 Akosua Pokua Adjei1
Akosua Pokua Adjei1 Gideon Senyo Amevinya1
Gideon Senyo Amevinya1 Wilhemina Quarpong2
Wilhemina Quarpong2 Akua Tandoh1
Akua Tandoh1 Richmond Aryeetey1
Richmond Aryeetey1 Michelle Holdsworth3
Michelle Holdsworth3 Charles Agyemang4
Charles Agyemang4 Francis Zotor5Matilda E. Laar6
Francis Zotor5Matilda E. Laar6 Kobby Mensah7
Kobby Mensah7 Phyllis Addo5Dennis Laryea8Gershim Asiki9
Phyllis Addo5Dennis Laryea8Gershim Asiki9 Daniel Sellen10
Daniel Sellen10 Stefanie Vandevijvere11
Stefanie Vandevijvere11 Amos Laar1*
Amos Laar1*- 1Department of Population, Family and Reproductive Health, School of Public Health, University of Ghana, Accra, Ghana
- 2Nutrition and Health Sciences, Laney Graduate School, Emory University, Atlanta, GA, United States
- 3UMR MoISA (Montpellier Interdisciplinary Centre on Sustainable Agri-Food Systems), (Univ Montpellier, CIRAD, CIHEAM-IAMM, INRAE, Institut Agro, IRD), Montpellier, France
- 4Department of Public and Occupational Health, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands
- 5Department of Family and Community Health, University of Health and Allied Sciences, Ho, Ghana
- 6Department Family and Consumer Sciences, School of Agriculture, University of Ghana, Accra, Ghana
- 7Department of Marketing and Entrepreneurship, University of Ghana Business School, University of Ghana, Accra, Ghana
- 8Non-Communicable Disease Programme, Ghana Health Service, Accra, Ghana
- 9African Population and Health Research Center, Nairobi, Kenya
- 10Department of Nutritional Sciences, University of Toronto, Toronto, ON, Canada
- 11Sciensano, Service of Lifestyle and Chronic Diseases, Brussels, Belgium
Background: Intake of unhealthy foods is linked to the onset of obesity and diet-related non-communicable diseases (NCDs). Availability of unhealthy (nutritionally poor) foods can influence preference, purchasing and consumption of such foods. This study determined the healthiness of foods sold at modern retail outlets- supermarkets and mini-marts in the Greater Accra Region of Ghana.
Methods: All modern retail outlets located in six districts of Greater Accra were eligible. Those < 200 m2 of floor area and with permanent structures were categorized as mini-marts; and those ≥200 m2 as supermarkets. Shelf length of all available foods were measured. Healthiness of food was determined using two criteria - the NOVA classification and energy density of foods. Thus, ultra-processed foods or food items with >225 kcal/100 g were classified as unhealthy. The ratio of the area occupied by unhealthy to healthy foods was used to determine the healthiness of modern retail outlets.
Results: Of 67 retail outlets assessed, 86.6% were mini-marts. 85.0% of the total SHELF area was occupied by foods categorized as unhealthy (ranging from 9,262 m2 in Ashiaman Municipality to 41,892 m2 in Accra Metropolis). Refined grains/grain products were the most available, occupying 30.0% of the total food shelf space, followed by sugar-sweetened beverages (20.1% of total shelf space). The least available food group–unprocessed staples, was found in only one high income district, and occupied 0.1% of the total food shelf space. Retail outlets in two districts did not sell fresh fruits or fresh/unsalted canned vegetables. About two-thirds of food products available (n = 3,952) were ultra-processed. Overall, the ratio of ultra-processed-to-unprocessed foods ranged from 3 to 7 with an average (SD) of 5(2). Thus, for every healthy food, there were five ultra-processed ones in the studied retail outlets.
Conclusion: This study reveals widespread availability of ultra-processed foods in modern retail outlets within the selected districts. Toward a healthier food retail environment, public health and food regulators, in partnership with other stakeholders need to institute measures that improve availability of healthy foods within supermarkets and mini-marts.
Introduction
Obesity is a major public health issue that contributes to the development of other diet-related non-communicable diseases (NCDs) such as diabetes, hypertension, cardiovascular disease (CVD) and some cancers (1). Several policies and programmes have been recommended to limit the intake of unhealthy ultra-processed, energy-dense and nutrient-poor foods rich in calories, salt, sugar, and fat but poor in beneficial nutrients such as fiber, protein, and micronutrients (2, 3). This policy response to improve food environments are informed by evidence that suggests that availability of these foods in the individual's environment and individual factors such as attitudes, taste, income and food affordability influence food consumption, including within Africa (4, 5). This implies that limiting the availability of unhealthy foods, while increasing the availability of healthier foods can motivate healthier food acquisition or consumption, and may thus contribute to preventing obesity. To that end, many calls exist for creating and promoting healthier food environments while eliminating so called “obesogenic environments” that encourage unhealthy food consumption (5, 6).
Urbanization, poverty, globalization, industrialization, climate change and the emergence of a concentrated corporate food regime (1–3) are converging and mutually reinforcing global transitions such as the dietary transition (4). In Ghana, such transformations of global food systems understood as the web of processes, actors and infrastructure that govern food production, processing, distribution, and sale have contributed to a changing quality of diets and the rise in obesity and nutrition-related NCDs (5). Ghana is at an advanced stage of the nutrition transition, experiencing rapid urbanization, and increasing overweight/obesity and related NCDs (5, 6). This entails increasing consumption of ultra-processed, energy-dense and micronutrient-poor foods, compounded by sedentary lifestyles with reduced physical activity. The transformation of systems of food production toward industrial mass-production of ultra-processed food has been mirrored by other structural changes including the transformation of food retail (2).
Ghana has recently been ranked as highly attractive for retail investment in Africa and globally based on the Global Retail Development Index, which studies the global retailing landscape based on 25 criteria (including country risk, market attractiveness, market saturation, and national retail sales) (7). Ghana has also been described as the new “bright spot” of Africa, driven by increased foreign and public investment as well as urbanization of the population. As a result, modern retail in Ghana is gradually emerging, especially in the capital, Accra (7), therefore impacting on food environments. These changes have included more direct contractual connections between large-scale producers and suppliers, with centralized and consolidated procurement and distribution systems. These “upstream” trends are mirrored by the “downstream” diffusion and penetration of “supermarkets for the poor” into areas previously dominated by traditional and informal markets (8). In Ghana, not only has the number of modern retail outlets increased, but also the penetration of ultra-processed foods in traditional food retail outlets—including informal ones (9). Monteiro et al. (3), defined ultra-processed foods as industrial products consisting of various processed ingredients, including sugar, starches, emulsifiers or colors, salt and other additives that enhance the shelf life or modify the food's taste, texture and color. Typical examples consumed in Ghana are sweets and biscuits, fried sausage and instant noodles (10).
The NOVA framework categorizes food into four groups (ultra-processed foods and three others) based on their nature, purpose, and degree of processing (3). Ultra-processed food consumption reduces the likelihood of consuming fiber, protein and many micronutrient-rich foods that promote wellbeing, while increasing free sugar, sodium and unhealthy fats intake (3). Several studies have demonstrated a correlation between consumption of ultra-processed foods and increased risk for obesity and other NCDs (11–13). These studies and others indicate that not only are they available in retail outlets, they are also widely marketed, including in Ghana (14–16). Such wide availability and concerted marketing of ultra-processed foods a role in the purchasing and consumption of these foods (17).
Shelf space has been shown to have a substantial influence on the sales of a variety of food items (both healthy and unhealthy), indicating that the accessibility and prominence of potentially unhealthy foods in the supermarket, such as sugar sweetened beverages and salty snacks can also have an impact on the healthiness of customers' diets (18). Likewise, a classic marketing study showed that with a doubling of shelf space, sales of fruits and vegetables rose by about 40% (19). Elsewhere, studies that aimed to assess the healthiness of supermarket food environments have measured the shelf length of foods available for sale in food retail outlets and categorized them as healthy or unhealthy [e.g., (20, 21)]. These studies showed that simple measurements of shelf space can be used by researchers to characterize the healthfulness of the food environment and by policymakers to establish criteria for favorable policy treatment of stores (20, 21). Vandevijvere et al. (21) for instance reported that for every 1 m of shelf length for unhealthy foods, there was 42 cm of shelf length for healthy foods on average, with large variations between stores. The shelf length ratio was significantly lower in the most compared to the least/medium deprived socioeconomic areas.
In Ghana, while research on food retail environments is increasing in both scope and level of innovation (6, 15, 16, 22, 23), none has measured the amount of shelf space used for healthy and unhealthy foods in-store. Shelf space measurement is a useful measure of the in-store availability of healthy vs. less foods. The measure is a good proxy for product availability in food retail outlets. The current study determined the availability of food types sold at modern retail outlets according to their level and purpose of food processing and energy density through measuring shelf length located in the Greater Accra Region of Ghana.
Methods
Study design and site
This study is part of the Measurement, Evaluation, Accountability, and Leadership Support for NCDs Prevention Study (MEALS4NCDs) Project, which was implemented in the Greater Accra Region (GAR) of Ghana in 2019-2022 (24). MEALS4NCDs's overarching aim was to measure and support public sector actions that create healthy food marketing, retail, and provisioning environments for Ghanaian children, using adapted methods from the International Network for Food and Obesity/NCDs Research Monitoring and Action Support (INFORMAS) (25). The MEALS4NCDs project adopted a cross-sectional study design that applied both quantitative and qualitative methods. The study deployed a multistage sampling approach to select six administrative districts in the Greater Accra Region of Ghana (Figure 1). The first stage of the sampling process entailed purposively selecting the Greater Accra Region, which hosts the national capital, was/and remains the most urbanized and most marketed to, region of Ghana. The region was sub-divided into 16 administrative districts categorized as Metropolitan, Municipal, and Districts Assemblies (MMDAs). A representative sample of six districts (one metropolitan, three municipals and two districts) were selected using both probabilistic and non-probabilistic sampling approaches. Details about the sampling is reported elsewhere (24).
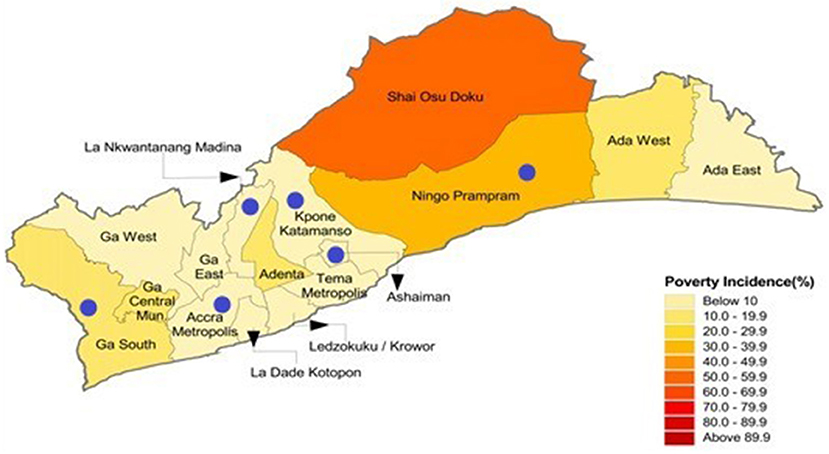
Figure 1. A map of the Greater Accra Region of Ghana highlighting the six selected districts and their poverty incidence.
All modern retail outlets located in these six districts were eligible to participate in the study.
Modern food retail outlet identification
An eligible “retail outlet” was defined as a self-service modern retail outlet (with aisles accessible to customers) that had at least one staffed checkout aisle or cash register. In this study, “modern food retail outlets” encompass supermarkets and mini-marts. All eligible ‘retail outlets with < 200 m2 of floor area were categorized as a “mini-mart” as opposed to supermarkets that were much larger in size. Of note, the 200 m2 criterion was not decided a priori. Its relevance came to the fore when the need arose to discriminate between usual supermarkets and “smaller marts/hypermarkets that were included in the assessment.” The derivation of the criterion was informed by the study team's collective knowledge and lived experiences. The criterion was deemed sensitive enough to discriminate between these two kinds of outlets. While local district offices were able to provide list of modern retail outlets found within their jurisdictions, field data collectors were trained to identify and map those that may not have been captured in the district database.
Summary of field procedures
Data were collected from July to August, 2020. Permission was obtained from retail outlet managers and owners to conduct in-store measurements. An in-store measurement tool adapted from INFORMAS was used to determine the total shelf length/breadth of foods available in the supermarkets—consistent with previous studies (20, 26). The shelf length and breadth for all food groups were measured: sugar-sweetened beverages, refined grains and refined grain products, whole grain cereal, legumes, fresh meat, processed meat/fish, milk product, eggs, fresh fruits and fresh fruit juice, fresh vegetables, fats and oil products, water, alcoholic beverages, unsweetened coffee, sweet foods and toffees, salted snack and vegetables, unprocessed staples, processed staples and condiments. When a food item type (e.g., sugar-sweetened beverage) was found in several places in the retail outlet, each location was measured separately and recorded in the in-store measurement tool. The total shelf area was added, once all measurements had been conducted. The total floor space was also determined by measuring the retail outlet's floor length and breadth. Digital photographs of all food products in-store were taken to facilitate their classification.
Each district had a team of two trained research assistants who conducted the in-store assessment (shelf space measurement with a tape measure and taking photographs). The research assistants went through several workshops to ensure clarity and consistency of comprehension. The data collection tool was pretested and validated before being used finally to collect data. The pretesting was done in La Nkwatanang-Madina Municipal Assembly. Based on the results obtained from the pretesting, necessary updates were done to the data collection tool.
Healthiness of food products
The foods were categorized according to the extent and nature of processing using the NOVA classification system (3). The NOVA food classification model categorizes foods into four groups—unprocessed/minimally processed foods, processed culinary ingredients, processed foods, and ultra-processed foods. In this study, unprocessed or minimally processed food were deemed healthy, whilst ultra-processed foods were not. Given our interest in calorie density of foods, food products were secondly categorized as healthy or unhealthy foods depending on calorie density. The NOVA classification does not specifically classify foods using calorie density. Foods that were energy-dense (>225 kcal/100 g) according to the (27) classification, were nutrient-poor, or were high in free/added sugar, sodium, and saturated fat were classified as unhealthy; healthy foods on the other hand were those that are nutrient dense. Details of the process of categorizing are given in our previously published paper (10). Other food categories including condiments/culinary ingredients were classified as miscellaneous. For every retail outlet we computed the ratio of all unhealthy to all healthy products, as well as ultra-processed food to minimally processed/unprocessed foods.
Healthiness of retail outlets
The ratio of total area of shelf space occupied by unhealthy vs. healthy food types available in retail outlets was calculated. In this study, a modern food retail outlet with a ratio less than one (< 1) was considered to be healthier; a ratio greater than or equal to one (≥1) was considered less healthy. Similarly, an outlet was scored based on the ratio of NOVA Class four (ultra-processed food) to NOVA Class one (unprocessed/minimally processed). Again, a ratio < 1 was considered as a healthier supermarket (< 1). A ratio ≥1 was considered less healthy.
Data analysis
Descriptive analyses were performed using Microsoft Excel Worksheet 2010 and IBM SPSS Version 21 to generate total areas occupied by the various food groups and the ratio of healthy to unhealthy foods. Descriptive statistics such as means, standard deviations and percentages were estimated for the features of the retail outlets and the relative availability of unhealthy foods.
Results
Within the six districts selected, 113 eligible modern food retail outlets were identified. Assessments were conducted in 67/113 (59%) of the food outlets in operation. Assessments were not conducted in the remaining retail outlets primarily because their managers did not grant permission for measurements or for pictures to be taken. Also, a few others were not operating and could not be accessed. The attributes of the retail outlets are shown in Table 1. We adopted Ghana Statistical Service's categorization of the districts by poverty incidence (also referred to as poverty headcount and defined in Table 1). La Nkwatanang Madina (LANMA) had the highest number of retail outlets assessed (22) and also the highest mean outlet floor size (207 m2). The sizes of the retail outlets differed by district. 86.6% of the retail outlets assessed were mini-marts (floor area < 200 m2). About 80% of the retail outlets were found in districts with low poverty incidence (≤ 10% poverty incidence). The average floor size of the supermarkets found in LANMA, one of the districts in the Greater Accra Region with low poverty headcount (2.8%) was 207 m2, followed by AMA (104 m2) whilst Ningo Prampram, a district with high poverty headcount - more than four times the regional average (poverty headcount of 31.2%), had an average outlet floor size of 63 m2. Ga South Municipal, a district with the highest number of poor persons (61,347) in the region had the least average supermarket floor size (46 m2).
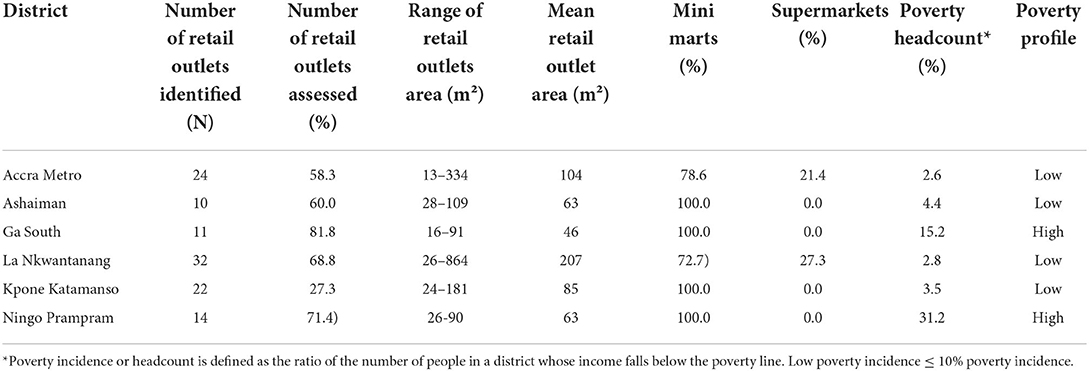
Table 1. Attributes of identified retail outlets located within the study districts.
Food items available in the modern retail outlets
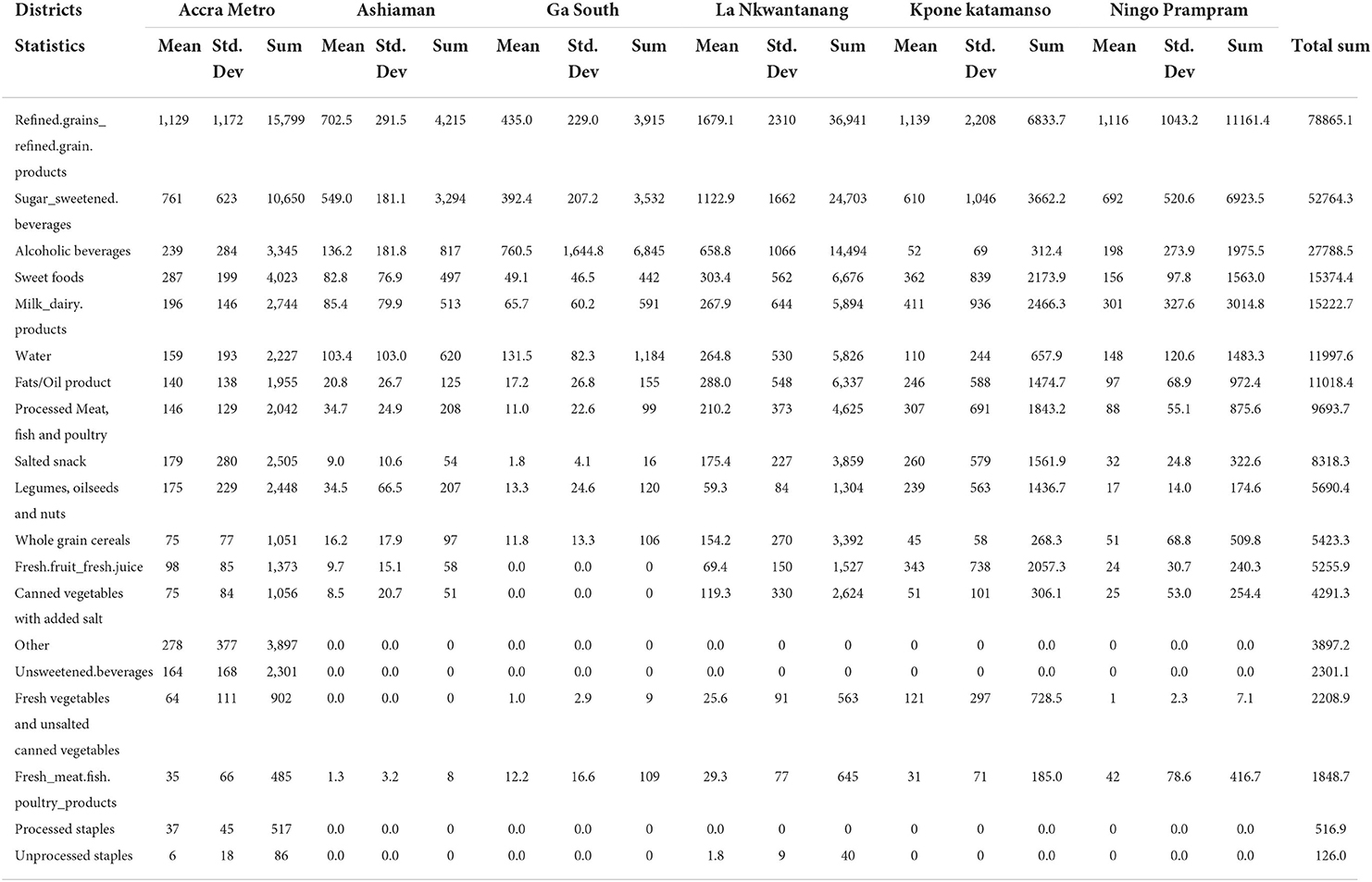
Refined grain/grain products such as noodles, cornflakes, biscuits, cake and cookies were the most available food groups in the retail outlets within the selected districts, except Ga South, where alcoholic beverages occupied the majority of the shelf area dedicated to foods in retail outlets (40.0%) (Figure 2). This was followed by sugar-sweetened beverages in all the districts except Ga South, where refined grains and refined grain products were the second most available food group (23%). Fresh vegetables and unsalted canned vegetables were not found in any of the retail outlets assessed in Ashaiman. No retail outlet assessed in Ga South sold fresh fruit. Additional data (Appendix 1) shows the availability [measured by shelf area (m2)] of the different food items in the retail outlets assessed in the six districts.
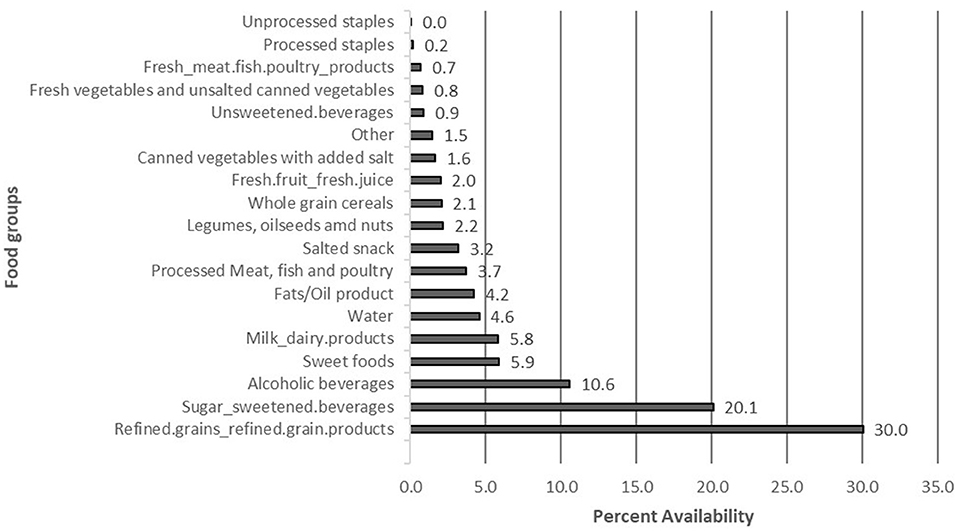
Figure 2. Availability (measured by proportion of total shelf area [%]) of different types of food items in modern retail outlets within the study districts.
Availability of healthy vs. unhealthy foods
Over eighty percent (83.1%) of the shelf space occupied by healthy foods were found in retail outlets located in low poverty incidence districts (Table 2). Overall, 78.7% of the area occupied by food products in both the mini-marts and supermarkets was allocated to “unhealthy” foods; about 20% of these were sugar-sweetened beverages (Appendix 1). Using the NOVA classification system, 68% (2669) food products identified in the food outlets were categorized as ultra-processed, 9% (337) were processed foods, 5% (211) were processed culinary foods and 18% (705) were unprocessed or minimally processed foods (Figure 3).
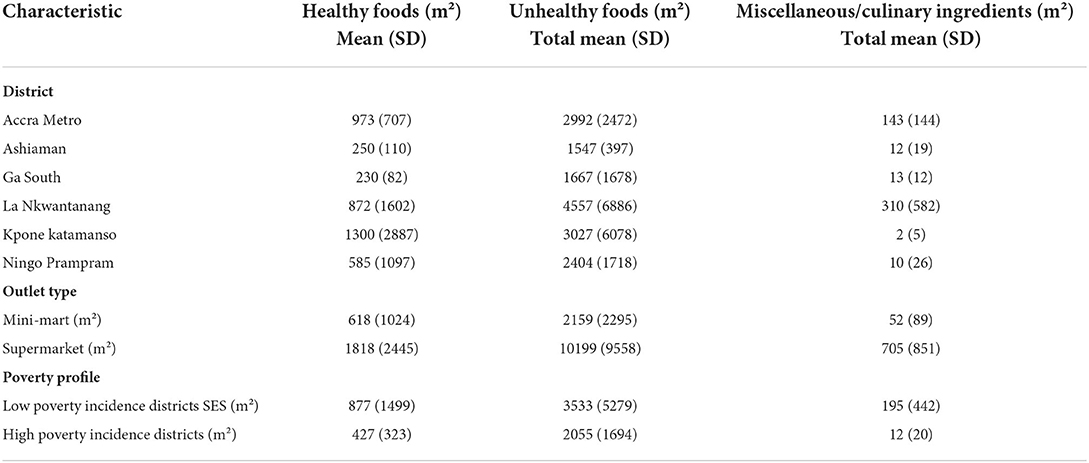
Table 2. Shelf area occupied by healthy and unhealthy foods in retail outlets by districts, outlet size, and district poverty level.
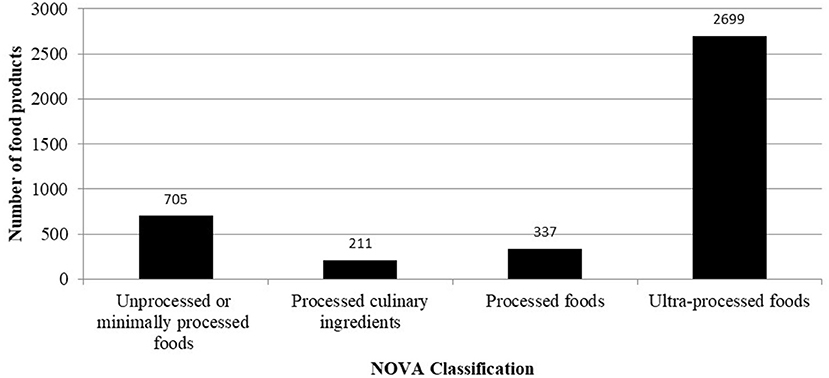
Figure 3. NOVA classification of unique food products in modern food outlets in all six study districts.
Healthiness of supermarkets
As per Table 3, overall, the ratio (±SD) of the shelf area for unhealthy-to-healthy foods is 4 (2). From the table, all retail outlets assessed in the six districts were found to be less healthy. The ratio of ultra-processed to unprocessed or minimally processed foods was also 4.8 with a standard deviation of 1.4.
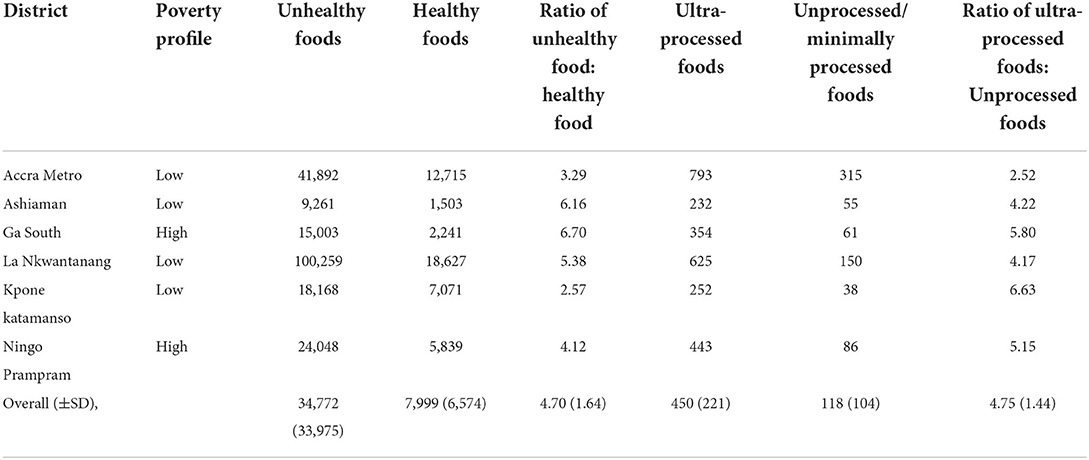
Table 3. Ratio of healthy/unprocessed/minimally processed foods to unhealthy/ultra-processed foods by district.
Discussion
Most of the modern retail outlets assessed were mini-marts. The most available food groups in the retail outlets were refined grains /grain products followed by sugar-sweetened beverages. Unprocessed staples, fresh meat, fish and poultry products, fresh vegetables and unsweetened beverages each occupied < 1% of the total shelf area allotted to food. Eighty-five percentage of the area occupied by food products in the modern retail outlets was allocated to unhealthy food categories. Almost of the food products were categorized as ultra-processed foods. Per ration of unhealthy-to-healthy foods or ultra-processed-to-unprocessed/minimally processed foods, all the retail outlets assessed were found to be unhealthy.
It has been previously reported that unhealthy foods are widely available in Ghana (9, 16, 28). As all outlets were assessed to be unhealthy overall, these outlets contribute to making ultra-processed and other unhealthy energy-dense, nutrient-poor foods more available. Notably, this study is cross-sectional and thus the findings of this study reflect the situation at a given time. However, all the retail outlets were assessed in a short period of time, so the findings are comparable within the sampled retail outlets.
Comparison of retail outlets and socio-economic status of districts using poverty headcount levels from the Ghana Statistical Service (29) shows important differences between the districts assessed. Although all the districts assessed in this study are located in the Greater Accra Region of Ghana, the most urbanized region of Ghana, the degrees of poverty incidence are clearly different. The number of supermarkets and mini-marts in Ga South (n = 11), a district with high poverty headcount, was modest compared to that in LANMA (n = 32), a district with low poverty incidence. A study conducted in Brazil (30) presented similar findings where lower socially deprived neighborhoods presented greater density of supermarkets. This may be because higher poverty incidence districts are less likely to attract high-end commercial establishments with a variety of food options because of their unstable urban infrastructure and lower consumer purchasing power.
In all the retail outlets assessed in Ga South, fresh fruits were not sold. Likewise, in Ashaiman, fresh vegetables and unsalted canned vegetables were not sold. This is similar to an earlier study in Ghana, where only five out of 13 supermarkets sold any fresh fruit or vegetables (23). Logistics such as transportation, preservation and storage of fresh food may be a barrier to the availability of fresh fruit and vegetables in the modern retail outlets assessed. Another explanation could be the status of supermarkets/mini-marts in the wider food environment. For instance, it is likely the role of these food retail outlets in supplying customers in Ghana with fresh fruit and vegetables is quite low due to the significance and usage of other retailers such as greengrocers or open markets (23). Also, the relatively small sizes of the supermarkets found in Greater Accra compared to supermarket sizes found in other studies, for example in the USA (20, 31) could account for the unavailability of fruits and vegetables in the supermarkets. This is expected as mini-marts and smaller supermarkets would assign less shelf space to all products given their limited space.
While supermarkets/mini-marts provide access to healthier foods such as whole grain cereals, legumes, oilseeds and nuts, fresh milk, fresh yogurt, sugar-free milk and fresh fruit juice, a larger shelf area was devoted to unhealthy foods. For instance, the NOVA classification showed that 68% of the food products identified in all the supermarkets assessed were ultra-processed. In addition, a study conducted in Brazil, a middle-income country, showed that about 50% of ultra-processed foods were purchased from super/hypermarkets and mini-marts (32). This confirms the conclusion drawn from previous studies in Ghana that energy-dense, unhealthy foods are widely available (9, 16, 22, 28). And that, widespread availability of unhealthy food is therefore an issue of concern since a relatively high availability of such foods can influence preference and consumption of energy-dense, nutrient-poor foods. Relative availability of products is a major determinant of purchasing decisions and thus consumption (33).
Implications of findings
Our findings have implications for both researchers and policymakers. The widespread availability of ultra-processed foods (a proxy indicator of unhealthy foods) in the supermarkets/minimarts should be concerning to public health professionals. Governments, as well as the food industry, need to take actions. Policy makers seeking to improve health through dietary change, need to institute measures that improve relative availability of healthy, minimally processed foods within retail outlets. Such measures may include a mix of low-agency (fiscal policies, marketing restrictions) and high-agency (appropriate labeling) interventions.
Limitations
While this study has some strengths as discussed, there are a number of important limitations to be noted. First, we recorded a high non-response rate. Forty-one percentage of the managers of the modern retail outlets we approached declined to participate in the study—citing COVID-19 pandemic-related reasons. Relatedly, a few other retail outlets were not operating and could not be accessed. This limited the number of retail outlets assessed which could have led to a possible selection bias. It is possible that the retail outlet that denied us access had healthier food categories than unhealthy ones or vice versa. The current study's operational definition of supermarkets and mini-marts may not be comparable with that used in high income countries, and thus limits comparability. Indeed, given that the study was delimited to food retail outlets in the Greater Accra Region, we will discourage any attempt to do such extrapolations or generalizations. In addition, the retail outlets assessed used different display formats. For instance, some displayed vegetables on four smaller shelves placed on top of each other (where we measured the shelf length and breadth of all four shelves) and others placed the vegetables in one high bin (where we only measured 1 shelf length and breadth); the former might appear to have more vegetables than the latter, while actually the latter might have more if the quantity was measured. However, this was a rare occurrence. Finally, this analysis did not take into consideration food product price. Food product price has been highlighted as one of the strongest drivers of food acquisition and consumption, were not taken. Finally, while available evidence shows a very strong correlation between ultra-processed foods and high content of free/added sugars, sodium and saturated fatty acids, we note that calorie density and level of processing are not foolproof indicators of healthiness or lack thereof.
Conclusions
This study reveals widespread availability of unhealthy/ultra-processed foods in supermarkets/mini-marts in Greater Accra. For every 1 m2 of shelf area for healthy foods, there was 5 m2 of shelf area for unhealthy foods on average. For each unprocessed or minimally processed food product, there were 5 ultra-processed food products available in the supermarket/mini-mart on average. Relevant actors (the Food and Drugs Authority, Ministry of Food and Agriculture, Local Government, private sector, etc.) need to institute measures that improve relative availability of healthy, minimally processed foods within supermarkets/mini-marts.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ghana Health Service Ethics Review Committee (GHS-ERC 005/06/19) and the University of Ghana Ethics Review Committee for the Humanities (ECH 152/18-19).
Author contributions
AA and AL conceptualized the research question. AA performed the analysis and drafted the manuscript. GSA coordinated the data collection. WQ, AT, SV, and PA assisted in data collection. GSA, WQ, AT, RA, MH, CA, FZ, ML, KM, PA, DL, GA, DS, SV, and AL provided critical feedback, helped shape the research, analysis, and manuscript. AL supervised the work. All authors contributed to the manuscript and approved the submitted version.
Funding
This study was supported by funding from the International Development Research Centre (IDRC) Food, Environment, and Health Program—IDRC, Canada—Grant Number: 108983-001. The funder, however, played no role in the study design, data collection, analysis or interpretation, or in writing the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Stringhini S, Carmeli C, Jokela M, Avendaño M, Muennig P, Guida F, et al. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1·7 million men and women. Lancet. (2017) 389:1229–37. doi: 10.1016/S0140-6736(16)32380-7
2. Dubois P, Griffith R, O'connell M. The effects of banning advertising in junk food markets. Rev Econ Stud. (2018) 85:396–436. doi: 10.1093/restud/rdx025
3. Monteiro CA, Cannon G, Levy RB, Moubarac JC, Louzada MLC, Rauber F, et al. Ultra-processed foods: What they are and how to identify them. Public Health Nutr. (2019) 22:936–41. doi: 10.1017/S1368980018003762
4. Osei-Kwasi H, Mohindra A, Booth A, Laar A, Wanjohi M, Graham F, et al. Factors influencing dietary behaviours in urban food environments in Africa: A systematic mapping review. Public Health Nutr. (2020) 23:2584–601. doi: 10.1017/S1368980019005305
5. Swinburn BA, Sacks G, Hall KD, McPherson K, Finegood DT, Moodie ML, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. (2011) 378:804–14. doi: 10.1016/S0140-6736(11)60813-1
6. Tsrah P, Quarpong W, Laar A. Healthiness of foods on promotional flyers of fast-food outlets located within Accra-based shopping malls. World Nutr. (2020) 11:51–61. doi: 10.26596/wn.202011351-61
7. GEPA. Ghana Ranks 1st in Africa, 4th Globally in Latest Global Retail Development Index - GEPA Exporters Portal. GEPA GHANA. (2020). Available online at: https://www.gepaghana.org/ghana-ranks-1st-in-africa-4th-globally-in-latest-global-retail-development-index/
8. Balineau G, Bauer A, Kessler M, Madariaga N. Food Systems in Africa. Food Syst Africa Rethink Role Mark. (2021). Available online at: https://openknowledge.worldbank.org/handle/10986/34919
9. Andam KS, Tschirley D, Asante SB, Al-Hassan RM, Diao X. The transformation of urban food systems in Ghana: Findings from inventories of processed products. Outlook Agric. (2018) 47:233–43. doi: 10.1177/0030727018785918
10. Holdsworth M, Pradeilles R, Tandoh A, Green M, Wanjohi M, Zotor F, et al. Unhealthy eating practices of city-dwelling Africans in deprived neighbourhoods: Evidence for policy action from Ghana and Kenya. Glob Food Sec. (2020) 26:100452. doi: 10.1016/j.gfs.2020.100452
11. Crimarco A, Landry MJ, Gardner CD. Ultra-processed foods, weight gain, and co-morbidity risk. Curr Obesity Rep. (2021) 1:3. doi: 10.1007/s13679-021-00460-y
12. Hall KD, Ayuketah A, Brychta R, Cai H, Cassimatis T, Chen KY, et al. Ultra-processed diets cause excess calorie intake and weight gain: an inpatient randomized controlled trial of ad libitum food intake. Cell Metab. (2019) 30:67–77.e3. doi: 10.1016/j.cmet.2019.05.008
13. Vandevijvere S, Jaacks LM, Carlos |, Monteiro A, Moubarac J-C, Girling-Butcher M, et al. Global trends in ultraprocessed food and drink product sales and their association with adult body mass index trajectories. Obes Rev. (2019) 20:10–9. doi: 10.1111/obr.12860
14. Benton JS, Anderson J, Hunter RF, French DP. The effect of changing the built environment on physical activity: A quantitative review of the risk of bias in natural experiments. Int J Behav Nutr Phys Act. (2016) 13:e0433. doi: 10.1186/s12966-016-0433-3
15. Amevinya GS, Quarpong W, Laar A. Commercial food advertising on the campus of Ghana's largest University. World Nutr. (2020) 11:57–73. doi: 10.26596/wn.202011257-73
16. Green MA, Pradeilles R, Laar A, Osei-Kwasi H, Bricas N, Coleman N, et al. Investigating foods and beverages sold and advertised in deprived urban neighbourhoods in Ghana and Kenya: a cross-sectional study. BMJ Open. (2020) 10:e035680. doi: 10.1136/bmjopen-2019-035680
17. Cairns G, Angus K, Hastings G, Caraher M. Systematic reviews of the evidence on the nature, extent and effects of food marketing to children. A retrospective summary. Undefined. (2013) 62:209–15. doi: 10.1016/j.appet.2012.04.017
18. Gan WY, Mohamed SF, Law LS. Unhealthy lifestyle associated with higher intake of sugar-sweetened beverages among malaysian school-aged adolescents. Int J Environ Res Public Health. (2019) 16:15. doi: 10.3390/ijerph16152785
19. Curhan RC. The effects of merchandising and temporary promotional activities on the sales of fresh fruits and vegetables in supermarkets. J Mark Res. (1974) 11:286–94. doi: 10.1177/002224377401100307
20. Farley TA, Rice J, Bodor JN, Cohen DA, Bluthenthal RN, Rose D. Measuring the food environment: Shelf space of fruits, vegetables, and snack foods in stores. J Urban Heal. (2009) 86:672–82. doi: 10.1007/s11524-009-9390-3
21. Vandevijvere S, Mackenzie T, Mhurchu CN. Indicators of the relative availability of healthy versus unhealthy foods in supermarkets: a validation study. Int J Behav Nutr Phys Act. (2017) 14:e0512. doi: 10.1186/s12966-017-0512-0
22. Kroll F, Swart EC, Annan RA, Thow AM, Neves D, Apprey C, et al. Mapping obesogenic food environments in South Africa and Ghana : Correlations and contradictions. Sustainability. (2019). 11:3924. doi: 10.3390/su11143924
23. Aryeetey R, Oltmans S, Owusu F. Food retail assessment and family food purchase behavior in Ashongman Estates, Ghana. African J Food Agric Nutr Dev. (2016) 16:11386–403. doi: 10.18697/ajfand.76.15430
24. Laar A, Kelly B, Holdsworth M, Quarpong W, Aryeetey R, Amevinya GS, et al. Providing measurement, evaluation, accountability, and leadership support (MEALS) for non-communicable diseases prevention in ghana: project implementation protocol. Front Nutr. (2021) 8:e644320. doi: 10.3389/fnut.2021.644320
25. Mhurchu CN, Vandevijvere S, Waterlander W, Thornton LE, Kelly B, Cameron AJ, et al. Monitoring the availability of healthy and unhealthy foods and non-alcoholic beverages in community and consumer retail food environments globally. Obes Res Clin Pract. (2013) 7:e18. doi: 10.1016/j.orcp.2013.12.535
26. Vandevijvere. Towards Healthier Supermarkets - Google Search. Available online at: https://www.google.com/search?q=vandevijvere+et+al.%2C+(2018).+towards+healthier+supermarkets&oq=vandevijvere&aqs=chrome.2.69i59j69i57j35i39j0i30l3j0i10i30j0i30l3.6514j0j9&sourceid=chrome&ie=UTF-8
27. World Cancer Research Fund International. Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective. Washington, DC: American Institute for Cancer Research. (2007).
28. Dake FAA, Thompson AL, Ng SW, Agyei-Mensah S, Codjoe SNA. The local food environment and body mass index among the urban poor in Accra, Ghana. J Urban Heal. (2016) 93:438–55. doi: 10.1007/s11524-016-0044-y
29. Poverty Index Ghana Statistical Service - Google Search. Available online at: https://www.google.com/search?q=POVERTY+INDEX%2C+GHANA+STATISTICAL+SERVICE&oq=POVERTY+INDEX%2C+GHANA+STATISTICAL+SERVICE&aqs=chrome.69i57j35i39j0i512l8.52983j0j7&sourceid=chrome&ie=UTF-8
30. Leite M, Assis M, Carmo A, Costa B, Claro R, Castro I, et al. Is neighbourhood social deprivation in a Brazilian city associated with the availability, variety, quality and price of food in supermarkets? Public Health Nutr. (2019) 22:3395–404. doi: 10.1017/S1368980019002386
31. Rose D, Hutchinson PL, Bodor JN, Swalm CM, Farley TA, Cohen DA, et al. Neighborhood food environments and body mass index the importance of in-store contents. Am J Prev Med. (2009) 37:214. doi: 10.1016/j.amepre.2009.04.024
32. Costa JC, Claro RM, Martins AP, Levy RB. Food purchasing sites. Repercussions for healthy eating. Appetite. (2013) 70:99–103. doi: 10.1016/j.appet.2013.06.094
33. Thornton LE, Cameron AJ, McNaughton SA, Waterlander WE, Sodergren M, Svastisalee C, et al. Does the availability of snack foods in supermarkets vary internationally? Int J Behav Nutr Phys Act. (2013) 10:1–9. doi: 10.1186/1479-5868-10-56
Appendix
Appendix 1. The availability [measured by shelf area (m2)] of the different food items in the retail outlets assessed in the six.
Keywords: ultra-processed food, modern retail outlets, supermarket, non-communicable diseases, Ghana
Citation: Adjei AP, Amevinya GS, Quarpong W, Tandoh A, Aryeetey R, Holdsworth M, Agyemang C, Zotor F, Laar ME, Mensah K, Addo P, Laryea D, Asiki G, Sellen D, Vandevijvere S and Laar A (2022) Availability of healthy and unhealthy foods in modern retail outlets located in selected districts of Greater Accra Region, Ghana. Front. Public Health 10:922447. doi: 10.3389/fpubh.2022.922447
Received: 18 April 2022; Accepted: 26 September 2022;
Published: 09 November 2022.
Edited by:
Peter Delobelle, University of Cape Town, South AfricaReviewed by:
Farhana Akter, Chittagong Medical College, BangladeshLarissa Loures Mendes, Federal University of Minas Gerais, Brazil
Copyright © 2022 Adjei, Amevinya, Quarpong, Tandoh, Aryeetey, Holdsworth, Agyemang, Zotor, Laar, Mensah, Addo, Laryea, Asiki, Sellen, Vandevijvere and Laar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amos Laar, QUxhYXJAdWcuZWR1Lmdo