
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 13 September 2022
Sec. Aging and Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.982095
This article is part of the Research TopicInnovations in Older Adult Care and Health Service Management: A Focus on the Asia-Pacific RegionView all 15 articles
 Sabuj Kanti Mistry1,2,3,4*
Sabuj Kanti Mistry1,2,3,4* A. R. M. Mehrab Ali1
A. R. M. Mehrab Ali1 Uday Narayan Yadav2,5
Uday Narayan Yadav2,5 Md. Nazmul Huda1,6
Md. Nazmul Huda1,6 Md. Mahmudur Rahman7Manika Saha8Md. Ashfikur Rahman9
Md. Mahmudur Rahman7Manika Saha8Md. Ashfikur Rahman9 David Lim6,10Saruna Ghimire11
David Lim6,10Saruna Ghimire11The onset of the coronavirus disease (COVID-19) pandemic and its overwhelming physical and mental health burden can result in stigmatization toward the disease and those affected. This study aimed to measure the prevalence of COVID-19-related stigma and its associated factors among older people in Bangladesh. This cross-sectional study was conducted among 1,045 Bangladeshi older adults aged 60 years and above through telephone interviews in September 2021. The outcome was measured using an eight-point Stigma Scale, adapted to the Bengali language. Level of stigma was indicated by the cumulative score of the eight-items, ranging from 0 to 8, with a higher score indicating a higher level of stigma. On average, participants had stigmas on three of the eight items, and 62.6% had a high stigma score. The most prevalent stigmas were as follows: COVID-19 is a punishment from God (79.3%), patients with previous COVID-19 must be isolated (67.3%), and people infected with COVID-19 did not meet hygiene standards (63.9%). Participants who lived in rural areas (β: 0.67, 95% CI: 0.39 to 0.95) and who perceived needing additional care during the pandemic (β: 0.35, 95% CI: 0.09 to 0.60) had a higher average stigma score, whereas stigma scores were lower among unemployed/retired participants (β: −0.22, 95% CI: −0.45 to 0.00). The study findings suggest implementing interventions to raise awareness through appropriate health literacy interventions and mass media campaigns.
The novel coronavirus disease (COVID-19) pandemic is recognized as one of the biggest global public health challenges of the century. According to the Director-General of the World Health Organization, “Our greatest enemy right now is not the virus itself. It's fear, rumors, and stigma” (1). Stigma is an important public health issue because of its direct correlation with adverse physical and mental health (2). Furthermore, stigma creates constraints to access to health and social services, disrupts health-seeking behavior, and creates social discrimination, exclusion, mental distress, and violence (3). Stigma may lead to distress and can affect early detection and timely treatment (4). Delayed diagnosis is linked with prognostic deterioration of the disease among vulnerable groups such as the older population, facilitating the quick spread of the infection, and increasing disease severity and complications (5). Stigma is also closely related to discrimination and injustice (6).
Despite its strong relationship with adverse health consequences, historically, stigma has been prevalent during the peak of many infectious diseases, including HIV/AIDS, tuberculosis and COVID-19 (7). Several factors facilitate stigma, including the lack of awareness, misinformation, fake news, extreme fears, and anxiety about the diseases, which are widespread during the COVID-19 pandemic (8). Misconceptions about various aspects of the pandemics as well as fear of the disease further reinforce the stigma in societies (9, 10). In line with these, evidence suggests that facilitators of stigma are widespread. Studies from Jordan (11), Uganda (12), and Lebanon (13) found COVID-19-related stigma to be prevalent among the general population. Notably, these studies include younger adults, and there is scarce COVID-19-related stigma research among the older population. In a study from Ghana, patients with COVID-19 reported experiencing various forms of stigma, e.g., stereotyping, social exclusion, mockery, finger-pointing, and insults (14). In another study from Ghana, nearly half of the participants exhibited stigma and discriminatory tendencies toward COVID-19 survivors (15). In the study from Malaysia, COVID-19-recovered participants expressed experiencing being labeled and blamed by the people around them (16). For several reasons, mentioned in the following paragraph, we believe that the level of COVID-19 stigma would be higher among older adults, in general, and more especially among Bangladeshi older adults, which warrants a separate study. In resource-constraint countries, such as Bangladesh, some critical social factors, including poverty, poor living conditions, low illiteracy rates, ethnic disparity, age, and gender disparities, can make COVID-19-related stigma conditions more complicated than in other resource-rich countries (4, 17). In line with the international studies, stigma against specific groups, such as healthcare professional, returning migrant workers, and persons with a travel history from COVID-19 hotspot countries (18–21), was also observed in Bangladesh (22–24).
The population groups most vulnerable to stigma are those directly and indirectly affected by the disease or those highly susceptible to the infections (6). Evidence has already proved that older adults (the age group of 65 and above) are one of the most vulnerable groups impacted by the COVID-19 disease globally. Compared to other age groups, older adults are at increased risk of developing severe disease, requiring hospitalization, and dying from COVID-19. According to Kaiser Family Foundation (KFF) data, as of 19 September 2021, about 80% of COVID-19 deaths were among those aged 65 and above (25). Recent studies conducted among older Bangladeshi adults aged 60 years and above revealed significant misconceptions and an overwhelming fear of COVID-19 (9, 10). Bangladeshi older adults also faced difficulty in getting medicine and receiving COVID-19-related information during this pandemic (26). The literacy rate and access to health information, two important determinants of stigma, are low among Bangladeshi older adults (27). While all these characteristics suggest that stigmas can be higher among Bangladeshi older adults, there is no evidence from Bangladesh regarding the extent to which COVID-19-related stigmas are present among them. In this context, using an analytical approach, our paper investigates the level of stigma toward people with COVID-19 and its associated factors among older adults in Bangladesh.
This cross-sectional study was conducted remotely through telephone interviews in September 2021 by the Aureolin Research, Consultancy and Expertise Development (ARCED) Foundation. The primary challenge for this study was to develop a sampling frame to select the participants during the COVID-19 pandemic, and thus, we utilized a pre-established registry, developed through merging the contact information of households from 10 different community-based studies accomplished by Aureolin Research, Consultancy, and Expertise Development (ARCED) Foundation during 2016–2020, which included households from all eight administrative divisions of Bangladesh, as a sampling frame. Based on the population distribution of older adults by geography in Bangladesh, we adopted a probability proportionate to size (of the eight-division) approach to select older adults in each division (28). The inclusion criterion was the minimum age of 60 years. Considering 50% prevalence with a 5% margin of error, at the 95% level of confidence, 90% power of the test, and 95% response rate, a sample size of 1,096 was required. However, of the 1,096 eligible participants approached, 1,045 responded to the study with an overall response rate of approximately 95%.
Level of stigma was measured using the eight-item Stigma Scale, which was previously translated and validated in the Bengali language (11). Each item was nominally coded as a yes/no statement where a correct response scored 0 and each stigma scored 1. The cumulative of the eight items generated a stigma score for each participant. The cumulative score of the eight-items ranged from 0 to 8, with a higher score indicating a higher level of stigma. We further classified COVID-19-related stigma into low (if the stigma score was below the mean of the scale value, i.e., <4) or high (if the stigma score was equal to or higher than the mean of the scale value, i.e., ≥4). The scale is reliable among the study participants, as indicated by the high internal consistency (Cronbach's alpha 0.74).
Explanatory variables considered in this study were age (categorized as 60–69 and ≥70), sex (male/female), marital status (married/without partner), formal education (no/yes), family size ( ≤ 4 or >4), family income in Bangladeshi Taka (BDT) (<5,000, 5,000–10,000, >10,000), residence (urban/rural), current work arrangements (employed and unemployed/retired), living arrangements (living alone or with family), walking distance to the nearest health center (<30 /≥30 min), memory or concentration problems (no problem/low memory or concentration), the presence of prevalent non-communicable chronic conditions (yes/no), concerned about COVID-19 (not concerned/somewhat to very concern), overwhelmed by COVID-19 (hardly, sometimes/often), perceived to be at risk of COVID-19 (low risk/high), difficulty in obtaining food, medicine, routine medical care, and earning during COVID-19 (no/yes), perceived isolation (hardly, sometimes/often), frequency of communication with friends and family during COVID-19 (less than previous/same as previous), perceived that family members are non-responsive (yes/no), and that they required additional care during COVID-19 (yes/no). Self-reported information on pre-existing medical conditions, such as arthritis, hypertension, heart diseases, stroke, hypercholesterolemia, diabetes, chronic respiratory diseases, chronic kidney disease, and cancer, was collected.
A pre-tested semi-structured questionnaire was used to collect the information through a telephone interview. Data collection was accomplished electronically using SurveyCTO mobile app (https://www.surveycto.com/) by trained research assistants, who were recruited based on previous experience administering health surveys using the same electronic platform. The research assistants were trained extensively before the data collection through Zoom meetings.
The English version of the questionnaire was first translated into Bengali language and then back-translated to English by two researchers to ensure the contents' consistency. The questionnaire was then piloted among a small sample (n = 10) of older adults to refine the language in the final version. The tool used in the pilot study did not receive any corrections/suggestions from the participants in relation to the contents developed in the Bengali language.
The distribution of the variables was assessed through descriptive analysis. We used linear regression models to explore the factors associated with stigma. The initial model was run with all potential covariates, and then, using the backward elimination criteria with the Akaike information criterion (AIC), the variables for the final model were selected and executed. Adjusted beta-coefficient and associated 95% confidence interval (95% CI) were reported. We also performed the model diagnostics, such as normality of the residuals and multicollinearity using variance inflation factor (VIF). All analyses were performed using the statistical software package Stata (version 14.0).
Table 1 describes the sociodemographic and lifestyle characteristics of participants. A higher proportion of participants were aged 60–69 years (75.6%), male (59.3%), married (76.5%), without formal schooling (51.7%), from a family with more than four members (66.8%), with monthly family income between 5,000 and 10,000 BDT (44.9%), from rural areas (82.6%), unemployed/retired (61.1%), living with family members (94.9%), and residing <30 min of walking distance to the nearest health center (55.6%). Many participants also reported pre-existing non-communicable chronic conditions (57.2%). The majority of participants reported that they were concerned about (66.7%) and overwhelmed by (67.9%) COVID-19 but perceived themselves as at low risk of developing COVID-19 (72.7%). In total, 37.2% of the participants reported reduced communication during the pandemic, and many reported experiencing difficulties in obtaining food (50.3%) and earning money (72.3%). More than a quarter of the participants reported feeling isolated (31.3%) and perceived that they required additional care during the pandemic (26.3%), but their family members were non-responsive (29.4%).
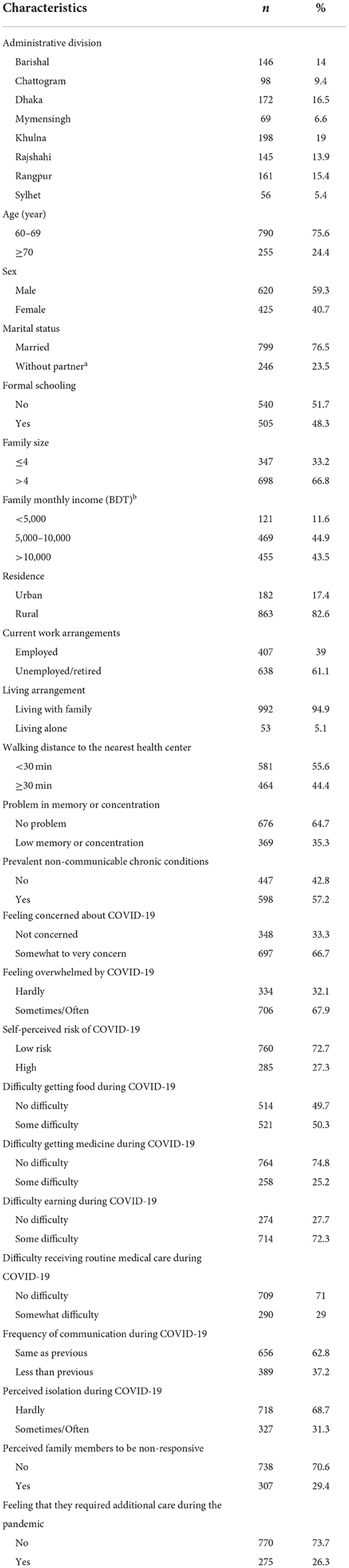
Table 1. Characteristics of the participants (N = 1,045).
Table 2 shows the prevalence of stigma related to COVID-19 among the participants. On average, participants had stigma on three items (mean stigma score = 2.97 and range 0–8). We found that 62.6% of the participants had a high level of stigma. The most prevalent stigmas were as follows: infection with COVID-19 is a punishment from God (79.3%), previous patients with COVID-19 have to be isolated (67.3%), people who were infected with COVID-19 did not meet the standards for hygiene (63.9%), it is unsafe to deal with people who have been infected with COVID-19 (62.4%), and people who have been infected with COVID-19 should expect some restrictions on their freedom (59.6%). Other less prevalent yet notable stigmas related to COVID-19 included: it should not be allowed to work for those who have been infected with COVID-19 (33.8%), to be friends with someone who has been infected with COVID-19 (27.3%), and those infected with COVID-19 should be ashamed of themselves (18.4%).
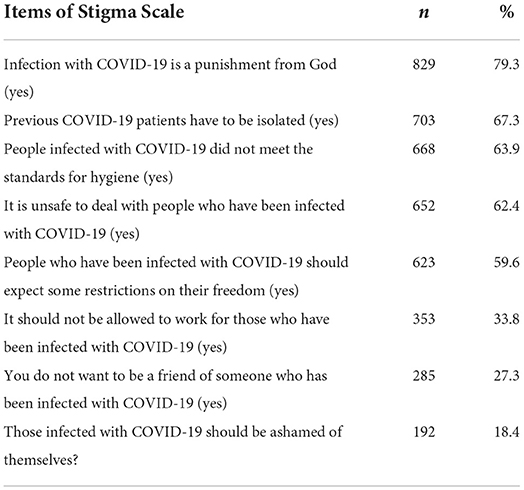
Table 2. Prevalence of stigma among the participants (N = 1,045).
An initial regression model was run with all the variables presented in Table 1, and a final model was executed with variables retained from the initial model based on the lowest AIC values. The result of the final model is presented in Table 3. The Q-Q plot of the residuals of the model shows that the data are normally distributed, whereas VIF values of <10 for each variable (Supplementary Tables S1, S2) suggest the absence of multicollinearity. In both adjusted and unadjusted analyses, residence and perception that they need additional care during the pandemic was associated with higher stigma score. In the adjusted analysis, participants who lived in rural areas had 0.67 units (β: 0.67, 95% CI: 0.39 to 0.95) higher stigma than those living in urban areas. Likewise, participants who felt that they required additional care during the pandemic had 0.35 unit higher stigma score (β: 0.35, 95% CI: 0.09 to 0.60) than those who did not feel so. On the other hand, stigma scores were 078 unit lower among unemployed/retired participants than those employed (β: −0.22, 95% CI: −0.45 to 0.00).
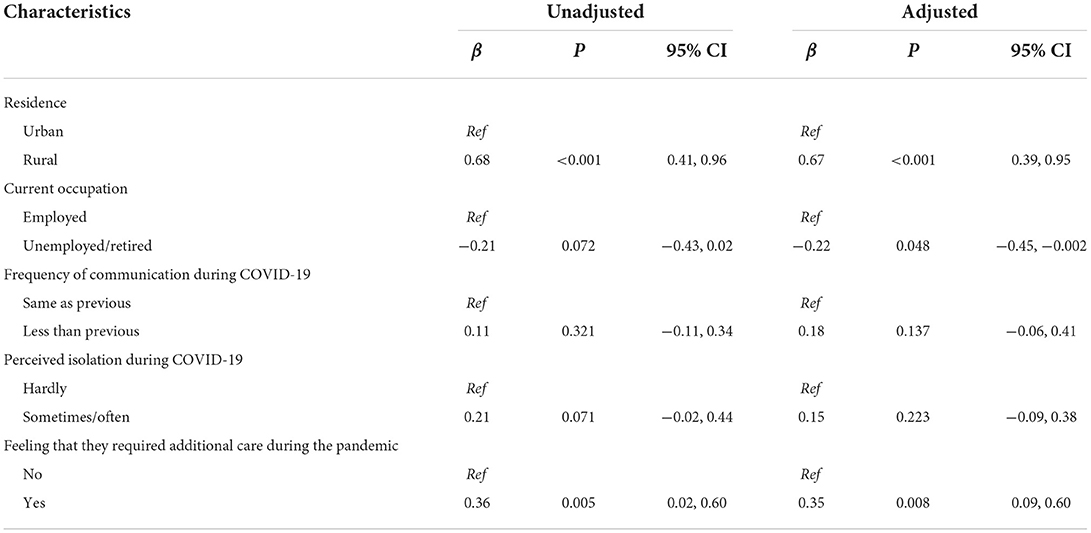
Table 3. Factors associated with stigma among the participants (N = 1,045).
This study assessed the COVID-19-related stigma and its associated factors among Bangladeshi older people. Overall, our study found a high prevalence of stigma among participants. Although we did not find any studies exploring COVID-19-related stigma among older adults in Bangladesh and worldwide, our findings are consistent with similar literature among younger people. Our findings are similar to studies among COVID-19 survivors (24–59 years) in Uganda (12), COVID-19-infected Jordanian people (18–65 years) (11), Lebanese adults (>18 years) (13), and Chinese adults (aged ≥18) living in the United States (8). These studies reported highly prevalent COVID-19-related stigma, ranging from 62 to 65%. Likewise, in two studies from Ghana, patients with COVID-19 reported experiencing stigma and discrimination (14, 15). In the study from Malaysia, COVID-19-recovered participants expressed experiencing being labeled and blamed by the people around them (16). While being novel among the older population, our study extends and supplements previous research among younger adults (8, 11–13) to enrich our understanding of COVID-19 stigma. Our study's finding may not be surprising and could be attributable to various factors. One potential reason for a high COVID-19-related stigma in older people in our study can be their limited literacy and inadequate understanding of the disease and how the SARS-CoV-2 virus is transmitted (11). Specifically, in Bangladesh, literacy rate is only 39.4% among older adults aged 65 years or above (29). Furthermore, given that the second wave of the COVID-19 pandemic was ongoing in Bangladesh during the data collection period, and COVID-19-related misinformation, fear, and panic may be other reasons for the observed stigma (30). As COVID-19-related mortality instigates fear and panic among individuals (8, 31), having family members, relatives, friends, colleagues, and neighbors die from the SARS-CoV-2 virus may be another reason for increasing COVID-19-related stigma (30). Irrespective of the reasons, prevalent stigma during the pandemic could threaten public health preventive measures. High COVID-19-related stigma may increase the risk of spreading the SARS-CoV-2 virus by delaying the early testing and detection of COVID-19, hampering individuals' health-seeking behaviors (32), and utilization of healthcare services (30). Furthermore, COVID-19-related stigma may increase individuals' psychological distress (12). Our findings suggest that it is vital to tailor interventions to this specific group of older people to reduce COVID-19-related prejudices and stigmas.
In our study, compared to urban residents, those living in rural areas in Bangladesh had a higher COVID-19-related stigma. Given that stigma is highly correlated with literacy and can be reduced with appropriate educational interventions (33), the wide gap in literacy rate between urban and rural Bangladesh (34) may explain this finding. Rural Bangladesh has a low literacy rate and limited access to health information (34). Studies have already shown that people with limited knowledge or education are more stigmatized than others (35). As such individuals with limited knowledge about COVID-19 transmission and prevention may have increased stereotypes and stigma related to the disease (36), additionally, they have limited awareness about the pandemic and increased fear of SARS-CoV-2 virus infection, which may further increase the likelihood of COVID-19-related stigma (37). Our finding highlighted the importance of providing older residents in rural areas of Bangladesh with appropriate knowledge about the prevention and transmission of COVID-19, which can potentially reduce COVID-19-related stigma among in the community.
In our study, stigma scores were also higher in the older adults who felt that they required additional care during the COVID-19 pandemic. No previously documented studies are available for cross-comparisons. The potential explanations for the finding could be attributed to personal insecurities amidst the pandemic. When a person is highly concerned about their inadequate medical support and care during COVID-19 and its consequence (e.g., possible deterioration of existing comorbidities, illness, death, etc.), mental trauma is likely to be high (38). Further, in the context of Bangladesh, where financial support from governmental and non-governmental organizations are limited (39) and financial and food insecurities are high, the COVID-19 pandemic has negatively impacted livelihood directly or indirectly (39). This disruption in household food supply and livelihood strategies may have exacerbated their fear and mental trauma (40). In addition, health facilities were disrupted, and routine medical care and medications were inaccessible in Bangladesh during the pandemic (26). Such concerns may have produced negative thoughts about COVID-19, leading to COVID-19-related stigma (30).
We also found that unemployed/retired participants had lower COVID-19-related stigma than those employed. We did not find any study in the literature to compare this finding with. The probable reason is that unemployed/retired older people mostly stay at home and get adequate time to read newspapers, watch live television news, and engage in interactions and communications with families, which can be a vital source of COVID-19 information (10). Furthermore, they are less fearful about the infection of COVID-19, given that their limited exposure at the workplace or outside of the home. Thus, they may be less fearful and less stigmatized against COVID-19 (30).
To the best of our knowledge, this is the first study that explored the level of COVID-19-related stigma and associated factors among older people in Bangladesh. However, the study has specific limitations. First, our research was cross-sectional in nature. Therefore, causality cannot be established. Second, our study is limited to quantitative analysis, as we did not explore the qualitative aspects of older people's COVID-19-related stigma.
Overall, we found that the prevalence of stigmas related to COVID-19 is high among the older population in Bangladesh, which has an implication for policy and practice in COVID-19 management and moving beyond the WHO's world goal of 70% fully vaccinated by mid-2022. It is important that policymakers and public health practitioners working in this space are cognizant of the prevalent stigma while designing and planning for mass media campaigns to inform, educate, and counter the stigma associated with COVID-19. Failure to consider the context for stigma may result in suboptimal reach and social exclusion of the people affected with COVID-19 in Bangladesh. Given the high level of COVID-19 stigma in rural areas of Bangladesh, initiatives should be directed toward this targeted population.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
The Institutional Review Board of the Institute of Health Economics, University of Dhaka, Bangladesh approved the study protocol (Ref: IHE/2020/1037). All participants enrolled in the study provided voluntary verbal informed consents.
SKM conceived and designed the study. MMR and SKM carried out the data analysis and interpretation of the result. SKM, AMA, UNY, MNH, MMR, MS, MAR, and DL contributed to the first draft of the manuscript. SG, UNY, DL, and MNH extensively edited the first draft to finalize. All authors approved the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.982095/full#supplementary-material
1. World Health Organization. WHO Director-General's Opening Remarks at the Media Briefing on COVID-19 - 28 February 2020. (2020). Available online at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-−28-february-2020 (accessed November 15, 2021).
2. Hatzenbuehler ML, Phelan JC, Link BG. Stigma as a fundamental cause of population health inequalities. Amer J Public Health. (2013) 103:813–21. doi: 10.2105/AJPH.2012.301069
3. Johnco C, Rapee RM. Depression literacy and stigma influence how parents perceive and respond to adolescent depressive symptoms. J Affect Disord. (2018) 241:599–607. doi: 10.1016/j.jad.2018.08.062
4. Roelen K, Ackley C, Boyce P, Farina N, Ripoll S. COVID-19 in LMICs: the need to place stigma front and centre to its response. Eur J Dev Res. (2020) 32:1592–612. doi: 10.1057/s41287-020-00316-6
5. Rong X, Yang L, Chu H, Fan M. Effect of delay in diagnosis on transmission of COVID-19. Math Biosci Eng. (2020) 17:2725–40. doi: 10.3934/mbe.2020149
6. Karamouzian M, Hategekimana C. Ebola treatment and prevention are not the only battles: understanding Ebola-related fear and stigma. Int J Health Policy Manag. (2015) 4:55–6. doi: 10.15171/ijhpm.2014.128
7. George LS, Rakesh PS, Vijayakumar K, Kunoor A, Kumar A. Social stigma associated with TB and HIV/AIDS among kudumbashree members: a crosssectional study. J Fam Med Prim Care. (2020) 9:4062–6. doi: 10.4103/jfmpc.jfmpc_437_20
8. Grivel MM, Lieff SA, Meltzer GY, Chang VW, Yang LH, Des Jarlais DC. Sociodemographic and behavioral factors associated with COVID-19 stigmatizing attitudes in the US. Stigma Health. (2021) 6:371. doi: 10.1037/sah0000345
9. Mistry SK, Ali ARMM, Akther F, Yadav UN, Harris MF. Exploring fear of COVID-19 and its correlates among older adults in Bangladesh. Glob Health. (2021) 17:47. doi: 10.1186/s12992-021-00698-0
10. Mistry SK, Ali ARMM, Yadav UN, Irfan NM, Rayamajhee B, Stanners MN. COVID-19 related misconceptions among older adults in Bangladesh: findings from a cross-sectional study. F1000 Res. (2021) 10:216. doi: 10.12688/f1000research.51597.1
11. Abuhammad S, Alzoubi KH, Khabour O. Fear of COVID-19 and stigmatization towards infected people among Jordanian people. Int J Clin Pract. (2021) 75:e13899. doi: 10.1111/ijcp.13899
12. Amir K. COVID-19 and its related stigma: a qualitative study among survivors in Kampala, Uganda. Stigma Health. (2021) 6:272–6. doi: 10.1037/sah0000325
13. Haddad C, Bou Malhab S, Malaeb D, Sacre H, Saadeh D, Mourtada V, et al. Stigma toward people with COVID-19 among the Lebanese population: a cross-sectional study of correlates and mediating effects. BMC Psychol. (2021) 9:164. doi: 10.1186/s40359-021-00646-y
14. Adom D, Mensah JA, Osei M. The psychological distress and mental health disorders from COVID-19 stigmatization in Ghana. Soc Sci Hum Open. (2021) 4:100186. doi: 10.1016/j.ssaho.2021.100186
15. Osei E, Amu H, Appiah PK, Amponsah SB, Danso E, Oppong S, et al. Stigma and discrimination tendencies towards COVID-19 survivors: evidence from a nationwide population-based survey in Ghana. PLOS Glob Public Health. (2022) 2:e0000307. doi: 10.1371/journal.pgph.0000307
16. Chew C-C, Lim X-J, Chang C-T, Rajan P, Nasir N, Low W-Y. Experiences of social stigma among patients tested positive for COVID-19 and their family members: a qualitative study. BMC Public Health. (2021) 21:1624. doi: 10.1186/s12889-021-11679-8
17. Logie CH, Turan JM. How do we balance tensions between COVID-19 public health responses and stigma mitigation? Learning from HIV research. AIDS Behav. (2020) 24:2003–6. doi: 10.1007/s10461-020-02856-8
18. Bhanot D, Singh T, Verma SK, Sharad S. Stigma and discrimination during COVID-19 pandemic. Front Public Health. (2021) 8:577018. doi: 10.3389/fpubh.2020.577018
19. The Indian Express. Delhi: Man Assaults Safdarjung Doctor, Sister, Accuses them of Spreading Virus. (2020). Available online at: https://indianexpress.com/article/cities/delhi/delhi-doctors-out-to-buy-fruit-assaulted-accused-of-spreading-coronavirus-6353862/ (accessed August 6, 2022).
20. The Times of India. Coronavirus: After Taali-Thaali, Health Workers Face Social Stigma. (2020). Available online at: https://timesofindia.indiatimes.com/india/coronavirus-after-taali-thaali-health-workers-face-social-stigma/articleshow/74801988.cms (accessed August 6, 2022).
21. The Guardian. Indian Doctors Being Evicted From Homes Over Coronavirus Fears. (2020). Available online at: https://www.theguardian.com/world/2020/mar/30/indian-doctors-being-evicted-from-homes-over-coronavirus-fears (accessed August 6, 2022).
22. Hennebry J, Hari KC. Quarantined! Xenophobia and Migrant Workers During the COVID-19 Pandemic. Geneva: International Organization for Migration (IOM) (2020).
23. Razu SR, Yasmin T, Arif TB, Islam M, Islam SMS, Gesesew HA, et al. Challenges faced by healthcare professionals during the COVID-19 pandemic: a qualitative inquiry from Bangladesh. Front Public Health. (2021) 9:647315. doi: 10.3389/fpubh.2021.647315
24. Sorkar MNI. COVID-19 Pandemic Profoundly Affects Bangladeshi Workers Abroad with Consequences for Origin Communities. Migration Information Source. MPI (2020).
25. KFF. COVID-19 Deaths Among Older Adults During the Delta Surge Were Higher in States with Lower Vaccination Rates. (2021). Available online at: https://www.kff.org/policy-watch/covid-19-deaths-among-older-adults-during-the-delta-surge-were-higher-in-states-with-lower-vaccination-rates/ (accessed November 20, 2021).
26. Mistry SK, Ali ARMM, Ahmed MS, Yadav UN, Khan MS, Hossain MB, et al. Prevalence and correlates of total sleep time among the older adults during COVID-19 pandemic in Bangladesh. Sleep Epidemiol. (2021) 1:100008. doi: 10.1016/j.sleepe.2021.100008
27. Rana AKMM, Wahlin Å, Lundborg CS, Kabir ZN. Impact of health education on health-related quality of life among elderly persons: results from a community-based intervention study in rural Bangladesh. Health Promot Int. (2009) 24:36–45. doi: 10.1093/heapro/dan042
28. BBS. Elderly Population in Bangladesh: Current Features and Future Perspectives. Dhaka: Bangladesh Bureau of Statistics, Ministry of Bangladesh, Government of Bangladesh (2015).
29. Trading Economics,. Bangladesh - Elderly Literacy Rate, Population 65+ Years, Both Sexes. (2022). Available online at: https://tradingeconomics.com/bangladesh/elderly-literacy-rate-population-65-years-both-sexes-percent-wb-data.html (accessed August 6, 2022).
30. Dye TD, Alcantara L, Siddiqi S, Barbosu M, Sharma S, Panko T, et al. Risk of COVID-19-related bullying, harassment and stigma among healthcare workers: an analytical cross-sectional global study. BMJ Open. (2020) 10:e046620. doi: 10.1136/bmjopen-2020-046620
31. Cho H, Li W, Cannon J, Lopez R, Song C. Testing three explanations for stigmatization of people of Asian descent during COVID-19: maladaptive coping, biased media use, or racial prejudice? Ethn Health. (2021) 26:94–109. doi: 10.1080/13557858.2020.1830035
32. Kamal A-HM, Huda MN, Dell CA, Hossain SZ, Ahmed SS. Translational strategies to control and prevent spread of COVID-19 in the Rohiynga refugee camps in Bangladesh. Glob Biosecur. (2020) 1:1–10. doi: 10.31646/gbio.77
33. Griffiths KM, Carron-Arthur B, Parsons A, Reid R. Effectiveness of programs for reducing the stigma associated with mental disorders. A meta-analysis of randomized controlled trials. World Psychiatry. (2014) 13:161–75. doi: 10.1002/wps.20129
34. Das S, Mia MN, Hanifi SMA, Hoque S, Bhuiya A. Health literacy in a community with low levels of education: findings from Chakaria, a rural area of Bangladesh. BMC Public Health. (2017) 17:203. doi: 10.1186/s12889-017-4097-y
35. Jiang T, Zhou X, Lin L, Pan Y, Zhong Y, Wang X, et al. COVID-19-related stigma and its influencing factors: a nationwide cross-sectional study during the early stage of the pandemic in China. BMJ Open. (2021) 11:e048983. doi: 10.1136/bmjopen-2021-048983
36. Islam A, Pakrashi D, Vlassopoulos M, Wang LC. Stigma and misconceptions in the time of the COVID-19 pandemic: a field experiment in India. Soc Sci Med. (2021) 278:113966. doi: 10.1016/j.socscimed.2021.113966
37. Schmidt T, Cloete A, Davids A, Makola L, Zondi N, Jantjies M. Myths, misconceptions, othering and stigmatizing responses to Covid-19 in South Africa: a rapid qualitative assessment. PLoS ONE. (2020) 15:e0244420. doi: 10.1371/journal.pone.0244420
38. Mistry SK, Ali ARMM, Yadav UN, Ghimire S, Hossain MB, Das Shuvo S, et al. Older adults with non-communicable chronic conditions and their health care access amid COVID-19 pandemic in Bangladesh: findings from a cross-sectional study. PLoS ONE. (2021) 16:e0255534. doi: 10.1371/journal.pone.0255534
39. Mandal SC, Boidya P, Haque MI-M, Hossain A, Shams Z, Mamun A-A. The impact of the COVID-19 pandemic on fish consumption and household food security in Dhaka city, Bangladesh. Glob Food Secur. (2021) 29:100526. doi: 10.1016/j.gfs.2021.100526
Keywords: stigma, COVID-19, older adults, aged, Bangladesh
Citation: Mistry SK, Ali ARMM, Yadav UN, Huda MN, Rahman MM, Saha M, Rahman MA, Lim D and Ghimire S (2022) Stigma toward people with COVID-19 among Bangladeshi older adults. Front. Public Health 10:982095. doi: 10.3389/fpubh.2022.982095
Received: 30 June 2022; Accepted: 08 August 2022;
Published: 13 September 2022.
Edited by:
Bijaya Kumar Padhi, Post Graduate Institute of Medical Education and Research, IndiaReviewed by:
Reham Shalaby, University of Alberta, CanadaCopyright © 2022 Mistry, Ali, Yadav, Huda, Rahman, Saha, Rahman, Lim and Ghimire. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabuj Kanti Mistry, c21pdHJhNDExQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.