 Lijing Ling
Lijing Ling Hua Yuan
Hua Yuan Jin Ma
Jin Ma
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 13 January 2023
Sec. Disaster and Emergency Medicine
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.979238
This article is part of the Research Topic Evaluation of Global Health, Disaster Response, and Humanitarian Projects and Programs View all 11 articles
Aim: The purpose of this study was to evaluate the effectiveness of the graded transport mode in the intrahospital transport (IHT) of critically ill patients.
Methods: This is a retrospective study, including 800 patients and categorized them into control and observation groups. The control group included 420 critically ill patients who were transported via conventional methods from our emergency resuscitation unit from June 2017 to December 2017. The observation group included 380 critically ill patients who were transported through a graded transport mode from January 2018 to June 2018. We performed intergroup comparisons of the incidence rates and causes of adverse events (AEs), transport time, length of stay, and mortality rate.
Results: The observation group had significantly lower transport time and AE incidence rates than the control group. However, no significant differences were observed in terms of the length of stay and mortality rate between the two groups.
Conclusion: The most notable merits of the graded transport mode in the IHT of critical care patients include the fact that it significantly reduces the incidence of AEs during IHT, shortens the transport time, and improves transport efficiency, thereby ensuring the safety of critically ill patients.
The emergency resuscitation room is the first admission unit for critically ill patients; patients whose condition does not improve after the initial evaluation and resuscitation need to be transported to appropriate departments for further diagnosis, examination, treatment, and hospitalization, known as intrahospital transport (IHT) (1). IHT exposes patients to a mobile environment and increases their susceptibility to the occurrence of adverse events (AEs). Severe AEs can exacerbate diseases and even endanger patient lives and are associated with significant mortality and increased healthcare costs. To ensure the timeliness and safety of IHT for these patients, standardization and optimization of the IHT process are urgently required (2, 3).
In recent years, graded transport mode, as a new IHT method, has been widely applied in Chinese hospitals. According to the severity of patients, the graded transport mode divides IHT into three risk levels, namely Grade I (high risk), Grade II (medium risk), and Grade III (low risk). However, the differences in transport time, length of hospital stay, and mortality between graded transport mode and traditional transport mode remain unknown.
In this study, we developed a new set of quality standards for IHT in critically ill patients. We aimed to explore whether the graded transport mode can effectively reduce the incidence of IHT related adverse events, shorten transport time and improve transport efficiency.
We collected critically ill patients admitted to the emergency department of our hospital from June 2017 to June 2018 and divided them into graded transport and traditional transport. We selected patients according to the following inclusion criteria: (1) critically ill patients admitted to the emergency resuscitation room requiring IHT owing to the need for CT and other imaging examinations, emergency interventions, emergency surgery, and hospitalization; (2) age > 18 years; (3) signed informed consent for the risk of transport obtained from the families of all patients; and (4) complete medical records. Exclusion criteria were pregnancy, infectious disease, hospital transfer, and patients with missing values.
Patients in the control group received conventional transport. After the attending physician assessed the patients' condition and permitted the transport, the families of the patients were involved in the transport process. In addition, emergency nurses and physicians carried respiratory support, resuscitation supplies, cardiac monitors, and other facilities for assistance.
Patients in the observation group received the graded transport. The steps of graded transport are as follows: (1) evaluation of transport risk grading: the transport risk grading is determined according to the patient's condition classification standard, and the corresponding medical staff, instruments, equipment and drugs are allocated according to different risk levels. Classification criteria are mainly referred to Vital Signs, Glasgow Coma Scale (GCS) score for consciousness state, Respiratory support, Circular support and primary clinical symptoms; (2) preparation before transport: the nurse in charge of transport must check the patient's physical status, equipment, drugs, etc., and fill in the form for graded transport; (3) transport: during the transport, the patient's physical condition and condition change must be observed at all times, ensure the safe placement and normal operation of medical equipment, prepare for emergency treatment, and try to avoid the occurrence of adverse events in transport; and (4) end of transport: the nurse in charge of transfer shall evaluate the situation of the patient after transfer and record the relevant contents of graded transport. Finally, the doctor in charge of the transfer and the doctor of the department receiving the patient jointly confirm the completion of the whole transfer process. Transport risk was categorized into Grades I, II, and III (from high to low), and the specific measures are presented in Tables 1, 2.
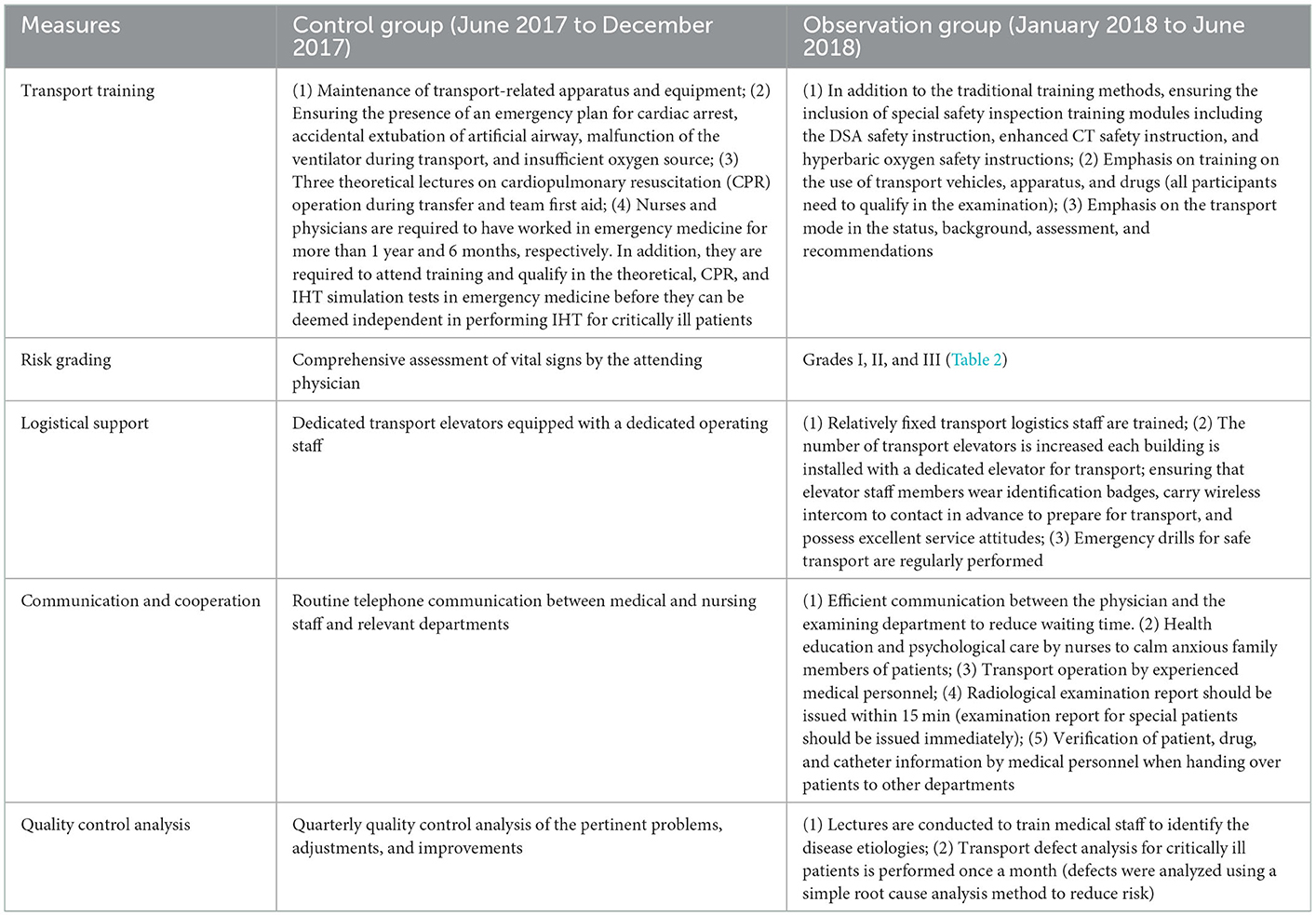
Table 1. Specific measures related to intrahospital transport for critically ill patients in the control and observation groups.
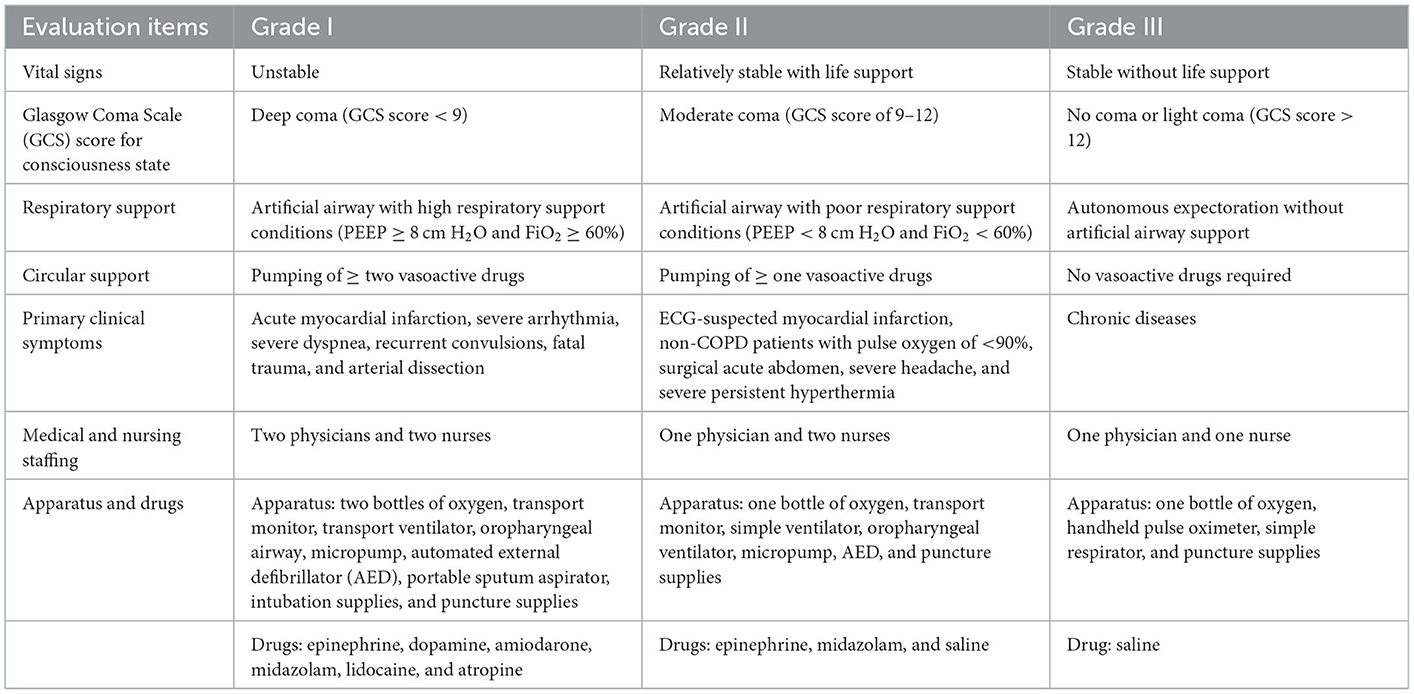
Table 2. Transport risk grading.
In both groups, the average transport time was calculated from the time the patients were transferred from the emergency resuscitation room by the medical staff till they returned to the hospital bed (or arrived at the relevant inpatient unit) after the examination or treatment was completed. The transport time only included the time spent during the transport process, excluding the examination, treatment, and patient handover processes. In addition, we performed intergroup comparisons of the incidence of AEs related to IHT, including the AEs related to the disease (sudden change of consciousness, increase or decrease in heart rate or blood pressure by > 20%, decrease of peripheral oxygen saturation by > 20 or < 90%, sudden cardiac arrest, and massive hemorrhage), personnel (tube dislodgement, displacement, and communication between the teams), and apparatus and drugs (apparatus malfunction [oxygen/respirator failure, black screen, inadequate battery level, non-inflatable cuff, and other technical problems] and inadequate preparation of drugs). Finally, the total length of stay and 30-day intrahospital mortality were compared between the two groups.
IBM SPSS version 25.0 was used for data analyses. Measurements conforming to normal distribution were expressed as mean ± standard deviation (x ± SD). An independent samples t-test was used to perform intergroup comparisons of the means. Enumeration data were expressed as percentages. In addition, two rates or constituent ratios were compared using the chi-square test, and ranked data were compared using the rank-sum test for multiple ratios. P < 0.05 indicated a significant difference.
The critically ill patients transported via conventional methods (control group) were collected from June 2017 to December 2017 (n = 420; mean age, 66.23 ± 19.64 [range, 18–92] years). The observation group included critically ill patients who were transported via graded transport from January 2018 to June 2018 (n = 380; mean age, 65.45 ± 20.37 [range, 18–94] years). The control group comprised 92, 71, 63, 46, 65, and 83 patients with neurological diseases, cardiovascular diseases, respiratory diseases, digestive system diseases, trauma, and other diseases, respectively. There were 79, 68, 60, 54, 63, and 56 patients with neurological diseases, cardiovascular diseases, respiratory diseases, digestive system diseases, trauma, and other diseases in the observation group, respectively. In addition, no significant intergroup difference was observed in the general information (P > 0.05) (Table 3).
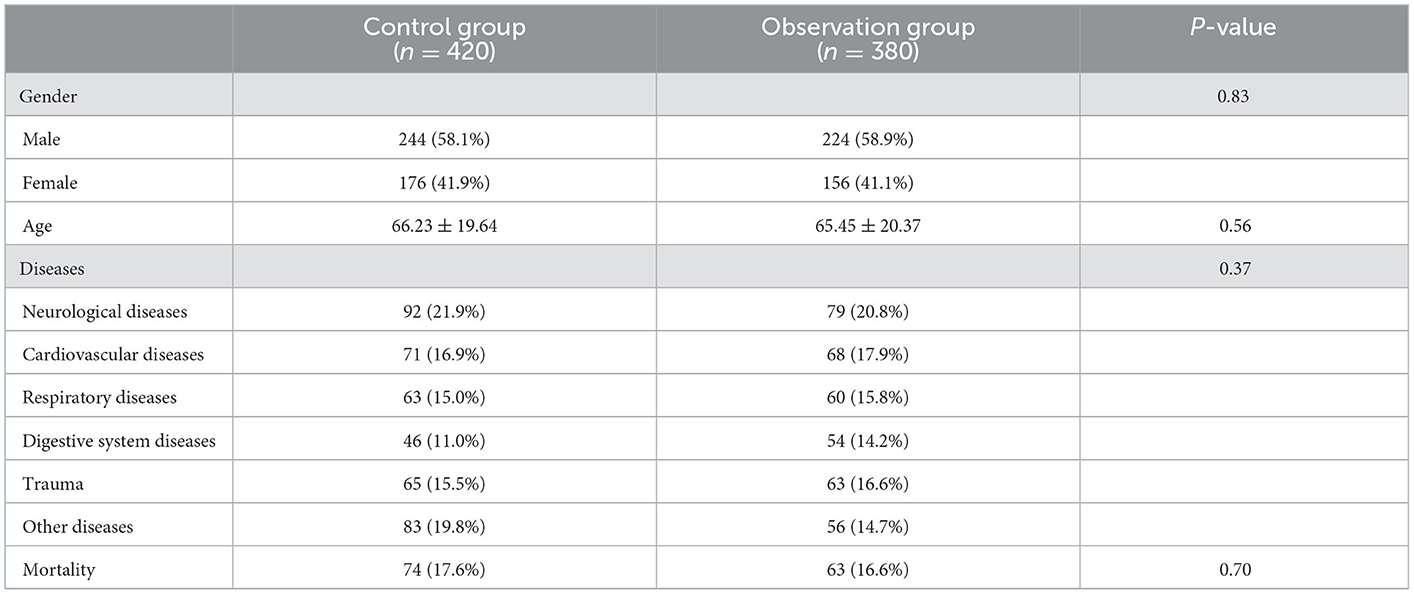
Table 3. Baseline characteristics of patients.
The IHT time of patients in the observation group from the emergency department to CT/MRI examination, interventional room, surgery room, ICU ward, and general wards was significantly lesser than that of patients in the control group (P < 0.05) (Table 4).

Table 4. Incidence of adverse events (AEs) in the observation and control groups.
One hundred patients in the control group developed AEs during transport (AE incidence rate, 23.81%). In addition, 43 patients in the observation group developed AEs during transport (AE incidence rate, 11.32%). Therefore, there was a significant intergroup difference in the AE incidence (P < 0.05). In the control group, the incidence rates of disease-, personnel-, apparatus-, and drug-related AEs were 8.81, 5.71, 5, and 4.29%, respectively, whereas the incidence rates for patients in the observation group were 4.73, 2.63, 2.11, and 1.84%, respectively; both groups showed significant intergroup differences (P < 0.05) (Table 5).

Table 5. Intrahospital transport time of patients in the observation and control groups.
The total lengths of stay of patients in the observation and control groups were 19.63 ± 13.95 and 19.18 ± 13.58 days, respectively. Furthermore, the 30-day intrahospital mortality rates were 16.58 and 17.62%, respectively, in the two groups (Table 6). There were no significant intergroup differences in terms of the length of stay and 30-day mortality (P > 0.05).
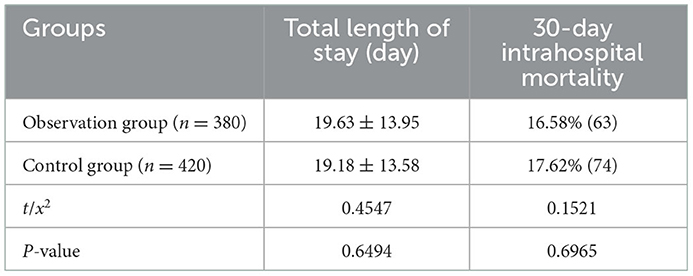
Table 6. Length of stay and 30-day intrahospital mortality in the observation and control groups.
IHT is a crucial and unavoidable step for critically ill patients to receive further diagnosis and treatment. However, such patients are susceptible to significant changes during IHT owing to reasons related to disease progression, apparatus used, medications, and transport personnel, which may cause serious complications and could even result in mortality (4). Findings of a recent meta-analysis indicated that critically ill patients may develop AEs during IHT, with a 26.2% incidence rate of mild-to-moderate AEs but a relatively low incidence rate of severe AEs (5). This meta-analysis facilitated a risk-benefit analysis of the diagnostic or therapeutic procedures for critically ill patients requiring IHT. In addition, the incidence rate of AEs was reportedly as high as 79.8% in a study on 441 patients admitted to the ICU undergoing IHT (6). Effective care during IHT is a challenge (7, 8). Owing to the high demand for emergency transport and the exposure to the patient's family during the transport process, medical disputes frequently occur, which places a considerable burden on transport physicians and nurses (9). Consequently, improving the safety of IHT is an area of great interest in research. Overall, meticulous transport planning and procedures, well-performing transport equipment, and well-trained professional teams are necessary to ensure the safety of critically ill patients during transport and reduce the incidence rate of AEs, thereby facilitating the treatment of patients (10–13).
The results of the present study suggested that the IHT time of patients in the observation group from the emergency department to CT/MRI examination, interventional room, surgery room, ICU ward, and the general ward was significantly shorter than that of patients in the control group. This phenomenon could be attributable to the following factors: First, the dedicated transport elevator and staff reduced the waiting time for the elevator; second, transport risk grading allowed medical staff to prepare supplies rapidly and reduce omissions; third, rational manpower allocation and collaboration of medical and nursing teams improved the transport efficiency (14); fourth, communication with medical and technical departments before transport reduced unnecessary waiting time; fifth, changes in the perceptions of medical and technical staff and pre-transport examination of critically ill patients by experienced technicians shortened the transport time. These factors reduced the stress and anxiety of patients and their families and saved the time of medical staff. Furthermore, the reduced waiting time alleviated the lack of oxygen storage, which reduced AEs caused by the low battery level of the monitor and ventilator.
In the present study, the incidence rates of AEs during ITH showed significant intergroup differences, i.e., 23.81 and 11.32% for the control and the observation groups, respectively. In addition, the incidence rate of AEs related to personnel, apparatus, and environment (or hidden problems) was significantly lower in the observation group than in the control group. This phenomenon may be attributed to the following factors. First, after defining and classifying AEs, we changed the perceptions of medical and technical personnel. After realizing the importance of the safety of IHT in the treatment of critically ill patients, the medical and nursing staff carefully evaluated the patients before transport, provided considerable attention to the associated details, and strengthened the assessment of all aspects of the process, which reduced the incidence rate of disease-related AEs. In addition, the selection and use of a graded transport list greatly reduced the lack of pre-transport materials. Furthermore, after theoretical training, operational training, objective structured examinations, and monthly quality control improvements, the medical personnel were calm, prepared, and skilled in the face of emergencies and could appropriately and promptly handle changes related to specific conditions, thereby reducing the incidence rate of personnel-related AEs. Finally, the provision of dedicated transport elevators and operating personnel reduced the unnecessary waiting time, transport time, and power consumption by hypoxia monitors and ventilators, thereby reducing the incidence rate of the environment- and apparatus-related AEs (11).
Studies on the relationship between IHT and the length of stay and mortality in critically ill patients have reported inconsistent findings. Several studies have demonstrated the correlation of the number of IHTs with delirium, length of stay, and mortality (15–17). Meanwhile, Erika et al. (18) observed no significant impact of IHT-related AEs on patient hospitalization. Despite the absence of any significant intergroup differences in terms of the impact of IHT-related AEs on the length of stay and mortality, further measures should be implemented to reduce these adverse factors.
A graded transport model can significantly improve transport efficiency, shorten transport time, and reduce the incidence rate of AEs during the transport process. This mode is a successful innovation in emergency medicine as it can reasonably optimize the allocation of emergency medical resources and improve the safety and efficiency of IHT. Unlike previously used transport modes, the graded transport mode contributes to the establishment of a safe and efficient IHT system for emergency patients. Different transport modes can be applied to corresponding levels of transport to achieve rationalization and safety of medical resource allocation. In addition, effective assessment and grading of the risk of patient transport and prompt preparation according to the actual situation can aid the reasonable allocation of medical resources and further improve the safety of transport, thereby enabling better treatment of critically ill patients.
This study has some limitations. First, the sample size of this study was relatively small. In addition, the retrospective nature of this study may have led to bias in patient selection. Moreover, we could not conduct a survey on the satisfaction of patients and the receiving departments owing to the specificity of the emergency setting. Finally, patient hospitalization costs could not be analyzed in comparative studies. Consequently, further studies are warranted to validate our findings.
In summary, the graded transport mode has a unique value in clinical settings. It can effectively improve the safety of transport and reduce the incidence of AEs. As a result, vital signs of patients at all risk grades can be effectively maintained during the transport process. Although no significant intergroup differences were observed in terms of the length of stay and 30-day mortality, the graded transport mode can shorten the IHT time of critically ill patients and reduce the AE incidence rates.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the study was approved by the Ethics Committee of Kunshan Hospital Jiangsu University (Kunshan, China). The patients/participants provided their written informed consent to participate in this study.
JM and LL conceived, designed, and coordinated the study. LL, JM, and ZG drafted this manuscript. XX, HY, CZ, SL, and JM were responsible for collecting and measuring the imaging data. LL, CZ, XX, and SL were responsible for collecting clinical data. JM and ZG were responsible for data analysis. All authors read, approved, and contributed to the final manuscript.
This study was supported by Kunshan Science Project under Grant KSZ2169.
We thank the patients and staff of the emergency department at Kunshan Hospital, Jiangsu University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bergman LM, Pettersson ME, Chaboyer WP, Carlström ED, Ringdal ML. Safety hazards during intrahospital transport: a prospective observational study. Crit Care Med. (2017) 45:e1043–9. doi: 10.1097/CCM.0000000000002653
2. Lu KK, Zhang MM, Zhu YL, Ye C, Li M. Improving the quality of emergency intrahospital transport for critically ill patients by using Toyota production system methods. J Multidiscip Healthc. (2022) 15:1111–20. doi: 10.2147/JMDH.S360261
3. Brunsveld-Reinders AH, Arbous MS, Kuiper SG, de Jonge E. A comprehensive method to develop a checklist to increase safety of intra-hospital transport of critically ill patients. Crit Care. (2015) 19:214. doi: 10.1186/s13054-015-0938-1
4. Hajjej Z, Gharsallah H, Boussaidi I, Daiki M, Labbene I, Ferjani M. Risk of mishaps during intrahospital transport of critically ill patients. Tunis Med. (2015) 93:708–13.
5. Murata M, Nakagawa N, Kawasaki T, Yasuo S, Yoshida T, Ando K, et al. Adverse events during intrahospital transport of critically ill patients: a systematic review and meta-analysis. Am J Emerg Med. (2022) 52:13–9. doi: 10.1016/j.ajem.2021.11.021
6. Jia L, Wang H, Gao Y, Liu H, Yu K. High incidence of adverse events during intra-hospital transport of critically ill patients and new related risk factors: a prospective, multicenter study in China. Crit Care. (2016) 20:12. doi: 10.1186/s13054-016-1183-y
7. Kue R, Brown P, Ness C, Scheulen J. Adverse clinical events during intrahospital transport by a specialized team: a preliminary report. Am J Crit Care. (2011) 20:153–62. doi: 10.4037/ajcc2011478
8. Venn AM, Sotomayor CA, Godambe SA, Vazifedan T, Jennings AD, Qureshi FA, et al. Implementation of an intrahospital transport checklist for emergency department admissions to intensive care. Pediatr Qual Saf. (2021) 6:e426. doi: 10.1097/pq9.0000000000000426
9. Salt O, Akpinar M, Sayhan MB, Örs FB, Durukan P, Baykan N, et al. Intrahospital critical patient transport from the emergency department. Arch Med Sci. (2018) 16:337–44. doi: 10.5114/aoms.2018.79598
10. Picetti E, Antonini MV, Lucchetti MC, Pucciarelli S, Valente A, Rossi I, et al. Intra-hospital transport of brain-injured patients: a prospective, observational study. Neurocrit Care. (2013) 18:298–304. doi: 10.1007/s12028-012-9802-1
11. Alizadeh Sharafi R, Ghahramanian A, Sheikhalipour Z, Ghafourifard M, Ghasempour M. Improving the safety and quality of the intra-hospital transport of critically ill patients. Nurs Crit Care. (2021) 26:244–52. doi: 10.1111/nicc.12527
12. Veiga VC, Postalli NF, Alvarisa TK, Travassos PP, Vale RT, Oliveira CZ, et al. Adverse events during intrahospital transport of critically ill patients in a large hospital. Eventos adversos durante transporte intra-hospitalar de pacientes críticos em hospital de grande porte. Rev Bras Ter Intensiva. (2019) 31:15–20. doi: 10.5935/0103-507X.20190003
13. Knight PH, Maheshwari N, Hussain J, Scholl M, Hughes M, Papadimos TJ, et al. Complications during intrahospital transport of critically ill patients: focus on risk identification and prevention. Int J Crit Illn Inj Sci. (2015) 5:256–64. doi: 10.4103/2229-5151.170840
14. Latzke M, Schiffinger M, Zellhofer D, Steyrer J. Soft factors, smooth transport? The role of safety climate and team processes in reducing adverse events during intrahospital transport in intensive care. Health Care Manag Rev. (2020) 45:32–40. doi: 10.1097/HMR.0000000000000188
15. Goldberg A, Straus SE, Hamid JS, Wong CL. Room transfers and the risk of delirium incidence amongst hospitalized elderly medical patients: a case-control study. BMC Geriatr. (2015) 15:69. doi: 10.1186/s12877-015-0070-8
16. Perimal-Lewis L, Bradley C, Hakendorf PH, Whitehead C, Heuzenroeder L, Crotty M. The relationship between in-hospital location and outcomes of care in patients diagnosed with dementia and/or delirium diagnoses: analysis of patient journey. BMC Geriatr. (2016) 16:190. doi: 10.1186/s12877-016-0372-5
17. Schwebel C, Clec'h C, Magne S, Minet C, Garrouste-Orgeas M, Bonadona A, et al. Safety of intrahospital transport in ventilated critically ill patients: a multicenter cohort study. Crit Care Med. (2013) 41:1919–28. doi: 10.1097/CCM.0b013e31828a3bbd
Keywords: emergency treatment, critically ill patients, intrahospital transport, adverse events, graded transport
Citation: Ling L, Xia X, Yuan H, Liu S, Guo Z, Zhang C and Ma J (2023) Effectiveness of the graded transport mode for the intrahospital transport of critically ill patients: A retrospective study. Front. Public Health 10:979238. doi: 10.3389/fpubh.2022.979238
Received: 27 June 2022; Accepted: 26 December 2022;
Published: 13 January 2023.
Edited by:
Stephen Waller, Uniformed Services University, United StatesReviewed by:
Zhixun Bai, Zunyi Medical University, ChinaCopyright © 2023 Ling, Xia, Yuan, Liu, Guo, Zhang and Ma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jin Ma,  MTAzMTE4OTAwQHFxLmNvbQ==
MTAzMTE4OTAwQHFxLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.