 Xinfei Shi
Xinfei Shi Di Zong1,2
Di Zong1,2 Zhongqian Lu
Zhongqian Lu Shixue Li
Shixue Li Fanlei Kong
Fanlei Kong- 1Centre for Health Management and Policy Research, School of Public Health, Shandong University, Jinan, China
- 2NHC Key Lab of Health Economics and Policy Research, Shandong University, Jinan, China
Due to the acceleration of China's urbanization, the number of migrant older with children (MOC) continued to increase. This study aimed to clarify the effects of childcare disagreement with children, social support, and health status on unmet healthcare-seeking behavior among the MOC to Jinan, China. A cross-sectional study included 656 MOC (36.3% men and 63.7% women) using multi-stage cluster random sampling in Jinan, China. Childcare disagreement was evaluated by the differences between parents and grandparents on the diet, dressing, education, and childcare consumption. Social support was assessed using the social support rating scale (SSRS). Descriptive analysis, chi-squared test, and binary logistic regression were applied to analyze the association between childcare disagreement with children, social support, health status, and unmet healthcare-seeking behavior of the MOC. Approximately 41.3% of participants had unmet healthcare-seeking behavior. Logistic regression analysis showed that the MOC whose health status compared to last year get better were more likely to have unmet healthcare-seeking behavior, while who were women, had partial will of migration, hired a nanny, had smaller childcare disagreement with children on dressing, had smaller childcare disagreement with children on consumption, and had moderate social support, were less likely to experience unmet healthcare-seeking behavior. Recommendations were given to the government and family members to improve the health services-seeking behavior of the MOC.
Introduction
With the fast population aging in recent decades, China owned the largest number of older adults in the world (1). According to the latest data from the China National Bureau of Statistics, older adults aged 60 and more was 264 million in 2020, accounting for 18.7% of the total population of China. Of these, population aged 65 and older was 190 million, accounting for 13.50% of the total population of China. Compared with 2010, the proportion of people aged 60 and over has increased by 5.44%, and the proportion of people aged 65 and over has increased by 4.63% (2). Migrants were defined as individuals who have resided in the destination place for at least 6 months without local household registration status in China (3). In 2015, China's migrant population reached 247 million, accounting for 18% of the total population, and the trend of household mobility was increasing. According to the National Health and Family Planning Commission, the number of older migrants accounted for 7.2% of the total migrants in 2015. Of them, 43% migrated to take care of the younger generation (4). However, the disconnection of medical insurance between the inflow city and their hometown, unfamiliarity with the local medical environment, different rights to use healthcare services, etc. put the health of the migrant older with children (MOC) at risk. Maintaining and promoting the population health and providing healthcare services had always been the concern of the government (5). Thus, clarifying unmet healthcare behavior and needs of the MOC became very important for the government and healthcare service researchers.
Unmet healthcare needs are defined as a state in which individuals do not have access to healthcare when needed (6, 7). Healthcare-seeking behavior, defined as a “tool for investigating the individual's or population's interaction with the health system,” is fit-for-purpose to study how people perceive health and how they access and use available services to promote it (8). Insufficient opportunities to seek healthcare may lead to inappropriate or delayed healthcare, leading to adverse outcomes, such as a high prevalence of infectious diseases (9). Many studies reported the poor healthcare-seeking behavior, for example, in South Korea, and more than 14.5% of research subjects reported unmet healthcare needs since 2009 (10). Based on qualitative data from in-depth interviews with 90 rural-to-urban migrants, Hong's study found that migrants had limited access to regular medical services (11). Xie's study found that aged rural migrant workers who moved to the east or to first- or second-tier cities were less likely to seek medical care (12).
The older migrant who had disagreement with children may affect their healthcare-seeking behavior. A previous study showed that the living habits and consumption concept of the MOC were quite different from their children, and that they were easy to have friction with their children (13). A study of older immigrants in the USA found that those with more negative family relations had more doctor visits and were marginally more likely to use inpatient services, indicating that family conflict was a predictor of healthcare service use (14). Family conflict was also shown to be associated with mental health status and the use of healthcare services among Chinese Americans (15).
Social support refers to communication and contact between individuals and others for the purpose of obtaining information and comfort (16). The effect of social support on health has been widely reported. A study of Japanese older adults showed that respondents who received instrumental support were less likely to experience unmet healthcare needs, except for men aged 65–69 (17). In the USA, social support for older people has been shown to delay further deterioration in their health (18). Some scholars pointed out that social support was positively related to the health status of older people in developing countries (19). It was also found that medical decisions made by the older migrant was associated with their family support in China (20). Existing research also found that social support did not promote the physical health of older people in rural areas in China, but had significant positive effects on their mental health, especially in terms of emotional support (21).
Studies on the relationship between health status and unmet healthcare-seeking behavior mainly indicated that health status was an important factor affecting the healthcare-seeking behavior of migrants, yet limited studies focused on the MOC. It was found that the healthcare-seeking behavior of the older migrant in China were affected by self-rated health, income, employment status, and medical insurance participation no matter they were from rural to urban area or from urban to urban area (5). A study showed ~70.7% of the older migrant used inpatient services when they suffered from diseases requiring hospitalization (22). Residents of difficult-to-reach areas had a high prevalence of health problems and experienced social and structural barriers to healthcare services access (23). Patients with good self-rated health status were more likely to have an unmet need for outpatient services compared with those with poor health status (24).
To conclude, no study simultaneously explored the association between childcare disagreement with children, social support, health status, and unmet healthcare-seeking behavior, let alone took MOC as the object of research. Thus, this study aimed to clarify the effects of childcare disagreement with children, social support, health status on unmet healthcare-seeking behavior among the MOC in Jinan, China, and to further provide evidence-based suggestion for China and other developing countries facing similar challenges.
Methods
Data source
The data were collected in August 2020 in Jinan, Shandong province, China. Shandong province is located in eastern China, and Jinan City is the provincial capital of Shandong province. In 2020, its GDP will be 1.01 trillion Chinese Yuan (CNY) (≈157,285.51 million USD) (25). As of 1 July 2020, Jinan has jurisdiction over 10 districts and two counties (132 subdistricts and 29 towns) (26). By the end of 2020, the local resident population was 9.20 million, while the registered population was 8.06 million (27). In 2020, the migrants in Jinan were 3.29 million (28). Migrants aged above 60 and followed their children to Jinan City were the participants of this study.
Multi-stage cluster sampling was employed to select study participants. In the first stage of data collection, three districts were chosen from the 10 districts as the primary sampling units (PSUs), considering their economic development and geographic location. In the second stage, a total of three sub-districts were selected from each of the PSUs as the secondary sampling units (SSUs). In the third stage, three communities were selected from each of the SSUs. All older migrants who were over 60 years and followed their children to Jinan in these three communities constituted the total sample of this study.
A total of 33 college students became study investigators after training on study background information, questionnaire content, and social survey techniques. Of these students, 11 investigators came from Shandong University, 13 from Jinan University, two from Dongying Vocational College, and seven from Weifang Medical University. Participants were conducted face-to-face interviews for ~20 min to collect the data. Initially selected and 670 MOC were interviewed. However, 14 of them were excluded due to obvious logical errors in their answer or an unfinished questionnaire. A total of 656 participants eventually participated in the study.
Variables
Dependent variable
The dependent variable for the study was defined by asking respondents two questions, “Did you have the experience of not taking the outpatient service in case of disturbing your child?” and “Did you have the experience of not taking the inpatient service in case of disturbing your child?”, and it was calculated by combining these two variables to a new variable named unmet healthcare-seeking behavior. Unmet healthcare-seeking behavior had two options, “yes” and “no.” The “yes” refers to having at least one experience and “no” means the absence of these two experiences.
Independent variables
Demographic characteristics
Demographic characteristics included gender, age, body mass index (BMI), source of living expenses, marriage, employment, education level, monthly income, household monthly income, Hukou (commonly known as household registration, every person is assigned a type of Hukou based on his or her birthplace), will of migration, and hired a nanny. Participants' age is described by the mean and standard deviation (SD); education level including middle school and below, high school, and high school and above; and marriage status (married, unmarried, divorced, widowed, and others). BMI was calculated as weight divided by height squared (kg/m2). A BMI < 18.5 kg/m2 was considered underweight, between 18.5 and 23.9 kg/m2 was considered normal, between 24 and 27.9 kg/m2 was considered overweight, and ≥28 kg/m2 was considered obese (29). There were four types of migration space range: trans-county, trans-city, trans-provincial, and trans-national.
Childcare disagreement with children
Childcare disagreement was assessed by the childcare differences between parents and grandparents on diet, dressing, education, and consumption. Childcare disagreement with children was captured by four indicators, including “differences with childcare disagreement with children on diet (30),” “childcare disagreement with children on dressing,” “childcare disagreement with children on education (31),” and “childcare disagreement with children on consumption (13).” All of these variables had four options, “none,” “smaller,” “larger,” and “completely.”
Social support
Social support was assessed using the social support rating scale (SSRS), which was developed by Xiao Shuiyuan in 1994 for the Chinese population. It is composed of three dimensions: subjective support, objective support, and support utilization (32), which contains 10 kinds of support: friends, residents, neighbors, colleagues, family members, economy, comfort, talk, help, and activities. The higher the total social support score, the more social support the subjects received. The full score is 66 points; a total score of ≤22 points is the low level; 23 ≤ total score ≤44 is the medium level; 45 ≤ total score ≤66 is considered to be the high level (33).
Health status
Health status included “health status compared to peers (34)” and “health status compared to last year (35).” Respondents were asked about the variable of health status compared to peers “How is your health like compared to your peers?” Respondents were asked about the variable of health status compared to last year “How is your health like compared to last year?”
Statistical analysis
All data were analyzed with SPSS 26.0, and p < 0.05 was considered statistically significant. The percentages of the nominal variables were determined. Firstly, a descriptive analysis and the chi-squared test were performed to show the relationship between related variables and unmet healthcare-seeking behavior. Four binary logistic regression models were then adopted to clarify the associations between childcare disagreement with children, social support, health status, and unmet healthcare-seeking behavior. Meanwhile, crude odds ratios (ORs) and 95% confidence intervals (95% CI) were calculated. In Model 1, basic demographic information variables were included; Model 2 included basic demographic information and childcare disagreement with children; Model 3 included demographic, childcare disagreement with children, and social support; and Model 4 included demographic, childcare disagreement with children, social support, and health status.
Results
Demographic characteristics
Table 1 shows the basic demographic information of the 656 MOC in Jinan, China. Overall, 41.3% of participants had unmet healthcare-seeking behavior. Approximately 36.3% of participants were men and 63.7% were women. Almost half of participants had source of living expenses of child support (49.7%). The majority of the MOC had a monthly income level of CNY0–100 (USD0–15.5) (33.7%) and a household monthly income level of CNY101–600 (USD15.6–92.7) (29.6%). More than half of participants were willing to migrate (67.7%). Most participants had no nanny (99.1%). A statistically significant difference between gender, source of living expenses, monthly income, household monthly income, will of migration, hired a nanny, and unmet healthcare-seeking behavior were found based on the chi-squared test among the MOC in Jinan, China.

Table 1. Demographic characteristics of the migrant older with children (MOC).
Childcare disagreement with children
Table 2 shows childcare disagreement with children of the MOC. Most of the MOC had no childcare disagreement with children on diet (76.1%), 78.5% had no childcare disagreement with children on dressing, and most people had no childcare disagreement with children on education (79.7%). Approximately 72.4% of participants never had childcare disagreement with children on consumption. A statistically significant difference between childcare disagreement with children on diet, childcare disagreement with children on dressing, childcare disagreement with children on education, childcare disagreement with children on consumption, and unmet healthcare-seeking behavior was found based on the chi-squared test among the MOC in Jinan, China.
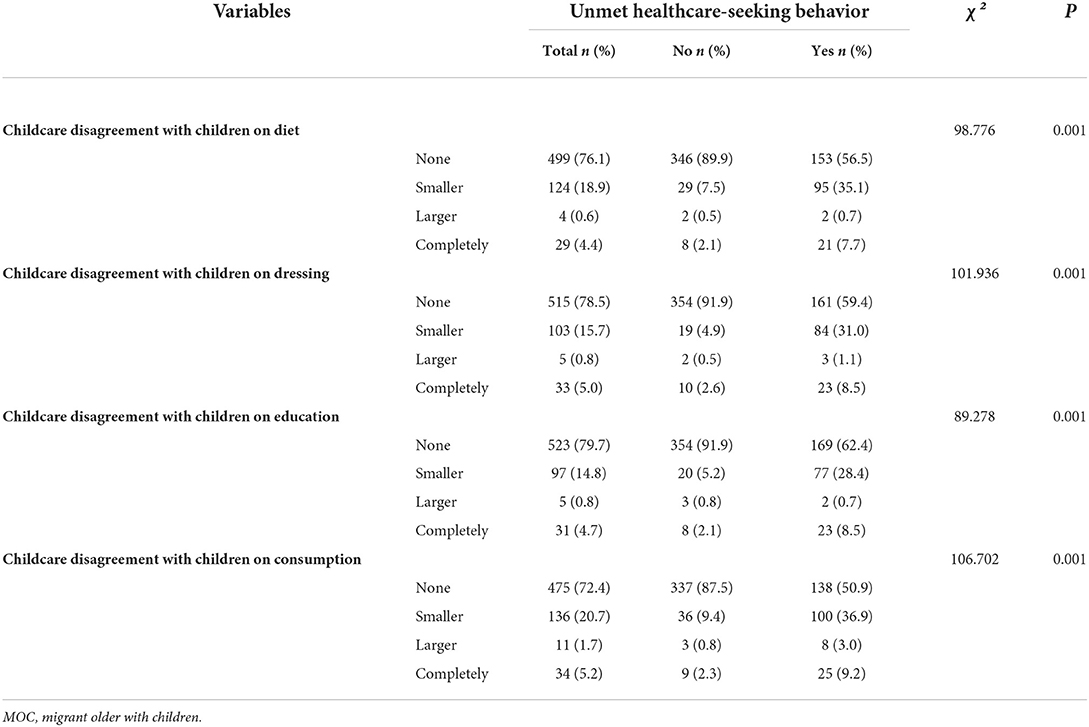
Table 2. Childcare disagreement with children of the MOC.
Social support and health status of the MOC
Table 3 shows the social support and health status of the MOC. Most of the MOC had a moderate level of social support (76.7%). More than half of participants had the same health status compared to peers (54.6%), and 67.5% of participants had the same health status compared to last year. A statistically significant difference between social support, health status compared to peers, and health status compared to last year, and unmet healthcare-seeking behavior was found based on the chi-squared test among the MOC in Jinan, China.
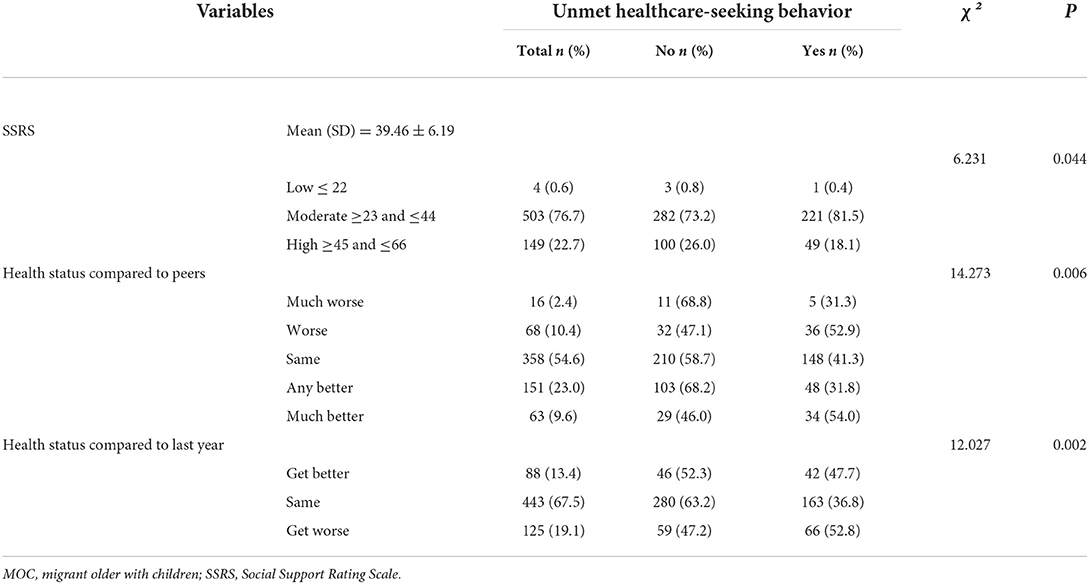
Table 3. Social support and health status of the MOC.
The relationship between demographic characteristics, childcare disagreement with children, social support, health status, and unmet healthcare-seeking behavior
Table 4 shows the relationship between demographic characteristics, childcare disagreement with children, social support, health status, and unmet healthcare-seeking behavior using logistic regression. The Bonferroni correction results showed that two variables (source of living expenses and will of migration) were statistically significant, implying that the robustness check was passed and that the results of the binary logistic regression in this study were acceptable.
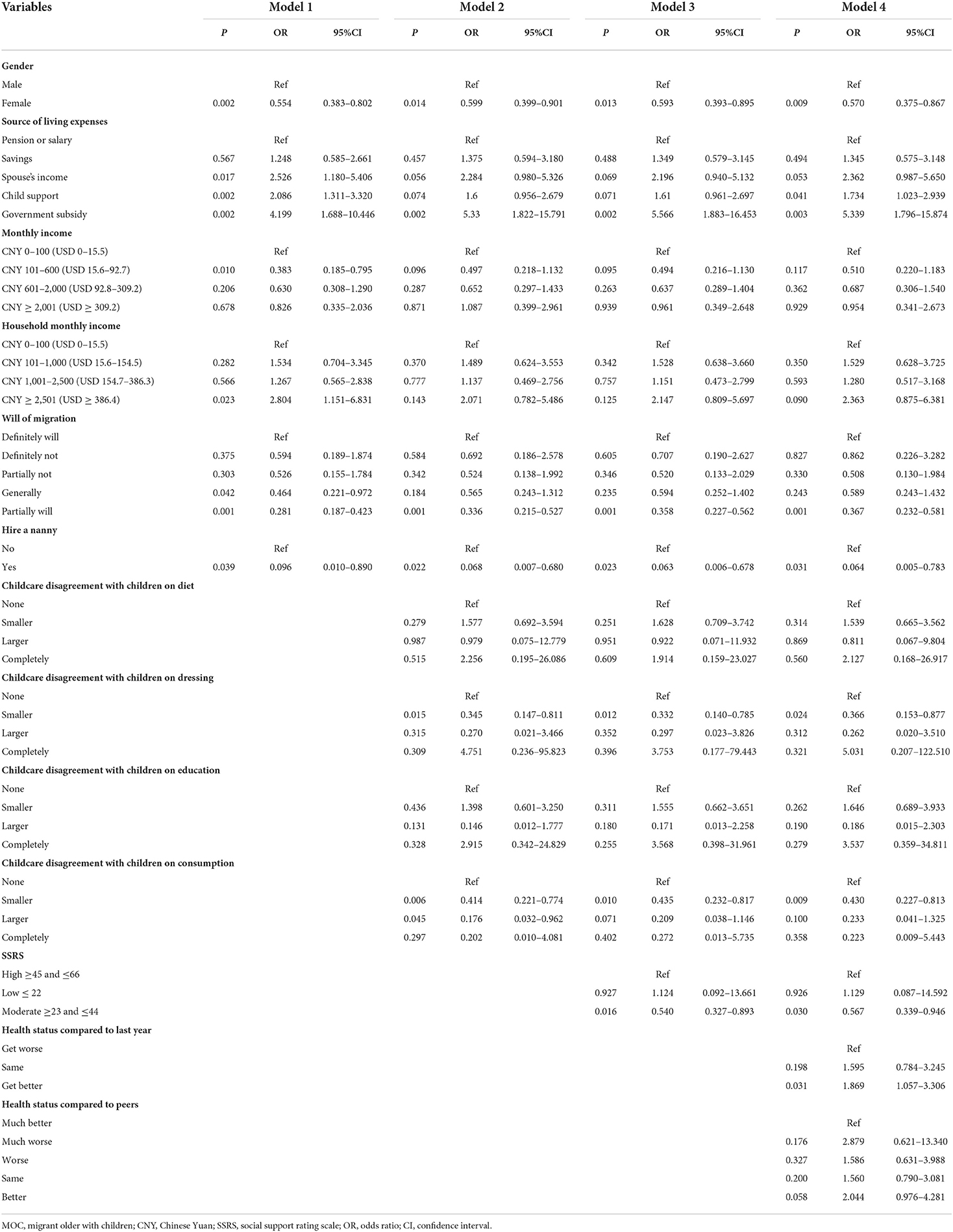
Table 4. The binomial logistic regression of demographic characteristics, disagreements, social support, health status, and unmet healthcare-seeking behavior of the MOC.
In Model 1, basic demographic information variables were included. The results showed that gender, source of living expenses, monthly income, household monthly income, will of migration, hiring a nanny, and unmet healthcare-seeking behavior among the MOC were statistically significant. When childcare disagreement with children variables was entered into Model 2, gender, source of living expenses, will of migration, and hiring a nanny remained significant, but the significance of monthly income and household monthly income disappeared. Childcare disagreement with children on dressing and childcare disagreement with children on consumption were also significant. In Model 3, social support was also significant.
In Model 4, female MOC were less likely to experience unmet healthcare-seeking behavior than men (OR = 0.570, 95%CI = 0.375–0.867, p = 0.009). The MOC with partial will of migration were less inclined to have unmet healthcare-seeking behavior than those with definite will of migration (OR = 0.367, 95%CI = 0.232–0.581, p < 0.001). The MOC who hired a nanny were less likely to report unmet healthcare-seeking behavior than those who did not have a nanny (OR = 0.064, 95%CI = 0.005–0.783, p = 0.031). The MOC who had smaller childcare disagreement with children on dressing were less likely to have unmet healthcare-seeking behavior than those who had none (OR = 0.366, 95%CI = 0.153–0.877, p = 0.024). The MOC who had smaller childcare disagreement with children on consumption were less inclined to have unmet healthcare-seeking behavior than those who had none (OR = 0.430, 95%CI = 0.227–0.813, p = 0.009). The MOC having moderate social support were less inclined to have unmet healthcare-seeking behavior than those having higher social support (OR = 0.567, 95%CI = 0.339–0.946, p = 0.030). The MOC whose health status compared to last year get better were more likely to have unmet healthcare-seeking behavior than those who did worse (OR = 1.869, 95% CI = 1.057–3.306, p = 0.031).
Discussion
Association between demographic characteristics and unmet healthcare-seeking behavior
The results of this study showed that 41.3% (n = 271) of the MOC experienced unmet healthcare-seeking behavior. This result was consistent with previous studies, which showed that migrants had a poor initiative in seeking treatment and were reluctant to seek medical care (36). The choice of healthcare-seeking behavior reflected the weak health awareness of the older migrant. Moreover, statistically significant correlations between gender, source of living expenses, will of migration, hiring a nanny, and unmet healthcare-seeking behavior were found in this study. Concerning gender, the results in Table 4 in this study showed that the MOC with women were less likely to report unmet healthcare-seeking behavior, this was similar with the study conducted by Zeng et al. who also found that female older individuals were more likely to utilize healthcare services (37). This may be due to women's relatively higher cautious health beliefs. Another study found that older men were significantly more likely to have inpatient disease compared to women, but there were no significant gender differences in decisions regarding hospitalization (38), which was different from our result. This might be due to the different research participants between our study and that study.
The results of this study showed that the MOC with source of living expenses from child support and a government subsidy were more likely to report unmet healthcare-seeking behavior than those with a pension or salary. This result was similar to a study conducted among the Karnataka older, which found that lack of earning capacity and financial dependence on others may cause them to forego treatment (39). The MOC with lower migration will (named as “partial will of migration” in Table 4) were less inclined to have unmet healthcare-seeking behavior than those with higher migration will (named as “definite will of migration” in Table 4). The result was different from Long's study, which found a positive association between willingness for long stay and the use of essential public health services (40). This might be because MOC with high migration may ignore or sacrifice their own healthcare service needs to provide better care for their younger generations (41). The MOC who hired a nanny were less likely to report unmet healthcare-seeking behavior than those did not have a nanny. This might be because when their grandchildren could be taken care by the nanny, it was more realizable and convenient for the MOC to seek healthcare services without disturbing their children's routine work and life arrangement.
Association between childcare disagreement with children and unmet healthcare-seeking behavior
The MOC who had smaller childcare disagreement with children on dressing were less likely to have unmet healthcare-seeking behavior than those who had none, while the MOC who had smaller childcare disagreement with children on consumption were also found to be less likely to have unmet healthcare-seeking behavior than those who had none. The above results differed from the study by Lu and Deng, which found no statistically significant effect of intergenerational economic support of children on older adults' healthcare-seeking behavior (42). With the fast social and economic development, more and more differences in values and behaviors appeared between parents and children. According to Jorgensen et al.'s study, intergenerational upward social mobility may lead to a stressful relation between adult offspring and their older parents (43). Taking into account that 87.5% of the MOC were from the rural area (as shown in Table 1), most of the children of MOC should have been firstly born in the rural area and are currently working in the big cities. This indicated an intergenerational upward social mobility between the MOC and their children, but also brought a negative impact on the intergenerational relationship between them, such as the different understandings of dressing and consumption of the baby in this study. Wu and Chiou's study showed that poor intergenerational relationships were associated with a worse mental state among the elderly (44). The worse mental status of the MOC furtherly made them to seek healthcare services, in other words, the MOC who had smaller childcare disagreement with children were less likely to have unmet healthcare-seeking behavior than those who had none.
Association between social support and unmet healthcare-seeking behavior
In this study, a significant association between social support and unmet healthcare-seeking behavior was observed, specifically, the current results demonstrated that participants with a moderate level of social support were less likely to experience unmet healthcare-seeking behavior than those with a high level. This was different from a previous study, which showed that low social support was associated with refraining from seeking medical care and medical non-adherence (45). Long's study showed that outer social support is positively associated with the use of health services in older migrants in China (46). Another research demonstrated that, compared to the medium- or low-level social support group, seafarers with a high level of social support had better scores in the general facet of health, quality of life, physical health, psychological health, social relations, and environment domains (33). Social support networks play a significant role in promoting healthy aging (47). High levels of social support were more beneficial to an individual's physical and mental health than lower levels of support among older adults (48). This may indicate that the MOC with a high level of social support were in good health and had a lower likelihood of healthcare-seeking behavior, while those with a moderate level of social support needed more healthcare-seeking behavior, that is, the MOC with a moderate level of social support were less likely to experience unmet healthcare-seeking behavior than those with a high level.
Association between health status and unmet healthcare-seeking behavior
The MOC whose health status compared to last year get better were more likely to have unmet healthcare-seeking behavior than those who worsened. The result was the same as the study by Shao, which found that migrants with moderate and severe status of symptoms have a higher likelihood of seeking healthcare services (49). This result was also the same as the study that showed people who thought their illness was serious were more likely to visit a doctor (50). This was different from a previous study, which showed that old-aged migrants in better health condition had a significantly sufficient utilization rate (51). It was important for the MOC to pay attention to their own health conditions and enhance their health status.
Implications
In view of these findings, the following policy recommendations were given. Firstly, the community could develop recreational programs to reinforce the relationship between the neighbors and friends of the MOC to increase their social support network. Secondly, low-educated and low-income MOC deserve more focus, the government should pay more attention to increase accessibility to healthcare services and medical subsidies to achieve health equality (52). Thirdly, the primary healthcare center is advised to conduct more health education on MOC, which could increase the awareness of the healthy lifestyle to promote their own health status and improve their healthcare-seeking behavior (53). Finally, children of internal or cross-nation older migrants should spend more time with family members and be filial to their parents to reduce the contradiction and create a harmonious family atmosphere, which was also the basic requirement of filial piety in traditional Confucianism Chinese culture (54).
Limitations
This study has some limitations. Firstly, individual health levels in this study were based on a self-report measure, which might have a certain impact on the results of our data analysis. Compared with a comprehensive health evaluation scale, a self-rated assessment of health is a subjective evaluation, which may be less objective and lead to recall bias. Secondly, the total number of family members was not collected in this study, and the household monthly income per capita could not be calculated. Thirdly, the use of variables in data analysis may need more consideration because continuous variable may be more acceptable in regression analysis rather than the categorical variable. Fourthly, this study was a cross-sectional design, so causality cannot be determined.
Conclusions
In this study, 41.3% of the MOC were found to have unmet healthcare-seeking behavior. The MOC whose health status compared to last year get better were more likely to have unmet healthcareseeking behavior; while who were women, had partial will of migration, hired a nanny, had smaller childcare disagreement with children on dressing, had smaller childcare disagreement with children on consumption, and had moderate social support, were less likely to experience unmet healthcare-seeking behavior. In summary, smaller childcare disagreement with children, moderate social support, and worse health status would result in less unmet healthcare-seeking behavior of the MOC. As an initial study on the effects of childcare disagreement with children, social support, and health status on unmet healthcare-seeking behavior among the MOC in Jinan, China, the results of this study provide evidence-based information for the government and the public on enhancing the healthcare-seeking behavior of the MOC.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
XS analyzed the data and drafted this manuscript. FK applied the fund to support this study, designed this study, completed the questionnaire design, supervised and combined the collected data, instructed the writing, performed statistical analysis and data processing, and provided comments on the modification of this manuscript. SL provided some valuable comments on the draft to further polish it. All authors read and approved the final manuscript. All authors read and agreed to the published version of this manuscript.
Funding
This study was supported and funded by the National Natural Science Foundation of China (No. 71804094), China Postdoctoral Science Foundation (No. 2016M592161), Natural Science Foundation of Shandong province (No. ZR2016GB02), Postdoctoral Science Foundation of Shandong province (No. 201603021), and The Fundamental Research Funds of Shandong University (Nos. 2015HW002 and 2018JC055).
Acknowledgments
The research team greatly appreciates the funding support and research participants for their cooperation and support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Li L, Yang Y. The impact of population aging to the growth of health care cost. Soc Security Stud. (2017) 10:27–39.
2. National Bureau of Statistics of China. Bulletin of the Seventh National Population Census (No.5). (2021). Available online at: http://www.gov.cn/guoqing/2021–05/13/content_5606149.htm (accessed January 11, 2022).
3. Liang Z, Ma Z. China's floating population: new evidence from the 2000 census. Popul Dev Rev. (2004) 30:467–88. doi: 10.1111/j.1728-4457.2004.00024.x
4. National Health and Family Planning Commission Migrant Population Service Center of China. China's Migrant Population Development Report.2016. National Health Commission of the People's Republic of China. (2016). Available online at: http://www.nhc.gov.cn/rkjcyjtfzs/pgzdt/201610/57cf8a2bbafe4b4d9a7be10d10ae5ecf.shtml (accessed January 11, 2022).
5. Song Q, Yin K. Study on the First Diagnosis choice and its influencing factors of the elderly migrants in China. Dong Yue Tribune. (2021) 42:136–47+92. doi: 10.15981/j.cnki.dongyueluncong.2021.01.014
6. Kim T, Soonim H. Changes in the financial burden of health expenditures by income level. Health Policy Manag. (2008) 18:23–48. doi: 10.4332/KJHPA.2008.18.4.023
7. Park H, Park J. Prevalence of unmet healthcare needs in adolescents and associated factors: data from the seventh Korea National Health and Nutrition Examination Survey (2016–2018). Int J Environ Res Public Health. (2021) 18:12781. doi: 10.3390/ijerph182312781
8. Mackian S, Bedri N, Lovel H. Up the garden path and over the edge: where might health-seeking behaviour take us? Health Policy Plan. (2004) 19:137–46. doi: 10.1093/heapol/czh017
9. Wang L, Wang X. Influence of temporary migration on the transmission of infectious diseases in a migrants' home village. J Theor Biol. (2012) 300:100–9. doi: 10.1016/j.jtbi.2012.01.004
10. Ko H. Unmet healthcare needs and health status: panel evidence from Korea. Health Policy. (2016) 120:646–53. doi: 10.1016/j.healthpol.2016.04.005
11. Hong Y, Li X, Stanton B, Lin D, Fang X, Rong M, et al. Too costly to be ill: healthcare access and health-seeking behaviours among rural-to-urban migrants in China. World Health Popul. (2006) 8:22–34. doi: 10.12927/whp.2006.18280
12. Xie Y, Guo Q, Meng Y. The health service use of aged rural-to-urban migrant workers in different types of cities in China. BMC Health Serv Res. (2021) 21:606. doi: 10.1186/s12913-021-06638-3
13. Aishui Y. The Study on Social Adaptation of the Elderly Immigrants from the Perspective of Intergenerational Relations–Take H Community in Kunming as an Example. (2018). p. 99.
14. Guo M, Sabbagh SN, Dong X, Tiwari A. Is family relations related to health service utilisation among older immigrants: evidence from chinese elderly in the United States. Health Soc Care Community. (2019) 27:215–25. doi: 10.1111/hsc.12642
15. Abe-Kim J, Takeuchi D, Hwang W-C. Predictors of help seeking for emotional distress among chinese americans: family matters. J Consult Clin Psychol. (2002) 70:1186–90. doi: 10.1037/0022-006X.70.5.1186
16. Wallston BS, Alagna SW, DeVellis BM, DeVellis RF. Social support and physical health. Health Psychol. (1983) 2:367–91. doi: 10.1037/0278-6133.2.4.367
17. Higuchi M, Suzuki K, Ashida T, Kondo N, Kondo K. Social support and access to health care among older people in Japan: Japan gerontological evaluation study (Jages). Asia Pac J Public Health. (2018) 30:425–36. doi: 10.1177/1010539518786516
18. Choi NG, Wodarski JS. The relationship between social support and health status of elderly people: does social support slow down physical and functional deterioration? Social Work Res. (1996) 20:52–63.
19. Chung S, Jeon H, Song A. The influence of social networks and social support on health among older Koreans at high risk of depression. Care Manag J. (2016) 17:70–80. doi: 10.1891/1521-0987.17.2.70
20. Luchan L. Off-site medical treatment for elderly floating population: behavior characteristics, support system and institutional guarantee. Popul Soc. (2019) 35:39–51. doi: 10.14132/j.2095-7963.2019.01.006
21. Bai Y, Bian F, Zhang L, Cao Y. The impact of social support on the health of the rural elderly in China. Int J Environ Res Public Healt. (2020) 17:2004. doi: 10.3390/ijerph17062004
22. Fu Y, Lin W, Yang Y, Du R, Gao D. Analysis of diverse factors influencing the health status as well as medical and health service utilization in the floating elderly of China. BMC Health Serv Res. (2021) 21:438. doi: 10.1186/s12913-021-06410-7
23. Tran BX, Nguyen LH, Nong VM, Nguyen CT. Health status and health service utilization in remote and mountainous areas in Vietnam. Health Qual Life Outcomes. (2016) 14:85. doi: 10.1186/s12955-016-0485-8
24. Peng B, Zhang H, Shi L, Ling L. Migration status and healthcare seeking behaviours among the Chinese labor-force: a nationally representative study. BMJ Open. (2019) 9:e031798. doi: 10.1136/bmjopen-2019-031798
25. Jinan's Gdp Breaks Trillion! Shandong Adds “Promoters”. (2021). Available online at: http://www.sd.chinanews.com.cn/2/2021/0126/77357.html (accessed January 23, 2022).
26. Jinan Municipal Government. Districts in Jinan. (2020). Available online at: http://www.jinan.gov.cn/col/col24699/index.html (accessed January 20, 2022).
27. Jinan Municipal Bureau of Statistics. Overview of Jinan City. (2022). Available online at: http://jntj.jinan.gov.cn/col/col18249/index.html (accessed April 21, 2022).
28. Jinan Municipal Bureau of Statistics. Bulletin of the Seventh National Population Census of Jinan. (2021). Available online at: http://jntj.jinan.gov.cn/art/2021/6/16/art_18254_4742896.html (accessed April 21, 2022).
29. National Health Family Planning Commission of the People's Republic of China. Criteria of Weight for Adults. (2013). Available online at: http://www.nhc.gov.cn/wjw/yingyang/201308/a233d450fdbc47c5ad4f08b7e394d1e8.shtml (accessed February 19, 2022).
30. Eli K, Howell K, Fisher PA, Nowicka P. A question of balance: explaining differences between parental and grandparental perspectives on preschoolers' feeding and physical activity. Soc Sci Med. (2016) 154:28–35. doi: 10.1016/j.socscimed.2016.02.030
31. Chen Hong, Ting G. Study on intergenerational differences between grandparents and parents in intergenerational education. Children Study. (2019) 29:46–63.
32. Xiao S. The theoretical basis and research application of social support rating scale. J Clin Psychiatry. (1994) 4:98–100.
33. Xiao J, Huang B, Shen H, Liu X, Zhang J, Zhong Y, et al. Association between social support and health-related quality of life among chinese seafarers: a cross-sectional study. PLoS ONE. (2017) 12:e0187275. doi: 10.1371/journal.pone.0187275
34. Kalyoncu IO, Tanboga I. Oral health status of children with autistic spectrum disorder compared with non-authentic peers. Iran J Public Health. (2017) 46:1591–3.
35. Peters E, Kasten M, Katalinic A, Waldmann A. [The health-related quality of life as measured with the Sf-12v1 in Elderly people living in Luebeck 2010/11 in comparison with the german norm data in 1994]. Gesundheitswesen. (2016) 78:49–55. doi: 10.1055/s-0034-1390420
36. Zhang J, Cai J, Huang Y, He Z, Tang G. China's floating population's healthcare utilization choices and influencing factors. Chin Gen Pract. (2021) 24:2008–14. doi: 10.12114/j.issn.1007-9572.2021.00.125
37. Zeng Y, Wan Y, Yuan Z, Fang Y. Healthcare-seeking behavior among chinese older adults: patterns and predictive factors. Int J Environ Res Public Health. (2021) 18:2969. doi: 10.3390/ijerph18062969
38. Jiang J, Xie Y. A study on the behavior and influencing factors of seeking medical treatment in the elderly floating population. J Nanjing Med Univ. (2020) 20:41–9. doi: 10.7655/NYDXBSS20200110
39. Rent PD, Kumar S, Dmello MK, Purushotham J. Psychosocial status and economic dependence for healthcare and nonhealthcare among elderly population in rural coastal Karnataka. J Midlife Health. (2017) 8:174–8. doi: 10.4103/jmh.JMH_46_17
40. Long C, Tang S, Wang R, Ji L, Wang Y, Wu T, et al. The migrating mediators and the interaction associated with the use of essential public health services: a cross-sectional study in Chinese older migrants. BMC Geriatr. (2020) 20:475. doi: 10.1186/s12877-020-01878-0
41. Chen H, Chi I, Liu R. Hospital utilization among Chinese older adults: patterns and predictors. J Aging Health. (2019) 31:1454–78. doi: 10.1177/0898264318780546
42. Lu J, Deng Q, Ceng Z, Zheng Y, Liu W. Effect of intergenerational support on medical seeking behavior of the elderly. J Fujian Med Univ. (2021) 22:39–42.
43. Jorgensen TSH, Nilsson CJ, Lund R, Siersma V, Fors S. Intergenerational relations and social mobility: social inequality in physical function in old age. Arch Gerontol Geriatr. (2019) 80:58–64. doi: 10.1016/j.archger.2018.10.006
44. Wu HY, Chiou AF. Social media usage, social support, intergenerational relationships, and depressive symptoms among older adults. Geriatr Nurs. (2020) 41:615–21. doi: 10.1016/j.gerinurse.2020.03.016
45. Berglund E, Lytsy P, Westerling R. Living environment, social support, and informal caregiving are associated with healthcare seeking behaviour and adherence to medication treatment: a cross-sectional population study. Health Soc Care Community. (2019) 27:1260–70. doi: 10.1111/hsc.12758
46. Long C, Wang R, Feng D, Ji L, Feng Z, Tang S. Social support and health services use in people aged over 65 years migrating within china: a cross-sectional study. Int J Environ Res Public Health. (2020) 17:4651. doi: 10.3390/ijerph17134651
47. Wu F, Sheng Y. Social support network, social support, self-efficacy, health-promoting behavior and healthy aging among older adults: a pathway analysis. Arch Gerontol Geriatr. (2019) 85:103934. doi: 10.1016/j.archger.2019.103934
48. Kim J, Lee JE. Social support and health-related quality of life among elderly individuals living alone in south korea: a cross-sectional study. J Nurs Res. (2018) 26:316–23. doi: 10.1097/jnr.0000000000000241
49. Shao S, Wang M, Jin G, Zhao Y, Lu X, Du J. Analysis of health service utilization of migrants in Beijing using Anderson health service utilization model. BMC Health Serv Res. (2018) 18:462. doi: 10.1186/s12913-018-3271-y
50. Huang M, Zhang H, Gu Y, Wei J, Gu S, Zhen X, et al. Outpatient health-seeking behavior of residents in Zhejiang and Qinghai Province, China. BMC Public Health. (2019) 19:967. doi: 10.1186/s12889-019-7305-0
51. Tang S, Long C, Wang R, Liu Q, Feng D, Feng Z. Improving the utilization of essential public health services by Chinese elderly migrants: strategies and policy implication. J Glob Health. (2020) 10:010807. doi: 10.7189/jogh.10.010807
52. Li X, Deng L, Yang H, Wang H. Effect of socioeconomic status on the healthcare-seeking behavior of migrant workers in China. PLoS ONE. (2020) 15:e0237867. doi: 10.1371/journal.pone.0237867
53. Li X, Yang H, Wang H, Liu X. Effect of health education on healthcare-seeking behavior of migrant workers in China. Int J Environ Res Public Health. (2020) 17:2344. doi: 10.3390/ijerph17072344
Keywords: unmet healthcare-seeking behavior, childcare disagreement with children, social support, health status, migrant older with children
Citation: Shi X, Zong D, Lu Z, Li S and Kong F (2022) Effects of childcare disagreement with children, social support, and health status on unmet healthcare-seeking behavior among the migrant older with children to Jinan, China. Front. Public Health 10:957619. doi: 10.3389/fpubh.2022.957619
Received: 31 May 2022; Accepted: 11 August 2022;
Published: 10 October 2022.
Edited by:
Tang Shangfeng, Huazhong University of Science and Technology, ChinaReviewed by:
Zhong Li, Nanjing Medical University, ChinaChengxu Long, King's College London, United Kingdom
Copyright © 2022 Shi, Zong, Lu, Li and Kong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shixue Li, c2hpeHVlbGlAc2R1LmVkdS5jbg==; Fanlei Kong, a29uZ2ZhbmxlaUBzZHUuZWR1LmNu