those who have already fallen, the determination of the fall mechanism is vital for the implementation of measures for the prevention of recurrent falls (1, 4, 6, 10, 19).
There is a scarce investigation on documentation of episodes of falls and their recurrence. Although there is a recommendation to record all fall episodes, including near-falls, in clinical practice, it is common to identify many episodes of falls that are not witnessed or are witnessed by healthcare professionals and are not recorded in patients' clinical records (8, 9, 14, 19). This issue is even more evident in the community, where most fall episodes occur at the person's home and are not communicated to health professionals. Damián et al. (16) also raise the possibility of underreporting of fall episodes in their study and consider that this underreporting is lower in cases of falls with severe injuries (16). Regarding documentation, when assessing a program to prevent falls in a hospital environment, a team of researchers affirmed that the use of documentation systems, such as care plans and self-records for reporting accidents, can be prevention measures, because they concentrate the attention of professionals, raise awareness for the existence of risk factors of fall, and promote action to eliminate or minimize them (15). Furthermore, prevention protocols recommend that after a fall, healthcare professionals should make a complete evaluation of each incident, with documentation and reporting of all associated factors, following the guidelines of the institution on what measures should be put into practice immediately after a fall (14, 16, 19). Therefore, considering this evidence, this study aimed to map the evidence on information to document episodes of falls in older adults.
Considering the state of the art on the subject and the aim of the study, we opted for conducting a scoping review (SR). This method rapidly maps the key concepts underpinning a research area and the main sources and types of evidence available (20, 21). We followed the Joanna Briggs Institute (JBI) protocol for this type of study (20), which included six steps: (1) identification of the review question, (2) designation of the inclusion and exclusion criteria of studies and identification of relevant studies, (3) selection of the studies, (4) assessment of the level of evidence of the collected literature, according to Joanna Briggs Institute (JBI) guidelines, (5) discussion of the results, and (6) synthesis and presentation of the results obtained (20–22). According to the acronym PCC, the research question was “What recommendations emerge from the research on the documentation of falls in older adults?”
The object of study and the research question guide the definition of the eligibility criteria for the studies included in this SR.
The inclusion criteria defined were as follows:
P—(Population) older adult who had at least one fall;
C—(Concept) nursing documentation after a fall has occurred;
C—(Context) nursing homes, hospitals, community, and long-term care.
The acceptance of studies focusing on the documentation of fall episodes, alone or in association with other interventions, was predefined. Exclusion criteria were studies on the documentation of falls in children and adults and studies on the documentation of risk factors and/or preventive measures of the first fall.
A time limit of 2016 to 2021 was set. This choice is because an initial exploratory search revealed a vast research publication on the topic under study, and researchers are looking for the most current information.
The search was performed on the EBSCOhost platforms (MEDLINE and CINAHL databases), Scopus, and Cochrane Database of Systematic Reviews, in January 2022, for studies in Portuguese, English, and Spanish. First, a search was conducted using Health Sciences descriptors DeCS/MeSH, using keywords built from natural language relative to the theme. Table 1 shows the strategy used in Medline.
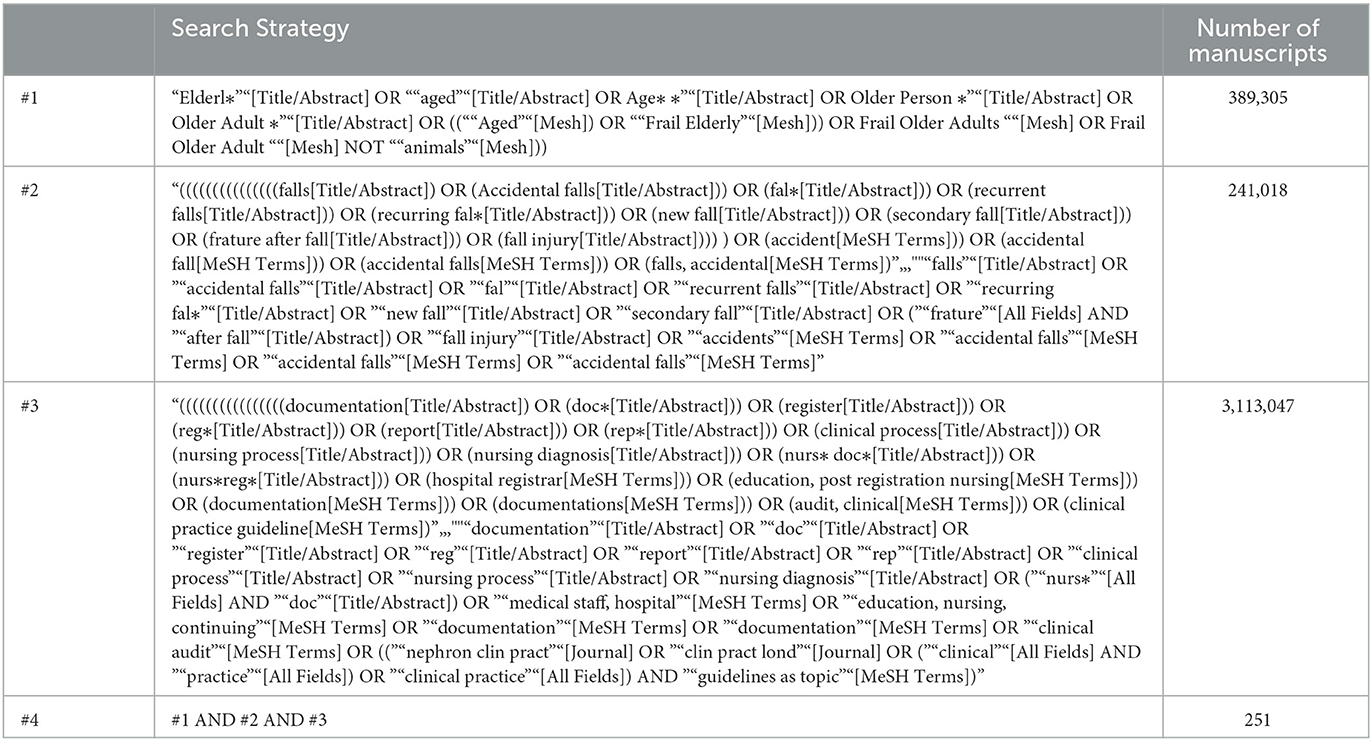
Table 1. Search strategy.
In databases, the descriptors were operationalized using the expressions OR and AND. The search codes were constructed using these expressions.
Afterward, the research was extended to Google Scholar, repositories of theses, and official sites of associations/organizations of reference in the area to identify guidelines and gray literature on the subject.
Data extraction was carried out by two reviewers independently (MP and IA), and doubts and disagreements were resolved with the inclusion of a third reviewer (CLB).
During the extraction phase, the content of the articles was thoroughly analyzed, allowing not only to answer the research question but also to understand whether the studies explored the fall risk and its prevalence, as well as the recurrence of interventions focusing on the documentation of falls.
In order to record the contents extracted from the articles in the final bibliographic sample, researchers elaborated a table using MS Excel that included the following items: identification of the title of the article/document; author(s), publication year, type of article; methods and main results/conclusions. The results of the articles that allowed answering the research question were extracted and submitted to narrative synthesis.
Two reviewers carried out data analysis independently, and all research team members validated the narrative synthesis.
This study includes one of the work packages of a research study on the management of fall risk in older adults that was authorized by an Ethics Committee (PARECER No. CE/IPLEIRIA/46/2020). This is a secondary study that followed the principles of integrity in research. The problem formulation adhered to the principles of clarity, precision, objectivity, and delimitation, allowing its results to contribute to the resolution of a prevalent problem in healthcare, benefiting not only people with neurological diseases but also other older adults at risk of falling.
The study protocol was followed rigorously to ensure the validity of the study. The extraction and analysis of data from the primary study constituents of the bibliographic sample were done with evident respect for the research and results obtained by the other researchers. The reference of the authors who supported the elaboration of this article also followed the recommendations of good academic and scientific practice.
A total of 854 articles were obtained. After removing duplicates (n = 51), reading the titles of the articles (n = 803), abstracts (n = 357), and the complete document (n = 49), we identified three articles that allowed answering the investigation question (Figure 1). The articles were thoroughly read. Articles focusing on recording fall risk or prevention interventions were excluded. The search in Google Scholar and the repositories of theses enabled the identification of 34 documents, which after analysis allowed the integration of three guidelines focusing on information to document fall episodes (Figure 1).
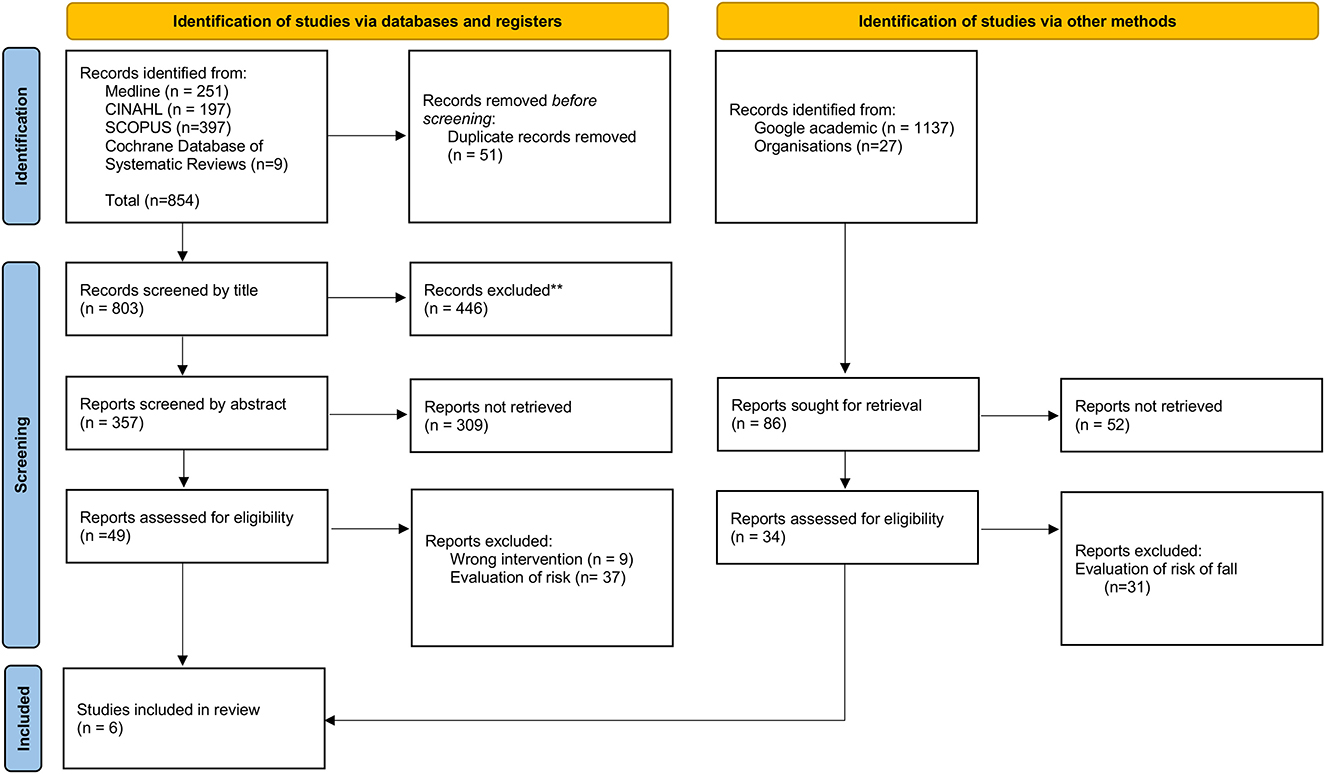
Figure 1. PRISMA-ScR flowchart.
Thus, the bibliographic sample of this SR accounts for six documents (Table 2).

Table 2. Data extraction.
The articles included in this SR show that identifying older adults at risk of falling is the first preventive measure for falls. After a fall, correctly identifying this accident is the first step to preventing its recurrence (23–28).
According to the findings of this review, when a person falls, it is mandatory that the professional who witnessed the fall or to whom the fall was reported, whether by the person himself or by another, registers the notification of the fall while taking into account the following elements (Table 3).
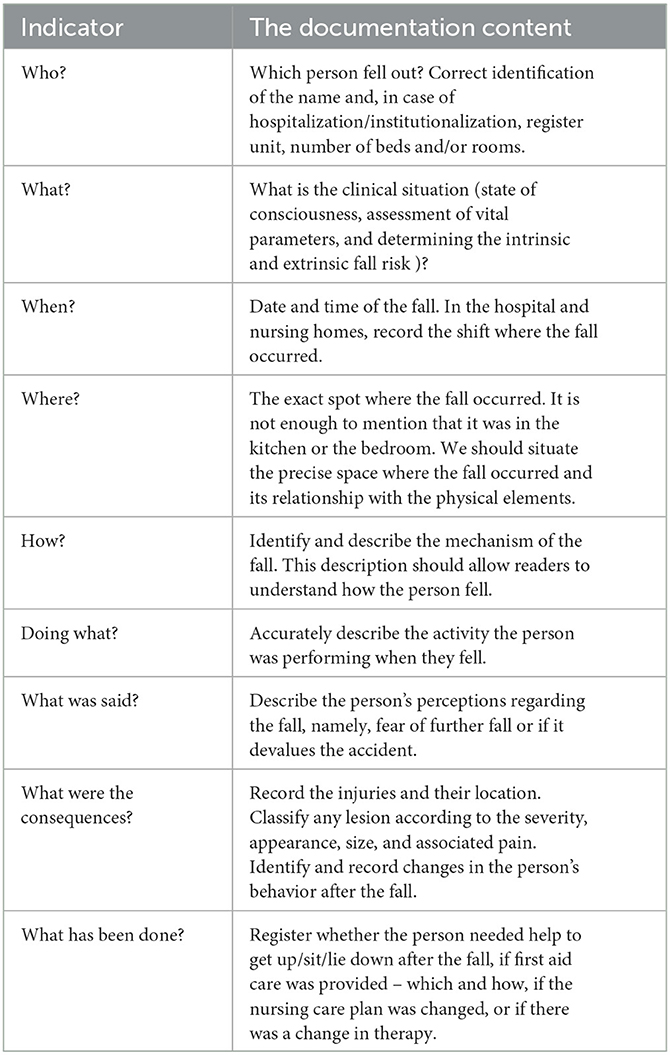
Table 3. What to record after a fall?
Nurses play a key role in maintaining quality care, for whom the responsibility of documenting in detail and with objectivity makes part (29). Unlike the study by Krakau et al. (30), this review found that the fall episode is not always adequately documented, or lacks detail, due to its own complexity.
Many of the factors assessed by nurses (e.g., data related to symptoms, minor injuries, medication, and limitations in daily living activities) are taken into account before, during, and after the fall event but may not always be recorded. For example, Bjarnadottir and Lucero (31) observed that the documentation made by nurses contains critical information for the clinical evaluation of a fall, but that those factors are not always explicitly mentioned. The nursing records, regarding the event of the fall, present clinical consistency, as identified by this review, including the nature and location of possible injuries, sociodemographic data at the time of the event, vital signs, data about the balance and pattern of walking of the person, as well as an overview of the event itself. Therefore, the documentation of the event can be summarized in five major themes: initial evaluation, nursing diagnoses, care goals, nursing interventions, and evaluation (32).
The documentation concerning the fall event, as well as its prevention and therapeutic intervention, follows an interdependent multifactorial structure. Therefore, there are intrinsic and extrinsic factors that the nurse and the multidisciplinary team should consider in the planning of care. This reality is expressed in some guidelines for preventing falls (33), which can also be used to structure the recording of fall events, namely the fall risk assessment, health literacy, strengthening exercises and balance training, and medical devices. It should be noted that documentation is a fundamental strategy for the prevention of these accidents (8) since many of the people who fall have repeated falls at about the same time while doing the same activities. Therefore, it is necessary to understand the fall pattern so that the subsequent falls can be prevented (8, 9, 19). However, documentation is not always easy to achieve, due to ethical, technological, organizational, social, and individual barriers (34). One solution to better documenting fall events involves making Nursing Information System (NIS) cost-effective and more efficient (35). A recent systematic review (36), with important implications for the management of health services, concluded that the correct use of electronic records to document falls reduces the person's risk and improves the identification of the person and associated factors, increasing the quality of care provided. However, using NIS is not always effective, with some studies indicating the omission of up to one-third of the falls that have occurred (37).
As a result of the rapid implementation of the NIS, there is difficulty in standardizing the data and information recorded, reducing the effectiveness of care, especially prevention. Particularly in the documentation of falls, it can be effective to develop models of information, as suggested by some authors (38), allowing to encode variables and factors related to the person, environment, and organization.
We consider that the results of this SR provide valid indicators to be transposed to the NIS to assist nurses and the multidisciplinary team in the rigorous documentation of fall events.
It should be emphasized that this documentation has increased challenges in the community where the fall events occur in a population that is still active and without physical consequences, and the difficulties of access to healthcare or the devaluation of this type of accident make them difficult to report to health professionals (8, 14, 19, 39). Caregivers and family members should be informed about the importance of reporting falls to health professionals in primary healthcare (40). Underreporting of episodes of falls does not allow for early intervention to prevent recurrence (14).
A strength of this review is that it allows the systematization of what should be recorded after a fall, ensuring that the documentation of these episodes is complete and allowing for the individualization of preventive measures to avoid their recurrence. In contrast, the indicators in Table 3 can be used in computer systems that support the clinical practice of healthcare professionals for the registration and extraction of indicators.
The limitations of this review include language restrictions and free access to full text, and some articles that met the pre-established eligible criteria may have been excluded a priori. Another limitation is related to the study's design, which allowed for the mapping of studies on the subject without evaluating their methodological quality.
The six articles included in the SR allow us to answer the aim of the study. After a fall, registration should include the identification of the person who fell, the time of fall, place, mechanism, activity being performed, the consequences of the fall, and what was done after the fall. Exhaustive documentation of the fall and the fear of falling again is a good clinical practice strategy that allows an understanding of the history of the fall (risk factors, mechanism, and consequences) and the introduction of individualized preventive measures that can prevent its recurrence.
The findings from this review allow us to state that there is no randomized controlled trial that associates the documentation practices depending on the history of falls to the occurrence of second or more adverse events. Therefore, we recommend that future studies evaluate the effectiveness of documentation of episodes of falls in preventing their recurrence, preventive measures adopted, and the control of fear of falls. We also recommend that stakeholders develop training programs that allow healthcare professionals to gain a deeper understanding of documenting falls and use data from these records to create tailored care plans to prevent falls' recurrence.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
CB: conceptualization, resources, supervision, project administration, and funding acquisition. MP, IA, and CB: methodology and software. MP, IA, RB, JB, and CB: validation, data curation, writing—reviewing and editing, investigation, and visualization. MP, IA, RB, and CB: formal analysis and writing—original draft preparation. All authors contributed to the article and approved the submitted version.
This publication was financed by national funds through the FCT—Foundation for Science and Technology, I.P., under the project UIDB/04585/2020.
This publication is financed by national funds through the FCT-Foundation for Science and Technology, I.P., under the project UIDB/04585/2020. The researchers would like to thank the Centro de Investigação Interdisciplinar Egas Moniz (CiiEM) for the support provided for the publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Battaglia G, Giustino V, Messina G, Faraone M, Brusa J, Bordonali A, et al. Walking in natural environments as geriatrician's recommendation for fall prevention: preliminary outcomes from the “passiata day” model. Sustainability. (2020) 12:2684. doi: 10.3390/su12072684
2. Fernandes JB, Teixeira F, Godinho C. Personalized care and treatment compliance in chronic conditions. J Pers Med. (2022) 12:737. doi: 10.3390/jpm12050737
3. Ehrhardt A, Hostettler P, Widmer L, Reuter K, Petersen JA, Straumann D, et al. Fall-related functional impairments in patients with neurological gait disorder. Sci Rep. (2020) 10:21120. doi: 10.1038/s41598-020-77973-4
4. World Health Organization Falls—Key Facts. (2018) Available online: https://www.who.int/news-room/fact-sheets/detail/falls (accessed January 22, 2021).
5. Fernandes JB, Fernandes SB, Almeida AS, Vareta DA, Miller CA. Older adults' perceived barriers to participation in a falls prevention strategy. J Pers Med. (2021) 11:450. doi: 10.3390/jpm11060450
6. Liu-Ambrose T, Davis JC, Best JR, Dian L, Madden K, Cook W, et al. Effect of a home-based exercise program on subsequent falls among community-dwelling high-risk older adults after a fall: a randomized clinical trial [published correction appears in JAMA. JAMA. (2019) 321:2092–100. doi: 10.1001/jama.2019.5795
7. Xu, T., Clemson, L., O'Loughlin, K., Lannin, N.A., Dean, C., Koh, G. Risk factors for falls in community stroke survivors: a systematic review and meta-analysis. Arch Phys Med Rehabil. (2018) 99:563–73. doi: 10.1016/j.apmr.2017.06.032
8. Panneman MJM, Sterke CS, Eilering MJ, Blatter BM, Polinder S, Van Beeck EF, et al. Costs and benefits of multifactorial falls prevention in nursing homes in the Netherlands. Exp Gerontol. (2021) 143:111173. doi: 10.1016/j.exger.2020.111173
9. Vlaeyen E, Poels J, Colemonts U, Peeters L, Leysens G, Delbaere K, et al. Predicting falls in nursing homes: a prospective multicenter cohort study comparing fall history, staff clinical judgment, the care home falls screen, and the fall risk classification algorithm. J Am Med Dir Assoc. (2021) 22:380–7. doi: 10.1016/j.jamda.2020.06.037
10. Baixinho CL, Bernardes RA, Henriques MA. How to evaluate the risk of falls in institutionalized elderly people. REV BAIANA ENFERM. (2020) 34:e34861. doi: 10.18471/rbe.v34.34861
11. Ferreira L, Ribeiro K, Jerez-Roig J, Araújo J, Lima KC. Recurrent falls and risk factors among institutionalized older people. Cien Saude Colet. (2019) 24:67–75.
12. Cameron EJ, Bowles S, Marshall EG, Andrew MK. Falls and long-term care: a report from the care by design observational cohort study. BMC Fam Pract. (2018) 19:73. doi: 10.1186/s12875-018-0741-6
13. Castaldo A, Giordano A, Incalzi R, Lusignani M. Risk factors associated with accidental falls among Italian nursing home residents: A longitudinal study. (FRAILS) Geriatr Nurs. (2020) 41:75–80. doi: 10.1016/j.gerinurse.2019.06.003
14. Baixinho CL, Dixe MA. Team practices in fall prevention in institutionalized elderly people: scale design and validation. Texto contexto - enferm. (2017) 26:e2310016. doi: 10.1590/0104-07072017002310016
15. Healey F, Monro A, Cockram A, Adams V, Heseltine D. Using targeted risk fator reductionto prevent falls in older in-patients: a randomised controlled trial. Age Ageing. (2004) 33:390–5. doi: 10.1093/ageing/afh130
16. Damián J, Pastor-Barriuso R, Valderrama-Gama E, Pedro-Cuesta J. Fators associated with falls among older adults living in institutions. BMC Geriatr. (2013) 13:6. doi: 10.1186/1471-2318-13-6
17. Moraes SA, Soares WJ, Ferriolli E, Perracini MR. Prevalence and correlates of dizziness in community-dwelling older people: a cross sectional population based study. BMC Geriatr. (2013) 13:4. doi: 10.1186/1471-2318-13-4
18. Nurmi IS, Luthje PM, Kataja JM. Long-term survival after falls among the elderly in institutional care. Arch Gerontol Geriatr. (2004) 38:1–10. doi: 10.1016/S0167-4943(03)00079-7
19. Baixinho CRSL, Dixe MACR, Henriques MAP. Falls in long-term care institutions for elderly people: protocol validation. Rev Bras Enferm. (2017) 70:740–6. doi: 10.1590/0034-7167-2017-0109
20. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Social Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
21. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aroamtaris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. (2018) 18:143. doi: 10.1186/s12874-018-0611-x
22. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews. (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
23. Krakau K, Andersson H., Dahlin Å. F., Egberg L., Sterner E., Unbeck M. (2021). Validation of nursing documentation regarding in-hospital falls: a cohort study. BMC Nursing. (2021) 20:14–27. doi: 10.1186/s12912-021-00577-4
24. Yang Y, Komisar V, Shishov N, Lo B, Korall AMB, Feldman F, et al. The effect of fall biomechanics on risk for hip fracture in older adults: a cohort study of video-captured falls in long-term Care. J Bone Mineral Res. (2020) 35:1914–22. doi: 10.1002/jbmr.4048
25. Montgomery CD, Pereira DE, Hatcher JB, Kilbury D, Ballance S, Bradham T, et al. Improving the assessment and documentation of patient mobility using a quality improvement framework. Geriatr Nurs. (2021) 42:325–30. doi: 10.1016/j.gerinurse.2021.01.002
26. Moncada LVV, Mire LG. Preventing falls in older persons. Am Fam Physician. (2017) 96:240–7. Available online at: https://www.aafp.org/afp/2017/0815/afp20170815p240.pdf
27. National Falls Prevention Coordination Group. (NFPCG). Guidance: Falls and Fractures: Consensus Statement and Resources Pack. London: PHE publications. (2017).
28. Direção Geral S. Norma DGS - Prevenção e Intervenção na Queda do Adulto em Cuidados Hospitalares. Lisboa: DGS. (2019).
29. Oldland E, Hutchinson AM, Redley B, Mohebbi M, Botti M. Evaluation of the validity and reliability of the nurses' responsibility in healthcare quality questionnaire: an instrument design study. Nurs Health Sci. (2021) 23:525–37. doi: 10.1111/nhs.12844
30. Krakau K, Andersson H, Dahlin AF, Egberg L, Sterner E, Unbeck M, et al. Validation of nursing documentation regarding in-hospital falls: a cohort study. BMC Nurs. (2021) 20:58.
31. Bjarnadottir RI, Lucero RJ. What can we learn about fall risk factors from HER nursing notes? A text mining study. EGEMS. (2018) 6:21. doi: 10.5334/egems.237
32. Moldskred PS, Snibsoer AK, Espehaug B. Improving the quality of nursing documentation at a residential care home: a clinical audit. BMC Nurs. (2021) 20:103. doi: 10.1186/s12912-021-00629-9
33. Schoberer D, Breimaier HE, Zuschnegg J, Finding T, Schaffer S, Archan T, et al. Fall prevention in hospitals and nursing homes: clinical practice guideline. Worldviews Evid Based Nurs. (2022) 19:86–93. doi: 10.1111/wvn.12571
34. Bjerkan J, Valderaune V, Olsen RM. Patient safety through nursing documentation: barriers identified by healthcare professionals and students. Front. Comput. Sci. (2021) 3:624555. doi: 10.3389/fcomp.2021.624555
35. Jin Y, Kim H, Jin T, Lee SM. Automated fall and pressure injury risk assessment systems: nurses' experiences, perspectives, and lessons learned. Comput Inform Nurs. (2021) 39:321–8. doi: 10.1097/CIN.0000000000000696
36. Saraswasta IWG, Hariyati RTS. A systematic review of the implementation of electronic nursing documentaiton toward patient safety. Enferm Clin. (2021) 31:S205–9. doi: 10.1016/j.enfcli.2020.12.023
37. Trinh LTT, Achat H, Assareh H. Use of routinely collected data in reporting falls in hospitals in a local health district in New South Wales, Australia. Health Inf Manag. (2017) 46:15–22. doi: 10.1177/1833358316653490
38. Lytle KS, Westra BL, Whittenburg L, Adams M, Akre M, Ali S, et al. Information models offer value to standardize electronic health record flowsheet data: a fall prevention exemplar. J Nurs Scholarsh. (2021) 53:306–14. doi: 10.1111/jnu.12646
39. Iamtrakul P, Chayphong S, Jomnonkwao S, Ratanavaraha V. The association of falls risk in older adults and their living environment: a case study of rural area, Thailand. Sustainability. (2021) 13:13756. doi: 10.3390/su132413756
Keywords: accidental falls, aged, documentation, clinical audit, recurrent falls, risk
Citation: Pernes M, Agostinho I, Bernardes RA, Belo Fernandes J and Baixinho CL (2023) Documenting fall episodes: a scoping review. Front. Public Health 11:1067243. doi: 10.3389/fpubh.2023.1067243
Received: 12 October 2022; Accepted: 27 February 2023;
Published: 02 May 2023.
Edited by:
Antonino Patti, University of Palermo, ItalyReviewed by:
Valerio Giustino, University of Palermo, ItalyCopyright © 2023 Pernes, Agostinho, Bernardes, Belo Fernandes and Baixinho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Lavareda Baixinho, Y3JiYWl4aW5ob0Blc2VsLnB0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.