
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Public Health , 25 August 2022
Sec. Occupational Health and Safety
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.989977
This article is part of the Research Topic Qualitative and Quantitative Risk Assessment of Hazardous Substances in the Workplace View all 14 articles
 Alexandre Acramel1,2*†
Alexandre Acramel1,2*† Sandy Blondeel-Gomes3†
Sandy Blondeel-Gomes3† Carla Matta4Subramanian Narayani5Olivier Madar3,6†Romain Desmaris1Laurence Escalup1†
Carla Matta4Subramanian Narayani5Olivier Madar3,6†Romain Desmaris1Laurence Escalup1† Julien Fouque6†
Julien Fouque6†Antineoplastic drugs (ADs) are still the standard treatment of cancer by acting on dividing cells to inhibit the uncontrolled reproduction of cancer cells but also on healthy cells by a non-targeted action. As a consequence, the majority of those medications are regarded as being hazardous to reproduction, carcinogenic, or mutagenic (CMR). In the past, nurses would prepare anticancer medications on the bench top without taking any special safety measures, which had negative effects on the workers who were exposed. There have been reported incidents of rashes, allergies, infertility, miscarriage, birth abnormalities, leukemia, and other malignancies (1). These hazardous drugs are also referenced in the monographs of the International Agency for Research on Cancer (IARC) according to a classification considering the risk of carcinogenicity for humans (2). Several methods have been used to assess occupational exposure directly in biological fluids or indirectly by searching for traces of ADs in the environment.
The implications of long-term exposure to ADs residues in hospitals are still unknown, despite the fact that this risk is now well-documented. The exposure is primarily caused by skin contact with contaminated surfaces. Subsequent biological (3) and toxicological (4) research also confirm that healthcare practitioners continue to be exposed to residual levels of contaminants. Hence, it's critical to manage and reduce the risk of exposure for healthcare professionals.
The European Union emphasized the significance of protecting workers who are exposed to carcinogens or mutagens as a result of the preparation, management, or disposal of hazardous drugs and all work involving exposure to carcinogens or mutagens in light of the fact that 1,5 million healthcare workers in Europe are exposed to ADs [DIRECTIVE (EU) 2019/130].
In western countries, injectable chemotherapy preparations are mainly centralized in hospital pharmacies. It has led to the implementation of additional protective measures throughout the chemotherapy process and setting of environmental monitoring (5) or healthcare workers biological fluids monitoring (3). Nevertheless, a lack of adherence to safety protecting measures and cleaning procedures (6–9), and poor knowledge of contamination risk (10–12) still described in healthcare population.
As we are convinced that the lack of communication conducts to a slackening of daily basis vigilance, we are focusing here on establishing proper feedback and discussions with healthcare workers regarding environmental monitoring campaigns.
Analysis of biological fluids are more informative about the contamination of healthcare workers than environmental monitoring but much more complex to conduct. Environmental monitoring by surface wipe sampling is the most commonly used method to evaluate the contamination throughout the chemotherapy process. It's therefore based on the choice of drugs tracers and the development of an exact, precise and as sensitive as possible analytical method (13).
Manual handling or automatic manufacturing of preparations, infusion of treatment, patients care waste management, and cleaning procedures are all steps during which the risk of contamination is present. Healthcare workers might be exposed when aerosols, leaking or spillage are generated, or when they come in contact with contaminated surfaces during the manufacturing of the preparations, infusion procedure disposal of waste, or cleaning (armchair, toilets, floor or bedding) (14–22).
Regular monitoring of environmental contamination has been carried out for several years in German (23), Italian (24), Czechoslovakian (19), Canadian (20) or American hospitals (21). These monitoring have shown that the risk of healthcare exposure is not systematically related to the level of environmental contamination or to the activity of the chemotherapy process but more to the practices and awareness of healthcare workers. However, these monitoring are useful to evaluate the efficacy of protective equipment, cleaning procedures (25–27), medical devices used for preparation or infusion [for example, Closed System Drug-Transfer Device (CSTDs) (28)], etc.
In some countries environmental monitoring are mandatory and some threshold values have been proposed to graduate the level of contamination and particularly for cyclophosphamide (23, 29–31). Considering the diversity of Ads used throughout the same facility, a multi-component analyzes is advisable. Analytical method must be representative of the activity and take into account the physio-chemical properties of the different ADs used. Several but reasonable number of tracers (5–10 tracers) should be considered but trying to analyze all the ADs of the chemotherapy process could complicate the interpretation. Liquid chromatography in tandem with mass spectrometry is an adequate method for environmental monitoring (13).
Fazel et al. described in a recent paper the “barriers and facilitators for the safe handling” of ADs (10). Although there are recommendations on safe-handling of ADs, evidence suggests that compliance is usually very low. The most common barriers and facilitators identified in this review are, respectively, “poor training” and “adequate safety training.” These authors also emphasize the importance of “creating work environments where safety is a priority for the safe handling” of ADs.
In another paper, Boiano et al. described examples of activities which increase exposure risk reported by workers: “failure to wear appropriate nonabsorbent gown”; “intravenous tubing primed with antineoplastic drug”; “contaminated clothing taken home”; “spill or leak of antineoplastic drug during administration”; “failure to wear chemotherapy gloves”; and “lack of hazard awareness training” (8). In this study, respondents believed that dermal exposure to ADs was minimal and therefore did not wear the required PPE during administration. However, it has been demonstrated that skin contact during handling and administration is possible without precautionary work practices and use of personal protective equipment (PPE). Nowadays, dermal exposure resulting from skin contact with contaminated environmental surface is the main source of contamination. Similarly, despite the fact that safe handling recommendations have long been available, respondents did not always adhere to the advised procedures, highlighting the significance of training and education for both employers and employees. Curiously, the majority of respondents stated that they had received instruction on how to handle antineoplastic medications safely. The risk of exposure perceived by the workers is therefore an important factor in adherence to these safe handling recommendations. Thus, the authors suggest that “employers may be unaware of the adverse health risks,” but also that “better communication is needed to ensure that employers and workers are fully aware of the hazards and precautionary measures” to decrease exposures to ADs.
We described in a recent paper a comparative study of environmental contamination by cyclophosphamide on the two hospital sites of Institut Curie (22). Not surprisingly, this work has shown that our preparation and administration areas are contaminated in very specific locations with cyclophosphamide and we know that other toxic drugs could be detected. The observations conducted in this study, allowed us to assess procedure compliance and identify potential determinants of environmental contamination.
Recently, the French Agency for Food, Environmental and Occupational Health & Safety (Anses) published a report classifying work involving exposure to cytotoxic substances as carcinogenic processes. There is no obligation to make periodic environmental monitoring in France. However, identifying a few representative points of contamination and follow their evolution over times is a pertinent approach of quality improvement and risk management. It seemed essential to us to set up an environmental monitoring procedure in order to periodically check the state of contamination, to assess preventive measures, process changes or decontamination procedures. This also helps educational purposes, specifically to re-sensitize the healthcare workers who trivialize this risk as part of their daily practice. Considering the data available, an annual surface wipe sampling procedure was validated to assess the impact of the corrective measures. This annual surface wipe sampling procedure also include an assessment of professional practices and experience feedback related to contamination. This project, named “Curie CONTA,” is coordinated by a multidisciplinary working group (i.e., the Curie CONTA Committee) composed by pharmacists, pharmacologists, Occupational physicians, Health managers and a Hygiene Health Environment manager. The general procedure of this environmental monitoring is described in Figure 1.
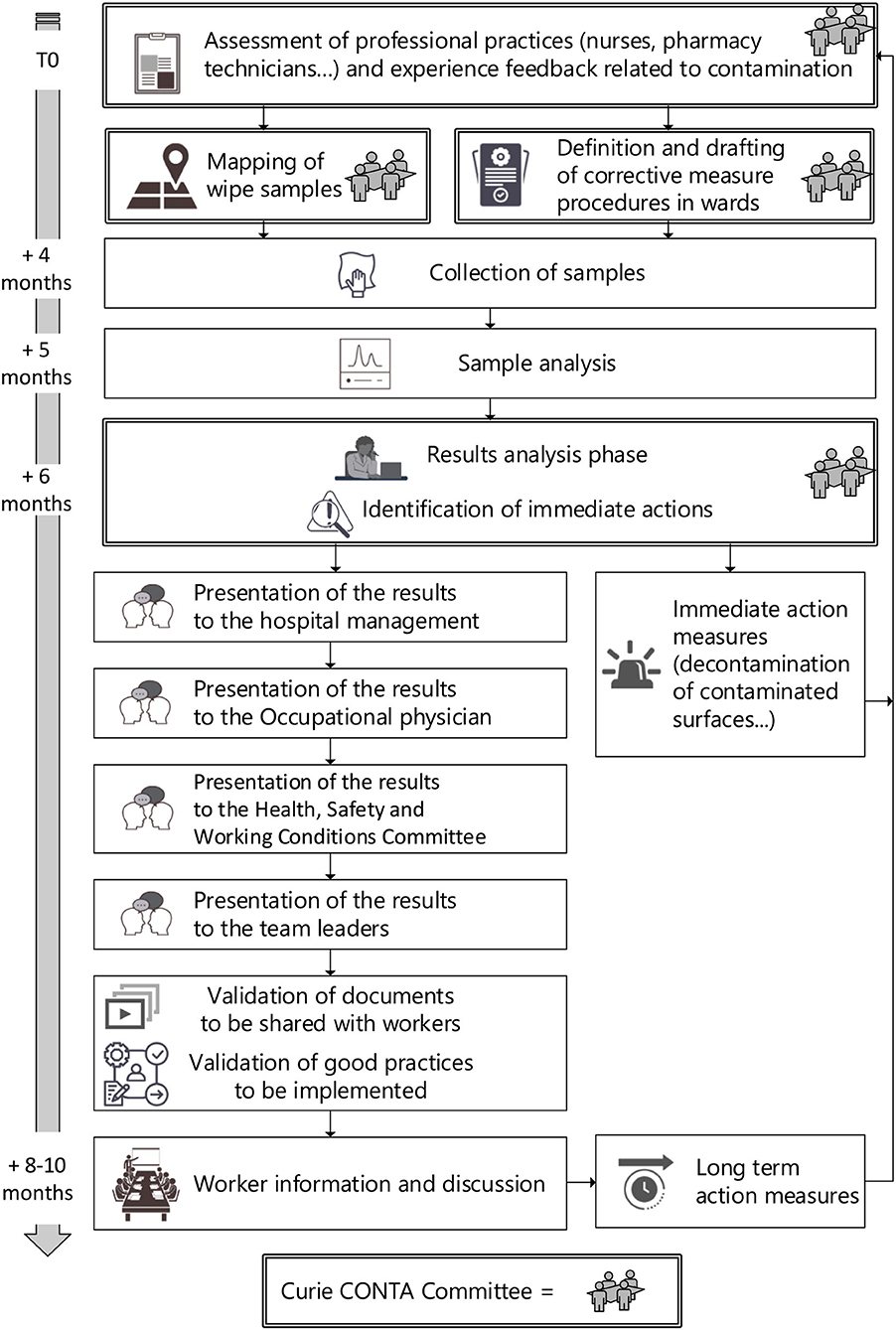
Figure 1. Annual environmental monitoring procedure and communication strategy at Institut Curie.
To our knowledge, the communication of results to healthcare workers is poorly detailed in the literature. That is why we proposed an example of annual communication strategy usually carried out in our hospital since 2018 (Figure 1). In the first place, the Curie CONTA Committee meets to discuss about the evolution of practices and feedback on contamination incidents, to define the mapping of the samples and the corrective measures to be evaluated during the environmental monitoring campaign. The collection of samples is planned with enough time to implement the corrective measures. After the analysis of the surface wipe samples, the results are discussed by the Curie CONTA Committee and if needed, immediate actions are validated. Then the results are presented to the management of the hospital, to the Occupational physician and to the Health, Safety and Working Conditions Committee. Finally, the results are presented to the healthcare workers including cleaning staff. These presentations are adapted for the different audience and validated by the Curie CONTA Committee This communication not only presents the evolution of the environmental contamination but also provides recommendations for controlling this risk of occupational exposure (i.e., long term action measures). Details of this annual environmental monitoring procedure and communication strategy is described in Figure 1.
We are convinced that this descending/ascending communication to healthcare workers is essential. It need to include every worker in order to answer questions, sensitize them to the risk of exposure, and encourage them to follow the defined recommendations. The feedback from the healthcare workers during these presentations are very positive. However, we should assess our approach, for example by using a questionnaire. In our experience, reporting these results of surface contamination measurements is an essential educational tool that raises awareness and helps healthcare professionals to decrease the risk of occupational exposure.
Even if ADs are defined as hazardous drugs, they are still extensively used in hospitals because of the continuous increasing number of cancers. Despite established guidelines, studies indicate poor compliance with current best practices, placing healthcare workers and their family at risk of exposure. The misuse of protective gloves and gowns suggest that there is a perception that exposures are inconsequential or so rare that they do not justify their use (8). The exposures observed through urine (32) or blood samples (33, 34) clearly reflect this lack of effectiveness or compliance with the preventive measures put in place.
Surface wipe sampling is now currently used as a standard method to determine workplace contamination in many countries. It is well-established that success of preventive and corrective measures occurred when surface contamination data are obtained but also properly communicated. The restitution of the results is therefore an important step for an awareness of the risk of exposure and a reminder of good practices. Improvements in prevention actions are therefore necessary and they must relate both to the information and training of workers and to the provision of suitable PPE and organizational measures allowing the control of contamination. An assessment of the impact and effectiveness of these preventive measures must therefore be carried out regularly. In the near future, we are waiting for a European harmonized definition of hazardous drugs. We are also waiting for new independent but comparable environmental monitoring studies from more and more hospitals. To help with this, those monitoring could be centralized by certified laboratories that have the expertise and the means to perform these analyses. Creating a European or International database and defining reference levels for hazardous drugs, specifically ADs would be an ambitious perspective but essential to meet the expectations of this issue. At last, we are also waiting for more ongoing training and education on this issue.
Finally, exposure monitoring and his management are essential. Our opinion is that reporting environmental contamination results to healthcare workers could play a crucial role in decreasing the risk of occupational exposure to hazardous drugs.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors thank the Institut Curie management to support the Curie CONTA project. The authors also thank Marie-Bernard Salines for her help in writing the manuscript in English.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. NIOSH. NIOSH Alert: Preventing Occupational Exposures to Antineoplastic and Other Hazardous Drugs in Health Care Settings. Centers for Disease Control and Prevention (2004). Available online at: http://www.cdc.gov/niosh/docs/2004-165/pdfs/2004-165.pdf (accessed July 1, 2022).
2. IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Volume 100A. Pharmaceuticals. A Review of Human Carcinogens. WHO. (2012). Available online at: http://monographs.iarc.fr/ (accessed July 1, 2022).
3. Leso V, Sottani C, Santocono C, Russo F, Grignani E, Iavicoli I. Exposure to antineoplastic drugs in occupational settings: a systematic review of biological monitoring data. Int J Environ Res Public Health. (2022) 19:3737. doi: 10.3390/ijerph19063737
4. Gianfredi V, Nucci D, Fatigoni C, Salvatori T, Villarini M, Moretti M. Extent of primary DNA damage measured by the comet assay in health professionals exposed to antineoplastic drugs: a systematic review and meta-analysis. IJERPH. (2020) 17:523. doi: 10.3390/ijerph17020523
5. Petit M, Curti C, Roche M, Montana M, Bornet C, Vanelle P. Environmental monitoring by surface sampling for cytotoxics: a review. Environ Monit Assess. (2017) 189:52. doi: 10.1007/s10661-016-5762-9
6. Kim O, Lee H, Jung H, Jang HJ, Pang Y, Cheong H. Korean nurses' adherence to safety guidelines for chemotherapy administration. Eur J Oncol Nurs. (2019) 40:98–103. doi: 10.1016/j.ejon.2019.04.002
7. Silver SR, Steege AL, Boiano JM. Predictors of adherence to safe handling practices for antineoplastic drugs: A survey of hospital nurses. J Occup Environ Hyg. (2016) 13:203–12. doi: 10.1080/15459624.2015.1091963
8. Boiano JM, Steege AL, Sweeney MH. Adherence to safe handling guidelines by health care workers who administer antineoplastic drugs. J Occup Environ Hyg. (2014) 11:728–40. doi: 10.1080/15459624.2014.916809
9. Turci R, Minoia C, Sottani C, Coghi R, Severi P, Castriotta C, et al. Occupational exposure to antineoplastic drugs in seven Italian hospitals: the effect of quality assurance and adherence to guidelines. J Oncol Pharm Pract. (2011) 17:320–32. doi: 10.1177/1078155210381931
10. Fazel SS, Keefe A, Shareef A, Palmer AL, Brenner DR, Nakashima L, et al. Barriers and facilitators for the safe handling of antineoplastic drugs. J Oncol Pharm Pract. (2021) 2021:10781552211040176. doi: 10.1177/10781552211040176
11. Asefa S, Aga F, Dinegde NG, Demie TG. Knowledge and practices on the safe handling of cytotoxic drugs among oncology nurses working at tertiary teaching hospitals in Addis Ababa, Ethiopia. Drug Healthc Patient Saf. (2021) 13:71–80. doi: 10.2147/DHPS.S289025
12. Keat CH, Sooaid NS, Yun CY, Sriraman M. Improving safety-related knowledge, attitude and practices of nurses handling cytotoxic anticancer drug: pharmacists' experience in a general hospital, Malaysia. Asian Pac J Cancer Prev. (2013) 14:69–73. doi: 10.7314/APJCP.2013.14.1.69
13. Portilha-Cunha MF, Alves A, Santos MSF. Cytostatics in indoor environment: an update of analytical methods. Pharmaceuticals (Basel). (2021) 14:574. doi: 10.3390/ph14060574
14. Crauste-Manciet S, Sessink PJM, Ferrari S, Jomier J-Y, Brossard D. Environmental contamination with cytotoxic drugs in healthcare using positive air pressure isolators. Ann Occup Hyg. (2005) 49:619–28. doi: 10.1093/annhyg/mei045
15. Breukels O, van der Gronde T, Simons-Sanders K, Crul M. Antineoplastic drug contamination on the outside of prepared infusion bags. Int J Pharm Compd. (2018) 22:345–9.
16. Crul M, Hilhorst S, Breukels O, Bouman-d'Onofrio JRC, Stubbs P, van Rooij JG. Occupational exposure of pharmacy technicians and cleaning staff to cytotoxic drugs in Dutch hospitals. J Occup Environ Hyg. (2020) 2020:1−10. doi: 10.1080/15459624.2020.1776299
17. Hilliquin D, Tanguay C, Bussières J-F. External contamination of commercial containers by antineoplastic agents: a literature review. Eur J Hosp Pharm. (2020) 27:313–4. doi: 10.1136/ejhpharm-2018-001705
18. Redic KA, Fang K, Christen C, Chaffee BW. Surface contamination of hazardous drug pharmacy storage bins and pharmacy distributor shipping containers. J Oncol Pharm Pract. (2018) 24:91–7. doi: 10.1177/1078155216679027
19. DoleŽalová L, Bláhová L, Kuta J, Hojdarová T, Kozáková Š, Bláha L. Levels and risks of surface contamination by thirteen antineoplastic drugs in the Czech and Slovak hospitals and pharmacies. Environ Sci Pollut Res. (2022) 29:26810–9. doi: 10.1007/s11356-021-17607-y
20. Delafoy C, Roussy C, Hudon A-F, Cirtiu CM, Caron N, Bussières J-F, et al. Canadian monitoring program of the surface contamination with 11 antineoplastic drugs in 122 centers. J Oncol Pharm Pract. (2022) 2022:10781552211072876. doi: 10.1177/10781552211072877
21. Jeronimo M, Arnold S, Astrakianakis G, Lyden G, Stewart Q, Petersen A, et al. Spatial and temporal variability in antineoplastic drug surface contamination in cancer care centers in Alberta and Minnesota. Ann Work Exposures Health. (2021) 65:760–74. doi: 10.1093/annweh/wxab013
22. Acramel A, Fouque J, Blondeel-Gomes S, Huguet S, Rezai K, Madar O, et al. Application of an environmental monitoring to assess the practices and control the risk of occupational exposure to cyclophosphamide in two sites of a French comprehensive cancer center. Ann Work Exposures Health. (2022) 2022:wxac035. doi: 10.1093/annweh/wxac035
23. Schierl R, Böhlandt A, Nowak D. Guidance values for surface monitoring of antineoplastic drugs in German pharmacies. Ann Occup Hyg. (2009) 53:703–11. doi: 10.1093/annhyg/mep050
24. Sottani C, Grignani E, Oddone E, Dezza B, Negri S, Villani S, et al. Monitoring surface contamination by antineoplastic drugs in Italian hospitals: performance-based hygienic guidance values (HGVs) project. Ann Work Expo Health. (2017) 61:994–1002. doi: 10.1093/annweh/wxx065
25. Simon N, Odou P, Decaudin B, Bonnabry P, Fleury-Souverain S. Efficiency of degradation or desorption methods in antineoplastic drug decontamination: A critical review. J Oncol Pharm Pract. (2019) 25:929–46. doi: 10.1177/1078155219831427
26. Simon N, Guichard N, Odou P, Decaudin B, Bonnabry P, Fleury-Souverain S. Efficiency of four solutions in removing 23 conventional antineoplastic drugs from contaminated surfaces. PLoS ONE. (2020) 15:e0235131. doi: 10.1371/journal.pone.0235131
27. Bláhová L, Kuta J, DoleŽalová L, Kozáková Š, Krovová T, Bláha L. The efficiency of antineoplastic drug contamination removal by widely used disinfectants-laboratory and hospital studies. Int Arch Occup Environ Health. (2021) 94:1687–702. doi: 10.1007/s00420-021-01671-5
28. Tang Y, Che X, Wang YL, Ye X, Cao WL, Wang Y. Evaluation of closed system transfer devices in preventing chemotherapy agents contamination during compounding process—a single and comparative study in China. Front Public Health. (2022) 10:e827835. doi: 10.3389/fpubh.2022.827835
29. Sessink PJ. Environmental contamination with cytostatic drugs: past, present and future. Saf Consid Oncol Pharm. (2011) 2011:3–5.
30. Hedmer M, Wohlfart G. Hygienic guidance values for wipe sampling of antineoplastic drugs in Swedish hospitals. J Environ Monitor. (2012) 14:1968–75. doi: 10.1039/c2em10704j
31. Kiffmeyer TK, Tuerk J, Hahn M, Stuetzer H, Hadtstein C, Heinemann A, et al. Application and assessment of a regular environmental monitoring of the antineoplastic drug contamination level in pharmacies - the MEWIP project. Ann Occup Hyg. (2013) 57:444–55. doi: 10.1093/annhyg/mes081
32. Villa A, Molimard M, Sakr D, Lassalle R, Bignon E, Martinez B, et al. Nurses' internal contamination by antineoplastic drugs in hospital centers: a cross-sectional descriptive study. Int Arch Occup Environ Health. (2021) 94:1839–50. doi: 10.1007/s00420-021-01706-x
33. Béchet V, Benoist H, Beau F, Divanon F, Lagadu S, Sichel F, et al. Blood contamination of the pharmaceutical staff by irinotecan and its two major metabolites inside and outside a compounding unit. J Oncol Pharm Pract. (2021) 28:777–84. doi: 10.1177/10781552211012059
Keywords: antineoplastic drugs, occupational exposure, environmental monitoring, wipe samples, hospital, healthcare worker, communication
Citation: Acramel A, Blondeel-Gomes S, Matta C, Narayani S, Madar O, Desmaris R, Escalup L and Fouque J (2022) Reporting environmental contamination results to healthcare workers could play a crucial role in decreasing the risk of occupational exposure to antineoplastic drugs. Front. Public Health 10:989977. doi: 10.3389/fpubh.2022.989977
Received: 09 June 2022; Accepted: 05 August 2022;
Published: 25 August 2022.
Edited by:
Jianlin Lou, Zhejiang Academy of Medical Sciences, ChinaReviewed by:
Giuseppe De Palma, University of Brescia, ItalyCopyright © 2022 Acramel, Blondeel-Gomes, Matta, Narayani, Madar, Desmaris, Escalup and Fouque. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandre Acramel, YWxleGFuZHJlLmFjcmFtZWxAZ21haWwuY29t
†ORCID: Alexandre Acramel orcid.org/0000-0002-7793-7374
Sandy Blondeel-Gomes orcid.org/0000-0002-6437-8753
Olivier Madar orcid.org/0000-0003-1374-0879
Laurence Escalup orcid.org/0000-0003-3093-339X
Julien Fouque orcid.org/0000-0002-9914-8819
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.