
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 28 September 2022
Sec. Public Mental Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.919827
This article is part of the Research TopicNoncommunicable Diseases and Mental Health Experiences Before and After the COVID-19 PandemicView all 14 articles
 Flavio Mandlate1,2*
Flavio Mandlate1,2* M. Claire Greene3Luis F. Pereira4
M. Claire Greene3Luis F. Pereira4 Annika C. Sweetland4Donald Kokonya5
Annika C. Sweetland4Donald Kokonya5 Cristiane S. Duarte4
Cristiane S. Duarte4 Francine Cournos4Maria A. Oquendo6
Francine Cournos4Maria A. Oquendo6 Milton L. Wainberg4
Milton L. Wainberg4 Mohsin Sidat7Esperança Sevene7
Mohsin Sidat7Esperança Sevene7 Marcelo F. Mello2
Marcelo F. Mello2Introduction: Depression is the most common mental disorder among people living with HIV/AIDS and has a negative impact on HIV treatment outcomes. Training lay HIV counselors to identify and manage depression may contribute to improved patient access and adherence to treatment, and reduce stigma and discrimination among lay health workers toward both HIV and depression. The purpose of this study was to assess the current knowledge and attitudes of lay HIV counselors toward managing depression in primary care in Mozambique.
Methods: We conducted a mixed-methods cross-sectional study to assess depression-related knowledge and attitudes among lay HIV counselors in 13 primary healthcare facilities in Mozambique. We used the quantitative Depression Attitude Questionnaire (DAQ) scale, followed by open-ended questions to further explore three key DAQ domains: the nature of depression, treatment preferences, and professional attitudes or reactions.
Results: The sample included 107 participants (77.6% female, mean age: 32.3 years, sd = 7.4). Most (82.2%) had less than a high/technical school education. Findings suggested that some HIV counselors had knowledge of depression and described it as a cluster of psychological symptoms (e.g., deep sadness, anguish, apathy, isolation, and low self-esteem) sometimes leading to suicidal thoughts, or as a consequence of life stressors such as loss of a loved one, abuse, unemployment or physical illness, including being diagnosed with HIV infection. HIV counselors identified talking to trusted people about their problems, including family and/or counseling with a psychotherapist, as the best way for patients to deal with depression. While acknowledging challenges, counselors found working with patients with depression to be rewarding.
Conclusion: Lay health counselors identified HIV and psychosocial issues as key risk factors for depression. They believed that the treatment approach should focus on social support and psychotherapy.
In 2019, UNAIDS estimated that 38 million people were living with HIV infection worldwide, and over 54.47% of the people with HIV and AIDS in Sub-Saharan Africa (1, 2). Mozambique is disproportionately affected by HIV and AIDS; in 2019, it had an estimated 2,183,786 people living with HIV (PWH), with 59% on antiretroviral treatment (3), and 23% who did not know their HIV status and therefore were not in treatment (2). The burden of depression among people with HIV in sub-Saharan Africa is estimated at 27% (4). The prevalence of major depressive disorder in Mozambique is 12.1% while the prevalence of depressive symptoms is 26.9% (4). Results from studies from 15 sub-Saharan countries found an estimated prevalence of depression between 6 and 59% among people living with HIV using screening tools such as the PHQ-9 (5).
Psychiatric disorders are commonly diagnosed among PWH, and depression is the most common diagnosis; some studies estimate a prevalence of over 50% (6). Depression and HIV infection have a bidirectional relationship. First, HIV infection increases the risk for depressive symptoms due to direct viral effects (HIV infects central nervous system cells), activation of the hypothalamic-pituitary-adrenal axis, increase in various inflammatory markers (TNFα, IFNγ, IL-1, and IL-6), side effects of antiretrovirals, as well as psychological stressors and vulnerabilities commonly seen in populations affected by HIV, including stigma, disability, isolation, discrimination, and poor social support (7). Second, depression has been shown to increase the progression of HIV infection, in part by affecting adherence to medications and medical care (8) as well as by its association with higher morbidity and mortality (9, 10). Depression can also be seen as a risk factor for HIV infection due to the increased likelihood of risky behaviors such as unprotected sex, multiple sex partners, and the use of intravenous drugs (7, 11). Despite the known burden and public health effects of depression on HIV infection (4), this psychiatric disorder is still underdiagnosed and undertreated in PWH (5, 12, 13).
Due to the shortage of health workers in low- and middle-income countries (LMICs) lay health counselors play a crucial role in service delivery and psychosocial support in HIV and AIDS services, mainly in primary health care (14, 15). Non-communicable disease providers in Malawi reported limited knowledge and lack of training about depression, along with inadequate resources (e.g., staff shortages, drug supply, high workload, long patient waiting times for appointments, lack of physical space) as the greatest barriers to integrating depression treatment into primary care (16). The shortage of mental health specialists in low-income countries is associated with low capacity for diagnosing and treating depression (4). To overcome this shortage, a task-shifting approach (i.e., training non-specialists to deliver mental health interventions) has been utilized in many LMICs to treat mental health problems such as depression, anxiety, and substance use in primary care and other healthcare settings (17). Mounting evidence suggests that lay health workers can be trained to deliver evidence-based treatments for depression through task-shifting when provided adequate clinical supervision (18, 19). Evidence-based interventions delivered by non-specialized health workers in primary health care settings for the treatment of depression could relieve or improve depressive symptoms and medical treatment outcomes for patients (20).
Many approaches to task shifting have been successfully tested and implemented in LMICs, indicating that through appropriate capacity building, non-mental health professionals and community health workers can assess and successfully manage mental health problems, including as part of HIV care (21, 22). As an example, depression treatment was successfully integrated into HIV care in Malawi; non-mental health care service providers were trained to screen, diagnose, and treat depression using antidepressants and psychotherapy (23–25). However, some implementation challenges arose regarding sustainability, patient retention, and providers' workloads given the limited-resource setting (23). Another study conducted in Cameroon found that primary care providers demonstrated poor knowledge and negative attitudes toward depression (26). Lay counselors often have different educational backgrounds and usually receive short-term intensive courses in counseling skills, but they do not receive any training in other mental health care topics (17, 19, 27). Skills development and technical ability are essential for effective counseling services, which goes beyond empathy and understanding of the client (17). Ongoing clinical supervision beyond the intensive training phase is a critical component of this approach (28).
Effective interventions for the treatment of depression delivered by lay health workers in low resource settings, such as group interpersonal therapy and problem-solving therapy, have demonstrated improvement in ART adherence and depressive symptoms among PWH in South Africa and Zimbabwe (29–31). Among patients with HIV, additional behavioral interventions have reduced depression relapses and improved wellness (28). However, additional studies are needed to understand the best way to implement evidence-based depression treatment (32). Gaps and challenges in integrating mental health into HIV treatment in general care health systems are evident, particularly in primary health care settings (33, 34). These gaps call for adaptation and implementation of feasible mental health interventions targeting community health workers and other stakeholders to improve the mental health of PWH (35), and have shown promising outcomes (24).
In Mozambique, lay health counselors play a key role in providing HIV counseling and testing services and psychosocial support follow-up for PWH on antiretroviral treatment (ART) (27, 36, 37). However, lay HIV health counselors are only assigned to facilities that treat a minimum of 1,000 PWH; smaller rural facilities lack support from this cadre of workers (37). The training of lay HIV counselors aims to improve overall communication, differentiate and apply diverse counseling techniques, with an emphasis on adherence counseling, and provide essential psychosocial support to PWH (36, 38). Because these HIV counselors are not trained in mental health and do not have appropriate instruments for depression screening (38, 39), referrals to mental health professionals are rare and usually occur only when there are overt changes in mood or poor adherence to ART. A task-shifting approach to mental health could minimize these challenges in HIV care if lay HIV counselors were trained to identify and manage depression (20), as they are the first contact point for PWH with health services at the primary care level (40). Notably, advocacy for mental health integration may also help to reduce HIV-associated stigma and discrimination and contribute to enhanced treatment outcomes among PWH (41). This task-shifting approach must be accompanied by adequate and continuous training, supervision, mentorship, and emotional support for lay health workers to effectively integrate mental health in HIV treatment services (14, 28, 42).
In this study, we evaluated the knowledge and attitudes of lay HIV counselors in Mozambique regarding depression to better understand the potential gaps in their practice. The secondary aim was to gather evidence that could be used to improve any future training program for lay counselors in the management of depression and other mental health related issues among PWH.
This study was a mixed-methods cross-sectional study investigating knowledge and attitudes among lay HIV counselors in Mozambique toward depression. Between April and November 2019, we randomly selected 13 primary health care centers from two provinces: six in Maputo Province and seven in Maputo city, and invited all HIV counselors to participate. This yielded a convenience sample of 107 providers (93.04% response rate). We considered the following eligibility criteria: currently working as a lay HIV counselor at primary care health centers (HIV, TB, Maternal and Child Health), having been a lay HIV counselor for more than 3 months, and providing written informed consent to participate in the study.
Participants provided basic information about their clinical background as well as sociodemographic information, including age, sex, education, marital status, type of counselor, years of counseling experience, and whether they had prior training in managing mental health problems. A research assistant administered the Depression Attitudes Questionnaire (DAQ) (43). We chose the DAQ because it was relevant to the research question, available in Portuguese, and culturally adaptable to Mozambique context. The DAQ includes 20 statements with 5-point Likert Scale response options ranging from strongly agree to strongly disagree. For the analysis, we collapsed the 5-point Likert scale responses to 3 points “disagree”; “neutral” and “agree.” The 20 statements/questions are grouped into three domains. The three domains include: nature of depression (nine items: Q1, Q2, Q4, Q5, Q6, Q7, Q8, Q10 and Q11); treatment of depression (eight items: Q3, Q12, Q14, Q16, Q17, Q18, Q19, and Q20), and professional attitudes (three items: Q9, Q13 and Q15). The domain “nature of depression” corresponded to depression risk factors and clinical features (44). The “treatment of depression” domain describes the treatment orientation and confidence in types of treatment, and the “professional reaction” domain is the professional confidence and ease in managing the needs of depressed patients (45).
After completing the DAQ, each participant was asked a brief set of open-ended qualitative questions to further explore participants knowledge about diagnosis, symptoms, related risk factors, management and prevention of depression. These follow up questions were structured around the three domains of the DAQ, in order to further elucidate the participants' perspectives on these topics. For the first domain, “nature of depression,” after administering the series of structured questions from the DAQ, we asked providers to use their own words to define depression, the common symptoms, and the perceived risk factors. We also asked specifically whether they considered HIV and AIDS to be a risk factor for depression, as well as to identify barriers to mental health treatment among people with HIV. For the second domain, “treatment of depression,” after asking their agreement to various statements about treatment alternatives for depression from the DAQ, we asked participants to use their own words to describe the types of depression treatment available locally, and where the services were provided. For the third domain, “professional attitudes,” we asked counselors to describe in their own words how they help patients with depression, and if they knew of any strategies to prevent depression in people with and without HIV. The qualitative interviews were recorded and then transcribed by the research assistants. The researcher revised each transcript to verify the accuracy of the data. After transcription of the interview, the voice records were stored on a password-protected computer, only accessed by the researcher. The average duration of each interview was 25 to 30 minutes. All interviews were conducted in Portuguese.
All study procedures were reviewed and approved by the two Ethics Committees (from Federal University of São Paulo in Brazil and Eduardo Mondlane University in Mozambique).
We used an explanatory QUANT = >QUAL sequential mixed-methods approach to data collection and analysis whereby the quantitative questions were asked first, and the qualitative questions were used to further explain and expand upon each domain (46, 47). For the quantitative data, we used frequency statistics to describe the distribution of demographic characteristics, training, and clinical experience in the sample for the quantitative data. We used Stata, Version 17 for the quantitative analysis. We also calculated the internal consistency of the three DAQ subscales using Cronbach's alpha.
For the qualitative data, we used software NVIVO version 10 to file and organize verbatim transcriptions of the interviews. We utilized a directed content analytic approach wherein we began analysis examining the three sub-domains of the DAQ and then broadened our analysis to include additional pre-defined topics (47). We thereafter quantified all qualitative data by coding, thematic analysis and describing patterns that emerged in the data (48, 49). All qualitative data were coded according to predominant themes identified by FM and LFG independently. The raters worked collaboratively to develop a taxonomy of the initial themes that emerged from the data. MCG and ACS supervised the coding and re-coding at different steps of this process to verify that findings were grounded in the data. Finally, we compared the qualitative responses by domain to the quantitative findings to help interpret those observations. When there was overall agreement in the sentiment of the qualitative statements and the quantitative findings, we had more confidence that questions were being understood in the correct way. When apparent contradictions emerged between the qualitative and quantitative data, we looked to the qualitative data to try to understand if those differences were real or if another explanation–such as the misunderstanding of one or more questions–could better explain the observations.
In this sample of 107 study participants, the average age was 32.3 years (SD = 7.4), 77.6% were female, 82.2% reported their educational level as being less than middle/technical school, and 42.1% were married. About one-third of the study participants provided HIV testing and counseling, and few had prior mental health training (15.0%). On average, participants had 4 years of HIV counseling experience (range 1–15, SD = 3.5, Median = 2) (Table 1). Examination of the psychometric properties of the DAQ revealed poor internal consistency across the subscales: nature of depression (alpha = 0.393), depression treatment (alpha = 0.422), and professional attitudes (alpha = 0.338). A post-hoc analysis revealed that the internal consistency of the scales was slightly higher, but still relatively low, among the study participants with prior mental health training (nature of depression: alpha = 0.648; depression treatment: alpha = 0.512; professional attitudes: alpha = 0.586) (Table 2).
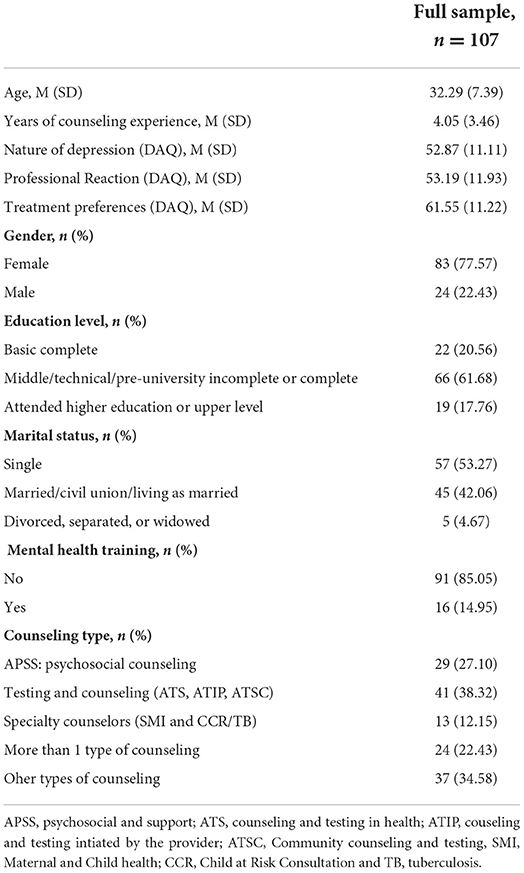
Table 1. Characteristics of the sample.
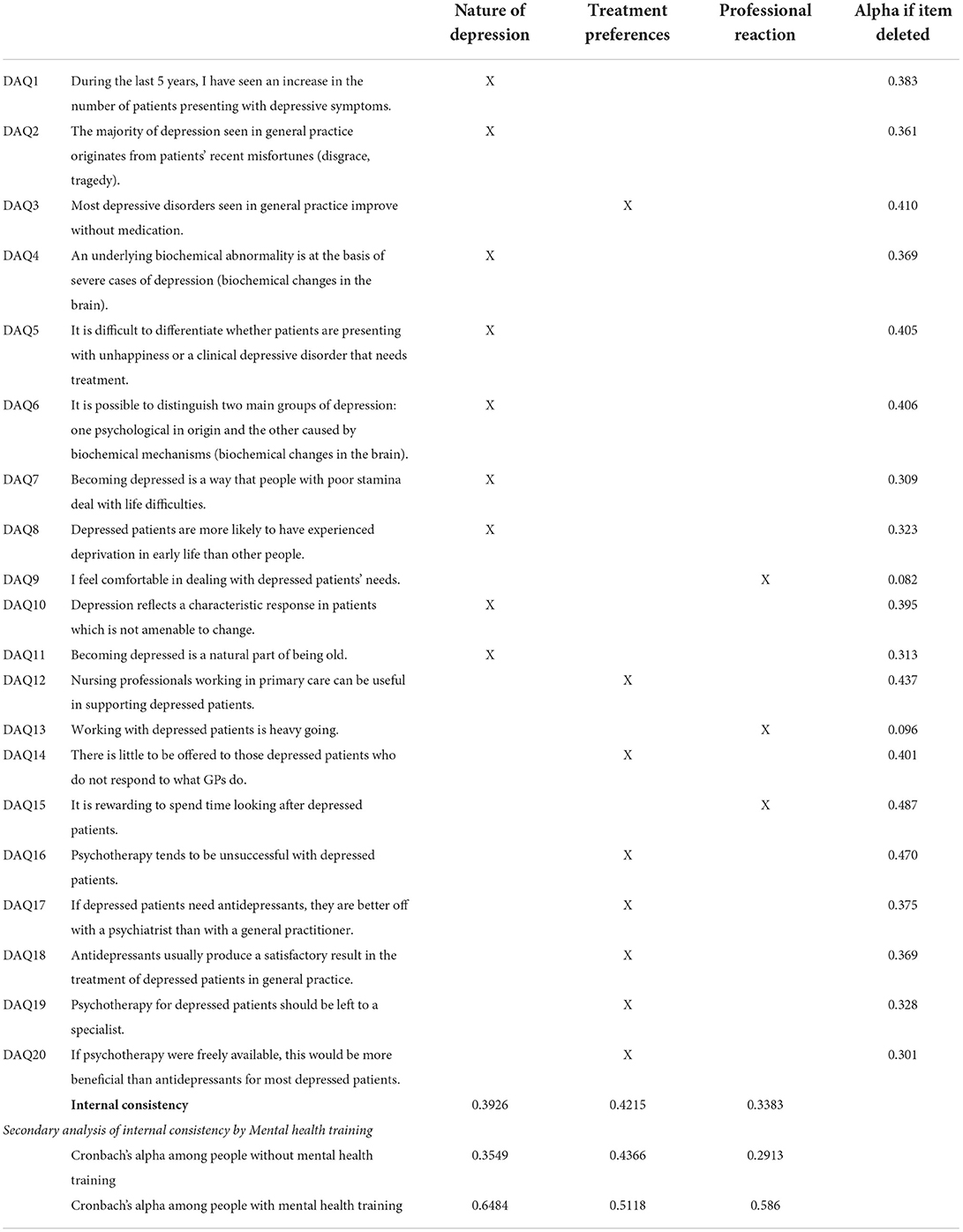
Table 2. Psychometric characteristics.
There was substantial variation in the proportion of participants who agreed with certain statements regarding the nature of depression, depression treatment, and professional attitudes, which are detailed below (Table 3).
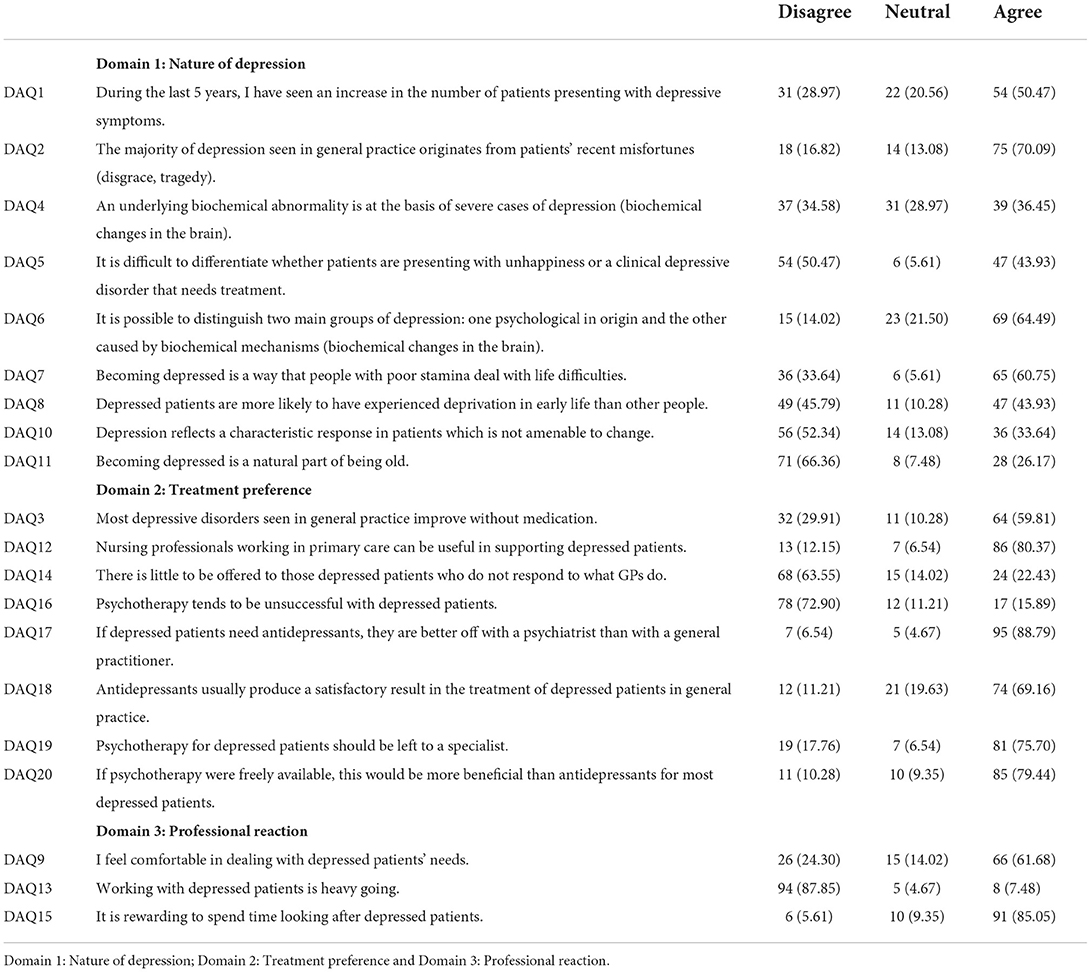
Table 3. Summary of quantitative findings by domain.
Almost all (98.1%) participants reported that they had heard of depression, but fewer than half of the participants reported personally knowing someone with depression. The majority of the counselors reported having learned about depression through their professional practice, while a few learned about it through in-service training and academia or had found information about depression through reading books. On the DAQ scale, a majority (64.49%, n = 71) disagreed that “becoming depressed is a natural part of being old” (question 11) and 52.34% (n = 56) disagreed that “depression reflects a characteristic response in patients which is not amenable to change” (question 10). Almost half of participants 50.47% (n = 54) agreed that during the last 5 years, [they] have observed an increase in the number of patients presenting with depressive symptoms (question 1) and most (70.09%, n = 75) agreed that “the majority of depression seen in general practice originates from patients' recent misfortunes (disgrace, tragedy)” (question 2). However, many counselors 60.75% (n = 65) revealed some stigmatizing attitudes by agreeing that becoming depressed is a way that “fragile” people deal with life's difficulties (question 7) (Table 3).
For other statements relating to the nature of depression, including biochemical and biological origins, there was limited agreement (34.58%, n = 37 disagreed; 28.97%, n = 31 were neutral; and 36.45%, n = 39 agreed) among participants (question 4); 60.75% (n = 69) considered that it was possible to distinguish different presentations of depression (psychological, biochemical, or related to adversity); and almost half 45.79% (n = 49) of the participants believed that patients with depression probably experienced more childhood deprivation than other people (question 8) (Table 3). When asked about risk factors for depression, only a few participants considered heredity as a biological risk factor, whereas most cited psychosocial factors such as marital, social, and financial problems; unemployment; and trauma, sexual, physical, or verbal violence happening in childhood and adulthood.
Subsequent qualitative inquiry revealed a more nuanced conceptualization of depression, characterized in two ways. The first description included one or more of the following words: a psychological or psychiatric illness that is characterized by a feeling of deep sadness, anguish, apathy, altered mood, isolation, low self-esteem, inactivity, guilt, and sometimes suicidal thoughts or ideation.
“Depression is a psychiatric illness characterized by a feeling of deep sadness, apathy, mood swings, inactivity, and sometimes suicidal thoughts or ideation…” Male HC, 46 years old
The second type was depicted as more of an emotional reaction to unexpected stressful situations (e.g., results of an HIV test) and difficulties in dealing with problems.
“(depression) is a disease that affects people with difficulties in overcoming certain problems in life; when it is not treated, it can become chronic and lead to suicide…” Female HC, 36 years old
Participants described depression in five main ways: (1) isolation (feeling alone, social isolation, being isolated, abandoned, not wanting to be with others, withdrawing, bashful, staying in your corner, hiding); (2) sadness (deep sadness, feeling depressed, distraught, disappointed, dysphoric mood; negative mood and behavior); (3) apathy (weak, haggard, passive); (4) restlessness (being out of your mind, becoming stressed, upset); and (5) suicidal ideation (loses desire to live, loses interest in living, thinking about wanting to die, wanting to take one's life) (Table 4).
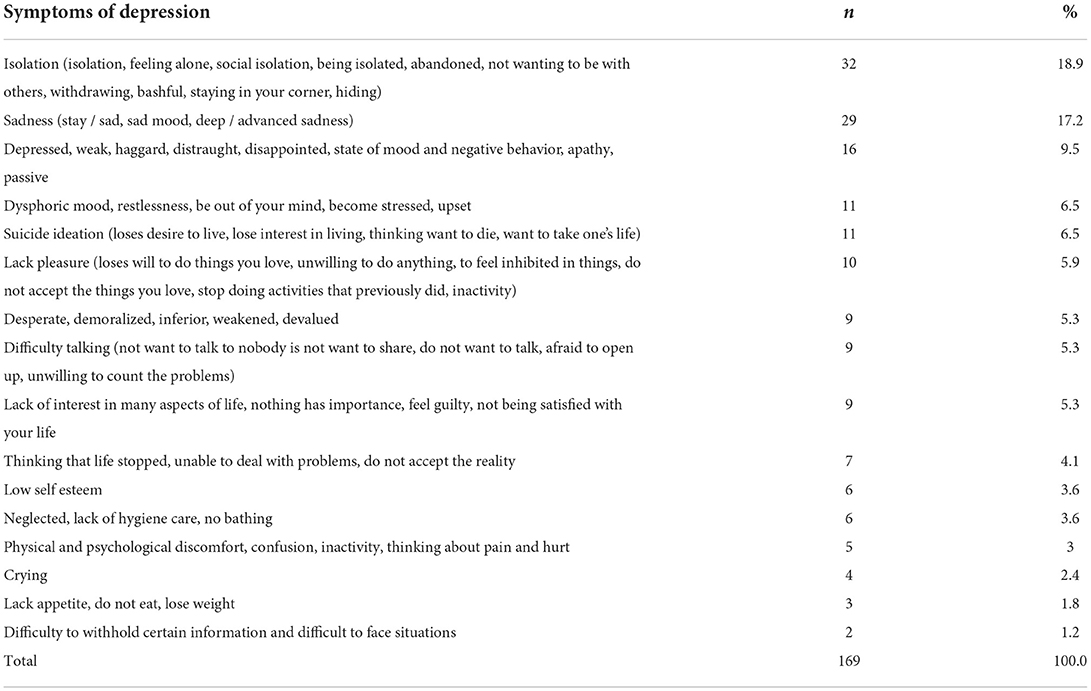
Table 4. Symptoms of depression.
When asked about risk factors for depression, participants mentioned low self-esteem; lack of resilience; heredity (genetic predisposition); isolation; marital, social, and financial problems; unemployment; trauma (verbal, physical, sexual, or psychological violence); alcohol and drug abuse; and/or death or loss of loved one. Nearly all believed HIV was a risk factor for depression due to learning of the HIV diagnosis as a chronic disease requiring medication for life, as well as introducing problems of discrimination, stigmatization, and prejudice (Table 5).
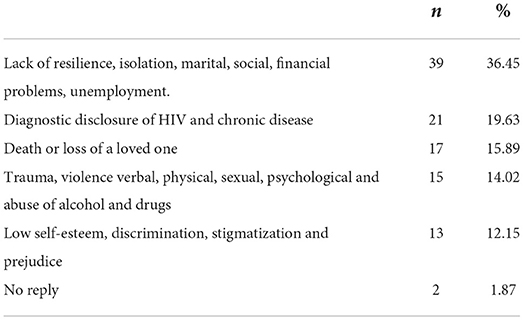
Table 5. Depression factors.
The four of the most commonly cited risk factors for depression were marital, social, financial, and unemployment problems followed by learning the diagnosis of chronic conditions such as HIV; death or loss of loved ones; and traumatic experiences during childhood and adulthood (verbal, physical, psychological, domestic and sexual abuse). Other risk factors mentioned were discrimination, stigmatization and prejudice, solitude and isolation, anxiety and worry, difficulty expressing oneself, unhealthy lifestyle (addiction, alcohol and substance abuse), low self-esteem, lack of resilience, expression difficulty, being postpartum, and heredity (Table 5).
“… Loss of a loved one, consumption of psychoactive substances, unresolved grief, job loss, unemployment and chronic illnesses …” Female HC, 37 years old
“… Abuses and mistreatment in childhood without opening up to someone can cause trauma in adult life; cost of living and wars that can lead to future depression…” Female HC. 37 years
“… Lack of employment, lack of family support, discrimination and grief …” Female HC, 41 years old
Almost all participants believed that HIV was a risk factor for depression. The association between HIV and depression was explained through difficulty accepting the test result; fear of disclosing the diagnosis to a partner and/or family member; fear of discrimination; hopelessness; difficulty facing HIV and AIDS as a chronic disease without cure requiring treatment for life. According to the health counselors, the main problems described by HIV positive patients that could increase the risk of depression were lack of family support, discrimination, and lack of support and conflict with a partner; not speaking or speaking little; not knowing what depression is; difficulty/fear in disclosure to the partner and acceptance of the diagnosis; taking medication and its side effects; poverty, hopelessness, financial/transportation/food difficulties; and poor treatment (Table 6).
“… Generally speaking, it can (cause depression). Those people who do not want to accept their status, think that HIV is the end of life and the person alone begins to feel discriminated against without others knowing what their status is …” Female HC, 33 years old
“… Yes, for example, when the person is tested and the result is positive (for HIV), he goes into depression because he thinks it is the end of his life and he is afraid to tell his family.…” Female HC, 34 years
“… Currently, since the care is integrated and people are informed about HIV, (depressive symptoms) do not develop. Years ago, people could develop depression because they thought it was the end of life …” Male HC, 24 years old
“… I think (HIV can cause depression), first because it is a disease that is not curable, and second, because the person with HIV is vulnerable to being discriminated against, the long-time treatment, and at some point, the side effects of the treatment …” Male HC, 41 years old.
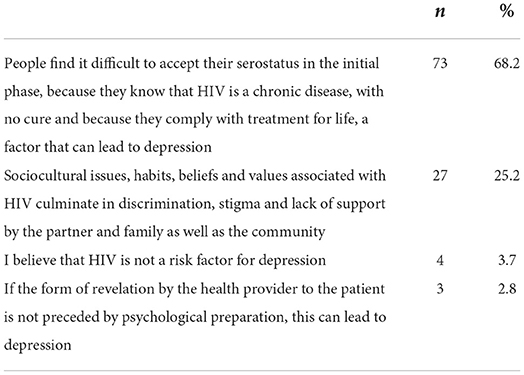
Table 6. HIV/AIDS associated with depression.
Providers also talked about the main problems described to them by patients, which included the lack of social and financial support, lack of partner and family support, discrimination, stigma, and interpersonal conflict. Other patient concerns reported by the counselors were uncertainty, the fear of revealing their diagnosis to their partners, and the fear of medication's side effects (Table 7).
“… There are people who talk. Sometimes they talk about lack of money for transport and food, abuse in the family and even in the hospital, they face some shame…” Male HC, 60 years old
“… They even talk when we do not have time to talk to them. Many of them do not open up. The problems are poverty, the illness itself and frequent losses in the family …” Female HC, 28 years old
“… Yes, they do (talk about depression). (They) often question whether they still will be the same individuals and are concerned too often with medication and what family or friends think of it ...” Female HC, 33 years
“… The lack of acceptance of the diagnosis and the fact that he is not debilitated makes him not accept his status …” Male HC, 23 years old
“…Some talk (about their problems), that they feel alone, that they don't have enough money (for transportation), stigma, lack of family support, non-acceptance of the (HIV) positive diagnosis and fear of going to the health facility…” Male HC, 26 years old.
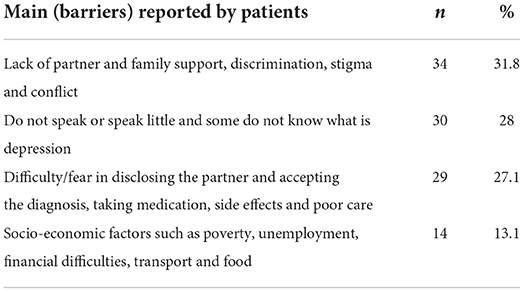
Table 7. Lay counselors' description of barriers reported by patients.
The most cited preventive mechanisms for depression were communication (conversation/dialogue) with family members or trusted people about problems and concerns; seeking support from friends; counseling and follow-up with a psychologist; and self-esteem, socialization, avoiding stress, stigma, violence, and other life situations. The other forms of prevention were disseminating information and lectures on depression through social media (TV, radio), relaxation, and sports to cope with problems (Table 8).
“… Talking more to people, someone trustworthy exposing the problems. Having the habit of looking for a psychologist to express concerns…” Female HC, 29 years old
“… Talk to trusted and experienced people in case of any discomfort or difficulty, seek support at the level of health units for better clarification…” Female HC, 37 years old
“… More community involvement and events, as an alternative for dissemination …” Male HC, 26 years old
“… First, there must be dialogue in a family, health providers must try to listen or listen to the patient and help him …” Female HC, 36 years old
“… I believe that conversation and counseling help to distract the mind so that the person does not always think about being HIV positive …” Female HC, 38 years old
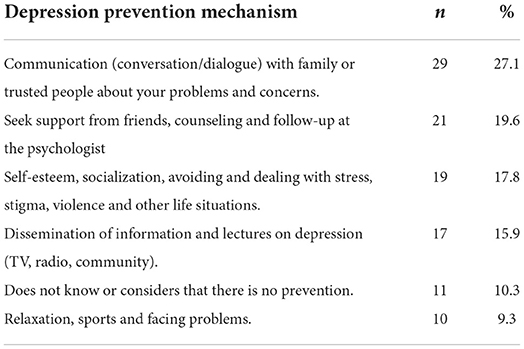
Table 8. Depression prevention mechanisms reported by lay health counselors.
Most lay HIV counselors supported psychotherapy and medication to treat depression but most believed mental health specialists should provide it. The majority 75.70% (n = 81) agreed with the statement “psychotherapy in patients with depression should be left to the specialist” (question 19) and 59.81% (n = 64) agreed with the statements “most depressive disorders seen in general practice improve without medication” (question 3) and 80.37% (n = 86) believed that “nursing professionals working in primary care can be useful in supporting depressed patients” (question 12). Many 63.55% (n = 68) did not endorse the statement “there is very little to offer patients with depression who do not get better with the treatment proposed by the general practitioner” (question 14); however 72.90% (n = 78) disagreed that “psychotherapy in patients with depression does not usually give good results” (question 16), and 79.44 (n = 85) agreed that “if psychotherapy were freely available, it would have more benefits than antidepressants for most patients with depression” (question 20) (Table 3). When asked qualitatively, the counselors reported that they believed it was possible to treat depression, and this treatment could be through a psychologist, psychiatric technician or specialist for medications and the other option was counseling, psychosocial support and/or through support groups (family and community) (Table 9).
“… I think it is possible (to treat depression), there are several forms of treatment, through counseling, empathy, medication, lectures and socializing with people who have already been through the same situation.…” Male HC, 24 years old
“… It is (treatable), depending on the type, there are cases in which the treatment can be through physical exercises, some relaxation techniques. In other cases, specific treatment with antidepressants indicated by the specialist is necessary.…” Male HC, 41 years old
“… I think so, doing some sessions with psychologists or psychiatrists…” Female HC. 30 years
“Some people have chronic depression, which is difficult to treat but still treatable. It is talking to the person or meeting with a psychologist …” Female HC, 36 years old
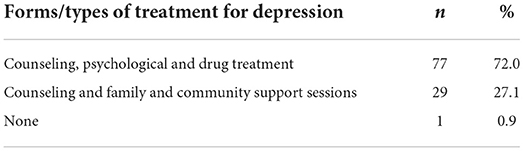
Table 9. Types of treatment for depression.
For the treatment of depression, participants suggested patients could seek psychological and psychiatric consultation with a doctor or trained counselor at health facilities (health center, hospital, pharmacy, clinic) or home, with family and/or friends. The participants said that at health facilities, treatment for depression could be found at the following services: Health Counseling and Testing, Psychosocial Support, and Young and Adolescent Friendly Services (Table 10).
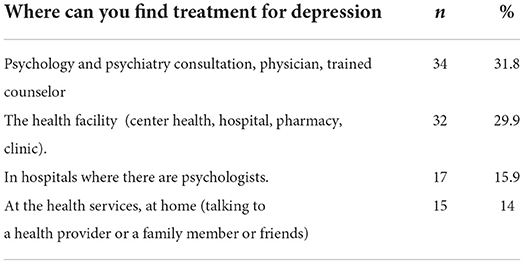
Table 10. Treatment setting.
Most participants 85.05% (n = 91) agreed that it was rewarding to spend time caring for depressed patients (question 15) and 87.85% (n = 94) disagreed that working with depressed patients is “heavy going” (question 13). Most lay HIV counselors 61.68% (n = 66) reported feeling comfortable dealing with depressed patients' needs (question 9). Participants suggested the strategies for helping patients presenting with depressive symptoms were: to refer to a psychologist, psychiatric technician, or specialist; conversation, welcoming, and counseling; and demonstrating empathy and actively listening to the patients' difficulties (Table 11).
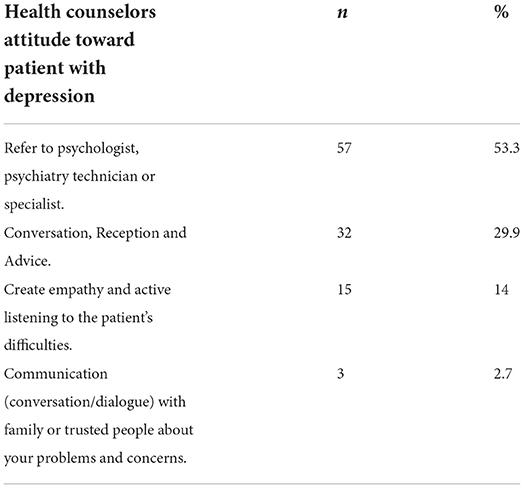
Table 11. Lay health counselors attitude toward depression.
This is, to our knowledge, the first study exploring knowledge and attitudes about mental health among lay HIV counselors in Mozambique. The key findings in our study are: first, the counselors demonstrated limited knowledge regarding the biological risk factors for depression (such as genetic and biochemical changes in the brain) and considerable knowledge about depression symptoms, psychosocial risk factors and management. Few had received specific or formal training in mental health and thus much of their knowledge about the presentation and management of depression was acquired through self-learning, books, or information from the media. Participants' conception of depression was based on their experiences in dealing with HIV positive patients in their daily routine, with considerable social and financial hardship. Most providers believed healthy lifestyles, family and community support, counseling, psychotherapy, medication treatment with mental health specialists could help to prevent and treat depression.
In contrast with other settings, non-mental health specialists and family practitioners in Saudi Arabia displayed high levels of knowledge and positive attitudes regarding depression and anxiety (50); this was attributed to their additional training in the management of mental disorders. When the R-DAQ was used among non-psychiatric physicians in Saudi Arabia, they showed optimism and confidence in managing depression, a positive attitude toward depression, but discriminatory and stigmatizing explanations for causes of depression–such as lack of willpower, poor stamina, part of the aging process (51). Furthermore, participation in any training related to mental health during the previous 5 years improved attitudes by 17% compared to other professionals (45). Moreover, despite their lack of mental health training, lay health counselors did not report religious or supernatural explanations for depression (such as witchcraft, evil spirits, divine punishment), which were reported by physicians not specialized in psychiatry in Pakistan (52) and by church volunteers in Nigeria (53). The participants demonstrated weak knowledge regarding the nature of depression. Only 52% disagreed that “depression reflects a characteristic response in patients which is not amenable to change” (DAQ 10) and 60% considered depression to be a way that “fragile people deal with life's difficulties” (DAQ 7). The former observation is similar to what was found in a study among general practitioners in Brazil (54). Similarly, consideration that depression is how fragile people deal with life's difficulties was also observed among nurses in Spain before receiving training on mental health (44). These findings suggest that more targeted training on depression is needed, with active components of stigma reduction to address negative stereotypes and false conceptions.
In our study, most participants had heard of depression, although most did not personally know people with depression. Most believed that depression was associated with HIV and AIDS. Providers also recognized the relationship between depression and other chronic conditions as contributing to low self-care with negative impact to patients' health (55). HIV and AIDS leads to depression through stigma and self-blame (56) or because of the challenge of accepting the diagnosis and the chronic demands involved in taking medications. Lack of income associated with unemployment and other difficulties associated with subsistence living, older age, distance to facility, stigma, and concerns about diagnostic disclosure and side-effects from ART (5, 57, 58) were also reported in our study as mental health stressors. Fear of disclosing one's HIV status to their partners can reduce the likelihood that people will adopt protective measures (such as condom use), which can increase the risk of transmission to others (59–62). Futhermore, HIV disclosure can have negative consequences such as stigma and discrimination, divorce and partner violence (63, 64) which are risk factors for depression (65). Disclosure of HIV serostatus has also been related to optimal adherence and freedom to use ART (58) as well as increased emotional and financial support (63, 66).
Our sample considered counseling, psychological and drug treatment and effective treatment strategies. The use of antidepressants was less frequently mentioned, which may be related to a false belief that treating depression with antidepressants may have a negative impact on HIV treatment adherence and outcomes (67). This is consistent with the fact that most counselors felt that psychologists and psychiatrists should manage depression, and that the HIV counselors lacked the skills to manage it. As seen in our study, active and empathic listening of patients' concerns, distress, and questions about treatment were seen as ways to improve engagement in treatment. Similar findings have been reported in studies conducted among other types of healthcare professionals, such as pharmacists (68).
The preventive measures and treatments reported by lay health counselors are in line with those recommended for populations outside of Mozambique, which include physical and recreational activity, social interactions, relaxation techniques, and seeking counseling either by professionals (licensed psychotherapists, psychiatrists, family medicine physicians, pharmacists) or by family members, friends, and acquaintances (69). This is consistent with the answers provided in the DAQ which suggested counselors believed that psychotherapy is more beneficial than antidepressants for the treatment of depression.
Training health providers to manage mental illness, mainly depression, is essential in resource-limited settings, and such training has been shown to improve knowledge and competence, as well as the delivery of effective mental health services (26, 45, 50). There was general agreement, not only among the lay health counselors but other non-mental health providers, that a psychiatrist or psychologist would better manage depression, not only because of the lack of integration of mental health services in primary care settings but also because of self-reported challenges in the identification of depressive symptoms by primary care providers (26, 45, 54, 70–72); there is ample evidence demonstrating that both lay health counselors and other non-mental health providers can be trained to effectively identify depression (73, 74). Mental health training may improve depression-related knowledge, attitudes, and practices in this group (45, 75). Our study suggests that training lay health counselors has the potential to improve their knowledge and attitudes toward depression in PWH and also care and outcomes as part of mental health in HIV services within primary healthcare setting.
The data for this study were collected in primary care health centers at the level of primary care located in Maputo city and Maputo province, so they may not be generalized to the rest of the country. The instrument for this study may be subject to information bias due to the poor mental health literacy of the participants. That said, one strength of our study–in light of the low internal consistency of the DAQ instrument–was the qualitative component. After each set of quantitative “agreement statements” by domain, we encouraged participants to use their own words to describe the same concepts. This extra step proved invaluable to us in order to be able to interpret some of the findings that were apparently in contrast. The small sample size for the quantitative survey limits the generalizability of its findings; however, having collected a small amount of qualitative data from such a large sample was a strength in this study. Other studies have also shown weak internal consistency of the DAQ in general and its subscales (45, 76). Since the qualitative interviews were conducted after administering the DAQ, the degree to which the answers may have been influenced by the survey questions is unclear. For this reason, it is reasonable to suggest adjustments that include additional items tailored to the professionals being assessed (71).
The DAQ is a tool primarily used to determine attitudes toward depression among medical doctors and other health professionals, but one of its limitations is low internal consistency (70). Studies provided insufficient information regarding psychometric properties and did not include internal consistency (45, 76). In the first Portuguese version study of the DAQ, the factorial analysis was omitted due to the small sample size for each item (54).
This study describes the knowledge and attitudes of lay HIV counselors regarding depression associated with their daily practice/routine, especially those already providing psychosocial support. Training lay counselors in mental health is associated with better knowledge, attitudes, and practices in LMICs (75). Additional research will be needed to understand sustainable ways of incorporating evidence-based interventions and community-based participatory methods in order to reduce mental health disparities (73). Training and supervising lay health workers to deliver effective counseling interventions (39) can address depression among PWH in LMIC. Since lay counselors are the first point of contact for PWH in primary care, and given the shortage of mental health professionals, the training of HIV counselors in the identification and management of depression could enhance access to and improvements in care. Depression among PWH is associated with poor social connections, lower help-seeking, and adverse health behaviors (77). Health counselors have the potential to improve patient care in HIV clinics. By improving their competency to screen for and manage depression, they can potentially mitigate the negative impact of depression on adherence to ART and, hopefully, improve the prognosis of HIV infection.
Understanding medical practitioners' attitudes can guide and assess the needs for training at the primary healthcare level. This is also true for lay HIV counselors, who organize service delivery specifically for PWH and manage treatment outcomes (54, 78). Of note, most of our participants accurately linked the conditions of depression and HIV/AIDS.
Basic brief training positively impacts non-mental health professionals' knowledge and attitudes toward depression and impacts patients' education and care, especially for those with chronic disease and/or involved in long-term treatment (79, 80). Investing in the training of lay health counselors can significantly impact patient care for PWH and people with other chronic illnesses where depressive symptoms may affect patients' quality of life, adherence, and prognosis.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committees (from Federal University of São Paulo in Brazil and Eduardo Mondlane University in Mozambique). The patients/participants provided their written informed consent to participate in this study.
FM, MG, LP, and AS drafted the manuscript. MG did statistical analysis. AS did qualitative analysis. MG, CD, FC, MS, ES, DK, MO, and MW reviewed the manuscript. FM and MM designed the protocol. All authors agreed to the final version of the manuscript.
This study was supported by NIMH grants U19MH113203 and T32MH096724; and Fogarty International Center grant D43TW009675.
We thank the Maputo City Municipality and Health Department, Maputo Province Health Department, Matola, Manhiça and Marracuene District Health Directorate, and research assistants for facilitating data collection and all study participants for their contribution to this work.
Author MO receives royalties from the Research Foundation for Mental Hygiene for the Columbia Suicide Severity Rating Scale's commercial use and owns shares in Mantra, Inc. She serves as an advisor to Alkermes and Fundacion Jimenez Diaz (Madrid). Her family owns stock in Bristol Myers Squibb.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AIDS, Acquired Immunodeficiency Syndrome; ART, Antiretroviral Treatment; ARV, Antiretroviral; ART, Highly Active Antiretroviral Therapy; DAQ, Depression Attitude Questionnaire; HIV/AIDS, Human Immunodeficiency Virus/ Acquired Immunodeficiency Syndrome; IL, Interleukin (IL-1IL-6); IFNγ, Interferon gama; LMIC, Low and Middle Income Country; PWH, People Living With Human Immunodeficiency Virus/ Acquired Immunodeficiency Syndrome; PHQ-9, Patient Health Questionnaire 9; TB, Tuberculosis; TNFα, Tumor Necrosis Factor alfa.
1. UNAIDS – Global HIV and AIDS Statistics – 2020 Fact Sheet. Available online at: https://www.unaids.org/en/resources/fact-sheet (accessed September 27, 2021).
2. UNAIDS Data (2020). Available online at: https://www.unaids.org/sites/default/files/media_asset/2020_aids-data-book_en.pdf (accessed September 27, 2021).
3. Ministério da Saúde (Misau), Serviço Nacional de Saude, (SNS), Relatório Anual 2019- Relatório Anual de Actividade Relacionadas ao, HIV/SIDA, Março de (2020),. https://www.misau.gov.mz/index.php/relatorios-anuais?download=989:relatorio-anual-hiv-2020-final (accessed September 27, 2021).
4. Lofgren SM, Bond DJ, Nakasujja N, Boulware DR. Burden of depression in outpatient HIV-infected adults in sub-Saharan Africa; systematic review and meta-analysis. AIDS Behav. (2020) 24:1752–64. doi: 10.1007/s10461-019-02706-2
5. Mwangala PN, Mabrouk A, Wagner R, Newton CRJC, Abubakar AA. Mental health and well-being of older adults living with HIV in sub-Saharan Africa: a systematic review. BMJ Open. (2021) 11:e052810. doi: 10.1136/bmjopen-2021-052810
6. van Coppenhagen B, Duvenage HS. Prevalence of depression in people living with HIV and AIDS at the Kalafong provincial tertiary hospital antiretroviral clinic. S Afr J Psychiatr. (2019) 25:1175. doi: 10.4102/sajpsychiatry.v25i0.1175
7. Nanni MG, Caruso R, Mitchell AJ, Meggiolaro E, Grassi L. Depression in HIV infected patients: a review. Curr Psychiatry Rep. (2015) 17:530. doi: 10.1007/s11920-014-0530-4
8. Ickovics JR, Hamburger ME, Vlahov D, Schoenbaum EE, Schuman P, Boland RJ, et al. Mortality, CD4 cell count decline, and depressive symptoms among HIV-seropositive women: longitudinal analysis from the HIV epidemiology research study. JAMA. (2001) 285:1466–74. doi: 10.1001/jama.285.11.1466
9. Machado MO, Veronese N, Sanches M, Stubbs B, Koyanagi A, Thompson T, et al. The association of depression and all-cause and cause-specific mortality: an umbrella review of systematic reviews and meta-analyses. BMC Med. (2018) 16:112. doi: 10.1186/s12916-018-1101-z
10. Gilman SE, Sucha E, Kingsbury M, Horton NJ, Murphy JM, Colman I. Depression and mortality in a longitudinal study: 1952-2011. CMAJ. (2017) 189:E1304–10. doi: 10.1503/cmaj.170125
11. Benton TD, Kee Ng WY, Leung D, Canetti A, Karnik N. Depression among youth living with HIV/AIDS. Child Adolesc Psychiatr Clin N Am. (2019) 28:447–59. doi: 10.1016/j.chc.2019.02.014
12. Mitchell AJ, Vaze A, Rao S. Clinical diagnosis of depression in primary care: a meta-analysis. Lancet. (2009) 374:609–19. doi: 10.1016/S0140-6736(09)60879-5
13. Samples H, Stuart EA, Saloner B, Barry CL, Mojtabai R. The role of screening in depression diagnosis and treatment in a representative sample of US primary care visits. J Gen Intern Med. (2020) 35:12–20. doi: 10.1007/s11606-019-05192-3
14. Dewing S, Mathews C, Schaay N, Cloete A, Simbayi L, Louw J. Improving the counselling skills of lay counsellors in antiretroviral adherence settings: a cluster randomised controlled trial in the Western Cape, South Africa. AIDS Behav. (2015) 19:157–65. doi: 10.1007/s10461-014-0781-4
15. Sanjana P, Torpey K, Schwarzwalder A, Simumba C, Kasonde P, et al. Task-shifting HIV counselling and testing services in Zambia: the role of lay counsellors. Hum Resour Health. (2009) 7:44. doi: 10.1186/1478-4491-7-44
16. Zimba CC, Akiba CF, Matewere M, Thom A, Udedi M, Masiye JK, et al. Facilitators, barriers and potential solutions to the integration of depression and non-communicable diseases (NCDs) care in Malawi: a qualitative study with service providers. Int J Ment Health Syst. (2021) 15:59. doi: 10.1186/s13033-021-00480-0
17. Kagee A. Training lay counsellors in public health: Considerations for social workers, professional counsellors and psychologists. Glob Public Health. (2020) 15:918–24. doi: 10.1080/17441692.2020.1730931
18. Munetsi E, Simms V, Dzapasi L, Chapoterera G, Goba N, Gumunyu T, et al. Trained lay health workers reduce common mental disorder symptoms of adults with suicidal ideation in Zimbabwe: a cohort study. BMC Public Health. (2018) 18:227. doi: 10.1186/s12889-018-5117-2
19. Connolly SM, Vanchu-Orosco M, Warner J, Seidi PA, Edwards J, Boath E, et al. Mental health interventions by lay counsellors: a systematic review and meta-analysis. Bull World Health Organ. (2021) 99:572–82. doi: 10.2471/BLT.20.269050
20. Patel V, Weobong B, Weiss HA, Anand A, Bhat B, Katti B, et al. The Healthy Activity Program (HAP), a lay counsellor-delivered brief psychological treatment for severe depression, in primary care in India: a randomised controlled trial. Lancet. (2017) 389:176–85. doi: 10.1016/S0140-6736(16)31589-6
21. Hoeft TJ, Fortney JC, Patel V, Unützer J. Task-sharing approaches to improve mental health care in rural and other low-resource settings: a systematic review. J Rural Health. (2018) 34:48–62. doi: 10.1111/jrh.12229
22. Sweetland AC, Belkin GS, Verdeli H. Measuring depression and anxiety in sub-Saharan Africa. Depress Anxiety. (2014) 31:223–32. doi: 10.1002/da.22142
23. Stockton MA, Minnick CE, Kulisewa K, Mphonda SM, Hosseinipour MC, Gaynes BN, et al. A mixed-methods process evaluation: integrating depression treatment into HIV care in Malawi. Glob Health Sci Pract. (2021) 9:611–25. doi: 10.9745/GHSP-D-20-00607
24. Udedi M, Stockton MA, Kulisewa K, Hosseinipour MC, Gaynes BN, Mphonda SM, et al. Integrating depression management into HIV primary care in central Malawi: the implementation of a pilot capacity building program. BMC Health Serv Res. (2018) 18:593. doi: 10.1186/s12913-018-3388-z
25. Synowski J, Weiss HA, Velleman R, Patel V, Nadkarni A. A lay-counsellor delivered brief psychological treatment for men with comorbid alcohol use disorder and depression in primary care: secondary analysis of data from a randomized controlled trial. Drug Alcohol Depend. (2021) 227:108961. doi: 10.1016/j.drugalcdep.2021.108961
26. Mulango ID, Atashili J, Gaynes BN, Njim T. Knowledge, attitudes and practices regarding depression among primary health care providers in Fako division, Cameroon. BMC Psychiatry. (2018) 18:66. doi: 10.1186/s12888-018-1653-7
27. Bemelmans M, Baert S, Negussie E, Bygrave H, Biot M, Jamet C, et al. Sustaining the future of HIV counselling to reach 90-90-90: a regional country analysis. J Int AIDS Soc. (2016) 19:20751. doi: 10.7448/IAS.19.1.20751
28. Chibanda D, Mesu P, Kajawu L, Cowan F, Araya R, Abas MA. Problem-solving therapy for depression and common mental disorders in Zimbabwe: piloting a task-shifting primary mental health care intervention in a population with a high prevalence of people living with HIV. BMC Public Health. (2011) 11:828. doi: 10.1186/1471-2458-11-828
29. Petersen I, Hanass Hancock J, Bhana A, Govender K. A group-based counselling intervention for depression comorbid with HIV/AIDS using a task shifting approach in South Africa: a randomized controlled pilot study. J Affect Disord. (2014) 158:78–84. doi: 10.1016/j.jad.2014.02.013
30. Chibanda D, Weiss HA, Verhey R, Simms V, Munjoma R, Rusakaniko S, et al. Effect of a primary care-based psychological intervention on symptoms of common mental disorders in Zimbabwe: a randomized clinical trial. JAMA. (2016) 316:2618–26. doi: 10.1001/jama.2016.19102
31. Nyamayaro P, Bere T, Magidson JF, Simms V, O'Cleirigh C, Chibanda D, et al. A task-shifting problem-solving therapy intervention for depression and barriers to antiretroviral therapy adherence for people living with HIV in Zimbabwe: case series. Cogn Behav Pract. (2020) 27:84–92. doi: 10.1016/j.cbpra.2018.10.003
32. Stockton MA, Udedi M, Kulisewa K, Hosseinipour MC, Gaynes BN, Mphonda SM, et al. The impact of an integrated depression and HIV treatment program on mental health and HIV care outcomes among people newly initiating antiretroviral therapy in Malawi. PLoS ONE. (2020) 15:e0231872. doi: 10.1371/journal.pone.0231872
33. Joska JA, Sorsdahl KR. Integrating mental health into general health care: lessons from HIV. Afr J Psychiatry. (2012) 15:420–3. doi: 10.4314/ajpsy.v15i6.52
34. Jack H, Wagner RG, Petersen I, Thom R, Newton CR, Stein A, et al. Closing the mental health treatment gap in South Africa: a review of costs and cost-effectiveness. Glob Health Action. (2014) 7:23431. doi: 10.3402/gha.v7.23431
35. Duffy M, Sharer M, Cornman H, Pearson J, Pitorak H, Fullem A. Integrating mental health and hiv services in Zimbabwean communities: a nurse and community-led approach to reach the most vulnerable. J Assoc Nurses AIDS Care. (2017) 28:186–98. doi: 10.1016/j.jana.2015.09.003
36. Mwisongo A, Mehlomakhulu V, Mohlabane N, Peltzer K, Mthembu J, Van Rooyen H. Evaluation of the HIV lay counselling and testing profession in South Africa. BMC Health Serv Res. (2015) 15:278. doi: 10.1186/s12913-015-0940-y
37. Ministerio da Saude (Misau), Programa Nacional de Combate a ITS-, HIV/SIDA, Avaliação do Plano de Aceleração da Resposta ao HIV e SIDA em, Moçambique, 2013-2017- Relatorio, Final, Junho (2020). Available online at: https://www.misau.gov.mz/index.php/planos-estrategicos-do-hiv (accessed September 28, 2021).
38. Ministério da Saúde (Misau) Direcção Nacional de Assistência Médica (DNAM) Directriz Nacional de Apoio Psicossocial e Prevenção Positva (APSS and PP) (2015). Available online at: https://www.misau.gov.mz/index.php/hiv-sida-directrizes-nacionais?download=947:directriz-nacional-de-apoio-psicossocial-nos-cuidados-e-tratamento-do-hiv (accessed September 28, 2021).
39. Petersen I, Fairall L, Egbe CO, Bhana A. Optimizing lay counsellor services for chronic care in South Africa: a qualitative systematic review. Patient Educ Couns. (2014) 95:201–10. doi: 10.1016/j.pec.2014.02.001
40. Cele WB, Mhlongo EM. Knowledge of health practitioners regarding mental health integration into human immunodeficiency virus management into primary healthcare level. Curationis. (2020) 43:e1–8. doi: 10.4102/curationis.v43i1.2041
41. Booth A, Scantlebury A, Hughes-Morley A, Mitchell N, Wright K, Scott W, et al. Mental health training programmes for non-mental health trained professionals coming into contact with people with mental ill health: a systematic review of effectiveness. BMC Psychiatry. (2017) 17:196. doi: 10.1186/s12888-017-1356-5
42. Kemp CG, Mntambo N, Weiner BJ, Grant M, Rao D, Bhana A, et al. Pushing the bench: a mixed methods study of barriers to and facilitators of identification and referral into depression care by professional nurses in KwaZulu-Natal, South Africa. SSM Ment Health. (2021) 1:100009. doi: 10.1016/j.ssmmh.2021.100009
43. Botega N, Mann A, Blizard R, Wilkinson G. General practitioners and depression—first use of the depression attitude questionnaire. Int J Methods Psychiatr Res. (1992) 4, 169–80. doi: 10.1037/t08271-000
44. López-Cortacans G, Aragonès Benaiges E, Caballero Alías A, Piñol Moreso JL. Efecto de una intervención formativa en las actitudes de las enfermeras de atención primaria ante la depresión [Effect of an educational intervention on the attitudes of the nurses of primary care on depression]. Enferm Clin. (2015) 25:254–61. doi: 10.1016/j.enfcli.2015.03.007
45. Haddad M, Walters P, Tylee A. District nursing staff and depression: a psychometric evaluation of depression attitude questionnaire findings. Int J Nurs Stud. (2007) 44:447–56. doi: 10.1016/j.ijnurstu.2006.07.005
46. Palinkas LA, Aarons GA, Horwitz S, Chamberlain P, Hurlburt M, Landsverk J. Mixed method designs in implementation research. Adm Policy Ment Health. (2011) 38:44–53. doi: 10.1007/s10488-010-0314-z
47. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. (2005) 15:1277–88. doi: 10.1177/1049732305276687
48. Bernard HR. Qualitative data, quantitative analysis. CAM J. (1996) 8:9–11. doi: 10.1177/1525822X960080010401
49. Green EC. Can qualitative research produce reliable quantitative findings? Field Methods. (2001) 13:3–19.
50. Al-Atram AA. Physicians' knowledge and attitude towards mental health in Saudi Arabia. Ethiop J Health Sci. (2018) 28:771–8. doi: 10.4314/ejhs.v28i6.12
51. Aldahmashi T, Almanea A, Alsaad A, Mohamud M, Anjum I. Attitudes towards depression among non-psychiatric physicians in four tertiary centres in Riyadh. Health Psychol Open. (2019) 6:2055102918820640. doi: 10.1177/2055102918820640
52. Haddad M, Waqas A, Qayyum W, Shams M, Malik S. The attitudes and beliefs of Pakistani medical practitioners about depression: a cross-sectional study in Lahore using the revised depression attitude questionnaire (R-DAQ). BMC Psychiatry. (2016) 16:349. doi: 10.1186/s12888-016-1069-1
53. Iheanacho T, Kapadia D, Ezeanolue CO, Osuji AA, Ogidi AG, Ike A, et al. Attitudes and beliefs about mental illness among church-based lay health workers: experience from a prevention of mother-to-child HIV transmission trial in Nigeria. Int J Cult Ment Health. (2016) 9:1–13. doi: 10.1080/17542863.2015.1074260
54. Botega NJ, Silveira GM. General practitioners attitudes towards depression: a study in primary care setting in Brazil. Int J Soc Psychiatry. (1996) 42:230–7. doi: 10.1177/002076409604200307
55. Held RF, DePue J, Rosen R, Bereolos N, Nu'usolia O, Tuitele J, et al. Patient and health care provider views of depressive symptoms and diabetes in American Samoa. Cultur Divers Ethnic Minor Psychol. (2010) 16:461–7. doi: 10.1037/a0020089
56. Chan BT, Pradeep A, Mayer KH, Kumarasamy N. Attitudes of Indian HIV clinicians toward depression in people living with HIV. Ann Glob Health. (2016) 82:792–7. doi: 10.1016/j.aogh.2016.04.672
57. Bernard C, Font H, Diallo Z, Ahonon R, Tine JM, Abouo F, et al. Prevalence and factors associated with physical function limitation in older West African people living with HIV. PLoS ONE. (2020) 15:e0240906. doi: 10.1371/journal.pone.0240906
58. Dibaba D, Kajela G, Chego M, Ermeko T, Zenbaba D, Hailu S, et al. Antiretroviral treatment adherence level and associated factors among adult HIV-positive patients on both HIV/AIDS care models: comparative study in selected hospitals of Western Ethiopia, 2019. HIV AIDS. (2021) 13:1067–78. doi: 10.2147/HIV.S327784
59. Ismail N, Matillya N, Ratansi R, Mbekenga C. Barriers to timely disclosure of HIV serostatus: a qualitative study at care and treatment centers in Dar es Salaam, Tanzania. PLoS ONE. (2021) 16:1–14. doi: 10.1371/journal.pone.0256537
60. Simbayi LC, Kalichman SC, Strebel A, Cloete A, Henda N, Mqeketo A. Disclosure of HIV status to sex partners and sexual risk behaviours among HIV-positive men and women, Cape Town, South Africa. Sex Transm Infect. (2007) 83:29–34. doi: 10.1136/sti.2006.019893
61. Cook CL, Staras SAS, Zhou Z, Chichetto N, Cook RL. Disclosure of HIV serostatus and condomless sex among men living with HIV/AIDS in Florida. PLoS ONE. (2018) 13:1–11. doi: 10.1371/journal.pone.0207838
62. Kalichman SC, Kalichman MO, Cherry C, Grebler T, HIV. Disclosure and transmission risks to sex partners among HIV-positive men. AIDS Patient Care STDS. (2016) 30:221–8. doi: 10.1089/apc.2015.0333
63. Yonah G, Fredrick F, Leyna G. HIV serostatus disclosure among people living with HIV/AIDS in Mwanza, Tanzania. AIDS Res Ther. (2014) 11:1–5. doi: 10.1186/1742-6405-11-5
64. Colombini M, James C, Ndwiga C, Team I, Mayhew SH. The risks of partner violence following HIV status disclosure, and health service responses: narratives of women attending reproductive health services in Kenya. J Int AIDS Soc. (2016) 19:1–7. doi: 10.7448/IAS.19.1.20766
65. Mitzel LD, Vanable PA, Carey MP, Hospital TM, Island R. HIV-related stigmatization and medication adherence: indirect effects of disclosure concerns and depression. Stigma Health. (2019) 4:282–92. doi: 10.1037/sah0000144
66. Shacham E, Small E, Onen N, Stamm K, Overton ET. Serostatus disclosure among adults with HIV in the era of HIV therapy. AIDS Patient Care STDS. (2012) 26:29–35. doi: 10.1089/apc.2011.0183
67. Chakraborty K, Avasthi A, Kumar S, Grover S. Attitudes and beliefs of patients of first episode depression towards antidepressants and their adherence to treatment. Soc Psychiatry Psychiatr Epidemiol. (2009) 44:482–8. doi: 10.1007/s00127-008-0468-0
68. Scheerder G, De Coster I, Van Audenhove C. Community pharmacists' attitude toward depression: a pilot study. Res Social Adm Pharm. (2009) 5:242–52. doi: 10.1016/j.sapharm.2008.08.008
69. Jorm AF, Medway J, Christensen H, Korten AE, Jacomb PA, Rodgers B. Attitudes towards people with depression: effects on the public's help-seeking and outcome when experiencing common psychiatric symptoms. Aust N Z J Psychiatry. (2000) 34:612–8. doi: 10.1080/j.1440-1614.2000.00743.x
70. Aragonès E, Piñol JL, López-Cortacans G, Hernández JM, Caballero A. Actitudes y opiniones de los médicos de familia frente a la depresión: una aproximación con el depression attitudes questionnaire (DAQ) [attitudes and opinions of family doctors on depression: application of the depression attitudes questionnaire (DAQ)]. Aten Primaria. (2011) 43:312–8. doi: 10.1016/j.aprim.2010.05.009
71. Haddad M, Menchetti M, Walters P, Norton J, Tylee A, Mann A. Clinicians' attitudes to depression in Europe: a pooled analysis of depression attitude questionnaire findings. Fam Pract. (2012) 29:121–30. doi: 10.1093/fampra/cmr070
72. Ohtsuki T, Kodaka M, Sakai R, Ishikura F, Watanabe Y, Mann A, et al. Attitudes toward depression among Japanese non-psychiatric medical doctors: a cross-sectional study. BMC Res Notes. (2012) 5:44. doi: 10.1186/1756-0500-5-441
73. Barnett ML, Gonzalez A, Miranda J, Chavira DA, Lau AS. Mobilizing community health workers to address mental health disparities for underserved populations: a systematic review. Adm Policy Ment Health. (2018) 45:195–211. doi: 10.1007/s10488-017-0815-0
74. Han HR, Kim K, Murphy J, Cudjoe J, Wilson P, Sharps P, et al. Community health worker interventions to promote psychosocial outcomes among people living with HIV—a systematic review. PLoS ONE. (2018) 13:e0194928. doi: 10.1371/journal.pone.0194928
75. Andrews L. Non-specialist health worker interventions for the care of mental, neurological, and substance-abuse disorders in low- and middle-income countries. Issues Ment Health Nurs. (2016) 37:131–2. doi: 10.3109/01612840.2015.1128299
76. Norton JL, Pommié C, Cogneau J, Haddad M, Ritchie KA, Mann AH. Beliefs and attitudes of French family practitioners toward depression: the impact of training in mental health. Int J Psychiatry Med. (2011) 41:107–22. doi: 10.2190/PM.41.2.a
77. Perazzo JD, Currie J, Horvat Davey C, Lambert J, Webel AR. Depression and social capital in people living with HIV. J Psychiatr Ment Health Nurs. (2020) 27:54–61. doi: 10.1111/jpm.12552
78. Dowrick C, Gask L, Perry R, Dixon C, Usherwood T. Do general practitioners' attitudes towards depression predict their clinical behaviour? Psychol Med. (2000) 30:413–9. doi: 10.1017/S0033291799001531
79. Butler MP, Quayle E. Training primary care nurses in late-life depression: knowledge, attitude and practice changes. Int J Older People Nurs. (2007) 2:25–35. doi: 10.1111/j.1748-3743.2007.00054.x
Keywords: depression, knowledge, attitude, lay health counselors, HIV/AIDS
Citation: Mandlate F, Greene MC, Pereira LF, Sweetland AC, Kokonya D, Duarte CS, Cournos F, Oquendo MA, Wainberg ML, Sidat M, Sevene E and Mello MF (2022) Lay HIV counselors' knowledge and attitudes toward depression: A mixed-methods cross-sectional study at primary healthcare centers in Mozambique. Front. Public Health 10:919827. doi: 10.3389/fpubh.2022.919827
Received: 14 April 2022; Accepted: 31 August 2022;
Published: 28 September 2022.
Edited by:
Aliya Naheed, International Centre for Diarrhoeal Disease Research, BangladeshReviewed by:
Sayward Elizabeth Harrison, University of South Carolina, United StatesCopyright © 2022 Mandlate, Greene, Pereira, Sweetland, Kokonya, Duarte, Cournos, Oquendo, Wainberg, Sidat, Sevene and Mello. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Flavio Mandlate, Zm1hY2hhZG8xNEBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.