 Khwaja Mir Islam Saeed
Khwaja Mir Islam Saeed Narges Neyazi
Narges Neyazi Khushal Nabizada4
Khushal Nabizada4
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 17 November 2022
Sec. Disaster and Emergency Medicine
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.983197
This article is part of the Research Topic Health in Afghanistan: Some Insights from Socio-epidemiological Research View all 5 articles
COVID-19 pandemic disrupted the social and economic norms. Knowledge, Attitude and Practices studies are used to address the information gap for further strategic decision making to control the pandemic. This study aimed to find the level of Knowledge, Awareness, Attitudes, and behavioral practices of the people of Afghanistan about the COVID-19 and its impact on health and socio-economic dimension of their routine lives. We used a cross-sectional method with two stage sampling design. Data analysis was performed using SPSS v.20. The survey focused on adults including men and women all over the country to represent the country, including the urban and rural areas. Most of the respondents are in the age group of 21–30 years (46.5%); 60.15% of the participants are married. Almost 75% of females and 84% of males were literate and most participants have a bachelor's degree (34%). More than 80% of participants knew they can prevent themselves from contacting COVID-19 through hand washing frequently with soap and water and wearing a mask. More than 80% of participants responded that they would go for a lab test for detection of the virus as well as COVID-19 vaccination if it is available. Almost 35% reported always wearing a mask to prevent COVID-19 transmission; more than half of participants always wash their hands, more than 60% of them do not touch their eyes, nose, and mouth frequently. Nearly 60% of participants indicated that their household had problems satisfying food needs partly during the COVID-19 pandemic. Nearly half of participants believed that the government was successful in applying lockdown measures and in awareness rising (56.8 and 69.8%). The study findings provide some useful insight about the KAP of communities in Afghanistan, which could assist policy makers in public health to design and implement interventions based on the information gaps reported.
Coronavirus disease 2019 (COVID-19) is an emerged respiratory disease which is high infectious. On January 30, 2020, the WHO announced the outbreak as the Public Health Emergency of International Concern (PHEIC) (1), which later in March 2020, it was propagated as a pandemic. From the start of pandemic, five variants of concern (VOCs) of COVID-19 have been recognized in the world (Alpha, Beta, Gamma, Delta, and Omicron) (2). As of June 5, 2022, over 529 million confirmed cases and more than six million deaths globally have been reported. Based on WHO COVID-19 status report, only Alpha and Delta variants of COVID-19 were reported as of 26 June 2022 in Afghanistan (3) with a cumulative 182,352 cases and 7,722 deaths reported on 30 June 2022 (4).
Like other pandemics in the history, this pandemic also resulted in interruption of social and economic norms. Many studies were conducted to find out about these disruptions in the world (5–8). These studies assessed the level of Knowledge, Attitudes, Perceptions of selected populations and how the economy of people affected by the pandemic. To address the information gap for strategic decision making, a series of KAP studies were planned and implemented in Afghanistan too (9–11). Afghanistan, with a fragile health system, low economy and continuing conflicts has been more vulnerable to the pandemics. While the insufficient technical expertise and lab capacity to diagnose and treat the COVID-19 cases toughen up the severe effect of pandemic, health authorities declared that the actual number of positive cases could be higher than the numbers reported officially in the country (12). To control the pandemic, partial movement restrictions followed by bans on mass gathering and school closing were implemented in the country (13) which negatively affected the economic situation and worsened the poverty level in the country.
The level of Knowledge, Attitudes, and Practices (KAP) towards the disease affect the community practices and compliances with preventive measures. Having information on community perspectives regarding COVID-19 is crucial and will contribute to informed decision making, policy development and revision of risk communication and community engagement strategy by health authorities to fight against current and future pandemics.
In this study, we aimed to find the level of Knowledge, Awareness, Attitudes, and behavioral practices of the people in Afghanistan about COVID-19 and its impact on health and socio-economic dimension of their routine lives.
A cross-sectional study using a two-stage sampling design was conducted to provide information for addressing the overall purpose and specific objectives of the survey. The survey focused on adults (over the age of 18) including men and women all over the country to represent the country, including the urban and rural areas. The data was collected at community level by randomly approaching the households and interviewing the head of the family. All 34 provinces were included in the survey and data collection was completed within 3 months from February to April 2021 in the field. Persons who did not have consent and pregnant women were excluded from the study. Trained surveyors from the Afghanistan Institute of Strategic Studies (AISS) were given an orientation on how to collect data using a face-to-face structured questionnaire.
For sample size calculations, key factors such as acceptable margin of error, desired level of confidence of the survey results, estimated baseline levels of the indicators, design effect of the sampling methodology, and anticipated non-response rate, were taken into consideration. The sample size of the KAP survey was calculated by considering a 5% margin of error, 95% confidence level, and 35% of the reference indicator. Due to cluster sampling, the design effect was assumed to 1.5. So, if we multiply 350 by 1.5, it will be 525. A response rate of 90% was assumed to participate. For the anticipated response rate of 90%, the current sample come to (525 *1.11) 583 in each region. As the survey was planned to represent regional and national data, the sample was multiplied by five and finally the total sample size came to 2,915 households in 34 provinces. The sample size for each province was calculated based on its proportion to size. There was a two-stage cluster design; in the first stage, five districts were selected randomly by simple random sampling methods; in the second stage two areas were selected within each district.
The research team developed a questionnaire containing seven sections: (1) general information, (2) Knowledge, (3) Attitude, (4) Practices, (5) socio-economic impact of COVID-19 on people lives, (6) the channels through which people receive information on COVID-19 and (7) the people's satisfaction on the government's response to COVID-19 pandemic. Most of the questions were designed based on a Likert scale to be answered. The answer options were selected based on the literature review and extracted from similar studies. The data collectors obtained the consent orally from the participants.
Data was collected using a face-to-face structured questionnaire by trained interviewers in the target areas. The team were consisting of two male and female interviewers supervised and monitored by a group of staff in Kabul and other provinces. After briefing the survey team, the pilot testing was conducted in the field and the tool was tested and improved. The study population consisted of a men and women in age group of 18 years and older who agreed to be interviewed in the study. However, severely ill, and pregnant women who are not able to be interviewed were excluded. The AISS team regularly supervised the process of the survey including recruitment of staff, training, and fieldwork to avoid any deviation. The questionnaires were distributed to participants who were literate and for those who were illiterate, the questions and answer options were read loudly by interviewers. The AISS team was responsible to timely execution of all activities including monitoring and quality assurance of field work. Each data collector entered the data into the excel sheet. A data entry clerk based in Kabul then cleaned, and edited the data, and entered them in an excel database.
A data entry clerk based in Kabul conducted data quality check before analysis, and it was cleaned and validated in the Kabul AISS office. Data analysis was performed using SPSS v.20. Descriptive statistics were performed to calculate the proportions, rates, and ratios, which were used to prepare graphs and tables for better visualization of data. Frequencies of correct knowledge answers and various attitudes and practices were described. The statistical report is comprised of cross-tabulations of selected study variables representing knowledge (one question, have you heard about COVID-19/Coronavirus?), attitude (one question, if there is community transmission of COVID-19, will you participate in meetings, religious activities, events, and other social gatherings or any crowded place in areas?), and practices (two questions, do you wear mask to prevent and control COVID-19 transmission? And do you wash hands to prevent and control COVID-19 transmission?) as well as the demographic characteristics of respondents (residency place, gender, marital status, literacy, education, and income; Tables 1–3). We used Chi-Square to test bivariate relationships of study variables across the different background variables. Chi-Square test is used to test the relationship between a qualitative dependent variable and a qualitative independent variable. P < 0.05 was considered of statistical significance.
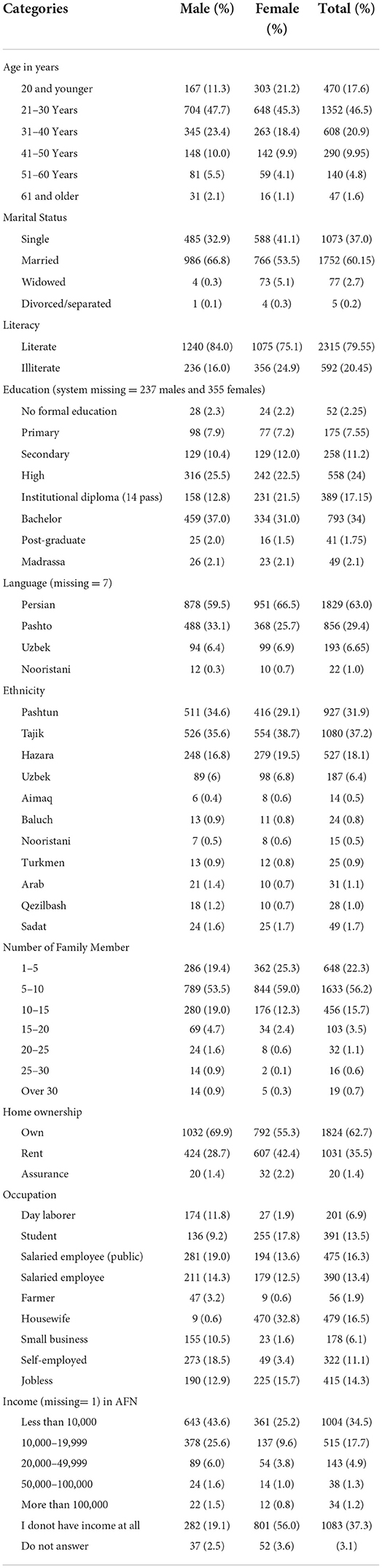
Table 1. Frequency distribution of the background characteristics of study participants (N = 2907).
The study protocol was approved by Institutional Review Board (IRB) of Ministry of Public Health. The purpose of the survey was explained to all participants and informed consent from the interviewees was obtained. Each participant was informed that participation is voluntary, and they are free to withdraw of study at any time without any responsibilities. Participant confidentiality was maintained throughout the study. Data were entered into the database anonymously using the assigned identification numbers.
2907 respondents from 34 provinces of Afghanistan, with maximum rate (16.6%) from Kabul province and the minimum rate (0.6%) from Nimroz province completed the survey. The differences are due to population proportion living in these provinces. Almost 82% of participants in this study live in urban areas and the remaining (18%) live in rural areas. However, it should be noted that the study was mostly implemented in urban settings and due to existing insecurity, we had only 18% of data collection from rural areas.
As shown in Figure 1, most participants were from regional provinces such as Kabul, Balkh, Nangarhar, Herat and Kandahar. The lowest participation was from, Nooristan, Panjshir and Nimroz provinces.
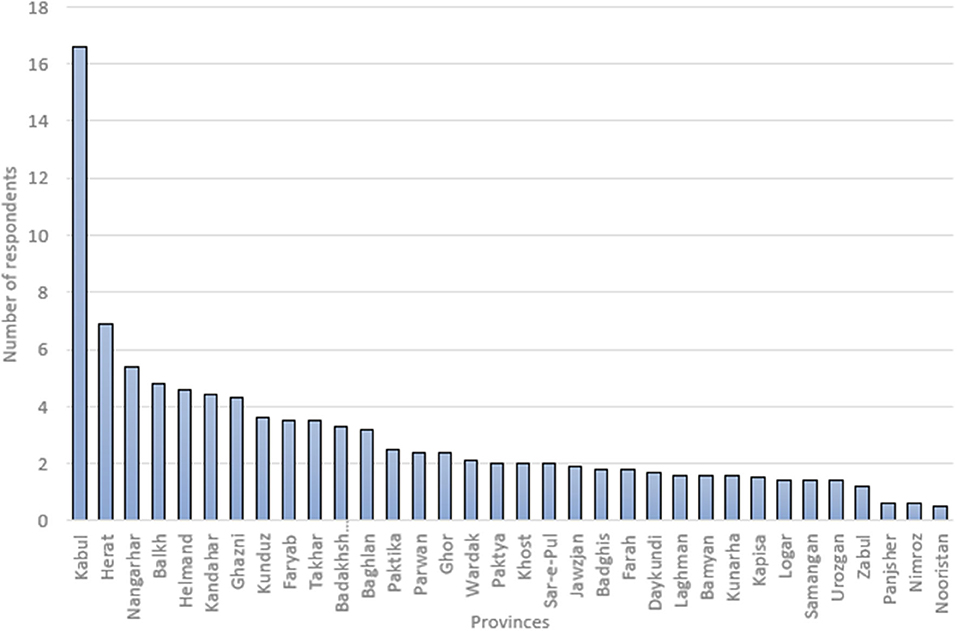
Figure 1. Proportion of respondents per province in KAP survey.
The socioeconomic and background characteristics of respondents are reflected in Table 1. As seen, most of the respondents are in the age group of 21–30 years (46.5%); 60.15% of the participants are married. Almost 75% of females and 84% of males were literate and almost one third of participants have a bachelor's degree (34%). Nearly 63% of participants speak in Dari, 29.4% speak in Pashto and the remaining speak in Uzbek, Nooristani and other languages. Most participants were Pashtun and Tajik (69.1%). Most of respondents owned their home (62.7%). One third of the female participants were housewives (32.8%); and the majority of the male participants were salaried employees (33.3%). More than half of the females did not have an income at all and nearly half of males had an income of less than 10,000 AFN (Afghani) monthly. It should be noted that the proportion of males (50.8%) and females (49.2%) were almost equal in this study. The highest number of family members were less than five people living under one ceiling.
As reflected in Table 2, almost all the participants have heard about the Coronavirus. They believed that COVID-19 spreads via contact with droplets from an infected person, including cough (62.8%), going to crowded areas (59.6%), touching surfaces that someone infected has touched/cough on (49.5%), normal talking (43.3%), and by eating and drinking (38.4%) respectively. The subjects responded that fever (77.1%), cough (66.5%), headache (66.4%), sore throat (57.4%), and shortness of breath (57.7%) were the symptoms of COVID-19. More than three fourths of the participants believed that people who donot have the signs and symptoms of the COVID-19 can spread the disease. More than 80% of participants knew they can prevent themselves from contacting COVID-19 through hand washing frequently with soap and water and wearing a mask, and more than half of participants believed in the effectiveness of other measures such as avoiding close contact with those who are sneezing and coughing; avoiding handshakes, hugging, and kissing; avoiding going to crowded areas; and keeping physical distance. More than half of the respondents believed that suspected people with COVID-19 should be kept in quarantine for 2 weeks. Almost 41% of people who participated in this study believed that there (during period of this study) is an effective treatment available for COVID-19, and more than half (59.7%) believed that there is an effective vaccine available for this disease. Nearly 22% of participants did not know about any effective treatment and vaccine availability for COVID-19 during data collection. The participants responded that the elderly, people with hypertension, cardiovascular diseases, and suppressed immunity are the major populations who are at most risk for developing sever illness from COVID-19. A chi-square test of independence was performed to examine the relation between the demographic characteristics of participants and the level of their knowledge. As Table 3 shown, there is a significant relation between knowledge about COVID-19 and gender (X = 6.987, p = 0.008), marital status (X = 20.108, p = 0.000), literacy (X = 34.317, p = 0.000), education (X = 19.227, p = 0.008), and income (X = 28.955, p = 0.002).
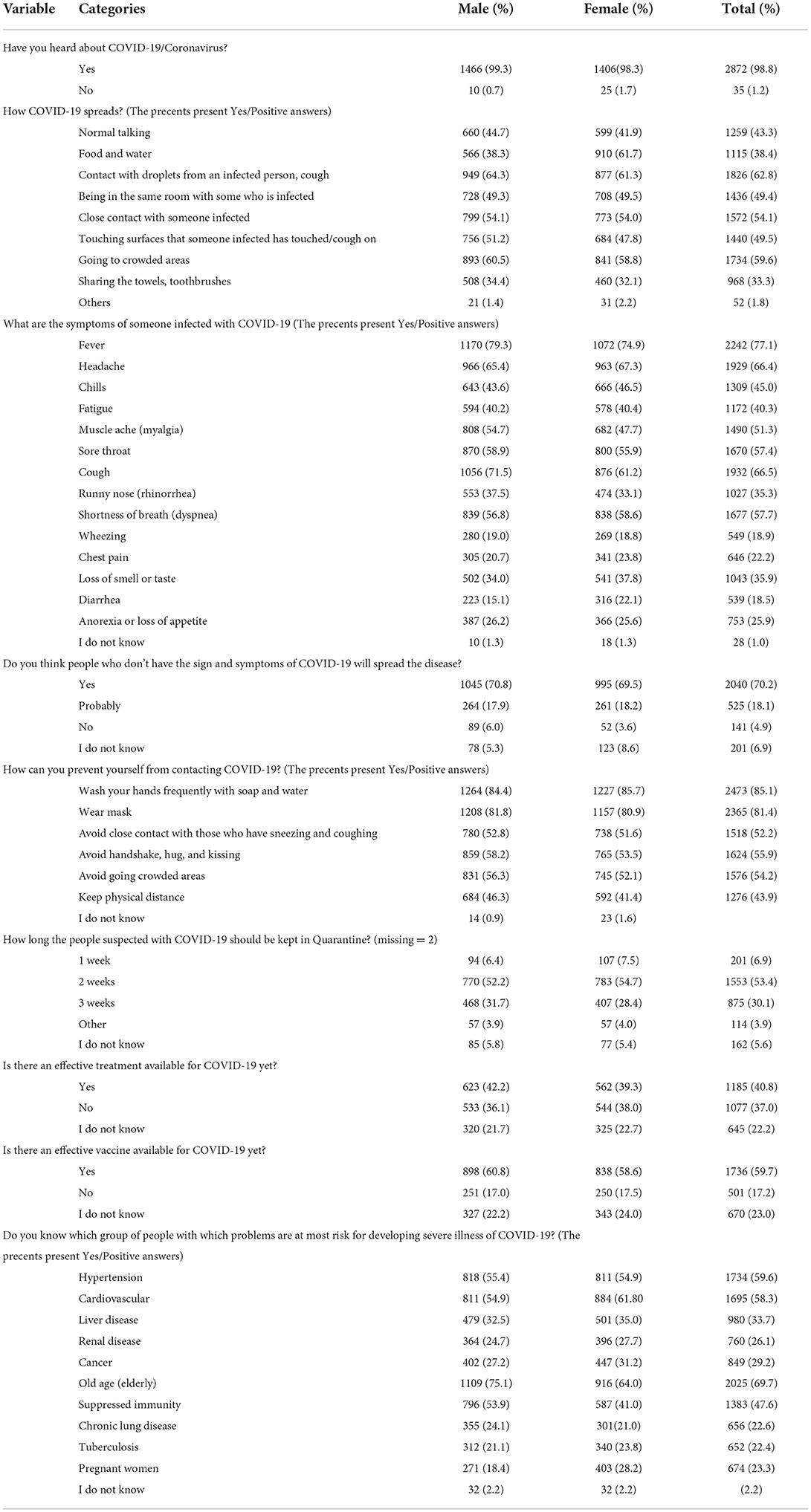
Table 2. Frequency distribution on knowledge of participant (N = 2907).
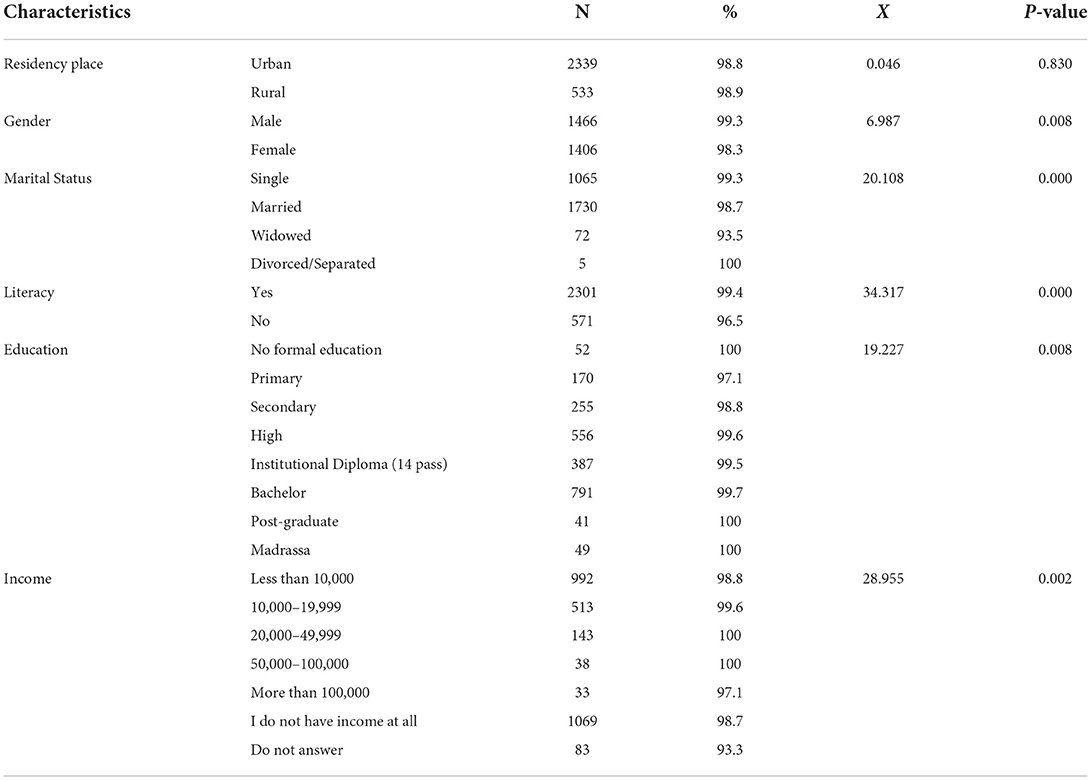
Table 3. Knowledge score of COVID-19 by demographic characteristics.
The attitude related responses of participants are summarized in Table 4. As reflected in this Table more than half of the participants believed that the risk and threat of COVID-19 disease is very high. Also, nearly half of the participants believed that they have not contracted COVID-19 yet. More than 80% of participants responded that they would go for a lab test for detection of the virus as well as COVID-19 vaccination if it is available. Almost 67% of participants reported that they will not go to meetings, religious activities, big events, other social gathering, or any crowded places if a community transmission of COVID-19 exists. Most respondents were neutral or disagreed with this idea that there is no COVID-19 virus, and it is just a story devised by profit seeking companies and individuals. But nearly half of the participants believed that COVID-19 is a clear indication of the Almighty Allah's anger on wrong doers or committing sins. The relation between the attitude of participants and their demographic characteristics also was examined using a chi-square test. As Table 5 shown, there is a relation only between the gender (X = 18,610, p = 0.000) and the attitude of the participants but not between the participant's attitudes and residence place, marital status, literacy, education and income. It means the attitude toward COVID-19 is different between two genders and females had more positive attitude toward COVID-19 in this study.
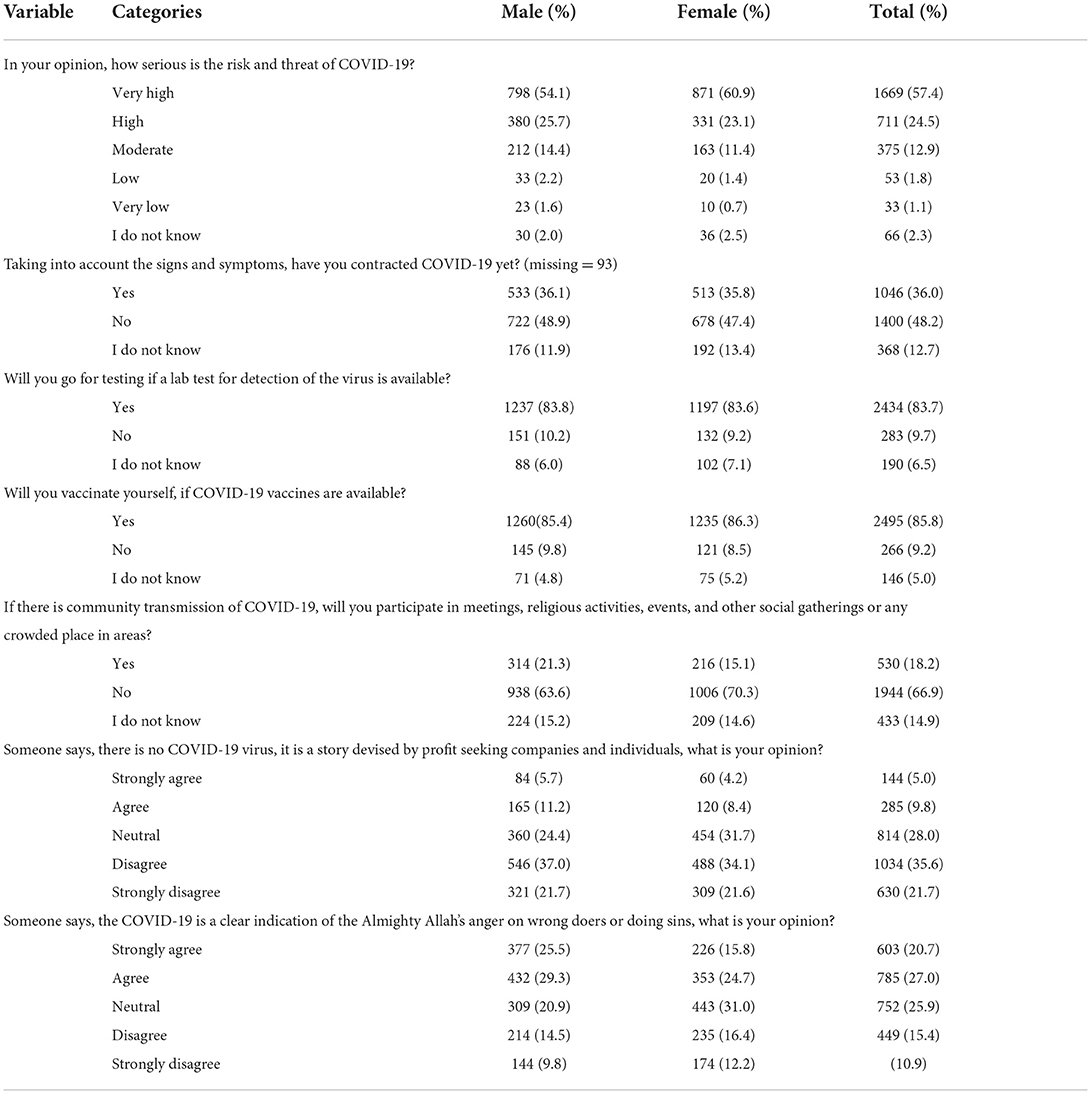
Table 4. Frequency distribution on attitudes of participants toward COVID-19 disease (N = 2907).
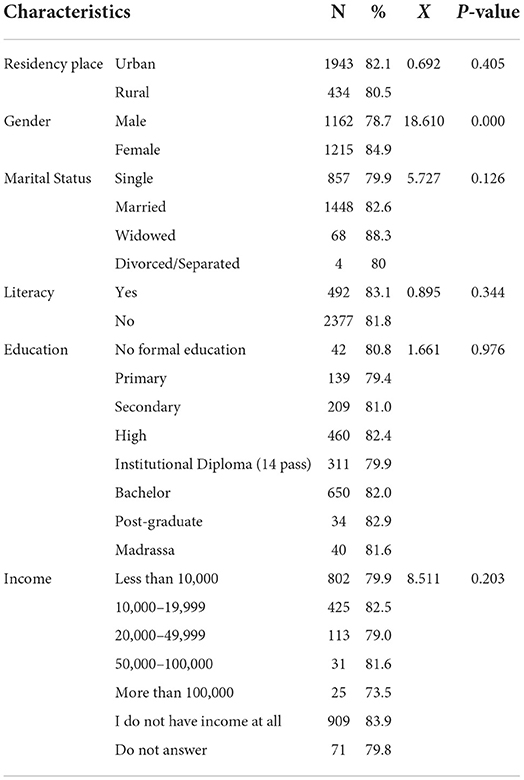
Table 5. Attitude score of COVID-19 by demographic characteristics.
According to the results of this study almost 35% reported always wearing a mask to prevent COVID-19 transmission; more than half of participants always wash their hands, more than 60% of them do not touch their eyes, nose, and mouth frequently. The majority kept the physical/social distancing by remaining 2 m away from each other's, nearly half of participants cover their nose and mouth during coughing or sneezing with the elbow or a tissue and then throw the tissue away, and the majority often listen to and follow the directions of their health authorities. Most of the participants said that they or their family will call a doctor or go to a doctor's office or a hospital if they have been infected or if they have some of the common COVID-19's symptoms (84.6%), but most of the respondents prefer and trust governmental health facilities (60.5%). Meanwhile, in the case of a COVID-19 positive test, more than half of participants will stay home and self-isolate. In addition, nearly 40% of participants said that they will rarely or never participate in communal prayers, funerals, and celebrations such as Eid, or go to friend's houses or to work during the COVID-19 pandemic (Table 6). We chose two main indicators (wearing mask and washing hands) to find out the relation between the practice and demographic characteristics. As Table 7 shows, the practice of wearing mask has relation with residency place (people living in urban wear mask more than rural people), gender (female used mask more than male), marital status, literacy rate (literate people used mask more than illiterate people), and education level. As shown, the income level has no relation with using mask in this study. Also, our study shows that washing hands has relation with residency place (people in urban area wash their hands more), gender, marital status, education, and income level.
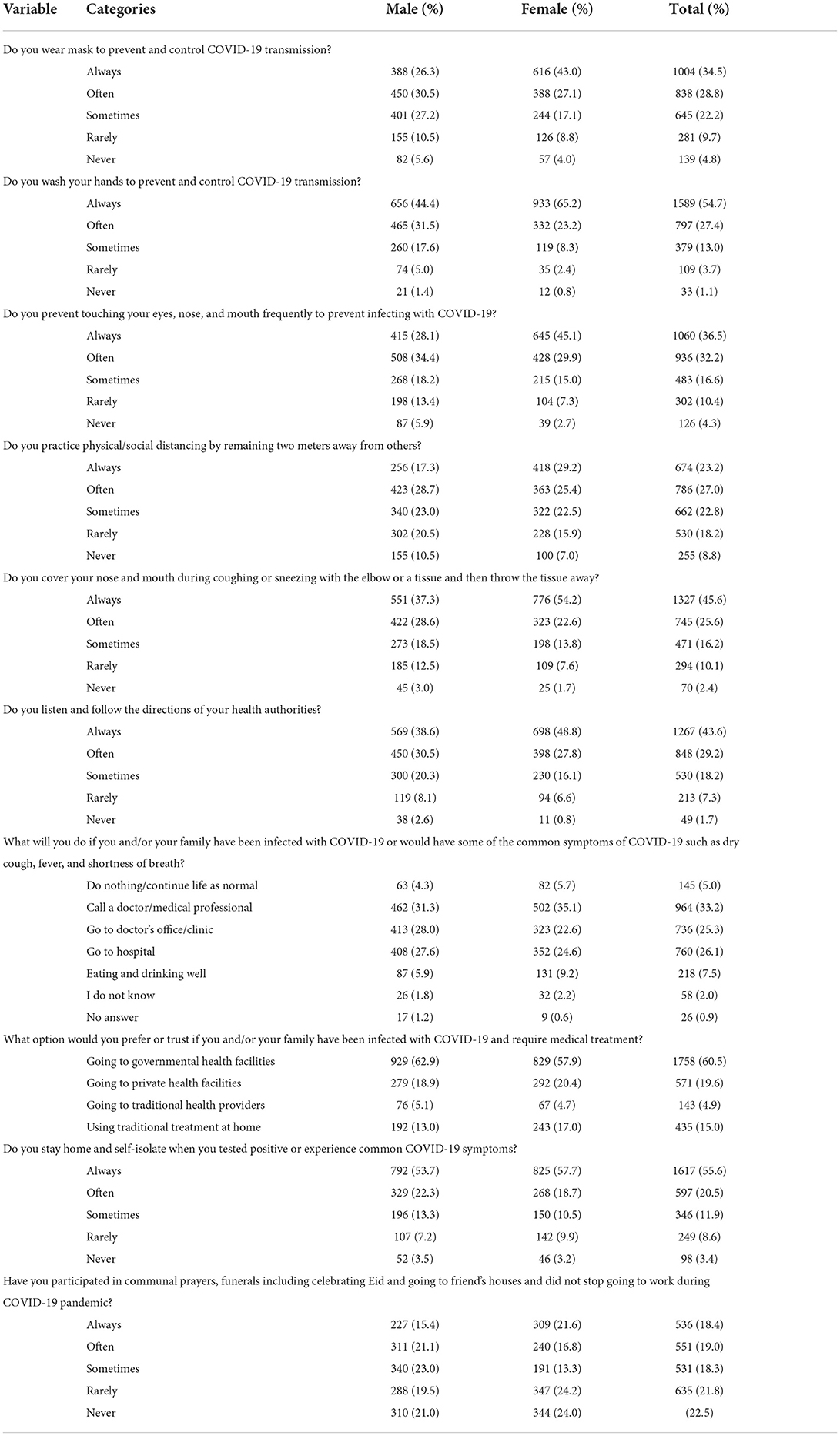
Table 6. Frequency distribution on practices of participants toward COVID-19 disease (N = 2907).
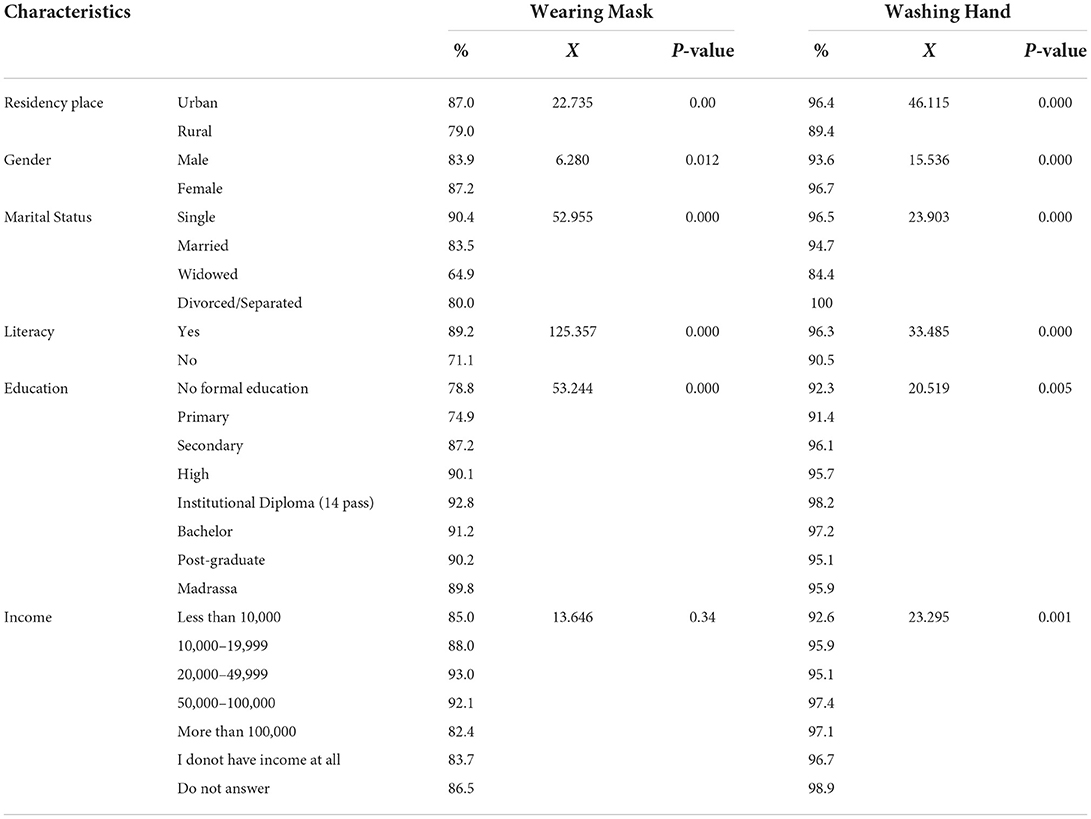
Table 7. Practice score of COVID-19 by demographic characteristics.
Nearly 60% of participants indicated that their household had problems satisfying food needs partly during the COVID-19 pandemic. Moreover, the majority (82.5%) stated that they applied for food rations during the lockdown. Most of the participants had to seek financial assistance and loans from their friends, relatives, colleagues, and communities (47.9%) during the lockdown. However, the majority also could afford to buy masks, disinfectants, and medicine when they were prescribed during COVID-19 pandemic. Almost 44% of participants stated that they lost part of their source of income in the mentioned period. This study shows that 45.3% of participant's families have students who faced problems in following their education during the pandemic period; the majority also believed that the COVID-19 pandemic caused an increase in the level of violence at family and/or in the community (Table 8).
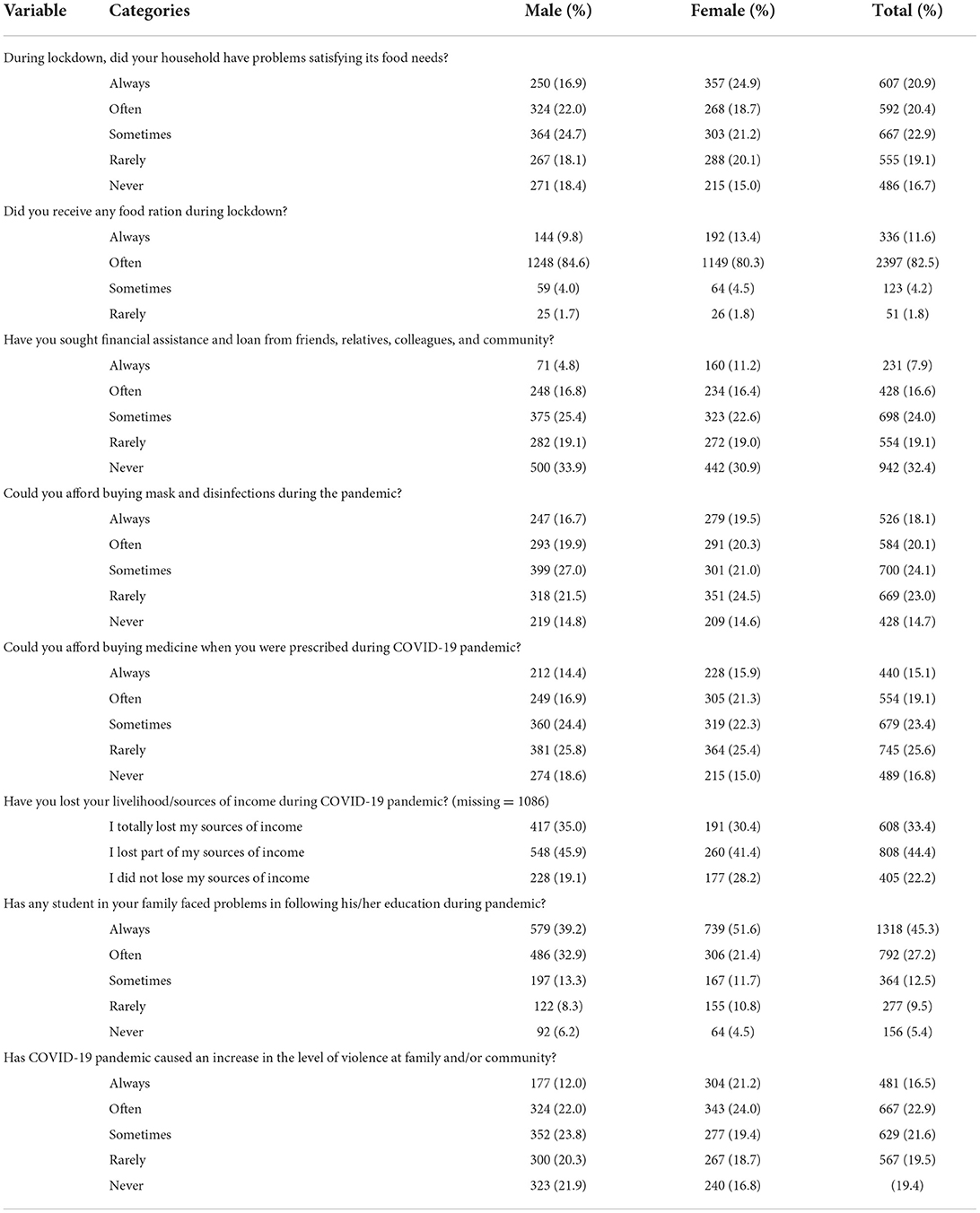
Table 8. Frequency distribution on socio-economic Impact of COVID-19 pandemic (N = 2907).
Table 9 indicates the frequency distribution of the source of information of respondents about the COVID-19 pandemic. It reflects that 90.2% of participants have a mobile and more than half of them have access to internet sometimes. Most of the respondents also have radio and television in their home (60.0% and 82.9% respectively) and listen to the radio and watch TV often. The participants heard about COVID-19 mainly through television (67.8%); social media (42.3%); radio (35.1%); and health facility staff (32.7%). However, they mostly trust television (62.6%) and health facility staff (48.1%).
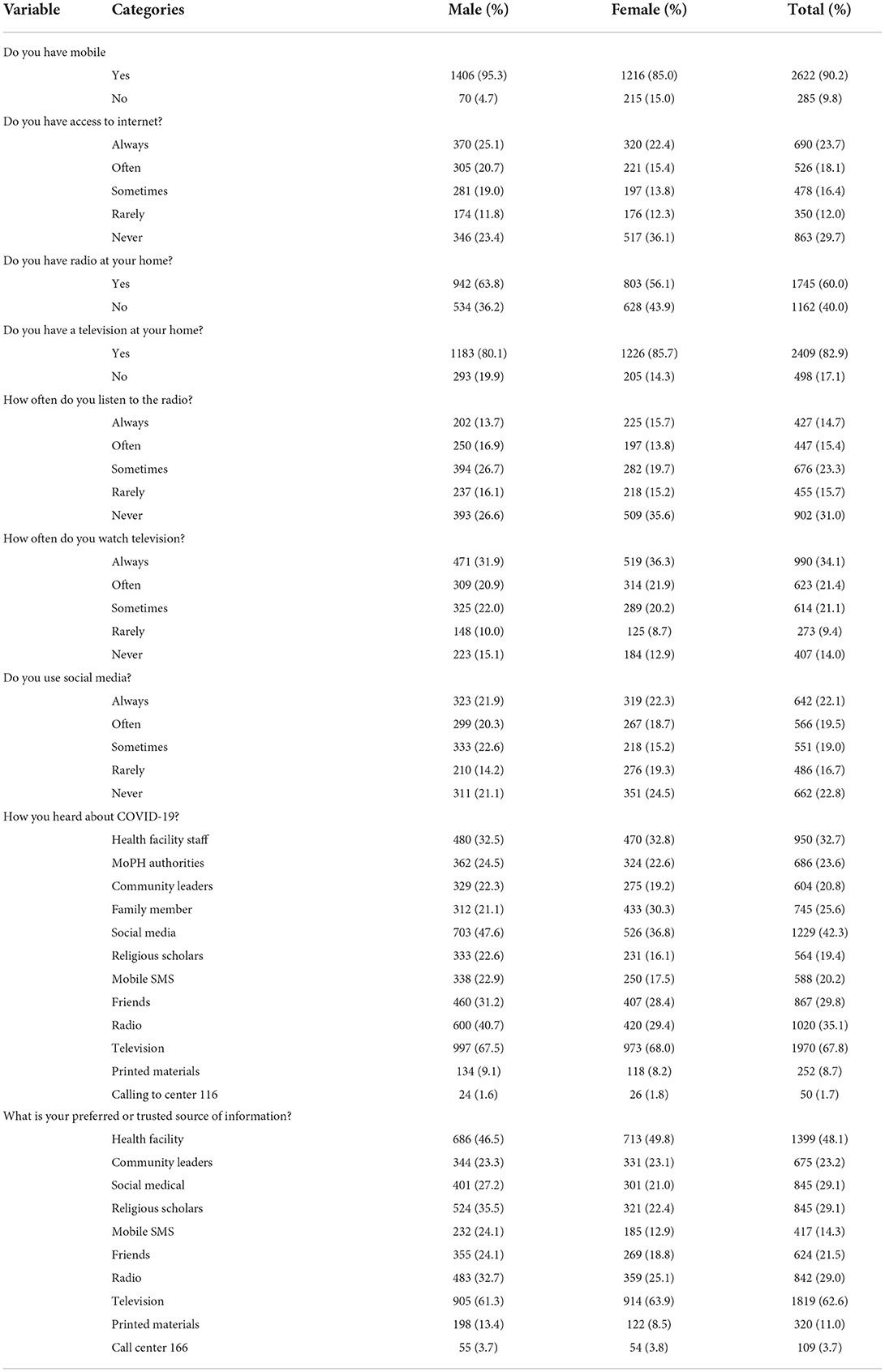
Table 9. Frequency distribution of source of information about COVID-19 (N = 2907).
Nearly half of participants believed that the government was successful in applying lockdown measures and in awareness rising (56.8% and 69.8%) during the COVID-19 pandemic in Afghanistan. Analysis showed that 44.2% of respondents believed that the government was/is successful in providing isolation centers in the mentioned period. However, most of them were not satisfied in terms of the provision of treatment services (49.7%), referral/ambulance services (50.2%), death management services (51.3%), or the provision of food and essential needs to poor families by the government (67.8%) during the pandemic, respectively (Table 10).
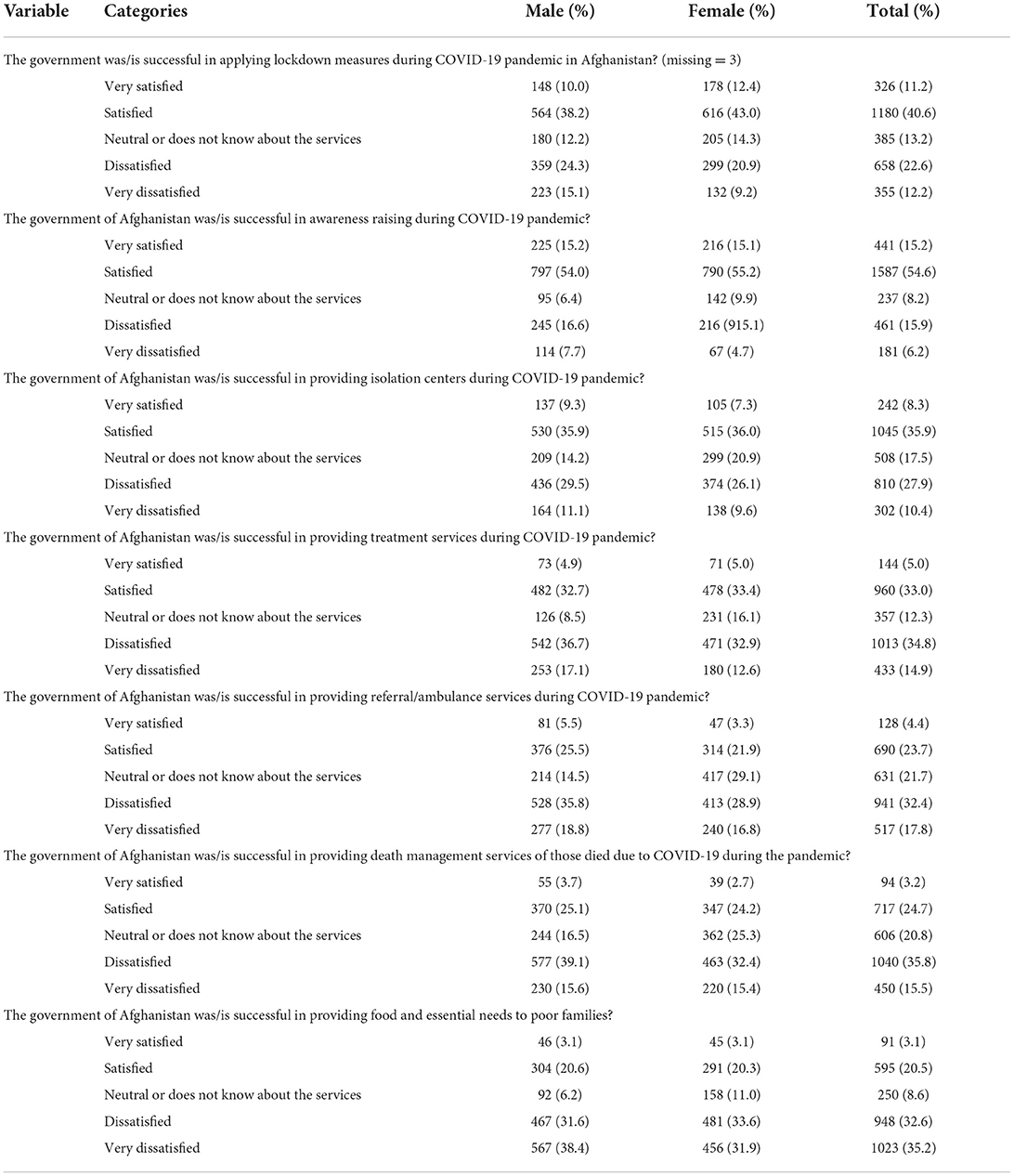
Table 10. Level of satisfaction from government by participants related to COVID-19 control and prevention (N = 2907).
Like other KAP surveys, this study was conducted to find the level of Knowledge, Attitudes, and Practices towards COVID-19, as well as the gaps and behavioral patterns among various subgroups in Afghan society. Using result of study effective public health interventions can be designed and implemented to improve the situation (14). This study was conducted almost one year after the detection and prevalence of the COVID-19 pandemic in Afghanistan; that is why the findings of this study reflected that the study participants had sufficient knowledge about COVID-19 all over the country. In addition, they knew adequately the modes of transmission of the virus through the respiratory droplets of infected people. Most respondents are literate with higher education which is certainly an important input for better knowledge and appropriate practices.
Furthermore, the respondents were able to correctly identify the signs and symptoms of the disease. This high level of knowledge about COVID-19 and its preventive measures shows that the campaigns and communications conducted by government have worked. Participants had knowledge and information about preventive measures such as hand washing, personal hygiene, cough hygiene, using a mask, and social distancing. These are similar with other studies' findings (15, 16) and 1 year of exposure to the pandemic could be the reason for this high level of knowledge on various aspects of the disease in the community. Although having knowledge directly affects the behavior of people, it is not easy to claim that a certain level of knowledge is sufficient to cause positive changes. However, it should be noted that the impact of knowledge on health behaviors has been investigated in various studies (17–19). Our study also showed that small portion of respondents believed on misconceptions caused by “infodemic”. WHO says “an infodemic is an overabundance of information, both online, and off line. It includes deliberate attempts to disseminate wrong information to undermine the public health response and advance alternative agendas of groups or individuals. Mis- and disinformation can be harmful to people's physical and mental health; increase stigmatization; threaten precious health gains; and lead to poor observance of public health measures, thus reducing their effectiveness and endangering countries' ability to stop the pandemic” (20). The infodemic has been a big challenge during the COVID-19 pandemic (21–23). Therefore, specific procedures should be followed to provide accurate information to neutralize myths and misguided information through the internet and social media. This is an important finding because during the implementation of this study, the vaccine was widely available and still effective treatment was not available for the disease. These are important points that should be focused on health education and promotion interventions.
In addition, most respondents believed that COVID-19 is a viral disease with some believing it could be Almighty Allah's anger on wrong doers or committers of sins. A similar expression was given by 60% of Muslim communities in Nigeria where it was perceived that the pandemic is due to God's punishment (24). This is an important point to be focused on by the government as well as religious leaders to discuss and develop interventions for betterment. Levels of knowledge about the source of infection, modes of transmission and ways of prevention are important findings in this study. Another important finding is the level of social distancing by respondents and listening to messages from health authorities. However, there is a big gap between having knowledge and the actual attitudes and practices of the community. Meaning that appropriate knowledge has not always influenced good attitude or practice. For instance, only one third of respondents reported wearing mask when needed and half of them wash their hands frequently. Two third are not touching their mouth, nose, and eyes. These are the areas for more focus in future sessions for risk communication.
The pandemic destroyed the socioeconomic status of the countries throughout the world. In Afghanistan, almost two third were negatively affected during mobility restriction last year limiting their ability to earn and provide food. The coping mechanisms such as applications of rations and seeking financial assistance and loans during lockdown were implemented by households. Almost half of participants stated that they had lost part of their source of income during the lockdown period. Furthermore, the prices of all goods and services were rising during restrictions/lockdowns, for sure it has affected the price of mask, sanitary material, and disinfectants. Such impact of pandemic has been recorded in other studies as well (25). The increased level of violence at home and the disturbance to the education of children are important points to be focused while implementing restriction of normal activities and other measures. As the majority had access to mobile, radio, TV and sometimes to internet facilities, the main sources of information were mostly radio and TV followed by social media and healthcare workers. However, the most trusted channels of information were television and healthcare staff. Therefore, the most high-ranking channels such as TV, radio and healthcare workers should be utilized for risk communication messages and community engagement. The government's level of success in response to this pandemic was assessed as satisfactory by half of respondents. The main reasons for failure of the health system were identified as poor treatment services, referral/ambulance services, death management services, or inadequate provision of food and essential needs to poor families. These are the main lessons to be learned for future waves of this pandemic as well as future emergencies. This study had few limitations which needs to be expressed. First, like all other studies, it was difficult to include and consider all related factors with respect to Knowledge, Attitudes, and Practices. In addition, although we designed the study to collect data from urban and rural setting, due to existing insecurity in rural areas, the study has been mostly implemented in urban settings (82% of the respondents) with good access to information and better socioeconomic status and the rural area, certainly with less access to key source of information as their counterparts, are missing. Therefore, the results would be generalizable nationally only to people living in urban setting.
The study findings provide some useful insight about the KAP of communities in Afghanistan, which could assist policy makers in public health to design and implement interventions based on the information gaps reported. Considering the findings of this study, the following recommendations are given:
• All stakeholders in controlling the COVID-19 pandemic can use the information from this KAP study to revise their risk communication strategies to control COVID-19 efficiently The government and public health authorities should establish and implement appropriate policies and interventions that are tailored to the level of understanding of communities. According to findings of our study, males and people living in urban areas, has good knowledge. In addition, based on our findings, illiterate people do not use mask or wash their hands to prevent getting infected with COVID-19. So, the health authorities should focus mostly on females and the illiterate population living in rural settings with proper strategies to enhance their knowledge and promote their practice toward controlling and preventing COVID-19 in their community.
• We recommend for further KAP study among population living in rural setting to fill the gap presented in our study and generate evidence for people living in rural areas.
• Public health officials should further enhance the knowledge of communities living in rural areas while considering the contextual factors which adversely affect the transfer of knowledge to behavior change such as some cultural and traditional related factors.
• Information about modes of transmission of the virus should be communicated clearly targeting all misconceptions and rumors. The survivors from COVID-19 and fully vaccinated individuals with high-risk behaviors should be encouraged to share their experiences as a point for mobilizations.
• Despite having good knowledge and attitudes, the health authorities should focus more on awareness campaigns at the community level. There are a wide range of channels to be used such as face-to-face health education, posters, billboards, social channels, radio, and TV advertisements to fill these practice gaps and improve the situation.
• There is a need for more relevant communication, and engagement of communities by local and religious leaders in the promotion of adherence to preventive measures. Religious leaders especially Mullahs from mosques should be enlightened about various aspects of the pandemic and its negative impacts because their advice and recommendation are sufficiently working in a sensitive and religious communities like Afghanistan.
• Information and health education (IEC) programs and behavior change communication interventions (BCC) in health promotion department of MoPH with respect to COVID-19 are important to maintain appropriate knowledge and improve positive practices by targeting people with low knowledge and education levels.
• A good level of coordination should be made between various parties involved in fighting the COVID-19 pandemic in Afghanistan, especially those organizations who reach to poor people and provide them with in-kind and financial assistance. Different international and national donors such as UN agencies (World Food Program, World Health Organizaion, UNICEF, UNDP), provincial governments, provincial public health directorates and the Ministry of Public Health should be the main members of this coordination.
• As the majority proportion of Afghanistan's population is below the age of 18 and can be the source of transmission for the COVID-19 virus, it is recommended that another KAP survey be conducted among the 7–18-year-old age group population (especially school students) to measure their Knowledge, Attitude, and Practices toward the COVID-19 pandemic.
• Simultaneously with emergence of different types of COVID-19 in the world as well as Afghanistan, the main actors in combating with this pandemic, especially the MoPH and other international stakeholders such as WHO should update the public on the signs and symptoms of each variant and the ways of preventing and treating it.
• Recent power transfer and change of government in Afghanistan also hit the health system hardly, a situation analysis through the rapid assessments, along with re-planning for combatting COVID-19 is highly recommended.
The original contributions presented in the study are included in the article/supplementary files, further inquiries can be directed to the corresponding author.
NN, KS, and KN designed the research and wrote the paper. NN analyzed the data and had primary responsibility for final content. All authors read and approved the final manuscript.
The funding for implementation of this study was granted by Open Society Foundation.
We received constructive comments from several distinguished scholars in different stages of this research. Without their contribution, this would not have been a comprehensive work. As a nationwide study, enumerators from all over the country have actively participated in the data collection process, in spite of existing COVID-19 threats in Afghanistan. They completed the data collection in a timely manner. Their efforts and contribution are much appreciated. After the report of the research was drafted, it was shared with distinguished experts for review. We owe a debt of thanks to Dr. Abdul Hafiz Rasooly, Dr. Mohammad Dauod Altaf, Health Emergency Officer (WHO); and Dr. Maisam Najafizada, Assistant Professor of Health Policy, Memorial University of Newfoundland for their time and honest suggestions in further improving the report. Special thanks also go to colleagues in the Afghanistan National Public Health Institute (ANPHI) and the Institutional Review Board (IRB) at the Ministry of Public Health of Afghanistan that reviewed and approved the protocol of this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wang FS, Zhang C. What to do next to control the 2019-nCoV epidemic? Lancet. (2020) 395:391–3. doi: 10.1016/S0140-6736(20)30300-7
2. WHO. Tracking SARS-CoV-2 variants. (2021). Available online at: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on December 23, 2021).
4. WHO. Health Emergency Dashboard. (2022). Available online at: https://covid19.who.int/region/emro/country/af (accessed June 30, 2022).
5. Pal R, Yadav U, Grover S, Saboo B, Verma A, Bhadada SK. Knowledge, attitudes, and practices towards COVID-19 among young adults with Type 1 Diabetes Mellitus amid the nationwide lockdown in India: A cross-sectional survey. Diab Res Clin Prac. (2020) 166:108344. doi: 10.1016/j.diabres.2020.108344
6. Saefi M, Fauzi A, Kristiana E, Adi WC, Muchson M, Setiawan ME, et al. Survey data of COVID-19- related knowledge, attitudes, and practices among Indonesian undergraduate students. Data Brief. (2020) 31:105855. doi: 10.1016/j.dib.2020.105855
7. Erfani A, Shahriarirad R, Ranjbar K, Mirahmadizadeh A, Moghadami M. Knowledge, attitude and practice toward the novel coronavirus (COVID-19) outbreak: a population-based survey in Iran. Bull world Health organ. 30:10–2471. doi: 10.2471/BLT.20.256651
8. Narayana G, Pradeepkumar B, Ramaiah JD, Jayasree TH, Yadav DL, Kumar BK. Knowledge, perception, and practices towards COVID-19 pandemic among general public of India: a cross-sectional online survey. Curr Med Res Prac. (2020) 10:153–9. doi: 10.1016/j.cmrp.2020.07.013
9. APEX Consulting. Knowledge, Attitude, Practice (KAP) and Perception Survey on COVID-19 With Residents of Afghanistan. Kabul (2020).
10. Hall S. COVID-19 in Afghanistan: Knowledge, Attitudes, Practices and implications. Kabul: Research Brief (2020).
11. Nemat A, Raufi N, Sediqi MF, Rasib AR, Asady A. Knowledge, attitudes, and practices of medical students regarding COVID-19 in Afghanistan: a cross-sectional study. Risk Manag Healthc Policy. (2021) 14:1491. doi: 10.2147/RMHP.S308039
12. Nemat A, Asady A, Raufi N, Zaki N, Ehsan E, Noor NA, et al. A Survey of the Healthcare Workers in Afghanistan during the COVID-19 pandemic. Am J Trop Med Hyg. (2020) 104:537. doi: 10.4269/ajtmh.20-1367
13. GARDA World. Afghanistan: Authorities Extend COVID-19 Lockdown in Kabul April 11/Update 3. Kabul (2020).
14. Papagiannis D, Malli F, Raptis DG, Papathanasiou IV, Fradelos EC, Daniil Z, et al. Assessment of knowledge, attitudes, and practices towards new coronavirus (SARS-CoV-2) of health care professionals in Greece before the outbreak period. Int J Environ Res Public Health. (2020) 17:4925. doi: 10.3390/ijerph17144925
15. Rugarabamu S, Ibrahim M, Byanaku A. Knowledge, attitudes, and practices (KAP) towards COVID-19: A quick online cross-sectional survey among Tanzanian residents. Medrxiv. (2020) 216:1–18. doi: 10.1101/2020.04.26.20080820
16. Qutob N, Awartani F. Knowledge, attitudes and practices (KAP) towards COVID-19 among Palestinians during the COVID-19 outbreak: A cross-sectional survey. PLoS One. (2021) 16:e0244925. doi: 10.1371/journal.pone.0244925
17. Lau LL, Hung N, Go DJ, Ferma J, Choi M, Dodd W, et al. Knowledge, attitudes and practices of COVID-19 among incomepoor households in the Philippines: A cross-sectional study. J Global Health. (2020) 10:011007. doi: 10.7189/jogh.10.011007
18. Jung M, Lin L, Viswanath K. Associations between health communication behaviors, neighborhood social capital, vaccine knowledge, and parents'H1N1 vaccination of their children. Vaccine. (2013) 31:4860–6. doi: 10.1016/j.vaccine.2013.07.068
19. Lee M, Kang BA, You M. Knowledge, attitudes, and practices (KAP) toward COVID-19: a cross-sectional study in South Korea. BMC Pub Health. (2021) 21:1–10. doi: 10.1186/s12889-021-10285-y
20. Ashrafi-Rizi H, Kazempour Z. Information typology in coronavirus (COVID-19) crisis; a commentary. Arch Acad Emerg Med. (2020) 8:e19
21. Zarocostas J. How to fight an infodemic. Lancet. (2020) 395:676. doi: 10.1016/S0140-6736(20)30461-X
23. Habib MA, Dayyab FM, Iliyasu G, Habib AG. Knowledge, attitude and practice survey of COVID-19 pandemic in Northern Nigeria. PLoS ONE. (2021) 16:e0245176. doi: 10.1371/journal.pone.0245176
24. Hmad T, Haroon MB, Hui J. Coronavirus Disease 2019 (COVID19) Pandemic and economic impact. PaK J Med Sci. (2020) 36:S73. doi: 10.12669/pjms.36.COVID19-S4.2638
Keywords: Afghanistan, KAP survey, COVID-19 pandemic, socio-economic effect, knowledge, practice, attitude
Citation: Saeed KMI, Neyazi N and Nabizada Kh (2022) Knowledge, attitudes, practice of people toward the COVID-19 pandemics, and its impact in Afghanistan. Front. Public Health 10:983197. doi: 10.3389/fpubh.2022.983197
Received: 30 June 2022; Accepted: 21 October 2022;
Published: 17 November 2022.
Edited by:
Stefanie Harsch, University of Education Freiburg, GermanyReviewed by:
Palwasha Anwari, University of London, United KingdomCopyright © 2022 Saeed, Neyazi and Nabizada. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Narges Neyazi, bmV5YXppbmFyZ2VzQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.