
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 03 February 2023
Sec. Public Health Policy
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1039688
This article is part of the Research TopicInsights in Public Health Policy: 2022View all 8 articles
 Lorena Aguilera-Cobos1,2*†
Lorena Aguilera-Cobos1,2*† Patricia García-Sanz1*†
Patricia García-Sanz1*† María Piedad Rosario-Lozano1
María Piedad Rosario-Lozano1 M. Gonzalo Claros2,3,4,5Juan Antonio Blasco-Amaro1
M. Gonzalo Claros2,3,4,5Juan Antonio Blasco-Amaro1Background: Personalized medicine (PM) is now the new frontier in patient care. The application of this new paradigm extends to various pathologies and different patient care phases, such as diagnosis and treatment. Translating biotechnological advances to clinical routine means adapting health services at all levels is necessary.
Purpose: This article aims to identify the elements for devising a framework that will allow the level of PM implementation in the country under study to be quantitatively and qualitatively assessed and that can be used as a guideline for future implementation plans.
Methods: A systematic review was conducted per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The research question was: What are the domains for determining the level of implementation of PM at the national level? The domains for assessing the degree of PM implementation, which would form the framework, were established.
Results: 19 full-text studies that met the inclusion criteria were peer-selected in the systematic review. From all the studies that were included, 37 elements—encompassed in 11 domains—were extracted for determining the degree of PM implementation. These domains and their constituent elements comprise the qualitative and quantitative assessment framework presented herein. Each of the elements can be assessed individually. On the other hand, the domains were standardized to all have the same weight in an overall assessment.
Conclusions: A framework has been developed that takes a multi-factorial approach to determine the degree of implementation of PM at the national level. This framework could also be used to rank countries and their implementation strategies according to the score they receive in the application of the latter. It could also be used as a guide for developing future national PM implementation strategies.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022338611, Identifier: CRD42022338611.
Great strides have been made in health over the past few decades, resulting in various interventions that have increased the effectiveness and efficiency of healthcare. Thanks to the combination of continuous (bio)technological developments and the need for patient-centered decision-making, medicine has entered an era where greater personalization is possible. Within this context, the term personalized medicine (PM) has arisen. PM is defined as an approach aimed at the prevention, diagnosing, and treating disease based on an individual's specific profile, i.e., taking into account the genetic heterogeneity among individuals, the environment, and their lifestyle (1). PM is a new frontier in healthcare that combines omics, big data analytics, and population health (2). In this study, PM should be understood as an umbrella term for stratified medicine and precision medicine. The authors decided to employ the initialism PM because it is widely used in the scientific literature (3).
PM represents a complete paradigm shift in healthcare thanks to incorporating new diagnosis strategies and allowing new treatments for a wide range of pathologies. In this context, omics play an essential part in PM development (4). Omics are a family of technologies that study biological or molecular elements whose analysis affords a better understanding of the pathophysiology and contextualization of diseases, thus permitting their diagnosis and prevention and/or the application of the correct treatment based on individual differences (5). There are as many omics as there are biological or molecular elements that can be studied using these technologies. They are generally named by adding the suffix “-omics” to the set of molecules and elements studied. Omics technologies should be combined according to the pathology and related to the patient's phenotype. This requires algorithms that integrate both types of data, in addition to other possible patient data such as comorbidities, lifestyle or patient preferences (6, 7). These algorithms can currently be developed thanks to artificial intelligence and machine learning. In addition, data collection can benefit from the use of wearable smart sensors (8).
Genomics is the omics that is leading the implementation in health systems (5, 9). Despite tremendous technological and scientific advances in the medical field, there are significant obstacles to the incorporation of PM into clinical routine. First, collecting genomic and molecular data in healthcare for research purposes is still rare. Secondly, in most cases, clinical and genomic databases are neither homogenized nor interoperable, which hinders progress in understanding diseases. Lastly, the results of data analyses are not always included in the clinical decision-making process or are not efficiently included (10–13).
Health professionals should be trained and motivated to overcome these obstacles using PM and understand its value. Moreover, it would be advantageous if patients, relatives, and the general public were aware of the medical importance of these innovations. Indeed, this awareness-raising should be based on a dialogue between stakeholders to achieve acceptance of implementation (e.g., clinicians, patients/citizens, administration, policymakers). Thus, the full implementation of PM poses significant ethical, legal, regulatory, organizational, and knowledge challenges (4, 14, 15).
In short, a holistic approach to health systems is recommended to achieve the implementation of PM and omics (16). To achieve this, some countries have devised PM implementation strategies. The goal of these strategies is to come up with implementation plans that have a holistic view of patient care and to establish collaborative networks of experts and entities that operate under common standards and protocols (17).
The primary purpose hereof is to develop a framework for determining the level of implementation of PM at the national level based on identifying elements through a systematic review (SR). This framework will allow the degree of implementation to be qualitatively and quantitatively assessed. Additionally, it will be possible to use it as the basis for devising future PM implementation strategies.
The development of the framework for determining the level of implementation of PM at the national level was based on the results of a systematic review. This systematic review was conducted per the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement (18). The protocol for this review was registered in the PROSPERO repository with ID no CRD42022338611.
What are the domains for determining the level of implementation of PM at the national level?
For reviewing the scientific evidence, a literature search was carried out (date of search: 14 February 2022) in the following databases of reference: Medline (Ovid), Embase (Excerpta Medica Database), WoS (SCI Science Citation Index), and PubMed (Ahead of print/First online).
Both controlled language (descriptors) and free terminology (genomic service, personalized medicine, health national program) were used to search for studies, the initial strategy having been adapted to each database's syntax. These searches were limited by date to studies conducted after 2016. The strategies used are listed in Supplementary material.
Likewise, a secondary search was also performed based on the references of the included studies. In addition, the identification of the studies was complemented with a search through the INAHTA database to detect reports from international health technology assessment agencies and a search through institutional or governmental resources for national health policy documents, strategies and regulations.
The references identified during the primary and secondary searches in the databases mentioned above were imported into the reference management section of the software application Covidence (https://www.covidence.org/), where duplicate references were then identified and deleted. Two authors (LAC, PGS) independently reviewed them to filter out the remaining references by title and abstract using pre-established inclusion and exclusion criteria. Subsequently, both reviewers (LAC, PGS) filtered the full-text studies independently according to the same criteria. Any discrepancies- in both rounds were resolved by both reviewers by consensus.
Technical documents, implementation projects, scientific publications, and regulations dealing with the implementation of PM at the national level and/or its assessment were included. Studies that did not have this purpose were left out, and comments, editorials, review protocols, and clinical trials were excluded by design. Studies published in either English or Spanish after 2016 were included.
The data were extracted by two independent authors (LAC, PGS). First, the authors conducted a descriptive analysis to examine and report the existing methodological frameworks and their characteristics. To this end, general information was extracted from the studies included in the report (authors, year of publication, type of study, features according to study type, and purpose of the study). Secondly, the authors performed a thematic analysis according to the method described by Thomas and Harden (19). Following this methodology, two independent authors (LAC, PGS) identified and extracted the items considered in each of the studies reviewed and included. The classification into domains was based on the list of these items retrieved from the thematic analysis, by a consensus process. After this classification, the items acquired the status of assessable elements of the framework.
The quality of the studies included was assessed independently by two authors (LAC, PGS), which resolved any disagreements they had by consensus. Different quality assessment tools were used depending on the type of study. The AMSTAR-II tool (20) was used to assess the quality of systematic reviews; the SANRA tool (21) was used to assess the quality of narrative reviews, and the checklist published by Humphrey-Murto (22) was used to assess the quality of interviews and expert panels.
The items extracted from the included studies in the SR were used to develop a framework for the qualitative and quantitative determination of PM implementation at the national level. It should be noted that the exclusion criteria were not based on the number of studies in which these items appeared. The authors used the items extracted through the thematic analysis (19) of the selected studies to generate the framework. Then, the authors grouped these items into domains to generate a comprehensible and functional tool. Following this classification, the items acquired the status of assessable elements of the framework. These domains were developed ad-hoc, and their definitions and the elements they contained were established by the authors using a consensus methodology. These elements were individually assessable and quantifiable with a simple scoring system. This simple approach to assigning points across the different domains was based on the idea that the value of each domain was the same according to the contained elements. This assumption enables standardizing all domains' weight in the final score. This scoring system allows the implementation level to be quantitatively determined and is based on similar quantitative assessment tools (23, 24).
A total of 1,432 studies were found in the initial search. After eliminating duplicates, 1,369 potentially relevant studies were left. The studies were independently filtered by title and abstract by both authors, yielding 115 potentially relevant studies. After the peers filtered the studies by full text, 19 full-text studies were ultimately included (11, 12, 23–39). It should be noted that only one study was found that met the inclusion criteria from the secondary and complementary research (24). This filtering process is shown in the PRISMA flowchart in Figure 1.
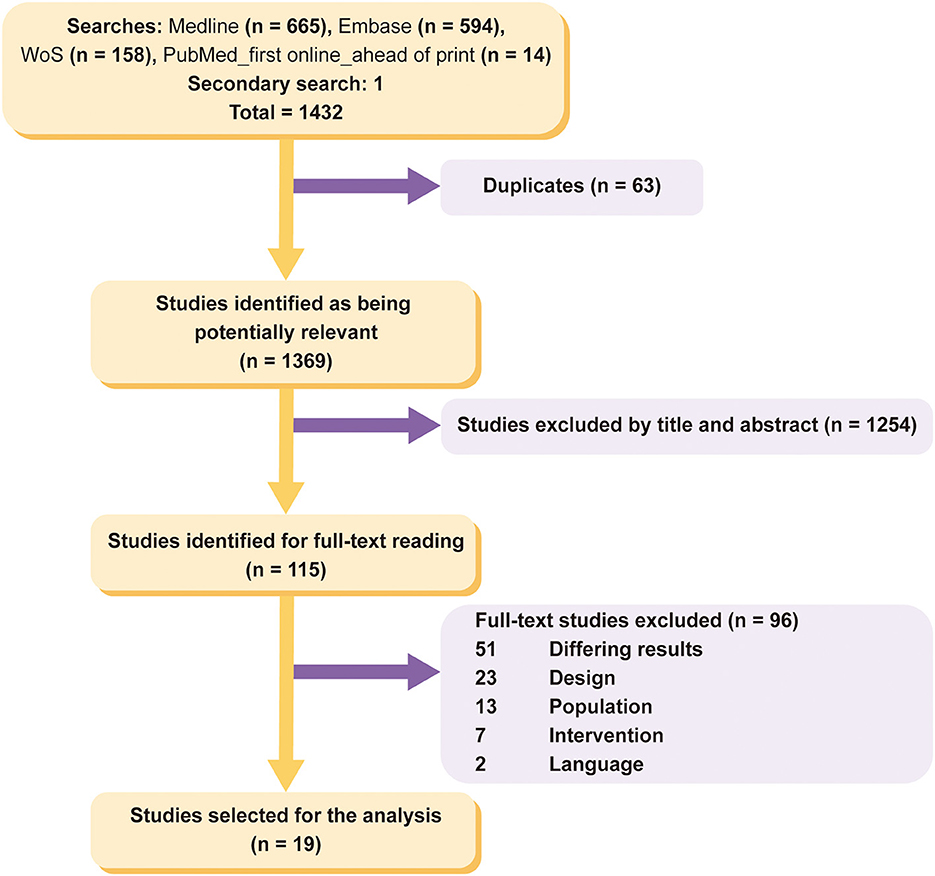
Figure 1. PRISMA flowchart.
The information about the description of the studies included in this review was extracted by two independent authors as described in Methods. Tables listing these characteristics, divided by type of study, are shown in Supplementary Tables S1–S3. Those reviews that also included interviews or an expert panel are listed in the corresponding two tables. It is worth noting that some of the narrative reviews included lacked a methodology, which prevented the authors from extracting the information they contained.
The quality of the studies included was assessed using different tools according to the type of study: AMSTARII (20) for systematic reviews, SANRA (21) for narrative reviews, and the checklist proposed by Humphrey-Murto (22) for interviews and expert panels. In the case of the reviews that also included interviews or expert panels, both elements were assessed separately.
The quality of each of the studies included is listed in Supplementary Table S4. According to the criteria of the AMSTARII tool, the quality of the systematic reviews was rated moderate, low, or critically low; none of the reviews included in the SR had the high quality that is the top level in this tool. According to the SANRA tool's criteria, the quality of the narrative reviews ranged from 12 to 5, 12 being the maximum possible score in this tool. The authors of the SANRA tool (21) suggest that a score of 4 or lower indicates the inferior quality of the review in question. The quality of the interviews and expert panels scored, according to the checklist published by Humphrey-Murto, between 11 and 3, 11 being the maximum possible score in this tool. No studies were ultimately excluded on low-quality grounds.
The elements for determining the level of implementation of PM at the national level were extracted from the studies included in the SR via a thematic analysis and after classification into domains through a consensus process. Figure 2 represents these domains graphically. Each of these domains contains several quantifiable elements. Table 1 lists all domains and the scoring elements for each domain. The domains and the assessable elements of which they are composed are described below. The references cited in each domain name refer to the studies where their assessable elements were identified. The results of the extraction of the included studies to obtain the assessable elements that constitute the framework can be found in Supplementary Table S5.

Figure 2. Graphical representation of framework domains. Source: Flaticon.com.
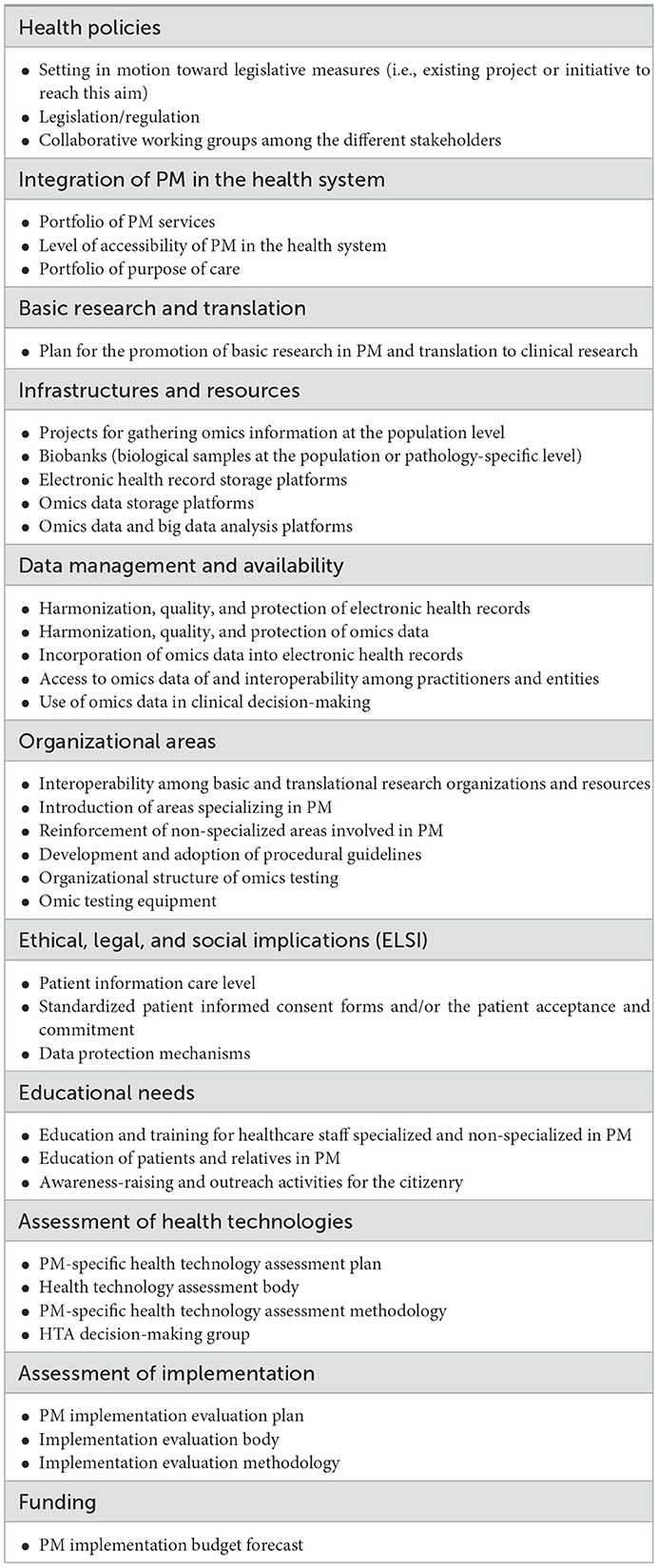
Table 1. Framework domains and elements for determining the level of PM implementation.
This domain refers to the setting in motion of legislative measures that will provide an adequate legal framework for patients to access to PM with the utmost guarantees. This domain also gathers the possibility that the legislative rules never materialize, for that reason, includes the following elements: Setting in motion toward legislative measures (i.e., existing project or initiative), the existence of specific legislation or regulations for one or more areas of PM, and the creation of legislative working groups for laying down these rules or devising projects or initiatives are included in this domain as valuable elements (23, 27, 31, 33, 38).
This domain envisages the incorporation of PM and omics into the corresponding national health system. The quantifiable elements included in this domain are the existence of a portfolio of PM services, a high level of accessibility to PM for patients in the health system, and the collection of the care purposes for which the use of PM is being considered (23, 34, 36–39).
This domain contains a single scorable element: the existence of a plan for promoting basic and translational research in PM (30, 31, 38).
This domain deals with gathering samples and clinical data at the population or pathology-specific level and their proper storage and analysis. This domain includes five scorable elements: the existence of projects for gathering omics information at the population level; the existence or setting up of biobanks for depositing and preserving biological samples; and the existence of platforms for storing and analyzing electronic medical records and omics data (24, 29, 37–39).
This domain considers the specific needs at the level of the data generated in omics tests and PM so that they may be used effectively in clinical decision-making. Five scorable elements were considered to assess this domain: harmonization, quality, and protection of electronic health records and omics data; incorporation of omics data into electronic health records; data access by and interoperability among practitioners and organizations; and use of omics data in clinical decision-making (11, 24, 28–30, 34, 37, 38).
Changes are required at the organizational level after considering PM to be a change in the approach to medicine. These changes arise from a need for specialization of the health system and staff and are included in the six measurable elements this domain comprises: interoperability among organizations and research resources; implementation of health areas specializing in PM; reinforcement of non-specialized health areas involved in PM; development and adoption of procedures that include PM; setting up of organizational structures for omics testing; and the existence of omic testing equipment (12, 23–25, 27, 29, 31, 34, 37, 39).
This domain refers to the fact that it is essential to develop PM implementation strategies within an ethical and legal framework that boosts potential health benefits while minimizing potential damages, such as misuse of information, stigmatization, or discrimination. To this end, patients need to be adequately informed and their PM data legally protected, given its sensitivity, the potential impact of the results on their health, and the likelihood of accidental findings in some tests. Thus, this domain includes the following assessable elements: The existence of standardized patient informed consent forms and/or the patient acceptance and commitment prior to testing; data and results in protection mechanisms; standardization of the level of care in charge of patient information (11, 25, 26, 29, 38).
Given that PM will be a major innovation for health staff, patients, relatives, and society, it is essential that they be adequately trained in how to use it and made aware of when it is being used. This is a complex issue and refers to the so-called public engagement. Hence, efficient and successful engagement entails a coordinated strategy and organizational effort across various fields, from public health to science and education. This domain includes three elements to cover all educational needs: the existence of educational plans for patients and families in PM; the existence of educational plans for patients and families in PM; and the existence of awareness-raising and outreach activities for the citizenry (social awareness and citizens' omics science literacy) (26, 27, 29, 31, 38).
The health technologies used in omics testing have peculiarities that require adapting the HTA methodology. Four elements have been included to ensure that these peculiarities do not become an obstacle to the assessment of these technologies and, hence, to their implementation: the existence of a specific assessment plan for HTA in PM; the creation of a reference body for the HTA of PM technologies; the specific adaptation of an HTA methodology to PM; and the creation of a group of experts for HTA decision-making (35, 37, 38).
The current boom in implementing PM-related technologies calls for devising implementation evaluation plans for monitoring it and identifying areas for improvement. The elements considered in this domain were: the existence of a plan for evaluating the implementation of PM at the national level; the existence of a competent body; and the existence of an appropriate evaluation methodology (25, 31, 33, 36, 37).
The creation and development of all the domains above must be adequately funded. Only one scorable element was considered to assess this domain: the existence of a funding plan for the implementation of PM (25, 31).
The domains proposed here for determining the level of PM implementation and their assessable elements extracted from the studies included in the systematic review allowed us to develop a framework. This framework allows this level of implementation at the national level to be qualitatively and quantitatively determined and is designed to be applicable to any country and health system.
This tool includes 11 domains comprising 37 individually quantifiable elements in all. If a national implementation plan does not include an element or no information about it can be found, it will be given a score of 0. If a national implementation plan includes an element, it will be given a score of 1. If an element is already in the implementation phase, it will be given a score of 2.
Based on two of the studies included, (23, 24) a mathematical formula was applied to standardize the weight of the domains in the final assessment of the implementation. In such a way, those domains with a higher number of assessable elements do not have a bigger weight in the implementation's final score. A spreadsheet for automatically making these calculations is included in the Supplementary material.
When applying the framework to compare or rank countries, consideration should be given to whether it was possible to gather and collect enough information from each country. Otherwise, the benchmarking may not represent the actual situation of each health system compared.
A multidisciplinary team of experts in this kind of study and PM conducted a systematic review as part of this study and identified the elements needed to develop a new framework following a thematic analysis and consensus methodology. This proposed framework will allow the degree of PM implementation in different international health systems to be qualitatively and quantitatively determined.
Our research question and systematic review provide a comprehensive approach to implementing a PM that considers the many interrelationships existing in today's health systems. In particular, we devised a literature search strategy with a holistic approach to correctly implementing PM in health systems. The basic elements we identified in other frameworks, models or studies served as a basis for developing a framework. The framework we developed allows the different aspects of PM implementation in various countries and their strengths and weaknesses to be qualitatively and quantitatively assessed. This framework may also be used at the health policy strategy level and for planning the implementation of PM.
To our knowledge, this is the first time a framework for determining the country-level implementation of PM in different countries has been proposed and described with a holistic approach in health systems. Some of the studies we considered when developing our framework include partial tools for assessing PM implementation in specific organizational areas and applications (12, 23, 32). Agarwal et al. (23) focus on assessing the integration of PM in US health organizations. Doyle et al. (32) solely focus on the organizational aspects of the centers providing PM. Lee et al. (12) developed a global investment innovation framework with regional, technical and organizational dimensions to lay the foundations for a global, national PM strategy, but it focused only on South Korea.
Another original aspect of our framework stems from an SR conducted by a multidisciplinary team of experts in this type of study and PM. This SR allowed us to identify the domains for determining the level of PM implementation and the assessable elements of which they are composed. The studies we included in the SR have different authors from different countries, which allows us to assert that it will be possible to use our framework in different countries. We extracted these domains and their elements from the studies we included in the SR, which we discussed in the results section and in this section below. In summary, the included studies we reviewed highlighted critical themes from our findings that endorse the domains of the proposed framework for determining the level of PM implementation.
The European Health Systems & Policies report, and the WHO report indicate that health policies and policymakers need to consider concrete, change-driven actions to strengthen health systems and enhance their performance (40). In this way, health systems can adapt to change and improvement. This means that any effort to improve the performance of health systems must be developed through policy implementation challenges (41). Because of this and the holistic changes required for PM implementation, health policy is one of the primary keys to the actual and full implementation of PM in health systems. In fact, health policy is one of the domains of our framework that encompasses three elements from five included studies (23, 27, 31, 33, 38). This domain focuses on setting legislative measures in motion that will provide an adequate legal framework for patients to access PM with the utmost guarantees. Ultimately, this domain also depicts potential transformative strategies and methods for defining and measuring value at all decision-making levels aligned with PM, where the collaborative working groups among the different stakeholders also play an essential role (42). Regarding this, a well-coordinated health policy facilitates PM integration into healthcare systems (39). This integration is contemplated in our framework with a domain composed of three elements drawn from six of the included studies (23, 34, 36–39). Indeed, patient access to PM is variable since there is no uniform standard for integrating PM into healthcare systems (43). Proper and standardized integration will allow the PM to be applied in appropriate delivering points of care and health care purposes. To carry out this integration, all stakeholders, their needs, and benefits must be taken into account (32).
Promoting basic and translational science in PM favors the bidirectional flow of development and implementation between the laboratory and clinical practice, which is essential for PM implementation. This comprises a domain with a single assessable element drawn from three of the included studies (30, 31, 38). This promotion should include long-term actions due to the long development times of the scientific studies until their incorporation into clinical routine (44).
The necessary and adequate resources must be available for PM proper implementation. The framework includes five elements from five studies (24, 30, 37–39) related to these needs. Some of these needs imply the reinforcement of existing resources and infrastructures, and others imply the creation of new structures. These resources are essential for the storage, preservation, and accessibility of biological samples and electronic patient data, as well as for their adequate analyze (45). It also identified as essential in implementing PM the need for standardized digital systems, remarkably reliable information formats, and digital decision support tools in electronic health records (27, 46, 47). The growing PM data must not only be stored or analyzed, but also managed in a specific way that ensures interoperability, standardization, and security. Some of the characteristics of these data are specific, e.g., their large volume, high sensitivity, and need for interoperability, and would therefore require specific actions (48). These necessities have been considered in our framework, which includes five elements extracted from eight of the included studies (11, 24, 28–30, 34, 37, 38) about this issue. Proper PM data management and safety would hasten their availability in clinical practice and increase patient confidence in the healthcare system. Health systems and their organizational areas must be understood as living systems adaptable to change and improvement. This need for adaptation becomes imperative in the case of PM implementation, which requires system-wide adaptations. This adaptation appears in 10 of the included studies (12, 23–25, 27, 29, 31, 34, 37, 39), from which the six elements that constitute the domain “Organizational areas” were extracted. Therefore, adaptations of organizational areas should not only be understood as the creation of new areas but also as the strengthening of pre-existing areas and the relationships between them (49).
PM implementation's success depends increasingly on its competence to improve healthcare for all population groups and citizens' commitment (50). The ethical, legal, and social implications of PM emerge as an essential key to addressing this aim due to the sensitivity of the data generated linked to PM application, the potential impact of the results on health, and the likelihood of accidental findings. Indeed, the ethical, legal, and social implications have an identity as a domain in our framework, whose elements were extracted from five included studies (11, 25, 26, 29, 38). This domain considers correct patient information and engagement based on standardized protection and information mechanisms. Although PM progresses rapidly, the problem of the need for more ethical, legal, and social regulations remains. There should be regulation on the return of results, confidentiality, and privacy that should be carried out by both policymakers and legislators together. In addition, they should encourage policies that promote PM education and fund initiatives that bring together the interests of different stakeholders (50, 51). Hence, the existence of specific legislation or initiatives toward this end, bioethics committees, and society's awareness of PM would facilitate PM implementation (52). Evidence points out that public awareness about PM could be higher due to a lack of trust and trustworthiness, which are essential in supporting the acceptance of the PM. There must be mechanisms to enhance this trust and trustworthiness via promoting transparency about the social value of PM, the correct use of the new data generated, and the consequence of ethical issues (46). In this context emerges the need for public engagement in PM. Public engagement is a complex theme that encompasses the commitment and acceptance of society at large and the patients, families, and groups most directly affected by the diseases addressed by PM. Therefore, there is no doubt about the importance of education and awareness raising in PM for its proper implementation. This education should be tailored to stakeholders (policymakers, scientists, clinicians, patients, or citizens). Awareness-raising must be based on a dialogue between stakeholders to achieve PM acceptance (51), being able to lead by the government or different organizations already actively engaging the public (46). These differential educational needs according to the target audience are reflected in the domain “Educational needs” of our framework, whose elements have been extracted from five included studies (26, 27, 29, 31, 38).
The increasing growth of medical innovation, especially in PM, creates a need to improve patient involvement in the health technology assessment (HTA) process. Therefore, the methodology for HTA needs to be adapted to the particularities of technologies used in PM. The lack of standardized methods due to different national policies and cultural disparities has led to different recommendations for the same healthcare technology (43). Indeed, the new European HTA legislation is developing to solve this and prioritizes assessing some of the leading health technologies in PM, such as advanced therapies (53, 54). HTA agencies have acquired a key role in assessing and approving these new technologies related to PM. Expert and multidisciplinary teams from these agencies should carry out these assessments and their adaptation process. Three of the included studies (35, 37, 38) consider the three elements necessary for this assessment that is included in the framework. Agencies and stakeholders involved in HTA should work together to elevate the patient voice in HTA worldwide in a creative and transformative way.
As we have seen so far, several mechanisms are necessary for implementing PM, so evaluating the correct functioning and development of each of them in all phases of implementation is necessary. This evaluation should be done by specialized teams and with appropriate methodological evaluation tools (4). This will allow the detection of possible shortcomings or barriers in the implementation and suggest possible improvements. The assessment of the implementation domain that encompasses these features in our framework contains three assessable elements from five studies (25, 31, 33, 36, 37). Funding is another essential domain to ensure that all the domains mentioned above work and interact appropriately in a stable, long-term, and secure manner. This assessment element is addressed in two of the included studies (25, 31). Such project-based funding across different PM domains will provide the necessary support for PM from the research phase to its implementation in the clinical routine.
As far as the study's limitations are concerned, a possible publication bias in the detection of studies is worth noting, despite having conducted a search in other sources (such as governmental websites) of information in addition to the primary search. This could be one of the reasons why the studies detected that met the inclusion criteria were less numerous. It must be considered that the assessment of PM commitment and patient acceptance has yet to develop by a specific methodology fully. Hence, this element will be more complex to identify. Another limitation is that this study does not directly include the opinion of experts; nevertheless, studies that contain expert opinions have been included. Moreover, it may be necessary to successively update this study, given the continuous evolution and development of PM. We expect to publish a report on the application of the results of this study in the future.
The framework we have discussed herein permits a quantitative determination of the level of PM implementation thanks to the standardized scoring system we have developed. This system assigns equal weight to all domains in the final score. The adoption of this system is warranted by different studies (23, 39) suggesting that for the PM to be properly implemented, it must be understood as a gear in which all its parts interact and are equally important to its operation. The scores chosen (0, 1, and 2) allow those countries that are in the process of taking measures to be rewarded, it is understood that the complexity of some measures may cause them to take longer to implement in practice. A similar scoring methodology was developed in Agarwal et al.'s framework (23). Our tool penalizes studies with a score of 0 when no information can be found on any of the elements. This penalty can spur the countries concerned to do a better job of publishing and raising awareness of their national PM implementation strategies.
Since this is a quantitative framework, countries could be tentatively ranked or sorted, for guidance purposes, based on their levels of PM implementation. Such ranking could allow the highest-scoring national initiatives to be detected. Additionally, it might be useful to identify them as models or benchmarks that could then be used by other countries to come up with their own PM implementation initiatives in the future.
Something that has become clear after conducting the systematic review of studies and extracting therefrom the domains on which this framework is based is that the different stakeholders need to work together. In other words, for the PM to be properly implemented in different countries, the process needs to include different types of profiles, such as legislators, scientists, health professionals, patients, and different public and private entities. The involvement and collaboration of an educated, aware society are necessary for the implementation process to be successful. In view of these numerous collaborations and interrelationships, plans for articulating these initiatives should be drawn up. These plans should encompass all profiles and consider all implementation domains for which strong and stable funding is essential.
It is advisable for each country to evaluate its own PM implementation plan so that it may understand its strengths and weaknesses. This could allow preventative solutions to be found and new domains of action detected. Determining the level of PM implementation may be an ongoing process, given the rate of progress of both basic science and translational science in this field. In light of the many areas, professionals, and patients that have a bearing on PM, this determination should be understood as a PM-specific health system performance assessment (HSPA).
The correct implementation of PM in current health environments poses a major challenge in that the concept of PM encompasses many kinds of basic sciences, clinical specialties, pathologies, and patients. Thus, it will cause a paradigm shift in current medicine that will necessitate reforming the national health systems. This is why this study aims at a holistic approach to properly implementing PM in these health systems. It should also be taken into consideration, however, that the development of PM and its initial application must take place within each country's regulatory framework.
This study develops and proposes the first framework for the qualitative and quantitative determination of the degree of PM implementation at the international level. This innovative framework is based on a systematic review and can be used by countries with a high level of PM implementation, countries in the process of implementing PM, and countries interested in embarking on this implementation process. The adaptability of this framework to different health systems and its methodological rigor give it additional value in dealing with an emergent field with so much potential to benefit the stakeholders involved in implementing PM (e.g., scientists, clinicians, policymakers, patients, citizens). This framework, which includes a broad collection of domains obtained from a systematic review of studies, ensures PM will have a holistic and integrative approach within the different national health systems.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
LAC and PGS: conceptualization, methodology, collecting data, data extraction and analysis, interpreting the results, drafting, editing, and reviewing the manuscript. MPRL: methodology, design, and the bibliographic strategy and search. MGC: reviewing the manuscript. JABA: coordination, interpreting the results, reviewing the manuscript, and financial support. All authors have reviewed and approved the manuscript's contents and the authorship requirements have been met.
The Andalusian Health Technology Assessment Area (AETSA) has carried out this article within the framework of funding from the Ministry of Health for the development of the activities of the Annual Work Plan of the Spanish Network of Health Technology Assessment Agencies and NHS Benefits, approved in the Plenary Session of the Interterritorial Council of the NHS on 26 May 2021.
The authors kindly acknowledge Arroyo Translation Partner for writing translation contributions. The authors also thank Carmen Martín Gomez for her assistance and suggestions for PROSPERO registration of the protocol.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1039688/full#supplementary-material
1. ICPerMed ERA, PerMed. European Partnership for Personalised Medicine – EP PerMed. Madrid: ISCIII. (2022). Available online at: https://erapermed.isciii.es/wp-content/uploads/2021/02/Partnership_draft_document_EP_PerMed_2020_10_05.pdf (accessed 4 April, 2022).
2. European Science Foundation. ESF Forward Look. Personalised Medicine for the European Citizen. Strasbourg: ESF. (2012). Available online at: http://archives.esf.org/fileadmin/Public_documents/Publications/Personalised_Medicine.pdf (accessed 5 April, 2022).
3. Pearson ER. Personalized medicine in diabetes: the role of 'omics' and biomarkers. Diabet Med. (2016) 33:712–7. doi: 10.1111/dme.13075
4. Nevado Blanco J, Arribas López J, Pérez Jurado LA, Tenorio Castaño JA, Martínez Olmos J, et al. Medicina preventiva personalizada. Madrid: Fundación Instituto Roche. (2018). Available online at: https://www.institutoroche.es/static/archivos/informe-anticipando-mpp-final.pdf (accessed 3 May, 2022).
5. Orfao A, Benítez J, Corrales F, Martín-Subero I, Ordovás JM, Carracedo Á, et al. Ciencias ómicas. Madrid: Fundación Instituto Roche. (2019). Available online at: https://www.institutoroche.es/static/archivos/Informes_anticipando_CIENCIAS_OMICAS.pdf (accessed 4 May, 2022).
6. Camela E, Potestio L, Ruggiero A, Ocampo-Garza SS, Fabbrocini G, Megna M. Towards personalized medicine in psoriasis: current progress. Psoriasis. (2022) 12:231–50. doi: 10.2147/PTT.S328460
7. Yan D, Gudjonsson JE, Le S, Maverakis E, Plazyo O, Ritchlin C, et al. New Frontiers in psoriatic disease research, part i: genetics, environmental triggers, immunology, pathophysiology, and precision medicine. J Invest Dermatol. (2021) 141:2112–2122.e3. doi: 10.1016/j.jid.2021.02.764
8. Lin B, Wu S. Digital transformation in personalized medicine with artificial intelligence and the internet of medical things. Omics. (2022) 26:77–81. doi: 10.1089/omi.2021.0037
9. Tebani A, Afonso C, Marret S, Bekri S. Omics-based strategies in precision medicine: toward a paradigm shift in inborn errors of metabolism investigations. Int J Mol Sci. (2016) 17:1555. doi: 10.3390/ijms17091555
10. Flannery DB. Challenges and opportunities for effective delivery of clinical genetic services in the U.S. healthcare system. Curr Opin Pediatr. (2018) 30:740–5. doi: 10.1097/MOP.0000000000000693
11. Isaacson Barash C. Translating translational medicine into global health equity: what is needed? Appl Transl Genom. (2016) 9:37–9. doi: 10.1016/j.atg.2016.03.004
12. Lee D, Kim K. Public R&D projects-based investment and collaboration framework for an overarching south korean national strategy of personalized medicine. Int J Environ Res Public Health. (2022) 19:1291. doi: 10.3390/ijerph19031291
13. Mulder N. Development to enable precision medicine in Africa. Per Med. (2017) 14:467–70. doi: 10.2217/pme-2017-0055
14. Garrido P, Aldaz A, Calleja MÁ, De Álava E, Lamas MJ, Martín M, et al. Proposal for the creation of a national strategy for precision medicine in cancer: a position statement of SEOM, SEAP and SEFH. Farm Hosp. (2017) 41:688–91.
15. Antiñolo G, Cruz Cigudosa J, García-Foncillas J, Lamas MJ, Llerena A, López Otín C. Propuesta de Recomendaciones para una Estrategia Estatal de Medicina Personalizada de Precisión. Madrid: Fundación Instituto Roche. (2017). Available online at: https://www.institutoroche.es/static/pdfs/Propuesta_de_Recomendaciones_MPP.pdf (accessed 5 May, 2022).
16. Manolio TA. Implementing genomics and pharmacogenomics in the clinic: the National Human Genome Research Institute's genomic medicine portfolio. Atherosclerosis. (2016) 253:225–36. doi: 10.1016/j.atherosclerosis.2016.08.034
17. Raza S, Blackburn L, Moorthie S, Cook S, Johnson E, Gaynor L, et al. The Personalised Medicine Technology Landscape. Cambridge: PHG Foundation. (2018). Available online at: https://www.phgfoundation.org/media/126/download/phgf-personalised-medicine-technology-landscape-report-50918.pdf?v=1 (accessed 5 May, 2022).
18. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. (2009) 62:e1–34. doi: 10.1016/j.jclinepi.2009.06.006
19. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. (2008) 8:1–10. doi: 10.1186/1471-2288-8-45
20. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. (2017) 358:j4008. doi: 10.1136/bmj.j4008
21. Baethge C, Goldbeck-Wood S, Mertens S. SANRA-a scale for the quality assessment of narrative review articles. Res Integr Peer Rev. (2019) 4:5. doi: 10.1186/s41073-019-0064-8
22. Humphrey-Murto S, Varpio L, Gonsalves C, Wood TJ. Using consensus group methods such as Delphi and Nominal Group in medical education research. Med Teach. (2017) 39:14–9. doi: 10.1080/0142159X.2017.1245856
23. Agarwal A, Pritchard D, Gullett L, Amanti KG, Gustavsen G, A. Quantitative framework for measuring personalized medicine integration into US healthcare delivery organizations. J Pers Med. (2021) 11:196. doi: 10.3390/jpm11030196
24. Kovanda A, Zimani AN, Peterlin B. How to design a national genomic project-a systematic review of active projects. Hum Genomics. (2021) 15:20. doi: 10.1186/s40246-021-00315-6
25. Pastorino R, Lang M, Zawati MnH, Calabrò GE, Hoxhaj I, Houwink EJF, et al. Ethico-legal and Policy Issues Surrounding Personalised Medicine. In:Boccia S, Ádány R, Villari P, Cornel MC, De Vito C, Pastorino R, , editors. Personalised Health Care: Fostering Precision Medicine Advancements for Gaining Population Health Impact. Cham: Springer International Publishing. (2021). p. 57–76. doi: 10.1007/978-3-030-52399-2_4
26. Vrijenhoek T, Tonisson N, Kääriäinen H, Leitsalu L, Rigter T. Clinical genetics in transition-a comparison of genetic services in Estonia, Finland, and the Netherlands. J Community Genet. (2021) 12:277–90. doi: 10.1007/s12687-021-00514-7
27. Whitsel LP, Wilbanks J, Huffman MD, Hall JL. The role of government in precision medicine, precision public health and the intersection with healthy living. Prog Cardiovasc Dis. (2019) 62:50–4. doi: 10.1016/j.pcad.2018.12.002
28. Chanfreau-Coffinier C, Peredo J, Russell MM, Yano EM, Hamilton AB, Lerner B, et al. A logic model for precision medicine implementation informed by stakeholder views and implementation science. Genet Med. (2019) 21:1139–54. doi: 10.1038/s41436-018-0315-y
29. Delnord M, Van Valckenborgh E, Hebrant A, Antoniou A, Van Hoof W, Waeytens A, et al. Precision cancer medicine: what has translated into clinical use in Belgium? Semin Cancer Biol. (2021) 84:255–62. doi: 10.1016/j.semcancer.2021.06.010
30. Pritchard DE, Moeckel F, Villa MS, Housman LT, McCarty CA, McLeod HL. Strategies for integrating personalized medicine into healthcare practice. Per Med. (2017) 14:141–52. doi: 10.2217/pme-2016-0064
31. Ricciardi W, Boccia S. New challenges of public health: bringing the future of personalised healthcare into focus. Eur J Public Health. (2017) 27:36–39. doi: 10.1093/eurpub/ckx164
32. Pearce C, Goettke E, Hallowell N, McCormack P, Flinter F, McKevitt C. Delivering genomic medicine in the United Kingdom National Health Service: a systematic review and narrative synthesis. Genet Med. (2019) 21:2667–75. doi: 10.1038/s41436-019-0579-x
33. Pitini E, D'Andrea E, De Vito C, Rosso A, Unim B, Marzuillo C, et al. A proposal of a new evaluation framework towards implementation of genetic tests. PLoS ONE. (2019) 14:e0219755. doi: 10.1371/journal.pone.0219755
34. Unim B, Pitini E, Lagerberg T, Adamo G, De Vito C, Marzuillo C, et al. Current genetic service delivery models for the provision of genetic testing in europe: a systematic review of the literature. Front Genet. (2019) 10:552. doi: 10.3389/fgene.2019.00552
35. Bilkey GA, Burns BL, Coles EP, Bowman FL, Beilby JP, Pachter NS, et al. Genomic testing for human health and disease across the life cycle: applications and ethical, legal, and social challenges. Front Public Health. (2019) 7:40. doi: 10.3389/fpubh.2019.00040
36. Burns BL, Bilkey GA, Coles EP, Bowman FL, Beilby JP, Pachter NS, et al. Healthcare system priorities for successful integration of genomics: an australian focus. Front Public Health. (2019) 7:41. doi: 10.3389/fpubh.2019.00041
37. Chong HY, Allotey PA, Chaiyakunapruk N. Current landscape of personalized medicine adoption and implementation in Southeast Asia. BMC Med Genomics. (2018) 11:94. doi: 10.1186/s12920-018-0420-4
38. Doyle DL, Clyne M, Rodriguez JL, Cragun DL, Senier L, Hurst G, et al. Proposed outcomes measures for state public health genomic programs. Genet Med. (2018) 20:995–1003. doi: 10.1038/gim.2017.229
39. Kurnat-Thoma E. Educational and ethical considerations for genetic test implementation within health care systems. Netw Syst Med. (2020) 3:58–66. doi: 10.1089/nsm.2019.0010
40. Rajan D, Papanicolas I, Karanikolos M, Koch K, Rohrer-Herold K, Figueras J. Health system performance assessment. A primer for policy-makers. WHO: Copenhagen. (2022). Available online at: https://apps.who.int/iris/rest/bitstreams/1477293/retrieve (accessed 21 December, 2022).
41. Garrison LP Jr, Towse A. A strategy to support efficient development and use of innovations in personalized medicine and precision medicine. J Manag Care Spec Pharm. (2019) 25:1082–87. doi: 10.18553/jmcp.2019.25.10.1082
42. Faulkner E, Holtorf AP, Walton S, Liu CY, Lin H, Biltaj E, et al. Being precise about precision medicine: what should value frameworks incorporate to address precision medicine? A report of the personalized precision medicine special interest group. Value Health. (2020) 23:1522. doi: 10.1016/j.jval.2019.11.010
43. De Maria Marchiano R, Di Sante G, Piro G, Carbone C, Tortora G, Boldrini L, et al. Translational research in the era of precision medicine: where we are and where we will go. J Pers Med. (2021) 11:216. doi: 10.3390/jpm11030216
44. Hulsen T, Jamuar SS, Moody AR, Karnes JH, Varga O, Hedensted S, et al. From big data to precision medicine. Front Med (Lausanne). (2019) 6:34. doi: 10.3389/fmed.2019.00034
45. Alarcón Garavito GA, Moniz T, Déom N, Redin F, Pichini A, Vindrola-Padros C. The implementation of large-scale genomic screening or diagnostic programmes: a rapid evidence review. Eur J Hum Genet. (2022). doi: 10.1038/s41431-022-01259-8
46. Sitapati A, Kim H, Berkovich B, Marmor R, Singh S, El-Kareh R, et al. Integrated precision medicine: the role of electronic health records in delivering personalized treatment. Wiley Interdiscip Rev Syst Biol Med. (2017) 9:10.1002/wsbm.1378. doi: 10.1002/wsbm.1378
47. Vicente AM, Ballensiefen W, Jönsson JI. How personalised medicine will transform healthcare by 2030: the ICPerMed vision. J Transl Med. (2020) 18:180. doi: 10.1186/s12967-020-02316-w
48. Nardini C, Osmani V, Cormio PG, Frosini A, Turrini M, Lionis C, et al. The evolution of personalized healthcare and the pivotal role of European regions in its implementation. Per Med. (2021) 18:283–94. doi: 10.2217/pme-2020-0115
49. Atutornu J, Milne R, Costa A, Patch C, Middleton A. Towards equitable and trustworthy genomics research. EBioMedicine. (2022) 76:103879. doi: 10.1016/j.ebiom.2022.103879
50. Haiech J, Kilhoffer MC. Personalized medicine and education: the challenge. Croat Med J. (2012) 53:298–300. doi: 10.3325/cmj.2012.53.298
51. Pratt NL, Kalisch Ellett LM, Sluggett JK, Ramsay EN, Kerr M, LeBlanc VT, et al. Commitment questions targeting patients promotes uptake of under-used health services: Findings from a national quality improvement program in Australia. Soc Sci Med. (2015) 145:1–6. doi: 10.1016/j.socscimed.2015.09.019
52. Regulation (eu) 2021/2282 of the European Parliament and of the Council of 15 December 2021 on health technology assessment and amending Directive 2011/24/EU. Official Journal of the European Union (2021). Available online at: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32021R2282 (accessed April 5, 2022).
53. Aguilera-Cobos L, Rosario-Lozano MP, Ponce-Polo A, Blasco-Amaro JA, Epstein D. Barriers for the evaluation of advanced therapy medicines and their translation to clinical practice: Umbrella review. Health Policy. (2022) 126:1248–55. doi: 10.1016/j.healthpol.2022.10.007
54. Fundación Instituto Roche. Proposal of Recommendations for a Personalised Precision Medicine National Strategy. Madrid: Fundación Instituto Roche. (2017). Available online at: https://www.institutoroche.es/static/pdfs/Propuesta_de_Recomendaciones_MPP_INGLES.pdf (accessed 21 December, 2022).
Keywords: personalized medicine (PM), health policy, health system, implementation, framework
Citation: Aguilera-Cobos L, García-Sanz P, Rosario-Lozano MP, Claros MG and Blasco-Amaro JA (2023) An innovative framework to determine the implementation level of personalized medicine: A systematic review. Front. Public Health 11:1039688. doi: 10.3389/fpubh.2023.1039688
Received: 08 September 2022; Accepted: 16 January 2023;
Published: 03 February 2023.
Edited by:
Christina Mitropoulou, The Golden Helix Foundation, United KingdomReviewed by:
Michaela Th. Mayrhofer, Biobanking and Biomolecular Resources Research Infrastructure Consortium-European Research Infrastructure Consortium (BBMRI-ERIC), AustriaCopyright © 2023 Aguilera-Cobos, García-Sanz, Rosario-Lozano, Claros and Blasco-Amaro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lorena Aguilera-Cobos,  bG9yZW5hLmFndWlsZXJhQGp1bnRhZGVhbmRhbHVjaWEuZXM=; Patricia García-Sanz, cGF0cmljaWEuZ2FyY2lhLnNhbnpAanVudGFkZWFuZGFsdWNpYS5lcw==
bG9yZW5hLmFndWlsZXJhQGp1bnRhZGVhbmRhbHVjaWEuZXM=; Patricia García-Sanz, cGF0cmljaWEuZ2FyY2lhLnNhbnpAanVudGFkZWFuZGFsdWNpYS5lcw==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.