
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health, 10 August 2022
Sec. Public Mental Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.919818
This article is part of the Research TopicNoncommunicable Diseases and Mental Health Experiences Before and After the COVID-19 PandemicView all 14 articles
 Diana C. Oviedo1,2,3*†
Diana C. Oviedo1,2,3*† María Sofía Pinzón2†
María Sofía Pinzón2† Sofía Rodríguez-Araña1
Sofía Rodríguez-Araña1 Adam E. Tratner4
Adam E. Tratner4 Elianne Pauli-Quirós2
Elianne Pauli-Quirós2 Carlos Chavarría2
Carlos Chavarría2 Camilo Posada Rodríguez1
Camilo Posada Rodríguez1 Gabrielle B. Britton1,3
Gabrielle B. Britton1,3Background: The impact of the COVID-19 pandemic and the associated restrictions on mental health is being studied.
Objective: To analyze the psychosocial response to the COVID-19 pandemic in adults residing in Panama.
Methods: A community sample of 480 adult residents of Panama completed a survey that included sociodemographic questions, COVID-19 related questions (e.g., health concerns regarding the virus, knowledge and behaviors in biosafety) and scales of stress, anxiety, depression, prosocial behavior, resilience, perceived social support, and insomnia.
Results: Most of the participants (>60%) reported being negatively affected by the pandemic. Women experienced greater depression, anxiety, and stress symptoms than men, and age was negatively associated with depression, anxiety, and stress symptoms. Self-perceived health status and self-perceived social support were negatively associated with depression, anxiety, and stress symptoms. Self-perceived social isolation was positively associated with depression, anxiety, and stress symptoms. Psychiatric illness and insomnia were positively associated with depression, anxiety, and stress symptoms, whereas psychological resilience was negatively associated with depression, anxiety, and stress symptoms.
Discussion: These results corroborate other studies regarding COVID-19 and mental health. This study highlights the need for specific prevention and intervention mechanisms related to the COVID-19 pandemic in different population groups. This is the first report of the psychological impact of COVID-19 in the general Panamanian population and one of the only studies in the Latin American region and, therefore, contributes to research in the Latino population and lower-middle income countries.
By early 2020, the SARS-CoV-2 coronavirus disease 2019 (COVID-19) had spread rapidly throughout the world and was officially declared a pandemic in March 2020. To prevent the propagation of the virus, many countries adopted different mitigation strategies such as quarantines, rigorous lockdowns, mobility restrictions, closure of schools and the isolation of vulnerable populations (1). Research on previous epidemics, such as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS), documented that these measures are associated with an increase in mental health-related distress (2, 3). Studies have reported high-stress levels, sleep disturbances such as insomnia and nightmares, an increase in depressive and anxiety symptoms, and poor concentration, among others (4).
Moreover, research on the effects of COVID-19 lockdowns has documented high anxiety, depression, and stress levels, as well as post-traumatic stress disorder symptoms, irritability, isolation, fear, uncertainty, anger, loneliness, and guilt in people who experienced ongoing restrictions (5–7). These psychological manifestations are associated with personal, social, behavioral and cognitive variables that, taken together, encompass psychosocial determinants of how people respond to menacing situations (8). These social determinants of the pandemic have impacted individual emotional distress (9). Research has shown that the social determinants related to worse psychological responses to the pandemic include being female, age, previous mental health diagnosis, lower income, racial and ethnic disparities, poor subjective and objective health status, and being a healthcare worker (10–13). Furthermore, the rise in psychological and psychiatric symptoms is also a result of COVID-19 related deaths and illnesses as well as social unrest and economic crises (14, 15).
Most research investigating mental health during the pandemic has focused on high-income countries, and there is limited empirical research on COVID-19's psychosocial effects on low and middle-income countries (LMIC), specifically in Latin America (16). For instance, in Panama, the only reported study regarding mental health in healthcare workers, has evidenced a high prevalence of mental health disorders in this population group (17). Panama had one of the strictest lockdown measures in the world (18), which lasted until late 2021 (19). The country implemented various restrictive mechanisms to mitigate and control the spread of the pandemic: mobility and travel restrictions according to ID number and sex, suspension of in-person educational activities and social activities, border closures, sanitary and epidemiological control, staff rotation and teleworking modality (20).
Furthermore, in Panama as well as in other LMIC, the COVID-19 pandemic exposed economic, social, health and educational inequalities that affected the most disadvantaged and vulnerable individuals (21). While many affluent countries have experienced severe health crises, low and middle-income countries have undergone more pronounced economic crises that are projected to continue (22). In developing countries, it is estimated that 255 million full-time jobs have been lost (23). Additionally, the informal sector has been severely impacted by the pandemic. Around 67% of people with informal jobs live in developing countries, and most have been affected by lockdown measures, affecting economic stability (22). Moreover, in developing countries there is a high prevalence of comorbidities, coupled with limited access to health services, particularly mental health resources (24, 25). All these factors increase the toll on the mental health of residents in developing countries. Therefore, this study aims to explore the psychosocial determinants associated with the pandemic in the Panamanian population. The objective of this study was to analyze the psychosocial response to the COVID-19 pandemic in adults residing in Panama.
This was a descriptive, quantitative, cross-sectional study. Participants were 480 adult residents of Panama (80.8% women), aged 18 years or older (M = 32.7; SD = 14.6, Range = 18–66). Participants were recruited using convenience sampling. Sample size was calculated using Raosoft Sample Size Calculator. Considering 2,958,577 as the population of people 18 years and older in Panama (26), prevalence of psychosocial effects of the pandemic at 30% (average reported psychosocial effects of pandemic in previous studies), at 95% confidence levels and 5% error margin, the estimated minimum sample size was 323. The research team used advertisements on social media platforms (e.g., Instagram, Facebook, Twitter), which included a description of the study and the principal investigator's contact information. Those who voluntarily contacted the principal investigator were provided access to an online survey via a Google Forms link if they met the inclusion criteria of being an adult over 18 years old resident of Panama, having access to a technological device such as a laptop, cellphone or tablet, and not having a physical condition that would make it difficult or preclude accessing the link or answering questions (e.g., visual impairment, cognitive impairment, illiteracy). Recruitment and data collection took place from March 26, 2021 to May 11, 2021. This study was approved by the National Research Bioethics Committee of Panama (CNBI). Participants provided informed consent in compliance with the Declaration of Helsinki principles (1964). The online survey consisted of sociodemographic questions regarding sex, age, marital status, the number of cohabitants living in the same household, employment status, and monthly income. Participants also indicated how many chronic illnesses (e.g., diabetes, hypertension) and psychiatric disorders (e.g., depression, anxiety) they had been diagnosed with, as well as their self-perceived health status (0 = Very bad, 2 = Average, 4 = Very good). In addition, questions assessed biosafety knowledge and behaviors, as well as attitudes and health concerns pertaining to COVID-19. Lastly, several scales that measure psychological symptoms and manifestations linked to COVID-19 pandemic outcomes were included.
The Depression, Anxiety and Stress Scale-21 (DASS-21) (27) was used to report symptoms of depression, anxiety, and stress. The Athens Scale of Insomnia (ASI) (28, 29) was included to indicate if participants experienced sleep difficulties at least 3 times in the past month and the severity of their symptoms. Participants also completed a self-report measure of prosocial behavior (Prosociality Scale) (30). Additionally, participants reported perceived psychological resilience during the past month using the Connor-Davidson Resilience Scale (CD-RISC) (31). Finally, the Multidimensional Scale of Perceived Social Support (MSPSS) (32) was included to assess the perceived quality of social support from family, friends, and relationship partners.
Statistical analyses were conducted using IBM SPSS Statistics version 27.0. Descriptive statistics were used to summarize the demographic characteristics of the sample. Means and standard deviations were calculated for quantitative variables, and categorical variables were presented as frequencies and percentages. Univariate analyses were used to compare groups and examine relationships between variables of interest. Specifically, we used analysis of variance to investigate sex and age cohort differences, and hierarchical linear regression to examine the unique contribution of demographic, economic, health, social psychological, and psychiatric factors on psychological distress symptoms. Results for which p < 0.05 were accepted as significant.
Table 1 summarizes the sample's sociodemographic characteristics. The majority of participants were Panamanian nationals (88.5%), single (79.4%), educated (76.1% completed a bachelor's degree or higher), female (80.8%), and cohabitated with one or more people (94.4%). More than one-third (37.3%) of participants were unemployed at the time of the survey, and less than half of the sample (46.3%) earned a monthly income higher than $2,000.
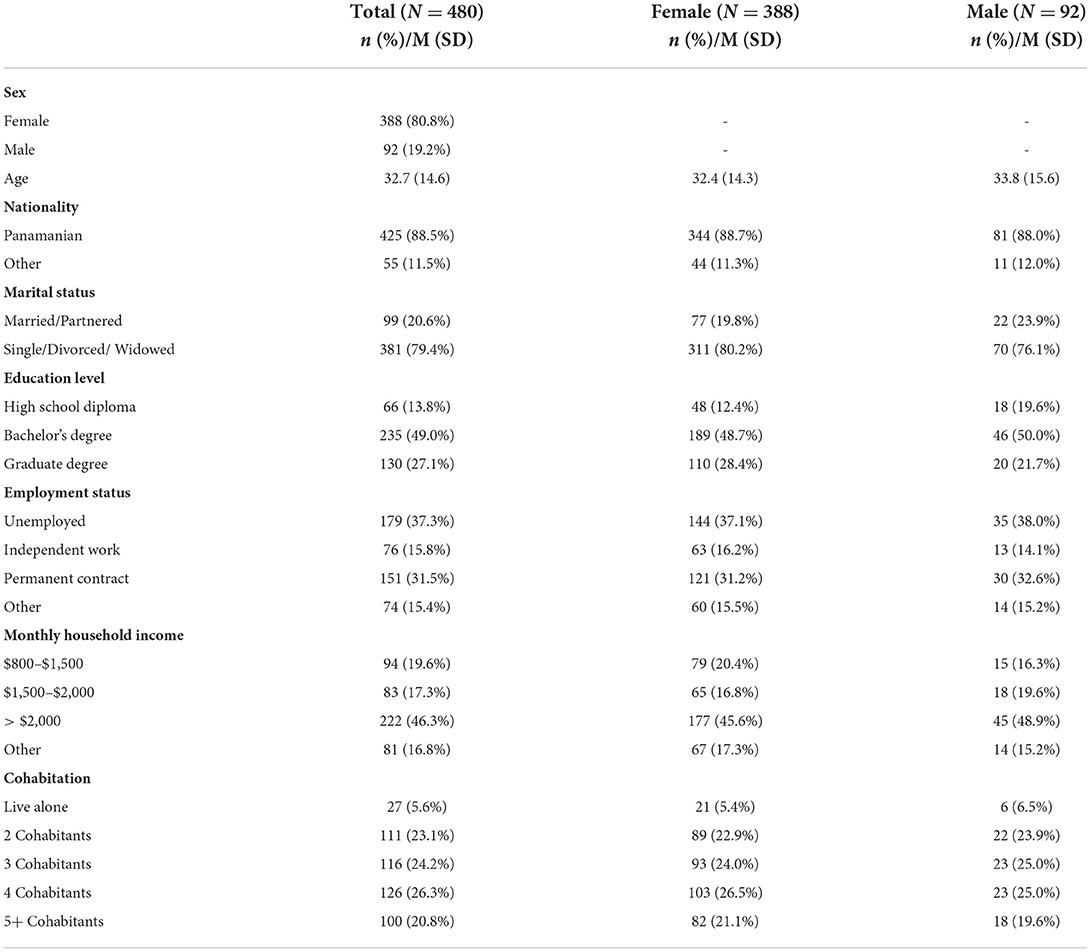
Table 1. Sociodemographic characteristics.
Table 2 shows the perception of risk and health factors. Most participants (79.2%) reported their overall health as “Good” or “Very good,” whereas 26.9% reported having one or more chronic illnesses (e.g., diabetes, hypertension, obesity). Additionally, 21% of participants reported having a psychiatric diagnosis (e.g., depression, anxiety, agoraphobia), and nearly one-third of the sample (32.1%) reported taking at least one prescribed medication. In addition, most participants did not report an increase in cigarette (14.6%) or alcohol (22.1%) consumption. However, most participants (78.3%) reported changes in their amount of physical activity.
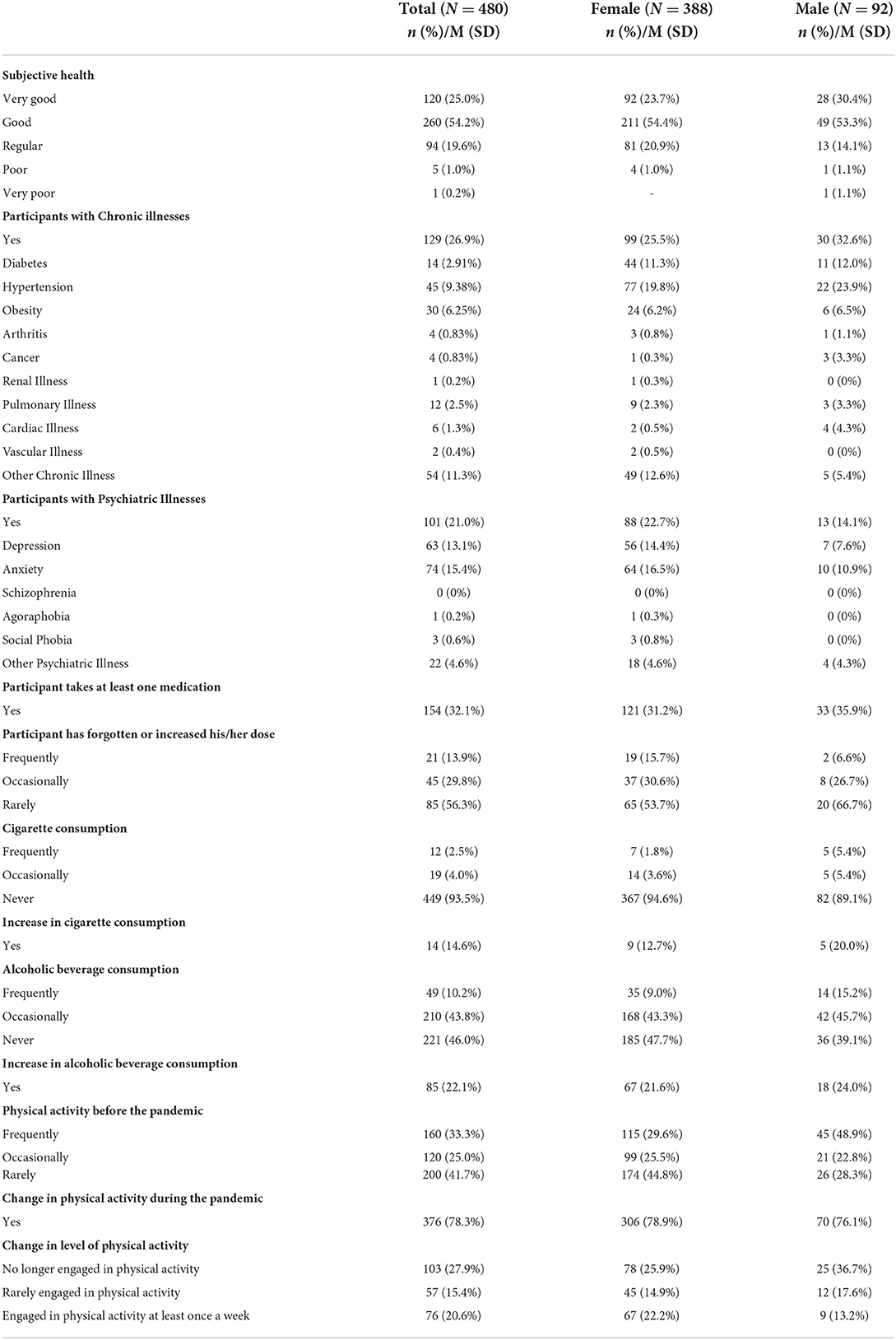
Table 2. Subjective health and risk factors.
Many participants reported disturbances to their psychosocial well-being during the pandemic. For instance, 35% of participants reported mild to moderate levels of depression, 25% reported mild to moderate anxiety symptoms, and 51% reported mild to moderate levels of stress. Table 3 summarizes the aspects of participants' lives that were most affected by the pandemic, as well as perceived risk of contagion, social isolation, and the ability to overcome the pandemic. For example, 44.1% of participants reported that they had felt socially isolated from others during confinement. Most participants reported that the areas that were most negatively impacted were recreational activities and hobbies (74.6%), social relationships (67.7%), mental health (62.9%), and the economy (50.4%). Regarding risk of contagion, 12% of participants believed that they are at risk of COVID-19 infection due to having a chronic disease, 9% due to being an older adult, and 7% due to high exposure to the virus at work. Nine percent of participants reported that they are at risk due to being pregnant, immunosuppressed, a smoker, and not following biosecurity measures.
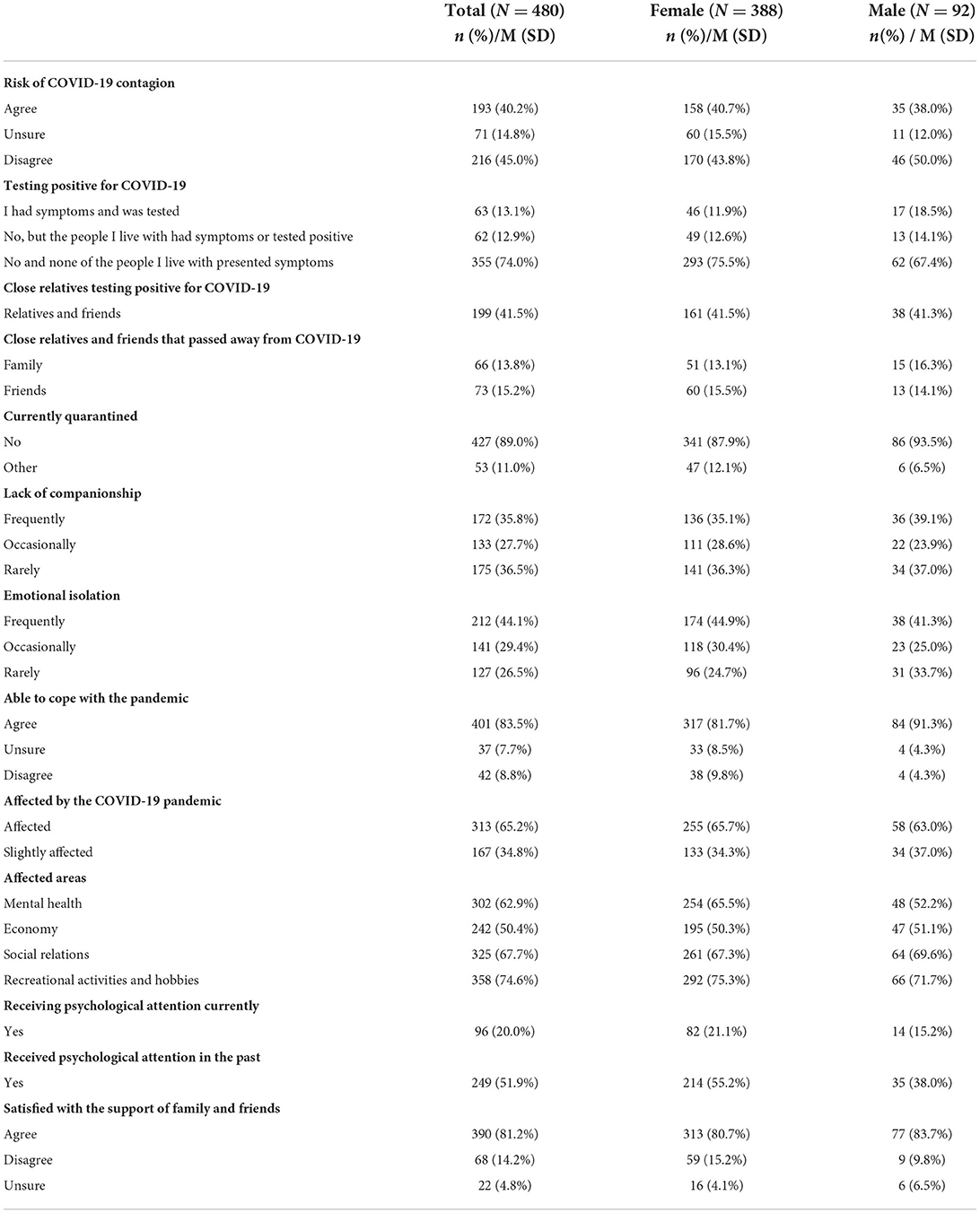
Table 3. Contagion risk, affected areas and psychological attention.
Additionally, approximately one in 10 of those surveyed (11%) were placed under mandatory quarantine (imposed by the government) because they had either tested positive for COVID-19 or were in close contact with someone who had tested positive for the virus. Half of the sample indicated that they frequently received information about the virus, and most of the participants (93%) reported that they knew, complied with, and agreed with the biosafety measures recommended by the Ministry of Health (MINSA). Most participants (93.8%) stated that they complied with biosafety measures because they wanted to take care of their health and that of others, while the rest complied with these measures because they were forced to do so, they were afraid of receiving a fine, or they were afraid of being detained by authorities.
Analysis of variance was used to examine sex differences. There was a significant difference between men and women in depression scores, such that women (M = 13.8) had a higher mean score of depression than men (M = 10.6), F(1, 479) = 4.76, p = 0.03. Women (M = 10.0) also had higher anxiety scores than men (M = 6.8), F(1, 479) = 9.48, p = 0.002, and higher (M = 17.0) stress scores than men (M = 13.0), F(1, 479) = 12.44, p < 0.001. However, there were no sex differences in resilience scores, F(1, 479) = 3.73, p = 0.054, insomnia scores, F(1, 479) = 1.92, p = 0.167, perceived social support, F(1, 479) = 0.64, p = 0.423, or prosociality, F(1, 479) = 2.50, p = 0.114. In sum, women reported higher depression, anxiety, and stress scores compared to men, but there were no significant differences in resilience, insomnia, prosociality, or perceived social support.
Similarly, analysis of variance was used to examine differences between age groups. Participants were divided into two groups: young adults (18–29 years of age) and adults (aged 30 and older). There was a statistically significant difference between those younger than 29 and those older than 30 years of age in depression scores, such that those younger adults (M = 14.5) had significantly higher scores than older adults (M = 9.0), [F(1, 478) = 44.00, p < 0.001. Younger adults (M = 11.0) also reported higher anxiety scores than older adults (M = 7.1), F(1, 478) = 21.49, p < 0.001, and higher stress scores (M = 18.4) than older adults (M = 13.1), F(1, 478) = 36.14, p < 0.001. Conversely, older adults (M = 76.12) reported significantly higher resilience scores than younger adults (M = 68.6), F(1, 478) = 34.60, p < 0.001. Further, older adults (M = 47.4) reported higher prosociality scores than younger adults (M = 45.7), F(1, 478) = 4.01, p = 0.046. There was not a significant difference between groups in insomnia scores, F(1, 478) = 1.23, p = 0.268, or perceived social support scores, F(1, 478) = 1.47, p = 0.227. In sum, younger adults reported worse depression, anxiety, and stress scores than older adults, while older adults reported higher resilience and prosociality scores than younger adults.
A hierarchical multiple regression analysis was performed to investigate whether sociodemographic characteristics, economic factors, physical health, social factors, and mental health are uniquely related to depression, anxiety, and stress symptoms (Table 4). The composite sum score of all DASS-21 subscales was used as the criterion variable. Predictor variables were entered stepwise: education level, marital status, sex, and age were added as predictor variables in Step 1, monthly income and employment status were added as predictor variables in Step 2, self-perceived health status and the number of diagnosed chronic illnesses were added as predictor variables in Step 3, the composite sum score of all MSPSS subscales, self-perceived loneliness, number of cohabitants, and self-perceived isolation were added as predictors in Step 4, and the total number of diagnosed psychiatric disorders, the composite sum score of all CD-RISC subscales, and the composite sum score of all AIS subscales were added as predictors in Step 5.
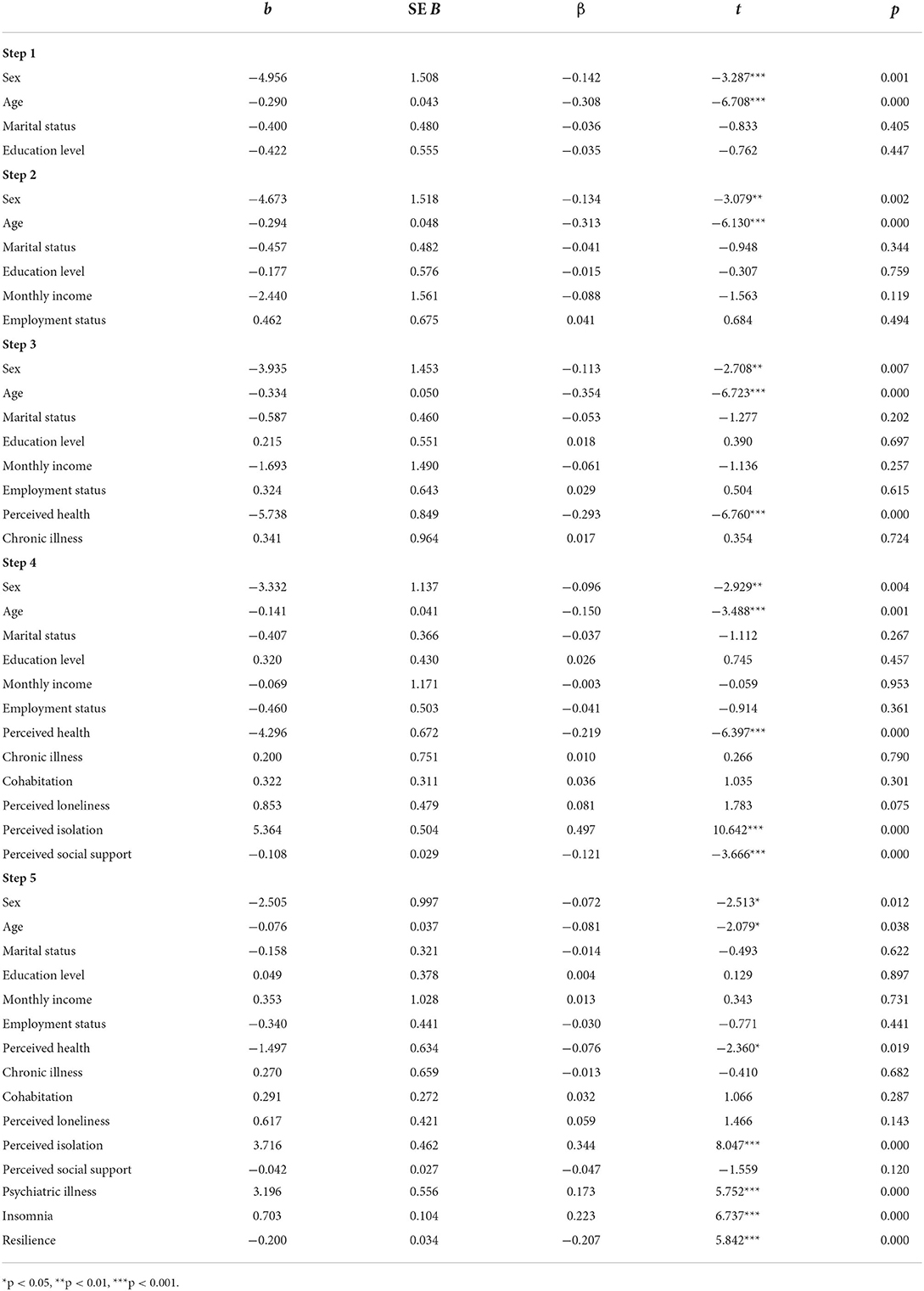
Table 4. Hierarchical multiple linear regression.
Step 1 explained a significant portion of the variance [F (4, 473) = 17.391, MSE = 12.850, R2 = 0.128, p < 0.001] in DASS-21, and indicated significant effects for sex and age but not civil status and education level. Step 2 explained additional variance but did not indicate significant model fit [FΔ (2, 471) = 1.257 MSE = 12.84, R2Δ = 0.005, R2 = 0.133, p = 0.285]. Monthly income and employment status were not significantly associated with depression, anxiety, and stress symptoms. Step 3 explained additional variance [FΔ (2, 469) =25.649, MSE = 12.219, R2Δ = 0.085, R2 = 0.218, p < 0.001] and indicated significant effects for self-perceived health status, but not the number of diagnosed chronic illnesses. Step 4 explained additional variance [FΔ (4, 465) =77.885, MSE = 9.496, R2Δ = 0.314, R2 = 0.532, p < 0.001] and indicated significant effects for self-perceived isolation, perceived social support but not self-perceived loneliness and the number of cohabitants. Step 5 explained additional variance [FΔ (3, 462) =48.842, MSE = 8.301, R2Δ = 0.113, R2 = 0.645, p < 0.001] and indicated significant effects for the number of diagnosed psychiatric disorders, insomnia, and resilience.
The main objective of this study was to analyze the psychosocial response to the COVID-19 pandemic in adults residing in Panama. Overall findings indicate several protective and risk factors associated with mental health outcomes for this sample of Panamanian adults during the COVID-19 pandemic. Social psychological factors, such as perceived social isolation (33, 34) and social support (35) accounted for the greatest proportion of the variance in depression, anxiety, and stress symptoms (36).
Our findings suggest that quarantine, isolation, and social distancing had a significant impact on the participants; more than half reported feeling affected by the COVID-19 pandemic, specifically regarding recreational activities and hobbies, social relations, mental health, and their income. These findings are in line with other recent studies showing that the biosafety measures implemented to stop the spread of the virus have significant implications for the psychosocial well-being of humans (37–39). Nevertheless, some people reported that during confinement they did not feel alone and that they were satisfied with the support of their loved ones. In this study, we reported negative relationships between the perception of social support and resilience on depression, anxiety, and stress symptoms. Similarly, several other studies have shown that social support, social well-being, prosocial behaviors, and resilience are factors that can enhance an adaptive response to stressful situations (40, 41). Thus, these findings point toward potential protective factors for individuals undergoing quarantine and lockdowns (42).
Regarding the risk factors for exposure to the virus, the current study documented a higher risk of infection among younger adults. Although older adults are a vulnerable group due to higher rates of chronic illnesses and increased mortality rates, emerging adults are more prone to contagion and spread of the virus due to social exposure and the belief that they are less at risk for severe symptoms (43–45). Moreover, other factors linked to the risk of contagion include having high exposure to the virus due to one's profession (e.g., healthcare worker), pregnancy, being immunosuppressed, smoking, and not following biosafety measures. Studies also indicate that vulnerable groups are affected by deficiencies, risks, or limitations related to health services, economic conditions, overcrowding, family dysfunction, unhealthy housing and environment, social insecurity, and discrimination. These risk factors increase the probability of comorbidities such as diabetes, obesity, hypertension, immunosuppression, or smoking (24, 25).
Furthermore, results indicated that male participants reported an increase in the consumption of cigarettes and alcoholic beverages. Some studies show that the stress derived from isolation can be a potential trigger for cigarette and alcohol consumption, which may indicate a maladaptive response to the pandemic (46, 47). In contrast, other studies documented that the pandemic encouraged some people to quit smoking, as smoking has been identified as a risk factor for more severe COVID-19 symptoms (48–51).
In line with other recent studies, results indicated that women experienced greater depression, anxiety, and stress symptoms than men (8–11). Sex differences in mental health symptoms are widely documented (52, 53) and recent research suggests that the COVID-19 pandemic uniquely affected the mental health of men and women. For example, many adult women experienced greater stress during confinement due to increased childcare demands and economic concerns (e.g., loss of employment, work from home mandates (54).
Our analyses also indicated that marital status, education, and economic factors (i.e., monthly income and employment status) were unrelated to depression, anxiety, and stress symptoms. Age and self-perceived health status—but not chronic illness—were negatively associated with depression, anxiety, and stress symptoms. Self-perceived social isolation was positively associated with depression, anxiety, and stress symptoms, whereas self-perceived social support was negatively associated with depression, anxiety, and stress symptoms. However, perceived loneliness and the number of cohabitants were unrelated to depression, anxiety, and stress symptoms. Psychiatric illness and insomnia were positively associated with depression, anxiety, and stress symptoms, whereas psychological resilience was negatively associated with depression, anxiety, and stress symptoms.
The results of this study corroborate previous research documenting an association between self-perceived health status and symptoms of depression, anxiety, and stress (55). Moreover, these results showed that chronic illnesses were not associated with symptoms of depression, anxiety, and stress (56, 57). One possibility for this finding is that most participants were young adults (aged 18–29) who had relatively few chronic illnesses. In addition, depression, anxiety, and stress was unrelated to the marital status, level of education, monthly income, and current employment status of participants. This further contradicts recent research documenting that lower education, low socioeconomic status, and unemployment is associated with greater symptoms of depression, anxiety, and stress (10, 58, 59). However, psychiatric illnesses were associated with symptoms of depression, anxiety, and stress. Feelings of loneliness and isolation are detrimental to mental health as they can be considered risk factors for the development of mental disorders such as depression, anxiety, adjustment disorder, chronic stress, insomnia, or dementia in old age (60, 61). Hence, preexisting mental health problems may be a notable risk factor for psychological distress during lockdowns (62).
In this study, young adults reported higher levels of depression, anxiety, and stress compared to adults. One study indicated that there were higher levels of stress, anxiety, and depression in adults aged 18 to 25 years compared to adults aged 26 to 60 years, and that people over 61 years old scored the lowest in stress, anxiety, and depression (56). Another study documented that people between 18-and 30 years old and over 60 years old presented higher levels of stress compared to middle aged adults (63). In contrast, other research documented that emerging adults experienced higher stress levels, whereas older adults experienced greater anxiety and depression (64). Additionally, women presented higher levels of depression, anxiety, and stress, similarly to other recent studies (65). Results also indicated a negative association between psychological resilience and symptoms of depression, anxiety, and stress. This corroborates previous research documenting that depression, anxiety, stress, insomnia, social disturbance, and somatic symptoms are associated with lower resilience (66). This finding may highlight the importance of resilience as a protective factor in the development of mental health problems in the context of pandemic lockdowns. Likewise, other factors, such as low income, familial problems, and less educational attainment may reduce individuals' resilience (67). In this sample, emerging adults scored lower in resilience compared to older adults. Previous research has indicated that emerging adults are affected more acutely by experiencing a loss or a traumatic situation, therefore, they may have difficulty understanding and controlling negative thoughts and unpleasant emotions such as fear, anger, irritability, and aggressiveness that arise due to social isolation and health-related stress (66, 68, 69).
This research employed a correlational and cross-sectional design, which prevents from drawing causal conclusions about the psychosocial effects of lockdowns. Participants were recruited via online convenience sampling, which constrained the pool of potential participants, thereby rendering the study's results as less generalizable. For instance, this study was limited to people with access to social media, computers, or smartphones, which may have resulted in the recruitment of participants who were younger, more educated, and more affluent than the general population. This sampling method may have also yielded a greater number of female participants because women are more interested and willing to participate in online psychological research than men (70). Indeed, several recent COVID-19 online survey studies that used similar recruitment methods obtained samples comprised of a disproportionate number of female participants (54, 71, 72). Nevertheless, at the time of the study, lockdown restrictions affected participants' and researchers' mobility, therefore online surveys were the only feasible option to collect data.
Despite the study's limitations, these data provide useful information about the mental health of Panamanian residents during the pandemic. The strengths of this study include the recruitment of a large sample and the utilization of valid instruments previously used and reported in similar studies. This study is the first report on the psychological impact of COVID-19 in the Panamanian general population and one of the only studies on the psychological impact of COVID-19 in the Latin American region, thus contributing to research on the Latin American population and low-middle income countries.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by National Research Bioethics Committee of Panama (Comité Nacional de Bioética de la Investigación, CNBI). The patients/participants provided their written informed consent to participate in this study.
DCO conceived the study and manuscript. DCO and MSP wrote the manuscript. SR-A, AET, EP-Q, CC, CPR, and GBB read, reviewed, wrote sections and equally contributed to the intellectual content and format of the manuscript. All authors approved the submitted version.
This work was supported by the Sistema Nacional de Investigación (SNI), the Secretaría Nacional de Ciencia, Tecnología e Innovación (SENACYT).
DCO and GBB acknowledge and thank the financial support of Sistema Nacional de Investigación (SNI), Secretaría Nacional de Ciencia, Tecnología e Innovación (SENACYT). All authors acknowledge and thank Universidad Santa María La Antigua (USMA) and the Instituto de Investigaciones Científicas y Servicios de Alta Tecnología (INDICASAT).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Onyeaka H, Anumudu CK, Al-Sharify ZT, Egele-Godswill E, Mbaegbu P. COVID-19 pandemic: A review of the global lockdown and its far-reaching effects. Sci Prog. (2021) 104:1–8. doi: 10.1177/00368504211019854
2. Jeong H, Yim HW, Song Y-J, Ki M, Min J-A, Cho J, et al. Mental health status of people isolated due to Middle East Respiratory Syndrome. Epidemiol Health. (2016) 38:e2016048. doi: 10.4178/epih.e2016048
3. Khalid I, Khalid TJ, Qabajah MR, Barnard AG, Qushmaq IA. Healthcare workers emotions, perceived stressors and coping strategies during a MERS-CoV outbreak. Clin Med Res. (2016) 14:7–14. doi: 10.3121/cmr.2016.1303
4. Lee AM, Wong JGWS, McAlonan GM, Cheung V, Cheung C, Sham PC, et al. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can J Psychiatry. (2007) 52:233–40. doi: 10.1177/070674370705200405
5. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
6. Dosil Santamaría M, Ozamiz-Etxebarria N, Redondo Rodríguez I, Jaureguizar Alboniga-Mayor J, Picaza Gorrotxategi M. Impacto psicológico de la COVID-19 en una muestra de profesionales sanitarios españoles. Rev Psiquiatr Salud Ment. (2021) 14:106–12. doi: 10.1016/j.rpsm.2020.05.004
7. Bueno Ferrán M, Barrientos-Trigo S. Caring for the caregiver: the emotional impact of the coronavirus epidemic on nurses and other health professionals. Enferm Clin. (2021) 31:S35–9. doi: 10.1016/j.enfcli.2020.05.006
8. Jawad MJ, Abbas MM, Jawad MJ, Hassan SM, Hadi NR. Mental Health and psychosocial considerations post covid-19 outbreak. Wiad Lek. (2021) 74:3156–9. doi: 10.36740/WLek202112106
9. Dubey S, Biswas P, Ghosh R, Chatterjee S, Dubey MJ, Chatterjee S, et al. Psychosocial impact of COVID-19. Diabetes Metab Syndr Clin Res Rev. (2020) 14:779–88. doi: 10.1016/j.dsx.2020.05.035
10. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) Epidemic among the General Population in China. Int J Environ Res Public Health. (2020) 17:1–25. doi: 10.3390/ijerph17051729
11. Sureima A, Fernández C, Margarita O, Ortiz G, Cruz V, Longevidad P, et al. Manifestaciones psicológicas en adultos mayores en aislamiento social durante la pandemia COVID-19. Ciencias Básicas Biomédicas. (2021) 1:1–12.
12. Britos Esquivel M, Estigarribia RE, Ferreira Moreira JR, Valenzuela Almada JA. Sociodemographic factors associated with hopelessness and anxiety in the Covid 19 quarantine period, in people residing in Paraguay. Rev Científica la UCSA. (2021) 8:3–13. doi: 10.18004/ucsa/2409-8752/2021.008.01.003
13. Parrado-González A, León-Jariego JC. [Covid-19: factors associated with emotional distress and psychological morbidity in spanish population]. Rev Esp Salud Publica. (2020) 94:e1–16.
14. Galindo-Vázquez O, Ramírez-Orozco M, Costas-Muñiz R, Mendoza-Contreras LA, Calderillo-Ruíz G, Meneses-García A. Symptoms of anxiety, depression and self-care behaviors during the COVID-19 pandemic in the general population. Gac Med Mex. (2020) 156:298–305. doi: 10.24875/GMM.M20000399
15. Joaquim RM, Pinto ALCB, Guatimosim RF, de Paula JJ, Souza Costa D, Diaz AP, et al. Bereavement and psychological distress during COVID-19 pandemics: the impact of death experience on mental health. Curr Res Behav Sci. (2021) 2:100019.
16. Gallegos M, Consoli A, Franco I, Cervigni M, de Castro V, Martino P, et al. COVID-19: impacto psicosocial y salud mental en América Latina. Fractal Rev Psicol. (2021) 33:226–32. doi: 10.22409/1984-0292/v33i3/51234
17. Espinosa-Guerra E, Rodríguez-Barría E, Donnelly C, Carrera J-P. Mental health consequences of COVID-19 in house staff physicians. F1000Research. (2022) 11:303. doi: 10.12688/f1000research.74191.1
18. Hale T, Angrist N, Goldszmidt R, Kira B, Petherick A, Phillips T, et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat Hum Behav. (2021) 5:529–38. doi: 10.1038/s41562-021-01079-8
19. Información Importante-ACNUR Panamá-Ayuda para refugiados y solicitantes de asilo. ACNUR Panamá (2020). Available online at: https://help.unhcr.org/panama/covid-19-2/avisos-importantes/
20. Sistema de. Información Centroamericana. Decretos y medidas adoptadas por Panamá. Portal del SICA. (2020).
21. The Lancet. COVID-19 in Latin America: a humanitarian crisis. Lancet. (2020) 396:1463. doi: 10.1016/S0140-6736(20)32328-X
22. Dasgupta S, Dierckxsens M, Verick S. The Impact of the COVID-19 Crisis on Middle-income Countries. Indian Econ J. (2021) 69:534–52. doi: 10.1177/00194662211023847
23. Webber M, Newhouse D. Developing countries introduced an unprecedented social protection and jobs policy response to mitigate the effects of the pandemic. World Bank Blogs. (2021). Available online at: https://blogs.worldbank.org/jobs/developing-countries-introduced-unprecedented-social-protection-and-jobs-policy-response (accessed April 13, 2022).
24. Quintanar F. Análisis de experiencias exitosas en seguridad social y salud mental de grupos vulnerables ante el impacto de la COVID-19. Centro Interamericano de Estudios de Seguridad Social. (2021) 1–61.
25. Cortés-Meda A, Ponciano-Rodríguez G. Impacto de los determinantes-sociales-de la COVID-19 en México. Boletín sobre COVID-19, UNAM. (2021) 2:9–13.
26. Banco Interamericano del Desarrollo. Población por edad y género - Minerpa. Mapa de Información Económica de la República de Panamá (2020). Available online at: https://minerpa.com.pa/poblacion-por-edad-y-genero/
27. Apóstolo JLA, Mendes AC, Azeredo ZA. Adaptación para la lengua Portuguesa de la Depression, Anxiety and Stress Scale (DASS). Rev Lat Am Enfermagem. (2006) 14:863–71. doi: 10.1590/S0104-11692006000600006
28. Portocarrero AN, Jiménez-Genchi A. Estudio de validación de la traducción al Español de la Escala Atenas de Insomnio. Salud Ment. (2005) 28:34−9.
29. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. Athens Insomnia Scale: validation of an instrument based on ICD-10 criteria. J Psychosom Res. (2000) 48:555–60. doi: 10.1016/S0022-3999(00)00095-7
30. Caprara GV, Steca P, Zelli A, Capanna C. A New Scale for Measuring Adults' Prosocialness. Eur J Psychol Assess. (2005) 21:77–89. doi: 10.1027/1015-5759.21.2.77
31. Broche-p Y, Abreu M, Villas L, Rodr BC, Abreu M, Villas L. Escala de Resiliencia de Connor-Davidson (CD-RISC). Feijoo. (2012) 1:71–98.
32. Ruiz Jiménez Maand Saiz Galdós J Montero Arredondo Maand Navarro Bayón D. Adaptation of the Multidimensional Scale of Perceived Social Support in people with severe mental disorders. Rev la Asoc Española Neuropsiquiatría. (2017) 37:415–37. doi: 10.4321/s0211-57352017000200006
33. González-Sanguino C, Ausín B, Castellanos MÁ, Saiz J, López-Gómez A, Ugidos C, et al. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav Immun. (2020) 87:172–6. doi: 10.1016/j.bbi.2020.05.040
34. Clair R, Gordon M, Kroon M, Reilly C. The effects of social isolation on well-being and life satisfaction during pandemic. Humanit Soc Sci Commun. (2021) 8:1–6. doi: 10.1057/s41599-021-00710-3
35. Grey I, Arora T, Thomas J, Saneh A, Tohme P, Abi-Habib R. The role of perceived social support on depression and sleep during the COVID-19 pandemic. Psychiatry Res. (2020) 293:1−7. doi: 10.1016/j.psychres.2020.113452
36. Mautong H, Gallardo-Rumbea JA, Alvarado-Villa GE, Fernández-Cadena JC, Andrade-Molina D, Orellana-Román CE, et al. Assessment of depression, anxiety and stress levels in the Ecuadorian general population during social isolation due to the COVID-19 outbreak: a cross-sectional study. BMC Psychiatry. (2021) 21:1–15. doi: 10.1186/s12888-021-03214-1
37. Etchevers MJ, Garay CJ, Putrino NI, Helmich N, Lunansky G. Argentinian mental health during the COVID-19 pandemic: a screening study of the general population during two periods of quarantine. Clin Psychol Eur. (2021) 3:20−36. doi: 10.32872/cpe.4519
38. Caccia PA, De Grandis MC, Perez G. Somatizaciones y Apoyo Social Funcional percibido en el contexto de Aislamiento Social Preventivo y Obligatorio por Covid-19, en Buenos Aires, Argentina. Psicol UNEMI. (2021) 5:8–18. doi: 10.29076/issn.2602-8379vol5iss8.2021pp8-18p
39. Sala E. Covid 19 Medidas restrictivas: cuarentena, aislamiento y estado de alarma ¿precursores de delirios? Universidad de Valencia-Hospital Clínico Universitario (2021).
40. Brailovskaia J, Margraf J. Predicting adaptive and maladaptive responses to the Coronavirus (COVID-19) outbreak: a prospective longitudinal study. Int J Clin Heal Psychol. (2020) 20:183–91. doi: 10.1016/j.ijchp.2020.06.002
41. Macías-Valadez Treviño ME, Gama Campillo LM, Zurita Macías-Valadez M, Rodríguez Quevedo F. UNA MIRADA A LA HISTORIA PARA LA RESILIENCIA ANTE EL COVID-19. Kuxulkab'. (2020) 26:79–92. doi: 10.19136/kuxulkab.a26n56.3847
42. Santamaría-García H, Burgaleta M, Legaz A, Flichtentrei D, Córdoba-Delgado M, Molina-Paredes J, et al. The price of prosociality in pandemic times. Humanit Soc Sci Commun. (2022) 9:1–12.
43. Módenes JA, Marcos M, García DM. Covid-19: ¿la vivienda protege a los mayores en América Latina? Argentina y Colombia comparadas con España. Perspect Demogràfiques. (2020) 20:1–4. doi: 10.46710/ced.pd.esp.20
44. Nupia O. Cuarentena y poscuarentena en Colombia: preocupaciones económicas, aislamiento social y aprobación del Gobierno. Cuad Econ. (2021) 40:921–55. doi: 10.15446/cuad.econ.v40n85.92053
45. Organización Panamericana de la Salud. Hospitalizaciones y muertes por COVID-19 de adultos jóvenes se disparan en las Américas (2021).
46. García-Álvarez L, Fuente-Tomás LD la, Sáiz PA, García-Portilla MP, Bobes J. ¿Se observarán cambios en el consumo de alcohol y tabaco durante el confinamiento por COVID-19? Adicciones. (2020) 32:85–9. doi: 10.20882/adicciones.1546
47. Sixto Costoya A, Lucas Domínguez R, Agulló Calatayud V. COVID-19 Y SU REPERCUSIÓN EN LAS ADICCIONES. Heal Addict y Drog. (2021) 21:259–78. doi: 10.21134/haaj.v21i1.582
48. Cai H. Sex difference and smoking predisposition in patients with COVID-19. Lancet Respir Med. (2020) 8:e20. doi: 10.1016/S2213-2600(20)30117-X
49. Hefler M, Gartner CE. The tobacco industry in the time of COVID-19: time to shut it down? Tob Control. (2020) 29:245–6. doi: 10.1136/tobaccocontrol-2020-055807
50. Hamer M, Kivimäki M, Gale CR, Batty GD. Lifestyle risk factors, inflammatory mechanisms, and COVID-19 hospitalization: a community-based cohort study of 387,109 adults in UK. Brain Behav Immun. (2020) 87:184−7. doi: 10.1016/j.bbi.2020.05.059
51. Tan HT, Chai BC, Lui YS. Effects of COVID-19 on Substance Use in Singapore. Subst Abus Res Treat. (2021) 15:1–7. doi: 10.1177/11782218211030533
52. Jalnapurkar I. Sex differences in anxiety disorders: a review. Psychiatry, Depress Anxiety. (2018) 4:1–9. doi: 10.24966/PDA-0150/100011
53. Bale TL, Neill Epperson C, Neurosci N. Sex differences and stress across the lifespan HHS Public Access Author manuscript. Nat Neurosci. (2015) 18:1413–20. doi: 10.1038/nn.4112
54. Fenollar-Cortés J, Jiménez Ó, Ruiz-García A, Resurrección DM. Gender differences in psychological impact of the confinement during the COVID-19 outbreak in Spain: a longitudinal study. Front Psychol. (2021) 12:1–11. doi: 10.3389/fpsyg.2021.682860
55. Buneviciene I, Bunevicius R, Bagdonas S, Bunevicius A. The impact of pre-existing conditions and perceived health status on mental health during the COVID-19 pandemic. J Public Health. (2022) 44:e88–95. doi: 10.1093/pubmed/fdab248
56. Ozamiz-Etxebarria N, Idoiaga Mondragon N, Dosil Santamaría M, Picaza Gorrotxategi M. Psychological symptoms during the two stages of lockdown in response to the COVID-19 outbreak: an investigation in a sample of citizens in northern Spain. Front Psychol. (2020) 11:1–17. doi: 10.3389/fpsyg.2020.01491
57. Wu T, Jia X, Shi H, Niu J, Yin X, Xie J, et al. Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. (2021) 281:91–8. doi: 10.1016/j.jad.2020.11.117
58. Johnson MC, Saletti-Cuesta L, Tumas N. Emociones, preocupaciones y reflexiones frente a la pandemia del COVID-19 en Argentina. Cien Saude Colet. (2020) 25:2447–56.
59. Mejia C, Quispe A, Franco J, Valero L. Factores asociados al fatalismo ante la COVID-19 en 20 ciudades del Perú en marzo 2020 | Mejia | Revista Habanera de Ciencias Médicas. Rev habanera ciencias médicas. (2020) 19:1–13.
60. Banerjee D, Rai M. Social isolation in Covid-19: the impact of loneliness. Int J Soc Psychiatry. (2020) 66:525–7. doi: 10.1177/0020764020922269
61. Llibre-Rodriguez J, Noriega-Fernández L, Guerra-Hernández M, Zayas-Llerena T, Llibre-Guerra J, Alfonso-Chomat R, et al. Soledad y su asociación con depresión, ansiedad y trastornos del sueño en personas mayores cubanas durante la pandemia por COVID-19. Anales de la Academia de Ciencias de Cuba. (2021) 11:1–8.
62. Gobbi S, Płomecka MB, Ashraf Z, Radziński P, Neckels R, Lazzeri S, et al. Worsening of Preexisting Psychiatric Conditions During the COVID-19 Pandemic. Front Psychiatry. (2020) 11:1–9. doi: 10.3389/fpsyt.2020.581426
63. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatry. (2020) 33:1–3. doi: 10.1136/gpsych-2020-100213
64. Gutiérrez R, González A. Importancia de los factores que influyen en el desarrollo de ansiedad, depresión y estrés durante la pandemia de la COVID-19. Rev Habanera Ciencias Médicas. (2021) 20:1–3.
65. Frontini R, Rebelo-Gonçalves R, Amaro N, Salvador R, Matos R, Morouço P, et al. The relationship between anxiety levels, sleep, and physical activity during COVID-19 lockdown: an exploratory study. Front Psychol. (2021) 12:1–8. doi: 10.3389/fpsyg.2021.659599
66. Martínez Arriaga RJ, González Ramírez LP, Navarro Ruiz NE, De la Roca -Chiapas JM, Reynoso González OU. Resiliencia asociada a factores de salud mental y sociodemográficos en enfermeros mexicanos durante COVID-19. Enfermería Glob. (2021) 20:1–16. doi: 10.6018/eglobal.452781
67. Lacomba-Trejo L, Mateu J, Cabajo E, Oltra A. Percepción de amenaza de la enfermedad renal crónica avanzada y su asociación con la sintomatología ansiosa y depresiva. Rev Psicol LA SALUD. (2021) 8:123–36.
68. Ang SY, Uthaman T, Ayre TC, Mordiffi SZ, Ang E, Lopez V. Association between demographics and resilience-a cross-sectional study among nurses in Singapore. Int Nurs Rev. (2018) 65:459–66. doi: 10.1111/inr.12441
69. Pérez J, Dorado A, Rodríguez-Brioso M, López J. Resiliencia para la promoción de la salud en la crisis Covid-19 en España/ Resilience for health promotion in the Covid-19 crisis in Spain. Rev Ciencias Soc. (2020) XXVI:52–63. doi: 10.31876/rcs.v26i4.34649
70. Gosling SD, Vazire S, Srivastava S, John OP. Should We Trust Web-Based Studies? A Comparative Analysis of Six Preconceptions About Internet Questionnaires. Am Psychol. (2004) 59:93–104. doi: 10.1037/0003-066X.59.2.93
71. Liu N, Zhang F, Wei C, Jia Y, Shang Z, Sun L, et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: gender differences matter. Psychiatry Res. (2020) 287:1–7. doi: 10.1016/j.psychres.2020.112921
Keywords: COVID−19, psychological distress, mental health, restrictions, depression, anxiety, stress
Citation: Oviedo DC, Pinzón MS, Rodríguez-Araña S, Tratner AE, Pauli-Quirós E, Chavarría C, Posada Rodríguez C and Britton GB (2022) Psychosocial response to the COVID-19 pandemic in Panama. Front. Public Health 10:919818. doi: 10.3389/fpubh.2022.919818
Received: 13 April 2022; Accepted: 15 July 2022;
Published: 10 August 2022.
Edited by:
Jerome T. Galea, University of South Florida, United StatesReviewed by:
Muhammad Syawal Amran, National University of Malaysia, MalaysiaCopyright © 2022 Oviedo, Pinzón, Rodríguez-Araña, Tratner, Pauli-Quirós, Chavarría, Posada Rodríguez and Britton. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diana C. Oviedo, ZC5vdmlAaG90bWFpbC5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.