 Tilahun Mengistie1
Tilahun Mengistie1 Teshale Mulatu
Teshale Mulatu Afework Alemayehu
Afework Alemayehu Merga Dheresa
Merga Dheresa
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 27 September 2022
Sec. Public Health Policy
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.949943
This article is part of the Research TopicAddressing the Inequalities in Maternal and Child Healthcare UtilizationView all 15 articles
Background: A compassionate and respectful care during pregnancy and childbirth is one of the essential components of safe motherhood. However, most of the women in developing countries experience disrespectful and abusive maternity care during childbirth. Hence, this study assessed the status of respectful maternity care and associated factors to bridge the gap.
Methodology: Facility-based cross-sectional study was conducted among mothers who delivered in public Hospitals in the Hadiya Zone, South Ethiopia from March 01 to 30, 2020. Data were collected using a pretested questionnaire through face-to-face interviews. Descriptive statistics was computed and multivariable logistic regression was fitted to identify predictors. Adjusted Odds Ratio (AOR) with 95% Confidence Interval was used to show the strength of association and level of significance was declared at P-value < 0.05.
Result: This study showed that 67.8 % (95% CI: 62.4–70.8%) of mothers received respectful maternal care. Being married [AOR: 2.17, 95% CI (1.03–6.93)], Cesarean section delivery [AOR: 2.48, 95% CI (1.03–5.97)], and absence of complications during child birth [AOR: 4.37, 95% CI (1.41–13.56)], were significantly associated with respectful maternity care.
Conclusions: The level of RMC in this study was moderate. Being married, Cesarean section delivery, and absence of complications during child birth were identified predictors of respectful maternity care. Therefore, tailored interventions aimed at improving respectful maternity care should target unmarried women, and women with complications of labor regardless of mode of delivery.
Pregnancy and childbirth are critical events in the reproductive life of women and denote a period of high susceptibility. Thus, compassionate and respectful care should be given for all pregnant women during labor and child birth to promote safe motherhood. Respectful maternity care refers to harmonized care given to all women to the highest possible standard and safeguards them from harm and mistreatment during labor and childbirth (1, 2).
Globally, averting maternal mortality has remained unfinished agenda of sustainable development goals (SDG) (3, 4). Despite the tremendous effort to reduce maternal mortality, the rate is still as high as 239 per 100,000 live births in low-income countries. Furthermore, MMR in Ethiopia is still 412/per 100,000 live births. This figure is very far from the target under the SDG by 2030, which is <70/100,000 (5). Even though skilled birth attendance (SBA) prevents a toll of maternal death, about 75% of mothers do not deliver in health institution in developing countries (5, 6).
Disrespectful and abusive maternity care is one of the main reasons for not utilizing maternal health services. Mistreatment and humiliation during labor and delivery can hinder women from accessing maternal health care for subsequent deliveries (7, 8).
Despite the negative effect of disrespectful and abusive care on the use of skilled birth care, there is currently no international consensus on how disrespect and abuse should be scientifically defined and measured (9, 10). In the perspective of this gap, Bowser and Hill identified seven categories of traits that describe disrespectful and abusive care during facility based child birth. The categories are physical abuse, non-consented care, non-confidential care, non-dignified care, discrimination, abandonment/neglect of care, and detention in facilities until hospital bills are paid (11).
Studies in Ethiopia portrayed the prevalence of disrespectful and abusive care ranging from 21.1 to 98.9% and the pooled prevalence found to be 49.4% (12–14), which are unacceptably high levels of obstetric violence and mistreatment.
The Ethiopian government in its 5-year health sector transformation plan tailored compassionate and respectful maternity care incorporating it in maternal health services packages (15). Although such investment was in place to alleviate this burning problem, their implementation in the national context is not promising.
Assessment of respectful maternity care during facility-based childbirth is necessary for the design, monitoring, and evaluation of interventions to promote respectful care during childbirth, especially in low-resource settings. In Ethiopia, few studies were conducted and evidences on the status of respectful maternity care and associated factors is limited. Therefore, this study assessed the status of respectful maternity care and associated factors in public Hospitals, in Hadiya Zone, Southern Ethiopia.
The study was conducted at public hospitals in the Hadiya Zone, Southern Ethiopia. The zone has one teaching and referral hospital, two primary hospitals, 72 public health centers, 311 health posts, and 142 private clinics (16). The study was conducted from March 01 to 30/2020.
A hospital based cross-sectional study was conducted among all mothers who gave birth in Hadiya Zone Public Hospitals during the study period. Seriously ill women who were unable to respond and who were referred from other health facilities after the second stage of labor were excluded from the study.
The sample size was determined by using the double population proportion formula considering factors that are significantly associated with the outcome variable at (p < 0.05), a two-sided confidence level of 95%, a margin of error of 5%, power of 80%, and the ratio of exposed to unexposed 1:1 using Epi-calc statistical software. Taking the average monthly income as an exposure variable: outcome among exposed (79.6%) and among unexposed (67%) (17), and adding a 10% non-response rate the final sample size was 460.
All public hospitals were included in the study. Sample size was allocated to each hospital proportionally by considering the average number of attendants. A systematic random sampling was applied to select study participants using delivery registration logbook as a sampling frame.
A pre tested and structured questionnaires were prepared by reviewing literatures pertinent to the topic (7, 18–20). The tool contains socio demographic characteristics, obstetric characteristics of the participants and categories of RMC that women will get during facility based child birth. The status of RMC was measured using a validated tool for assessing RMC which was adapted from the Maternal and Child Health Integrated Program (18). Data were collected through an exit interview during discharge. Each eligible woman was approached privately in a separate room within the hospital environment. The data were collected by eight health professionals working outside the study Hospitals. A 2-day training was given to both the data collectors and the supervisors regarding the objective of the study, data collection tools, and ways of data collection. The collected data was checked by supervisors for its completeness and consistency daily.
Data were entered into the computer using Epi-data version 4.2 and exported to SPSS version 23 for analysis. Bi-variable analysis was carried out to see the association of each of the independent variables with the outcome variable (Respectful maternity care). Hosmer and Lemeshow's goodness-of-fit test was used to assess whether the necessary assumptions were fulfilled. All variables with a p-value ≤0.2 were taken into the multivariable model to control for all possible confounders. Finally, the results of multivariable logistic regression analysis were presented in the adjusted odds ratio with 95% confidence intervals. The level of statistical significance was declared at p-value < 0.05.
In this study, women were considered to have respectful maternity care during labor and childbirth if they answered yes to all of those questions assessing RMC or verification criteria used for assessing the seven categories (performance standards) of RMC during labor and childbirth (19–22).
Women were considered as experienced disrespect and abuse if they answered no to one or more of those questions assessing RMC or verification criteria used for assessing the seven categories of RMC (18, 23, 24).
A total of 451 mothers participated in the study; which yields a response rate of 98.04%. Among mothers, 178 (39.1%) of the study participants were within the age group of 25–29 years. The mean age of the mothers was 28.6 (SD ± 4.04) years.
Concerning their marital status and residency, 398 (88.2) of them were married and 237 (52.1%) of the respondents were from urban. Of the total 159 (35.3%) of them attended primary education and 203 (45%) are housewives (Table 1).
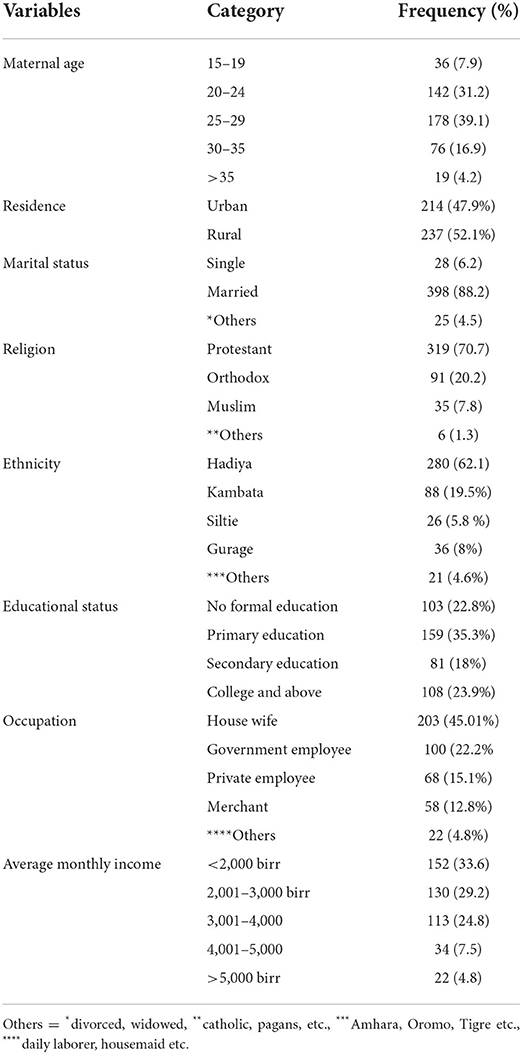
Table 1. Sociodemographic characteristics on respectful maternity care among mothers who gave birth at Hadiya Zone public hospitals Southern Ethiopia, 2020 (n = 451).
Of the total respondents, 439 (97.3.0%) had antenatal care follow up and 234 (51.4%) had two or more ANC visits. Regarding the gravidity of participants, 216 (47.5%) were multigravida. More than half 240 (53.2%) gave birth vaginally while 41 (14.4%) gave birth by caesarian section (Table 2).

Table 2. Provider related and obstetric characteristics of the respondents among mothers who gave birth at Hadiya Zone public hospitals Southern Ethiopia, 2020 (n = 451).
Overall, 67.8% (95%; CI: 62.4, 70.8%) of the women received respectful maternity care. Out of all participants, 41.9% didn't receive confidential care and 43.7% complained that HCPs (health care providers) did not take informed consent before any procedure (Table 3).
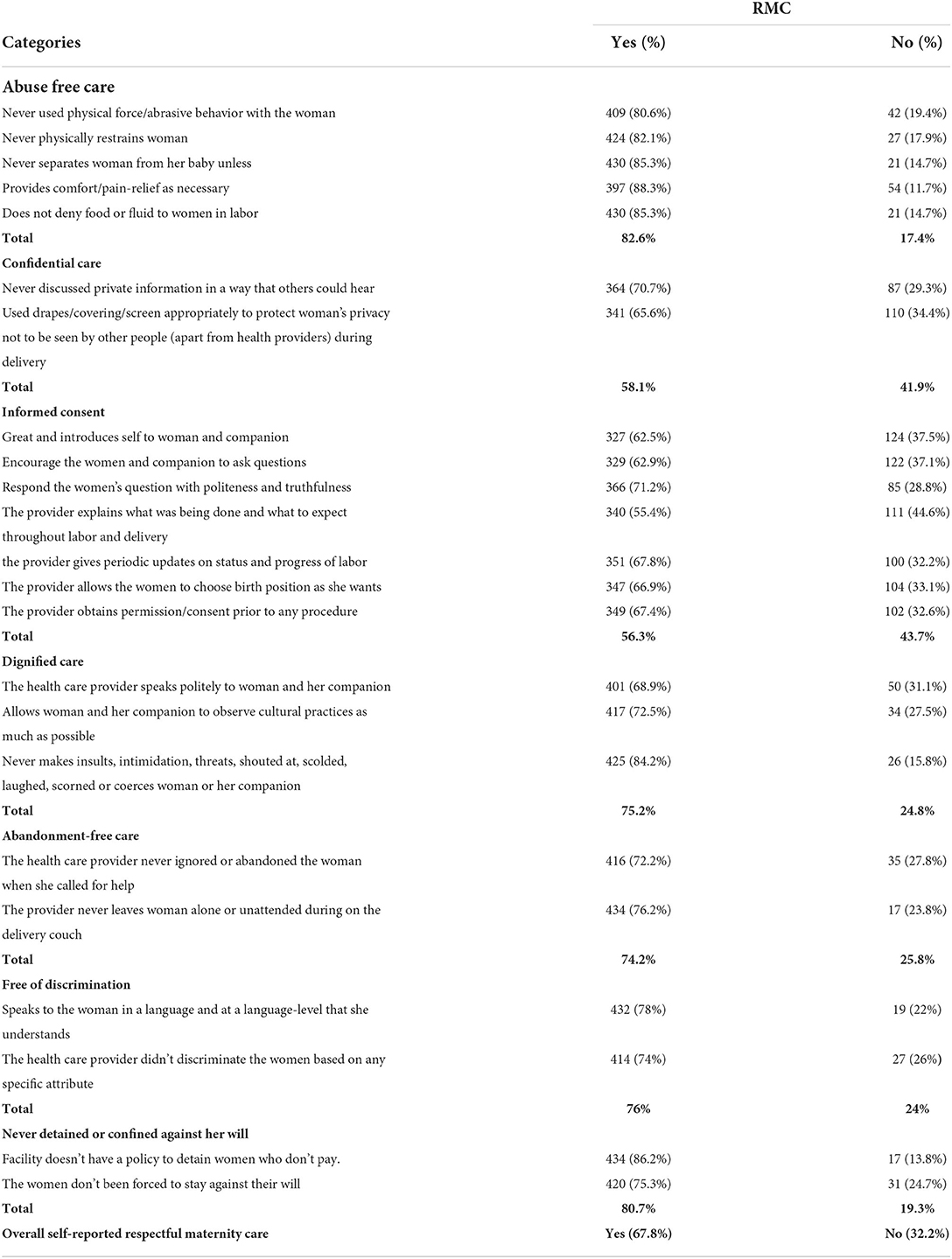
Table 3. Respectful maternity care categories among mothers who gave birth at Hadiya Zone public hospitals, Southern Ethiopia, 2020 (n = 451).
The bivariable analysis result showed that marital status, educational status, parity, the profession of health care provider, sex of health care provider, mode of delivery, birth outcome, length of hospital stay, complications during labor, and delivery were significantly associated with respectful maternity care. After adjusting for other variables; marital status, mode of delivery, and complications during labor and delivery remained significantly associated with respectful maternity care in multivariable logistic regression.
Married women were two times more likely to obtain respectful maternity care than single women [AOR: 2.17 (1.03–6.93)]. The odds of respectful maternity care were 2.48 times higher among mothers who delivered by cesarean section compared to those who gave birth by spontaneous vaginal delivery [AOR: 2.485, 95%CI (1.03, 5.97)]. The odds of respectful maternity care were four times higher among those women who did not face complications during childbirth as compared to their counterparts [AOR: 4.37, 95% CI (1.41–13.56)] (Table 4).
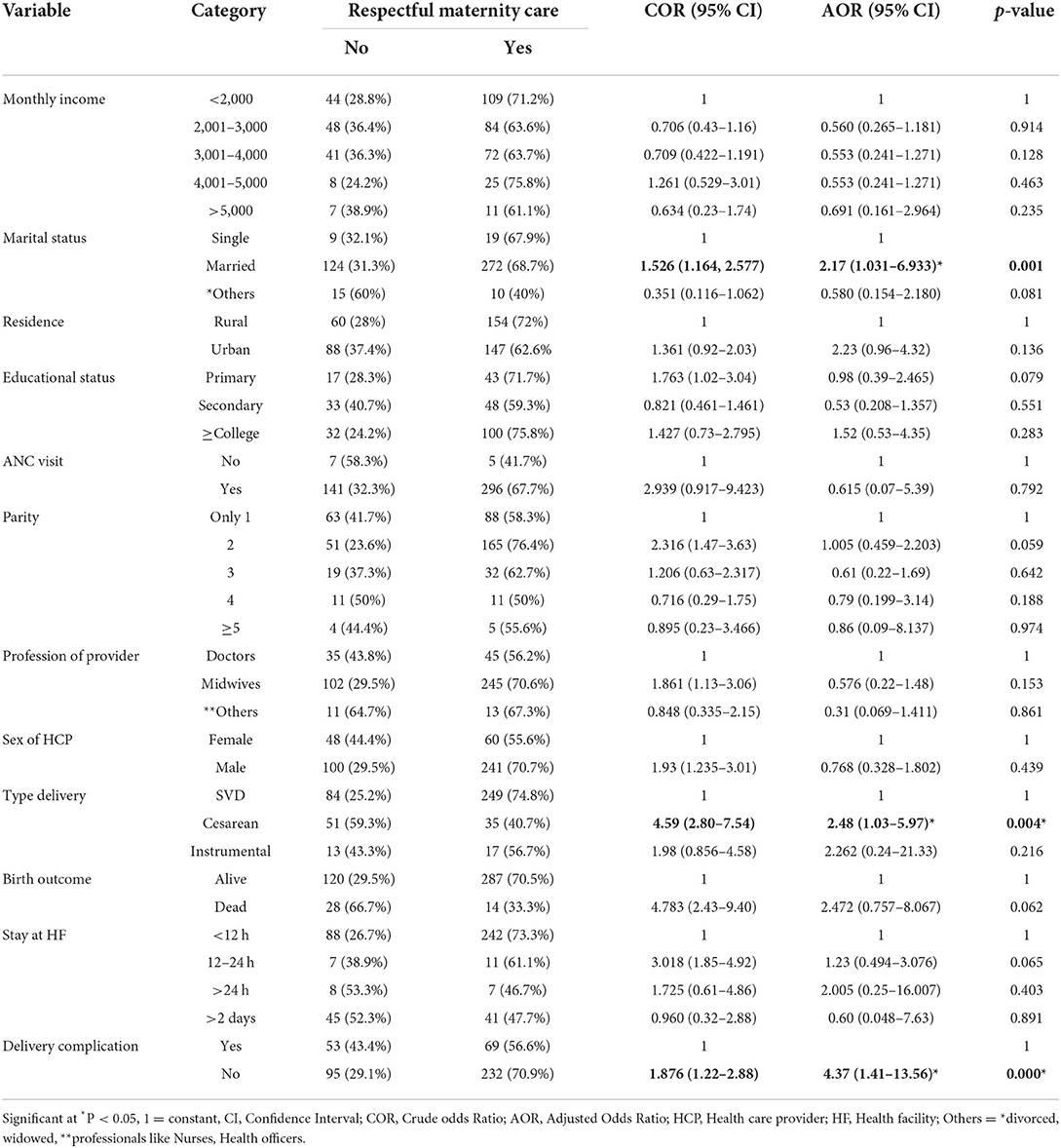
Table 4. Factors associated with respectful maternity care among mothers who gave birth at public hospitals of Hadiya Zone, southern, Ethiopia 2020 (n = 451).
A compassionate and respectful care during pregnancy and childbirth is one of the essential components of safe motherhood. In this study, the overall magnitude of respectful maternity care during labor and childbirth was 67.8 % (95% CI: 62.4–70.8%). On the other hand, about one-third of women (32.2%) reported disrespect and abusive (D&A) care during labor and childbirth which was unacceptably high.
The magnitude of RMC in this study is by far higher than the study conducted in Addis Ababa (21%) (20), Harar (38.4%) (21), West Shewa, Oromia region (35.8%) (22), and the study conducted in public Hospitals of Benishangul Gumuz Region, Ethiopia (12.6%) (23). However, this study finding is lower than the study finding from Tanzania (85%) (24) and Kenya (80%) (25). The difference could be due to study setting differences, methodological variation, participants' educational and socio-economic status, service quality, and the ability of participants to report disrespect and abusive care.
This study revealed that married women were two times more likely to receive respectful maternity care compared to those who are not in a marital union. This finding may be a result of companion, which indicates that providers are more likely to be cautious about how they act and speak to a client when a companion of the client is present. This finding is also supported by many other studies (17, 23, 25–27).
Furthermore, participants who gave birth by cesarean section were 2.48 times more likely to receive respectful maternity care compared to participants who gave birth by spontaneous vaginal delivery. The result is in contrast with the study done in Bahirdar, Northwest Ethiopia, and Addis Ababa, Ethiopia (17, 28). This could be justified by study setting differences, case flows, staff workload, and attitude of health care providers.
Unexpectedly, women who didn't face complications during childbirth were about four times to receive RMC as compared to those who faced complications during birth. This is aligned with other studies conducted in Ethiopia (17, 21, 28). This might be because those mothers who develop complications are admitted and stayed for an extended time and they might perceive poor quality of care provided by health professionals during their stay.
Finally, as a limitation this study was based on self-report, hence it was not possible to validate claims made by respondents in the course of questionnaire administration. There might be the possibility of underestimating disrespect and abusive care within short duration of data collection period due to its sensitive nature. To minimize this bias, the data were collected in a private room within the hospital setup.
The level of respectful maternity care in this study was moderate in comparison with other studies in the country. But still, about one-third of women experienced disrespect and abusive care while they gave birth at a health facility. Therefore, concerned body and stakeholders should devise strategies to avoid disrespect and abusive care during labor and childbirth. Furthermore, due emphasis should be given for improving RMC among unmarried women, and women with complications of labor regardless of mode of delivery.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Institutional Health Research Ethics Review Committee (IHRERC) of the College of Health and Medical Sciences, Haramaya University. The patients/participants provided their written informed consent to participate in this study.
TMe drafted the study. TY and MD monitored the study process. TMu and AA was involved in report writing and drafted the manuscript. All authors have read and approved the final manuscript.
This study was funded by Haramaya University. The funding organization has no role in designing the study, data collection, analysis, interpretation, protocol writing, and submission.
We gratefully acknowledge the study participants, data collectors, supervisors, hospital administrators, and staff for their willingness, to give their time and information for this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ANC, Antenatal Care; AOR, Adjusted Odds Ratio; CI, Confidence interval; D&A, Disrespect and Abuse; RMC, Respectful Maternity Care; MMR, Maternal Mortality Rate; SDG, Sustainable Development Goal; SBA, Skilled Birth Attendant.
1. World Health Organization. The Prevention and Elimination of Disrespect and Abuse During Childbirth. (2014). Available online at: http://apps.who.int/iris/bitstream/10665/134588/1/WHO_RHR_14.23_eng.pdf (accessed January 3, 2015).
2. WHO. World Health Organization Recommendations: Intrapartum Care for a Positive Childbirth Experience. Geneva: World Health Organization (2018). Available online at: https://apps.who.int/iris/bitstream/handle/10665/260178/9789241550215-eng.pdf (accessed June 25, 2018).
3. World Health Organization. Health in 2015: from MDGs, Millennium Development Goals to SDGs, Sustainable Development Goals. World Health Organization (2015). Available online at: https://apps.who.int/iris/handle/10665/200009
4. Magar V. Gender, health and the sustainable development goals. Bull World Health Organ. (2015) 93:743. doi: 10.2471/BLT.15.165027
5. Lee BX, Kjaerulf F, Turner S, Cohen L, Donnelly PD, Muggah R, et al. Transforming our world: implementing the 2030 agenda through sustainable development goal indicators. J Public Health Policy. (2016) 37:13–31. doi: 10.1057/s41271-016-0002-7
6. Central Statistical Agency (CSA), ICF. Ethiopia Demographic and Health Survey 2016: Key Indicators Report. Addis Ababa, Ethiopia; Rockville, MD: CSA and ICF (2016).
7. Miller S, Lalonde A. The global epidemic of abuse and disrespect during childbirth: history, evidence, interventions, and FIGOs mother– baby friendly birthing facilities initiative. Int J Gynecol Obstetr. (2015) 131:S49–52. doi: 10.1016/j.ijgo.2015.02.005
8. Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, et al. High-quality health systems in the Sustainable Development Goals era: time for a revolution. Lancet Global Health. (2018) 6:e1196–e252. doi: 10.1016/S2214-109X(18)30386-3
9. Warren C, Njuki R, Abuya T, Ndwiga C, Maingi G, Serwanga J, et al. Study protocol for promoting respectful maternity care initiative to assess, measure and design interventions to reduce disrespect and abuse during childbirth in Kenya. BMC Preg Childbirth. (2013) 13:1–9. doi: 10.1186/1471-2393-13-21
10. Silal SP, Penn-Kekana L, Harris B, Birch S, McIntyre D. Exploring inequalities in access to and use of maternal health services in South Africa. BMC Health Serv Res. (2011) 120:12. doi: 10.1186/1472-6963-12-120
11. Bowser D, Hill K. Exploring Evidence for Disrespect Abuse in Facility-Based Childbirth: Report of a Landscape Analysis. (2010). Available online at: http://www.mhtf.org/wp-content/uploads/sites/17/2013/02/Respectful_Care_at_Birth_9-20-101_Final.pdf (accessed March 10, 2014).
12. Banks AMK, Ratcliffe HL, Betemariam W. A Langer Jeopardizing quality at the frontline of healthcare: prevalence and risk factors for disrespect and abuse during facility-based childbirth in Ethiopia. Health Policy Plan. (2018) 33:317–27. doi: 10.1093/heapol/czx180
13. Ukke GG, Gurara MK, Boynito WG. Disrespect and abuse of women during childbirth in public health facilities in Arba Minch town, south Ethiopia–a cross-sectional study. PLoS ONE. (2019) 14:e0205545. doi: 10.1371/journal.pone.0205545
14. Kassa ZY, Husen S. Disrespectful and abusive behavior during childbirth and maternity care in Ethiopia: a systematic review and meta-analysis. BMC Res Notes. (2019) 12:83. doi: 10.1186/s13104-019-4118-2
15. Federal Democratic Republic of Ethiopia Ministry of Health. Ethiopian National Health Quality Strategy: Transforming Quality of Health Care in Ethiopia, 2016–2020. Addis Ababa: Federal Democratic Republic of Ethiopia Ministry of Health (2016).
16. Hadiya Zone Demographic and Health Division Annual Report Hadiya Zone Southern Ethiopia. GA UN, Transforming Our World: The 2030 Agenda for Sustainable (2018).
17. Kitaw M, Tessema M. Respectful maternity care and associated factors among mothers in the immediate post – partum period, in public health facilities of Addis Ababa. Int J Pregnancy Child Birth. (2019) 5:10–7. doi: 10.15406/ipcb.2019.05.00140
18. Reis V, Deller B, Carr C, Smith J. Respectful Maternity Care: Country Experiences: Survey Report. Washington, DC: United States Agency for International Development (2012).
19. Warren CAT, Obare F, Sunday J, Njue R, Askew I, Bellows B. Evaluation of the impact of the voucher and accreditation approach on improving reproductive health behaviors and status in Kenya. BMC Public Health. (2011) 11:177. doi: 10.1186/1471-2458-11-177
20. Asefa A, Bekele D. Morgan Aea. Service providers' experiences of disrespectful and abusive behavior towards women during facility based childbirth in Addis Ababa, Ethiopia. Reprod Health. (2018) 15:4. doi: 10.1186/s12978-017-0449-4
21. Bante A, Teji K, Seyoum B, Mersha A. Respectful maternity care and associated factors among women who delivered at Harar hospitals, eastern Ethiopia: a cross-sectional study. BMC Preg Childbirth. (2020) 20:1–9. doi: 10.2147/JMDH.S286458
22. Bulto GA, Demissie DB, Tulu AS. Respectful maternity care during labor and childbirth and associated factors among women who gave birth at health institutions in the West Shewa zone, Oromia region, Central Ethiopia. BMC Pregnancy Childbirth. (2020) 20:443. doi: 10.1186/s12884-020-03135-z
23. Amsalu B, Aragaw A, Sintayehu Y, Sema A, Belay Y, Tadese G, et al. Respectful maternity care among laboring women in public hospitals of Benishangul Gumuz Region, Ethiopia: a mixed cross-sectional study with direct observations. SAGE Open Med. (2022) 10:20503121221076995. doi: 10.1177/20503121221076995
24. Sando D, Ratcliffe H, McDonald K, Spiegelman D, Lyatuu G, Mwanyika-Sando M, et al. The prevalence of disrespect and abuse during facility-based childbirth in urban Tanzania. BMC Preg Childbirth. (2016) 16:236. doi: 10.1186/s12884-016-1019-4
25. Abuya T, Warren CE, Miller N, Njuki R, Ndwiga C, Maranga A, et al. Exploring the prevalence of disrespect and abuse during childbirth in Kenya. PLoS ONE. 10:e0123606. doi: 10.1371/journal.pone.0123606
26. Tekle Bobo F, Kebebe Kasaye H, Etana B, Woldie M, Feyissa TR. Disrespect and abuse during childbirth in Western Ethiopia: should women continue to tolerate? PLoS ONE. 14:e0217126. doi: 10.1371/journal.pone.0217126
27. Gebremichael MW, Worku A, Medhanyie AA, Berhane Y. Mothers' experience of disrespect and abuse during maternity care in northern Ethiopia. Glob Health Action. (2018) 11:1465215. doi: 10.1080/16549716.2018.1465215
Keywords: respectful maternity care, childbirth, public hospitals, Hadiya Zone, Southern Ethiopia
Citation: Mengistie T, Mulatu T, Alemayehu A, Yadeta TA and Dheresa M (2022) Respectful maternity care among women who gave birth at public hospitals in Hadiya Zone, Southern Ethiopia. Front. Public Health 10:949943. doi: 10.3389/fpubh.2022.949943
Received: 21 May 2022; Accepted: 09 September 2022;
Published: 27 September 2022.
Edited by:
Alexandra P. Leader, Eastern Virginia Medical School, United StatesReviewed by:
Yitagesu Sintayehu, Dire Dawa University, EthiopiaCopyright © 2022 Mengistie, Mulatu, Alemayehu, Yadeta and Dheresa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Teshale Mulatu, d295ZXNhZ0BnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.