
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 02 June 2023
Sec. Public Health Education and Promotion
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1056999
 Dorothy O. Asante1,2,3†
Dorothy O. Asante1,2,3† Anran Dai2,3†
Anran Dai2,3† Anita N. Walker4†Zhou Zhou3†Senam A. Kpogo5
Anita N. Walker4†Zhou Zhou3†Senam A. Kpogo5 Rongzhu Lu1*Kaizong Huang3*
Rongzhu Lu1*Kaizong Huang3* Jianjun Zou3*
Jianjun Zou3*Objective: Low awareness of hypertension and diabetes is a public health concern in Ghana. Assessing the general population’s behaviour via knowledge, attitude, and practice (KAP) will be invaluable in these diseases, where prevention and control need a lifelong commitment to a healthy lifestyle. Hence, our goal was to assess the behaviour of Akatsi South residents towards the diseases to assist health providers in implementing tailored intervention programs.
Methods: This was a population-based cross-sectional study with 150 adults (18–70 years) from November to December 2021. A semi-structured questionnaire with face-to-face interviews was used to obtain data. All variables in the model had descriptive statistics. The Chi-square (χ2) test was used to examine correlations between variables, and a value of p < 0.05 was considered statistically significant. The factors associated with checking blood sugar levels and blood pressure were determined using binary logistic regression.
Results: The respondents’ mean age and BMI were 32.40 years (± 12.07) and 24.98 kg/m2 (± 2.36), respectively. Only 46.67% of the respondents frequently monitor their blood pressure and 17.33% their blood glucose (at least once a year). Less than half of those surveyed had a good knowledge of hypertension (42.7%) and diabetes (32.0%), whereas nearly 3/4 had poor attitudes regarding both conditions. A binary logistic regression analysis revealed that having a good attitude toward hypertension (exp B = 2.479, p = 0.036) and diabetes (exp B = 4.547, p = 0.009) were the participants’ strongest predictor of blood pressure and sugar level checks. However, being overweight (exp B = 0.046, p = 0.002,) or obese (exp B = 0.144, p = 0.034) negatively influenced the frequency with which our respondents checked their blood glucose levels.
Conclusion: In the study, we found that the population generally has poor knowledge, which affects their behaviour (attitudes and practices) towards the diseases. To enable healthcare practitioners to reduce disease-associated mortality and morbidity in the future, frequent public health education and promotion about the conditions is critical to closing the knowledge gap.
Non-communicable diseases (NCDs) are chronic, life-long disorders resulting from a combination of environmental, genetic, behavioural, and physiological factors. Globally, NCDs claim the lives of 41 million people annually, with 77% occurring in low and middle-income countries (LMICs) (1, 2). Hence, they are predicted to overtake infectious diseases as the leading cause of premature mortality and morbidity by 2030 (3, 4). Hypertension (HT) and diabetes (DM) are two of the most common NCDs worldwide and are major risk factors for diseases like stroke and kidney disease. They are considered silent killers because they impair health without showing symptoms (5, 6). According to WHO, an estimated 1.28 billion adults (30–79 years) globally have HT, with 2/3 living in LMICs. The International Diabetes Federation (IDF), on the other hand, revealed that in 2021, 537 million adults (1 in 10 adults aged 20–79) had diabetes, with more than 3/4 coming from LMICs (2, 7).
A significant percentage of the global burden of HT and DM can be attributed to the recent epidemiological shift from communicable to non-communicable diseases across Africa (8), and Ghana is no exception. In Ghana, over one out of four adults (i.e., a prevalence rate of 27%) have HT (9), whereas 2–9% have DM (10, 11), thereby ranking them among the top 10 causes of death in the country (12). Minimizing the number of people who die from early-stage disease is therefore crucial and achievable if individuals have adequate knowledge, good attitudes, and practices towards the illness (13). Studies, however, show that approximately half of the hypertensive and one-third of diabetic individuals have not been diagnosed and are unaware of their conditions, respectively, (14, 15). The prevalence of HT and DM in Ghana varies in urban and rural areas, with low awareness levels. For example, a study in Keta Municipality (which borders our study district) found that rural residents had a higher HT prevalence with lower awareness than urban residents (16).
Specific interventions can be evaluated using knowledge, attitudes, and practices (KAPs) questionnaires. Awareness is the initial disease prevention strategy development stage (5). To assist in implementing initiatives and strategies for successful public health education, exploring the KAPs among the general population is crucial. However, there needs to be more research examining KAPs among the general population, especially in rural areas where HT and DM are on the rise. Those that exist focus on the KAP of diabetic and/or hypertensive patients towards their disease and management, whereas others focus on one condition, particularly hypertension, and its awareness (16). Inadequate or poor knowledge, bad attitudes, and practices toward these diseases will continue to rise as long as the general populace remains uneducated. Hence, exploring KAPs with the general public will help fill the knowledge gap reducing inpatient care and improving clinical outcomes.
As far as we know, research has yet to use KAP questionnaires to investigate the behaviour of the general population regarding HT and DM in a rural Ghanaian community or district. Based on the previous prediction model (17), we explored using simple KAP questions to understand the behaviour of the residents in Akatsi South District towards these diseases to assist healthcare providers in streamlining specific, targeted, and effective intervention programs.
Akatsi South District has a population of 98,684. 46.1% (45,497) of males and 53,187 females (53.9%). However, with a reported 2.4% annual growth rate, the population is predicted to reach 131,174 by 2022 (18). Akatsi is the sole urban town among the 20 main settlements in the district. Rural towns house two-thirds of the district’s population. The district had a crude death rate of 9.2, compared to 8.8 for the region in 2010. There are 29 healthcare facilities with malaria, acute and upper respiratory tract infections, hypertension, rheumatism and joint pains, anaemia, and skin diseases among the top 10 diseases in the district (18, 19).
Residents of the twenty major localities (Akatsi, Wute, Agbedrafor, Avenorpedo, Torve, Avenorpeme, Gefia, Dzogadze, Nyitawuta, Dagbamate, Avashive, Tsigbene, Lawui-Avedzi, Klokpe, Apeyime, Xavi, Guiga, Ngblebi, Adeheta, and Atidzive) who were between the ages of 18–70 and gave their consent to participate in the study were included. We excluded those seriously ill, residents who did not consent to participate, and pregnant or nursing mothers from the survey.
A multi-stage sampling strategy is shown in the sections below. We used this strategy to get the data.
The district coverage area was used to determine the study’s baselines and to correlate with prior predictions. The coverage areas were stratified into two groups. Each group included two notable nucleated settlements (Wute, Avenorpeme, Gefia, and Avenorpedo). Group 1 consisted of Akatsi, Wute, Gefia, Klokpe, Avashive, Lawui-Avedzi, Guiga, Ngblebi, Adeheta, and Atidzive, while Xavi, Avenorpedo, Avenorpeme, Torve, Agbedrafor, Dzogadze, Nyitawuta, Dagbamate, Apeyime, and Tsigbene made up Group 2.
Households were chosen at random for each area. A point of focus was located within every community, and the interviewer used an iPhone compass to identify their direction while standing at the central location. The interviewer entered the first house facing them. If a household had more than one qualified respondent, one was randomly chosen and interviewed. The exit was followed by a visit to a nearby building whose entrance faced the previous. Interviews were conducted with no more than two eligible individuals (aged 18–70, male or female). We selected Seven first responders from each community. However, in a crowded area like a market, we chose just 2% of the projected eligible population at random. Finally, 150 inhabitants were selected and interviewed based on the same eligibility criteria and sampling method.
While a large sample size may raise ethical concerns and time and money waste, a small sample size may cause misrepresentation, inefficiency, and results that are not statistically significant. Because of this, we used the scientific approach to ensure that our sample size was optimum for our study. Ultimately, our sample size met the criteria for efficiency, representativeness, validity, and flexibility (20). To estimate the sample size (21), we used the formula below:
Where, z (z score) = 1.96 at 95% confidence level.
d (the precision around the population mean) = 10%.
p (prevalence) = 55% and.
q = (1-p).
n = 95.
Applying a non-response rate of 5% to the minimum sample size increases the number of participants to 100. As a result, 100 participants were considered the bare minimum for the study. Hence, our sample size of 150 participants was sufficient for the analysis.
The District Health Directorate, Ghana Health Service’s NCD prevention and control program, and comparable publications (5, 8, 16) guided the questionnaire’s essential questions. We interviewed three health education and health promotion experts and non-infectious disease experts in a face-to-face and a group discussion to assess the tool’s face validity. Their opinions on the questionnaire’s difficulty, adequacy, the ambiguity of expressions, and insufficiency in meanings were considered.
Four experts in health education, health promotion, and non-infectious diseases were asked for qualitative content validity. After studying the tool, they wrote down their corrections for each item. Content validity was quantified using the content validity ratio (CVR) and index (CVI). The questionnaire’s total CVR score was 0.81–0.84 for knowledge, 0.89 for attitude, and 0.92 for practice, according to 4 experts. The CVI value for all questionnaire sections was derived by averaging the questions of each component, with knowledge 0.84, attitude 0.88, and practice 0.85. The questionnaire’s CVI was 0.86.
To measure reliability, we used a re-test strategy. For this reason, we provided 20 people with the verified questionnaire. After waiting a week, they were given another chance to complete the questionnaires. Overall, the questionnaire’s reliability was 0.86 (0.83 for knowledge, 0.90 for attitude, and 0.86), within the acceptable range. Finally, the tool was a questionnaire with 16 questions divided into three parts.
Educated health workers assisted in the data collection. We completed participating member input before data collection—an interviewer-administered a semi-structured questionnaire to collect data for the study. Three sections make up the survey. Section 1: Personal information; Section 2: Anthropometric measurements (weight, height, and BMI); and Section 3: nineteen (19) essential questions: hypertension knowledge (6 questions), hypertension attitude (3), diabetes knowledge (7 questions), diabetes attitude (3).
For the practice aspect, one question each enquiring about the frequency of checking blood pressure and blood glucose was used. The response to the practice was measured with “at least once every year,” “rarely,” or “never checkers.” Then, “at least once every year” were categorized as frequent checkers, while “rarely” or “never checkers” were categorized as infrequent checkers. The knowledge and attitude aspect were collected with a validated and reliable assessment questionnaire based on the WHO STEPWISE strategy to monitor non-communicable conditions.
The knowledge covered lifestyle modifications, risk factors, complications, prevention, and/or control. It was evaluated with “True,” “False,” and “I do not know.” Correct responses were coded as 1, while wrong answers were re-coded as 0. The responses were then summed, and a score of 6 for hypertension and 7 for diabetes could be obtained. After this, a score of more than half was denoted as knowledgeable about diabetes or hypertension. It has been observed that the reliability and validity of the knowledge evaluation questionnaire linked to the risk factors for chronic lifestyle illnesses are acceptable. Based on the findings of Frantz (22), the knowledge evaluation questionnaire possesses good and adequate psychometric qualities, as evidenced by its Cronbach Alpha coefficient of 0.80.
The attitude aspect consisted of questions regarding behaviours that could increase or reduce the risk of diabetes and hypertension. This aspect was evaluated with Yes or No. The right attitude towards reducing risk factors of diabetes and hypertension was re-coded as 1, while the opposite was re-coded as 0. The scores were summed, and a participant with a score of at least 2 was regarded as having a good attitude toward the condition. The dependent variables were “checking for blood glucose and blood pressure.” At the same time, the independent variables were knowledge and attitude towards hypertension and diabetes, family history of diabetes, family history of hypertension, and BMI.
We used a physician’s scale (Zhongshan Camry Electronic Co. Ltd., Guangdong, China) to record the respondents’ weights. Participants were asked to weigh themselves while wearing light clothing and no shoes, and we recorded the results to the nearest 0.5 kilograms (1.1 pounds). To ensure that the data collected was correct, we calibrated all measurement instruments before we used them for the first time.
Participants’ heights were measured accurately to within 0.1 centimeters using a Stadiometer. Weight in kilograms (kg) divided by height in meters squared (m2) was used to compute BMI (kg/m2). We categorized the BMI ranges according to the National Institute of Health (NIH) and World Health Organization (WHO) guidelines for white, Hispanic, and black adult individuals (23) as shown in Figure 1. Figure 1 shows the (A) Body Mass Index (BMI) table for white, Hispanic, and black people based on National Institute of Health and World Health Organization guidelines, and (B) The Practical Guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults (NIH Publication No. 00–4,084) (24).
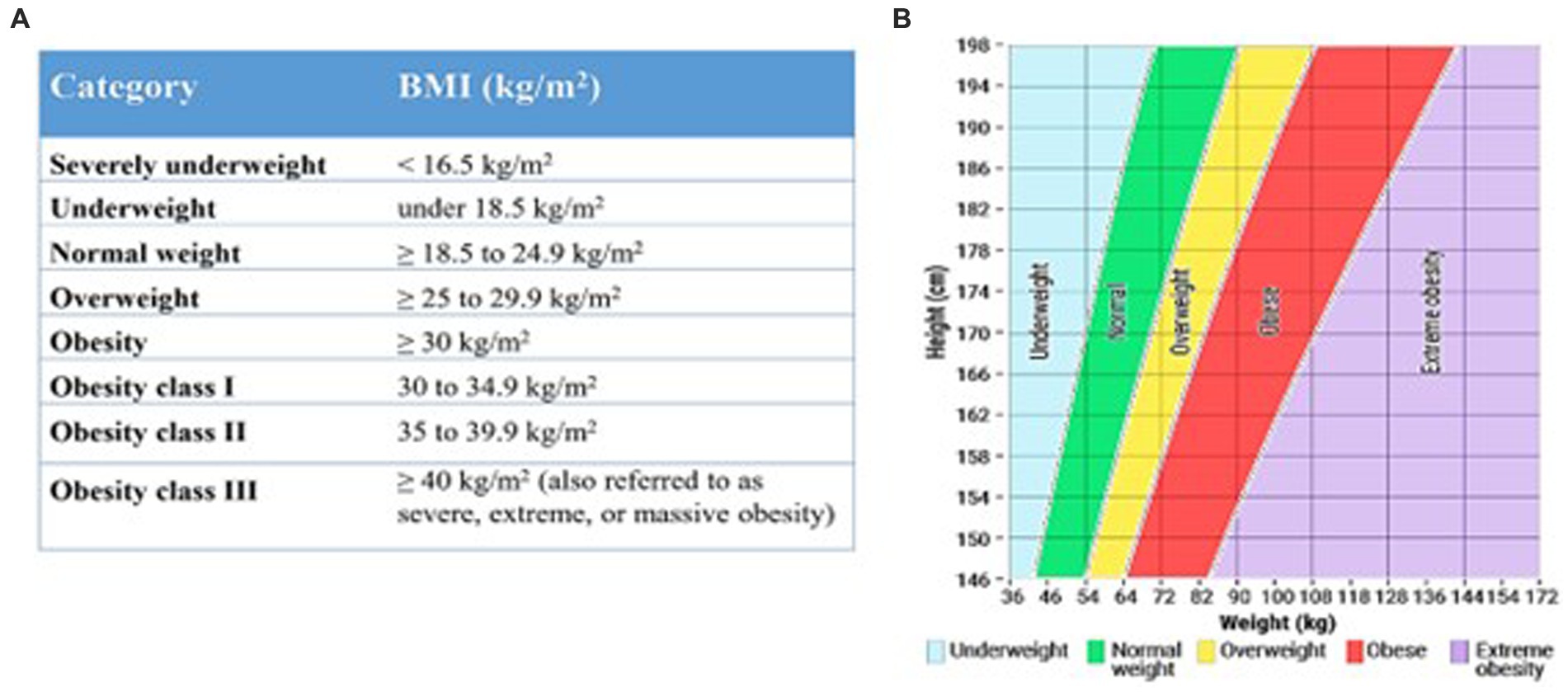
Figure 1. BMI ranges according to the National Institute of Health (NIH) and World Health Organization (WHO) guidelines for white, Hispanic, and black adult individuals.
As the research team was present at all sites, they were obligated to acquire informed permission. The interviewer read and checked the verbal questionnaire with the study respondent. Informed consent was offered in English, the official language, but interpretation in the local language, “Ewe,” was available for clearer understanding. Participants could quit at any time if they felt uncomfortable.
Version 26 of the Statistical Package for the Social Sciences (SPSS) was used for data entry and analysis. We provided descriptive statistics for all of the variables in the model. Means and standard deviations were used to summarize quantitative (continuous) data, whereas we used frequencies and percentages for qualitative (categorical) data. The Chi-square (χ2) test was used to examine correlations between variables. The factors associated with checking blood sugar levels and blood pressure were determined using binary logistic regression. The main factors established in other literature to affect the checking of blood glucose and sugar level were used in the model; hence, they were not adjusted. A p < 0.05 was considered statistically significant.
Before beginning the study, we requested ethical permission from the Ghana Health Service Ethical Review Committee. Approval number: GHS-ERC: 17/02/2020. The District Health Directorate granted authorization after the researcher informed them of its objectives. We explained the project’s involvement to each participant verbally. There was little or no risk to participants since the study was not intrusive and collected no identifiable information. Participation in this study was free of charge to the participants, and they were not compensated.
Table 1 provides an overview of the demographics of the survey participants. A total of 150 people were interviewed, with the majority of the participants being females, 56.0%. About 54.0% of the participants had basic or primary education while 15.3% had no formal education with less than a quarter (19.3%) having tertiary education. Of most participants, 40% were non-manual workers who engaged in domestic livestock farming, retail sales, crafts, and associated trades, service and sales, and domestic work.
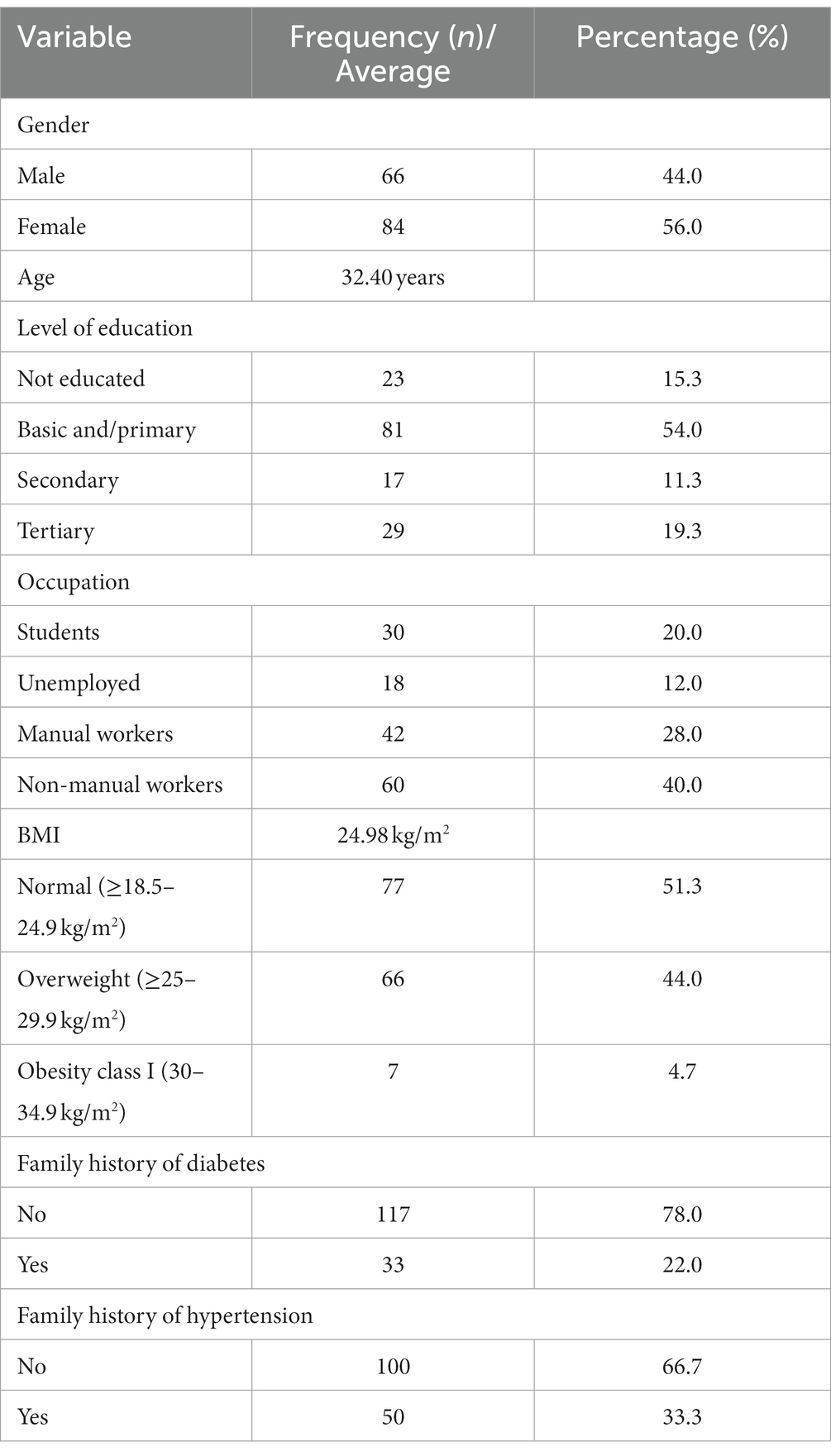
Table 1. Demographic characteristics of the respondents in the survey, N = 150.
Additionally, fewer than one-fourth worked in manual labour, primarily in the fields of skilled agriculture, forestry, and fishing work, as well as carpentry and construction work. But 20.0% were students, mostly at university level, with the majority unemployed or not engaged in any manual or non-manual work. Furthermore, 33.3 and 22.0% had a family history of hypertension and diabetes, respectively. However, 4.7% participants had BMIs in obesity class I, 51.3% had normal BMIs, and over one-third were overweight. Finally, the average age and BMI of the participants were 32.40 years and 24.98 kg/m2, with standard deviations of 12.07 and 2.36, respectively.
Figure 2A shows the respondents’ general knowledge and lifestyle practices related to high blood pressure (HBP), Figure 2B shows the respondents’ general knowledge and lifestyle practices related to blood glucose level (BGL), and Figure 2C show the respondents’ general attitude towards both diseases. 85.3 and 59.3% participants had heard of HT and DM, respectively. Most respondents (87.3%) said that becoming older increases your risk of developing HT and DM. 58.7 and 42.7% of the participants also answered that gender and unhealthy lifestyles are risk factors for both diseases, respectively, with only a quarter of the participants, 25.3%, stating that family history also puts you at risk.
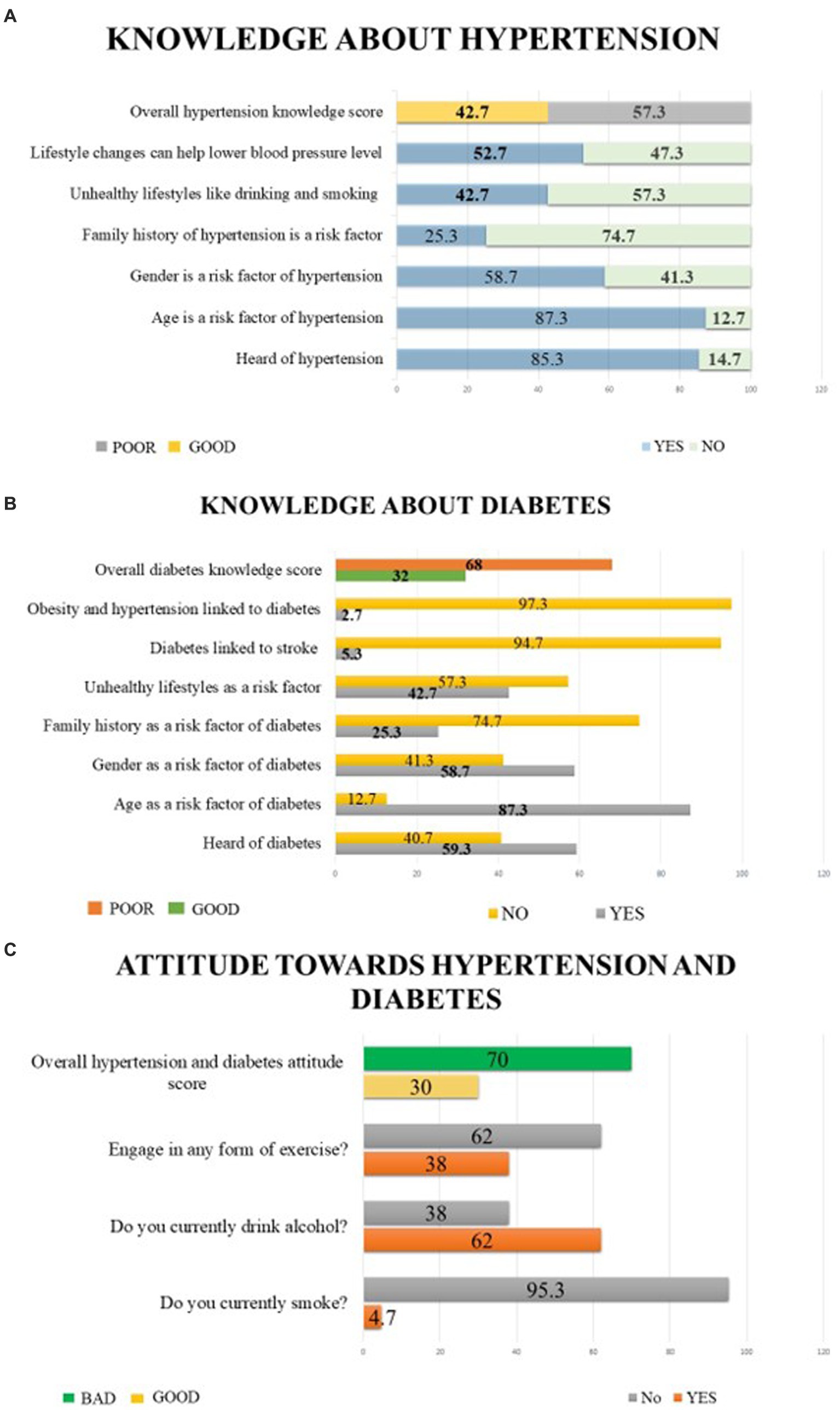
Figure 2. Respondents’ general knowledge, lifestyle practices and attitudes related to high blood pressure (HBP) and blood glucose level (BGL). (A) Respondents’ general knowledge and lifestyle practices related to hypertension, (B) Respondents’ general knowledge and lifestyle practices related to diabetes, (C) Respondents’ general attitude toward both diseases.
We also indicated lifestyle changes as a measure to help reduce HBP by 52.7% of the respondents. Only 2.7 and 5.3% participants knew obesity and HT are linked to DM, and DM is related to stroke. Furthermore, less than two-fourths of those surveyed were knowledgeable about HT, its modifiable and non-modifiable risk factors, and preventative strategies based on lifestyle changes. On the other hand, just 32% of those surveyed were knowledgeable about DM, its risk factors, and complications. Concerning attitudes towards both diseases, only 4.7% participants smoked, while more than half (62.0%) drank alcohol. Finally, only 38.0% of the surveyed respondents were engaged in some form of exercise. Nearly three-fourths of the participants had bad attitudes regarding HT and DM.
Table 2 shows the chi-square or Kruskal-Wallis test to see how our respondents’ demographic characteristics, knowledge, and attitudes varied regarding checking for blood pressure and blood sugar levels. Blood pressure checking varied across age (χ2 = 8.609, p =0 0.003), education (χ2 = 5.091, p = 0.024), occupation (χ2 = 7.484, p = 0.009), BMI (χ2 = 8.740, p = 0.025), family history of diabetes (χ2 = 4.592, p = 0.032), knowledge about hypertension (χ2 = 19.106, p < 0.001) and diabetes (χ2 = 19.965, p < 0.001), and both for attitude towards diabetes and hypertension (χ2 = 4.592, p-value = 0.032). Here, non-manual workers, those with basic or primary education, those aged 26 years and above, and obese individuals checked their blood pressure frequently. Inversely, more than half of the people who had poor knowledge about diabetes and hypertension, as well as those who had a bad attitude towards hypertension and diabetes, were less likely to monitor their blood pressure.
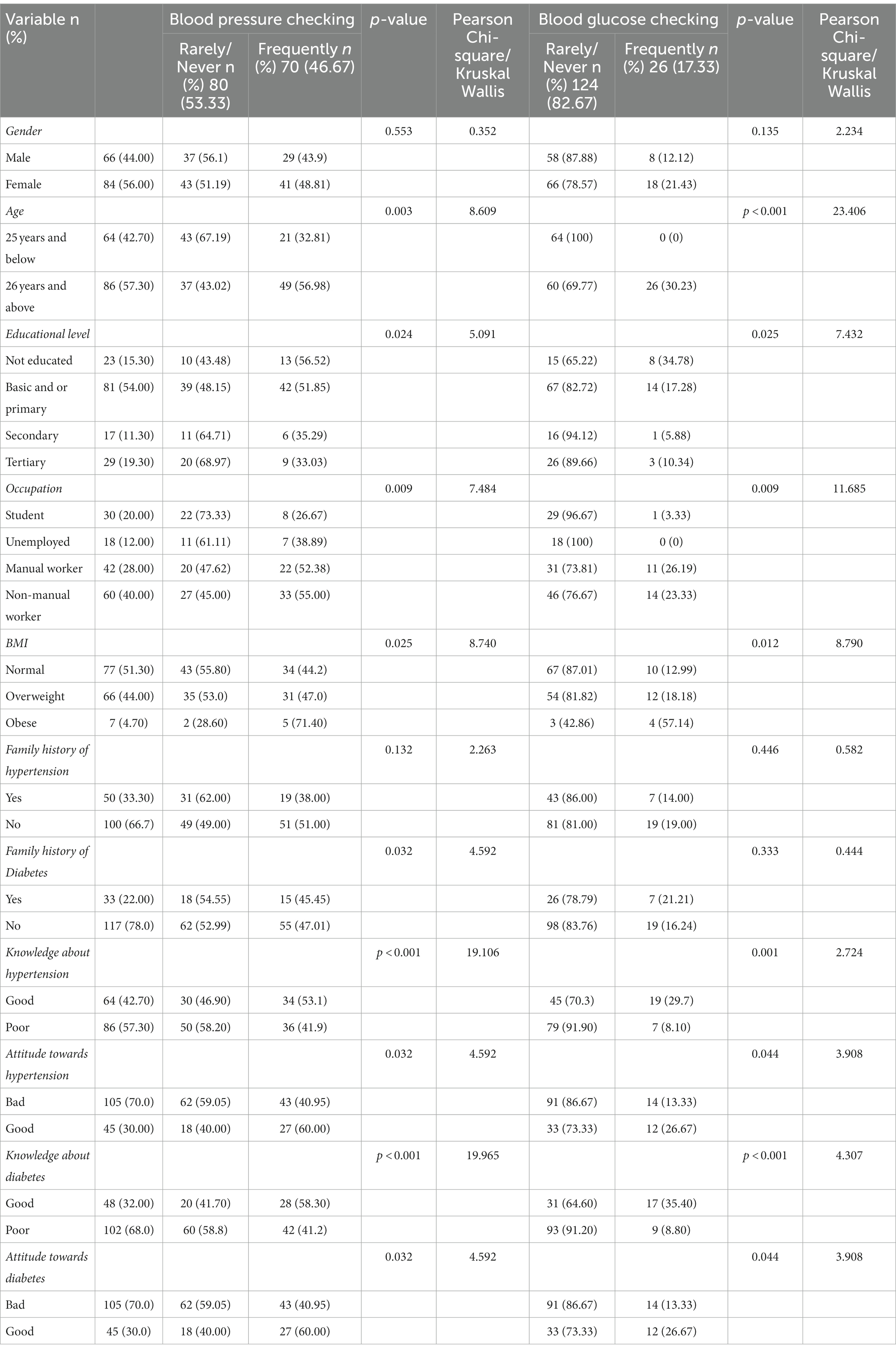
Table 2. Results of how often participants check their blood pressure level (BPL) and blood glucose level (BGL) in a year varies across demographic characteristics, knowledge and attitude using Chi square test or Kruskal Wallis test.
Similarly, except for gender, and family history of hypertension and diabetes, checking of blood sugar levels varied significantly across all other variables. Thus, BMI (χ2 = 8.790, p = 0.012), attitude towards hypertension and diabetes (χ2 = 3.908, p = 0.044), age (χ2 = 23.406, p < 0.001), education (χ2 = 7.432, p-value =0 0.025), occupation (χ2 = 11.685, p-value =0 0.009), knowledge about hypertension (χ2 = 2.724, p-value =0 0.001), and knowledge about diabetes (χ2 = 4.307, p < 0 0.001). Except for obese individuals, all other individuals were less likely to check their BGL frequently.
In the binary logistic regression analysis in Table 3, having a good attitude toward hypertension (exp B = 2.479, p = 0.036) was the strongest predictor of blood pressure checks among our participants. However, being overweight (exp B = 0.040, p = 0.010) and being knowledgeable about hypertension (exp B = 0.024, p = 0.001) negatively affected checking of blood pressure. On the other hand, as shown in Table 4, BMI group (overweight – exp. B = 0.046, p = 0.002) and (obese – exp. B = 0.144, p = 0.034) were negatively affected, while having a good attitude toward diabetes positively influenced the frequency with which our respondents checked their blood glucose levels (exp B = 4.547, p = 0.009). However, knowing about diabetes or having a family history of the disease had no effect on how often our respondents checked their blood sugar levels.
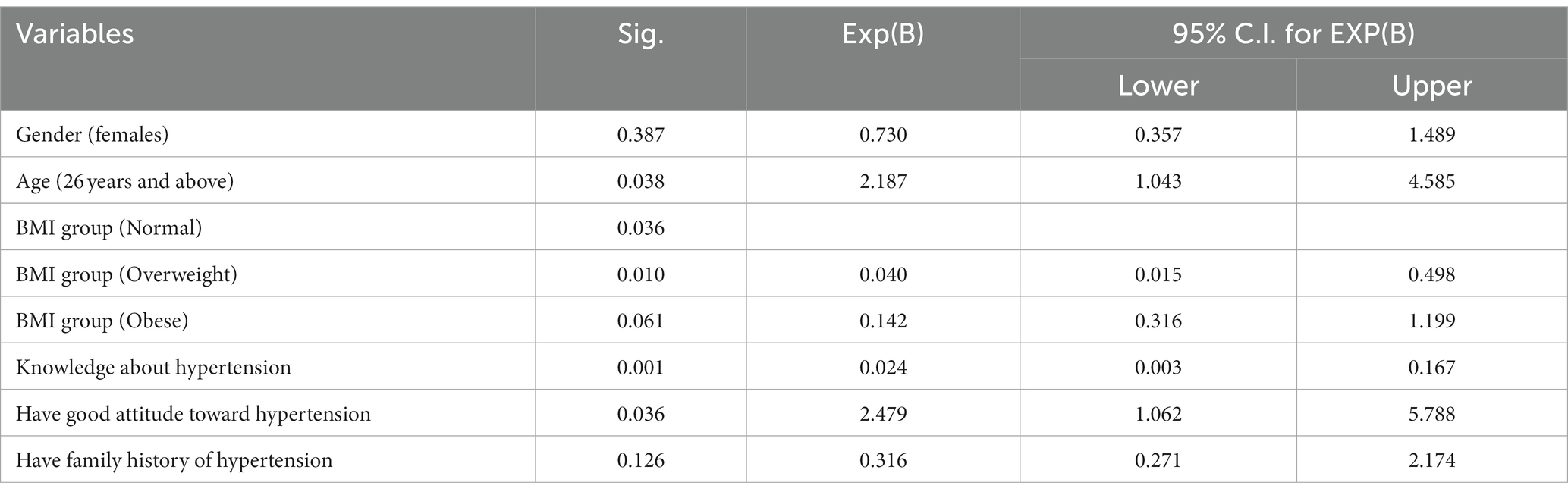
Table 3. Factors influencing checking of blood pressure among participants.
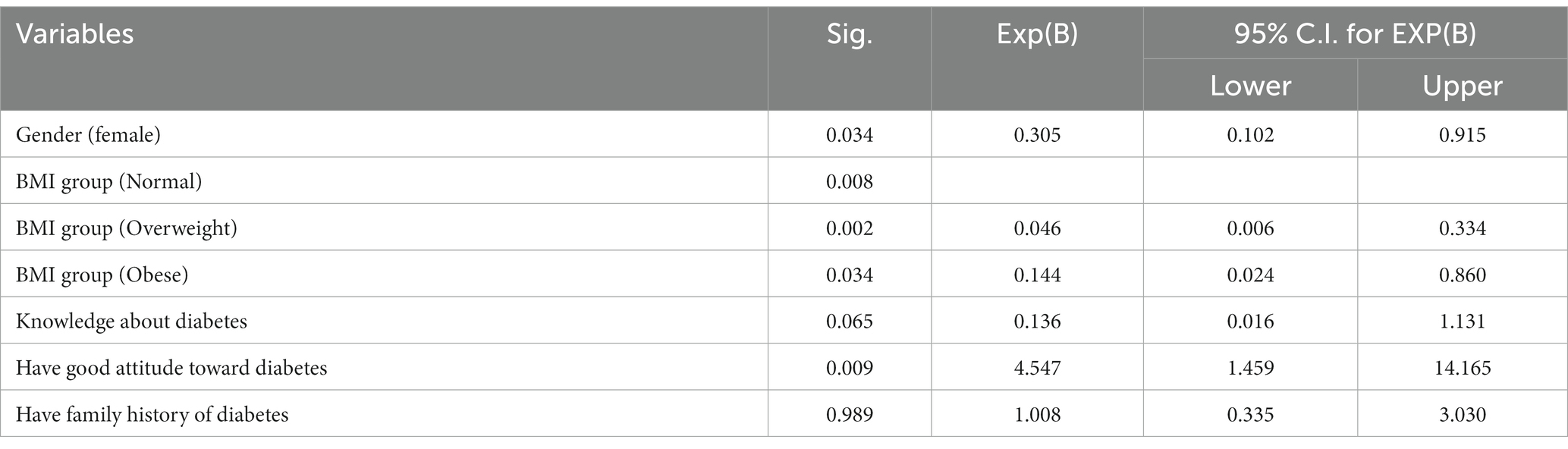
Table 4. Factors influencing checking of blood glucose level among participants.
Inadequate knowledge, screening, treatment, and prevention of HT, DM, and their complications increase the burden on healthcare systems. Hence, they significantly threaten public health and development (25, 26). Individuals with HT or DM or those at risk require long-term care that is tailored, preventive, and affordable. They are considered silent killers because they do not cause symptoms until the condition is advanced (27). However, despite the rising incidence, many individuals are unaware of their BPL and BGL or associated problems with both diseases. Unless addressed, these health issues’ mortality and morbidity burden will continue to rise.
Validated questionnaires for testing knowledge of hypertension and diabetes were adopted in this study. We noted that general knowledge about both diseases was poor, particularly with diabetes, leading to bad attitudes. Thus, only 32.0 and 42.7% of the surveyed knew about DM and HT, respectively, while nearly three-fourths had bad attitudes towards the diseases, which shows a lot of knowledge gaps concerning the two diseases. The findings of poor knowledge of hypertension and diabetes were consistent with previous studies (5, 28). However, the results of diabetes knowledge were inconsistent with those of Anyanti et al. (8), who reported a high level of knowledge among their research participants. The lack of understanding of the complications of diabetes among our participants could have been attributed to the differences.
Regular BPL and BGL examinations are essential to detect hypertension and diabetes at an early stage. Although gender did not affect BPL and BGL checks, it is to be noted that more females than males checked their BPL and BGL. In addition, similar to the findings of Anyanti et al. from Nigeria (8) the older participants checked their BPL and BGL more frequently than the younger participants. We note a worrisome finding in the BG check, in which no one under 25 checked their BGL regularly. This finding is attributable to the fact that studies have revealed that the risk of cardiovascular diseases, including hypertension and diabetes, rises with age (29). As a result, older people are more likely than younger people to be aware of the importance of regular BP and BG checks.
Additionally, those with high levels of education, and students, were less likely to check their BGL and BPL. However, these results contradict what was found among Nigerians. Similarly, unemployed individuals were also less likely to undertake routine BPL and BGL checks. Lower monthly incomes may hinder people from requesting these tests because of their high cost, and this could be a significant reason why those people would not routinely check their BGL, even though the study did not consider their monthly wage. Furthermore, it is well established that individuals who perceived themselves to be healthy are less likely to undertake medical screening as it was found in our study (30). Nevertheless, the overweight individuals not checking their BGL and BPL is an alarming situation which needs urgent attention as these individuals are more at risk of developing high BP and BG (31).
Furthermore, we discovered that most participants checked their BPL more frequently than their BGL this is similar to what was found in Nigeria (8). Unlike BG checks, BP checks are part of the standard examination for outpatients in Ghana, independent of the patient’s presentation. Nonetheless, less than two-thirds of these people monitor their BP at least once a year, which could be better given the need for regular BP monitoring to prevent hypertension progression.
Ultimately, the findings of this study revealed that neither knowledge of diabetes nor a family history of the disease affected how frequent our respondents checked their blood sugar levels. This contradicts the findings of Anyanti et al. where they found that being knowledgeable and having family history of diabetes made the respondents to check their blood glucose routinely. Our results could also be as a result of the myth in Ghana that, “if I do not know, it will not kill me.” In that, most uneducated Ghanaians believes that, when you are aware of your health condition you begin to think about it which can result in their death., Lastly, we discovered having a positive attitude toward both diabetes and hypertension to be the participants’ primary determinant of blood pressure or sugar checks. Positive attitude toward a condition has been established to improve the measures required to maintain or control the health condition (8, 32). As far as this study is concerned, it did not look at how hypertension and diabetes were related in terms of knowledge, practices, and prevalence because the study design did not include the screening of the participants. While this does not contradict the study’s findings, future research may focus on hypertension and diabetes screening to better establish the relationship between lifestyle and disease prevalence.
This study has several notable strengths. The study is the first to examine the behaviour of the general population in Akatsi South District, Ghana, regarding hypertension and diabetes using the KAP questionnaire. Also, we reduced the likelihood of residual confounding in our models by adjusting for any possible bias. Finally, our sample size was good enough to draw meaningful conclusions. Our study, on the other hand, had limitations. First and foremost, weight and height are the only anthropometric parameters measured in this study, and using the BMI is not the best indicator of obesity, but analyzing the body composition will be better in this case. In addition, the participants measured their body weight, usually accompanied by intentional and non-intentional personal errors. Nevertheless, previous studies have reported that self-reported weight and height are acceptable for determining BMI (33). Finally, knowledge about possible symptoms of both HT and DM was not considered in the survey, so we limited attitude questions to three.
Preventive behaviours may be encouraged when people have adequate knowledge about a disease to make them aware of its dangers. Hence, based on the findings of this study, we, therefore, recommend the district health directorate and healthcare professionals adopt periodic public health education and promotion via the mainstream media and community-to-community education to help bridge the knowledge gap.
Individuals can minimize early-stage disease mortality with adequate knowledge, attitudes, and practices. Significantly low levels of knowledge, attitude, and practice, which are challenges to eliminating determinants contributing to NCDs, were found in HT and DM in this district. Also, overweight and obese individuals should be a focus of health education as weight is a risk factor; meanwhile, they rarely or never check their blood pressure or sugar level. For people to be aware of the necessity of regular blood pressure and blood glucose screening as a preventive strategy and to avoid an increase in cardiovascular mortality, there is an urgent need to create awareness and educate the population accordingly.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ghana Health Service (GHS) Ethical Review Committee (ERC)-GHS-ERC: 17/02/2020. The patients/participants provided their written informed consent to participate in this study.
DA and AD conceived and designed the study. DA, AW, and SK collected the data and performed the analysis of all data. DA and ZZ provided a review of the previous literature. DA, AD, AW, ZZ, SK, RL, KH, and JZ all participated in the discussion of the results. DA, AD, AW, and ZZ wrote all versions of the manuscript and figures. DA, ZZ, and JZ polished this manuscript, including grammatical checks. All authors contributed to manuscript revision, read, and approved the submitted version.
This work was supported by the National Natural Science Foundation of China (grant 82173899).
The authors would like to express their profound gratitude to the District Health Directorate and the NCD prevention and control programme (Ghana Health Service), who granted permission upon request. Thanks also go to all the people who took part in the study and the field assistants who helped us collect data.
The authors declare that they conducted the research without any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gakidou, E, Afshin, A, Abajobir, AA, Abate, KH, and Abbafati, C. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet. (2017) 390:1345–422. doi: 10.1016/S0140-6736(17)32366-8
2. Noncommunicable diseases (n.d.). Available at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (Accessed April 21, 2022).
3. Mathers, CD, and Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. (2006) 3:e442. doi: 10.1371/journal.pmed.0030442
4. Yach, D, Hawkes, C, Gould, CL, and Hofman, KJ. The global burden of chronic diseases: overcoming impediments to prevention and control. JAMA. (2004) 291:2616–22. doi: 10.1001/jama.291.21.2616
5. Imran, M, and Hashmi, A. Knowledge, attitudes and practices of patients regarding knowledge, attitudes and practices of patients (2019) 32:166–72.
6. Budreviciute, A, Damiati, S, Sabir, DK, Onder, K, Schuller-Goetzburg, P, Plakys, G, et al. Management and prevention strategies for non-communicable diseases (NCDs) and their risk factors. Front Public Heal. (2020) 8:788. doi: 10.3389/fpubh.2020.574111
7. IDF (2021). IDF Diabetes Atlas | Tenth Edition, Int. Diabetes Fed. Available at: https://diabetesatlas.org/ (Accessed April 21, 2022).
8. Anyanti, J, Akuiyibo, SM, Fajemisin, O, Idogho, O, and Amoo, B. Assessment of the level of knowledge, awareness and management of hypertension and diabetes among adults in Imo and Kaduna states, Nigeria: a cross-sectional study. BMJ Open. (2021) 11:e043951. doi: 10.1136/bmjopen-2020-043951
9. Bosu, WK, and Bosu, DK. Prevalence, awareness and control of hypertension in Ghana: a systematic review and meta-analysis. PLoS One. (2021) 16:e0248137. doi: 10.1371/journal.pone.0248137
10. Gatimu, SM, Milimo, BW, and Sebastian, MS. Prevalence and determinants of diabetes among older adults in Ghana. BMC Public Health. (2016) 16:1–12. doi: 10.1186/s12889-016-3845-8
12. Agyei-Mensah, S, and De-Graft Aikins, A. Epidemiological transition and the double burden of disease in Accra, Ghana. J Urban Health. (2010) 87:879–97. doi: 10.1007/s11524-010-9492-y
13. Qureshi, NN, Hatcher, J, Chaturvedi, N, and Jafar, TH. Effect of general practitioner education on adherence to antihypertensive drugs: cluster randomised controlled trial. BMJ Br Med J. (2007) 335:1030. doi: 10.1136/bmj.39360.617986.AE
15. Mills, KT, Bundy, JD, Kelly, TN, Reed, JE, Kearney, PM, Reynolds, K, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. (2016) 134:441–50. doi: 10.1161/CIRCULATIONAHA.115.018912
16. Tarkang, E, Atinyi, R, Takramah, W, Axame, WK, Owusu, R, Parbey, PA, et al. Prevalence and awareness of hypertension among urban and rural adults in the Keta municipality, Ghana. J Med Res. (2017) 3:155–63. doi: 10.31254/jmr.2017.3313
17. Asante, DO, Walker, AN, Seidu, TA, Kpogo, SA, and Zou, J. Hypertension and diabetes in Akatsi South District, Ghana: modeling and forecasting. Biomed Res Int. (2022) 2022:1–11. doi: 10.1155/2022/9690964
18. D.P.C.-O.U.-A.S.D. Assembly, Ministry of Local Government and Rural Development Akatsi South District Assembly, (2017) 2014–2017. ASD, Pennsylvania.
20. Kadam, P, and Bhalerao, S. Sample size calculation. Int J Ayurveda Res. (2010) 1:55. doi: 10.4103/0974-7788.59946
21. Pourhoseingholi, MA, Vahedi, M, and Rahimzadeh, M. Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench. (2013) 6:14–7.
22. Frantz, J. A knowledge assessment questionnaire relating to risk factors for chronic disease of lifestyle for high school learners: validity and reliability. J Community Heal Sci. (2008) 3:30–7.
23. Weir, C.B., and Jan, A., BMI Classification Percentile and Cut Off Points, StatPearls. (2021). Available at: https://www.ncbi.nlm.nih.gov/books/NBK541070/ (Accessed April 12, 2022).
24. NHLBI Obesity Education Initiative, The Practical Guide Identification, Evaluation, and Treatment of Overweight and Obesity in Adults NHLBI, (2000) 9–11. Bethesda
25. De-Graft Aikins, M, Kushitor, K, Koram, S, and Gyamfi, GO. Chronic non-communicable diseases and the challenge of universal health coverage: Insights from community-based cardiovascular disease research in urban poor communities in Accra, Ghana. BMC Public Health. (2014) 14:S3. doi: 10.1186/1471-2458-14-S2-S3
26. Kayima, J, Wanyenze, RK, Katamba, A, Leontsini, E, and Nuwaha, F. Hypertension awareness, treatment and control in Africa: a systematic review. BMC Cardiovasc Disord. (2013) 13:1–11. doi: 10.1186/1471-2261-13-1
27. WHO. 2008-2013 Action Plan for the Global Strategy for the Prevention and Control of Noncommunicable Diseases. Geneva: WHO (2009).
28. Dussa, K, Parimalakrishnan, S, and Sahay, R. Assessment of diabetes knowledge using diabetes knowledge questionnaire among people with type 2 diabetes mellitus. Asian J pharm Clin Res. (2015) 8:254–6.
29. Arugu, GM, and Maduka, O. Risk factors for diabetes mellitus among adult residents of a rural district in southern Nigeria: implications for prevention and control. Niger J Clin Pract. (2017) 20:1544–9. doi: 10.4103/njcp.njcp_154_17
30. Chien, SY, Chuang, MC, and Chen, IP. Why people do not attend health screenings: factors that influence willingness to participate in health screenings for chronic diseases. Int J Environ Res Public Health. (2020) 17. doi: 10.3390/ijerph17103495
31. Oguoma, VM, Nwose, EU, Skinner, TC, Digban, KA, Onyia, IC, and Richards, RS. Prevalence of cardiovascular disease risk factors among a Nigerian adult population: relationship with income level and accessibility to CVD risks screening. BMC Public Health. (2015) 15:1–16. doi: 10.1186/s12889-015-1709-2
32. Kassie, AM, Abate, BB, Kassaw, MW, Aragie, TG, Geleta, BA, and Shiferaw, WS. Impact of knowledge and attitude on the utilization rate of cervical cancer screening tests among Ethiopian women: a systematic review and meta-analysis. PLoS One. (2020) 15:e0239927. doi: 10.1371/journal.pone.0239927
Keywords: hypertension, diabetes, knowledge, attitudes, health education, promotion
Citation: Asante DO, Dai A, Walker AN, Zhou Z, Kpogo SA, Lu R, Huang K and Zou J (2023) Assessing hypertension and diabetes knowledge, attitudes and practices among residents in Akatsi South District, Ghana using the KAP questionnaire. Front. Public Health. 11:1056999. doi: 10.3389/fpubh.2023.1056999
Edited by:
Christiane Stock, Charité–Universitätsmedizin Berlin, GermanyReviewed by:
Nahla Al-Bayyari, Al-Balqa Applied University, JordanCopyright © 2023 Asante, Dai, Walker, Zhou, Kpogo, Lu, Huang and Zou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianjun Zou, em91amlhbmp1bjEwMEAxMjYuY29t; Rongzhu Lu, bHVyekB1anMuZWR1LmNu; Kaizong Huang, a3podWFuZ0BuanUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.