
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 17 October 2022
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.995249
 Karin Neukam1,2*
Karin Neukam1,2* Alicia Lucero3
Alicia Lucero3 Alicia Gutiérrez-Valencia1,2Lucas Amaya3Natalia Echegoyen3Antonella Martelli3
Alicia Gutiérrez-Valencia1,2Lucas Amaya3Natalia Echegoyen3Antonella Martelli3 Cristina Videla3Federico A. Di Lello4,5*†Alfredo P. Martínez3†
Cristina Videla3Federico A. Di Lello4,5*†Alfredo P. Martínez3†Background: Management of the coronavirus disease 2019 (COVID-19) pandemic caused by a novel severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) requires rapid and simple methods to detect COVID-19 patients and identify potential infectors. This study aimed to evaluate the utility of a point-of-care (PoC) rapid antigen diagnostic test (Ag-RDT) in these settings.
Patients and methods: Individuals who consecutively presented for SARS-CoV-2 testing at a tertiary care center in Buenos Aires, Argentina, underwent PoC Ag-RDT testing and real-time RT-PCR (qRT-PCR) on the same day during June 2021.
Results: Of 584 included subjects, 108 (18.5%) were symptomatic for COVID-19 while the remaining presented for miscellaneous reasons unrelated to possible or confirmed contact with a SARS-CoV-2-infected individual. A positive Ag-RDT result was obtained in 26 (24.1%) symptomatic and 7 (1.5%) asymptomatic persons (p < 0.001), which was concordant with qRT-PCR in 105/108 [97.2%, Cohen's kappa coefficient (κ) = 0.927] symptomatic and 467/476 (98.1% κ = 0.563) asymptomatic participants, with a positive percentage agreement (PPA; 95% confidence interval) of 89.7% (71.5–97.3%) and 42.9% (18.8–70.4%), respectively. None of the 11 false-negative diagnoses showed a Ct-value ≤20. Considering only failures with a Ct-value below 31 as hypothetical infectivity threshold of 105 SARS-CoV-2 RNA copies/mL, concordance was observed in 98.1% (κ = 0.746) in the asymptomatic population, accounting for a PPA of 66.7% (30.9–91%).
Conclusions: PoC Ag-RDT accurately detected active SARS-CoV-2 infection and showed acceptable diagnostic performance in asymptomatic persons potentially spreading infectious virus. Ag-RDT may therefore be useful to slow down or stop transmission by enabling adequate decisions on isolation at a public health level.
The ongoing (coronavirus disease 2019) COVID-19 pandemic caused by novel severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has taught the importance of both early diagnosis of symptomatic patients (1) to ensure medical care for COVID-19 patients, as well as the implementation of rapid public health measures in order to limit or halt transmission (2). It is estimated that up to 45% of the SARS-CoV-2 infected people do not develop symptoms (3–6), yet asymptomatic transmission may occur (7–10). Therefore, surveillance of allegedly healthy persons and screening of at-risk populations represent essential constituents of curbing the pandemic. This sudden and urgent request of SARS-CoV-2 diagnostic devices for different settings was settled through multiple emergency use authorizations (11).
Detection of viral RNA in nasopharyngeal swabs (NPS) by nucleic acid amplification test (NAAT), such as quantitative reverse transcription (qRT-) polymerase chain reaction (PCR), represents the current standard for the diagnosis of SARS-CoV-2 infection. However, PCR techniques are costly, time-consuming and require both advanced operator training and laboratory infrastructure (12, 13). Rapid antigen diagnostic tests (Ag-RDT) represent an alternative suitable to be conducted at points-of-care (PoC) as they are considerably economic, easy-to-use, and provide rapid results (14). Most Ag-RDTs shows an overall specificity close to 100% while the sensitivity varies widely from ~70–100%. Sensitivity increases substantially when tests are applied in the first 5–7 days upon symptoms onset (13–16), which coincides with SARS-CoV-2 peak viral load in the upper respiratory tract (17). However, the accuracy of firstly available Ag-RDT remains below the reference standard NAAT (ECSMIDS).
The BD Veritor Ag-RDT is based on a chromatographic digital immunoassay that qualitatively detects SARS-CoV-2 nucleocapsid antigen from nasal swabs within 15 min (18). It shows adequate diagnostic performance (19), a high user friendliness (20) and in July 2020, an emergency use authorization was issued for its use to diagnose SARS-CoV-2 infection in people showing symptoms compatible with COVID-19 ≤5 days upon onset (21). However, given the low experience and information gaps, controversy arouse on the adequacy of first- and second-generation Ag-RDT as tool to diagnose COVID-19 in people without respiratory infection symptoms (22, 23) and many Ag-RDT, including Veritor, remain to be clinically validated in the asymptomatic population (18, 19). Still, testing of asymptomatic individuals is recommended in some settings (24) and NAAT techniques may not represent an appropriate standard reference in this population as they do not distinguish infectious and non-infectious virus, thus failing to identify persons with non-infectious SARS-CoV-2 infection in whom isolation could be spared. In contrast, recent studies suggest an association between positive Ag-RDT results and cell culture positivity, as well as the presence of subgenomic RNA, a surrogate for the presence of viable virus (25, 26).
The aim of this study was to determine the diagnostic performance and to evaluate the clinical implication of the Veritor Ag-RDT when applied in symptomatic vs. asymptomatic individuals in a real-life setting.
A cross-sectional study was conducted at the Center for Medical Education and Clinical Research “Norberto Quirno” (CEMIC), Buenos Aires, Argentina. From June 1st to 30th 2021, all subjects ≥18 years old who consecutively underwent testing for SARS-CoV-2 infection were recruited. Subjects may have been attended due to (i) presence of one or more symptoms compatible with COVID-19 during five days or less or (ii) other, non-SARS-CoV-2-related, circumstances such as pre-surgical evaluation, intended traveling, returning to restricted activities, or learning about their infection status while being asymptomatic for COVID-19. After explaining the protocol, the candidates were invited to join the study and upon acceptance, they were asked to give their written informed consent.
SARS-CoV-2 Ag-RDT (index test): Antigen testing was conducted from anterior nasal swabs by the Veritor™ System for Rapid Detection of SARS-CoV-2 (Becton, Dickinson and Company, Franklin Lake, NJ, USA). This test has a limit of detection of 140 50% tissue culture infective doses of nucleocapsid protein and was used according to the manufacturer's instructions (18). Briefly, swabs were added to extraction reagent tubes at room temperature within 60 min after sampling and mixed for at least 15s. Three drops extraction buffer/specimen mixture were then added to a test cartridge. After 15 min of incubation, the test devices were interpreted using a Veritor™ Analyzer.
RT-PCR (reference standard): RNA was extracted from NPS and purified using GenePure Pro, Nucleic Acid Purification System (Bioer Technology, Hangzhou, China). qRT-PCR was performed using the RealStar® SARS-CoV-2 RT-PCR kit 1.0 (Altona Diagnostics, Hamburg, Germany) on a Roche Cobas z 480 RT-PCR device.
Descriptive statistics were performed, expressing categorical values as number (percentage) and continuous variables as median (IQR). The outcome variable was the proportion of correct (true-positive and true-negative) Ag-RDT results as confirmed by qRT-PCR. For comparison of categorical variables, the Chi-square or the Fisher's tests were applied while continuous variables were analyzed by means of the Student's t-test or the Mann-Whitney U test. In order to assess the agreement between Ag-RDT and qRT-PCR outcomes, Cohen's kappa coefficient (κ) was calculated. Diagnostic performance was evaluated by calculating the positive (PPA), negative (NPA) and overall (OPA) percent agreement, as well as, the positive (PPV) and negative (NPV) predictive value with their respective 95% confidence interval (95CI). Statistical analyses were carried out using the SPSS statistical software package release 23.0 (IBM SPSS Inc., Chicago, IL, USA) and STATA 9.0 (StataCorp LP, College Station, TX, USA).
The study was designed and performed according to the Helsinki declaration and all blood donors gave their written informed consent (Study protocol EX-2021-06438339-UBA DME#SSA_FFYB, Ethics committee of the Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires).
A sample of 584 subjects was included in the study, 108 (18.5%) participants were symptomatic for COVID-19 while the remaining 476 (81.5%) did not present COVID-19-related symptoms. Thirty-one (41.9%) presented with only one symptom, 43 (58.1%) with ≥2, and 29 (39.2%) with ≥3. Among the 358 (61.3%) female participants, 61 (56.5%) were symptomatic and 297 (62.4%) were asymptomatic, p = 0.152. The proportions of the different symptoms are shown in Figure 1. The median (IQR) age was 43 (33–55) years, corresponding figures for those with and without symptoms were 46 (33–67) and 42 (33–54) years, p = 0.045, respectively.
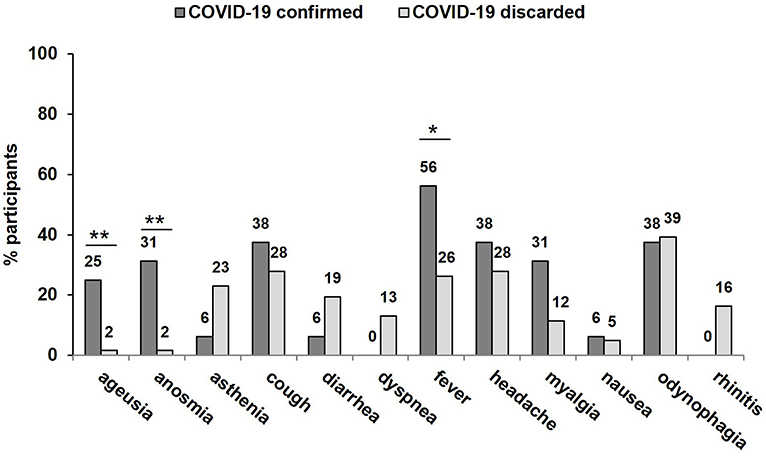
Figure 1. Proportions of different symptoms as reported at the day of testing for SARS-CoV-2-infection stratified for the presence of COVID-19. *p < 0.05; **p < 0.01.
A positive qRT-PCR result was obtained in 29 (26.9%) individuals who presented with symptoms and in 14 (2.9%) who did not (p < 0.001), accounting for 7.4% overall prevalence of SARS-CoV-2 infection in the study population. In symptomatic individuals, Ag-RDT testing yielded 26 (24.1%) positive results, while among the asymptomatic, 7 (1.5%) subjects tested positive (p < 0.001). Results from Ag-RDT and reference qRT-PCR were concordant in 572/584 (97.9%; κ = 0.831) determinations: 105/108 (97.2%; κ = 0.927) among symptomatic individuals and 467/476 (98.1% κ = 0.563) among the asymptomatic participants. Only one (8.3%) out of the 12 discordant diagnoses was false-positive. None (0%) of the individuals who presented with more than one symptom had a discordant result. Detailed diagnostic performance is shown in Table 1.
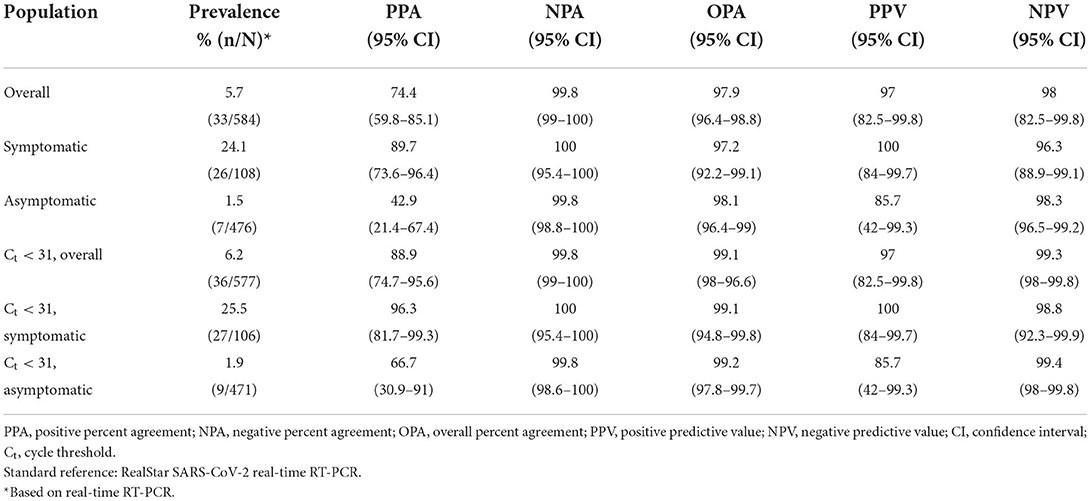
Table 1. Diagnostic performance of the BD Veritor System for Rapid Detection of SARS-CoV-2.
Ag-RDT results were not in agreement with qRT-PCR in 8 (2.2%) women and 4 (1.8%) males, p = 0.774. Median age among cases with a discordant vs. a concordant result was 43.4 (33.1–63.3) and 23 (33–54.9) years, respectively, p = 0.560. Overall median (IQR) qRT-PCR cycle threshold (Ct-values) were 21.8 (17.9–28.5): 21.6 (17.1–24.3) vs. 26.6 (20.2–33.2) for samples derived from symptomatic and asymptomatic participants (p = 0.034). Figure 2 shows the corresponding Ct-values stratified for testing agreement and the presence of symptoms. None of the 11 false-negative diagnoses by Ag-RDT showed a Ct-value ≤20 while 5 (45%) had a Ct-value ≥33. Considering only failures with a Ct-value below 31, accounting for a SARS-CoV-2 viral load of 105 copies/mL (27), overall agreement between Ag-RDT and qRT-PCR was observed in over 99% (κ = 0.923), being almost perfect among those with symptoms (κ = 0.975) and substantial in those without (κ = 0.746), respectively. The diagnostic performance in the overall population and the subgroups is presented in Table 1.
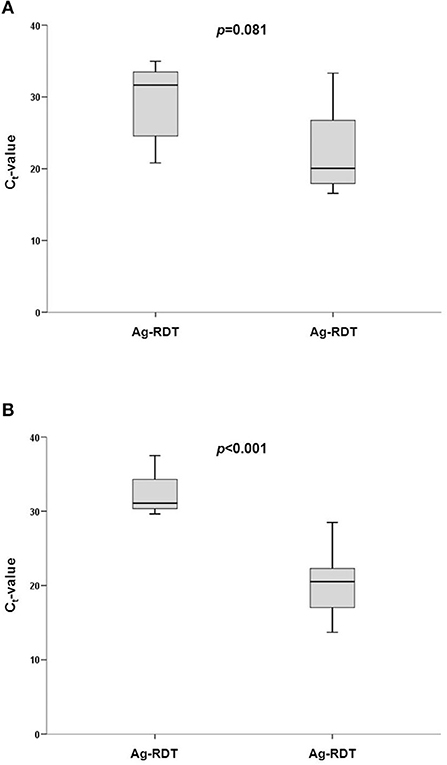
Figure 2. Cycle threshold (Ct)-values observed for SARS-CoV-2 determination by qRT-PCR according to agreement with BD Veritor System for Rapid Detection of SARS-CoV-2 (Veritor) in (A) asymptomatic and (B) symptomatic participants.
The present study confirms the accuracy of a commercially available PoC Ag-RDT to identify COVID-19 in a real-life setting of patients showing a flu-like symptomatic profile, which is crucial when rapid diagnosis is required for taking emergency clinical management decisions. Furthermore, in those without known prior contact with a SARS-CoV-2 index case and who were asymptomatic for COVID-19, the Ag-RDT showed a good clinical performance for Ct-values below a theoretical infectivity threshold.
While current guidelines strongly recommend the use of NAAT vs. Ag-RDT testing in individuals with symptoms compatible with severe or critical illness, or symptomatic persons at high risk for a severe course of infection, there is only a weak recommendation against Ag-RGT use in those with moderate symptoms, disregarding the age and the date of system onset (22). As these recommendations are based on a very low certainty of evidence, Ag-RGT testing is considered an alternative when NAAT are not available (23). In asymptomatic individuals at risk of exposure, testing is recommended in various settings (24) however, recommendations on the testing strategy is inconsistent or no recommendation is given due to the lack of evidence (22, 23). Thus, the benefits of PoC Ag-RDT at a population health level remain uncertain as available data is scarce and inconsistent, mainly due to deficient study designs (28). Even less is known about their performance in subjects who did not have contact with an index case and who are therefore likely to show a lower prevalence of SARS-CoV-2 infection as compared to symptomatic individuals, which positively correlates with test sensitivity (29). The considerably low sensitivity of Ag-RDTs observed in asymptomatic individuals (13) represents a major drawback. Indeed, in the present study, an overall PPA of 42.9% in the asymptomatic population, which lies within the considerably wide sensibility range previously reported for Veritor (30–33). However, it is worth to note that these low values are derived from comparisons with RT-PCR, in which a positive result does not necessarily imply infectiveness, since NAAT does not distinguish inactive from viable virus. Although shedding of SARS-CoV-2 RNA and consequently positive RT-PCR results may persist over weeks (17), data on cell culture of respiratory tract isolates suggest that infectious virus are only present during the first 8–12 days (34–37). It is estimated that, in general, viral shedding exceeds shedding of viable virus up to 45 days, whereas infectious virus may be present up to 6 days prior to symptom onset. Hence, an unsurprisingly low agreement between RT-PCR and cell culture has been found (34). In contrast, sensitivity roughly doubled from 24–50 to 50–82% when matched with cell culture (38) and the herein applied Veritor test in particular showed a PPV of 90% using viral culture as standard reference (34). This finding was confirmed in a recent study, in which Veritor showed a sensitivity of 74% when compared to cell culture (25). Similarly, a study on the diagnostic performance of different Ag-RGT by contrasting the results with detection of subgenomic RNA suggests their ability to determine the presence or absence of replication-competent, thus potentially transmissible, virus (26). In order to implement these findings to the clinical practice, one should take into account the role of infectivity. While various studies have investigated the infectivity of SARS-CoV-2 viral load, no standard threshold has been established. A relation between the Ct-value and cell culture positivity has widely been reported (7, 36, 37, 39, 40), with an observed decrease by 0.32–0.67 in the estimated odds ratio of recovering infectious virus with each unit increase in Ct-value (37, 40). In accordance with these findings, in the present study, the sensitivity of the Ag-RDT among asymptomatic participants increased more than 1.5-fold when only failures with Ct-values below 31 were considered, which is also below the Veritor Ag-RDT median Ct-value of 32 for false-negative results in asymptomatic individuals compared to NAAT, according to a recent study (32). Likewise, this threshold is within the range of previous reports where a low or no proportion of positive viral cultures were obtained for Ct-values varying from 28 to 34 (7, 36, 39). This variability may be explained by the fact that the Ct-value is subject to the RT-PCR parameters and comparisons between studies using it as surrogate for viral load have to be drawn with caution (41). Taken into account the RT-PCR assay applied in the present work, a Ct-value of 31 corresponds to a viral load of approximately 105 copies/mL (27). To note, this value is one to two orders of magnitude below the hypothetical infectiousness threshold range of 106-107 copies/mL as the in-vitro isolation of replicative virus suggests (40, 42, 43). Also, it corresponds to the range of viral load below which the sensitivity of the Veritor test becomes almost zero when compared to viral culture, as reported recently (25). In accordance, in a large contact tracing study, ~15 vs. 50% RT-PCR-positive contacts were identified when index cases presented a viral load below 104 vs. 106 copies/ml, respectively (44). Taken together, the Ag-RDT showed moderate performance in detecting SARS-CoV-2 infection amongCOVID-19 asymptomatic persons with a low prevalence of infection in a real-life setting. However, rather than detecting infection, the test may be useful to rapidly identify potential infectors during their viral load peak, who should be isolated and, at the same time, it may be able to spare confinement for those who are not infectious. Based on these findings, large prospective studies should be designed in order to confirm this issue.
In symptomatic individuals, an adequate diagnostic performance of many but not all commercially available Ag-RDT to detect SARS-CoV-2 infection has been demonstrated in various studies (13, 15, 16). Still, reports on the sensitivity Ag-RDT vary wildly. In the present study with a considerably high sample size, a sensitivity of 89.7 % (CI: 71.5–97.3%), with only 3 out of 26 false-negative results, and a specificity of 100 % (CI: 94.2–99.9%) was observed in symptomatic patients during the first 5 days of symptom onset. A similar performance has been reported in real-life studies, where sensitivities from 76% to over 90% were observed (20, 30, 33, 45). Likewise, a study on Veritor meeting the FDA criteria for emergency use authorization approval found a sensitivity of 82–88% during the first 6 days of symptom onset. The herein presented results therefore confirm the accuracy of the Veritor Ag-RDT for diagnosing COVID-19 in the early stage of symptomatic infection.
Another obstacle to ensure effective surveillance represents the identification of symptoms compatible with COVID-19. While the symptoms reported by the participants in this study were consistent with COVID-19 (1), the majority were also compatible with infection by influenza viruses (1, 18, 46). Of the individual symptoms, only ageusia, anosmia and, to a lesser extent, fever were significantly associated with confirmed COVID-19, which is in accordance with previous reports (46), while symptoms such as asthenia, diarrhea, and rhinitis were not. The similarity of COVID-19-related complex with influenza virus infection may cause actual SARS-CoV-2 infected persons to weigh up whether to present for testing. The possibility of obtaining a result fast and in a setting that is easy to access, together with the widely unconsidered fact that anterior nasal sampling results in far less objection than NPS required for NAAT, adds up to a higher probability of individuals actually undergoing a test when showing symptoms, therefore lowering the rate of undiagnosed infection. To note, this is also probably even more the case for asymptomatic testing.
In the present study, age and gender did not impact in the agreement between the Ag-RDT and RT-PCR results, which is in accordance with previously reported data (27). This is not surprising since no clinically relevant differences in SARS-CoV-2 viral loads according to age (47, 48) and gender (48) have been described. A mild age impact has been reported in a study on the use of Veritor Ag-RDT in self-sampling testing, however, the authors hypothesize that this is likely attributable to lower sampling skills rather than the age itself (49).
The main limitation of this study is that cell culture and RT-PCR calibration were not done in-house. To date, a considerable gap in understanding the viral dynamics, infectiousness, and prevention of disease spread remains, especially in this rapidly changing setting including emergent viral variants with a different infection profile and the availability of vaccines. Randomized clinical trials and large, prospective real-life studies are warranted to confirm the role of Ag-RDT as discussed herein. Additionally, no second test in asymptomatic persons was conducted as proposed by the manufacturer due to the lack of validation studies in asymptomatic individuals (18). The analysis of consecutive results may have been interesting as another study on the Veritor test described a positive rate of 63% 2 weeks after a false-negative determination (27). However, this study did not include follow-up visits in order to keep the burden for the patients as low as possible.
In conclusion, the PoC Ag-RDT showed a good performance in diagnosing COVID-19 in patients during the first days of symptom onset, allowing rapid medical care and isolation measures when molecular techniques are not available. However, prevention measures of viral spread to slow down or stop the pandemic cannot be limited to the symptomatic population. The use of economic, rapid, and simple Ag-RDT may be an appropriate approach for large-scale surveillance and screening conducted in remote settings in order to identify individuals who are likely to be shedding infectious virus, which would otherwise go unnoticed. Facilitating decisions on measures regarding isolation and contact tracing could represent an essential tool for public health management of the COVID-19 pandemic.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires. The patients/participants provided their written informed consent to participate in this study.
KN, FD, and APM: study design, conception, and drafting of the manuscript. LA, NE, AM, and CV: data collection. KN, AL, FD, and APM: data analysis and interpretation. All authors provided intellectual content of critical importance to the work described, read, and agreed to the published version of the manuscript.
This work was supported by the Instituto de Salud Carlos III, co-financed by the European Development Regional Fund (A way to achieve Europe), Subprograma Miguel Servet (grant numbers CP19/00159 to AG-V and CPII18/00033 to KN). FD is a member of the National Research Council (CONICET) Research Career Program. KN is the recipient of a Senior Researcher Contract by the Office for Families and Health of the Andalusian Council (RH-0019-2021).
We would like to thank to Mrs. Silvina Heisecke from CEMIC-CONICET for the copyediting of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization. Similarities and Differences Between Flu and COVID-19. (2022). Available online at: https://www.cdc.gov/flu/Symptoms/flu-Vs-Covid19.htm (accessed August 31, 2022).
2. World Health Organization. COVID-19 Strategic Preparedness and Response Plan. (2021). Available online at: https://apps.who.int/iris/bitstream/handle/10665/340072/WHO-WHE-2021.02-eng.pdf?sequence=1&isAllowed=y (accessed August 31, 2022).
3. Chen X, Huang Z, Wang J, Zhao S, Wong MCS, Chong KC, et al. Ratio of asymptomatic COVID-19 cases among ascertained SARS-CoV-2 infections in different regions and population groups in 2020: a systematic review and meta-analysis including 130 123 infections from 241 studies. BMJ Open. (2021) 11:e049752. doi: 10.1136/bmjopen-2021-049752
4. Oran DP, Topol EJ. The proportion of SARS-CoV-2 infections that are asymptomatic: a systematic review. Ann Intern Med. (2021) 174:655–62. doi: 10.7326/M20-6976
5. Sah P, Fitzpatrick MC, Zimmer CF, Abdollahi E, Juden-Kelly L, Moghadas SM, et al. Asymptomatic SARS-CoV-2 infection: a systematic review and meta-analysis. Proc Natl Acad Sci U S A. (2021) 118:1–12. doi: 10.1073/pnas.2109229118
6. Anderson RM, Vegvari C, Hollingsworth TD, Pi L, Maddren R, Ng CW, et al. The SARS-CoV-2 pandemic: Remaining uncertainties in our understanding of the epidemiology and transmission dynamics of the virus, and challenges to be overcome. Interface Focus. (2021) 11: 20210008. doi: 10.1098/rsfs.2021.0008
7. Arons MM, Hatfield KM, Reddy SC, Kimball A, James A, Jacobs JR, et al. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N Engl J Med. (2020) 382:2081–90. doi: 10.1056/NEJMoa2008457
8. Zhou R, Li F, Chen F, Liu H, Zheng J. Viral dynamics in asymptomatic patients with COVID-19. Int J Inf Dis. (2020) 96:288–90. doi: 10.1016/j.ijid.2020.05.030
9. Ravindra K, Malik VS, Padhi BK, Goel S, Gupta M. Asymptomatic infection and transmission of COVID-19 among clusters: systematic review and meta-analysis. Public Health. (2021) 203:100–9. doi: 10.1016/j.puhe.2021.12.003
10. Widders A, Broom A, Broom J. SARS-CoV-2: The viral shedding vs infectivity dilemma. Infect Dis Heal. (2020) 25:210–5. doi: 10.1016/j.idh.2020.05.002
11. U.S. Food and Drug Administration. In Vitro Diagnostics EUAs. (2022). Available online at: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/in-vitro-diagnostics-euas (accessed August 31, 2022).
12. World Health Organization. Recommendations For National SARS-CoV-2 Testing Strategies And Diagnostic Capacities. (2021) p. 1–16. Available online at: https://www.who.int/publications/i/item/WHO-2019-nCoV-lab-testing-2021.1-eng (accessed August 31, 2022).
13. Dinnes J, Deeks JJ, Berhane S, Taylor M, Adriano A, Davenport C, et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst Rev. (2021) CD013705. doi: 10.1002/14651858.CD013705
14. World Health Organization. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection. (2021). Available from: https://www.who.int/publications/i/item/antigen-detection-in-the-diagnosis-of-SARS-CoV-2infection-using-rapid-immunoassays (accessed August 1, 2022).
15. Brümmer LE, Katzenschlager S, Gaeddert M, Erdmann C, Schmitz S, Bota M, et al. Accuracy of novel antigen rapid diagnostics for SARS-CoV-2: a living systematic review and meta-analysis. PLoS Med. (2021) 18:1–41. doi: 10.1371/journal.pmed.1003735
16. Scheiblauer H, Filomena A, Nitsche A, Puyskens A, Corman VM, Drosten C, et al. Comparative sensitivity evaluation for 122 CE-marked rapid diagnostic tests for SARS-CoV-2 antigen, Germany, September 2020 to April 2021. Eurosurveillance. (2021) 26:1–13. doi: 10.2807/1560-7917.ES.2021.26.44.2100441
17. Walsh KA, Jordan K, Clyne B, Rohde D, Drummond L, Byrne P, et al. SARS-CoV-2 detection, viral load and infectivity over the course of an infection. J Infect. (2020) 81:357–71. doi: 10.1016/j.jinf.2020.06.067
18. Becton Dickinson and Company. Use of BD Veritor TM System for Rapid Detection of SARS-CoV-2 with the BD Veritor TM Plus Analyzer 2021. Food and Drug Administration. In: Vitro Diagnostics EUAs - Antigen Diagnostic Tests for SARS-CoV-2. Available online at: https://www.fda.gov/media/139755/download (accessed June 30, 2022).
19. Young S, Taylor SN, Cammarata CL, Varnado KG, Roger-Dalbert C, Montano A, et al. Clinical evaluation of BD veritor SARS-CoV-2 point-of-care test performance compared to PCR-based testing and versus the sofia 2 SARS antigen point-of-care test. J Clin Microbiol. (2021) 59:1–11. doi: 10.1128/JCM.02338-20
20. Yin N, Debuysschere C, Decroly M, Bouazza FZ, Collot V, Martin C, et al. SARS-CoV-2 Diagnostic tests: algorithm and field evaluation from the near patient testing to the automated diagnostic platform. Front Med. (2021) 8:650581. doi: 10.3389/fmed.2021.650581
21. Food Drug Administration. In Vitro Diagnostics EUAs - Antigen Diagnostic Tests for SARS-CoV-2. Available online at: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/in-vitro-diagnostics-euas-antigen-diagnostic-tests-SARS-CoV-2 (accessed August 31, 2022).
22. Fragkou PC, De Angelis G, Menchinelli G, Can F, Garcia F, Morfin-Sherpa F, et al. ESCMID COVID-19 guidelines: diagnostic testing for SARS-CoV-2. Clin Microbiol Inf. (2022). doi: 10.1016/j.cmi.2022.02.011
23. Hanson KE, Altayar O, Caliendo AM, Arias CA, Englund JA, Hayden MK, et al. The infectious diseases society of america guidelines on the diagnosis of coronavirus disease 2019 (COVID-19): antigen testing. Clin Inf Dis. (2021) ciab557. doi: 10.1093/cid/ciab557
24. Carrara E, Ong DSY, Hussein K, Keske S, Johansson AF, Presterl E, et al. ESCMID guidelines on testing for SARS-CoV-2 in asymptomatic individuals to prevent transmission in the health care setting. Clin Microbiol Inf. (2022) 28:672–80. doi: 10.1016/j.cmi.2022.01.007
25. Kirby JE, Riedel S, Dutta S, Arnaout R, Cheng A, Ditelberg S, et al. SARS-CoV-2 Antigen Tests Predict Infectivity based on viral culture: comparison of antigen, PCR viral load, and viral culture testing on a large Sample Cohort. Clin Inf Dis. (2022). doi: 10.1016/j.cmi.2022.07.010. [Epub ahead of print].
26. De Angelis G, Menchinelli G, Liotti FM, Marchetti S, Salustri A, Vella A, et al. SARS-CoV-2 antigen test results to infer active or non-active virus replication status in COVID-19 patients. Diagnostics. (2022) 12:1338. doi: 10.3390/diagnostics12061338
27. Visseaux B, Le Q, Collin G, Ferré V. Evaluation of the RealStar® SARS-CoV-2 RT-PCR kit RUO performances and limit of detection. J Clin Virol. (2020) 129:104520. doi: 10.1016/j.jcv.2020.104520
28. Walsh KA, Broderick N, Ahern S, Carrigan M, Fawsitt CG, Brien KMO, et al. Effectiveness of rapid antigen testing for screening of asymptomatic individuals to limit the transmission of SARS-CoV-2: a rapid review. Rev Med Virol. (2022) e2350. doi: 10.1002/rmv.2350
29. Becton Dickinson. BD VeritorTM System for Rapid Detection of SARS-CoV-2. (2022). Available online at: https://www.bd.com/en-uk/products/diagnostics-systems/point-of-care-testing/bd-veritor-system-for-rapid-detection-of-SARS-CoV-2 (accessed June 30, 2022).
30. Schuit E, Veldhuijzen IK, Venekamp RP, Van Den Bijllaardt W, Pas SD, Lodder EB, et al. Diagnostic accuracy of rapid antigen tests in asymptomatic and presymptomatic close contacts of individuals with confirmed SARS-CoV-2 infection: Cross sectional study. BMJ. (2021) 374:n1676. doi: 10.1136/bmj.n1676
31. Caruana G, Croxatto A, Kampouri E, Kritikos A, Opota O, Foerster M, et al. Implementing SARS-CoV-2 rapid antigen testing in the emergency ward of a swiss university hospital: the increase study. Microorganisms. (2021) 9:798–811. doi: 10.3390/microorganisms9040798
32. Robinson ML, Mirza A, Gallagher N, Boudreau A, Garcia L, Yu T, et al. Limitations of molecular and antigen test performance for SARS-CoV-2 in symptomatic and asymptomatic COVID-19 contacts. J Clin Microbiol. (2022) 60:e0018722. doi: 10.1128/jcm.00187-22
33. Venekamp RP, Veldhuijzen IK, Moons KGM, van den Bijllaardt W, Pas SD, Lodder EB, et al. Detection of SARS-CoV-2 infection in the general population by three prevailing rapid antigen tests: cross-sectional diagnostic accuracy study. BMC Med. (2022) 20:1–13. doi: 10.1186/s12916-022-02300-9
34. Pekosz A, Parvu V, Li M, Andrews JC, Manabe YC, Kodsi S, et al. Antigen-based testing but not real-time polymerase chain reaction correlates with severe acute respiratory syndrome Coronavirus 2 viral culture. Clin Infect Dis. (2021) 73:E2861–6. doi: 10.1093/cid/ciaa1706
35. Cevik M, Tate M, Lloyd O, Maraolo AE, Schafers J, Ho A. SARS-CoV-2, SARS-CoV, and MERS-CoV viral load dynamics, duration of viral shedding, and infectiousness: a systematic review and meta-analysis. Lancet Microbe. (2021) 2:e13–22. doi: 10.1016/S2666-5247(20)30172-5
36. Kim M-C, Cui C, Shin K-R, Bae J-Y, Kweon O-J, Lee M-K, et al. Duration of culturable SARS-CoV-2 in hospitalized patients with Covid-19. N Engl J Med. (2021) 384:671–3. doi: 10.1056/NEJMc2027040
37. Singanayagam A, Patel M, Charlett A, Bernal JL, Saliba V, Ellis J, et al. Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020. Eurosurveillance. (2020) 25:1–5. doi: 10.2807/1560-7917.ES.2020.25.32.2001483
38. Kohmer N, Toptan T, Pallas C, Karaca O, Pfeiffer A, Westhaus S, et al. The comparative clinical performance of four SARS-CoV-2 rapid antigen tests and their correlation to infectivity in vitro. J Clin Med. (2021) 10:1–11. doi: 10.3390/jcm10020328
39. La Scola B, Le Bideau M, Andreani J, Hoang VT, Grimaldier C, Colson P, et al. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur J Clin Microbiol Infect Dis. (2020) 39:1059–61. doi: 10.1007/s10096-020-03913-9
40. Bullard J, Dust K, Funk D, Strong JE, Alexander D, Garnett L, et al. Predicting infectious severe acute respiratory syndrome coronavirus 2 from diagnostic samples. Clin Infect Dis. (2020) 71:2663–6. doi: 10.1093/cid/ciaa638
41. Malecki M, Luesebrink J, Wendel AF, Mattner F. Analysis of external quality assessment samples revealed crucial performance differences between commercial RT-PCR assays for SARS-CoV-2 detection when taking extraction methods and real-time-PCR instruments into account. J Virol Methods. (2021) 295:114202. doi: 10.1016/j.jviromet.2021.114202
42. Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Müller MA, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. (2020) 581:465–9. doi: 10.1038/s41586-020-2196-x
43. van Kampen JJA, van de Vijver DAMC, Fraaij PLA, Haagmans BL, Lamers MM, Okba N, et al. Duration and key determinants of infectious virus shedding in hospitalized patients with coronavirus disease-2019 (COVID-19). Nat Commun. (2021) 12:8–13. doi: 10.1038/s41467-020-20568-4
44. Lee LYW, Rozmanowski S, Pang M, Charlett A, Anderson C, Hughes GJ, et al. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infectivity by viral load, s gene variants and demographic factors, and the utility of lateral flow devices to prevent transmission. Clin Infect Dis. (2022) 74:407–15. doi: 10.1093/cid/ciab421
45. Van der Moeren N, Zwart VF, Lodder EB, Van den Bijllaardt W, Van Esch HRJM, Stohr JJJM, et al. Evaluation of the test accuracy of a SARS-CoV-2 rapid antigen test in symptomatic community dwelling individuals in the Netherlands. PLoS ONE. (2021) 16:1–11. doi: 10.1371/journal.pone.0250886
46. Sudre CH, Keshet A. Graham MaS, Joshi AD, Shilo S, Rossman H, et al. Anosmia, ageusia, and other COVID-19-like symptoms in association with a positive SARS-CoV-2 test, across six national digital surveillance platforms: an observational study. Lancet Digit Heal. (2021) 3:e577–86. doi: 10.1016/S2589-7500(21)00115-1
47. Jones TC, Biele G, Mühlemann B, Veith T, Schneider J, Beheim-Schwarzbach J, et al. Estimating infectiousness throughout SARS-CoV-2 infection course. Science. (2021) 373:1–13. doi: 10.1126/science.abi5273
48. Jacot D, Greub G, Jaton K, Opota O. Viral load of SARS-CoV-2 across patients and compared to other respiratory viruses. Microbes Infect. (2020) 22:617–21. doi: 10.1016/j.micinf.2020.08.004
Keywords: SARS-CoV-2, COVID-19, point-of-care, rapid antigen testing, PCR, public health, viral kinetics, surveillance
Citation: Neukam K, Lucero A, Gutiérrez-Valencia A, Amaya L, Echegoyen N, Martelli A, Videla C, Di Lello FA and Martínez AP (2022) Point-of-care detection of SARS-CoV-2 antigen among symptomatic vs. asymptomatic persons: Testing for COVID-19 vs. infectivity. Front. Public Health 10:995249. doi: 10.3389/fpubh.2022.995249
Received: 15 July 2022; Accepted: 12 September 2022;
Published: 17 October 2022.
Edited by:
Daniel Diaz, Universidad Nacional Autónoma de México, MexicoReviewed by:
Luis M. Real, Hospital Universitario Nuestra Señora de Valme, SpainCopyright © 2022 Neukam, Lucero, Gutiérrez-Valencia, Amaya, Echegoyen, Martelli, Videla, Di Lello and Martínez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Karin Neukam, a2FyaW4ubmV1a2FtQGdtYWlsLmNvbQ==; Federico A. Di Lello, ZmFkaWxlbGxvQGZmeWIudWJhLmFy
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.