 Min Zhang
Min Zhang Jian Rong2†
Jian Rong2† Hong Ding
Hong Ding- 1Department of Health Service Management, School of Health Management, Anhui Medical University, Anhui, China
- 2Department of Scientific Research, The Second Hospital of Anhui Medical University, Anhui, China
Objective: This study aimed to explore the related factors of self-rated health (SRH) by using decision tree and logistic regression models among older adults in rural China.
Methods: Convenience sampling was employed with 1,223 enrolled respondents who met the inclusion criteria from 10 randomly selected villages in M County in China. The content of the questionnaire covered demographic characteristics, physical and mental health, sleep status, and risk of falling. The Pittsburgh Sleep Quality Index (PSQI) and the Morse Falls Risk Scale (MFS) were used to evaluate sleep status and risk of falling, respectively. The decision tree and logistic regression models were employed to analyze the related factors of SRH.
Results: Notably, 817 (68.7%) subjects had good SRH. The logistic regression model showed that living standard, alcohol consumption, sleep quality, labor, hospitalization, discomfort, the number of chronic diseases, and mental health were associated with SRH (P-value < 0.05), while the decision tree model showed that the number of chronic diseases, sleep quality, mental health, hospitalization, gender, and drinking were associated with SRH. The sensitivity and specificity of the logistic regression model were 67.7 and 75.5%, respectively, and the area under the ROC curve was 0.789 (0.763, 0.816); the sensitivity and specificity of the decision tree model were 71.5, and 61.4% respectively, and the area under the ROC curve was 0.733 (0.703, 0.763).
Conclusion: Decision tree and logistic regression models complement each other and can describe the factors related to the SRH of the elderly in rural China from different aspects. Our findings indicated that mental health, hospitalization, drinking, and sleep quality were the important associated factors.
Introduction
China has increasingly developed into an aging society, with 264 million people aged 60 and over, accounting for 18.70% of the total population (1). At the same time, there is an inversion of population aging in urban and rural areas. The proportion of the population aged over 60 and 65 years in rural China is 23.81 and 17.72%, respectively, with 7.99 and 6.61 percentage points higher than those in urban areas (2). With the change in physiological and social roles, the prevalence of noncommunicable chronic diseases, disability, and social role function loss has increased significantly in the elderly (3). Compared with the elderly in urban locations, the elderly in rural areas have poorer medical and health conditions, material living standards, and self-care awareness (4, 5). Therefore, how to improve the health of the elderly in rural areas is one of the major challenges facing Chinese society.
Self-rated health (SRH) is an individual's subjective assessment of his or her health status and expectations (6, 7) and is also a recommended health testing indicator by the World Health Organization (8). Based on an overview of an individual's current health status and relevance to future health outcomes, SRH has been shown to predict mortality, morbidity, etc. in various countries/settings (9–11). SRH is a composite concept that reflects not only aspects of an individual's physical, psychological, and social adaptations but also health behaviors and cultural beliefs (12, 13).
Self-rated health is affected by many factors, such as socio-demographics, including gender, age, income level, and education level (14, 15). Health indicators cover factors such as disease, drug abuse, and mental health (16, 17). Studies have shown that suffering from one or more chronic diseases could be an important factor in poor SRH status (18). In addition, studies have shown that smoking, alcohol consumption, physical activity, and other daily behaviors and lifestyles were related to SRH (19). Sleep quality was significantly related to SRH, as shown by Min-Fang Hsu's study (20). Furthermore, the risk of poor SRH increases with the number of chronic diseases (NCDs), mental health symptoms, and decreased social support (18). From the perspective of etiology, the influencing factors of diseases can be divided into proximal factors that directly play a role and distal factors that indirectly play a role; thus, many of the above factors are not independent but synergistic [e.g., low physical activity + age + smoking can all lead to cardiovascular disease and therefore to low SRH (21)].
Logistic regression and decision tree models can be used to construct predictive models for influencing factors (22, 23). Although logistic regression highlights the main effects of influencing factors, it does not deal well with interactions or provide good decision recommendations. In contrast, the decision tree model breaks the traditional linear processing method by eliminating the collinearity among variables and including a series of logical decisions. Each path from the root nodes to the leaf nodes corresponds to a rule. The importance of the indicators is ranked to determine the main influencing factors. However, the classification effect varies with the number of nodes, thus it could be less stable and forbid main effect analysis. As a result, the interpretation of the results is limited. The joint use of the decision tree and logistic regression models can complement each other and improve the analysis performance.
A combination of decision tree model and logistic regression is still lacking at home and abroad to analyze the factors related to the SRH status of rural elderly. In this study, focusing on a population sample of older adults in a rural area of Anhui Province, we proposed two models to analyze the factors related to SRH in older adults to gain an in-depth understanding of the health status of older adults and provide a reference basis for improving the health and quality of life of rural older adults.
Methods
Study design and data collection
A cross-sectional study was carried out from July to August 2021 in Anhui, China. Anhui Province is located in the central region of China and is one of the major agricultural provinces. The population aged 60 years and above is 11.469 million, accounting for 18.79%; of which, 9.159 million are aged over 65 years, accounting for 15.01%.
Using a convenience sampling method, a total of 10 villages in two townships in M County were selected as the study sites, taking into account the different economies and populations, and the rural elderly who met the inclusion criteria were selected as the subjects. Inclusion criteria were as follows: (1) age ≥ 60 years, (2) normal hearing, clear consciousness, and basic communication skills, and (3) voluntary participation in this study. With the assistance of local village committees and village doctors, five postgraduates from Anhui Medical University who had been uniformly trained conducted a face-to-face survey with each subject. Prior to the survey, the purpose and procedures of the study were verbally presented to all respondents, and verbal consent was obtained from them. The question-and-answer technique was adopted, and the investigator filled in the questionnaire according to the answers. A total of 1,223 questionnaires were distributed in this study, and 1,189 valid questionnaires were recovered, with an effective recovery rate of 97.2% (1,189/1,223).
Measurement of sleep quality
The Pittsburgh Sleep Quality Index (PSQI) was used to evaluate the sleep quality of the survey object in the past month. The scale contains 18 items measuring the following seven factors: sleep quality, sleep onset time, sleep duration, sleep efficiency, sleep disturbance, hypnotic medication, and daytime dysfunction. The score range for each factor is 0 to 3, and the cumulative score for each factor is the total PSQI score, with a total score range of 0 to 2l. A total score of ≤ 7 indicates good sleep quality, and >7 indicates poor sleep quality. This study verified that the Chinese version of the PSQI has good reliability and validity, with an overall reliability coefficient of 0.82 to 0.84 (24).
Measurement of mental health
Mental health was assessed using the 12-item General Health Questionnaire (GHQ-12), which is widely used in epidemiological surveys and screening for mental disorders in community groups. The scale consists of 12 items, and each item contains the following four options: (1) not at all, (2) the same as usual, (3) more than usual, and (4) much more than usual. The GHQ-12 is scored as 0 for those who choose to answer the first two items and 1 for those who answer the last two. A total score of 3 on the GHQ-12 is used as the threshold, i.e., a score of ≥3 indicates poor mental health. The GHQ-12 of the Chinese version has good reliability and validity, with Cronbach's alpha coefficients ranging from 0.75 to 0.82, and retest correlation coefficients ranging from 0.82 to 0.85 (25).
Measurement of risk of falling
The risk of falling was assessed using the Morse Falls Risk Scale (MFS). The scale assessment was not time-comsuming, was simple, operational, and had good reliability and validity with Cronbach's alpha coefficient of 0.891. Items and scoring criteria were as follows: history of falls (none = 0, yes = 25); 1 or more disease diagnoses (none = 0, yes = 15); use of mobility aids (none need, bed rest or nurse assistance = 0, crutches, walker, cane = 15, walking with furniture = 30); receiving medication (none = 0, yes = 20); gait (normal/immobility = 0, weakness = 10, severely frail = 20); and cognitive status (voluntary behavior = 0, no control = 15). A total score of <25 was considered low risk, 25–45 for moderate risk, and ≥45 for high risk of falling.
Measurement of other variables
Other variables included basic demographics and health-related information. Specifically, the following were included: gender (female and male), age (60–69, 70–79, and ≥80 years), marital status (stable, unstable consisting of divorce, widowed, and unmarried), residence status (living alone living with others: living with children, relatives, caregivers, etc.), the education level (illiterate and junior high school), source of income (employment income, child support, and government subsidy), smoking (yes or no), drinking: drinking alcohol twice or more a week for 1 year (yes or no), taste for food (moderate, light, and salty), living standard (good and poor; good: self-assessed living standard is very good, good, and average; poor: self-reported poor or very poor), labor: the daily physical work of the respondents (heavy and easy), BMI (healthy, overweight, and obese; healthy: 18.5–23.9, overweight: ≥24, obese: ≥28). Information was also collected on noncommunicable diseases, physical discomfort (within 2 weeks), and hospitalization (within 1 year).
The dependent variable in this study is SRH, which was measured and analyzed in responding to the questionnaire item “How do you feel about your current health status?” The answers to this question were set to five options: “very good,” “good,” “fair,” “bad,” and “very bad.” The first three options were categorized as “good,” while the last two were categorized as “poor.”
Statistical analysis
First, we used chi-square tests to examine differences between the different SRH groups (good and poor) and used ratios and percentages to describe the demographic characteristics of the participants.
Second, we tested correlations among the variables (Figure 1). The variables that were statistically significant in the chi-square test included logistic regression and decision tree models. To obtain the optimal model, we chose the exhaustive CHAID growth method, with a maximum growth depth of 3. The CHAID growth method uses the chi-square test or variance analysis principle to optimally segment data according to variable type and automatically judges and groups multivariate contingency tables according to P-value to generate a multi-tree, which can efficiently mine the main influencing factors. According to the variance expansion factor (VIF) results, there was no evidence of multicollinearity in the logistic regression model, and no factor exceeded the critical value (Supplementary Table S1).
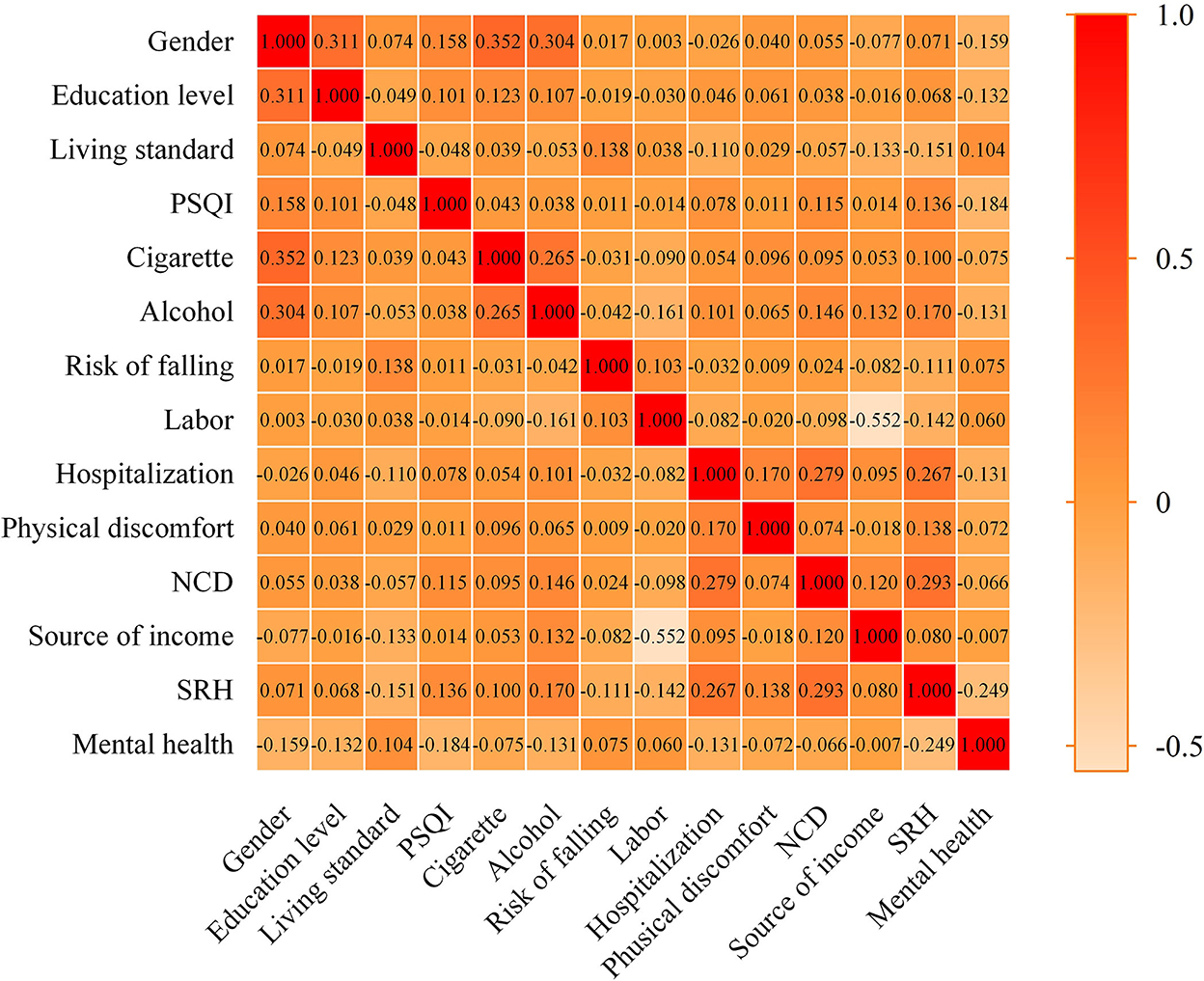
Figure 1. Correlation between variables.
Finally, the prediction effects of logistic regression and decision tree models were compared by constructing a subject operating characteristic curve (ROC curve), Z-value was calculated based on the area under the curve and standard deviation, and the corresponding P-value was matched to determine the difference between the two statistical models. The check level was set at α = 0.05.
All statistical analyses were performed using SPSS statistical software version 26. Two-tailed P-value of < 0.05 was considered statistically significant.
Results
Characteristics of participants
The general demographic characteristics of the respondents are shown in Table 1. A total of 1,189 subjects were included in this study, of which 817 subjects self-assessed good health. Significant statistical differences were found between the two groups on the dimensions of gender, education level, smoking, drinking, taste for food, physical labor, source of income, mental health, risk of falling, sleep quality, and NCD (P-value < 0.05). Among the 817 subjects, 51.8% (423/817) were female, 77.7% (635/817) did not smoke, 70.5% (576/817) did not drink, 66.6% (544/817) had not been hospitalized in the past year, and 55.3% (452/817) had economic income from their own work. At the same time, 86.3% (705/817) of the survey respondents who rated themselves as the ones having good health had a higher living standard.
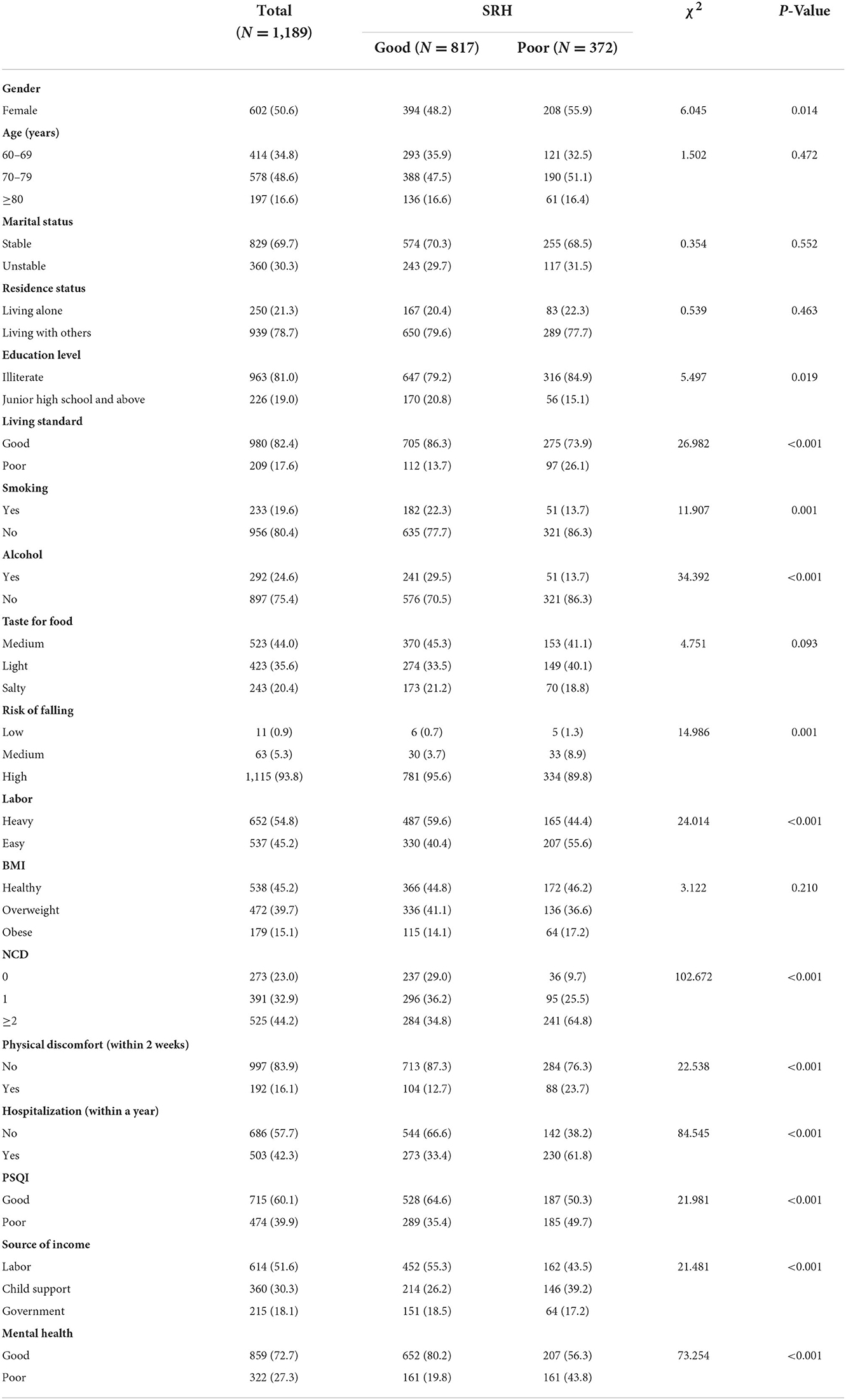
Table 1. General characteristics of the respondents (N = 1,189).
Results of logistic regression analysis
Table 2 shows the variable assignments. The results of multivariate logistic regression analysis (Figure 2) showed that living standard, drinking, PSQI, labor, hospitalization (within a year), discomfort (within 2 weeks), NCD, and mental health were influencing factors for SRH of the elderly (P-value < 0.05). In addition, the model did not show any statistically significant association between the risk of falling and SRH. Compared with the control group, the higher standard of living (OR = 0.476, 95% CI: 0.327–0.692), heavier physical labor (OR = 0.687, 95% CI: 0.486–0.971), and better mental health status (OR = 0.410, 95% CI: 0.302–0.558) were associated with better SRH. No drinking (OR = 1.701, 95% CI: 1.149–2.518), poor PSQI (OR = 1.397, 95% CI: 1.045–1.867), hospitalization (within a year; OR = 2.163, 95% CI: 1.619–2.890), discomfort (within 2 weeks; OR = 1.739, 95%CI: 1.209–2.500), NCD = 1 (OR = 1.647, 95%CI: 1.035–2.619), and NCD ≥ 2 (OR = 03.967, 95%CI: 2.558–6.153) were risk factors for SRH.
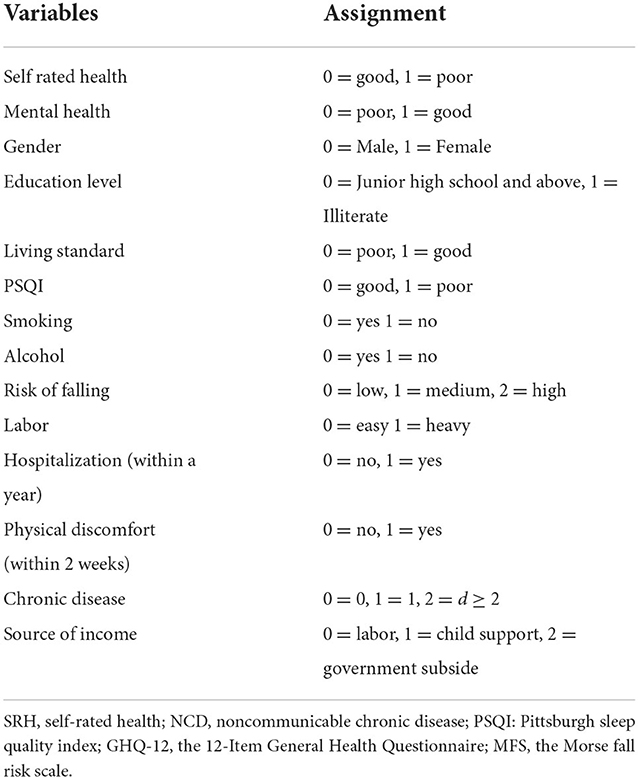
Table 2. Variable assignment table.
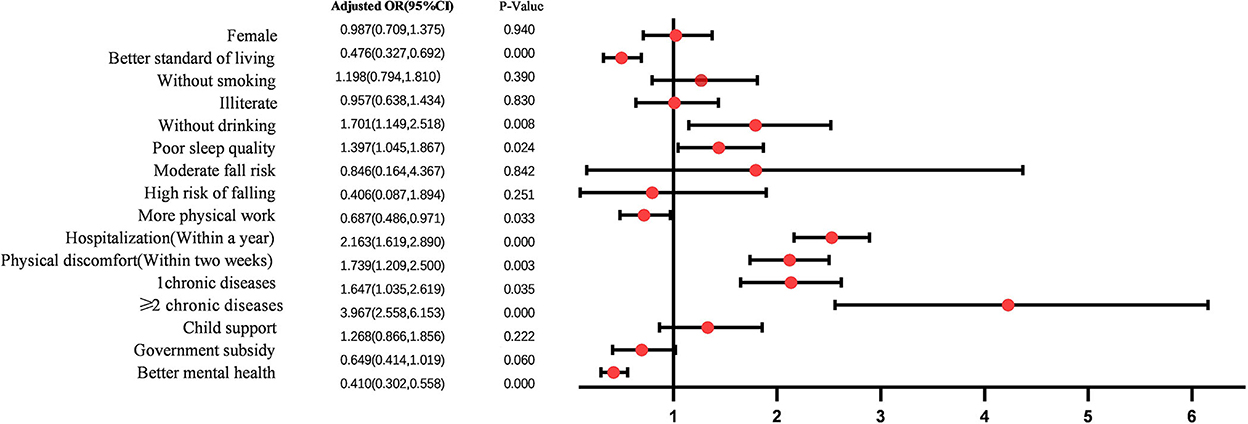
Figure 2. Logistic regression analysis results.
Results of classification and regression tree model
The results of the decision tree model are shown in Figure 3. SRH was mainly related to NCD, PSQI, mental health, hospitalization, gender, and drinking. NCD was the primary influencing factor for SRH. Taking NCD as the root node, the probability of having good SRH without chronic diseases in older adults is 86.85%. SRH was higher in women without chronic disease and with better sleep quality. Conversely, those with two or more chronic diseases, hospitalization within 1 year, and poor mental health have poor SRH.
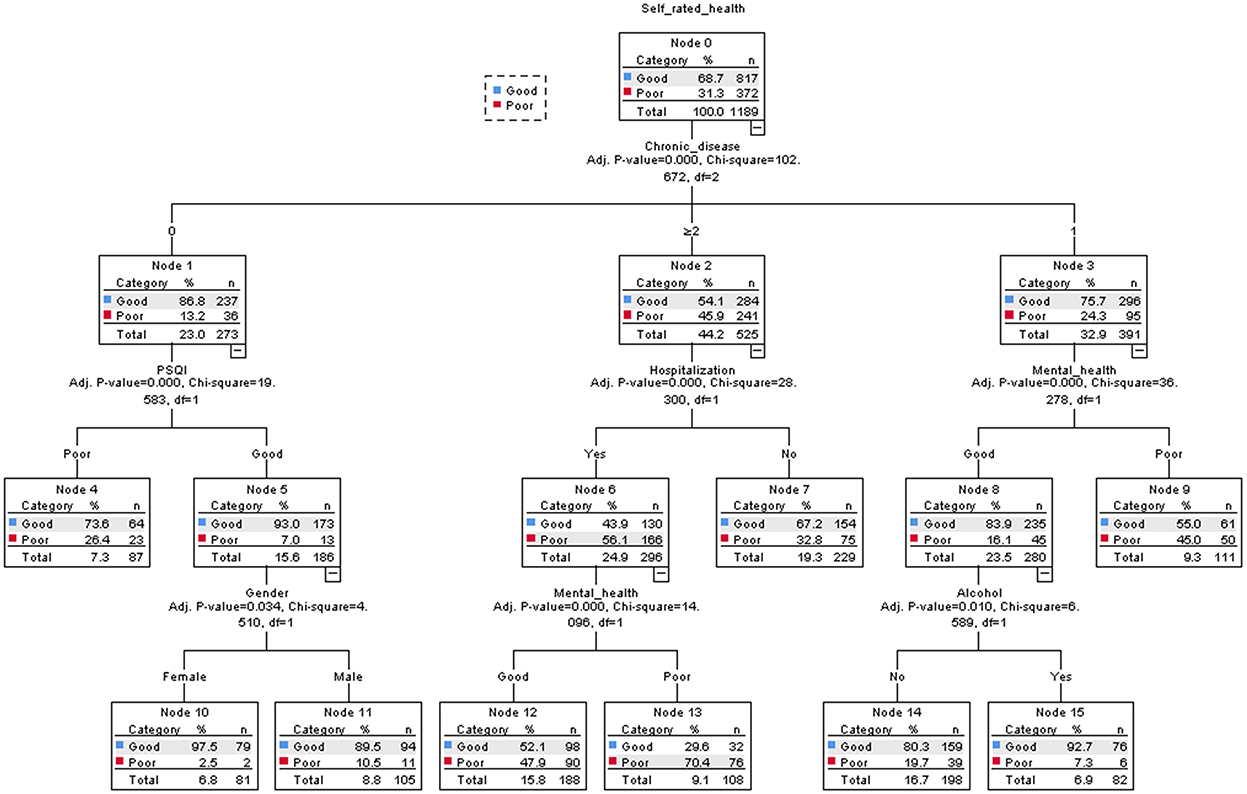
Figure 3. Classification and regression tree model (N = 1,189).
Comparison of model prediction results
According to the predicted probabilities obtained by the two models as test variables, ROC curves were drawn, respectively, as shown in Figure 4. The ROC curves of both models are far away from the diagonal line, indicating that the model has a certain predictive effect. The ROC curves of both models are almost coincident, indicating that the classification effects of the two models are similar. However, it should also be noted that there are differences between the two models. The influencing factors in the logistic regression model, living standard, discomfort, and labor are eliminated in the classification decision tree model, while gender in the decision tree model is not statistically significant in the regression model.

Figure 4. ROC curve predicted by decision tree and logistic regression model.
The common influencing factors screened by the logistic regression model and decision tree model were NCD, mental health, hospitalization, drinking, and PSQI. The logistic regression model had a sensitivity of 67.7%, a specificity of 75.5%, and an area under the ROC curve of 0.789 (0.763–0.816); the decision tree model had a sensitivity of 71.5%, a specificity of 61.4%, and the area under the ROC curve was 0.733 (0.703–0.763). The difference between the two models is statistically significant (Z = −2.729, P = 0.003), and the prediction effect of the two models was moderate (0.7–0.9).
Discussion
In this study, the prevalence of poor SRH was 31.3%. The prevalence of reported poor SRH in older adults varies in different studies. Ana M Pereira-de-Sousa found that 52.9% of Spaniards rated their health as “good” or “very good,” compared to 19% of Portuguese (P < 0.01) (26). A Chinese study showed that 38.33% of the study subjects reported good/excellent SRH (27). The percentage of subjects reporting good SRH in this study is somewhat higher than in the other studies discussed, possibly due to differences in national culture and historical background, as well as differences in assessment scales and samples. In general, due to age, physical function degradation, and other reasons, the elderly tend to choose a reference object in their self-assessment of health, such as relatives and friends, neighbors, and other elderly people of the same age group. Even when they are ill, they tend to adjust the reference object to maintain a more positive health self-assessment. The level of an individual's SRH depends on the selected reference group. This theory is often used to explain why people have a more positive evaluation of their own health (28).
Significant variables in the logistic regression model were different from the nodal variables that entered the decision tree model. The decision tree analysis did not reflect the effects of three factors: living standards, discomfort (within 2 weeks), and labor. The reason might be that the logistic regression model expresses the correlation of variables while the decision tree takes into account the interactions and relationships among variables and shows the function form of variables in each subcategory in detail, providing a wealth of information.
Influence of personal characteristics on SRH
In this study, gender, age, and marital status were not significantly associated with SRH, but the proportion of women was 11.8% higher than that of men in the 372 unhealthy samples, stable marital status was higher by 37% than those with an unstable marital status, and people aged 70–79 accounted for half of the unhealthy population. Elderly people with a high standard of living, heavy physical labor, and no medical treatment within 2 weeks tend to have higher levels of SRH, which is consistent with previous studies (29, 30).
The higher SRH rates are among older adults with better living standards than those with poorer living standards, suggesting that the living standards of the elderly have a significant positive effect on their health and that improved living conditions can improve the level of SRH. An adequate source of income is an important material basis for health. On the one hand, living standards directly affect health; on the other hand, they affect health through intermediary mechanisms such as lifestyle, psychological factors, and access to health resources. As a form of social activity, physical labor can increase social opportunities for the elderly, achieve group-coordinated development, and improve SRH levels (7). Elderly people who have not seen a doctor within 2 weeks may have higher physical fitness and therefore are more likely to have higher SRH.
NCD and SRH
Specifically, older adults who suffer from multiple chronic diseases may have lower SRH. This further confirms the consistency between the SRH and the objective state of the body. Henrike Galenkamp's study evaluated the impact of heart disease, peripheral atherosclerosis, stroke, diabetes, and other diseases on SRH and found an association between comorbidities and SRH (31). The association was nonlinear, with the effect of the individual disease being greater than the additive effect of concurrent diseases. However, starting with the second disease, the incidence of comorbid multi-morbidities was cumulatively negatively associated with SRH. At the same time, studies have shown that the elderly with multiple chronic diseases have deteriorating mental and physical health and can negatively affect SRH (32). One possible explanation for this result is that SRH in the elderly is affected by objective health, and chronic diseases bring problems such as pain, insufficient self-care ability, limitation in daily activities, and dependence on or incompatibility with drug therapy. At the same time, rural older adults with chronic diseases often require medication and hospitalization, which makes them more likely to be impoverished by their illness, thereby reducing the level of SRH. It is necessary to further improve the community supervision of chronic diseases, refine the management of chronic diseases, regularly carry out a physical examination of middle-aged and elderly people, and do a good job in community supervision of chronic diseases to further improve the health level of the population (33).
Mental health and SRH
In short, people with goodmental health have higher SRH when compared to those with poor mental health. This is consistent with Mikyong Byun's finding that depression appeared to be the strongest predictor of negative SRH (34). Death of a spouse, chronic diseases, and reduced interpersonal communication can all lead to mental health problems. Long-term experienceof negative emotions is consistent with SRH deterioration (35). People who have been experiencing negative emotions for a long time are more likely to subjectively believe that they are in poor health due to the hypochondria effect, thus exaggerating physical health problems. People with poor mental health may suffer from dull, irritable, and even depressed moods, are tired of social communication, and lack physical activity, resulting in poorer health status.
Hospitalization and SRH
Self-rated health tended to be more negative in older adults hospitalized within 1 year, which is consistent with the findings of Wang (36), further confirming that SRH is consistent with objective physical status (37). In this study, the elderly in rural areas were characterized by a high prevalence of chronic diseases and a low level of education. They lack knowledge about chronic diseases and their prevention and control, as well as the awareness of timely medical treatment and active use of health services (38). By the time medical care is consciously sought, the disease may have developed to a complex and severe level, therefore, SRH is lower in older adults with a history of hospitalization within 1 year. Tertiary prevention of chronic diseases to reduce their prevalence of chronic diseases and control their further development is an effective way to improve the SRH.
Drinking and SRH
An interesting phenomenon was found in this study that drinking is a protective factor for SRH. This is consistent with the findings of Li Tongyao and Riediger (7, 39). This may be due to “Optimistic bias,” that is, drinkers believe that drinking is less harmful to them than other drinkers. In addition, it may be because drinkers are in better physical condition to tolerate a certain amount of drinking and that there are social benefits to drinking (40). At the same time, those in poor health are more inclined to avoid alcohol consumption. Moderate drinking can produce positive emotional effects and protect against cardiovascular disease, but it is not recommended to drink to improve health. In view of this, relevant departments must implement health education, gradually deepen health promotion work, effectively advocate for the elderly to develop healthy habits, quit smoking and limit alcohol, eat well, and improve levels of daily exercise.
PSQI and SRH
Among the rural elderly population, those with better PSQI had higher SRH. This result is similar to a Japanese study of adequate sleep (COR = 5.22, P < 0.001), which was associated with high SRH (41). Anna Andreasson's study (42) showed that people with good sleep quality reported significantly higher SRH than those with moderate sleep quality (95% CI = 0.48, 0.89, P < 0.001). Insufficient sleep duration can affect circadian rhythms, impair insulin sensitivity, increase insulin resistance, decrease glucose tolerance, and lead to elevated levels of catecholamines, cortisol, and sympathetic activity, which are associated with various diseases (43). Also, poor sleep quality may increase daytime fatigue, leading to negative events and negative emotions, which can affect SRH levels. Attention should be paid to the role of sleep quality in promoting the health of the elderly. Through psychological counseling, knowledge explanation, and other means, the elderly can be helped to develop good sleep habits. Attention should always be paid to helping a pleasant mental state be maintained in order to improve physical and mental health.
Strengths and limitations
Our study has the following advantages. First, the effective response rate in this study was 97.2% (1,189/1,223), and it is known that the results of studies with a highly effective response rates are more reliable. Second, the combined use of decision tree and logistic regression models is beneficial, where each model can be learned from and where the strengths of each one can complement the other. The combined use of both can allow analysis of the factors affecting the SRH of the elderly at different levels and help to quickly find the most influential combination of factors. Taking advantage of the intuitive effect of the decision tree, ease of interpretation, and generation of partial classification rules, combined with the logistic regression model giving parameter estimates and hypothesis testing results for each variable, the main effect variables were filtered out through the logistic regression model, and then using the decision tree, the model further investigated the interactions between the variables.
However, the limitation of this study is that the selected samples were only from the rural elderly population in 10 villages of M county. In addition, this is a cross-sectional study with a limited inference of causality, which needs to be verified by a high-quality cohort study. At the same time, our study did not include all the potential factors of SRH, which will be considered in future studies.
Conclusion
The SRH of the rural elderly is affected by many factors such as personal characteristics, health level, behavior, and lifestyle. This study combined logistic regression and decision tree models to screen key influencing factors affecting SRH in older adults, including NCD, mental health, hospitalization, alcohol consumption, and PSQI. This study may be helpful to plan and take measures to improve SRH in older adults and promote active aging. Grass-roots medical and health institutions in rural areas should make full use of existing health resources to improve the community health care network and strengthen the rehabilitation and treatment of patients with chronic diseases, which is conducive to the improvement of the health status of the elderly in rural areas. With an increase in age, the elderly pay more attention to social environment and the degree of psychological and emotional pleasure; thus society and families should provide more care to the elderly to help them achieve healthy aging.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
All participants in this study were fully informed about the purpose and methods of this study. The purpose and procedures of the survey were explained to all respondents prior to conducting the survey, and informed consent for the survey was secured from all respondents. For illiterate respondents, informed consent was also obtained from the guardians.
Author contributions
MZ conceptualized the study and wrote the manuscript. JR, SL, and BZ contributed to the study design, data collection, data processing, and statistical analysis. JR contributed to the literature review. MZ, JR, YZ, and HW revised the manuscript. All authors reviewed the manuscript and approved the final manuscript.
Funding
This research was funded by the Research Projects of Humanities and Social Sciences in Colleges and Universities of Anhui Province (No. SK2018A0165) and the Doctoral Fund Project of Anhui Medical University (No. XJ201545).
Acknowledgments
The authors would like to appreciate the involvement of the participants who volunteered in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.952714/full#supplementary-material
References
1. National Bureau of Statistics. Main Data of the Seventh National Population Census [DB/OL]. Available online at: http://www.stats.gov.cn/tjsj/zxfb/202105/t20210510_1817176 (accessed October 28, 2022).
2. People's Daily Online. National Bureau of Statistics: The Proportion of the Population Aged 60 Above Reached 18.7%. (2021). Available online at: https://baijiahao.baidu.com/s?id=1699433233776674836&wfr=spider&for=pc (accessed January 21, 2022).
3. Li X, Zhang X, Ren Z, Fan X, Guo X, Shi H, et al. Self-rated health status and influencing factors among floating elderly population in Western China. Med Soc. (2021) 34:1–5. doi: 10.13723/j.yxysh.2021.04.001
4. Li F, Gao X. Retrospective analysis of health risk generation mechanism of rural elderly under the background of common prosperity. Lanzhou Acad J. (2022) 09:135–47. doi: 10.3969/j.issn.1005-3492.2022.09.011
5. Ran X, Hu H. Urban-rural disparity, digital divide and health inequality of the elderly. Popul J. (2022) 44:46–58. doi: 10.16405/j.cnki.1004-129X.2022.03.004
6. Li C. Application of random effects generalized ordered probit model in the research of the factors affecting self-rated health in China. Chin Health Econ. (2021) 40:75–7.
7. Li T, Bing J, Li X, Xue Q, Zhang Y. Self-rated health status of elderly people living alone in China and its influencing factors. Mod Prev Med. (2021) 48:2027–31.
8. De Bruin A, Picavet HS, Nossikov A. Health interview surveys: towards international harmonization of methods and instruments. WHO Reg Publ Eur Ser. (1996) 58:1–161.
9. Sitaresmi MN, Indraswari BW, Rozanti NM, Sabilatuttaqiyya Z, Wahab A. Health-related quality of life profile of Indonesian children and its determinants: a community-based study. BMC Pediatr. (2022) 22:103. doi: 10.1186/s12887-022-03161-0
10. Pérez-Zepeda MU, Belanger E, Zunzunegui MV, Phillips S, Ylli A, Guralnik J. Assessing the validity of self-rated health with the short physical performance battery: a cross-sectional analysis of the international mobility in aging study. PLoS ONE. (2016) 11:e0153855. doi: 10.1371/journal.pone.0153855
11. Feng Q, Zhu H, Zhen Z, Gu D. Self-rated health, interviewer-rated health, and their predictive powers on mortality in old age. J Gerontol B Psychol Sci Soc Sci. (2016) 71:538–50. doi: 10.1093/geronb/gbu186
12. Sivakumaran G, Margolis R. Self-rated health by sexual orientation among middle-aged and older adults in Canada. J Gerontol B Psychol Sci Soc Sci. (2020) 75:1747–57. doi: 10.1093/geronb/gbz067
13. Mcharo RD, Mayaud P, Msuya SE. Where and how do young people like to get their sexual and reproductive health (SRH) information? Experiences from students in higher learning institutions in Mbeya, Tanzania: a cross-sectional study. BMC Public Health. (2021) 21:1683. doi: 10.1186/s12889-021-11728-2
14. Stanojevic Jerkovic O, Sauliune S, Šumskas L, Birt CA, Kersnik J. Determinants of self-rated health in elderly populations in urban areas in Slovenia, Lithuania and UK: findings of the EURO-URHIS 2 survey. Eur J Public Health. (2017) 27:74–9. doi: 10.1093/eurpub/ckv097
15. Lamidi EO. Educational differences in self-rated health trends among middle-aged and older adults living alone, 1972-2018. Aging Health. (2022) 34:626–39. doi: 10.1177/08982643211052718
16. Xu D, Arling G, Wang K, A. cross-sectional study of self-rated health among older adults: a comparison of China and the United States. BMJ Open. (2019) 9:e027895. doi: 10.1136/bmjopen-2018-027895
17. Dong W, Wan J, Xu Y, Chen C, Bai G, Fang L, et al. Determinants of self-rated health among Shanghai elders: a cross-sectional study. BMC Public Health. (2017) 17:807. doi: 10.1186/s12889-017-4718-5
18. Yang H, Deng Q, Geng Q, Tang Y, Ma J, Ye W, et al. Association of self-rated health with chronic disease, mental health symptom and social relationship in older people. Sci Rep. (2021) 11:14653. doi: 10.1038/s41598-021-94318-x
19. Hohls JK, König HH, Quirke E, Hajek A. Anxiety, depression and quality of life-a systematic review of evidence from longitudinal observational studies. Int J Environ Res Public Health. (2021) 18:12022. doi: 10.3390/ijerph182212022
20. Hsu MF, Lee KY, Lin TC, Liu WT, Ho SC. Subjective sleep quality and association with depression syndrome, chronic diseases and health-related physical fitness in the middle-aged and elderly. BMC Public Health. (2021) 21:164. doi: 10.1186/s12889-021-10206-z
21. Xie HJ, Wang QK, Hu JQ. Health Niche: the research paradigm of healthy habitat theory in the perspective of epidemiology and ecology. Mod Urban Res. (2021) 09:124–30.
22. Lei Y, Nollen N, Ahluwahlia JS Yu Q, Mayo MS. An application in identifying high-risk populations in alternative tobacco product use utilizing logistic regression and CART: a heuristic comparison. BMC Public Health. (2015) 15:341. doi: 10.1186/s12889-015-1582-z
23. Yan R, Zhao S, Zhang X, Lv Y. Factors associated with older adults' intention to use community-based elderly care: a study using the decision tree and logistic regression models. Chin Gen Pract. (2022) 25:87–93. doi: 10.12114/j.issn.1007-9572.2021.00.321
24. Wu C, Peng C, Yuan B, Fang H, Wang Y, Li W. Relationship between sleep quality and hyperuricemia among the physical examination population, Guangzhou. Mod Prev Med. (2022) 49:931–4, 940. doi: 10.3969/j.issn.1003-8507.2022.5.xdyfyx202205032
25. Li C, Shi Z. Status quo and influencing factors of mental health for caregivers of patients with mental illness. Chin Nurs Res. (2021) 35:2757–60. doi: 10.12102/j.issn.1009-6493.2021.15.027
26. Pereira-de-Sousa AM, López-Rodríguez JA. Self-perceived health in Spanish and Portuguese young seniors after the great recession according to the European Health Survey: a cross-sectional study. Aten Primaria. (2021) 53:102064. doi: 10.1016/j.aprim.2021.102064
27. Song X, Wu J, Yu C, Dong W, Lv J, Guo Y, et al. The distribution and correlates of self-rated health in elderly Chinese: the China Kadoorie Biobank study. BMC Geriatr. (2019) 19:168. doi: 10.1186/s12877-019-1183-2
28. Kaplan G, Baron-Epel O. What lies behind the subjective evaluation of the health status. Soc Sci Med. (2003) 56:1669–76. doi: 10.1016/S0277-9536(02)00179-X
29. Cui S, Yu Y, Dong W, Xu T, Huang Y, Zhang X. Are there gender differences in the trajectories of self-rated health among chinese older adults? An analysis of the Chinese Longitudinal Healthy Longevity Survey (CLHLS). BMC Geriatrics. (2021) 21:563. doi: 10.1186/s12877-021-02484-4
30. Mingshu Si. Meiying Shao, Dandan Ge, Dong Liang, Qi Jing, Wu Y, et al. Health status and its influencing factors among the elderly dwelling in pension institutions providing integrated medication in Qingdao city. Chin J Public Health. (2021) 37:1611–5. doi: 10.11847/zgggws1126966
31. Galenkamp H, Braam AW, Huisman M, Deeg DJ. Somatic multimorbidity and self-rated health in the older population. J Gerontol B Psychol Sci Soc Sci. (2011) 66:380–6. doi: 10.1093/geronb/gbr032
32. Hu F, Zhang J, Jiang F, Gao Z, Hong Z, Zhang L, et al. Effect of chronic disease multimorbidity on self-rated health among rural elderly in Shandong province. Chin J Public Health. (2021) 37:1594–6. doi: 10.11847/zgggws1132246
33. Song H, Deng M, Li X. A study on self-assessed health status and influencing factors of the elderly in rural Jiangsu. Chin J Health Stat. (2021) 38:601–2, 606. doi: 10.3760/cma.j.issn.0254-9026.2018.06.022
34. Byun M, Kim E, Ahn H. Factors contributing to poor self-rated health in older adults with lower income. Healthcare. (2021) 9:1515. doi: 10.3390/healthcare9111515
35. Sun X, Tang S, Miyawaki CE Li Y, Hou T, Liu M. Longitudinal association between personality traits and homebound status in older adults: results from the National Health and Aging Trends Study. BMC Geriatr. (2022) 22:93. doi: 10.1186/s12877-022-02771-8
36. Wang L, Yang Y, Zeng X, Tang G, Tang X, He Z. Influencing factors of self-rated health among the rural elderly, Chongqing. Mod Prev Med. (2018) 45:2794–8.
37. Zhang J, Cai J, He Z, Zhou X, Tang G. Analysis on self-rated health status and influencing factors among rural left-behind elderly in Chongqing. Mod Prev Med. (2020) 47:2215–8, 2241.
38. Cheng Y, Wang Z, Guo M, Xie C, Wu J. Analysis on the influencing factors and marginal effects of hospitalization service utilization of rural elderly residents. Med Soc. (2021) 34:59–63. doi: 10.13723/j.yxysh.2021.06.012
39. Riediger ND, Bombak AE, Mudryj AN. Health-related behaviours and their relationship with self-rated health among Canadian adults. BMC Public Health. (2019) 19:960. doi: 10.1186/s12889-019-7249-4
40. Li J, Zhaxi D, Liu Y, Wan Y, Gesang P, Zhang Y, et al. Analysis of self-rated health status of the elderly in Tibet from the perspective of healthy aging. Mod Prev Med. (2021) 48:1439–43.
41. Ohta R, Sato M, Kitayuguchi J, Maeno T, Sano C. Potential help-seeking behaviors associated with better self-rated health among rural older patients: a cross-sectional study. Int J Environ Res Public Health. (2021) 18:9116. doi: 10.3390/ijerph18179116
42. Andreasson A, Axelsson J, Bosch JA, Balter LJ. Poor sleep quality is associated with worse self-rated health in long sleep duration but not short sleep duration. Sleep Med. (2021) 88:262–6. doi: 10.1016/j.sleep.2021.10.028
Keywords: SRH, rural elderly, logistic, decision tree, influencing factors
Citation: Zhang M, Rong J, Liu S, Zhang B, Zhao Y, Wang H and Ding H (2022) Factors related to self-rated health of older adults in rural China: A study based on decision tree and logistic regression model. Front. Public Health 10:952714. doi: 10.3389/fpubh.2022.952714
Received: 25 May 2022; Accepted: 08 November 2022;
Published: 30 November 2022.
Edited by:
R. David Hayward, Ascension St. John Hospital, United StatesReviewed by:
Shekhar Chauhan, International Institute for Population Sciences (IIPS), IndiaRavi Philip Rajkumar, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), India
Copyright © 2022 Zhang, Rong, Liu, Zhang, Zhao, Wang and Ding. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong Ding, ZGluZ2hvbmcyMDAzQDEyNi5jb20=
†These authors have contributed equally to this work