
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 09 September 2022
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.989337
This article is part of the Research Topic Current Research on Serological Analyses of Infectious Diseases View all 11 articles
 Peter Willeit1,2
Peter Willeit1,2 Janine Kimpel3
Janine Kimpel3 Hannes Winner4
Hannes Winner4 Teresa Harthaller3
Teresa Harthaller3 Helena Schäfer3David Bante3Barbara Falkensammer3
Helena Schäfer3David Bante3Barbara Falkensammer3 Annika Rössler3Lydia Riepler3Cornelia Ower5Magdalena Sacher6
Annika Rössler3Lydia Riepler3Cornelia Ower5Magdalena Sacher6 Dorothee von Laer3
Dorothee von Laer3 Wegene Borena3*
Wegene Borena3*In order to curb the rapid dissemination of the B.1.351 variant of SARS-CoV-2 in the district of Schwaz and beyond, the EU allocated additional vaccine doses at the beginning of March 2021 to implement a rapid mass vaccination of the population (16+). The aim of our study was to determine the seroprevalence of SARS-CoV-2 among the adult population in the district of Schwaz at the time of the implementation. Data on previous history of infections, symptoms and immunization status were collected using a structured questionnaire. Blood samples were used to determine SARS-CoV-2 specific anti-spike, anti-nucleocapsid and neutralizing antibodies. We recruited 2,474 individuals with a median age (IQR) of 42 (31–54) years. Using the official data on distribution of age and sex, we found a standardized prevalence of undocumented infections at 15.0% (95% CI: 13.2–16.7). Taken together with the officially documented infections, we estimated that 24.0% (95% CI: 22.5–25.6) of the adult population had prior SARS-CoV-2 infection. Hence, the proportion of undocumented infections identified by our study was 55.8% (95% CI: 52.7–58.5). With a vaccination coverage of 10% among the adults population at that time, we imply that a minimum of two-thirds of the target popuation was susceptible to the circulating threat when this unique campaign started.
As global efforts are in progress to cope with the uncontrolled transmission of SARS-CoV-2 infection, new variants surface as obstacles against the process of containment. The variant B.1.351, detected for the first time in South Africa in October 2020 (1), was found to have impaired neutralization by convalescent plasma from the wild type infection. A potential dominance of such immune escape variants may pose a serious threat to real world vaccine effectiveness.
Almost simultaneously with the introduction of the first vaccines at the beginning of the year 2021, Europe notified increased circulation of the variant B.1.351 (2).
Having reported over 300 cases of infections with this variant of concern (VOC) at that time, Austria came into focus as a hotspot (3, 4). Almost all reported cases originated from the district of Schwaz in the western part of the country. In order to curb the spread of this variant, the European Union chose the district to serve as a model region and provided Austria with 100,000 doses of the BNT162b2 (Comirnaty) vaccine by BioNTech/Pfizer for the immediate immunization of 50,000 adults living in this district. According to official reports, approximately 41,700 (61% of the adult population) received both doses of the vaccine as part of this immunization programme (4, 5).
Vaccine donors, regional or national health authorities, vaccine policy makers, other relevant institutions or even the general public may legitimately wonder what proportion of the community had already been exposed to the virus or what proportion was completely immuno-naïve as this unique immunization campaign started. The results may be used as baseline information in evaluating the performance of the mass immunization in achieving the goal it was aimed for (6). Although for this purpose data from the official registry of SARS-CoV-2 infections may be utilized, it is highly likely that a non-negligible proportion of the population might have gone through an infection that has remained undetected and unreported (7–10). Anti-nucleocapsid antibodies may help identify, irrespective of vaccination status, subjects with prior infections which were not detected by the conventional confirmatory tests.
With this study, we aimed to determine the prevalence SARS-CoV-2 infection status through the use of serological assays in the district of Schwaz at the time of the mass vaccination.
The study was conducted in March 2021. All adult residents of the district Schwaz in Tyrol, aged 18 years and above (n = 68,896), were invited through the local county office and local media. Consenting participants were asked to fill out a short questionnaire on sociodemographic aspects as well as their history of SARS-CoV-2 infection, history of hospitalization and the status of vaccination. Blood samples (EDTA) collected at the study site were used for the determination of SARS-CoV-2-specific antibodies targeting the spike (S) and nucleocapsid (N) proteins.
All samples were tested using the Chemiluminescent-based immunoassay—SARS-CoV-2 IgG II Quant (Abbott, Illinois, USA). The assay detects antibodies directed against S protein and was performed on the ARCHITECT i2000SR platform. Using standards of various concentrations, results were provided in a quantitative manner as binding antibody units per milliliter (BAU/ml). According to the manufacturer, the cutoff for positivity was defined to be >7.1 BAU/ml. All samples were further analyzed using a second serological assay—the Elecsys Anti-SARS-CoV-2 (Roche Diagnostics, Indianapolis, USA)—which detected antibodies against the N protein of SARS-CoV-2. Detection of anti-N immunoglobulin (anti-N Ig) has the additional value of differentiating between post-infection and post-vaccination antibody positivity. Individuals with positive anti-N Ig were further tested for the presence of neutralizing antibodies using an in-house pseudovirus-based assay (pVNT) as described previously (11, 12). In short, replication defective vesicular stomatitis virus (VSVΔG-GFP) pseudotyped with Wuhan-1 spike protein was used to infect susceptible cells (293T-ACE2) after pre-incubation with participant's plasma in serial four-fold dilutions. Cells infected with the pseudovirus expressed GFP. This signal was quantified approximately 16 hours after infection using a spot reader (ImmunoSpot® S5 analyzer). Continuous titers that resulted in 50% reduction of GFP expression (50% inhibition titer) as compared to virus-only wells were determined using a non-linear regression method as described before (13). Titers ≥1:16 (continuous titer of ≥16) were considered positive.
Our study population showed a slight predominance of women and subjects between 25 to 55 years of age as compared to the general (source) population (Supplementary Figure 1). In order to account for these discrepancies, we estimated the overall prevalence through age and sex standardization. To counteract a potential selection-bias of the study (i.e., more subjects with a history or suspicion of previous SARS-CoV-2 infection preferentially willing to participate), we estimated the serology-derived proportion of unreported infections and interpreted the result in combination with data from officially reported cases. For this purpose, we excluded subjects who gave a history of prior infection in the questionnaire and considered anti-N positivity among the rest of the study participants to represent the proportion of undocumented infections. Through direct age standardization using the official census data of the district (14), we estimated the seroprevalence in the adult population of Schwaz (source population). We defined the true cumulative incidence at the time of data collection to be the sum of the estimated undocumented infections and the officially reported daily numbers stratified by age and sex kindly provided by the Austrian Agency for Health and Food Safety (Dr. Daniela Schmid, AGES).
We used student's t-test or ANOVA to test for a difference in quantitative variables across groups. We applied non-parametric tests (Mann-Whitney U test and Kruskal-Wallis) for variables not fulfilling the criteria of normality. For variables of categorical nature, we used χ2-test (Fisher's exact where appropriate). For the main analysis of seroprevalence of unreported infections using Roche anti-N Ig we also provided a Rogan-Gladen correction for an imperfect diagnostic test. 95% CIs were calculated using the Clopper-Pearson exact method (15). The level of significance was set at 5% using two-sided tests where applicable.
The study was approved by Ethics Committee of the Medical University of Innsbruck (EK Nr:1093/2021).
As shown in Table 1, the total number of participants added up to 2,474 adults (n = 1,028 males and n = 1,446 females) between 18 and 89 years of age. While 593 participants (24%, 95% CI: 22.4–25.6) reported to have had a PCR (n = 591) or antigen (n = 2) confirmed SARS-CoV-2 infection, 94 (3.8%, 95% CI: 3.1–4.5) reported a previous infection based on a routine antibody test. Only 15 participants (2.1%) reported to have been hospitalized due to SARS-CoV-2 infection. Around 15% of subjects with a previous infection reported to have had no symptoms. Among participants with a history of infection and reporting symptoms (n = 578), the majority (52.8%) had only mild symptoms without being bedridden. Although symptom reporting was more common among females than males [OR, (95% CI) = 2.03 (1.34–3.14)], significantly more males reported to have been hospitalized [OR, (95% CI) = 3.04 (1.03–8.99)]. A total of 1,948 participants (79.2%) had received at least one dose of an mRNA or a vector vaccine approved in Europe at the time of the study (a single individual reported to have received BBIBP-CorV, Sinopharm). The majority (92%) of the vaccinated subjects had received Comirnaty—as part of the mass vaccination with a median (IQR) of 9 (7–10) days prior to the study—followed by Vaxzevria (ChAdOx1, AstraZeneca) (7.6%). No significant difference was observed in the vaccination status across sexes.
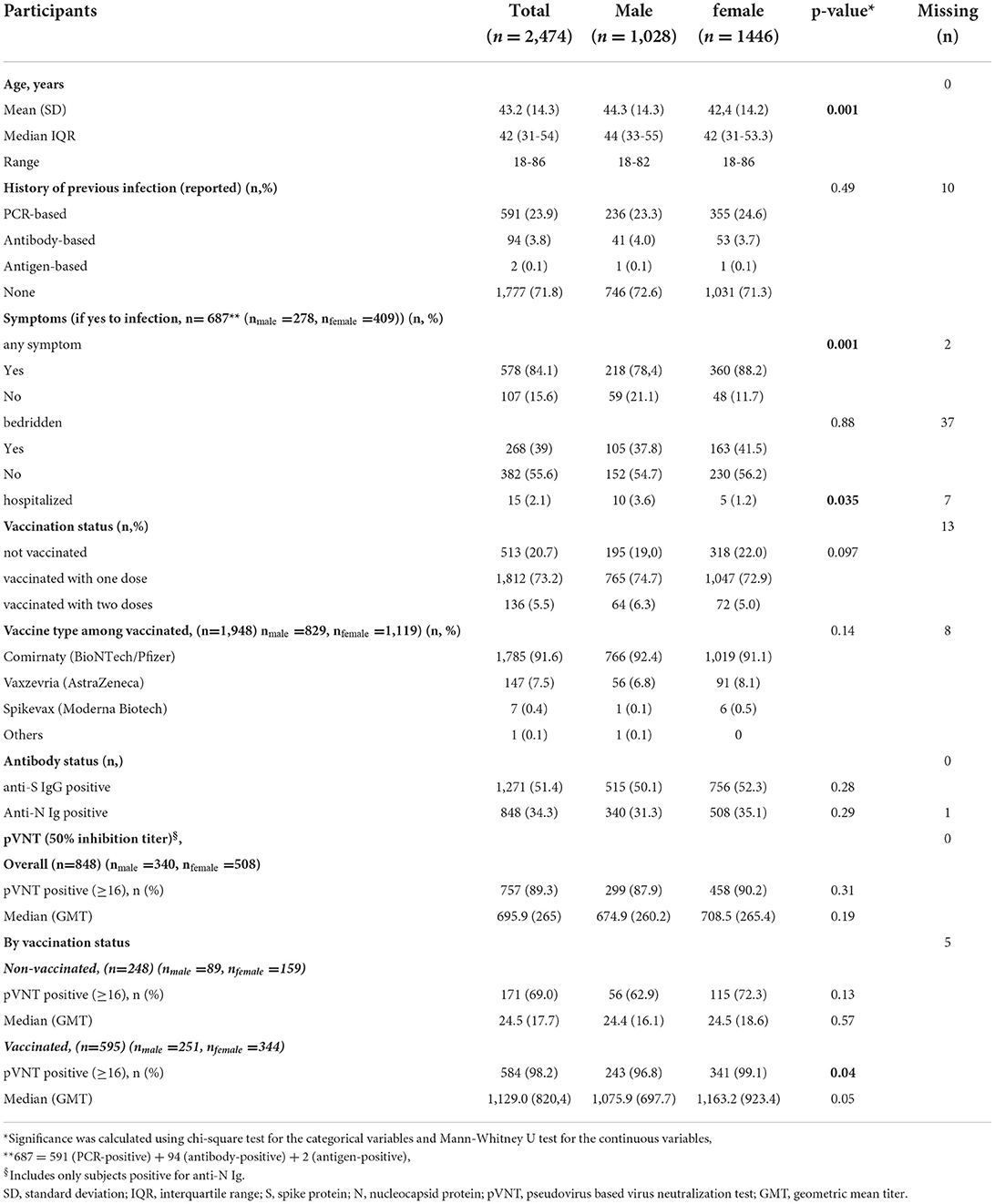
Table 1. Baseline characteristics of study participants (n = 2,474).
Independent of sex, the proportion of subjects positive for anti-S IgG antibody was 51.4% and positive for anti-N antibody 34.3% (p = 0.28 and 0.29, respectively) (Table 1). The proportion of anti-S positives was higher since there were participants who had been vaccinated prior to or as part of the mass immunization programme.
In order to assess the seroprevalence of SARS-CoV-2 antibodies before the mass vaccination, we characterized (as shown in Table 2) subjects with positive anti-N Ig antibodies (n = 848). We observed a significant association between anti-N Ig levels and age but no difference across sexes. The median concentration was three times higher among participants older than 60 years as compared to those below 40 years of age. Only 548 (64.6%) anti-N Ig positive subjects also reported a history of previous PCR- or antigen-confirmed SARS-CoV-2 infection. About one third of the remaining 296 subjects with no history of PCR- or antigen-confirmed SARS-CoV-2 infections reported to have found out about a previous infection based on an antibody test prior to the study, taking 205 participants (8.3% of the total study participants) by surprise. Participants reporting severe symptoms or a history of hospitalization had significantly higher anti-N Ig concentrations than participants without (p = 0.008 and 0.018, respectively). The mere presence or absence of symptoms showed no significant difference on the level of antibodies directed against N protein.
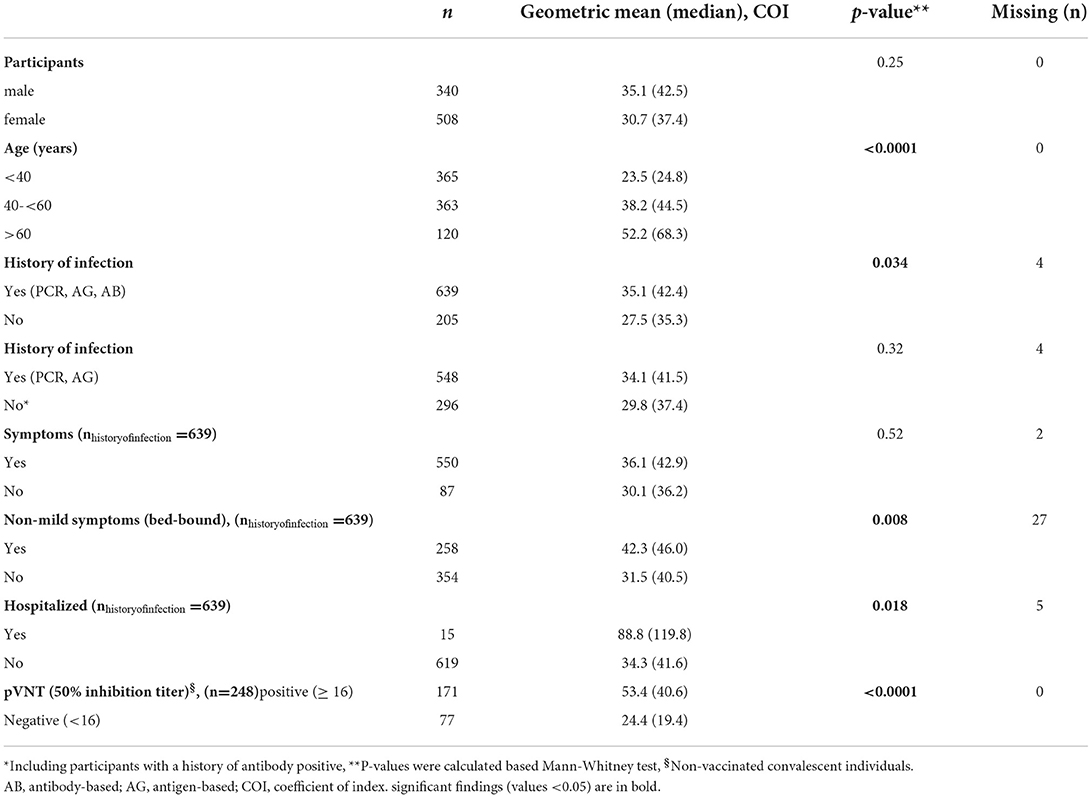
Table 2. Geometric mean (median) anti-N antibody concentrations across participant characteristics (n=848).
The majority of anti-N Ig positive subjects, 757 (89.3%), were also positive for neutralizing antibodies. However, a significant proportion had already received at least one dose of SARS-CoV-2 vaccines prior to our study impeding the interpretation of infection-induced neutralization activity. Compared to 98.2% of previously infected plus vaccinated individuals only 69.0% of the participants with previous infection without any history of vaccination were positive for neutralizing antibodies. The median 50% inhibition titer was 46 fold higher in the vaccinated plus infected group as compared to the non-vaccinated convalescent group (p < 0.0001). Concentrating on the group with a history of infection but no vaccination (n = 248), we observed a significant association between anti-N Ig level and positivity for neutralizing antibodies.
Undocumented infection was defined as being anti-N Ig positive despite reporting to have had no known SARS-CoV-2 infection in the past. After excluding 548 persons who explicitely reported to have had prior PCR- or antigen-based infection, we found the crude seroprevalence of undocumented infections among the study population reporting no history of infection to be 15.8% (95% CI: 14.2–17.6). Supplementary Figure 2 shows the quantitative distribution of anti-N Ig values across age.
Since the age and sex distribution of the study participants showed obvious deviation from the official distribution of the total population in Schwaz (Supplementary Figure 1), we estimated the age and sex standardized prevalence (95% CI) of undocumented infections as shown in Table 3. We initially estimated the number of individuals in the general population with undocumented infections by projecting the age-specific crude seroprevalence from the study population to the total population. We then determined the overall prevalence of undocumented infections across age categories and sex. The sum of the prevalences across these age strata (15.0%, 95% CI: 13.3–16.7) was the overall age standardized prevalence among adults in Schwaz. This translated into 9,228 (95% CI: 8,150–10,296) undocumented infections out of 61,576 adults officially never having a previous SARS-CoV-2 infection (Table 4). Taking 7,320 subjects officially reported to have had confirmed SARS-CoV-2 at the time of data collection (information obtained from AGES), the true total number of infections in the adult population of the district of Schwaz by March 2021 was estimated at 7,320 + 9,228 = 16,548 (95% CI: 15,494 – 17,616) which translates into an overall pre-mass vaccination SARS-CoV-2 prevalence of 24% (95% CI: 22.5–25.6) and a proportion of undocumented infections of 55.8% (95% CI: 52.7–58.5) in adults at that time.
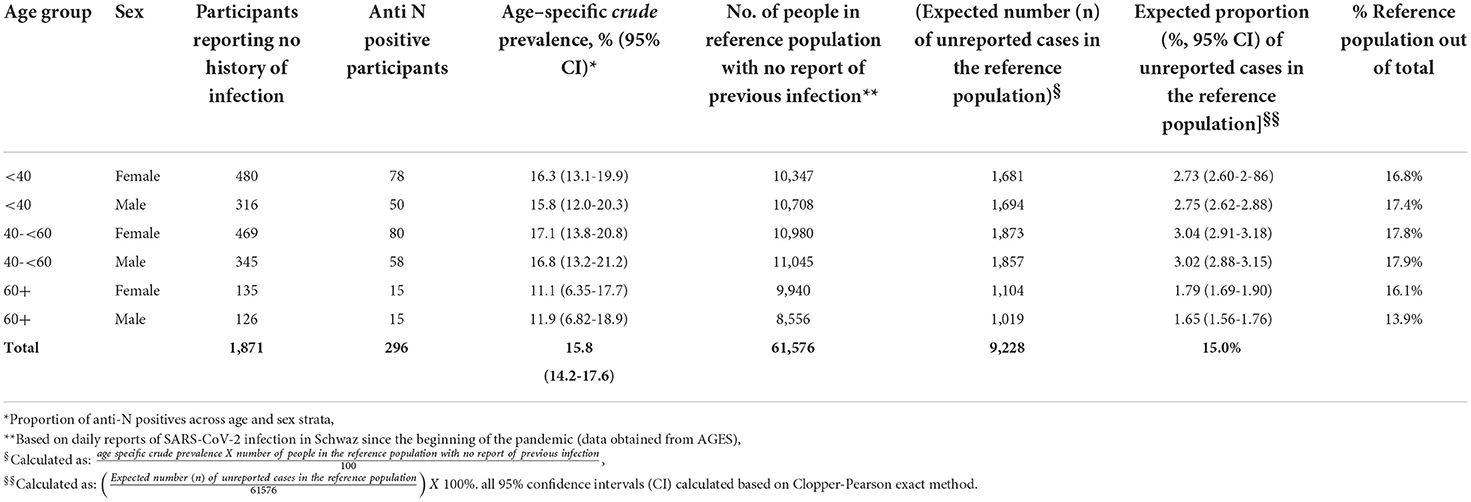
Table 3. Characterizing study population and source population without a known history of officially reported SARS-CoV-2 infection.
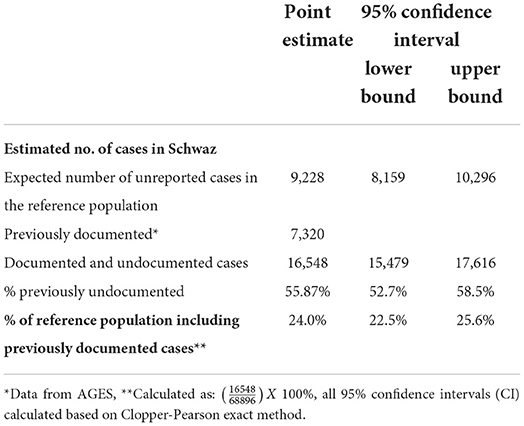
Table 4. Projected undocumented and overall point prevalence of SARS-SoV-2 infection in the district of Schwaz just before the mass immunization campaign.
In a sensitivity analysis that employed the Rogan-Gladen correction for an imperfect diagnostic test (Supplementary Table 1), the results were similar to the principal analysis, as expected given the sensitivity and specificity of the anti-N Ig assay close to 100%. In specific, in participants without a known history of SARS-CoV-2 infection, the age- and sex-standardized seroprevalence was 14.9% (95% CI: 13.2–16.6%) and the expected number of unreported cases in the reference population was 9,169 (95% CI: 8,103–10,233) after correction.
At the time of our data collection, the mass vaccination had been going on for about one week. In order to avoid a potential bias caused by anti-S IgG seroconversion following vaccination, we chose to use anti-N Ig in estimating the seroprevalence. This helps to doubtlessly exclude the effect of vaccination following SARS-CoV-2 infection, since earliest seroconversion has been described to occur within days post vaccination (16–20). The demonstrably good performance of the Roche anti-N immunoglobulin assay underscores the validity of our approach (21–23). Moreover, the assay proved a persistently high sensitivity even months after a confirmed infection (23).
With 7,320 officially documented cases above the age of 18 at the time of the study, the official SARS-CoV-2 prevalence would be estimated to 10.6% (95% CI: 10.4–10.9) at that time. The fact that 24% of the study participants reported to have had PCR- or antigen-confirmed infection led to the reasonable suspicion that our convenience sampling may have resulted in a selection bias. A seroprevalence of 34.3% based on anti-N positivity is thus likely to be an overestimation. Consequently we opted to include, in the main analysis, only subjects who reported no known history of infection (n = 1,871) and to estimate age standardized cumulative incidence of unreported infections in the general adult population of the district of Schwaz (n = 61,576). Using data obtained from official statistics in Austria (14), we accounted for disproportional age and sex distribution of the study population by conducting direct age and sex standardization. Our finding of standardized seroprevalence of 15.0% translates into previously undocumented 9,228 cases (95% CI: 8,159–10,296) in the general adult population of Schwaz. Adding this to 7,320 (10.6%) subjects officially reported to have had SARS-CoV-2 at the time of data collection (data from AGES), the overall prevalence of SARS-CoV-2 infection at the start of the mass vaccination among adults added up to 24% (95% CI: 22.5–25.6). With a vaccination coverage of 10% among the adult population of Schwaz prior to the mass immunization campaign (6), our result implies that a maximum of one third of the adult popuation had at least one SARS-CoV-2 specific immunological event.
Comprehensive meta-analysis studies indicate that a plethora of seroprevalence studies has been conducted across the globe since early on in the pandemic. A wide range of cumulative incidence has been reported depending on the population studied, the sample size used, the serological method applied, the time of the study since the start of the pandemic or whether or not vaccination status was considered (24, 25), making direct comparison of estimates very challenging.
Based on a review on population-based studies in Europe until September 2020, for example, the seroprevalence ranged from as low as 0.42% in some studies to as high as 23.3% in a highly affected region of Lombardy, Italy following the first wave of infection (24). Another study conducted in Ischgl, a once-a-corona-hotspot ski resort in western Austria in April 2020, found an even higher seroprevalence of 42% (26). A nation-wide study in Austria, conducted in Autumn of 2020 using a representative sample of the Austrian population, found a seroprevalence of 4.7% (95% CI: 3.8–5.6) and reported that the estimate for western Austria was higher (5.7%, 95% CI: 4.1–7.4) (27).
Our study was conducted at the end of the second infection wave, hence the higher seroprevalence highlighting the temporal continuum of the rising infection numbers. A follow-up nationwide survey conducted between October 2020 and January 2021 and global epidemiological data on seroprevalence over time also corroborate this temporal trend (25, 28).
Regarding antibody concentration and age, our findings are in accord with several previous works showing higher antibody titres in older adult populations, presumably owing to the fact that age is a known risk factor for severe disease (29–32). Since the very beginning of the pandemic, even before vaccines were available, several studies reported higher levels of both binding and neutralizing antibodies correlating with disease severity, which in turn has been shown to correlate with age among other factors (33–37).
Similarly, a superiority of the concentration and quality of antibodies generated by vaccinees with a history of infection compared to immuno-naïve vaccinees has also been reported previously, even following a single dose (18, 38–45). The robustness of this finding is strengthened by the observation that not only humoral response but also cellular immunity was generally superior in the non-naïve group (40, 43, 45).
Since seroprevalence surveys conducted after 2021 paralleled the vaccination rollout, interpretation of data has been a challenge unless non-vaccine-induced antibodies like the nucleocapsid protein antibodies are targeted. Similar to ours, several other studies investigated seroprevalence based on anti-N Ig in the post-vaccine era. Studies targeting health care workers or patients or residents of nursing homes found a much higher seroprevalence than ours owing to the high-risk target population (46–48). For instance, a prospective study from England, which examined the prevalence of SARS-CoV-2 among both residents and staff in long-term care facilities over a period of March through the beginning of May 2021 found a prevalence of anti-N Ig positivity of 34.6% among the residents and 26.1% among staff (47).
Blood donors, on the other hand, make up a comparable group to our study population. Contemporaneous to ours, another survey assessed seroprevalence among Tyrolean blood donors targeting anti-N antibodies. Siller et al. found seropositivity (95% CI) of 14.0% (13.0–15.1) among donor samples collected in March 2021 (49), a finding notably lower than ours (24%) in the district of Schwaz. Several factors may be accountable for this: First, the two studies used different serological platforms—chemiluminescent microparticle immunoassay from Abbott vs. Electrochemiluminescence immunoassay from Roche. These two assays were shown to have a significant gap in sensitivity of detecting anti-N antibodies particularly later in the post-infection period in favor of the Roche assay (40): Six months post confirmed SARS-CoV-2 infection, the Roche assay had a sensitivity of 94,3% (95% CI: 84.3–98.8) in detecting anti-N antibodies whereas for the Abbott system it was only at 45.3 % (95% CI: 31.6–59.6%) (39). Second, reports from official data indicated that the district of Schwaz had higher incidence rates (49, 50) in the second infection wave as compared to the rest of the Tyrolean districts, further accounting for the discrepancy.
Common to the majority of previously published seroprevalence data, as underpinned by a large global meta-analysis, is that the estimates based on serological approach are clearly higher than the officially reported ones with values ranging from as low as 1.5 times to as high as 10 times the reported cumulative incidence (51). With 55.8% of seropositive subjects having never been registered officially, our study underpins this notion.
Beyond the large sample size, the availability of data on daily infections in the study district across age and sex since the start of the pandemic, as well as the official census data that enabled a direct age standardization and projection of estimates to the general population, is one strength of the study. The main serological assay we used to determine seroprevalence has a high sensitivity and specificity (22, 23).
A major limitation of this study is the convenience-sampling approach in which individuals who were willing to participate may be significantly different from those who were not attracted by this approach. This might have resulted in selection bias toward higher prevalence. We aimed to balance this effect by concentrating on subjects reporting no known history of previous infection and by coupling the unreported infections to the officially registered cases. A further limitation is that our data concentrated only on the adult population as we lacked ethical clearance to include minors.
Our conclusions are twofold. First, by accounting for the undocumented cases through serological approach, our study confirmed once again that officially reported data on infection status markedly underestimate the true prevalence. Second, adding our finding to the vaccine coverage of 10% among the adults population shortly before the mass immunization campaign (6), our result implies that at least two-thirds of the adult population was immuno-naïve and susceptible to the circulating threat as this unique campaign started.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Ethics Committee of the Medical University of Innsbruck (EK Nr:1093/2021). The patients/participants provided their written informed consent to participate in this study.
Conceptualization: DL and WB. Data and sample acquisition: HS, DB, BF, TH, CO, MS, and WB. Laboratory work: JK, WB, AR, and LR. Data cleaning: TH and WB. Formal data analysis: PW, WB, and HW. Manuscript drafting: WB and PW. All authors have read, critically reviewed, and agreed to this version of the manuscript.
We thank Maria Huber, Albert Falch, Evelyn Peer, Lisa-Maria Raschbichler, and the whole diagnostic and research team at the Institute of Virology for excellent technical support. We are also grateful to Bianca Neurauter, Eva Hochmuth, and Luiza Hoch and the whole organization team for excellent coordination of the study both at the laboratory and at the study site.
DB declares to hold stocks of Pfizer.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.989337/full#supplementary-material
Supplementary Figure 1. Age structure of the study population as compared to the official age structure in Schwaz (source population) among men (A) and women (B) [Source population data from Statisik Austria (14)].
Supplementary Figure 2. Spearman‘s correlation coefficient (r) and 95% CI between anti N Ig and age of study participants with no reports of known prior infection (n = 1871) (A) and the whole study participants (n = 2472) (B). Dotted horizontal lines represent the cutoff values as recommended by the manufacturer. COI, coefficient of index; N, nucleocapsid; Ig, Immunoglobulin.
Supplementary Table 1. Seroprevalence of unreported SARS-CoV-2 infection after Rogan-Gladen correction.
1. Tegally H, Wilkinson E, Giovanetti M, Iranzadeh A, Fonseca V, Giandhari J, et al. Detection of a SARS-CoV-2 variant of concern in South Africa. Nature. (2021) 592:438–43. doi: 10.1038/s41586-021-03402-9
2. European Center For Disease Prevention Control,. Rapid Risk Assessment: SARS-CoV-2 – increased circulation of variants of concern vaccine rollout in the EU/EEA, 14th update. (2021). Available online at: https://www.ecdc.europa.eu/sites/default/files/documents/RRA-covid-19-14th-update-15-feb-2021.pdf (accessed November, 2021).
3. AGES Österreichische Agentur für Gesundheit und Ernährungssicherheit GmbH,. SARS-CoV-2-Varianten in Österreich. (2022). Available online at: https://www.ages.at/en/topics/pathogenic-organism/coronavirus/SARS-CoV-2-varianten-inoesterreich/"onavirus/SARS-CoV-2-varianten-in-oesterreich/ (accessed May, 2021).
4. AGES. Österreichische Agentur für Gesundheit und Ernährungssicherheit GmbH. SARS-CoV-2-Varianten in Österreich. (2022). Available online at: https://www.ages.at/themen/krankheitserreger/coronavirus/SARS-CoV-2-varianten-in-oesterreich/ (accessed May, 2021).
5. Gesundheitsministerium Österreich,. Impflage. (2022). Available online at: https://info.gesundheitsministerium.at/impflage (accessed June, 2022).
6. Paetzold J, Kimpel J, Bates K, Hummer M, Krammer F, von Laer D, Winner H. Impacts of rapid mass vaccination against SARS-CoV2 in an early variant of concern hotspot. Nat Commun. (2022) 13:612. doi: 10.1038/s41467-022-28233-8
7. Li R, Pei S, Chen B, Song Y, Zhang T, Yang W, Shaman J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science. (2020) 368:489–493. doi: 10.1126/science.abb3221
8. Grant R, Dub T, Andrianou X, Nohynek H, Wilder-Smith A, Pezzotti P, Fontanet A. SARS-CoV-2 population-based seroprevalence studies in Europe: a scoping review. BMJ Open. (2021) 11:e045425. doi: 10.1136/bmjopen-2020-045425
9. Sah P, Fitzpatrick MC, Zimmer CF, Abdollahi E, Juden-Kelly L, Moghadas SM, et al. Asymptomatic SARS-CoV-2 infection: a systematic review and meta-analysis. Proc Natl Acad Sci U S A. (2021) 118:e2109229118. doi: 10.1073/pnas.2109229118
10. Moghadas SM, Fitzpatrick MC, Sah P, Pandey A, Shoukat A, Singer BH, et al. The implications of silent transmission for the control of COVID-19 outbreaks. Proc Natl Acad Sci U S A. (2020) 117:17513–5. doi: 10.1073/pnas.2008373117
11. Riepler L, Rössler A, Falch A, Volland A, Borena W, von Laer D, et al. Comparison of four SARS-CoV-2 neutralization assays. Vaccines (Basel). (2020) 9:13. doi: 10.3390/vaccines9010013
12. Borena W, Bánki Z, Bates K, Winner H, Riepler L, Rössler A, et al. Persistence of immunity to SARS-CoV-2 over time in the ski resort Ischgl. EBioMedicine. (2021) 70:103534. doi: 10.1016/j.ebiom.2021.103534
13. Ferrara F, Temperton N. Pseudotype neutralization assays: from laboratory bench to data analysis. Methods Protoc. (2018) 1:8. doi: 10.3390/mps1010008
14. Statistik Austria,. Bevölkerung nach Alter und Geschlecht. (2021). Available online at: https://www.statistik.at/web_de/statistiken/menschen_und_gesellschaft/bevoelkerung/bevoelkerungsstruktur/bevoelkerung_nach_alter_geschlecht/index.html (accessed November, 2021).
15. Clopper CJ, Pearson ES. The use of confidence or fiducial limits illustrated in the case of the binomial. Biometrika. (1934) 26:404–13. doi: 10.1093/biomet/26.4.404
16. Gonçalves J, Juliano AM, Charepe N, Alenquer M, Athayde D, Ferreira F, et al. Secretory IgA and T cells targeting SARS-CoV-2 spike protein are transferred to the breastmilk upon mRNA vaccination. Cell Rep Med. (2021) 2:100468. doi: 10.1016/j.xcrm.2021.100468
17. Lustig Y, Sapir E, Regev-Yochay G, Cohen C, Fluss R, Olmer L, et al. BNT162b2 COVID-19 vaccine and correlates of humoral immune responses and dynamics: a prospective, single-centre, longitudinal cohort study in health-care workers. Lancet Respir Med. (2021) 9:999–1009. doi: 10.1016/S2213-2600(21)00220-4
18. Krammer F, Srivastava K, Alshammary H, Amoako AA, Awawda MH, Beach KF, et al. Antibody responses in seropositive persons after a single dose of SARS-CoV-2 mRNA vaccine. N Engl J Med. (2021) 384:1372–4. doi: 10.1056/NEJMc2101667
19. Walsh EE, Frenck RW Jr, Falsey AR, Kitchin N, Absalon J, Gurtman A, et al. Safety and immunogenicity of two RNA-based covid-19 vaccine candidates. N Engl J Med. (2020) 383:2439–50. doi: 10.1056/NEJMoa2027906
20. Shachor-Meyouhas Y, Hussein K, Szwarcwort-Cohen M, Weissman A, Mekel M, Dabaja-Younis H, et al. Single BNT162b2 vaccine dose produces seroconversion in under 60 s cohort. Vaccine. (2021) 39:6902–6. doi: 10.1016/j.vaccine.2021.10.016
21. Olbrich L, Castelletti N, Schälte Y, Garí M, Pütz P, Bakuli A, et al. Head-to-head evaluation of seven different seroassays including direct viral neutralisation in a representative cohort for SARS-CoV-2. J Gen Virol. (2021) 102:001653. doi: 10.1099/jgv.0.001653
22. Poljak M, Oštrbenk Valenčak A, Štamol T, Seme K. Head-to-head comparison of two rapid high-throughput automated electrochemiluminescence immunoassays targeting total antibodies to the SARS-CoV-2 nucleoprotein and spike protein receptor binding domain. J Clin Virol. (2021) 137:104784. doi: 10.1016/j.jcv.2021.104784
23. Kannenberg J, Schnurra C, Reiners N, Henschler R, Buhmann R, Kaiser T, et al. Sensitivity of SARS-CoV-2 antibody tests with late convalescent sera. J Clin Virol Plus. (2021) 1:100038. doi: 10.1016/j.jcvp.2021.100038
24. Vaselli NM, Hungerford D, Shenton B, Khashkhusha A, Cunliffe NA, French N. The seroprevalence of SARS-CoV-2 during the first wave in Europe 2020: a systematic review. PLoS ONE. (2021) 16:e0250541. doi: 10.1371/journal.pone.0250541
25. Bergeri I, Whelan M, Ware H, Subissi L, Nardone A, Lewis HC, et al. Global epidemiology of SARS-CoV-2 infection: a systematic review and meta-analysis of standardized population-based seroprevalence studies, Jan 2020-Oct 2021. medRxiv [preprint]. (2021). doi: 10.1101/2021.12.14.21267791
26. Knabl L, Mitra T, Kimpel J, Rössler A, Volland A, Walser A, et al. High SARS-CoV-2 seroprevalence in children and adults in the Austrian ski resort of Ischgl. Commun Med (London). (2021) 1:4. doi: 10.1038/s43856-021-00007-1
27. Medizinische Universität Wien,. Antikörperprevalenz. (2020). Available online at: https://www.meduniwien.ac.at/web/en/ueber-uns/news/detailseite/2020/news-im-dezember-2020/47-der-oesterreichischen-bevoelkerung-hatten-mitte/ende-oktober-2020-antikoerper-gegen-SARS-CoV-2/ (accessed November, 2021).
28. Kerbl R, Strenger V, Bernar B, Zurl C, Simma B. “Corona Task Force” der Österreichischen Gesellschaft für Kinder- und Jugendheilkunde (ÖGKJ). SARS-CoV-2-Seroprävalenz in Österreich. Die Situation vor der Omikronwelle [SARS-CoV-2 seroprevalence in Austria. The situation before the omicron wave]. Monatsschr Kinderheilkd. (2022) 170:487–9. doi: 10.1007/s00112-022-01491-y
29. Zhang H, Wu Y, He Y, Liu X, Liu M, Tang Y, et al. Age-related risk factors and complications of patients with COVID-19: a population-based retrospective study. Front Med (Lausanne). (2022) 8:757459. doi: 10.3389/fmed.2021.757459
30. Cordero-Franco HF, De La Garza-Salinas LH, Gomez-Garcia S, Moreno-Cuevas JE, Vargas-Villarreal J, González-Salazar F. Risk factors for SARS-CoV-2 infection, pneumonia, intubation, and death in northeast mexico. front public health. (2021) 9:645739. doi: 10.3389/fpubh.2021.645739
31. Herrera-Esposito D, de Los Campos G. Age-specific rate of severe and critical SARS-CoV-2 infections estimated with multi-country seroprevalence studies. BMC Infect Dis. (2022) 22:311. doi: 10.1186/s12879-022-07262-0
32. Poletti P, Tirani M, Cereda D, Trentini F, Guzzetta G, Marziano V, et al. Age-specific SARS-CoV-2 infection fatality ratio and associated risk factors, Italy, February to April (2020). Euro Surveill. (2020) 25:2001383. doi: 10.2807/1560-7917.ES.2020.25.31.2001383
33. Weisberg SP, Connors TJ, Zhu Y, Baldwin MR, Lin WH, Wontakal S, et al. Distinct antibody responses to SARS-CoV-2 in children and adults across the COVID-19 clinical spectrum. Nat Immunol. (2021) 22:25–31. doi: 10.1038/s41590-020-00826-9
34. Schlickeiser S, Schwarz T, Steiner S, Wittke K, Al Besher N, Meyer O, et al. Disease severity, fever, age, and sex correlate with SARS-CoV-2 neutralizing antibody responses. Front Immunol. (2021) 11:628971. doi: 10.3389/fimmu.2020.628971
35. Klein SL, Pekosz A, Park HS, Ursin RL, Shapiro JR, Benner SE, et al. Sex, age, and hospitalization drive antibody responses in a COVID-19 convalescent plasma donor population. J Clin Invest. (2020) 130:6141–50. doi: 10.1172/JCI142004
36. Zhang B, Zhou X, Zhu C, Song Y, Feng F, Qiu Y, et al. Immune phenotyping based on the neutrophil-to-lymphocyte ratio and igg level predicts disease severity and outcome for patients with COVID-19. Front Mol Biosci. (2020) 7:157. doi: 10.3389/fmolb.2020.00157
37. Zhao J, Yuan Q, Wang H, Liu W, Liao X, Su Y, et al. Antibody responses to SARS-CoV-2 in patients with novel Coronavirus Disease (2019). Clin Infect Dis. (2020) 71:2027–34. doi: 10.1093/cid/ciaa344
38. Anichini G, Terrosi C, Gandolfo C, Gori Savellini G, Fabrizi S, Miceli GB, et al. SARS-CoV-2 antibody response in persons with past natural infection. N Engl J Med. (2021) 385:90–2. doi: 10.1056/NEJMc2103825
39. Manisty C, Otter AD, Treibel TA, McKnight Á, Altmann DM, Brooks T, et al. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet. (2021) 397:1057–8. doi: 10.1016/S0140-6736(21)00501-8
40. Prendecki M, Clarke C, Brown J, Cox A, Gleeson S, Guckian M, et al. Effect of previous SARS-CoV-2 infection on humoral and T-cell responses to single-dose BNT162b2 vaccine. Lancet. (2021) 397:1178–81. doi: 10.1016/S0140-6736(21)00502-X
41. Stamatatos L, Czartoski J, Wan YH, Homad LJ, Rubin V, Glantz H, et al. mRNA vaccination boosts cross-variant neutralizing antibodies elicited by SARS-CoV-2 infection. Science. (2021) 372:1413–8. doi: 10.1126/science.abg9175
42. Ebinger JE, Fert-Bober J, Printsev I, Wu M, Sun N, Prostko JC, et al. Antibody responses to the BNT162b2 mRNA vaccine in individuals previously infected with SARS-CoV-2. Nat Med. (2021) 27:981–4. doi: 10.1038/s41591-021-01325-6
43. Goel RR, Apostolidis SA, Painter MM, Mathew D, Pattekar A, Kuthuru O, et al. Distinct antibody and memory B cell responses in SARS-CoV-2 naïve and recovered individuals following mRNA vaccination. Sci Immunol. (2021) 6:eabi6950. doi: 10.1126/sciimmunol.abi6950
44. Saadat S, Rikhtegaran Tehrani Z, Logue J, Newman M, Frieman MB, Harris AD, et al. Binding and neutralization antibody titers after a single vaccine dose in health care workers previously infected with SARS-CoV-2. JAMA. (2021) 325:1467–9. doi: 10.1001/jama.2021.3341
45. Reynolds CJ, Pade C, Gibbons JM, Butler DK, Otter AD, Menacho K, et al. Prior SARS-CoV-2 infection rescues B and T cell responses to variants after first vaccine dose. Science. (2021) 372:1418–23. doi: 10.1126/science.abh1282
46. Allen N, Brady M, Ni Riain U, Conlon N, Domegan L, Carrion Martin AI, et al. Prevalence of antibodies to SARS-CoV-2 following natural infection and vaccination in Irish hospital healthcare workers: changing epidemiology as the pandemic progresses. Front Med (Lausanne). (2022) 8:758118. doi: 10.3389/fmed.2021.758118
47. Krutikov M, Palmer T, Tut G, Fuller C, Azmi B, Giddings R, et al. Prevalence and duration of detectable SARS-CoV-2 nucleocapsid antibodies in staff and residents of long-term care facilities over the first year of the pandemic (VIVALDI study): prospective cohort study in England. Lancet Healthy Longev. (2022) 3:e13–21. doi: 10.1016/S2666-7568(21)00282-8
48. Gonçalves J, Sousa RL, Jacinto MJ, Silva DA, Paula F, Sousa R, et al. Evaluating SARS-CoV-2 seroconversion following relieve of confinement measures. Front Med (Lausanne). (2020) 7:603996. doi: 10.3389/fmed.2020.603996
49. Siller A, Seekircher L, Wachter GA, Astl M, Tschiderer L, Pfeifer B, et al. Seroprevalence, waning and correlates of anti-SARS-CoV-2 igg antibodies in tyrol, austria: large-scale study of 35,193 blood donors conducted between June 2020 and September 2021. Viruses. (2022) 14:568. doi: 10.3390/v14030568
50. AGES Österreichische Agentur für Gesundheit und Ernährungssicherheit GmbH,. Dashboard COVID-19. (2020). Available online at: https://covid19-dashboard.ages.at/. (accessed March, 2021).
Keywords: seroprevalence, SARS-CoV-2, vaccination, Comirnaty, undocumented infection, seropositivity, anti-N, beta
Citation: Willeit P, Kimpel J, Winner H, Harthaller T, Schäfer H, Bante D, Falkensammer B, Rössler A, Riepler L, Ower C, Sacher M, von Laer D and Borena W (2022) Seroprevalence of SARS-CoV-2 infection in the Tyrolean district of Schwaz at the time of the rapid mass vaccination in March 2021 following B.1.351-variant outbreak. Front. Public Health 10:989337. doi: 10.3389/fpubh.2022.989337
Received: 08 July 2022; Accepted: 17 August 2022;
Published: 09 September 2022.
Edited by:
Nuno Sepulveda, Warsaw University of Technology, PolandReviewed by:
Helena Soares, New University of Lisbon, PortugalCopyright © 2022 Willeit, Kimpel, Winner, Harthaller, Schäfer, Bante, Falkensammer, Rössler, Riepler, Ower, Sacher, von Laer and Borena. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wegene Borena, d2VnZW5lLmJvcmVuYUBpLW1lZC5hYy5hdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.