
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 22 November 2022
Sec. Public Mental Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.991292
This article is part of the Research Topic The COVID-19 Pandemic, Problematic Internet Use, Post-traumatic Stress and Mental Health View all 21 articles
 Lara Hubenschmid1*
Lara Hubenschmid1* Isabella Helmreich1
Isabella Helmreich1 Göran Köber2,3
Göran Köber2,3 Donya Gilan1,4
Donya Gilan1,4 Svenja B. Frenzel5
Svenja B. Frenzel5 Rolf van Dick5Klaus Lieb1,4
Rolf van Dick5Klaus Lieb1,4The SARS-CoV-2 pandemic turned out to be a serious threat to mental and physical health. However, the relative contribution of corona-specific (DHs) and general stressors (DHg) on mental burden, and specific protective and risk factors for mental health are still not well understood. In a representative sample (N = 3,055) of the German adult population, mental health, potential risk, and protective factors as well as DHs and DHg exposure were assessed online during the SARS-CoV-2 pandemic (June and July 2020). The impact of these factors on mental health was analyzed using descriptive statistics, data visualizations, multiple regressions, and moderation analyses. The most burdensome DHg were financial and sleeping problems, respectively, and DHs corona-media reports and exclusion from recreational activities/important social events. 31 and 24% of total mental health was explained by DHg and DHs, respectively. Both predictors combined explained 36%, resulting in an increase in variance due to DHs of only 5% (R2 adjusted). Being female, older and a lower educational level were identified as general risk factors, somatic diseases as a corona-specific risk factor, and self-efficacy and locus of control (LOC) proved to be corona-specific protective factors. Further analyses showed that older age and being diagnosed with a somatic illness attenuated the positive influence of LOC, self-efficacy, and social support on resilience. Although the data showed that after the first easing restrictions, the stressor load was comparable to pre-pandemic data (with DHs not making a significant contribution), different risk and protective factors could be identified for general and corona-specific stressors. In line with observations from network analysis from other groups, the positive impact of resilience factors was especially diminished in the most vulnerable groups (elderly and somatically ill). This highlights the need to especially target these vulnerable groups to foster their resilience in upcoming waves of the corona pandemic.
The SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) pandemic has shown to be a threat to physical as well as mental health [e.g., (1, 2)]. Not only the existential fears evoked by the virus itself (fear of illness, suffering, and death) are stressful, but also the regulatory policies such as lockdown and their resulting social distancing, self-isolation, financial insecurity, or travel restrictions. Moreover, secondary consequences such as an impending economic crisis and recession are feared (3, 4). Different systematic reviews showed that the COVID-19 pandemic evoked significant increases in depression, anxiety, and posttraumatic stress symptoms in the general population during (5, 6) and after the first (3, 7) and subsequent COVID waves (8, 9). In the general population, studies also showed slightly higher levels of psychological distress compared to pre-pandemic data (3, 10, 11). Quarantine measures appeared to have a particularly negative impact on psychological wellbeing, with higher prevalence rates of psychological distress symptoms (e.g., irritability, insomnia, and emotional exhaustion) and mental disorders (e.g., depression) demonstrated thereafter [e.g., (12, 13)]. Both, fear appeals, that have intentionally been used to increase compliance rates for infection control measures (14, 15), as well as the spread of rumors (16) have also been shown to have negative psychological effects (including the loss of trust in mental health services or policies) (13).
Thereby, those with chronical illness or poorer health (7, 9, 17) or a relative or acquaintance infected with COVID-19 (17, 18) as well as women (3, 11, 19–23) were identified as particularly vulnerable. Further risk factors were catastrophizing thinking, the personality trait neuroticism, and the need for instrumental support (2). Research shows that specific resilience factors (as social support or optimism) help humans to cope with stressful life events (24, 25) and mitigate risk factors (26–28). There is corresponding evidence that some of those factors, e.g., positive appraisal and optimism (2, 29), perceived social support (18, 30, 31), self-efficacy, cognitive flexibility (32) and locus of control (LOC) (7, 30, 33), strengthened mental health during the pandemic. It should be noted, however, that these strategies were more difficult to apply (e.g., optimism) during periods of closure or constant negative news (34).
Although corona-specific stressors significantly contribute to the total stressor load experienced during a pandemic, also general micro-stressors (35, 36) or “daily hassles” [“demands that, to some degree, characterize everyday transactions with the environment and are classified as irritating, frustrating, and unsettling” (37), p. 3] are present, which also contribute to the total stressor load. Daily hassles are considered a good predictor of psychological symptoms, because they involve immediate adjustment processes (37) and may also have profound negative effects on mental health, especially if they are numerous and enduring (38). Seery et al. (39) examined u-shaped relationships across the lifespan between adversities and wellbeing (lower global distress, posttraumatic stress symptoms and functional impairment, and higher life satisfaction). Their results showed that individuals who experienced less lifetime adversity suffered comparatively more from being confronted with current adversity compared to people with moderate lifetime adversities. However, when there were too many cumulative stressors, this turned into a negative effect on wellbeing (e.g., stress-associated diseases).
Although numerous studies have been published researching stressor load as well as risk and resilience factors during the pandemic, only a few examined this in representative samples (3). Moreover, none of these studies examined the specific contribution of corona-specific (DHs) and general stressors (DHg) and their relative impact on mental burden during the pandemic. Our study, therefore, used a representative sample of the German population in order to investigate: (1) the stressor load (DHs and DHg and their relative contributions) in the German population during the SARS-CoV-2 pandemic in summer 2020, (2) the relative impact of DHs and DHg and their combination on mental health, and (3) risk and resilience factors with a special focus on their relevance in vulnerable groups such as older people. The study aim is also graphically represented in Figure 1.
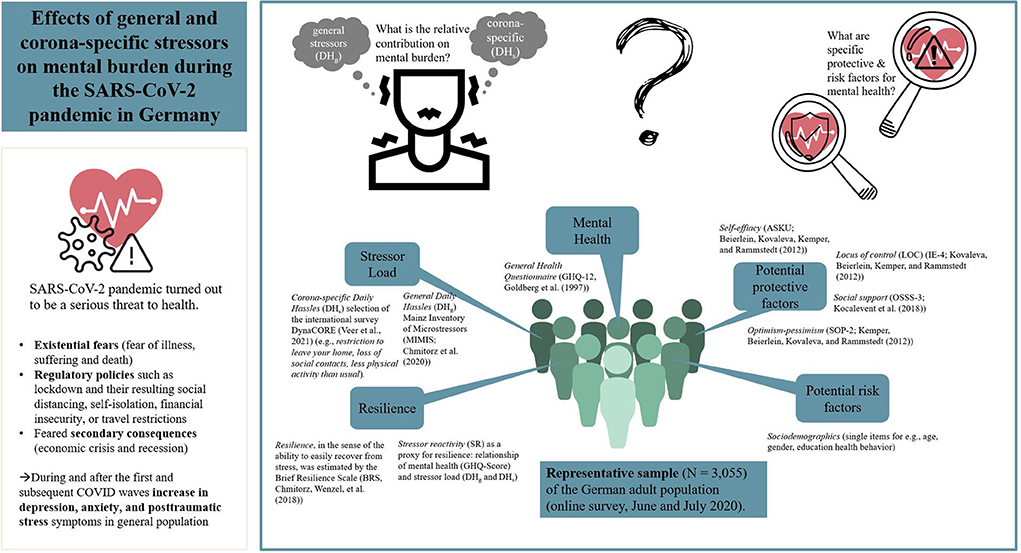
Figure 1. Graphical representation of the study aims.
A representative sample (N = 3,055) of the adult German population (18+ years) was assessed in cooperation with the infratest dimap polling institute between June 26th and July 19th, 2020. This time period was characterized by a steady decline in 7-day incidence (3.3 per 100,000 cases) after the first wave of the pandemic in March 2020. The hospitalization rate was 17%, and the mortality rate was just under 5%. Testing capacity was significantly expanded, and the Corona alert app for contact tracking was just introduced (40). Contact restrictions were lifted, stores and restaurants reopened, and schools resumed regular operations. Nevertheless corona-specific protective measures and restrictions (e.g., social distancing) and fears of infection and of the next wave were present (41). By using a weighting variable (with the variables age, education, state, and gender), slightly overrepresented populations can be weighted downward, and underrepresented populations can be weighted upward in the dataset so that the weighted dataset reflects the population. All calculations were computed once with and once without the weighting variable, and no differences emerged. We adopted the minimal correction by using the weighting variable. The design weights were used throughout the manuscript. The sample characteristics are shown in Table 1.
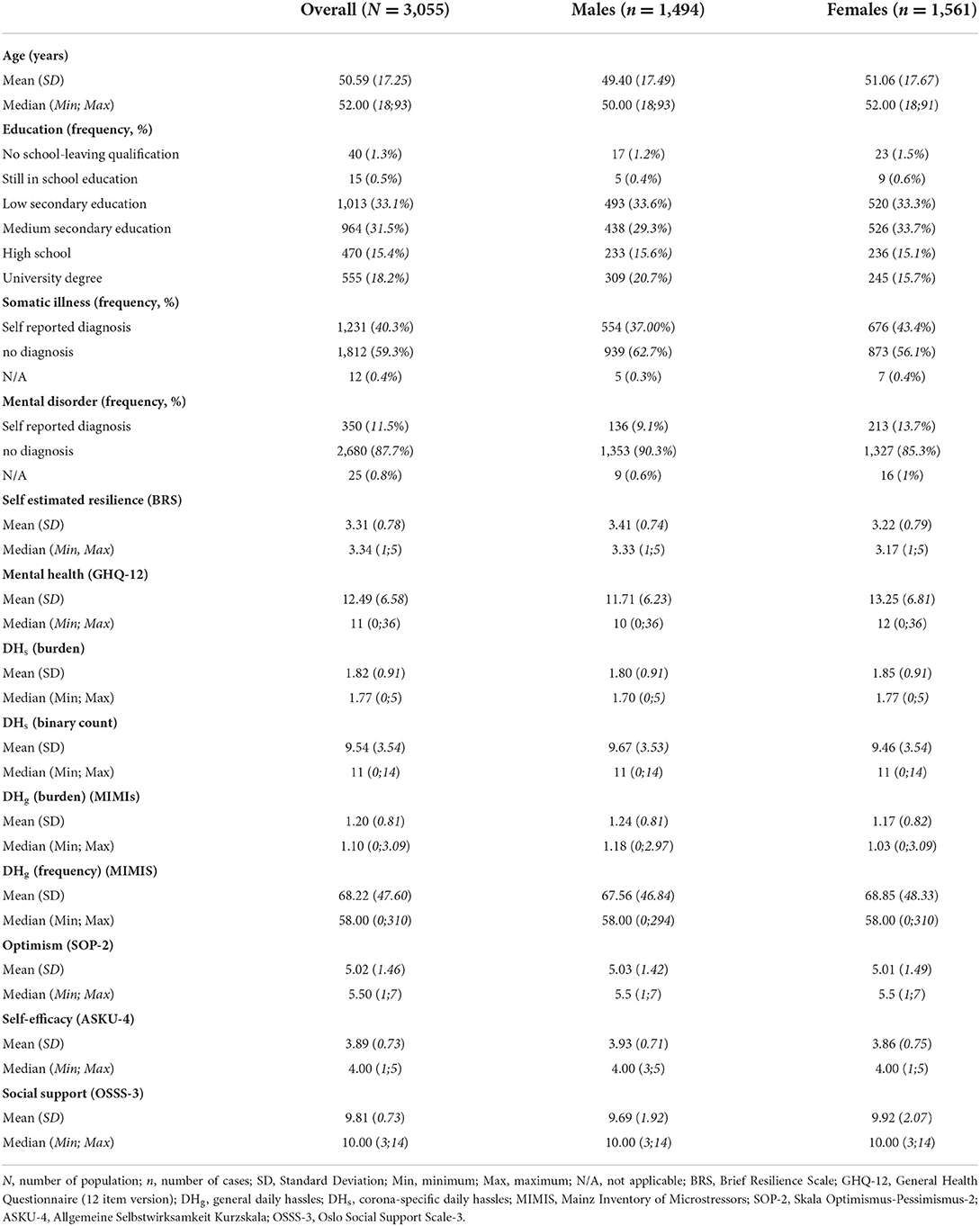
Table 1. Demographic characteristics of the sample.
The survey questionnaire contained 182 items and included the following sections: sociodemographics, mental health, resilience and resilience-associated constructs, stressor exposure as well as individual and social values. Except for the sociodemographic assessments, only validated questionnaires were used.
Sociodemographics were assessed using single items for, e.g., age, gender, or education as well as health behavior (in total 32 items). Based on the variables education, occupation and income, a socioeconomic status (SES) index was created using a predefined scoring system (42) and from there dividing participants into five equally populated groups (quintiles). This resulted in a classification into low (1st quintile), medium (2nd−4th quintile) and high (5th quintile) SES. Mental health was assessed by the General Health Questionnaire [GHQ-12, Goldberg et al. (43), 12 items on a 4-point Likert scale] for the last few weeks. Resilience, in the sense of the ability to easily recover from stress, was estimated by the Brief Resilience Scale [BRS, Chmitorz et al. (44); 6 items on a five-point Likert scale—“strongly disagree” to “strongly agree”].Total scores were obtained by taking the mean of the item scores. Due to restrictions of the questionnaire length, only four well established resilience-associated constructs (45–47) were included: optimism-pessimism [SOP-2; (48), 2 items; from “not optimistic/pessimistic at all” to “very optimistic/pessimistic” on a seven-point Likert scale], locus of control (LOC) [IE-4; (49), 4 items; from “does not apply at all” to “applies fully” on a five-point Likert scale], self-effiacy [ASKU; (50), 3 items; from “does not apply at all” to “applies fully” on a five-point Likert scale], and social support [OSSS-3; (51), 3 items; response format differs on a 4 resp. 5-point Likert scale].
For stressor exposure, we assessed three different types of stressors, general daily hassles (DHg), corona specific daily hassles (DHs) and life events (LE). For assessing DHg, we used the Mainz Inventory of Microstressors [MIMIS; (52); 58 items]. The MIMIS assessed the frequency each stressor occurs (up to the last 7 days, DHfg) as well as the perceived burden (from “not at all burdensome” to “very burdensome” on a five-point Likert scale, DHbg). DHs were measured with a selection of 13 items of the international survey DynaCORE (29), which had been introduced to assess stress due to the pandemic and respective measures (e.g., restriction to leave your home, loss of social contacts, less physical activity than usual). We asked whether a stressor occurred (on up to the last 7 days, total binary frequency, DHfs), and if so—how the burden was classified (from “not at all burdensome” to “very burdensome” on a five-point Likert scale, DHbs). For LE as macro stressors, we used a self-developed question that queried one LE within the last 12 months. The Response to Stressful Experiences Scale [RSES-4; (53), 4 items, “strongly disagree” to “strongly agree” on a five-point Likert scale] was used to determine the burden of it. Additionally, we used the Perceived Stress Scale [PSS-4; (54), 4 items “never” to “very often” on a five-point Likert scale] in order to assess the subjectively perceived stress. We also collected Social Identification with social groups [adapted from Doosje et al. (55), 4 items, “strongly disagree” to “strongly agree” on a five-point Likert scale], values [Individuelle reflexive Werte: (56); 16 items, “very unimportant” to “very important” on a seven-point Likert scale], political attitudes [Sozio-Politische Einstellungen, (57), 16 items, “correct” and “not correct”] and cultural diversity [Pro-diversity beliefs; adapted from Kauff and Wagner (58), 2 items, “not at all” to “full” on a four-point Likert scale]. The complete questionnaire is shown in Supplementary material 1. In this manuscript, we focus on the following outcomes and risk/protective factors: resilience (BRS), mental health (GHQ-12), stressor exposure (DHg, DHs) as well as risk (sociodemographic and health behavior) and protective factors (SOP-2, IE-4, ASKU, OSSS-3). Detailed results of the other items will be published elsewhere.
For all statistical analyses a significance level of α = 0.05, two-tailed, was adopted. All analyses were conducted with the weighting variable included. Data analysis was performed in R (v4.2.0, www.r-project.org/), in particular the packages ggplot2 (59), effects (60) and lavaan (all regressions were calculated with the scores of the confirmatory factor analysis) (61). All analyses are exploratory in nature; hence, p-values and 95% confidence bands are descriptive and not corrected for multiple comparisons.
To investigate the most frequent and most burdensome DH, descriptive methods (mean values and frequencies) were used. In addition, (weighted) heat maps—frequency of general DH (DHfg) and burden of corona-specific DH (DHbs)—were generated. A clustered heat map is a data visualization technique for showing patterns based on color intensities. To obtain information about which stressors (general vs. corona-specific) had a stronger impact on mental health, we calculated a regression analysis with either DHfg, DHfs or both combined (DHfc) as well as DHbg and DHbs or both combined (DHbc) (each modeled as a second-degree polynomial) as independent variable.
Following Kalisch et al. (62), resilience has been defined as a mental health outcome. However, since this study was a cross-sectional study which did not allow for a longitudinal assessment of mental health outcomes, we used the relationship of mental health (here the GHQ score) and stressor load (general daily hassles and corona-specific daily hassles) as a proxy for resilience. The GHQ-DH regression curve shows the normative predicted stressor reactivity (SR). Subjects residuals, which deviate from the normative predicted SR, contain information about their individuals SR (i.e., their vulnerability/resilience level): If the individual residual is located above this curve, it expresses a relative over-reactivity (=vulnerable), a value below the curve expresses a relative under-reactivity (=resilience) (29, 45, 62). We aimed to assess the stressor load as objectively as possible and therefore summed up the frequency of occurrence of each stressor as a total sum value: DHfg were counted continuously (Range: 0–406), DHfs were counted binarily (Range: 0–13). For the conceptualization of resilience, three different univariate regression analyses were applied considering the best model fit to get the subjects' stressor reactivity (SR) score: The GHQ score served in each calculation as criterion and either DHfg, DHfs or both combined (DHfc) as predictors. For convenience of interpretation, we calculated individuals' inverse residuals, so that high values indicate high resilience (63). The retrospectively assessed single, most burdensome life event didn't explain any variance in regression analysis, therefore, we omitted it from further analysis. The BRS, which measures the ability to recover from stress, is also frequently used as a resilience measure (44). It therefore served as a benchmark to compare the results of this study with those before and during the pandemic.
To identify risk factors, we used moderation analyses with the GHQ score as criterion and DHfg or DHfs as predictor. Sociodemographic characteristics (age, gender, education) and health status (physical illness or mental disorder) were used as moderators of this analysis. We controlled either for DHfg or DHfs. To identify protective factors, we also calculated the same moderation analyses, but with the different resilience factors (RF), i.e., optimism, self-efficacy, LOC and social support, as moderators. We controlled either for DHfg and DHfs and for age, gender, education, somatic illness, and mental disorder. To identify protective factors for the previously identified vulnerable groups, moderation analyses were calculated using SR score as the criterion and the RF as independent variables and the previously identified risk factors as moderators.
The final sample included 3,055 participants. Table 1 shows the demographic characteristics. Around half of the participants were women (51.1%). Age was distributed equally between18 and 93 years (median age = 52.00 years; mean age = 50.59 years; SD = 17.25 years). About one-third had either the low secondary education (33.5%) or medium secondary education (33.1%), and nearly one-sixth of participants had a university degree (18.2%) or high school (15.4%). Only 1.3% of the participants had no school-leaving qualification or were still in school (0.5%). About 40% of the respondents reported to be affected by any somatic disease, about 12% by a mental disorder. The proportion of women was higher in both groups (43% in females vs. 37% in males and 14% in females and 9% in males, respectively). The mean BRS score of respondents was 3.31 (SD = 0.78), with men's scores (mean = 3.41, SD = 0.74) indicating higher self-estimated resilience than women's (mean = 3.22, SD = 0.74). Similar results were found regarding GHQ (mean = 12.49; SD = 6.58; lower values indicate better mental health): mean values were higher in women (mean = 13.25; SD= 6.81) than in men (mean = 11.71; SD = 6.23). The values of frequency and burden of DH and the resilience-associated constructs (e.g., optimism) are shown in Table 1 (total and gender-separated).
Our first aim was to gain insights into the stressor load of the German population during the SARS-CoV-2 pandemic: The most frequent and most burdensome DHg and DHs were examined. The most frequently reported DHfg were housekeeping [reported by 83.64% of participants occurring on at least one and up to 7 day(s) in each case], followed by bad news in media (80.73%), negative political incident (72.42%), own physical complaints (65.95%), bad weather (71.15%), and sleeping problems (59.41%). Financial problems (average severity rating mean 2.31, possible answer range 1–4, percentage of those affected 28.5%), followed by sleeping problems (2.29; 51.30%), own physical complaints (2.13; 57.34%), and bad behavior of others and time pressure (both 2.10; 38.04% resp. 38.27%) were the most burdensome DHbg. Among the most frequently stated DHg, the average perceived burden was relatively low: housekeeping (1.23; 53.49%), negative political incident (1.71; 58.23%), and bad weather (1.61; 52.64%). To gain more knowledge about the temporal structure of the stressors, clustered heat maps for the DHfg are presented in Figure 2: It shows the overall mean and temporal frequency patterns of stressors (weighted, DHg), which were vertically sorted according to the cluster solution. By visual inspection of the dendrogram, seven distinct clusters can be identified regarding the temporal occurrence: In Cluster A it is characteristic that DHg tended to occur not at all or very often, i.e., on no or up to 7 days. In Cluster B DHfg occurred rather rarely (i.e., once, or twice or three times). This temporal clustering also unveils some contentual structure: Cluster A and B primarily contain problems with others or at work (e.g., “boring work” or “problems with an institution”). Cluster C primarily concerns insecurity (related to financial, health, or environmental status). This cluster was characterized by a low stressor load, i.e., DH did not occur just once. Cluster D includes external conditions (e.g., “delays” to “doctor visit”). In Cluster D stressors load is slightly elevated, by stressor occurrence on either 1–2 days or not at all. Cluster E includes “commuting” and has a clear peak at 5 days (every workday). Cluster F primarily indicates internal problems (e.g., “slander” or “careless mistake”) and the frequency of occurrence is highest for this cluster (on at least one or two up to 7 days). And Cluster G (“housekeeping”), has the highest frequency of occurrence on 7 days.
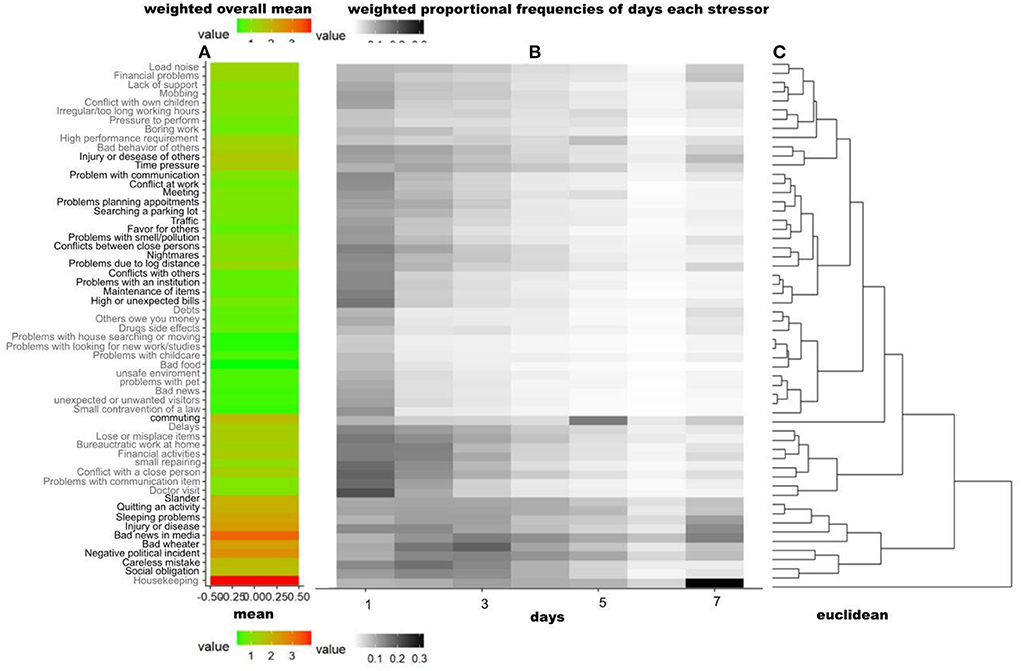
Figure 2. DHfg Heat Map, indicating the overall and temporal frequencies of stressors (weighted DHfg) vertically clustered by their temporal occurrence patterns. The figure consists of three parts: (A) showing the weighted overall mean of each item. (B) showing the weighted proportional frequencies of days each stressor was experienced–the darker the background, the more people experienced the stressor on the corresponding number of days (1–7): for example, “housekeeping” were experienced by many respondents on 7 days, “Doctor visit” was also reported to have been experienced once that week or some individuals reported “commuting” on 5 days. (C) Dendrogram indicating the difference between the items and their clusters of temporal patterns of relative frequencies. This cluster solution was also used to vertically sort the stressor items (using hierarchical clustering, euclidean distance and complete linkage). The proportional frequencies of each item (e.g., housekeeping 1 day: 10%, 2 days 13%, …, 7 days 30%) are successively merged into clusters. The fusion of different clusters is marked in the dendrogram by vertical lines. The heterogeneity within the clusters is plotted on the x-axis, it is growing with increasing cluster size. Longer horizontal lines indicate an increase in heterogeneity (of clusters) between the temporal occurrence patterns of the items: Cluster A includes 10 items (“loud noise” to “bad behavior of others”). Cluster B includes 17 items (“injury or disease of others” to “maintenance of items”). Cluster C includes 12 items (“Depts” to “small contravention of a law”). Cluster D includes 8 items (“Delays” to “Doctor visit”). Cluster E includes “commuting”. Cluster F includes 9 items (“slander” to “social obligation”), and Cluster G includes “housekeeping”.
The most frequently reported corona-specific DHfs were corona-media reports (reported by 96.60% of participants occurring on up to the last 7 days), followed by the loss of ability to participate in recreational activities or in important social events (93.29%), loss of social contacts (87.24%), less physical activity (83.84%), restrictions to leave home (81.87%), and economic damage (69.68%). The DHbs, sorted according to their degree of burden, are shown in the heat map of Figure 3. As shown in Figure 2A, which demonstrates the weighted overall mean of each stressor item, the most burdensome DHs were corona-media reports (average severity rating mean: 2.88, possible answer range: 1–5, percentage of those affected: 96.60%), followed by the loss of ability to participate in recreational activities or in important social events (“Loss of activity”: 2.80; 93.52%), private or professional travel not feasible (“No journey”: 2.53; 85.07%), loss of social contacts (“Loss of contacts”: 2.35; 87.36%), and less physical activity than usual (“Less physical activity”: 2.23; 84.08%). As shown in Figure 3B, which illustrates the weighted proportional load with which a particular stressor was experienced, corona-specific stressors were clustered into 3 clusters according to their relative degree of stress and sorted vertically (see right part C). It was frequently stated that Cluster A's items, e.g., “Restriction to leave home” or “Work/ childcare problems”, occurred, but most of participants did not associate burden with them. Cluster B includes “Other”, which included answers concerning additional problems (e.g., “Goods and services problems”), fears (e.g., second wave) and anger (e.g., ignoring measures/recklessness). Cluster C, e.g., “corona-media reports”, most often had a medium load (2).
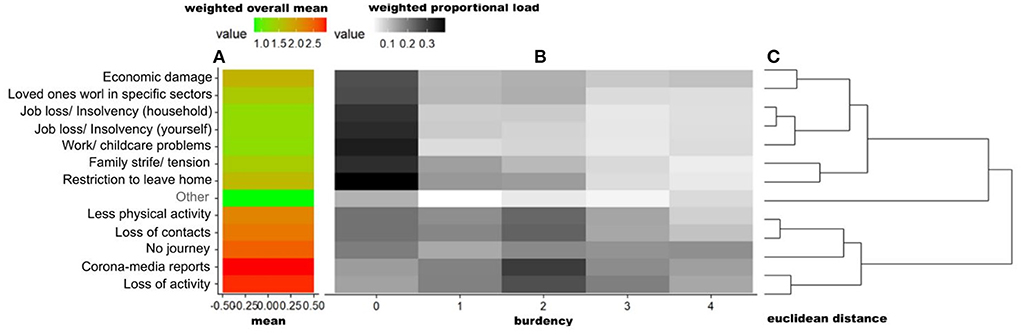
Figure 3. DHbs Heat Map, indicating the burden's mean of stressors (weighted DHbs) vertically clustered by their burden patterns. The figure consists of three parts: (A) showing the weighted overall mean of each item. (B) illustrates the weighted proportional load with which a particular stressor was experienced–the darker the background, the more burdensome the stressor was experienced (from “not at all burdensome” to “very burdensome” on a five-point Likert scale). For example, “media-corona reports” were experienced by many respondents as burdensome (average severity rating mean: 2.88). (C) Dendrogram indicating the difference between the items and their clusters of patterns of relative burden. This cluster solution was also used to vertically sort the stressor items (using hierarchical clustering, euclidean distance and complete linkage). The proportional burden of each item (e.g., loss of activity “not at all burdensome”: 13%, …, “very burdensome” 10%) are successively merged into clusters. The fusion of different clusters is marked in the dendrogram by vertical lines. The heterogeneity within the clusters is plotted on the x-axis, it is growing with increasing cluster size. Longer horizontal lines indicate an increase in heterogeneity (of clusters) between the temporal occurrence patterns of the items: Cluster A includes 7 items (“economic damage” to “restriction to leave home”). Cluster B includes “Other” with answers concerning additional problems (“Goods & services problems”, “Burden due to mandatory masks”, “Deterioration of mental situation” or “Digital study/school”), fears (“Second wave”, “economic impact/lockdown”, “Social change”, “Infection itself/others” and “Further measures”) and anger (“Ignoring measures/recklessness”, “Measures/policy” and “Media reporting”). Cluster C includes 5 items (“Less physical activity” to “loss of activities”).
In order to analyze the perceived stressor load, we used univariate regression models: 31 and 24% of the variance in mental health outcome (GHQ score, dependent variable) was explained by DHbg [R2 adjusted: 0.31; F2,3054) = 683.74, p < 0.001] and DHbs [R2 adjusted: 0.24; F2,3054) = 481.77, p < 0.001], respectively. DHbg and DHbs were modeled as second-degree polynomial considering best model fit. In the model with combined stressors (DHbc), DHbs explained only an additional 5% in the total perceived stressor load [determined by univariate regression with GHQ score as the dependent variable and DHbg and DHbs as the independent variables; adjusted R2 increase: 0.05–0.36, F4,3052) = 434.99, p < 0.001].
Our second goal was to estimate the SR, i.e., the stressor-mental health relationship (determined by univariate regression with GHQ score as the dependent variable and DHfg and DHfs as the independent variables). We found a curvilinear relationship due to a good model fit with DHfg and DHfs each modeled with a quadratic polynomial simultaneously (without controlling for LE, see Section Operationalization of stressor reactivity as a proxy for resilience). In the GHQ-DH regression, both predictors combined (DHfc) explained a substantial amount of variance of the GHQ score [adjusted R2 = 0.27; F4,3052) = 277.3, p < 2.2e-16]. Figures 4A,B show the normative predicted stressor-mental health models with GHQ score as dependent and DHfs or DHfg, respectively, as independent variables.
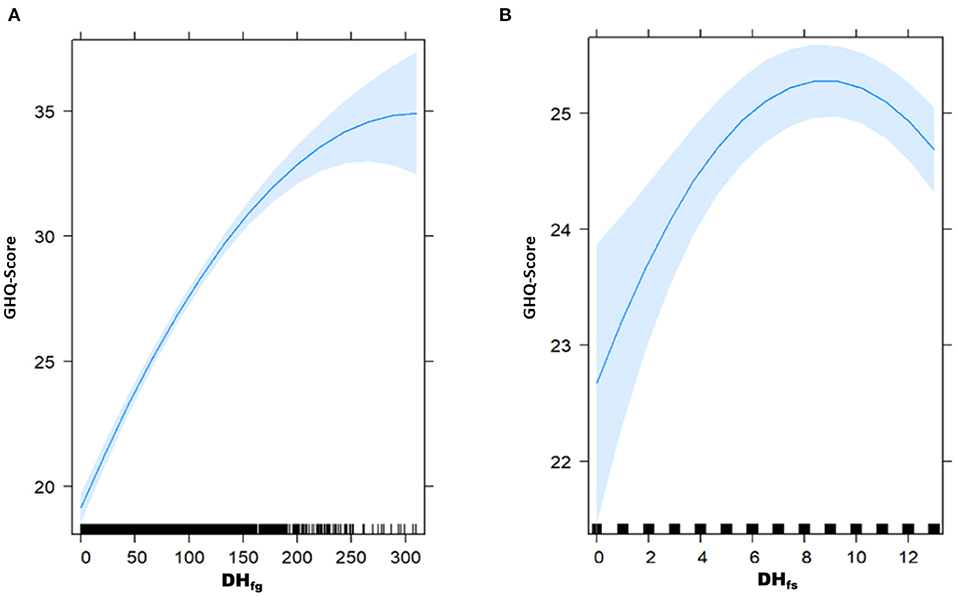
Figure 4. Predicted stressor-health relationship [multivariate regression analyses with GHQ score as criterion and DHfg (A) or DHfs (B) as predictors, respectively].
Regression analyses indicated that GHQ score is significantly related to DHfg (see Figure 4A). A peak was reached at about 250 DHfg, and then leveled off (ß1= 0.079; p < 2e-16; ß2= −0.0002; p < 4.94e-9). The higher the DH, the worse the mental health status until a specific saturation point (see Figure 4A). Regarding DHfs (see Figure 4B), regression analyses indicated that the GHQ score increased with increasing DHfs and then reached a peak at about 9 DHfs and flattened out. Statistically, only the main effect of the second polynomial in the GHQ- DHfs score relationship became significant (ß1= −0.04373; p = 0.261; ß2= −0.0337636; p = 0.0004). The relationship between DHfg and GHQ is considerably stronger than the relationship of DHfs with GHQ, as visible from comparing Figure 4A with Figure 4B.
Our third goal was to identify risk factors resp. vulnerable groups based on the different stressors (general or corona-specific). All results are presented in Table 2. To identify general vulnerable groups, we examined the effect of sociodemographic characteristics (e.g., age) or health status (e.g., physical illness) on the DHfg-health relationship (controlling for DHfs). Gender, age, and education level significantly influenced the relationship: female gender (p = 0.000) and higher age (p = 5.11e-6) were identified as general risk factors. Participants with higher educational attainment, i.e., high school (p = 0.002), and those with a university degree (p = 0.009) were less vulnerable compared to those with low secondary or medium secondary education (also see Supplementary Figure 5). Socioeconomic status and a diagnosed mental disorder or somatic illness did not significantly influence the DHfg-health relationship, i.e., they were not identified as general risk factors. To identify corona-specific vulnerable groups, we examined the moderating effect of sociodemographic characteristics and health status on the DHfs-health relationship (controlling for DHfg). Being diagnosed with a somatic illness significantly and negatively influenced the relationship (p = 0.037). Neither gender, age, SES, education level or a diagnosis of a mental disorder were identified as corona-specific risk factors.
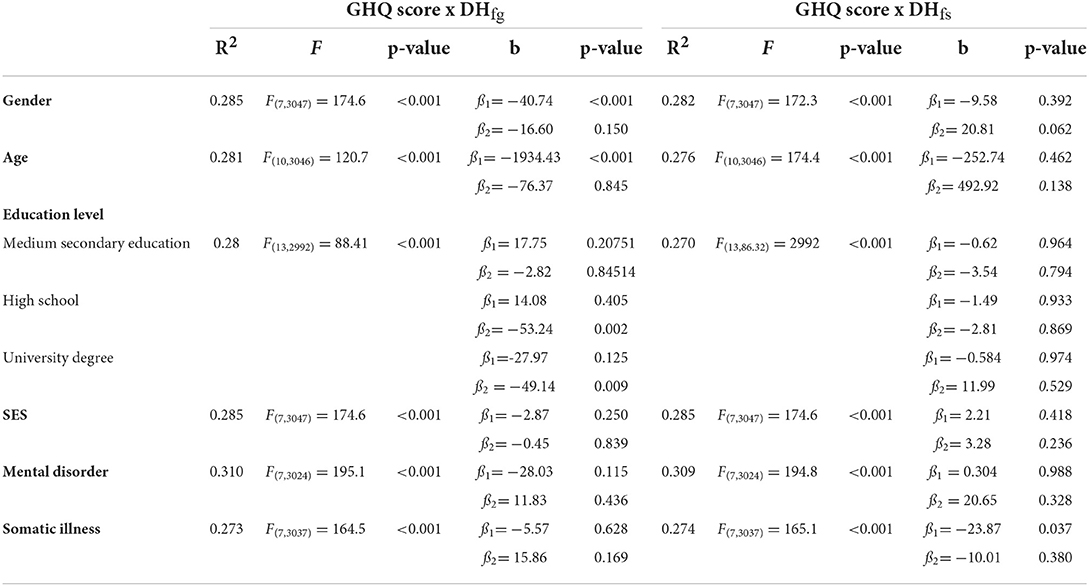
Table 2. Moderation analysis—vulnerable groups (controlling for DHfg or DHfs).
Our fourth objective was to identify protective factors based on the different stressors (general or corona specific). To identify general protective factors, we examined the effect of resilience factors (RF; e.g., optimism) on the DHfg-mental health relationship (controlling for DHfs, age, gender, education, somatic illness, and mental disorder). All results are presented in Table 3. We found that social support is a significant moderator of the DHfg-health relationship (p = 0.047). Neither self-efficacy, LOC, nor optimism were identified as protective factors. Regarding DHfs-health relationship, self-efficacy (p = 0.004) and LOC (p = 0.003) were significant moderators (reinforcing effect on the second polynomial negative relationship between DHfs and GHQ score). Optimism and social support were not identified as protective factors regarding coping with DHfs.

Table 3. Moderation analysis—protective factors (controlling for DHfs or DHfg, age, gender, education, somatic illness, and mental disorder).
Finally, moderation analyses were conducted to identify protective factors for the vulnerable groups previously identified. For the in-depth analysis, we examined the moderating effect of gender, age, education, and being diagnosed with a somatic illness on the relationship between RF (optimism, LOC, social support, and self-efficacy as independent variable) and the stressor reactivity score (SRc combined predictor of DHfg and DHfs). The results are presented in Table 4. They did not indicate any specific protective factor for the previously identified vulnerable groups (all analyses with p > 0.05). Rather, they showed that some protective factors lost their mitigating effect: Regarding female gender, the relationship between SRc and optimism, or LOC, or self-efficacy or social support was not moderated by female gender. Neither optimism nor social support could be identified as protective factors for higher age. The otherwise positive relationship between LOC or self-efficacy and SRc is even weakened by the moderating age effect (p2LOC = 0.007; p1self−efficacy = 0.0129; p2self−efficacy= 0.0001). The presence of somatic disease also weakened the otherwise positive effect of self-efficacy (p = 0.034) and social support (p = 0.046) on SRc. LOC and optimism were not identified as protective factors for those with a somatic illness. Neither optimism (p = 0.669), nor LOC (p = 0.193) or self-efficacy (p = 0.843) were identified as protective factors for lower educational attainment.
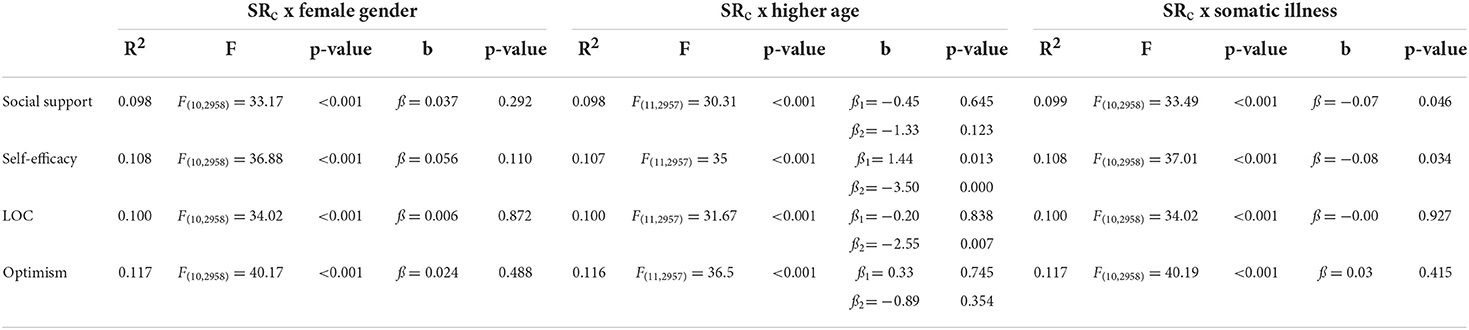
Table 4. Moderation analysis—in depth analysis (controlling for age, gender, education, somatic illness, and mental disorder, resp.).
The present study gained deeper insight into the mental health burden and its contributing general and corona-specific stressor load, potential risk and protective factors as well vulnerable groups during an early stage of the SARS-CoV-2 pandemic in a representative sample of the German adult population. At first, we analyzed the stressor load of the representative sample regarding frequency and burden. 83–60% were affected by the general DHfg such as housekeeping, bad news in media, negative political incident, own physical complaints or bad weather. Their average perceived burden, however, was relatively low (even almost not burdensome, ranging from 1.23 to 1.71). The most burdensome DHbg were sleeping problems and own physical complaints (affecting 51–57% of respondents), bad behavior of others and time pressure (38%), as well as financial problems (28%). Among corona-specific DHfs, almost all the responds (97–84%) were affected by media reports, loss of ability to participate in recreational activities or in important social events, not feasible private or professional travels, loss of social contacts, and less physical activity than usual. The perceived stressor burden had a high influence on mental health outcome (GHQ), i.e., higher occurrence of DH, resulted in higher mental burden. It explained about one-third of the variance: 36% by combined stressors, 31% by DHbg, and 24% by DHbs alone, respectively. In comparison, almost 10% less variance of mental health is explained, if instead of stressor burden, their frequency of occurrence (DHfg and DHfs) is used (R2 adjusted: 26.56). Our third and fourth goal were to identify general resp. corona-specific vulnerable groups and protective factors: female gender, higher age, and lower education level (low secondary or medium secondary education) were identified as general, somatic diseases as a corona-specific risk factor. Whereas self-efficacy and locus of control (LOC) proved to be corona-specific protective factors, social support was not: a high degree of social support attenuated mental health among high occurrence of DHfs. Further analysis did not indicate any specific protective factor for the previously identified vulnerable groups, they even showed that older age and being diagnosed with a somatic illness had a negative impact on RF, in the sense of attenuating the positive influence of LOC, self-efficacy, and social support on stressor reactivity (SR). In the following we will discuss the results in more detail.
An impact of the crisis on participants' mental health was evident since our sample showed a higher mean GHQ score (12.49, SD = 6.58) compared to pre-pandemic mean scores (mean = 9.70, SD = 4.94) measured in a representative German sample in 2012 (64), but also lower scores compared to the most intense phase of the lockdown in Europe (March 22 to April 19, 2020) (mean = 15.5, SD = 6.2) measured in Europe (29). This is in line with the observation that the impact of COVID-19 on mental health varied due to different time points of examination, different restrictions in different countries (6, 65), lockdown situations (66, 67) or during isolation in suspected COVID-19 cases (7, 19, 68). The German population was relatively less affected in an international comparison (i.e., less fear of job loss or financial losses due to government intervention) (29), but nevertheless showed elevated generalized or COVID-19-related anxiety symptoms as well as depressive symptoms (20, 69) and psychological distress compared with pre-pandemic data (34). Consistent with previous findings in a representative German sample (52) housekeeping, time pressure, and bad weather were also the most frequently occurring DHg in pre-pandemic times. However, in our sample, we observed a shift in attention to Corona-related issues, which was also identified from Veer et al. (29): while pre-pandemic bullying, problems with a pet and conflicts or disagreements with relatives were identified as the most distressing DHg (52), in our study negative political events (DHg) were also mentioned frequently. This is not only consistent with other findings during the pandemic in Germany (29), but also known to be a risk factor for mental burden (7, 20). The shift in attention to Corona-related issues could also be influenced by the use of fear-based media coverage implemented to prompt people to strictly adhere to the established guidelines (14, 15). A meta-analysis by Witte and Allen (70) showed that the dissemination of fear appeals, which are regularly used in other contexts (cf. deterrent images of a black lung in smoking prevention), can lead to behavioral changes when the concerned person feels able to deal with the threat. A lack of expectation to be able to deal with it, however, can lead to defensive reactions (e.g., questioning the meaningfulness of the measures). A paradoxical societal effect regarding the fear-based media coverage would be possible: The more mentally burdened the population, the lower the expectation of self-efficacy in dealing with the threat and therefore compliance with individual health-protective behaviors decreases (34). This might result in higher infection rates and, as a consequence, in even more fear-based appeals (71). The occurrence frequency of Corona-related stressors (e.g., corona media reports or negative political events) was particularly notable in our study (80.73 and 72.42%, respectively). At the same time, no excessive burden to Corona-related stressors was found in our study. One explanation could be the decrease in reports of deaths, as the mortality rate was often perceived as particularly threatening (72). At the time of our survey in Germany the mortality rate was just under 5% (40, 73). Nevertheless, worldwide corona reports were mostly negative (74) and therefore affected behavior (e.g., social distancing, lower willingness to be vaccinated) and emotions (e.g., loneliness) (72). The associated aversive emotions may also have led to psychological defense mechanisms: As a link between psychological distress and higher media consumption times has also been demonstrated during the pandemic (74, 75), experts recommend curbing media consumption so that negative news are not permanently consumed (76). Compared with the findings of Veer et al. (29), who cited serious consequences (such as death or hospitalization of a loved one and concern about one's infection) as the primary corona stressor, concerns in our study shifted toward financial, health-related (e.g., sleep problems, injury or illness, less physical activity than usual, corona reporting), and leisure problems (non-participation in social events, fewer social contacts, neither personal nor professional travel) during the phase investigated in this study.
The mean scores of self-estimated resilience of our respondents (BRS: mean = 3.31; SD = 0.78) was similar to pre-pandemic data [mean = 3.35; SD = 0.95, for a study with N = 1,128 respondents in Germany (77)], but marginally lower as compared to other results obtained during the pandemic [April 2020, mean = 3.41; SD = 0.49, German sample sizes: 1.012 (3)]. However, these resilience scores are self-estimates of probands who are asked to describe how quickly they bounce back from stressful events, but no “real life” measures how their mental health relates to the number and burden of stressful experiences. We therefore calculated the SR score as a proxy for resilience as current psychological responsiveness (as measured by the GHQ) to daily stressors [as measured by MIMIS and/or a DynaCORE item selection (29)]. In our cross-sectional data, we observed a concave DHfg-health relationship (see Figure 4): The leveling of the mental health-stressor relationship, i.e., that it flattens out from a certain number of daily hassles, shows that in our sample from around 250 DHfg onward, further stressors have a less severely deteriorating effect on mental health. This could carefully be interpreted as a possible adaptation process to stressors (78). Our finding that corona-specific stressors frequently occurred, but were not perceived as burdensome by a large majority, may also be interpreted as hint for a possible adaptation process. Manchia et al. (33) showed that, after the restrictions were lifted, a large portion of the population recovered from the pandemic related stressor impact. This could be attributable to the corona-induced slowdown (79), but also to a successful adaption process described as “psychological gain from adversity” as suggested by Ahrens et al. (80). The sole occurrence of corona-specific stressors had little impact on mental health (corona-specific stress items clarified only 5% of the variance of the GHQ score additionally and non-significant effect in the regression; first polynomial, i.e., no decreasing GHQ score with increasing DHfs), which implies that DHg had more impact on the mental health than DHs. Counterintuitive our results also show with a higher incidence of corona-specific DH less mental burden (significant effect in the second polynomial). This might be a result of the summed binary operationalization of corona-specific DHfs (left skewed distribution), i.e., just under half of the respondents reported an occurrence corresponding to data point 13 (see Figure 4B) of the DHfs, leading to an underrepresentation of data points to the left of it.
The combined stressors (general and corona-specific) explained more variance of the GHQ score than the predictors separately. Furthermore, the perceived stressor burden is a better predictor (36%) than the frequency of its occurrence (26%), which is in line with other findings (29, 81) as well as with the Transactional Model of Stress and Coping (28), highlighting that the stress reaction depends on the specific appraisal of the stressor (i.e., as harm/loss, threats, and challenge) in relation to the resources available.
In line with other findings (2, 3, 9, 11, 19–23), women were identified as particularly vulnerable to psychological stress during the pandemic. Women's BRS (mean = 3.22, SD = 0.74) and GHQ scores (mean = 13.25; SD = 6.81) in our sample showed lower resilience and mental health, respectively, than men's BRS score (mean = 3.41, SD = 0.74) or GHQ score (mean = 11.71; SD = 6.23), which is consistent with other findings during the pandemic (8, 80). When considering the impact of general or corona-specific stressors on mental health, female gender was found to be a general risk factor. This may indicate that it is not a corona-specific vulnerability, e.g., because of domestic childcare, as has been cited in previous research (7, 33, 82). We also found lower education level (low and medium secondary education level) as risk factor: the GHQ score for the lower education groups continues to increase with more occurrence of DHfg. However, this result is based on comparatively few data points, i.e., few respondents had more than 250 DHfg (shown by the dashes on the x-axis in Supplementary Figure 5), so it should be interpreted with caution. At the same time, this result is consistent with other studies (8, 17, 83).
In many studies, younger age groups ( ≤ 40 years) are highlighted as particularly vulnerable during crisis: Older people are suggested to be protected through life experiences, thus more problem-solving skills and a stronger locus of control, and ultimately a more efficient psychological coping and adaptive capacity during COVID-19 (2, 7, 22, 30). In our study, this finding could not be replicated, which may be due to our use of SR as a proxy of resilience (predicting mental health as a function of stress). Furthermore, although older people tend to be exposed to fewer stressors (19, 36, 84), they might be likely to be more responsive to them. We identified a diagnosed somatic disease as a risk factor for corona-specific stressors. Somatic diseases are a well-researched risk factor for mental health (7, 9, 17) and the risk for somatic diseases and infections grows with increasing age (31). As Taquet et al. (68) showed in a retrospective US cohort study in August 2020, there is also a bidirectional association between SARS-CoV-2 infection and risk of mental disorder and vice versa. Regarding resilience factors as protective factors for mental burden, self-efficacy and LOC were found to be corona-specific protective factors, which is consistent with earlier findings (7, 30, 33). However, contrary to our expectations (2, 3, 29, 69), optimism and social support were not found to be protective factors in our study. Individuals reporting high levels of social support were even more affected by stressors on GHQ. This implies that this resilience factor loses its effect in times of social distancing. This would at least be supported by the study results that reported increased loneliness (6, 85). We could not demonstrate a specific protective factor for the previously identified vulnerable groups, i.e., females, older age, and lower education level. In contrast, the elderly and the somatically ill showed lower RF scores, which otherwise has a positive effect on resilience (LOC, self-efficacy, and social support) (24, 25). This could be seen in the context of the findings of Fritz et al. (27) on the interaction of different protective factors: Protective factors influence each other (intensification or inhibition), and network connectivity between protective factors is less responsive in vulnerable people, making already vulnerable groups even more vulnerable to stress. This may explain why vulnerable groups, e.g., elderly, or somatic ill, but also known from other findings have shown to be more vulnerable to the adversities of the pandemic (8, 68, 86).
Our data provide insights in especially vulnerable groups (women, older age, and lower education level) and specific starting points in order to strengthen protective factors, by identifying self-efficacy and LOC as protective factors during the pandemic. However, since we only researched a limited number of resilience factors, there are certainly other protective factors which we did not study here but which might be important to fostering mental health (e.g., certain coping styles). In other peri-pandemic analyses, for example, positive appraisal style (29, 80) was identified as a protective factor.
The strengths of the study are the large and representative sample, the use of well-established standardized measures that allow comparisons with other pre- as well as pandemic populations. We also not only relied on self-estimated resilience capability of the probands, but used the SR score (62) to describe a proxy for resilience which relates mental burden to the perceived stressor load. The study is also new as it disentangles the relative contributions of general and corona-specific DH to mental burden and resilience.
On the other hand, our study has the following limitations: First, we collected the representative data in an online survey, so we cannot exclude selection bias. In addition, we did not collect longitudinal data, which are considered the gold standard (52, 62). Furthermore, changes in mental health were assessed retrospectively over the past 2 weeks, which might have led to memory bias. In addition, the survey was conducted during a less severe phase of the pandemic, meaning that some of the restrictions (e.g., social distancing, closing of restaurants, closing of recreational and cultural facilities) had already been lifted. Although the corona pandemic caused measurable burden, it is likely that at a different time point during the course of the pandemic, corona-specific stress would have been more pronounced. Due to a reasonable questionnaire length, we had to severely limit the constructs we examined, which is why we only queried a selection of the RF and only examined a selection of corona-specific stressors. The last made the comparison to the general stressors more difficult. To the extent that resilience was operationalized as an outcome (stressor exposure relative to mental health), survey inaccuracies may have crept in: It cannot be ruled out that mental health problems have their genesis in other stressors or LE that were not surveyed in this instrument.
The corona pandemic seems to have an impact on the general population in the sense that corona-specific stressors were perceived but not as burdensome during this phase of the pandemic (e.g., general stressors such as bad news in the media or own physical complaints). At the same time, the corona-specific stressor load was hardly perceived as a burden: This is also reflected in the low impact on mental health. This result should be viewed in the context of the data collection period, for which some restrictions had already been lifted and may have led to adaption. As in many other studies, we were also able to show that there are vulnerable groups (women, lower education level, older age, and somatic illness), who are at a higher risk of being negatively affected by the pandemic. In addition, specific protective factors (self-efficacy and LOC) for the corona-specific stressors were identified in our study. Extending previous studies, we were also able to show that older people and people with somatic illnesses are particularly affected by corona-specific stressors, which again underlines their need for special support regarding an adaptive coping during and after the pandemic.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Department of Psychology and Sports Science of the Johann-Wolfgang-Goethe University Frankfurt (Prof. Andreas Klein). The patients/participants provided their written informed consent to participate in this study.
LH, IH, DG, and SF: conceptualization, methodology, and validation. GK: statistical analysis and data visualization. LH: investigation and writing of the original draft. KL and RD: project management, monitoring, and validation. IH, DG, and KL: writing—revised draft, monitoring, and validation. All authors contributed to the article and approved the submitted version.
This work was supported by the Leibniz-Gemeinschaft (Grant number: K83/2017 Resilience Factors in a Diachronic and Intercultural Perspective) to KL and a research grant from the Johannes Gutenberg University Mainz Top-level Research Area 40,000 Years of Human Challenges: Perception, Conceptualization and Coping in Premodern Societies funded by Research-Initiative Rhineland-Palatinate (2019–2023), coordinated by A. Busch and H. Frielinghaus, to KL and RD.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.991292/full#supplementary-material
1. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. General Psychiatry. (2020) 33:e100213. doi: 10.1136/gpsych-2020-100213
2. Riepenhausen A, Veer IM, Wackerhagen C, Reppmann ZC, Köber G, Ayuso-Mateos JL, et al. Coping with COVID: risk and resilience factors for mental health in a German representative panel study. Psychol Med. (2022) 1–11. doi: 10.1017/S0033291722000563
3. Gilan D, Röthke N, Blessin M, Kunzler A, Stoffers-Winterling J, Müssig M, et al. Psychomorbidity, resilience, and exacerbating and protective factors during the SARS-CoV-2 pandemic: a systematic literature review and results from the German COSMO-PANEL. Deutsches Aerzteblatt International. (2020) 117:625–630. doi: 10.3238/arztebl.2020.0625
4. Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surg. (2020) 78:185–93. doi: 10.1016/j.ijsu.2020.04.018
5. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. (2020) 288:112954. doi: 10.1016/j.psychres.2020.112954
6. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
7. Xiong J, Lipsitz O, Nasri F, Lui LM, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. (2020) 277:55–64. doi: 10.1016/j.jad.2020.08.001
8. Kunzler AM, Röthke N, Günthner L, Stoffers-Winterling J, Tüscher O, Coenen M, et al. Mental burden and its risk and protective factors during the early phase of the SARS-CoV-2 pandemic: systematic review and meta-analyses. Global Health. (2021) 17:1–29. doi: 10.1186/s12992-021-00670-y
9. Pérez-Gómez HR, González-Díaz E, Herrero M, de Santos-Ávila F, Vázquez-Castellanos JL, Juárez-Rodríguez P, et al. The Moderating Effect of Resilience on Mental Health Deterioration among COVID-19 Survivors in a Mexican Sample. In: Paper Presented at the Healthcare (2022).
10. Dawel A, Shou Y, Smithson M, Cherbuin N, Banfield M, Calear AL, et al. The effect of COVID-19 on mental health and wellbeing in a representative sample of Australian adults. Front Psychiatry. (2020) 11:579985. doi: 10.3389/fpsyt.2020.579985
11. Peters A, Rospleszcz S, Greiser KH, Dallavalle M, Berger K. The impact of the COVID-19 pandemic on self-reported health: early evidence from the German National Cohort. Deutsches Ärzteblatt International. (2020) 117:861. doi: 10.3238/arztebl.2020.0861
12. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
13. Fardin MA. COVID-19 and anxiety: a review of psychological impacts of infectious disease outbreaks. Archives of clinical infectious diseases, 15(COVID-19) (2020).
14. Bavel JJV, Baicker K, Boggio PS, Capraro V, Cichocka A, Cikara M, et al. Using social and behavioural science to support COVID-19 pandemic response. Nat Hum Behav. (2020) 4:460–71. doi: 10.1038/s41562-020-0884-z
15. Gvozden M, Stamenković A, Mitrović A, Draginić K, Miličić T, ŽeŽelj I. Content analysis of newspaper headlines related to the coronavirus epidemic in the period before and after the 2020 parliamentary elections in Serbia. Empirical Stud Psychol. (2021) 2021, 87.
16. Rubin GJ, Wessely S. The psychological effects of quarantining a city. BMJ. (2020) 368:m313. doi: 10.1136/bmj.m313
17. Mazza C, Ricci E, Biondi S, Colasanti M, Ferracuti S, Napoli C, et al. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: immediate psychological responses and associated factors. Int J Environ Res Public Health. (2020) 17:3165. doi: 10.3390/ijerph17093165
18. Cao W, Fang Z, Hou G, Han M, Xu X, Dong J, et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. (2020) 287:112934. doi: 10.1016/j.psychres.2020.112934
19. Alodhayani AA, Almutairi KM, Alshobaili FA, Alotaibi AF, Alkhaldi G, Vinluan JM, et al. Predictors of mental health status among quarantined COVID-19 patients in Saudi Arabia. Healthcare. (2021) 9:1271. doi: 10.3390/healthcare9101271
20. Bäuerle A, Teufel M, Musche V, Weismüller B, Kohler H, Hetkamp M, et al. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: a cross-sectional study in Germany. J Public Health. (2020) 42:672–8. doi: 10.1093/pubmed/fdaa106
21. Beames JR, Li SH, Newby JM, Maston K, Christensen H, Werner-Seidler A. The Upside: Coping and Psychological Resilience in Australian Adolescents During the COVID-19 Pandemic (2021).
22. Meda-Lara RM, Muñoz-Valle JF, Juárez-Rodríguez P, Figueroa-López C, Herrero M, de Santos Ávila F, et al. Psychological responses to COVID-19 in a Mexican population: an exploratory study during second and third phases. Psychol Health Med. (2022) 27:257–64. doi: 10.1080/13548506.2021.1883689
23. Zamarripa J, Delgado-Herrada M, Morquecho-Sánchez R, Baños R, de la Cruz-Ortega M, Duarte-Félix H. Adaptability to social distancing due to COVID-19 and its moderating effect on stress by gender. Salud Mental. (2021) 43:273–8. doi: 10.17711/SM.0185-3325.2020.037
24. Mancini AD, Bonanno GA. Predictors and parameters of resilience to loss: toward an individual differences model. J Pers. (2009) 77:1805–32. doi: 10.1111/j.1467-6494.2009.00601.x
25. Sapienza JK, Masten AS. Understanding and promoting resilience in children and youth. Curr Opin Psychiatry. (2011) 24:267–73. doi: 10.1097/YCO.0b013e32834776a8
26. Almeida DM. Resilience and vulnerability to daily stressors assessed via diary methods. Curr Dir Psychol Sci. (2005) 14:64–8. doi: 10.1111/j.0963-7214.2005.00336.x
27. Fritz J, Fried EI, Goodyer IM, Wilkinson PO, Van Harmelen A-L. A network model of resilience factors for adolescents with and without exposure to childhood adversity. Sci Rep. (2018) 8:1–13. doi: 10.1038/s41598-018-34130-2
28. Lazarus RS, Folkman S. Stress, Appraisal, and Coping. New York, NY: Springer Publishing Company (1984).
29. Veer IM, Riepenhausen A, Zerban M, Wackerhagen C, Puhlmann LM, Engen H, et al. Psycho-social factors associated with mental resilience in the Corona lockdown. Transl Psychiatry. (2021) 11:1–11. doi: 10.1038/s41398-020-01150-4
30. Ayalon L, Chasteen A, Diehl M, Levy BR, Neupert SD, Rothermund K, et al. Aging in times of the COVID-19 pandemic: avoiding ageism and fostering intergenerational solidarity. J Gerontol Series B. (2021) 76:e49–52. doi: 10.1093/geronb/gbaa051
31. Fuller HR, Huseth-Zosel A. Lessons in resilience: initial coping among older adults during the COVID-19 pandemic. Gerontologist. (2021) 61:114–25. doi: 10.1093/geront/gnaa170
32. Dawson DL, Golijani-Moghaddam N. COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. J Context Behav Sci. (2020) 17:126–34. doi: 10.1016/j.jcbs.2020.07.010
33. Manchia M, Gathier AW, Yapici-Eser H, Schmidt MV, de Quervain D, van Amelsvoort T, et al. The impact of the prolonged COVID-19 pandemic on stress resilience and mental health: a critical review across waves. Eur Neuropsychopharmacol. (2022) 55:22–83. doi: 10.1016/j.euroneuro.2021.10.864
34. Gilan D, Müssig M, Hahad O, Kunzler AM, Samstag S, Röthke N, et al. Protective and risk factors for mental distress and its impact on health-protective behaviors during the SARS-CoV-2 pandemic between March 2020 and March 2021 in Germany. Int J Environ Res Public Health. (2021) 18:9167. doi: 10.3390/ijerph18179167
35. D'Angelo B, Wierzbicki M. Relations of daily hassles with both anxious and depressed mood in students. Psychol Rep. (2003) 92:416–8. doi: 10.2466/pr0.2003.92.2.416
36. Stawski RS, Sliwinski MJ, Almeida DM, Smyth JM. Reported exposure and emotional reactivity to daily stressors: the roles of adult age and global perceived stress. Psychol Aging. (2008) 23:52. doi: 10.1037/0882-7974.23.1.52
37. Kanner AD, Coyne JC, Schaefer C, Lazarus RS. Comparison of two modes of stress measurement: daily hassles and uplifts versus major life events. J Behav Med. (1981) 4:1–39. doi: 10.1007/BF00844845
38. Serido J, Almeida DM, Wethington E. Chronic stressors and daily hassles: unique and interactive relationships with psychological distress. J Health Soc Behav. (2004) 45:17–33. doi: 10.1177/002214650404500102
39. Seery MD, Holman EA, Silver RC. Whatever does not kill us: cumulative lifetime adversity, vulnerability, and resilience. J Pers Soc Psychol. (2010) 99:1025. doi: 10.1037/a0021344
40. Robert Koch Institut,. Täglicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19). 01.04.2020 – AKTUALISIERTER STAND FÜR DEUTSCHLAND (2020). Available online at: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-04-01-de.pdf?__blob=publicationFile (accessed May 19, 2022).
41. Die Bundesregierung,. 17. Juni 2020: Gemeinsame Maßnahmen zum Corona-Virus. (2020). Available online at: https://www.bundesregierung.de/breg-de/leichte-sprache/17-juni-2020-gemeinsame-massnahmen-zum-corona-virus-1762788 (accessed May 19, 2022).
42. Lampert T, Kroll LE, Müters S, Stolzenberg H. Messung des sozioökonomischen Status in der Studie “Gesundheit in Deutschland aktuell” (GEDA), Vol. 56. Bundesgesundheitsblatt: Springer (2013). p. 131–143.
43. Goldberg DP, Gater R, Sartorius N, Ustun TB, Piccinelli M, Gureje O, et al. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol Med. (1997) 27:191–7. doi: 10.1017/S0033291796004242
44. Chmitorz A, Wenzel M, Stieglitz R, Kunzler A, Bagusat C, Helmreich I, et al. Population-based validation of a German version of the Brief Resilience Scale. PLoS ONE. (2018) 13:e0192761. doi: 10.1371/journal.pone.0192761
45. Chmitorz A, Kunzler A, Helmreich I, Tüscher O, Kalisch R, Kubiak T, et al. Intervention studies to foster resilience–A systematic review and proposal for a resilience framework in future intervention studies. Clin Psychol Rev. (2018) 59:78–100. doi: 10.1016/j.cpr.2017.11.002
46. Chmitorz A, Neumann RJ, Kollmann B, Ahrens KF, Öhlschläger S, Goldbach N, et al. Longitudinal determination of resilience in humans to identify mechanisms of resilience to modern-life stressors: the longitudinal resilience assessment (LORA) study. Eur Arch Psychiatry Clin Neurosci. (2021) 271:1035–51. doi: 10.1007/s00406-020-01159-2
47. Helmreich I, Kunzler A, Chmitorz A, König J, Binder H, Wessa M, et al. Psychological interventions for resilience enhancement in adults (Protocol). Cochrane Database Syst Rev. (2017) 2:CD012527. doi: 10.1002/14651858.CD012527
48. Kemper CJ, Beierlein C, Kovaleva A, Rammstedt B. Eine Kurzskala zur Messung von Optimismus-Pessimismus: GESIS Working Paper 15 (2012). Mannheim: GESIS - Leibniz-Institut für Sozialwissenschaften (2012). Available online at: https://nbn-resolving.org/urn:nbn:de:0168-ssoar-288585
49. Kovaleva A, Beierlein C, Kemper C, Rammstedt B. Eine Vier-Item-Skala zur Erfassung von internaler und externaler Kontrollüberzeugung (IE-4). GESIS. (2012).
50. Beierlein C, Kovaleva A, Kemper CJ, Rammstedt B. ASKU-Allgemeine Selbstwirksamkeit Kurzskala. Trier: ZPID (2012). doi: 10.23668/psycharchives.4527
51. Kocalevent R-D, Berg L, Beutel ME, Hinz A, Zenger M, Härter M, et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC Psychol. (2018) 6:1–8. doi: 10.1186/s40359-018-0249-9
52. Chmitorz A, Kurth K, Mey L, Wenzel M, Lieb K, Tüscher O, et al. Assessment of microstressors in adults: questionnaire development and ecological validation of the mainz inventory of microstressors. JMIR Mental Health. (2020) 7:e14566. doi: 10.2196/14566
53. Ponder WN, Prosek EA, Sherrill T. Validation of the adapted response to stressful experiences scale (RSES-4) among first responders. Professional Counselor. (2021) 11:300–12. doi: 10.15241/wnp.11.3.300
54. Cohen S, Kamarck T, Mermelstein R. Perceived stress scale (PSS). J Health Soc Beh. (1983) 24:285. doi: 10.1037/t02889-000
55. Doosje B, Ellemers N, Spears R. Perceived intragroup variability as a function of group status and identification. J Exp Soc Psychol. (1995) 31:410–36. doi: 10.1006/jesp.1995.1018
58. Kauff M, Wagner U. Valuable therefore not threatening: the influence of diversity beliefs on discrimination against immigrants. Soc Psychol Personal Sci. (2012) 3:714–21. doi: 10.1177/1948550611435942
60. Fox J, Weisberg S. An R Companion to Applied Regression. Thousand Oaks, CA: Sage publications (2018).
61. Rosseel Y. lavaan: An R package for structural equation modeling. J Stat Softw. (2012) 48:1–36. doi: 10.18637/jss.v048.i02
62. Kalisch R, Baker DG, Basten U, Boks MP, Bonanno GA, Brummelman E, et al. The resilience framework as a strategy to combat stress-related disorders. Nat Hum Behav. (2017) 1:784–90. doi: 10.1038/s41562-017-0200-8
63. Amstadter AB, Myers JM, Kendler KS. Psychiatric resilience: longitudinal twin study. Br J Psychiatry. (2014) 205:275–80. doi: 10.1192/bjp.bp.113.130906
64. Romppel M, Hinz A, Finck C, Young J, Brähler E, Glaesmer H. Cross-cultural measurement invariance of the General Health Questionnaire-12 in a German and a Colombian population sample. Int J Methods Psychiatr Res. (2017) 26:e1532. doi: 10.1002/mpr.1532
65. Fisher J, Tran T, Hammarberg K, Nguyen H, Stocker R, Rowe H, et al. Quantifying the mental health burden of the most severe covid-19 restrictions: a natural experiment. J Affect Disord. (2021) 293:406–14. doi: 10.1016/j.jad.2021.06.060
66. Prati G, Mancini AD. The psychological impact of COVID-19 pandemic lockdowns: a review and meta-analysis of longitudinal studies and natural experiments. Psychol Med. (2021) 51:201–11. doi: 10.1017/S0033291721000015
67. Vindegaard N, Benros ME. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav Immun. (2020) 89:531–42. doi: 10.1016/j.bbi.2020.05.048
68. Taquet M, Luciano S, Geddes JR, Harrison PJ. Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry. (2021) 8:130–40. doi: 10.1016/S2215-0366(20)30462-4
69. Petzold MB, Bendau A, Plag J, Pyrkosch L, Mascarell Maricic L, Betzler F, et al. Risk, resilience, psychological distress, and anxiety at the beginning of the COVID-19 pandemic in Germany. Brain Behav. (2020) 10:e01745. doi: 10.1002/brb3.1745
70. Witte K, Allen M. A meta-analysis of fear appeals: implications for effective public health campaigns. Health Educ Behav. (2000) 27:591–615. doi: 10.1177/109019810002700506
71. Stolow JA, Moses LM, Lederer AM, Carter R. How fear appeal approaches in COVID-19 health communication may be harming the global community. Health Educ Behav. (2020) 47:531–5. doi: 10.1177/1090198120935073
72. Giroux M, Park J, Kim J-E, Choi YK, Lee JC, Kim S, et al. The impact of communication information on the perceived threat of COVID-19 and stockpiling intention. Aust Mark J. (2021) 7:18393349211028670. doi: 10.1177/18393349211028670
73. Robert Koch Institut,. Täglicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19). 01.07.2020 – AKTUALISIERTER STAND FÜR DEUTSCHLAND (2020). Available online at: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-07-01-de.pdf?__blob=publicationFile (accessed May 19, 2022).
74. Bagus P, Peña-Ramos JA, Sánchez-Bayón A. COVID-19 and the political economy of mass hysteria. Int J Environ Res Public Health. (2021) 18:1376. doi: 10.3390/ijerph18041376
75. Riehm KE, Holingue C, Kalb LG, Bennett D, Kapteyn A, Jiang Q, et al. Associations between media exposure and mental distress among US adults at the beginning of the COVID-19 pandemic. Am J Prev Med. (2020) 59:630–8. doi: 10.1016/j.amepre.2020.06.008
76. World Health Organization. Mental Health and Psychosocial Considerations During the COVID-19 Outbreak. (2020). Available online at: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf?sfvrsn=6d3578af_10 (accessed September 20, 2022).
77. Kunzler AM, Chmitorz A, Bagusat C, Kaluza AJ, Hoffmann I, Schäfer M, et al. Construct validity and population-based norms of the German brief resilience scale (BRS). Eur J Health Psychol. (2018) 25:107–117. doi: 10.1027/2512-8442/a000016
78. Seery MD. Resilience: a silver lining to experiencing adverse life events? Curr Dir Psychol Sci. (2011) 20:390–4. doi: 10.1177/0963721411424740
79. Zhang Y, Ma ZF. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning Province, China: a cross-sectional study. Int J Environ Res Public Health. (2020) 17:2381. doi: 10.3390/ijerph17072381
80. Ahrens KF, Neumann RJ, Kollmann B, Brokelmann J, Werthern V, MalyshauWeichert D, et al. Impact of COVID-19 lockdown on mental health in Germany: longitudinal observation of different mental health trajectories and protective factors. Transl Psychiatry. (2021) 11:10. doi: 10.1038/s41398-021-01508-2
81. Kalisch R, Köber G, Binder H, Ahrens KF, Basten U, Chmitorz A, et al. A Generic Solution for the Operationalization and Measurement of Resilience and Resilience Processes in Longitudinal Observations: Rationale and Basic Design of the MARP and LORA Studies (2020). PsyArXiv. doi: 10.31234/osf.io/jg238
82. Shevlin M, McBride O, Murphy J, Miller JG, Hartman TK, Levita L, et al. Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open. (2020) 6:e125. doi: 10.1192/bjo.2020.109
83. Garcia de Avila MA, Hamamoto Filho PT, Jacob FLS, Alcantara LRS, Berghammer M, Jenholt Nolbris M, et al. Children's anxiety and factors related to the COVID-19 pandemic: an exploratory study using the children's anxiety questionnaire and the numerical rating scale. Int J Environ Res Public Health. (2020) 17:5757. doi: 10.3390/ijerph17165757
84. Almeida DM, Horn MC. Is daily life more stressful during middle adulthood. How healthy are we. (2004). p. 425–51.
85. Dahlberg L. Loneliness during the COVID-19 pandemic. Aging Mental Health. (2021) 25:1161–4. doi: 10.1080/13607863.2021.1875195
86. Pan K-Y, Kok AA, Eikelenboom M, Horsfall M, Jörg F, Luteijn RA, et al. The mental health impact of the COVID-19 pandemic on people with and without depressive, anxiety, or obsessive-compulsive disorders: a longitudinal study of three Dutch case-control cohorts. Lancet Psychiatry. (2021) 8:121–9. doi: 10.1016/S2215-0366(20)30491-0
Keywords: resilience, mental burden, risk factors, protective factors, vulnerable groups, SARS-CoV-2, stressor loads
Citation: Hubenschmid L, Helmreich I, Köber G, Gilan D, Frenzel SB, Dick Rv and Lieb K (2022) Effects of general and corona-specific stressors on mental burden during the SARS-CoV-2 pandemic in Germany. Front. Public Health 10:991292. doi: 10.3389/fpubh.2022.991292
Received: 11 July 2022; Accepted: 18 October 2022;
Published: 22 November 2022.
Edited by:
Guohua Zhang, Wenzhou Medical University, ChinaReviewed by:
Ayesha Mumtaz, Hangzhou Normal University, ChinaCopyright © 2022 Hubenschmid, Helmreich, Köber, Gilan, Frenzel, Dick and Lieb. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lara Hubenschmid, bGFyYS5odWJlbnNjaG1pZEBsaXItbWFpbnouZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.