
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 16 December 2022
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.969251
 Fortino Solórzano-Santos1†
Fortino Solórzano-Santos1† América Liliana Miranda-Lora2†
América Liliana Miranda-Lora2† Horacio Márquez-González3*
Horacio Márquez-González3* Miguel Klünder-Klünder4*
Miguel Klünder-Klünder4*Background: The new coronavirus SARS-CoV-2 pandemic has been relatively less lethal in children; however, poor prognosis and mortality has been associated with factors such as access to health services. Mexico remained on the list of the ten countries with the highest case fatality rate (CFR) in adults. It is of interest to know the behavior of COVID-19 in the pediatric population. The aim of this study was to identify clinical and sociodemographic variables associated with mortality due to COVID-19 in pediatric patients.
Objective: Using National open data and information from the Ministry of Health, Mexico, this cohort study aimed to identify clinical and sociodemographic variables associated with COVID-19 mortality in pediatric patients.
Method: A cohort study was designed based on National open data from the Ministry of Health, Mexico, for the period April 2020 to January 2022, and included patients under 18 years of age with confirmed SARS-CoV-2 infection. Variables analyzed were age, health services used, and comorbidities (obesity, diabetes, asthma, cardiovascular disease, immunosuppression, high blood pressure, and chronic kidney disease). Follow-up duration was 60 days, and primary outcomes were death, hospitalization, and requirement of intensive care. Statistical analysis included survival analysis, prediction models created using the Cox proportional hazards model, and Kaplan-Meier estimation curves.
Results: The cohort included 261,099 cases with a mean age of 11.2 ± 4 years, and of these, 11,569 (4.43%) were hospitalized and 1,028 (0.39%) died. Variables associated with risk of mortality were age under 12 months, the presence of comorbidities, health sector where they were treated, and first wave of infection.
Conclusion: Based on data in the National database, we show that the pediatric fatality rate due to SARS-CoV-2 is similar to that seen in other countries. Access to health services and distribution of mortality were heterogeneous. Vulnerable groups were patients younger than 12 months and those with comorbidities.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged in China at the end of 2019, has spread worldwide, and Coronavirus disease 2019 (COVID-19) was declared a pandemic by the World Health Organization (WHO) in March 2020 (1). As of March 21, 2022, more than 471,925,910 COVID-19 cases have been confirmed worldwide, with 6,104,420 deaths reported. In Mexico, 5,633,928 cases and 322,072 deaths have been reported (2, 3). Reported disease burden and case fatality rates vary considerably among different age groups during the different waves of the pandemic, and COVID-19 in children is thought to typically cause mild-to-moderate disease. Additionally, while fewer children appear to develop serious sequelae such as multisystem inflammatory syndrome (MIS-C) (4), some reports state that the age group with higher mortality is infants <1 year old (5, 6). The pediatric population accounts for 1–2% of the total cases; however, this number varies in the different waves of the pandemic, as reported by Rovida et al. (7). Approximately 6% of all infected children develop severe illness that requires pediatric intensive care unit (ICU) admission, and similar to adults, hospitalized patients, especially critically ill patients, have pre-existing underlying diseases or comorbidities (7). There appears to be an effect of age and comorbidities on the prognosis of children with COVID-19, according to a recent meta-analysis those <1 year old were more likely to be admitted to ICU, Odds Ratio (OR) = 1.63 (95% CI: 1, 40 to 1.90); and death, OR = 2.08 (95% CI: 1.57 to 2.86) and the odds of death increased among children aged 10–14 years OR = 2.15 and >14 years OR = 2.15. A meta-analysis showed a more significant association with outcomes (ICU and death) when comparing patients with and without comorbidities. For example, with an added disease, the OR was 1.49 for ICU admission and 2.34 for death; with three comorbidities, it increased to 4.32 and 5.56, respectively (8).
Using national open data and information from the Ministry of Health, Mexico, this cohort study aimed to identify clinical and sociodemographic variables associated with COVID-19 mortality in pediatric patients (3). Risk factors for severe disease and death in the pediatric population were analyzed, to identify those groups that should be priority for vaccination and in those that require other interventions to the risk reduction. It was made an analysis about if the attention in some sector of our health system influence over the patient's prognosis.
In Mexico, by official provision, hospitals of the health system that receive patients with suspected or confirmed SARS-CoV-2 virus infection have to register patient data in a public database created by the General Directorate of Epidemiology and contains the information of all public and private institutions in the country that treated hospitalized patients and that reported to the Ministry of Health of Mexico through the SISVER platform (for its acronym in Spanish, Epidemiological Surveillance System for Respiratory Diseases). Using this database (see Data Availability Statement), we analyzed data of a cohort of pediatric patients (under 18 years of age) from April 14, 2020, to January 16, 2022. The selection criteria applied were any gender and a positive PCR test for SARS-CoV-2 or antigen test plus positive criteria for COVID-19, as issued by a ruling committee. Cases with inconsistencies in the dates of diagnosis, hospitalization and death were excluded. Time zero was defined as the date of diagnostic confirmation, and follow-up was recorded up to day 60. Primary outcome was death related to COVID-19.
Risk factors evaluated were age group (according to the American Academy of Pediatrics (9): <12 months, 1–3, 3.1–5, 5.1–12, and 12.1–18 years), states of residence (Mexico is divided into 32 states), health system to which they had access (Mexican Institute of Social Security, IMSS; Institute of Security and Social Services for State Workers, ISSSTE; Ministry of Health, SSA; Private Hospitals and others such as well-being Regime, University Hospitals, Secretary of National Defense, Secretary of the Navy).
The contagion rates were divided into the following periods: first wave, from the first case in Mexico (April 2020) to September 30, 2020; the second wave, from October 1 to May 14, 2021; the third wave, from May 15 to December 3, 2021, and the fourth wave, from January 16, 2022, to the current date.
Other risk variables included were the presence of comorbidities such as obesity, diabetes, asthma, cardiovascular disease, immunosuppression, arterial hypertension, chronic kidney disease, and the need for mechanical ventilation.
Hospitalization, the complication of COVID-19 with pneumonia, and the need for intensive care were identified as confounding variables.
Qualitative variables are presented as frequencies and percentages, age (in years) is presented as a parametric distribution and is expressed as mean and standard deviation. Outcomes variables, namely, hospitalization, ICU requirement, and lethality, were estimated using the formula (10): outcome patient's number/number of patients exposed per 100 or 1,000 infected subjects by State and by sector of Health. The Chi-squared test was used to demonstrate differences in the variables between survivors vs. non-survivors. For the prediction models, the Cox proportional hazards with forward stepwise variable selection method was used, and variables entered into the multivariate models based on biological plausibility and initial significance level of p < 0.1 in the bivariate analysis. Models were created for mortality in the entire infected population, hospitalization, pneumonia, and ICU admission. Internal validation of each model was performed by calculating each patient's probability in the cohort with the formula (11), λ(t) = λ0(t) exp(βTX), in which, λ = hazard function; t = failure time of interest; and, βTX = It represents the probability of survival in time t of the subjects with a certain pattern of X values in the explanatory variables and by estimating the value of the area under the curve with death as the variable. Kaplan-Meier survival curves were created, and statistical significance was calculated using the Log-Rank test. All statistical analyses used SPSS (version 25, for MAC) and STATA version 16.
COVID-19 was suspected in 1,029,140 children and infection by SARS-CoV-2 was confirmed in 261,099. Mean age of the cohort was 11.2 ± 4 years, 131,045 (50.4%) were males, and 11,569 (4.43%) were hospitalized while 249,530 (95.5%) were ambulatory patients (Figure 1). Infections were the highest (50.8%) in children aged > 12.1 years while those aged < 12 months accounted for 5.6% of all infections.
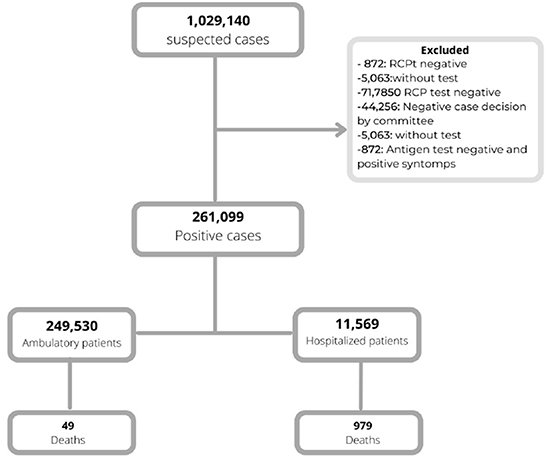
Figure 1. Selection of the cohort of pediatric patients with SARS-CoV-2.
Figure 2A shows the cumulative 7-day incidence rate of confirmed COVID-19 cases from April 2020 to January 2022.Fourth waves are visible in this chart. Those with the highest number correspond to the third (dominant delta variant) and fourth wave (dominant omicron variant). However, during the first and second waves caused the most deaths, as shown in Figure 2B.
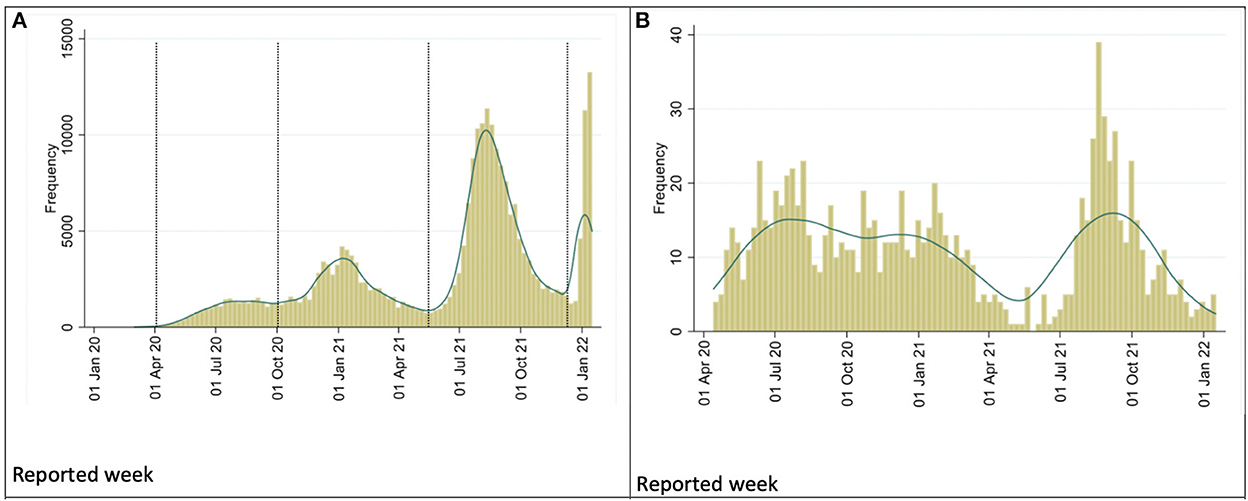
Figure 2. (A) Frequency of SARS-CoV-2 infections in the pediatric population in Mexico. (B) Frequency of deaths of pediatric patients due to SARS-CoV-2 Mexico.
There were 1,028 deaths (0.39%); of these, 49 (0.02%) were among ambulatory patients and 979 (8.46%) in hospitalized patients. Thus, hospitalized patients accounted for 95.2% of all deaths. The global case fatality rate (CFR) was 3.9% with an incidence density of deaths of 6.8 patients per 100,000 days. Lethality was more frequent in children < 12 months old (CFR 2.76) and those aged 1–3 years (CFR 0.60). Next, 33.1% of non-survivors presented with one or more comorbidities; this value was 6.7% among survivors, and the CFR was 2 (per 100 patients). The comorbidities with highest CFR were chronic kidney disease, cardiovascular disease, immunosuppression, and hypertension. Patients requiring mechanical ventilatory assistance had the highest CFR (Table 1).
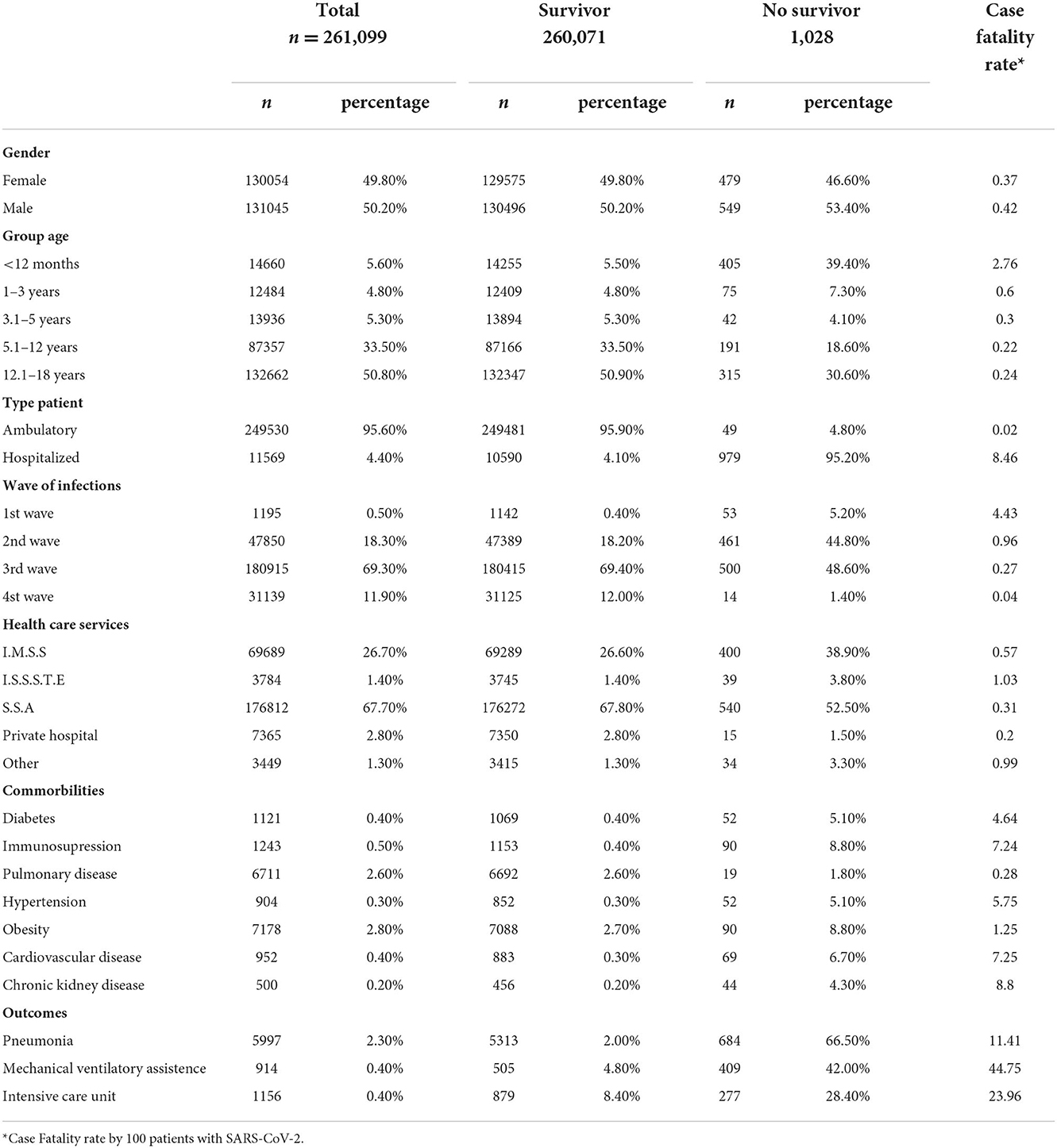
Table 1. General characteristics of pediatric patients with SARS-CoV-2 and the differences between survivors and non-survivors.
Analysis of outcomes, classified according to the health care institution used, showed that the lowest CFR was recorded in private hospitals (0.1 per 1,000 patients with SARS-CoV-2) even though rate of hospitalization was 3.5 per 100 infected patients. The SSA treated 54.8% of all hospitalized patients and 20% of patients treated in the country's ICUs. Data on other health care institutions are shown in Table 2.
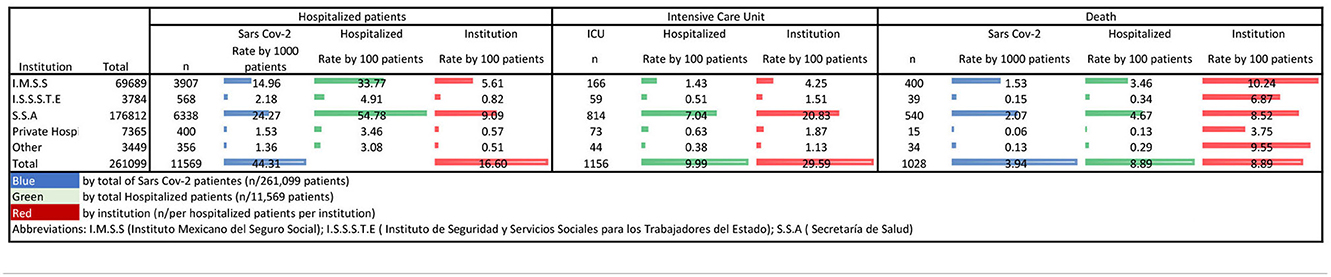
Table 2. Comparison of outcomes according to the health institutions that treated pediatric patients with SARS-CoV-2.
Data analysis stratified according to the 32 states of the Country showed that a majority of infections and hospitalization occurred in Mexico City (192.8 per 1,000 patients hospitalized). However, the highest CFR was recorded in other states and was related to access to ICU care (Supplementary Table S1). Kaplan-Meier univariate survival analysis showed that the age group with the lowest survival was children under 12 months of age (Figure 3A), and that the sum of comorbidities was associated with a lower probability of survival (Figure 3B).
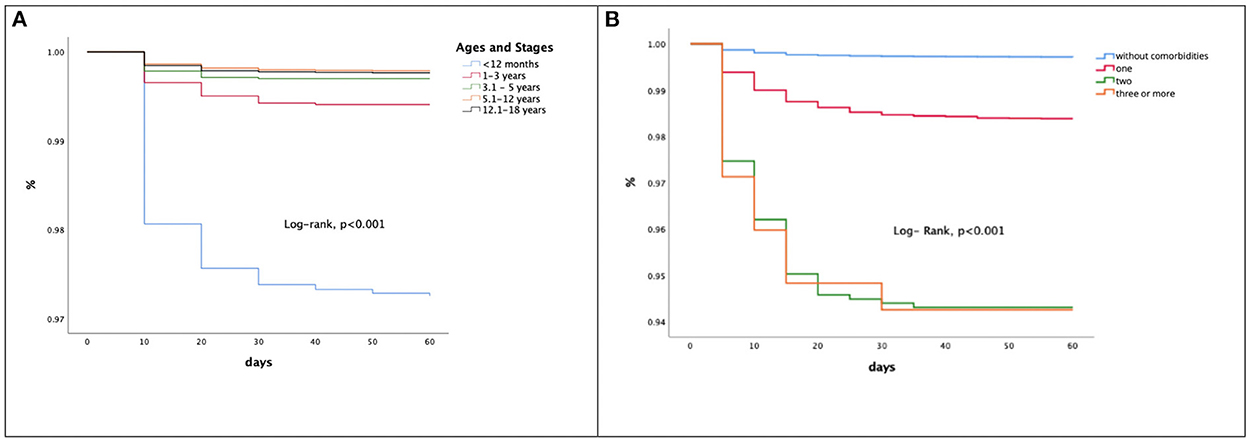
Figure 3. (A) Survival analysis of patients with SARS-CoV-2 by age groups. (B) Comparative survival function in pediatric patients with SARS-CoV-2 by comorbidities.
Table 3 shows mortality in the total population with SARS-CoV-2 and stratified mortality analysis by prediction models, namely, hospitalized, pneumonia and ICU patients. All models included age (years), comorbidities, health sector, waves of contagion, and fatality rate by state as variables. We found that predictive capacity decreased in patients with pneumonia (AUC = 0.56) and ICU admission (AUC = 0.32). Age in years, cardiovascular disease, and chronic kidney disease were the variables most related to death in all models.
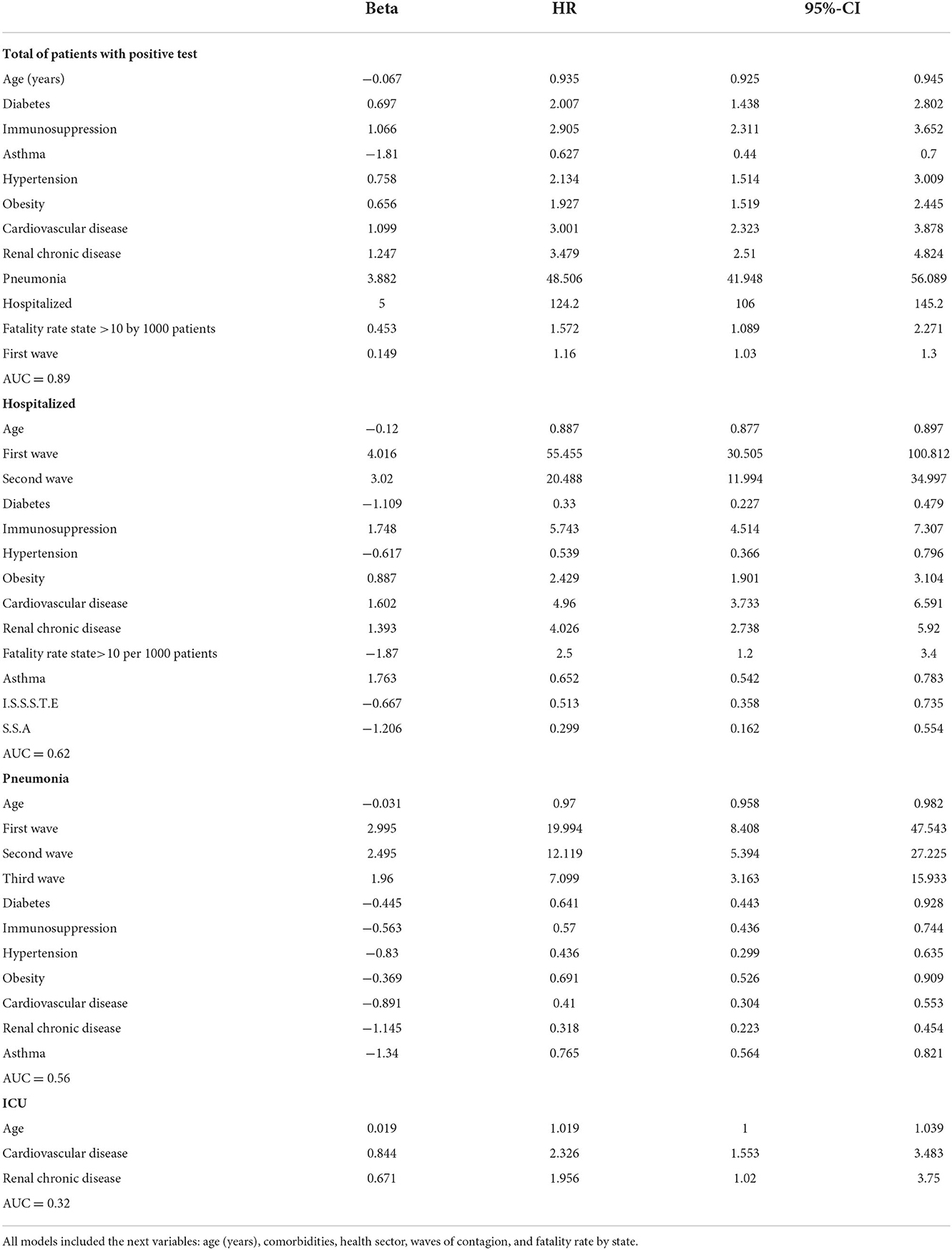
Table 3. Predictives models of mortality in pediatrics patients with SARS-CoV-2.
The emergence of COVID-19 has required rapid and continuous learning to face the challenges that this pandemic has presented. Concepts around SARS-CoV-2 that were prevalent at the start of the pandemic have changed; hence, frequent revision of the global outlook remains highly relevant. Although COVID-19 has mainly affected the adult population, it has also spread to the pediatric population, albeit to a lesser extent. Thus, identification of risk factors associated with mortality in the pediatric population is relevant as it can support decision-making aimed at prevention, care, and restoration of the damage caused by the disease.
In Mexico, the frequency of pediatric COVID-19 cases in the different waves was consistent with school closures and social distancing. Furthermore, Rovida et al. (7) reported a lower intensity of SARS-CoV-2 exposure was seen at the start of the pandemic. Additionally, the transition from lockdown to the reopening of schools coincided with an increase in the number of cases in the third and fourth waves. The change in frequency of infection in the recent months is related to the appearance of new variants with greater transmissibility, immune escape, and diagnostic failures (12). Nevertheless, CFR has decreased, which was much higher in the first wave compared to subsequent outbreaks (Table 1). This could be related to the saturation of health services prior to the opening of emergency medical units at the beginning of the pandemic as well as the steep learning curve for the care of COVID-19 patients.
Worldwide, more than 90% of pediatric patients were either asymptomatic or had mild-to-moderate disease (13) with low risk of mortality (14). Our results are consistent with this profile as more than 95% of the positive cases in our cohort exhibited satisfactory outcomes and did not require hospitalization. Moreover, compared to data in our previous report on trends in adults, frequency of hospitalization in Mexican children was 5 times lower, need for intubation was 43-fold less, admission to intensive care was 21 times lower, and mortality was 25-fold less (15).
Factors that can potentially explain the differences in COVID-19 severity between children and adults include immune response, angiotensin converting enzyme 2 distribution (limiting infection), androgen's transmembrane protease serine 2-mediated actions that might result in fewer fatalities in prepubertal children, observed divergence between the sexes in SARS-CoV-2 infection, age-related increase in endothelial damage and changes in clotting function, higher prevalence of comorbidities in adults that are associated with severe COVID-19, pre-existing immunity to other coronaviruses, and differences in melatonin levels (16–21). Nonetheless, mechanisms involved in milder COVID-19 disease in children are not fully understood.
The overall mortality rate in this study was 0.4%, which is similar to that reported in a meta-analysis by Badal et al. (0.3%, CI 95% 0.1–0.4) (20). However, the mortality rate of children who were hospitalized with COVID-19 in our cohort was 8.4%, which is significantly greater than that reported from the United States (1.8–5.2%) (22, 23) but lower than that seen in India (11.4%) (24) Indonesia (10.2%) (25) and Iran (13%) (19). These differences may be explained by variables such as predominant virus driving the outbreak at the time of reporting, social restriction measures enforced, prevalence of comorbidities, socioeconomic issues, health infrastructure, or even ethnicity as multisystem inflammatory syndrome has been more frequently reported in Hispanic children (26). We also hypothesize that the high prevalence of vitamin D deficiency in our country (27.3% in pre-school-age and 17.2% in school-age children) (27) could have contributed to COVID-19 mortality, as reported by Jayawardena R et al. (28).
Although Mexico City accounted for a majority of pediatric COVID-19 cases, CFR was lower compared to other States. This observation concurs with data from previous reports in the Mexican adult population (15) and with results from other studies that identified an inverse relation between death rate and population density (29–31). Additionally, this trend could be related to access to health care services, better infrastructure, availability of ICUs, and the impact of measures such as a social distancing, lockdowns, and immunizations.
Our analysis revealed differences in fatality rates among the health care services and also between the states. We surmise that socioeconomic inequalities could have contributed to higher mortality in our country, as reported by our colleagues in Mexico (26, 29) and Brazil (27, 32, 33). It is necessary to highlight the fact that these differences in case density did not coincide with higher frequency of hospitalization, admission to intensive care, or mortality. Therefore, such differences between states require a review of the social determinants of health, especially poverty index, transportation, and hospital infrastructure.
We show the perinatal period to be associated with a higher fatality rate than later childhood, indicating that the U-shaped COVID-19 mortality curve in the Mexican population is characterized by an initial decrease in mortality after 1 year of age, a nadir at 5–12 years, and a subsequent increase throughout life. This is similar to results reported by us previously in the same population (6, 15, 29), and the U-shaped mortality curve has been observed by others as well (5, 6, 34, 35). Worldwide, the highest mortality rate was seen in infants <1 year old, mainly in the lower and middle income countries (36), which lead to doubts about the usefulness of measures to control infection transmissibility in this age group as well as strategies to protect immunity during pregnancy and vaccinate pregnant women (37).
Risk factors associated with COVID-19 mortality identified here include a few that have been reported earlier, such as younger age (34, 37) and the presence of chronic conditions (19, 36–39). Further, our data show that a third of non-survivors had at least one comorbidity. Congruently, previous reports show that the presence of more than one pre-existing medical condition could increase the odds of death by up to 10-fold (16, 33, 40, 41). Some authors have proposed that the history of a comorbidity supersedes the effects of age, gender and race/ethnicity as risk factors for pediatric COVID-19 death (16), strongly advocating for vaccination of this vulnerable group (42).
Children with comorbidities had a higher mortality in our population, which concurs with other reports, including a meta-analysis that quantified mortality risk in children with underlying conditions (relative risk, 2.81, 95%CI 1.21–6.02). Further, obesity was associated with highest risk (RR 2.87, 95%CI 1.16–7.07) (41), and we report a HR of 1.92 (95%CI 1.5–2.4) for COVID-19 mortality due to obesity. Several studies have also found an association between obesity and general mortality, including in pediatric patients (29, 43–46). These observations are important given the high prevalence of overweight and obesity in the Mexican pediatric population (from 8.4% overweight children under 5 years of age to 43.8% joint prevalence of overweight and obesity in adolescents) (47).
Similar to observations in adults, diabetes was identified as another risk factor for mortality in this cohort (HR 2.0, 95%CI 1.4–2.8) (15). This finding is in agreement with reports from Iran (16) and with a previous report from Mexico (29). However, data from China, Italy, Spain, and United States suggest that children, adolescents, and youth with diabetes have similar COVID-19 outcomes compared to their non-diabetic-peers (47). These differences in trends could be explained by variation in metabolic control, access to health systems, and even differences in vaccination frequencies in this vulnerable population.
Among the comorbidities analyzed, immunosuppression had the highest CFR. This group includes oncology patients who suffer high mortality (48–50) or patients with primary immunodeficiency (51); however, other reports state that immunocompromised pediatric patients with cancer and hematopoietic cell transplant patients tended to experience clinical outcomes similar to that seen in the general population (52–54). Indirect effects of the pandemic, such as delayed treatment and the protection measures in this population, including the frequency and timing of immunization, may be contributing factors.
Other comorbidities associated with higher mortality in our study, such as chronic kidney disease (19, 29), cardiovascular disease (19) or hypertension (29), have also been identified in previous reports. Hence, children suffering from these diseases should be afforded vaccination priority, regardless of age. Although asthma was one of the most frequent comorbidities in this cohort (2.5%), it was not associated with greater mortality. This interesting finding provides a favorable outlook for asthmatic children infected by SARS-CoV-2 and is probably related to immune mechanisms (55).
The strengths of this study lie in the inclusion of all confirmed cases in Mexico using data from the national database. Further, stratification by variables that are directly related to death (hospitalization, pneumonia, and ICU) lowers the explanatory capacity of the models and demonstrates the need to include other undetermined variables such as the type of treatment. Notably, this strategy enables potential control of ecological fallacy bias; nevertheless, risks of bias inherent in retrospective studies are applicable here as well. As data was collected from reports that each hospital in the country provided daily, a memory bias cannot be excluded. Additionally, operational definitions used for exposure variables, such as comorbidities (mainly the variables of asthma, cardiovascular disease, and immunosuppression), were not standardized (risk of misclassification bias) and the follow-up strategy was different for each hospital (follow-up bias).
Based on data available in the national database, we show that infant fatality rate due to SARS-CoV-2 in Mexico is similar to that reported in other countries. Vulnerable groups are patients younger than 12 months and those with comorbidities, and the distribution of mortality and access to health care showed heterogeneity across the country.
Publicly available datasets were analyzed in this study. This data can be found here: https://www.gob.mx/salud/documentos/datos-abiertos-152127.
Ethical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent was not provided because Research subjects were obtained from the public database of the Secretariat of Health of Mexico. Access to the identity of the research subjects is not possible.
HM-G and MK-K organized the database and performed the statistical analysis. AM-L and FS-S wrote the first draft of the manuscript. AM-L, FS-S, HM-G, and MK-K wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.969251/full#supplementary-material
1. Lu X, Zhang L, Du H, Zhang J, Li YY, Qu J, et al. SARS-CoV-2 infection in Children. N Engl J Med. (2020) 382:1663–5. doi: 10.1056/NEJMc2005073
2. COVID Live–Coronavirus Statistics–Worldometer. Available online at: https://www.worldometers.info/coronavirus/ (accessed September 1, 2022).
3. COVID-19 Tablero México–CONACYT–CentroGeo–GeoInt–DataLab. Covid-19 México, Información General. (2022). Available online at: https://datos.covid-19.conacyt.mx/ (accessed September 1, 2022).
4. Wanga V, Gerdes ME, Shi DS, Choudhary R, Dulski TM, Hsu S, et al. Characteristics and clinical outcomes of children and adolescents aged. MMWR Morb Mortal Wkly Rep. (2021) 70:1766–72. doi: 10.15585/mmwr.mm705152a3
5. Najafinejad M, Cheraghali F, Aghcheli B, Rajabi A, Barati L, Naziri H, et al. COVID-19 in pediatrics: demographic, clinical, laboratory, and radiological characteristics of infected patients with SARS-CoV-2. Front Pediatr. (2022) 9:187. doi: 10.3389/fped.2021.808187
6. González-García N, Castilla-Peón MF, Solórzano Santos F, Jiménez-Juárez RN, Martínez Bustamante ME, et al. Covid-19 incidence and mortality by age strata and comorbidities in Mexico City: a focus in the pediatric population. Front Public Health. (2021) 9:e738423. doi: 10.3389/fpubh.2021.738423
7. Rovida F, Giardina F, Ferrari G, Paolucci S, Piralla A, Baldanti F. SARS-CoV-2 infections in pediatric patients: a comparison of three pandemic waves. Pediatr Allergy Immunol. (2022) 33 Suppl 27:93–5. doi: 10.1111/pai.13642
8. Harwood R, Yan H, Talawila Da Camara N, Smith C, Ward J, Tudur-Smith C, et al. Which children and young people are at higher risk of severe disease and death after hospitalisation with SARS-CoV-2 infection in children and young people: a systematic review and individual patient meta-analysis. EClinicalMed. (2022) 44:1287. doi: 10.1016/j.eclinm.2022.101287
9. Ages, & Stages– HealthyChildren.org. Available online at: https://www.healthychildren.org/English/ages-stages/Pages/default.aspx (accessed September 3, 2022).
10. Colditz GA, Rosner BA. What can be learnt from models of incidence rates? Breast Cancer Res. (2006) 8:1414. doi: 10.1186/bcr1414
11. Fisher LD, Lin DY. Time-dependent covariates in the cox proportional-hazards regression model. Annu Rev Public Health. (1999) 20:145–57. doi: 10.1146/annurev.publhealth.20.1.145
12. Boehm E, Kronig I, Neher RA, Eckerle I, Vetter P, Kaiser L. Novel SARS-CoV-2 variants: the pandemics within the pandemic. Clin Microbiol Infect. (2021) 27:1109–17. doi: 10.1016/j.cmi.2021.05.022
13. Dong Y, Dong Y, Mo X, Hu Y, Qi X, Jiang F, et al. epidemiology of COVID-19 among children in China. Pediatrics. (2020) 145:702. doi: 10.1542/peds.2020-0702
14. Bhopal SS, Bagaria J, Olabi B, Bhopal R. Children and young people remain at low risk of COVID-19 mortality. Lancet Child Adolesc Health. (2021) 5:e12–3. doi: 10.1016/S2352-4642(21)00066-3
15. Márquez-González H, Méndez-Galván JF, Reyes-López A, Klünder-Klünder M, Jiménez-Juárez R, Garduño-Espinosa J, et al. Coronavirus Disease-2019 Survival in Mexico: a cohort study on the interaction of the associated factors. Front Public Health. (2021) 9:114. doi: 10.3389/fpubh.2021.660114
16. Moreira A, Chorath K, Rajasekaran K, Burmeister F, Ahmed M, Moreira A. Demographic predictors of hospitalization and mortality in US children with COVID-19. Eur J Pediatr. (2021) 180:1659–63. doi: 10.1007/s00431-021-03955-x
17. Williams PCM, Howard-Jones AR, Hsu P, Palasanthiran P, Gray PE, McMullan BJ, et al. SARS-CoV-2 in children: spectrum of disease, transmission and immunopathological underpinnings. Pathology. (2020) 52:801–8. doi: 10.1016/j.pathol.2020.08.001
18. Warner S, Richter A, Stamataki Z, Kelly D. Understanding COVID-19: are children the key? BMJ Paediatr Open. (2021) 5:63. doi: 10.1136/bmjpo-2021-001063
19. Madani S, Shahin S, Yoosefi M, Ahmadi N, Ghasemi E, Koolaji S, et al. Red flags of poor prognosis in pediatric cases of COVID-19: the first 6610 hospitalized children in Iran. BMC Pediatr. (2021) 21: doi: 10.1186/s12887-021-03030-2
20. Badal S, Thapa Bajgain K, Badal S, Thapa R, Bajgain BB, Santana MJ. Prevalence, clinical characteristics, and outcomes of pediatric COVID-19: a systematic review and meta-analysis. J Clin Virol. (2021) 135:4715. doi: 10.1016/j.jcv.2020.104715
21. Zimmermann P, Curtis N. Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections. Arch Dis Child. (2020) 106:429–39. doi: 10.1136/archdischild-2020-320338
22. Kim TY, Kim EC, Agudelo AZ, Friedman L. COVID-19 hospitalization rate in children across a private hospital network in the United States: COVID-19 hospitalization rate in children. Arch Pediatr. (2021) 28:530–2. doi: 10.1016/j.arcped.2021.07.004
23. Bhalala US, Gist KM, Tripathi S, Boman K, Kumar VK, Retford L, et al. Characterization and outcomes of hospitalized children with coronavirus disease 2019: a report from a multicenter, viral infection and respiratory illness universal study (Coronavirus Disease 2019) registry. Crit Care Med. (2022) 50:E40–51. doi: 10.1097/CCM.0000000000005232
24. Singh P, Attri K, Mahto D, Kumar V, Kapoor D, Seth A, et al. Clinical profile of COVID-19 illness in children-experience from a tertiary care hospital. Indian J Pediatr. (2022) 89:45–51. doi: 10.1007/s12098-021-03822-5
25. Dewi R, Kaswandani N, Karyanti MR, Setyanto DB, Pudjiadi AH, Hendarto A, et al. Mortality in children with positive SARS-CoV-2 polymerase chain reaction test: lessons learned from a tertiary referral hospital in Indonesia. Int J Infect Dis. (2021) 107:78–85. doi: 10.1016/j.ijid.2021.04.019
26. Alsaied T, Tremoulet AH, Burns JC, Saidi A, Dionne A, Lang SM, et al. Review of cardiac involvement in multisystem inflammatory syndrome in children. Circulation. (2021) 143:78–88. doi: 10.1161/CIRCULATIONAHA.120.049836
27. Martins-Filho PR, de Souza Araújo AA, Quintans-Júnior LJ, Santos VS. COVID-19 fatality rates related to social inequality in Northeast Brazil: a neighbourhood-level analysis. J Travel Med. (2020) 27:128. doi: 10.1093/jtm/taaa128
28. Jayawardena R, Jeyakumar DT, Francis T, Misra A. Impact of the vitamin D deficiency on COVID-19 infection and mortality in Asian countries. Diabetes Metab Syndr. (2021) 15:757–64. doi: 10.1016/j.dsx.2021.03.006
29. Sanchez-Piedra C, Gamiño-Arroyo AE, Cruz-Cruz C, Prado-Galbarro FJ. Impact of environmental and individual factors on COVID-19 mortality in children and adolescents in Mexico: An observational study. Lancet Regional Health Americas. (2022) 8:184. doi: 10.1016/j.lana.2022.100184
30. Bhadra A, Mukherjee A, Sarkar K. Impact of population density on Covid-19 infected and mortality rate in India. Model Earth Syst Environ. (2021) 7:623–9. doi: 10.1007/s40808-020-00984-7
31. Hamidi S, Ewing R, Sabouri S. Longitudinal analyses of the relationship between development density and the COVID-19 morbidity and mortality rates: early evidence from 1,165 metropolitan counties in the United States. Health Place. (2020) 64:102378. doi: 10.1016/j.healthplace.2020.102378
32. Martins-Filho PR, Quintans-Júnior LJ, de Souza Araújo AA, Sposato KB, Souza Tavares CS, Gurgel RQ, et al. Socio-economic inequalities and COVID-19 incidence and mortality in Brazilian children: a nationwide register-based study. Public Health. (2021) 190:4–6. doi: 10.1016/j.puhe.2020.11.005
33. Sousa BLA, Brentani A, Costa Ribeiro CC, Dolhnikoff M, Grisi SJFE, Ferrer APS, et al. Non-communicable diseases, sociodemographic vulnerability and the risk of mortality in hospitalised children and adolescents with COVID-19 in Brazil: a cross-sectional observational study. BMJ Open. (2021) 11:724. doi: 10.1136/bmjopen-2021-050724
34. Khera N, Santesmasses D, Kerepesi C, Gladyshev VN. COVID-19 mortality rate in children is U-shaped. Aging. (2021) 13:19954–62. doi: 10.18632/aging.203442
35. O'Driscoll M, Ribeiro Dos Santos G, Wang L, Cummings DAT, Azman AS, Paireau J, et al. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature. (2021) 590:140–5. doi: 10.1038/s41586-020-2918-0
36. Kitano T, Kitano M, Krueger C, Jamal H, al Rawahi H, Lee-Krueger R, et al. The differential impact of pediatric COVID-19 between high-income countries and low- and middle-income countries: a systematic review of fatality and ICU admission in children worldwide. PLoS ONE. (2021) 16:e246326. doi: 10.1371/journal.pone.0246326
37. Falsaperla R, Leone G, Familiari M, Ruggieri M. COVID-19 vaccination in pregnant and lactating women: a systematic review. Expert Rev Vaccines. (2021) 20:1619–28. doi: 10.1080/14760584.2021.1986390
38. Sena GR, Lima TPF, Vidal SA. do Carmo Duarte MMB, Bezerra PGM, Fonseca Lima EJ, et al. Clinical characteristics and mortality profile of COVID-19 patients aged less than 20 years old in Pernambuco–Brazil. Am J Trop Med Hyg. (2021) 104:1507–12. doi: 10.4269/ajtmh.20-1368
39. Hendler JV, Miranda do Lago P, Müller GC, Santana JC, Piva JP, Daudt LE. Risk factors for severe COVID-19 infection in Brazilian children. Braz J Infect Dis. (2021) 25:1650. doi: 10.1016/j.bjid.2021.101650
40. Oliveira EA, Colosimo EA., Simões e, Silva AC, Mak RH, Martelli DB, Silva LR, et al. Clinical characteristics and risk factors for death among hospitalised children and adolescents with COVID-19 in Brazil: an analysis of a nationwide database. Lancet Child Adolesc Health. (2021) 5:559–68. doi: 10.1016/S2352-4642(21)00134-6
41. Tsankov BK, Allaire JM, Irvine MA, Lopez AA, Sauvé LJ, Vallance BA, et al. Severe COVID-19 infection and pediatric comorbidities: a systematic review and meta-analysis. Int J Infect Dis. (2021) 103:246–56. doi: 10.1016/j.ijid.2020.11.163
42. Wong BLH, Ramsay ME, Ladhani SN. Should children be vaccinated against COVID-19 now? Arch Dis Child. (2021) 106:225. doi: 10.1136/archdischild-2020-321225
43. Vera-Zertuche JM, Mancilla-Galindo J, Tlalpa-Prisco M, Aguilar-Alonso P, Aguirre-García MM, et al. Obesity is a strong risk factor for short-term mortality and adverse outcomes in Mexican patients with COVID-19: a national observational study. Epidemiol Infect. (2021) 149:1023. doi: 10.1017/S0950268821001023
44. Gardiner J, Oben J, Sutcliffe A. Obesity as a driver of international differences in COVID-19 death rates. Diabetes Obes Metab. (2021) 23:1463–70. doi: 10.1111/dom.14357
45. Tripathi S, Christison AL, Levy E, McGravery J, Tekin A, Bolliger D, et al. The impact of obesity on disease severity and outcomes among hospitalized children with COVID-19. Hosp Pediatr. (2021) 11:e297–316. doi: 10.1542/hpeds.2021-006087
46. Ciampo LA, Ferraz IS. del Ciampo IRL, Contini AA, Ued F. COVID-19 and obesity in childhood and adolescence: a clinical review. J Pediatr (Rio J). (2020) 96:546–58. doi: 10.1016/j.jped.2020.07.001
47. Shamah-Levy T, Cuevas-Nasu L, Romero-Martínez M, Gómez-Humaran IM, Ávila-Arcos MA, Rivera JA. Nutrition status of children, teenagers, and adults from national health and nutrition surveys in Mexico from 2006 to 2020. Front Nutr. (2021) 8:246. doi: 10.3389/fnut.2021.777246
48. Arous R, Djillali IS, Rouis NO, Boudiaf H, Amhis W, Ziane H, et al. High mortality of COVID-19 in children with cancer in a single center in Algiers, Algeria. Pediatr Blood Cancer. (2021) 68:898. doi: 10.1002/pbc.28898
49. Meena JP, Kumar Gupta A, Tanwar P, Ram Jat K, Mohan Pandey R, Seth R. Clinical presentations and outcomes of children with cancer and COVID-19: a systematic review. Pediatr Blood Cancer. (2021) 68:e29005. doi: 10.1002/pbc.29005
50. Madhusoodhan PP, Pierro J, Musante J, Kothari P, Gampel B, Appel B, et al. Characterization of COVID-19 disease in pediatric oncology patients: the New York-New Jersey regional experience. Pediatr Blood Cancer. (2021) 68:843. doi: 10.1002/pbc.28843
51. Delavari S, Abolhassani H, Abolnezhadian F, Babaha F, Iranparast S, Ahanchian H, et al. Impact of SARS-CoV-2 pandemic on patients with primary immunodeficiency. J Clin Immunol. (2021) 41:345–55. doi: 10.1007/s10875-020-00928-x
52. Belsky JA, Tullius BP, Lamb MG, Sayegh R, Stanek JR, Auletta JJ. COVID-19 in immunocompromised patients: a systematic review of cancer, hematopoietic cell and solid organ transplant patients. J Infect. (2021) 82:329–38. doi: 10.1016/j.jinf.2021.01.022
53. Millen GC, Arnold R, Cazier JB, Curley H, Feltbower RG, Gamble A, et al. Severity of COVID-19 in children with cancer: report from the United Kingdom paediatric coronavirus cancer monitoring project. Br J Cancer. (2021) 124:754–9. doi: 10.1038/s41416-020-01181-0
54. Dorantes-Acosta E, Ávila-Montiel D, Klünder-Klünder M, Juárez-Villegas L, Márquez-González H. Survival and complications in pediatric patients with cancer and COVID-19: a meta-analysis. Front Oncol. (2021) 10:82. doi: 10.3389/fonc.2020.608282
Keywords: SARS-CoV-2, comorbidity, COVID-19, mortality, pediatrics, Mexico
Citation: Solórzano-Santos F, Miranda-Lora AL, Márquez-González H and Klünder-Klünder M (2022) Survival analysis and mortality predictors of COVID-19 in a pediatric cohort in Mexico. Front. Public Health 10:969251. doi: 10.3389/fpubh.2022.969251
Received: 14 June 2022; Accepted: 08 November 2022;
Published: 16 December 2022.
Edited by:
Fariba Ahmadizar, University Medical Center Utrecht, NetherlandsReviewed by:
Alvaro Moreira, The University of Texas Health Science Center at San Antonio, United StatesCopyright © 2022 Solórzano-Santos, Miranda-Lora, Márquez-González and Klünder-Klünder. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Horacio Márquez-González, aG9yYWNpb2hpbWZnQGdtYWlsLmNvbQ==; Miguel Klünder-Klünder, a2x1bmRlcmtAZ21haWwuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.