
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 14 September 2022
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.918921
This article is part of the Research TopicEpidemiology and Molecular Epidemiology of Childhood and Adolescent CancersView all 7 articles
 Janet Flores-Lujano1†
Janet Flores-Lujano1† David Aldebarán Duarte-Rodríguez1†
David Aldebarán Duarte-Rodríguez1† Elva Jiménez-Hernández2,3
Elva Jiménez-Hernández2,3 Jorge Alfonso Martín-Trejo4
Jorge Alfonso Martín-Trejo4 Aldo Allende-López1
Aldo Allende-López1 José Gabriel Peñaloza-González5
José Gabriel Peñaloza-González5 María Luisa Pérez-Saldivar1
María Luisa Pérez-Saldivar1 Aurora Medina-Sanson6
Aurora Medina-Sanson6 José Refugio Torres-Nava3Karina Anastacia Solís-Labastida4Luz Victoria Flores-Villegas7
José Refugio Torres-Nava3Karina Anastacia Solís-Labastida4Luz Victoria Flores-Villegas7 Rosa Martha Espinosa-Elizondo8
Rosa Martha Espinosa-Elizondo8 Raquel Amador-Sánchez9Martha Margarita Velázquez-Aviña5Laura Elizabeth Merino-Pasaye7Nora Nancy Núñez-Villegas2Ana Itamar González-Ávila9María de los Ángeles del Campo-Martínez2Martha Alvarado-Ibarra7
Raquel Amador-Sánchez9Martha Margarita Velázquez-Aviña5Laura Elizabeth Merino-Pasaye7Nora Nancy Núñez-Villegas2Ana Itamar González-Ávila9María de los Ángeles del Campo-Martínez2Martha Alvarado-Ibarra7 Vilma Carolina Bekker-Méndez10Rocío Cárdenas-Cardos11
Vilma Carolina Bekker-Méndez10Rocío Cárdenas-Cardos11 Silvia Jiménez-Morales12
Silvia Jiménez-Morales12 Roberto Rivera-Luna11
Roberto Rivera-Luna11 Haydee Rosas-Vargas13Norma C. López-Santiago14Angélica Rangel-López15
Haydee Rosas-Vargas13Norma C. López-Santiago14Angélica Rangel-López15 Alfredo Hidalgo-Miranda12
Alfredo Hidalgo-Miranda12 Elizabeth Vega16
Elizabeth Vega16 Minerva Mata-Rocha13Omar Alejandro Sepúlveda-Robles13
Minerva Mata-Rocha13Omar Alejandro Sepúlveda-Robles13 José Arellano-Galindo17
José Arellano-Galindo17 Juan Carlos Núñez-Enríquez1*
Juan Carlos Núñez-Enríquez1* Juan Manuel Mejía-Aranguré12,13,18*
Juan Manuel Mejía-Aranguré12,13,18*Introduction: Over the years, the Hispanic population living in the United States has consistently shown high incidence rates of childhood acute leukemias (AL). Similarly, high AL incidence was previously observed in Mexico City (MC). Here, we estimated the AL incidence rates among children under 15 years of age in MC during the period 2010–2017.
Methods: The Mexican Interinstitutional Group for the Identification of the Causes of Childhood Leukemia conducted a study gathering clinical and epidemiological information regarding children newly diagnosed with AL at public health institutions of MC. Crude age incidence rates (cAIR) were obtained. Age-standardized incidence rates worldwide (ASIRw) and by municipalities (ASIRm) were calculated by the direct and indirect methods, respectively. These were reported per million population <15 years of age; stratified by age group, sex, AL subtypes, immunophenotype and gene rearrangements.
Results: A total of 903 AL cases were registered. The ASIRw was 63.3 (cases per million) for AL, 53.1 for acute lymphoblastic leukemia (ALL), and 9.4 for acute myeloblastic leukemia. The highest cAIR for AL was observed in the age group between 1 and 4 years (male: 102.34 and female: 82.73). By immunophenotype, the ASIRw was 47.3 for B-cell and 3.7 for T-cell. The incidence did not show any significant trends during the study period. The ASIRm for ALL were 68.6, 66.6 and 62.8 at Iztacalco, Venustiano Carranza and Benito Juárez, respectively, whereas, other municipalities exhibited null values mainly for AML.
Conclusion: The ASIRw for childhood AL in MC is among the highest reported worldwide. We observed spatial heterogeneity of rates by municipalities. The elevated AL incidence observed in Mexican children may be explained by a combination of genetic background and exposure to environmental risk factors.
Acute leukemias (AL) are the most common childhood cancer worldwide (1), representing over one-third of all childhood cancer types (2). Populations with Hispanic (Latin American) ancestry living in the United States have exhibited high AL incidences, as also documented previously in Mexican children (3–6). Among Hispanics, the incidence of childhood AL is 55.0 cases per million children under 15 years of age. These rates are higher compared to those reported for other ethnic groups, such as White, Asian-Pacific, and African-American (7). In Mexico City (MC), the incidence rates of AL are among the highest in the world (3, 8–10) (Supplementary Table 1). Recent studies have reported an increasing trend in AL incidence among children (1.1 and 2.3% annually), particularly, in populations of Hispanic ancestry (7, 11–13); however, this tendency has not been consistently observed, neither broadly (14) nor particularly in MC (10).
Acute lymphoblastic leukemia (ALL) is the most frequent leukemia subtype in Mexican children where the B-cell ALL, also known as B-ALL, occurs with frequencies of 76.1–81.4%, followed by the T-cell subtype (12.4–23.6%) (3, 15). These immunophenotypes display frequencies of 87 and 13% in the Hispanic population, and 85 and 15% worldwide, respectively (16–23). Additionally, the prevalence of the most common gene rearrangements in Mexican population is as follows: ETV6-RUNX1 (7.4–13.5%), TCF3-PBX1 (7.1–11.5%), BCR-ABL1 (1.8–2.7%), and MLL rearrangements (1.4–8.7%) (24–26). These frequencies are similar to those found in other Hispanic populations (24, 25, 27–29), and those reported worldwide (13, 20, 23–25, 27–41). One important and recurrent finding in the Mexican population with childhood ALL is the low frequency of ETV6-RUNX1, a gene rearrangement associated with a good prognosis of the disease (42). Internationally, the prevailing assumption was that these gene rearrangements were the most important ones, which played an important role in the clinic (diagnosis, risk stratification and chemotherapy treatment). However, new genetic variants have been identified that provide additional information not only on the implications for treatment and relapse of this disease, but also on the ages at which they are most commonly observed (43).
MC not only exhibits among the highest AL incidence rates in the world, but it has also shown variable incidence trends over time, suggesting a potential role of non-genetic factors in disease development (44), such as an effect of the diversity of environmental exposure across municipalities (45). Several studies support this possibility, exhibiting differences in exposure among areas or municipalities—for example, to air pollution (46–49), metalsand chemicals of industrial, agriculture, commercial, and vehicular origin (50, 51), and to different near-surface air temperatures. This last variable has become of great epidemiological interest (52–56) since it is related to the atmospheric distribution of pollutants, and shows great variability between municipalities and areas of MC (57).
MC is composed by 16 municipalities, previously defined such as boroughs by political reasons (until 2018). No changes in delineation of these have occurred in the past 50 years (58, 59). The municipalities of Cuauhtémoc, Benito Juárez, Miguel Hidalgo, Azcapotzalco are in the central and northern territory; and to the south and southwest are the municipalities of Álvaro Obregón and Coyoacán. These have an abundance of fresh water, greater urban development, business, and service areas and have a medium population density. Also, these zones have greater railroad connections, which favored greater industrial development.
On the other hand, located to the east of MC are the municipalities of Iztapalapa, Iztacalco, and Venustiano Carranza; and to the northeast, the Gustavo A. Madero. These municipalities are densely populated and considered as a low socioeconomic status areas. The east of the city has a considerable extension of plain land which led to the construction of the airport of MC.
In the south of MC, the municipalities of La Magdalena Contreras, Cuajimalpa, Tlalpan, Xochimilco and Tláhuac are located. These have been the last to be urbanized, and even rural and agricultural activities still subsist. Currently, the municipality of Milpa Alta, located in the southeast, is almost entirely rural (60–62).
Moreover, MC possesses a bright land surface and a peculiar weather cycle and is in a high-altitude and semi-enclosed basin surrounded by mountains with unique planetary boundary layer dynamics (46). In addition, a spatial variability of mortality rates by municipalities has been reported in MC (63). Therefore, it is important to perform a constant monitoring and evaluation of AL trends of incidence rates by municipalities in MC.
In the present study, we aimed to assess the AL incidence rate and trends (age, sex, immunophenotype, and gene rearrangement) during the period 2010–2017, MC residents of 0–14 years of age, according to age groups and municipalities.
AL cases were identified using the population-based registry of the Mexican Interinstitutional Group for the Identification of the Causes of Childhood Leukemia (MIGICCL). Since 2006, the MIGICCL has collected information from public health institutions in MC: Instituto Mexicano del Seguro Social (IMSS) (three hospitals), Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (ISSSTE) (two hospitals), Secretaría de Salud (SS) (four hospitals), and Secretaría de Salud de la Ciudad de México (SS CDMX) (one hospital). These 10 hospitals provide care for an estimated 97.5% of children with leukemia who reside in MC (64).
Case registration required that trained personnel were assigned to each participating hospital to identify incident cases of leukemia through reviews of clinical charts. The parents of each child were required to sign an informed consent form if they agreed to participate in an in-person interview.
The interview was carried out using a questionnaire previously standardized and adapted from the questionnaire module of the National Cancer Institute. General information obtained included the child's sex, age at the time of diagnosis (in years), and municipality of residence. Additionally, the clinical chart of the child and an official document (photo-voting card) provided by the parents at the time of the interview were reviewed, when possible, to verify the accuracy of the information provided.
AL diagnosis was established based on clinical features, and bone marrow aspirate findings, including cell morphology, immunophenotype, and genetics, as defined in 2008 by the World Health Organization (WHO) for the classification of lymphoid neoplasms.
The MIGICCL registered all newly diagnosed AL cases from January 2010 to December 2017. Only cases with residence in MC were included.
The leukemia subtypes were defined according to ICD-O-2/ICD-O-3, forming the following three groups: ALL (9820, 9821, 9828), AML (9840, 9860, 9861, 9866, 9867, 9872, 9873, 9874, 9891, 9910), and other leukemias (OL) (9863, 9868, 9875, 880) (65). Furthermore, the immunophenotypes were classified according to WHO criteria: B-cell, T-cell, and AL of ambiguous lineage (ALAL) (66).
Gene rearrangements were detected by experts in two IMSS laboratories. The four most common gene rearrangements with clinical implications (ETV6-RUNX1, TCF3-PBX1, BCR-ABL1, and MLL rearrangements) were identified by reverse transcription polymerase chain reaction (RT-PCR) using a bone marrow sample that was collected by pediatric hematologists or oncologists from each patient at the time of diagnosis confirmation (67). The assessment of these gene rearrangements in the IMSS' laboratories began in 2010 through financial support of research studies and they were not routinely performed in most of the public institutions of MC.
The population base of children under 15 years old from each municipality was obtained through information from the 2000 and 2010 censuses of the National Institute of Statistics and Geography (INEGI) (68–71). The exponential projection method was used to estimate the population of children from 2011 to 2017 (72, 73).
The crude incidence rate was reported by age-specific groups (cAIR). This was calculated by dividing the number of new AL cases from each year (2010–2017) by the population of children from each municipality of MC during the same period. Afterwards, the rates were determined for overall AL and subtypes (ALL, AML and OL). In addition, the rates were calculated according to the immunophenotype classification (B-cell, T-cell, and ALAL) (66), gene rearrangement groups (TCF3-PBX1, ETV6-RUNX1, MLL-AFF1, BCR-ABL1, and other) and by the child's sex. These rates were reported per million children under 15 years of age.
Standardized incidence rates were calculated using the direct and indirect methods, they were also reported per million children under 15 years of age. The direct method compared age-standardized incidence rates of AL worldwide (ASIRw), with the reference being the world population as proposed by Segi (74), and modified by Doll et al. (75). Analyses were performed according to age groups (0–4, 5–9, and 10–14 years old), as well as by sex, AL subtype, immunophenotype, and gene rearrangements. The indirect method calculated the age-standardized incidence rates by municipalities (ASIRm), with the reference being population data reported in the 2010 census from INEGI for MC. Analyses were performed according to age groups (<1, 1–4, 5–9, and 10–14 years old), as well as by sex, AL subtype, immunophenotype, and gene rearrangements. We used this approach because some municipalities and age groups showed a lower or even null frequency of some AL subtypes. To understand the spatial distribution of incidence in each municipality, the ASIRm results were mapped using QGIS 3.14 software (Open Source Geospatial Foundation, Beaverton, Oregon, USA, QGIS, RRID:SCR_018507).
We also evaluated whether the incidence rates showed a temporal trend, among different AL subgroups, by estimating the average annual percent change (AAPC), using the Joinpoint Regression Program, Version 4.8.0.1 (National Cancer Institute, Bethesda, Maryland, USA, Joinpoint, RRID:SCR_018129). This program does not analyze years with incidence values of zero. To overcome this limitation, we used a correction strategy that has been applied in other studies (76, 77), in which an imputed incidence rate was generated by arbitrarily adding a half-case within the age group with the largest child population to the calculation. However, the AAPC could not be calculated when the correction required imputed data for more than 3 years.
A total of 3,484 incident cases were registered in the MIGICCL database during the period from 2010 to 2017, among which 903 (25.9%) patients were residents of MC (Figure 1). Of the included cases, 478 patients were male (52.9%) and 425 were female (47.1%). The diagnosis was ALL in 754 (83.5%) patients, AML in 137 (15.2%), and OL in 12 (1.3%). The most common subtype was B-cell (n = 669, 88.7%), followed by T-cell (7.0%) and ALAL (4.3%). Gene rearrangement data were available for 512 (56.7%) patients. Of these patients, 396 (77.4%) were negative for the four most common fusion genes. ETV6-RUNX1 was detected in 42 (8.2%) cases, and TCF3-PBX1 in 13 (2.5%) (Figure 1).
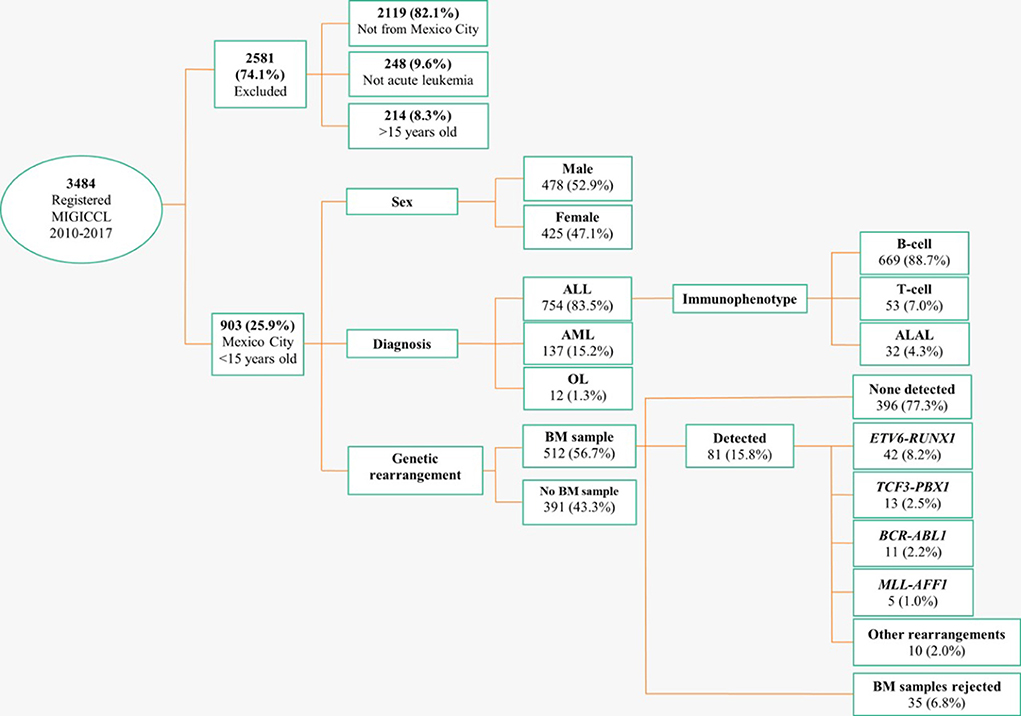
Figure 1. Flow chart of the selection process. The incidence rate of AL among children of MC during the period 2010–2017 based on the MIGICCL registry. MIGICCL, Mexican Interinstitutional Group for Identification of the Causes of Childhood Leukemia; ALL, acute lymphoblastic leukemia; AML, acute myeloblastic leukemia; OL, other leukemias; BM, bone marrow; ALAL, AL of ambiguous lineage.
The cAIR for all AL was 61.1 cases per million. By AL subtype, the cAIR was 51.0 for ALL, 9.3 for AML, and 0.8 for OL. The ASIRw was 63.3 cases per million for all AL, 53.1 for ALL, 9.4 for AML, and 0.8 for OL (Table 1).
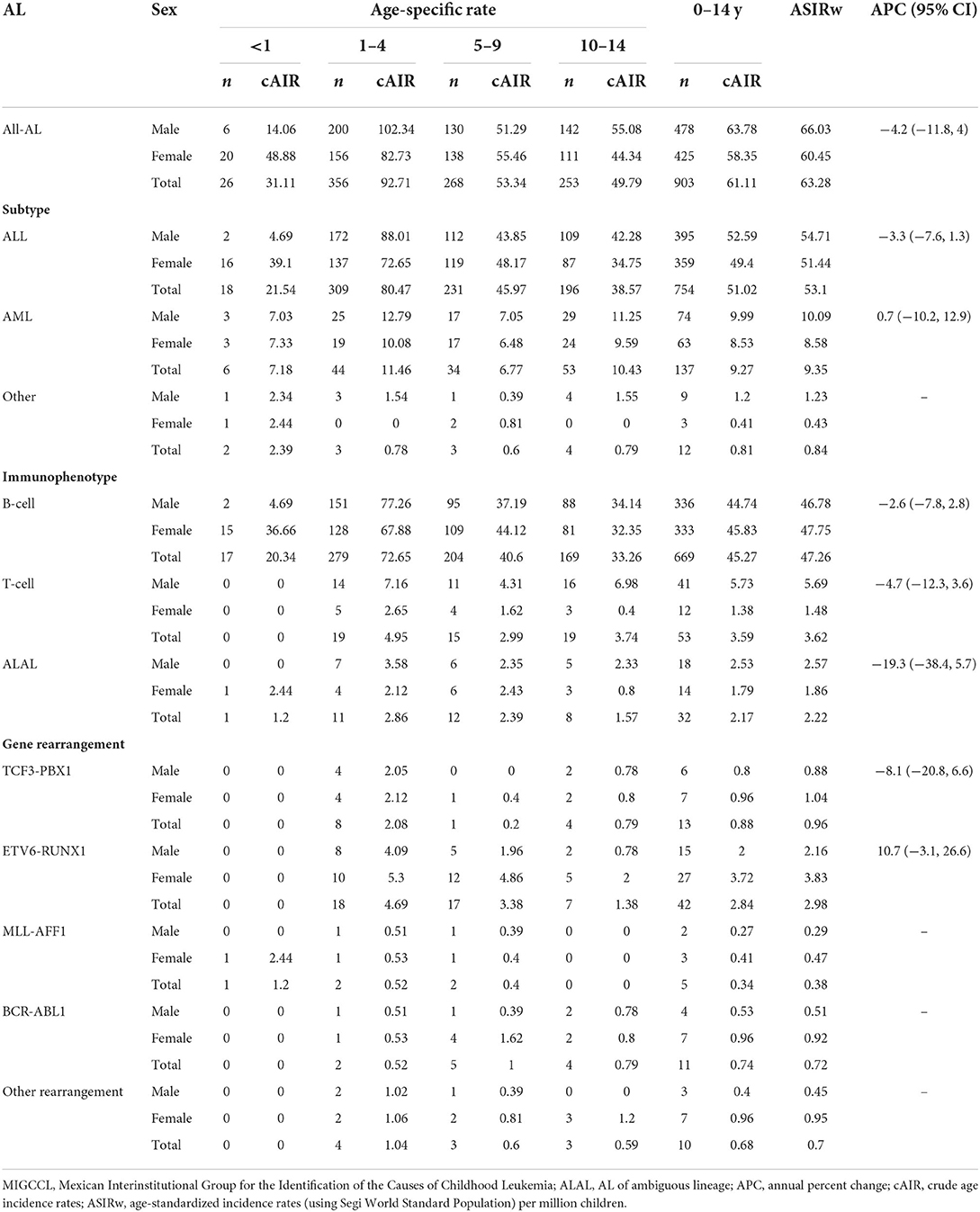
Table 1. The incidence rate of AL among children in MC, based on the MIGCCL registry during the period 2010–2017.
Figure 2 shows the ASIRm in cases per million. The highest ASIRm values for ALL were found in the municipalities of Iztacalco (68.6), Venustiano Carranza (66.6), and Benito Juárez (62.8) (Figure 2A). The highest ASIRm for AML was found in Venustiano Carranza (18.6) (Figure 2B). Notably, the highest ASIRm values for the ALL and AML subtypes were found in the Central and Eastern zones of MC.

Figure 2. (A) MC ASIRm Maps. The municipalities are alphabetically ordered. ALL ASIRm, age-standardized incidence rates by municipalities. (B) MC ASIRm Maps. The municipalities are alphabetically ordered. AML ASIRm, age-standardized incidence rates by municipalities.
The AAPC results did not show statistical evidence of an increasing or decreasing trend (p <0.05). Notably, only the ALAL subgroup was analyzed using the technique of rate imputation; analysis of the other subgroups was not possible due to the small number of patients. On the other hand, given the fact that we did not find joinpoints throughout the data series, the most appropriate way to refer to the trend summary measure is APC (annual percent change). Then the results displayed in Table 1 refer to APC.
The highest cAIR for ALL was observed in the 1–4 year age group (80.5 cases per million), where the cAIR for ALL was higher among males (88.1) than for females (72.6). In contrast, within the 5–9 year age group, the cAIR for ALL was higher among females than males. The highest cAIR values for AML were observed in the 1–4 year age group (11.5) and in the 10–14 year age group (10.4). The cAIR for AML was higher among males than females (Table 1).
The ASIRw was 47.3 (cases per million) for the B-cell subtype, and 3.7 for the T-cell subtype (Table 1).
Among cases of ALL, we observed the peak incidence at 3 years old, with a decrease at 10 years of age, and then a slight increase at 14 years old. Among cases of AML, we observed a peak incidence at 1 year old, with a slight increase between 10 and 12 years old (Figure 3A). No age-related pattern was observed for the OL subtype (not showed). For B-cell, we observed a major incidence age peak at 3 years old, and a slight increase at 14 years old. For T-cell AL, we observed multiple incidence age peaks at one, four, eight, and 12 years old (Figure 3B).
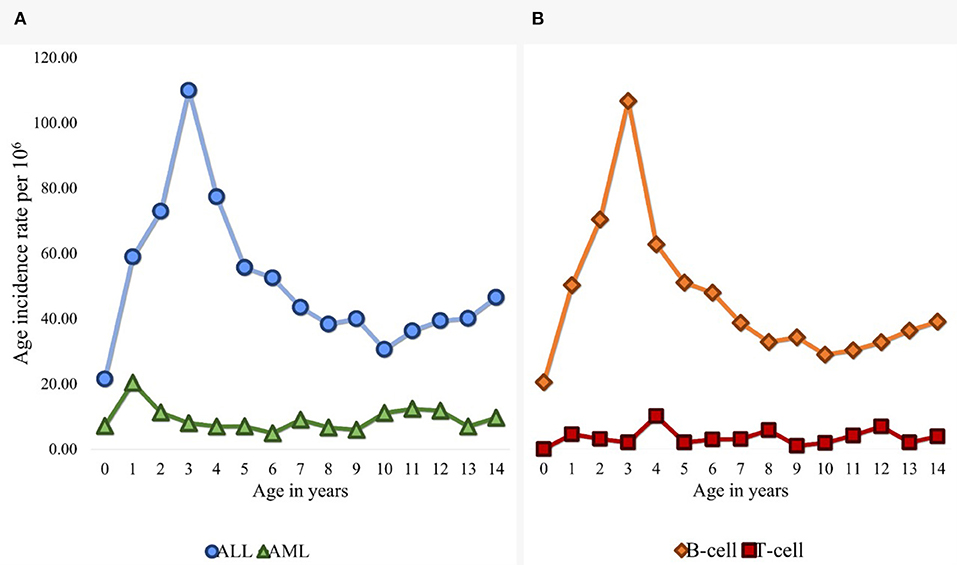
Figure 3. (A) Age-standardized incidence rates of childhood AL in MC (2010–2017) by subtype: ALL and AML. (B) Age-standardized incidence rates of childhood AL in MC (2010–2017) by immunophenotype: B-cell and T-cell ALL.
In this study, we determined the AL incidence rates in the population under 15 years of age from MC during the period of 2010–2017. The ASIRw of AL was slightly higher (63.3 cases per million) than those previously reported in studies conducted in MC: 58.4 during 1996–2000; 55.4 during 1996–2002; 62.2 during 1996–2013 and 57.6 during the period 2006–2007 (3, 8–10). This finding is consistent with the observed among Hispanic children living in the USA (65.4), Texas (59.8) and California (55.0) (2, 7, 78). Notably, the North American regions with Mexican, Canadian, and American populations display high incidence rates of AL (31.4–65.4) in comparison to other populations (2, 3, 8–10, 72, 78–81). Furthermore, studies in children of Hispanic ancestry, aged 0–19 years, have also shown incidence rates that are among the highest worldwide (7, 11, 82–89) (Supplementary Table 1).
Several studies show high AL incidence rates among Oceanians (Pacific Islanders) (56.4) (2), Australians (50.0–53.5) (90–92), and Europeans (42.1–57.1) (93–101); but these rates are slightly below than those reported for populations in the North American regions with Hispanic ancestry.
The incidence rates in Asia (30.7–53.5) (102–109) and African countries (0.5–33.6) (2, 110, 111) are appreciably lower than the rates reported in our study and worldwide. However, the rates reported from Africa should be interpreted cautiously, because it has been mentioned that the cancer registries of some African countries are likely affected by under-reporting (112).
Interestingly, in South America, Central America, and the Caribbean regions, which are home to children of Latin American ancestry, show lower AL rates (33.3–49.8) than those reported in the present research (2, 113, 114). One possible explanation is the fact that in the Caribbean subregion, the African ancestry is also prevalent, which has been associated with a low incidence rate of childhood AL. On the other hand, in the southernmost regions of South America and Costa Rica in Central America, the predominant component of the ancestry is European, which has been associated with moderate incidence rates of childhood AL instead of high rates (115). However, other relevant factors should be taken into consideration for explaining these differences, such as the quality of the cancer registries, the environmental, lifestyle factors among others.
Previous studies conducted in MC had already reported high incidence rates for childhood ALL during the periods 1996–2000 (44.9), 1996–2002 (43.2), and 2006–2007 (49.5), respectively. However, for the present study, a higher incidence rate than previously reported (53.1) was observed. It should be noted that all of these rates are among the highest in the world; nevertheless, to our knowledge, the incidence observed in the present study is one of the first reported above 50 cases per million in MC and globally. Additionally, the rate of incidence of ALL in MC is consistent with the reported in the population with Hispanic ancestry (116–118). This increase may not only be explained by genetic susceptibility but also with the interaction with the exposure to some environmental factors (119).
The ASIRw for AML was 9.4 cases per million in the present investigation. The incidence rate for this subtype of AL has remained stable and similar to that reported in previous studies conducted in MC throughout the periods of 1996–2000 (10.6), 1996–2002 (9.8), 2006–2007 (6.9) and 2010–2014 (7. 7) (3.8–10.6); as well as have been consistent to the rates reported worldwide in the regions of North America (7.0–10.6) (3, 8, 9, 72, 78, 79, 120); Europe (5.9–9.3) (94, 95, 99–101); Australia (7.2–8.7) (90, 91) and South America, Central America, and Caribbean (8.3–9.2) (112, 113); with the exception of the regions of Asia (5.4) (104) and Africa (0.3 to 6.0) (111). It has also been observed that AML occurs more frequently in infants and adolescents (121), in contrast to the ALL subtype. Moreover, several investigations support that the AML subtype present different etiopathogenic components compared to the subgroup of patients with ALL (122). However, the etiology for both leukemias remains unresolved until date, but, a small number of risk factors have been reported as established for the development of AML in children (121, 123–131).
During the period analyzed in the present work (2010–2017), no trends for AL incidence rates were observed. This is similar to the reported in MC from 2002 to 2013 where a phenomenon of stability in incidence rates for childhood AL had been described. Nonetheless, it should be noted that previous studies included data from a single health institution (IMSS) in contrast with the present research which was conducted in all public health institutions that care for children with cancer (IMSS, ISSSTE, SS, SSCDMX). This could support that the results obtained in the present study are representative for this disease in MC. On the other hand, this stable pattern also suggests that incidence rates for AL have remained high for at least over the last two decades in the population of MC (10). Moreover, the stability of the incidence rates described in this report is not consistent with those published in children of Hispanic ancestry in the USA, where the increasing trend is higher in comparison to other ethnic groups (Amerindian, Asian-Pacific, White, Afro-American) (12). A longer evaluation may be required.
The frequency of B-cell (88.7%) in our study is higher than the reported previously in MC (73.2–85.1%) (3, 15, 24, 132) but is similar to worldwide reported frequencies (80–92%) (111, 112), except to that reported in Asian countries (92.7%) (132). These differences could be associated with the genetic profile of our population with B-cell, as reported in a study by Moreno-Lorenzana et al. (133), who report a high frequency (54.1%) of dominant-negative IKZF1 isoform transcripts in a pediatric population from a single medical institution (133). One of the reasons why there is a greater frequency of B-cell among Hispanics may be its relationship with IKZF1 and ARID5B, which have also been reported more frequently in Hispanics. In this regard, it has been described that both the Hispanic ancestry and the presence of the germline IKZF1 variant are related to a poor response to treatment in children with B-cell (134). As well as it has been reported the role of ARID5B gene in B-cell development, particularly, in the Hispanic population (135, 136). Recently, the ARID5B gene has been associated with an increased risk of B-cell in Mexican children (137, 138).
In the present study, the frequency of T-cell ALL was of 7.0%. This finding is similar to the reported in the most of the studies conducted in MC (5.7–12.4%) (3, 24, 25, 139) and other regions of the world (10–15%) (140, 141). Conversely, in another study conducted in MC by Perez-Saldivar et al., where the authors reported a frequency around the 24% among ALL subtypes (3). Noteworthy, an elevated frequency of T-cell leukemias has also been reported in other developing countries (18–23.4%) (142, 143). It is well-recognized that the T-cell subtype is associated with a poor prognosis of the disease, particularly, a high incidence of isolated central nervous system relapse has been described in this group (144).
Regarding the age-specific incidence of ALL, previous studies conducted in MC have reported the existence of a maximum age peak in ALL occurring at the age of 3 years, which is consistent with the observed in the present investigation and which falls within the peak age range reported for ALL in international studies (2–5 years) (145). We also found a slight increase in incidence at 14 years of age, which was also observed in MC by Bernaldez-Rios et al. (15). Until this moment, we do not have an explanation for this last increase during adolescence but it has been observed that in countries where there is a lower frequency of the ETV6-RUNX1 rearrangement there is a higher frequency of ALL in adolescents and also a higher frequency of gene rearrangements with worse prognosis (146). In addition, some genetic factors such as the Ph-like phenotype may be one of the reasons for this observation due to the fact that its prevalence increase with the age in ALL patients. Nonetheless, this hypothesis should be studied further in Mexican population.
The overall detection of the four most common gene rearrangement was low as it has been reported in previous studies conducted in MC which also have reported a low frequency of ETV6-RUNX1, ranging from 7.4 to 13.5% (26, 27, 64), which is consistent with the findings of the present study (8.2%) and other Hispanic populations (27, 147) but lower than the frequency reported in developed countries (25–30%) (25, 29). Moreover, the low prevalence of ETV6-RUNX1 has implications in the ancestry component of the childhood ALL. In this regard, it has been described that when the Amerindian (indigenous) ancestry is higher, the ETV6-RUNX1 is less common. This type of ancestry has been consistently associated with a high incidence and poor prognosis of childhood ALL and in a recent study was reported that the Amerindian is the most prevalent ancestry in pediatric population of MC (148, 149). Until date, the reasons behind this relationship has not been established and further investigation is required for explaining the high incidence and mortality rates observed in Hispanic populations (150).
On the other hand, pediatric cases with ALL attended in public hospitals of MC consistently have displayed a higher frequency of the TCF3-PBX1 rearrangement (7.1–11.5%), in comparison to the reported in the worldwide literature in children with B-cell (5%) (26, 27). In the present study, this frequency was appreciably lower (2.5%) than previously reported. Our finding could be due to the fact that at the beginning of the study not all participating hospitals sent the leukemia patients' samples for analysis. This assumption is supported by a recent study of our research group where this gene rearrangement was found in 7.5% of ALL pediatric cases such as it has been previously reported (42). In addition, the prevalence of the other gene rearrangements that were analyzed in the present research were similar to the reported in MC and worldwide (1–3%) (42).
On the other hand, the highest ASIRm rates for the AL subtypes were predominantly concentrated among the municipalities of Venustiano Carranza, Iztacalco, Iztapalapa, and Benito Juárez. In particular, Venustiano Carranza showed higher rates of all AL subtypes compared to the other municipalities. Notably, the MC International Airport (AICM) is located in this municipality, which could increase children's exposure to air pollution. It has been suggested that exposure to pollution generated at airports is a possible environmental risk factor for AL development (151). However, further studies are required to determine if this factor contributes to the AL incidence considering that other population with high levels of air pollution did not show the highest incidence rates worldwide. Importantly, MC generally has highly harmful levels of air pollution (152–155) due to its geographic, climatic, and social conditions (49, 156). Prior studies have reported that living in an urban area or near an industrial zone (157–159) and being exposed to either vehicular traffic (160) or benzene derivatives (161, 162), are factors potentially contributing to the development of childhood AL (126, 163–166). On the other hand, we observed a relatively lower AL incidence rates in the municipalities located south and east of MC, such as Milpa Alta, Xochimilco, and Tláhuac, which are characterized by preserved areas of agricultural land production (60–62). Overall, the presently observed AL incidence rates are among the highest that have been reported in our country, and our findings highlight the predominance of this disease in the most urbanized municipalities. Notably, there remains controversy regarding international studies that have evaluated and compared the level of risk between urban and rural areas (159, 162, 167).
Another factor that must be considered is the role of ethnicity. In American countries, the highest AL incidence rates have been reported in children with an Amerindian (indigenous) ancestry (168). Quiroz et al. emphasized that mestizo countries, such as Mexico, Ecuador, and Colombia, had the highest pediatric AL incidence rates (40–57 cases per million) among the countries included. Conversely, to those American countries where the population was mainly from an European ancestry (e.g., the United States, Argentina, and Chile) exhibiting lower incidence rates (33–37) such as the reported for European populations (168). Notably, in Brazil, three zones have been identified: the zone with a greater indigenous presence exhibits the highest incidence rate (over 40), the zone with a larger European population presenting an intermediate incidence rate (~30), and the zone with a larger African ancestry population which have exhibited the lowest incidence for AL (20) (168, 169). The same phenomenon has been observed among White, Hispanic, and Afro-American populations from the United States (2, 7, 11, 79–81). This has also been reported in Mexico. For instance, in south Mexico, where the population is mostly of Amerindian (indigenous) ancestry, the incidence rates have been reported over the 70 cases per million, while in the north, where the population mainly has an European ancestry, the incidence rates (32) are similar to those reported in the White population in the United States (9, 170).
Notably, the geographical distribution of the ethnic groups and the socioeconomic status (SES) within populations is also relevant. In the present study the highest rates of AL were observed in municipalities located mainly at MC east (Venustiano Carranza, Iztacalco, and Iztapalapa), which are characterized by a low SES. Conversely, low incidence rates of AL were also observed in municipalities with a better SES (La Magdalena Contreras and Cuajimalpa de Morelos). SES cannot be separated from the ethnic composition, the lower the SES of a Mexican individual, the higher the probability to have an Amerindian ancestry (171). For instance, it has been reported in Mexico that the individuals with the darker skin colors also show significantly lower levels of education, lower remunerated jobs and higher probabilities of living in poverty conditions in comparison to people with lighter hues (172, 173).
One limitation of the present research was not to have included the children diagnosed and attended in private hospitals. Nonetheless, the main strength of the study is including nearly all cases of childhood leukemia and being able to include genetic data. Cases were recruited from public hospitals of MC in which an estimated 97.5% of children with leukemia who reside in MC are attended (64). Furthermore, the standardized incidence rates were obtained similarly to the previous report by our group during 2006–2007 in MC (3) considering characteristics such as the population, geography, health institutions and age groups. With respect to the previous study, in the present investigation we observed higher rates of ALL and AML. However, the APC results showed no trend for any AL subtype.
To our knowledge, this is the first article to actively study the incidence of childhood AL by using information from all public health institutions in MC during the research period of 2010–2017.
The incidence rate of childhood AL in MC continued to be among the highest in the world, at over 60 cases per million. Additionally, the results highlight the heterogeneous distributions of the incidence rates among different municipalities of MC. These data suggest possible roles of environmental, epigenetic, or lifestyle factors in AL development among Mexican children. It is important to conduct further research studies to examine the relationship between these factors and the risk of AL in these areas.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
JF-L, DD-R, JM-A, and JN-E: conceptualization. JF-L, DD-R, and JM-A: methodology. JF-L, DD-R, JM-A, and AA-L: formal analysis. JF-L and DD-R: investigation and writing—original draft preparation. EJ-H, JM-T, JP-G, AA-L, MP-S, AM-S, JT-N, KS-L, LF-V, RE-E, RA-S, MV-A, LM-P, NN-V, AG-Á, MC-M, MA-I, VB-M, RC-C, SJ-M, RR-L, HR-V, NL-S, AR-L, AH-M, EV, MM-R, OS-R, and JA-G: resources. JF-L, DD-R, JN-E, and JM-A: writing—review and editing, supervision, and funding acquisition. All authors reviewed the final manuscript, read, and approved the submitted version.
This work was supported by the Consejo Nacional de Ciencia y Tecnología [Grant Numbers: FORDECYT-PRONACES: 303019; CB 2015-1-258042-M; R-2020-785-022, FONCICYT/37/2018 and FIS/IMSS/PRIO/15/048], and Secretaría de Educación, Ciencia, Tecnología e Innovación (México) SECTEI/203/2019.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.918921/full#supplementary-material
1. Schüz J, Erdmann F. Environmental exposure and risk of childhood leukemia: an overview. Arch Med Res. (2016) 47:607–14. doi: 10.1016/j.arcmed.2016.11.017
2. Steliarova-Foucher E, Colombet M, Ries LAG, Moreno F, Dolya A, Bray F, et al. International incidence of childhood cancer, 2001–10: a population-based registry study. Lancet Oncol. (2017) 18:719–31. doi: 10.1016/S1470-2045(17)30186-9
3. Pérez-Saldivar ML, Fajardo-Gutiérrez A, Bernáldez-Ríos R, Martínez-Avalos A, Medina-Sanson A, Espinosa-Hernández L, et al. Childhood acute leukemias are frequent in Mexico City: descriptive epidemiology. BMC Cancer. (2011) 11:355. doi: 10.1186/1471-2407-11-355
4. Matasar MJ, Ritchie EK, Consedine N, Magai C, Neugut AI. Incidence rates of the major leukemia subtypes among US Hispanics, Blacks, and non-Hispanic Whites. Leuk Lymphoma. (2006) 47:2365–70. doi: 10.1080/10428190600799888
5. Monge P, Wesseling C, Rodríguez AC, Cantor KP, Weiderpass E, Reutfors J, et al. Childhood leukaemia in Costa Rica, 1981-96. Paediatr Perinat Epidemiol. (2002) 16:210–8. doi: 10.1046/j.1365-3016.2002.00422.x
6. Mejía-Aranguré JM, Fajardo-Gutiérrez A, Bernáldez-Ríos R, Farfán-Canto JM, Ortíz-Fernández A, Martínez-García MD. Incidence trends of acute leukemia among the children of Mexico City: 1982-1991. Arch Med Res. (1996) 27:223–7.
7. Giddings BM, Whitehead TP, Metayer C, Miller MD. Childhood leukemia incidence in California: high and rising in the Hispanic population. Cancer. (2016) 122:2867–75. doi: 10.1002/cncr.30129
8. Mejía-Aranguré JM, Bonilla M, Lorenzana R, Juárez-Ocaña S, de Reyes G, Pérez-Saldivar ML, et al. Incidence of leukemias in children from El Salvador and Mexico City between 1996 and 2000: population-based data. BMC Cancer. (2005) 5:33. doi: 10.1186/1471-2407-5-33
9. Fajardo-Gutiérrez A, Juárez-Ocaña S, González-Miranda G, Palma-Padilla V, Carreón-Cruz R, Ortega-Alvárez MC, et al. Incidence of cancer in children residing in ten jurisdictions of the Mexican Republic: importance of the Cancer registry (a population-based study). BMC Cancer. (2007) 7:68. doi: 10.1186/1471-2407-7-68
10. Fajardo-Gutiérrez A, González-Miranda G, Pachuca-Vázquez A, Allende-López A, Fajardo-Yamamoto LM, Rendón-Macías ME. Cancer incidence and mortality in children in the Mexican social security institute (1996-2013). Salud Publica Mex. (2016) 58:162–70. doi: 10.21149/spm.v58i2.7785
11. Barrington-Trimis JL, Cockburn M, Metayer C, Gauderman WJ, Wiemels J, et al. Trends in childhood leukemia incidence over two decades from 1992 to 2013. Int J Cancer. (2017) 140:1000–8. doi: 10.1002/ijc.30487
12. Feng Q, de Smith AJ, Vergara-Lluri M, Muskens IS, McKean-Cowdin R, Kogan S, et al. Trends in Acute Lymphoblastic Leukemia Incidence in the United States by Race/Ethnicity From 2000 to 2016. Am J Epidemiol. (2021) 190:519–27. doi: 10.1093/aje/kwaa215
13. Hubbard AK, Spector LG, Fortuna G, Marcotte EL, Poynter JN. Trends in international incidence of pediatric cancers in children under 5 years of age: 1988–2012. JNCI Cancer Spectr. (2019) 3:pkz007. doi: 10.1093/jncics/pkz007
14. Yi M, Zhou L, Li A, Luo S, Wu K. Global burden and trend of acute lymphoblastic leukemia from 1990 to 2017. Aging. (2020) 12:22869–91. doi: 10.18632/aging.103982
15. Bernaldez-Rios R, Ortega-Alvarez MC, Perez-Saldivar ML, Alatoma-Medina NE, Del Campo-Martinez M de LA, Rodriguez-Zepeda MDC, et al. The age incidence of childhood B-cell precursor acute lymphoblastic leukemia in Mexico City. J Pediatr Hematol Oncol. (2008) 30:199–203. doi: 10.1097/MPH.0b013e318162bcdc
16. Bathia S, Robison L. “Epidemiology of leukemia in childhood.,” In: Nathan D, Oski F, editors. Hematology of Infancy and Childhood. Philadelphia: Saunders (2003). p. 1081–100.
17. Kadan-Lottick NS, Ness KK, Bhatia S, Gurney JG. Survival variability by race and ethnicity in childhood acute lymphoblastic leukemia. JAMA. (2003) 290:2008–14. doi: 10.1001/jama.290.15.2008
18. Pui CH, Sandlund JT, Pei D, Rivera GK, Howard SC, Ribeiro RC, et al. Results of therapy for acute lymphoblastic leukemia in black and white children. J Am Med Assoc. (2003) 290:2001–7. doi: 10.1001/jama.290.15.2001
19. Yang W, Trevio LR, Yang JJ, Scheet P, Pui CH, Evans WE, et al. ARID5B SNP rs10821936 is associated with risk of childhood acute lymphoblastic leukemia in blacks and contributes to racial differences in leukemia incidence. Leukemia. (2010) 24:894–6. doi: 10.1038/leu.2009.277
20. Williams LA, Yang JJ, Hirsch BA, Marcotte EL, Spector LG. Is there etiologic heterogeneity between subtypes of childhood acute lymphoblastic leukemia? A review of variation in risk by subtype. Cancer Epidemiol Biomarkers Prev. (2019) 28:846–56. doi: 10.1158/1055-9965.EPI-18-0801
21. Pui C-H, Yang JJ, Hunger SP, Pieters R, Schrappe M, Biondi A, et al. Childhood acute lymphoblastic leukemia: progress through collaboration. J Clin Oncol. (2015) 33:2938–48. doi: 10.1200/JCO.2014.59.1636
22. Pizzo PA, Poplack DG. Principles Practice of Pediatric Oncology. Wolters Kluwer Health/Lippincott Williams Wilkins (2011). p. 1531. Available online at: https://books.google.co.in/books/about/Principles_and_Practice_of_Pediatric_Onc.html?id=ziPuQwAACAAJ&pgis=1 (accessed July 1, 2015).
23. Hunger SP, Mullighan CG. Acute lymphoblastic leukemia in children. N Engl J Med. (2015) 373:1541–52. doi: 10.1056/NEJMra1400972
24. Jiménez-Morales S, Miranda-Peralta E, Saldaña-Alvarez Y, Perez-Vera P, Paredes-Aguilera R, Rivera-Luna R, et al. BCR-ABL, ETV6-RUNX1 and E2A-PBX1: prevalence of the most common acute lymphoblastic leukemia fusion genes in Mexican patients. Leuk Res. (2008) 32:1518–22. doi: 10.1016/j.leukres.2008.03.021
25. Bekker-Méndez VC, Miranda-Peralta E, Núñez-Enríquez JC, Olarte-Carrillo I, Guerra-Castillo FX, Pompa-Mera EN, et al. Prevalence of gene rearrangements in Mexican children with acute lymphoblastic leukemia: a population study-report from the Mexican Interinstitutional Group for the identification of the causes of childhood leukemia. Biomed Res Int. (2014) 2014:8. doi: 10.1155/2014/210560
26. Pérez-Vera P, Salas C, Montero-Ruiz O, Frías S, Dehesa G, Jarquín B, et al. Analysis of gene rearrangements using a fluorescence in situ hybridization method in Mexican patients with acute lymphoblastic leukemia: experience at a single institution. Cancer Genet Cytogenet. (2008) 184:94–8. doi: 10.1016/j.cancergencyto.2008.04.003
27. Aldrich MC, Zhang L, Wiemels JL, Ma X, Loh ML, Metayer C, et al. Cytogenetics of Hispanic and White children with acute lymphoblastic leukemia in California. Cancer Epidemiol Biomarkers Prev. (2006) 15:578–81. doi: 10.1158/1055-9965.EPI-05-0833
28. Pui C-HH, Carroll WL, Meshinchi S, Arceci RJ. Biology, risk stratification, and therapy of pediatric acute leukemias: an update. J Clin Oncol. (2011) 29:551–65. doi: 10.1200/JCO.2010.30.7405
29. Malard F, Mohty M. Acute lymphoblastic leukaemia. Lancet. (2020) 395:1146–62. doi: 10.1016/S0140-6736(19)33018-1
30. Hein D, Borkhardt A, Fischer U. Insights into the prenatal origin of childhood acute lymphoblastic leukemia. Cancer Metastasis Rev. (2020) 39:161–71. doi: 10.1007/s10555-019-09841-1
31. Armstrong SA, Look AT. Molecular genetics of acute lymphoblastic leukemia. J Clin Oncol. (2005) 23:6306–15. doi: 10.1200/JCO.2005.05.047
32. Loh ML, Raetz E, Devidas M, Dai Y, Borowitz MJ, Carroll AJ, et al. Outcomes of children, adolescents, and young adults with acute lymphoblastic leukemia based on blast genotype at diagnosis: a report from the children's oncology group. Blood. (2016) 128:451–451. doi: 10.1182/blood.V128.22.451.451
33. Hunger SP, Loh ML, Whitlock JA, Winick NJ, Carroll WL, Devidas M, et al. Children's oncology Group's 2013 blueprint for research: acute lymphoblastic leukemia. Pediatr Blood Cancer. (2013) 60:957–63. doi: 10.1002/pbc.24420
34. Carroll WL. Race and outcome in childhood acute lymphoblastic leukemia. J Am Med Assoc. (2003) 290:2061–3. doi: 10.1001/jama.290.15.2061
35. Heerema NA, Sather HN, Ge J, Arthur DC, Hilden JM, Trigg ME, et al. Cytogenetic studies of infant acute lymphoblastic leukemia: poor prognosis of infants with t(4;11) - a report of the children's cancer group. Leukemia. (1999) 13:679–86. doi: 10.1038/sj.leu.2401413
36. El Chaer F, Keng M, Ballen KK. MLL-rearranged acute lymphoblastic leukemia. Curr Hematol Malig Rep. (2020) 15:83–9. doi: 10.1007/s11899-020-00582-5
37. Moorman AV, Ensor HM, Richards SM, Chilton L, Schwab C, Kinsey SE, et al. Prognostic effect of chromosomal abnormalities in childhood B-cell precursor acute lymphoblastic leukaemia: results from the UK medical research council ALL97/99 randomised trial. Lancet Oncol. (2010) 11:429–38. doi: 10.1016/S1470-2045(10)70066-8
38. Behm FG, Raimondi SC, Frestedt JL, Liu Q, Crist WM, Downing JR, et al. Rearrangement of the MLL gene confers a poor prognosis in childhood. Blood. (1996) 87:2870–7. doi: 10.1182/blood.V87.7.2870.bloodjournal8772870
39. Malouf C, Ottersbach K. Molecular processes involved in B cell acute lymphoblastic leukaemia. Cell Mol Life Sci. (2017) 75:1–30. doi: 10.1007/s00018-017-2620-z
40. Britten O, Ragusa D, Tosi S, Kamel YM. MLL-rearranged acute leukemia with t(4;11)(q21;q23)—current treatment options is there a role for CAR-T cell therapy? Cells. (2019) 8:1341. doi: 10.3390/cells8111341
41. Hunger SP, Mullighan CG. Redefining ALL classification: toward detecting high-risk ALL and implementing precision medicine. Blood. (2015) 125:3977–87. doi: 10.1182/blood-2015-02-580043
42. Mata-Rocha M, Rangel-López A, Jimenez-Hernandez E, Nuñez-Enríquez JC, Morales-Castillo BA, Sánchez-Escobar N, et al. Low prevalence of ETV6::RUNX1 fusion gene in a hispanic population. Front Pediatr. (2022) 0:637. doi: 10.3389/fped.2022.837656
43. Iacobucci I, Mullighan CG. Genetic basis of acute lymphoblastic leukemia. J Clin Oncol. (2017) 35:975–83. doi: 10.1200/JCO.2016.70.7836
44. Bunin GR. Nongenetic causes of childhood cancers: evidence from international variation, time trends, and risk factor studies. Toxicol Appl Pharmacol. (2004) 199:91–103. doi: 10.1016/j.taap.2003.12.028
45. Mejía-Aranguré JM, Fajardo-Gutiérrez A, Bernáldez-Ríos R, Paredes-Aguilera R, Flores-Aguilar H, Martínez-García MC. Incidencia de las leucemias agudas en niños de la ciudad de México, de 1982 a 1991. Salud Publica Mex. (2000) 42:431–7. doi: 10.1590/S0036-36342000000500009
46. Just AC, Wright RO, Schwartz J, Coull BA, Baccarelli AA, Tellez-Rojo MM, et al. Using High-resolution satellite aerosol optical depth to estimate daily pm25 geographical distribution in Mexico City. Environ Sci Technol. (2015) 49:8576–84. doi: 10.1021/acs.est.5b00859
47. Rivera-González LO, Zhang Z, Sánchez BN, Zhang K, Brown DG, Rojas-Bracho L, et al. An assessment of air pollutant exposure methods in Mexico City, Mexico. J Air Waste Manage Assoc. (2015) 65:581. doi: 10.1080/10962247.2015.1020974
48. Son Y, Osornio-Vargas ÁR, O'Neill MS, Hystad P, Texcalac-Sangrador JL, Ohman-Strickland P, et al. Land use regression models to assess air pollution exposure in Mexico City using finer spatial and temporal input parameters. Sci Total Environ. (2018) 639:40–8. doi: 10.1016/j.scitotenv.2018.05.144
49. Vega E, Namdeo A, Bramwell L, Miquelajauregui Y, Resendiz-Martinez CG, Jaimes-Palomera M, et al. Changes in air quality in Mexico City, London and Delhi in response to various stages and levels of lockdowns and easing of restrictions during COVID-19 pandemic. Environ Pollut. (2021) 285:117664. doi: 10.1016/j.envpol.2021.117664
50. Montoya CYO, López-Pérez AO, Monzalvo MU, Sánchez MLGR. Multidimensional urban exposure analysis of industrial chemical risk scenarios in mexican metropolitan areas. Int J Environ Res Public Heal. (2021) 18:5674. doi: 10.3390/ijerph18115674
51. Aguilera A, Bautista F, Gogichaichvili A, Gutiérrez-Ruiz ME, Ceniceros-Gómez AE, López-Santiago NR. Spatial distribution of manganese concentration and load in street dust in Mexico City. Salud Publica Mex. (2020) 62:147–55. doi: 10.21149/10577
52. Mostofsky E, Wilker EH, Schwartz J, Zanobetti A, Gold DR, Wellenius GA, et al. Short-term changes in ambient temperature and risk of ischemic stroke. Cerebrovasc Dis Extra. (2014) 4:9. doi: 10.1159/000357352
53. Phung D, Thai PK, Guo Y, Morawska L, Rutherford S, Chu C. Ambient temperature and risk of cardiovascular hospitalization: an updated systematic review and meta-analysis. Sci Total Environ. (2016) 550:1084–102. doi: 10.1016/j.scitotenv.2016.01.154
54. Rowland ST, Boehme AK, Rush J, Just AC, Kioumourtzoglou MA. Can ultra short-term changes in ambient temperature trigger myocardial infarction? Environ Int. (2020) 143:105910. doi: 10.1016/j.envint.2020.105910
55. Venter ZS, Brousse O, Esau I, Meier F. Hyperlocal mapping of urban air temperature using remote sensing and crowdsourced weather data. Remote Sens Environ. (2020) 242:111791. doi: 10.1016/j.rse.2020.111791
56. Romero-Lankao P, Qin H, Borbor-Cordova M. Exploration of health risks related to air pollution and temperature in three Latin American cities. Soc Sci Med. (2013) 83:110–8. doi: 10.1016/j.socscimed.2013.01.009
57. Gutiérrez-Avila I, Arfer KB, Wong S, Rush J, Kloog I, Just AC, et al. spatiotemporal reconstruction of daily ambient temperature using satellite data in the Megalopolis of Central Mexico from 2003 to 2019. Int J Climatol. (2021) 41:4095. doi: 10.1002/joc.7060
58. Congreso de los Estados Unidos Mexicanos. Ley Orgánica del Distrito y de los Territorios Federales (Reforma del 31 de diciembre de 1970). México (1970). Available online at: http://www.juridicas.unam.mx/publica/librev/rev/rap/cont/61/pr/pr23.pdf (accessed July 7, 2022).
59. Contreras Bustamante R. La Ciudad de México como Distrito Federal y entidad federativa. Mexico City: Porrúa (2001). p. 216–58.
60. Xochimilco CPC, Tláhuac Milpa, Alta,. Resumen del Plan Integral de Gestión del Polígono de Xochimilco, Tláhuac y Milpa Alta, inscrito en la lista del Patrimonio Mundial de la UNESCO. Ciudad de México (2006). p. 66. Available online at: http://arquitectura.unam.mx/uploads/8/1/1/0/8110907/plan_maestro_unesco_xochimilco.pdf (accessed February 3, 2021).
61. Sánchez C, Díaz-Polanco H. Pueblos, comunidades y ejidos en la dinámica ambiental de la Ciudad de México. Cuicuilco. (2011) 18:191–224.
62. Bonilla Rodríguez R. Agricultura y tenencia de la tierra en Milpa Alta. Un lugar de identidad. Argumentos Estud Críticos la Soc. (2009) 22:249–82.
63. Baca-López K, Fresno C, Espinal-Enríquez J, Flores-Merino MV, Camacho-López MA, Hernández-Lemus E. Metropolitan age-specific mortality trends at borough and neighborhood level: the case of Mexico City. PLoS ONE. (2021) 16:e0244384. doi: 10.1371/journal.pone.0244384
64. Fajardo-Gutiérrez A, Sandoval-Mex AM, Mejía-Aranguré JM, Rendón-Macías ME, Martínez-García M del C. Clinical and social factors that affect the time to diagnosis of Mexican children with cancer. Med Pediatr Oncol. (2002) 39:25–31. doi: 10.1002/mpo.10100
65. Kramárová E, Stiller C, Ferlay J, Parkin D, Draper G, Michaelis J, et al. International Classification of Childhood Cancer. In: Kramárová E, Stiller C, Ferlay J, Parkin D, Draper G, Michaelis J, Neglia J, Qureshi S, editors. Lyon: International Agency for Research on Cancer (1996). p. 48.
66. Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. (2016) 127:2391–405. doi: 10.1182/blood-2016-03-643544
67. Mata-Rocha M, Rangel-López A, Jiménez-Hernández E, Morales-Castillo BA, González-Torres C, Gaytan-Cervantes J, et al. Identification and characterization of novel fusion genes with potential clinical applications in Mexican children with acute lymphoblastic leukemia. Int J Mol Sci. (2019) 20:2394. doi: 10.3390/ijms20102394
68. INEGI. XII Censo General de Población y Vivienda 2000. Tabulados básicos. Distrito Federal (2000). Available online at: https://www.inegi.org.mx/programas/ccpv/2000/default.html#Tabulados (accessed December 7, 2020).
69. INEGI. XII Censo General de Población y Vivienda 2000. Tabulados básicos. México (2000). Available online at: https://www.inegi.org.mx/programas/ccpv/2000/default.html#Tabulados (accessed December 7, 2020).
70. INEGI. Tabulados, Distrito Federal, 2010. Censo Población y Vivienda 2010 Cuest básico. (2010). Available online at: www3.inegi.org.mx/sistemas/tabuladosbasicos/LeerArchivo.aspx?ct=29316&c=27302&s=est&f=1 (accessed December 7, 2020).
71. INEGI. Tabulados, México, 2010. Censo Población y Vivienda 2010 Cuest básico. (2010). Available online at: http://www3.inegi.org.mx/sistemas/tabuladosbasicos/default.aspx?c=27302&s=est (accessed December 7, 2020).
72. Mejía-Aranguré JM, Núñez-Enríquez JC, Fajardo-Gutiérrez A, Rodríguez-Zepeda MDC, Martín-Trejo JA, Duarte-Rodríguez DA, et al. Epidemiología descriptiva de la leucemia mieloide aguda (LMA) en niños residentes de la Ciudad de México: reporte del Grupo Mexicano Interinstitucional para la Identificación de las Causas de la Leucemia en Niños. Gac Med Mex. (2016) 152:66–77.
73. Torres-Degró A. Tasas de crecimiento poblacional (r): Una mirada desde el modelo matemático lineal, geométrico y exponencial. CIDE Digit. (2011) 2:142–160.
74. Segi M. Cancer Mortality for Selected Sites In 24 Countries [no. 1] (1950-1957). Sendai, Japan: Department of Public Health, Tohoku University, School of Medicine (1960).
75. Doll R, Payne P, Waterhouse J. Cancer Incidence in Five Continents. In: Doll R, Payne P, Waterhouse J, editors. Geneva, Switzerland: Springer (1966). p. 255.
76. Bidwell SS, Peterson CC, Demanelis K, Zarins KR, Meza R, Sriplung H, et al. Childhood cancer incidence and survival in Thailand: a comprehensive population-based registry analysis, 1990-2011. Pediatr Blood Cancer. (2019) 66:e27428. doi: 10.1002/pbc.27428
77. Demanelis K, Sriplung H, Meza R, Wiangnon S, Rozek LS, Scheurer ME, et al. Differences in childhood leukemia incidence and survival between Southern Thailand and the United States: a population-based analysis. Pediatr Blood Cancer. (2015) 62:1790–8. doi: 10.1002/pbc.25571
78. Services TD of SH. Texas Cancer Registry. SEER*Stat Database, 1995–2017 Incidence, Texas statewide. Child Adolesc Cancer. (2020) 1. https://www.dshs.state.tx.us/tcr/childhood.shtm (accessed December 16, 2020).
79. Chen X, Pan J, Wang S, Hong S, Hong S, He S. The epidemiological trend of acute myeloid leukemia in childhood: a population-based analysis. J Cancer. (2019) 10:4824–35. doi: 10.7150/jca.32326
80. Glazer ER, Perkins CI, Young JL, Schlag RD, Campleman SL, Wright WE. Cancer among Hispanic children in California, 1988-1994. Cancer. (1999) 86:1070–9.
81. Wilkinson JD, Fleming LE, MacKinnon J, Voti L, Wohler-Torres B, Peace S, et al. Lymphoma and lymphoid leukemia incidence in Florida children. Cancer. (2001) 91:1402–8. doi: 10.1002/1097-0142(20010401)91:7<1402::AID-CNCR1145>3.0.CO;2-6
82. Moore KJ, Hubbard AK, Williams LA, Spector LG. Childhood cancer incidence among specific Asian and Pacific Islander populations in the United States. Int J Cancer. (2020) 147:3339–48. doi: 10.1002/ijc.33153
83. Siegel DA, Henley SJ, Li J, Pollack LA, Van Dyne EA, White A. Rates and trends of pediatric acute lymphoblastic leukemia — United States, 2001–2014. MMWR Morb Mortal Wkly Rep. (2017) 66:950–4. doi: 10.15585/mmwr.mm6636a3
84. Karim-Kos HE, Hackl M, Mann G, Urban C, Woehrer A, Slavc I, et al. Trends in incidence, survival and mortality of childhood and adolescent cancer in Austria, 1994-2011. Cancer Epidemiol. (2016) 42:72–81. doi: 10.1016/j.canep.2016.03.015
85. Isaevska E, Manasievska M, Alessi D, Mosso ML, Magnani C, Sacerdote C, et al. Cancer incidence rates and trends among children and adolescents in Piedmont, 1967–2011. PLoS ONE. (2017) 12:e0181805. doi: 10.1371/journal.pone.0181805
86. Chen Q, Guo Z, Liu S, Quan P, Cao X, Guo L, et al. The cancer incidence and mortality among children and adolescents during the period of 2010-2014 in Henan Province, China. Cancer Med. (2019) 8:814–23. doi: 10.1002/cam4.1952
87. Erdmann F, Li T, Luta G, Giddings BM, Torres Alvarado G, Steliarova-Foucher E, et al. Incidence of childhood cancer in Costa Rica, 2000–2014: an international perspective. Cancer Epidemiol. (2018) 56:21–30. doi: 10.1016/j.canep.2018.07.004
88. de Oliveira MM, E Silva DRM, Ramos FR, Curado MP. Children and adolescents cancer incidence, mortality and survival a population-based study in Midwest of Brazil. Cancer Epidemiol. (2020) 68:101795. doi: 10.1016/j.canep.2020.101795
89. Bastos LNV, Silveira JC, Luna CF, Lucena-Silva N. Childhood and adolescent cancer in the state of pernambuco, Brazil: incidence, geographical distribution, and association with environmental health indicators. J Pediatr Hematol Oncol. (2018) 40:7–14. doi: 10.1097/MPH.0000000000001017
90. Youlden DR, Baade PD, Green AC, Valery PC, Moore AS, Aitken JF. The incidence of childhood cancer in Australia, 1983–2015, and projections to 2035. Med J Aust. (2020) 212:113–20. doi: 10.5694/mja2.50456
91. Baade PD, Youlden DR, Valery PC, Hassall T, Ward L, Green AC, et al. Trends in incidence of childhood cancer in Australia, 1983-2006. Br J Cancer. (2010) 102:620–6. doi: 10.1038/sj.bjc.6605503
92. Holland LR, Bradford NK, Youl P, Cossio D, Dunn N, Tran N, et al. Cancer incidence, mortality, and survival for children, adolescents, and young adults in Queensland between 1987 and 2016. J Adolesc Young Adult Oncol. (2020) 2:16. doi: 10.1089/jayao.2020.0151
93. Sommer G, Schindler M, Redmond S, Pfeiffer V, Konstantinoudis G, Ammann RA, et al. Temporal trends in incidence of childhood cancer in Switzerland, 1985–2014. Cancer Epidemiol. (2019) 61:157–64. doi: 10.1016/j.canep.2019.06.002
94. AIRTUM Working Group CCM AIEOP Working Group. I Tumori in Italia - Rapporto 2012 I tumori dei bambini e degli adolescenti. Epidemiol Prev. (2016) 40:1–24.
95. Jakab Z, Juhasz A, Nagy C, Schuler D, Garami M, Hungarian Paediatric Haemato-Oncology Network. Trends and territorial inequalities of incidence and survival of childhood leukaemia and their relations to socioeconomic status in Hungary, 1971-2015. Eur J Cancer Prev. (2017) 26:S183–90. doi: 10.1097/CEJ.0000000000000386
96. Krejci D, Zapletalova M, Svobodova I, Bajciova V, Mudry P, Smelhaus V, et al. Childhood cancer epidemiology in the Czech Republic (1994–2016). Cancer Epidemiol. (2020) 69:101848. doi: 10.1016/j.canep.2020.101848
97. Peris-Bonet R, Salmerón D, Martínez-Beneito MA, Galceran J, Marcos-Gragera R, Felipe S, et al. Childhood cancer incidence and survival in Spain. Ann Oncol. (2010) 21:iii103–10. doi: 10.1093/annonc/mdq092
98. Broccia G, Carter J, Ozsin-Ozler C, Meloni F, Pilia I, Satta G, et al. Haemolymphatic cancer among children in Sardinia, Italy: 1974-2003 incidence. BMJ Open. (2020) 10:37163. doi: 10.1136/bmjopen-2020-037163
99. González-García H, Garrote-Molpeceres R, Urbaneja-Rodríguez E, Gutiérrez-Meléndez P, Herráiz-Cristóbal R, Pino-Vázquez MA, et al. Differences in incidence and survival to childhood cancer between rural and urban areas in Castilla y León, Spain (2003–2014). Medicine. (2018) 97:e12797. doi: 10.1097/MD.0000000000012797
100. Paapsi K, Baburin A, Mikkel S, Mägi M, Saks K, Innos K. Childhood cancer incidence and survival trends in Estonia (1970-2016): a nationwide population-based study. BMC Cancer. (2020) 20:30. doi: 10.1186/s12885-019-6510-7
101. Reedijk AMJ, Kremer LC, Visser O, Lemmens V, Pieters R, Coebergh JWW, et al. Increasing incidence of cancer and stage migration towards advanced disease in children and young adolescents in the Netherlands, 1990–2017. Eur J Cancer. (2020) 134:115–26. doi: 10.1016/j.ejca.2020.04.011
102. Abood RA, Abdahmed KA, Mazyed SS. Epidemiology of different types of cancers reported in Basra, Iraq. Sultan Qaboos Univ Med J. (2020) 20:295–300. doi: 10.18295/squmj.2020.20.03.008
103. Akhtar S, Al-Abkal J, Al-Shammari A. Childhood leukaemia incidence and trends in a Middle Eastern country during 1980–2014: a population-based study. Cancer Causes Control. (2020) 31:231–40. doi: 10.1007/s10552-020-01267-3
104. Al-Asadi JN, Ibrahim SJ. Childhood cancer in Basrah, Iraq during 2012-2016: incidence and mortality. Asian Pacific J Cancer Prev. (2018) 19:2337–241. doi: 10.22034/APJCP.2018.19.8.2337
105. Belgaumi AF, Pathan GQ, Siddiqui K, Ali AA, Al-Fawaz I, Al-Sweedan S, et al. Incidence, clinical distribution, and patient characteristics of childhood cancer in Saudi Arabia: a population-based analysis. Pediatr Blood Cancer. (2019) 66:e27684. doi: 10.1002/pbc.27684
106. Jastaniah W, Essa MF, Ballourah W, Abosoudah I, Al Daama S, Algiraigri AH, et al. Incidence trends of childhood acute lymphoblastic leukemia in Saudi Arabia: Increasing incidence or competing risks? Cancer Epidemiol. (2020) 67:101764. doi: 10.1016/j.canep.2020.101764
107. Rahimi Pordanjani S, Kavousi A, Mirbagheri B, Shahsavani A, Etemad K. Temporal trend and spatial distribution of acute lymphoblastic leukemia in Iranian children during 2006-2014: a mixed ecological study. Epidemiol Health. (2020) 42:e2020057. doi: 10.4178/epih.e2020057
108. Shabani M, Saeedi Moghaddam S, Ataeinia B, Rezaei N, Mohebi F, Mohajer B, et al. Trends of national and subnational incidence of childhood cancer groups in Iran: 1990–2016. Front Oncol. (2020) 9:1428. doi: 10.3389/fonc.2019.01428
109. Wiangnon S, Jetsrisuparb A, Komvilaisak P, Suwanrungruang K. Childhood cancer incidence and survival 1985-2009, Khon Kaen, Thailand. Asian Pacific J Cancer Prev. (2014) 15:7989–93. doi: 10.7314/APJCP.2014.15.18.7989
110. Otoo MN, Lubbe MS, Steyn H, Burger JR. Childhood cancers in a section of the South African private health sector: Analysis of medicines claims data. Heal SA Gesondheid. (2020) 25:a1382. doi: 10.4102/hsag.v25i0.1382
111. Stefan C, Bray F, Ferlay J, Liu B, Parkin DM. Cancer of childhood in sub-Saharan Africa. Ecancermedicalscience. (2017) 11:755. doi: 10.3332/ecancer.2017.755
112. Cristina Stefan D. Patterns of distribution of childhood cancer in Africa. J Trop Pediatr. (2015) 61:165–73. doi: 10.1093/tropej/fmv005
113. Moreno F, Loria D, Abriata G, Terracini B. Childhood cancer: incidence and early deaths in Argentina, 2000-2008. Eur J Cancer. (2013) 49:465–73. doi: 10.1016/j.ejca.2012.08.001
114. Oliveira Friestino JK, Mendonça D, Oliveira P, Oliveira CM, Moreira Filho D de C. Cáncer infantil: incidencia y patrones espaciales en la ciudad de Campinas, Brasil, 1996-2005. Salud Colect. (2018) 14:51–63. doi: 10.18294/sc.2018.1200
115. Wang L, Gomez SL, Yasui Y. Racial and ethnic differences in socioeconomic position and risk of childhood acute lymphoblastic leukemia. Am J Epidemiol. (2017) 185:1263–71. doi: 10.1093/aje/kww164
116. Altekruse S, Kosary C, Krapcho M, Neyman N, Aminou R, Waldron W, et al. SEER Cancer Statistics Review, 1975-2012. (2010). Available online at: http://seer.cancer.gov/csr/1975_2007/ (accessed September 27, 2021).
117. Howlader N, Noone, A, Krapcho, M, Garshell, J, Miller, D, Altekruse, S . SEER Cancer Statistics Review, 1975-2012, National Cancer Institute. Bethesda, MD (2015). p. 1. Available online at: https://seer.cancer.gov/archive/csr/1975_2012/ (accessed September 27, 2021).
118. Zhao Y, Wang Y, Ma S. Racial Differences in four leukemia subtypes: comprehensive descriptive epidemiology. Sci Rep. (2018) 8:1–10. doi: 10.1038/s41598-017-19081-4
119. Feng Q, de Smith AJ, Vergara-Lluri M, Muskens IS, McKean-Cowdin R, Kogan S, et al. Trends in acute lymphoblastic leukemia incidence in the us from 2000-2016: an increased risk in latinos across all age groups. Am J Epidemiol. (2020) 190:519–527. doi: 10.1158/1538-7755.DISP19-A105
120. Glazer ER, Perkins CI, Young JL, Schlag RD, Campleman SL, Wright WE. Cancer among Hispanic children in California, 1988-1994: comparison with non-Hispanic white children. Cancer. (1999) 86:1070–9.
121. Puumala SE, Ross JA, Aplenc R, Spector LG. Epidemiology of childhood acute myeloid leukemia. Pediatr Blood Cancer. (2013) 60:728–33. doi: 10.1002/pbc.24464
122. de Rooij J, Zwaan C, van den Heuvel-Eibrink M. Pediatric AM. From biology to clinical management. J Clin Med. (2015) 4:127–49. doi: 10.3390/jcm4010127
123. Panagopoulou P, Skalkidou A, Marcotte E, Erdmann F, Ma X, Heck JE, et al. Parental age and the risk of childhood acute myeloid leukemia: results from the Childhood Leukemia International Consortium. Cancer Epidemiol. (2019) 59:158–65. doi: 10.1016/j.canep.2019.01.022
124. Adam M, Kuehni CE, Spoerri A, Schmidlin K, Gumy-Pause F, Brazzola P, et al. Socioeconomic status and childhood leukemia incidence in Switzerland. Front Oncol. (2015) 5:139. doi: 10.3389/fonc.2015.00139
125. Scélo G, Metayer C, Zhang L, Wiemels JL, Aldrich MC, Selvin S, et al. Household exposure to paint and petroleum solvents, chromosomal translocations, and the risk of childhood leukemia. Environ Health Perspect. (2009) 117:133–9. doi: 10.1289/ehp.11927
126. Raaschou-Nielsen O, Hvidtfeldt UA, Roswall N, Hertel O, Poulsen AH, Sørensen M. Ambient benzene at the residence and risk for subtypes of childhood leukemia, lymphoma and CNS tumor. Int J Cancer. (2018) 143:1367–73. doi: 10.1002/ijc.31421
127. Bailey HD, Fritschi L, Infante-Rivard C, Glass DC, Miligi L, Dockerty JD, et al. Parental occupational pesticide exposure and the risk of childhood leukemia in the offspring: Findings from the childhood leukemia international consortium. Int J Cancer. (2014) 135:2157–72. doi: 10.1002/ijc.28854
128. Metayer C, Milne E, Dockerty JD, Clavel J, Pombo-De-Oliveira MS, Wesseling C, et al. Maternal supplementation with folic acid and other vitamins and risk of leukemia in offspring: a childhood leukemia internotionol consortium study. Epidemiology. (2014) 25:811–22. doi: 10.1097/EDE.0000000000000141
129. Oksuzyan S, Crespi CM, Cockburn M, Mezei G, Kheifets L. Birth weight and other perinatal characteristics and childhood leukemia in California. Cancer Epidemiol. (2012) 36:e359–65. doi: 10.1016/j.canep.2012.08.002
130. Wang Y-F, Wu L-Q, Liu Y-N, Bi Y-Y, Wang H. Gestational age and childhood leukemia: a meta-analysis of epidemiologic studies. Hematology. (2018) 23:253–62. doi: 10.1080/10245332.2017.1396056
131. Marcotte EL, Thomopoulos TP, Infante-Rivard C, Clavel J, Petridou ET, Schüz J, et al. Caesarean delivery and risk of childhood leukaemia: a pooled analysis from the Childhood Leukemia International Consortium (CLIC). Lancet Haematol. (2016) 3:e176–85. doi: 10.1016/S2352-3026(16)00002-8
132. Ariffin H, Chen S-P, Kwok CS, Quah T-C, Lin H-P, Yeoh AEJ. Ethnic differences in the frequency of subtypes of childhood acute lymphoblastic leukemia: results of the malaysia-singapore leukemia study group. J Pediatr Hematol Oncol. (2007) 29:27–31. doi: 10.1097/MPH.0b013e318030ac4c
133. Moreno Lorenzana D, Juárez Velázquez MDR, Reyes León A, Martínez Anaya D, Hernández Monterde A, Salas Labadía C, et al. CRLF2 and IKZF1 abnormalities in Mexican children with acute lymphoblastic leukemia and recurrent gene fusions: exploring surrogate markers of signaling pathways. J Pathol Clin Res. (2021) 7:410–21. doi: 10.1002/cjp2.211
134. Harvey RC, Mullighan CG, Chen I-M, Wharton W, Mikhail FM, Carroll AJ, et al. Rearrangement of CRLF2 is associated with mutation of JAK kinases, alteration of IKZF1, Hispanic/Latino ethnicity, and a poor outcome in pediatric B-progenitor acute lymphoblastic leukemia. Blood. (2010) 115:5312–21. doi: 10.1182/blood-2009-09-245944
135. Ge Z, Han Q, Gu Y, Ge Q, Ma J, Sloane J, et al. Aberrant ARID5B expression and its association with Ikaros dysfunction in acute lymphoblastic leukemia. Oncogenesis. (2018) 7:1–10. doi: 10.1038/s41389-018-0095-x
136. Kreile M, Rots D, Zarina A, Rautiainen L, Visnevska-Preciniece Z, Kovalova Z, et al. Association of ARID5B genetic variants with risk of childhood B cell precursor acute lymphoblastic leukaemia in Latvia. Asian Pacific J Cancer Prev. (2018) 19:91–5. doi: 10.22034/APJCP.2018.19.1.91
137. Bekker-Méndez VC, Núñez-Enríquez JC, Torres Escalante JL, Alvarez-Olmos E, González-Montalvoc PM, Jiménez-Hernández E, et al. ARID5B, CEBPE and PIP4K2A germline genetic polymorphisms and risk of childhood acute lymphoblastic leukemia in mexican patients: a MIGICCL study. Arch Med Res. (2016) 47:623–8. doi: 10.1016/j.arcmed.2016.12.003
138. Reyes-León A, Ramírez-Martínez M, Fernández-García D, Amaro-Muñoz D, Velázquez-Aragón JA, et al. Variants in ARID5B gene are associated with the development of acute lymphoblastic leukemia in Mexican children. Ann Hematol. (2019) 98:2379–88. doi: 10.1007/s00277-019-03730-x
139. Jaime-Pérez JC, de los Santos JAH, Gómez-Almaguer D. Childhood T-cell acute lymphoblastic leukemia in a single Latin American center: impact of improved treatment scheme and support therapy on survival. Hematol Transfus Cell Ther. (2020) 42:320–5. doi: 10.1016/j.htct.2019.09.005
140. Pui CH. Acute lymphoblastic leukemia. Pediatr Clin North Am. (1997) 44:831–46. doi: 10.1016/S0031-3955(05)70532-0
141. Karrman K, Johansson B. Pediatric T-cell acute lymphoblastic leukemia. Genes Chromosom Cancer. (2017) 56:89–116. doi: 10.1002/gcc.22416
142. Marsán Suárez V, Macías Abraham C, Jiménez Rivero R, Sánchez Segura M, Socarrás Ferrer B, Gramatges Ortiz A, et al. Inmunofenotipaje y supervivencia global de pacientes pediátricos con leucemias agudas. Rev Cuba Hematol Inmunol Hemoter. (2002).
143. Paes CA, Viana MB, Freire RV, Martins-Filho OA, Taboada DC, Rocha VG. Direct association of socio-economic status with T-cell acute lymphoblastic leukaemia in children. Leuk Res. (2003) 27:789–94. doi: 10.1016/S0145-2126(03)00010-9
144. Tang J, Yu J, Cai J, Zhang L, Hu S, Gao J, et al. Prognostic factors for CNS control in children with acute lymphoblastic leukemia treated without cranial irradiation. Blood. (2021) 138:331–43. doi: 10.1182/blood.2020010438
145. Greaves MF, Colman SM, Beard ME, Bradstock K, Cabrera ME, Chen PM, et al. Geographical distribution of acute lymphoblastic leukaemia subtypes: second report of the collaborative group study. Leukemia. (1993) 7:27–34.
146. Schmiegelow K, Vestergaard T, Nielsen SM, Hjalgrim H. Etiology of common childhood acute lymphoblastic leukemia: the adrenal hypothesis. Leukemia. (2008) 22:2137–41. doi: 10.1038/leu.2008.212
147. Carranza C, Granados L, Morales O, Jo W, Villagran S, Tinti D, et al. Frequency of the ETV6-RUNX1, BCR-ABL1, TCF3-PBX1, and MLL-AFF1 fusion genes in Guatemalan pediatric acute lymphoblastic leukemia patients and their ethnic associations. Cancer Genet. (2013) 206:227–32. doi: 10.1016/j.cancergen.2013.05.017
148. Lee SHR, Antillon-Klussmann F, Pei D, Yang W, Roberts KG, Li Z, et al. Association of genetic ancestry with the molecular subtypes and prognosis of childhood acute lymphoblastic leukemia. JAMA Oncol. (2022) 8:354–63. doi: 10.1001/jamaoncol.2021.6826
149. Medina-Sanson A, Núñez-Enríquez JC, Hurtado-Cordova E, Pérez-Saldivar ML, Martínez-García A, Jiménez-Hernández E, et al. Genotype-environment interaction analysis of NQO1, CYP2E1, and NAT2 polymorphisms and the risk of childhood acute lymphoblastic leukemia: a report from the mexican interinstitutional group for the identification of the causes of childhood leukemia. Front Oncol. (2020) 10:1841. doi: 10.3389/fonc.2020.571869
150. Malvezzi M, Santucci C, Alicandro G, Carioli G, Boffetta P, Ribeiro KB, et al. Childhood cancer mortality trends in the Americas and Australasia: an update to 2017. Cancer. (2021) 127:3445–56. doi: 10.1002/cncr.33642
151. Senkayi SN, Sattler ML, Rowe N, Chen VCP. Investigation of an association between childhood leukemia incidences and airports in Texas. Atmos Pollut Res. (2014) 5:189–95. doi: 10.5094/APR.2014.023
152. Catalán-Vázquez M, Riojas-Rodríguez H, Jarillo-Soto EC, Delgadillo-Gutiérrez HJ. Percepción de riesgo a la salud por contaminación del aire en adolescentes de la Ciudad de México. Salud Publica Mex. (2009) 51:148–56. doi: 10.1590/S0036-36342009000200011
153. Hernández-Garduño E, Pérez-Neria J, Paccagnella AM, Piña-García MA, Munguía-Castro M, Catalán-Vázquez M, et al. Air pollution and respiratory health in Mexico City. J Occup Environ Med. (1997) 39:299–307. doi: 10.1097/00043764-199704000-00006
154. Sánchez-Carrillo CI, Cerón-Mireles P, Rojas-Martínez MR, Mendoza-Alvarado L, Olaiz-Fernández G, et al. Surveillance of acute health effects of air pollution in Mexico City. Epidemiology. (2003) 14:536–44. doi: 10.1097/01.ede.0000081801.90352.bf
155. Schifter I, Díaz L, López-Salinas E. Hazardous air pollutants from mobile sources in the metropolitan area of Mexico City. J Air Waste Manag Assoc. (2005) 55:1289–97. doi: 10.1080/10473289.2005.10464735
156. Vallejo M, Jáuregui-Renaud K, Hermosillo AG, Márquez MF, Cárdenas M. Efectos de la contaminación atmosférica en la salud y su importancia en la ciudad de México. Gac Med Mex. (2003) 139:57–63.
157. Iavarone I, Buzzoni C, Stoppa G, Steliarova-Foucher E. Cancer incidence in children and young adults living in industrially contaminated sites: from the Italian experience to the development of an international surveillance system. Epidemiol Prev. (2018) 42:76–85. doi: 10.19191/EP18.5-6.S1.P076.090
158. Rodriguez-Villamizar LA, Moreno-Corzo FE, Valbuena-Garcia AM, Uribe Pérez CJ, Brome Bohórquez MR, García García HI, et al. Childhood leukemia in small geographical areas and proximity to industrial sources of air pollutants in three colombian cities. Int J Environ Res Public Health. (2020) 17:7925. doi: 10.3390/ijerph17217925
159. García-Pérez J, López-Abente G, Gómez-Barroso D, Morales-Piga A, Pardo Romaguera E, Tamayo I, et al. Childhood leukemia and residential proximity to industrial and urban sites. Environ Res. (2015) 140:542–53. doi: 10.1016/j.envres.2015.05.014
160. Tamayo-Uria I, Boldo E, García-Pérez J, Gómez-Barroso D, Romaguera EP, Cirach M, et al. Childhood leukaemia risk and residential proximity to busy roads. Environ Int. (2018) 121:332–9. doi: 10.1016/j.envint.2018.08.056
161. Raaschou-Nielsen O, Reynolds P. Air pollution and childhood cancer: a review of the epidemiological literature. Int J Cancer. (2006) 118:2920–9. doi: 10.1002/ijc.21787
162. Carbonari D, Chiarella P, Mansi A, Pigini D, Iavicoli S, Tranfo G. Biomarkers of susceptibility following benzene exposure: influence of genetic polymorphisms on benzene metabolism and health effects. Biomark Med. (2016) 10:145–63. doi: 10.2217/bmm.15.106
163. García-Pérez J, Gómez-Barroso D, Tamayo-Uria I, Ramis R. Methodological approaches to the study of cancer risk in the vicinity of pollution sources: the experience of a population-based case-control study of childhood cancer. Int J Health Geogr. (2019) 18:12. doi: 10.1186/s12942-019-0176-x
164. Nelson L, Valle J, King G, Mills PK, Richardson MJ, Roberts EM, et al. Estimating the proportion of childhood cancer cases and costs attributable to the environment in California. Am J Public Health. (2017) 107:756–62. doi: 10.2105/AJPH.2017.303690
165. Filippini T, Heck JE, Malagoli C, Del Giovane C, Vinceti M. A review and meta-analysis of outdoor air pollution and risk of childhood leukemia. J Environ Sci Heal. (2015) 33:36–66. doi: 10.1080/10590501.2015.1002999
166. Ribeiro AG, Vermeulen R, Cardoso MRA, Latorre MDRDO, Hystad P, Downward GS, et al. Residential traffic exposure and lymphohematopoietic malignancies among children in the city of São Paulo, Brazil: An ecological stud. Cancer Epidemiol. (2021) 70:101859. doi: 10.1016/j.canep.2020.101859
167. Siegel DA, Li J, Henley SJ, Wilson RJ, Lunsford NB, Tai E, Van Dyne EA. Geographic variation in pediatric cancer incidence — United States, 2003–2014. MMWR Morb Mortal Wkly Rep. (2018) 67:707–13. doi: 10.15585/mmwr.mm6725a2
168. Quiroz E, Aldoss I, Pullarkat V, Rego E, Marcucci G, Douer D. The emerging story of acute lymphoblastic leukemia among the Latin American population – biological and clinical implications. Blood Rev. (2019) 33:98–105. doi: 10.1016/j.blre.2018.08.002
169. de Souza Reis R, de Camargo B, de Oliveira Santos M, de Oliveira JM, Azevedo Silva F, Pombo-De-Oliveira MS. Childhood leukemia incidence in Brazil according to different geographical regions. Pediatr Blood Cancer. (2011) 56:58–64. doi: 10.1002/pbc.22736
170. Silva-Zolezzi I, Hidalgo-Miranda A, Estrada-Gil J, Fernandez-Lopez JC, Uribe-Figueroa L, Contreras A, et al. Analysis of genomic diversity in Mexican Mestizo populations to develop genomic medicine in Mexico. Proc Natl Acad Sci U S A. (2009) 106:8611–6. doi: 10.1073/pnas.0903045106
171. Pérez Velasco Pavón JC. Economic behavior of indigenous peoples: the Mexican case. Lat Am Econ Rev. (2014) 23:1–58. doi: 10.1007/s40503-014-0012-4
172. Villarreal A. Stratification by skin color in contemporary mexico on JSTOR. Am Sociol Rev. (2010) 75:652–78. doi: 10.1177/0003122410378232
Keywords: incidence, childhood, acute leukemia, acute lymphoblastic leukemia, acute myeloblastic leukemia, Mexican population, epidemiology
Citation: Flores-Lujano J, Duarte-Rodríguez DA, Jiménez-Hernández E, Martín-Trejo JA, Allende-López A, Peñaloza-González JG, Pérez-Saldivar ML, Medina-Sanson A, Torres-Nava JR, Solís-Labastida KA, Flores-Villegas LV, Espinosa-Elizondo RM, Amador-Sánchez R, Velázquez-Aviña MM, Merino-Pasaye LE, Núñez-Villegas NN, González-Ávila AI, del Campo-Martínez Mdl, Alvarado-Ibarra M, Bekker-Méndez VC, Cárdenas-Cardos R, Jiménez-Morales S, Rivera-Luna R, Rosas-Vargas H, López-Santiago NC, Rangel-López A, Hidalgo-Miranda A, Vega E, Mata-Rocha M, Sepúlveda-Robles OA, Arellano-Galindo J, Núñez-Enríquez JC and Mejía-Aranguré JM (2022) Persistently high incidence rates of childhood acute leukemias from 2010 to 2017 in Mexico City: A population study from the MIGICCL. Front. Public Health 10:918921. doi: 10.3389/fpubh.2022.918921
Received: 12 April 2022; Accepted: 09 August 2022;
Published: 14 September 2022.
Edited by:
Dora Il'yasova, Duke University, United StatesReviewed by:
Keiu Paapsi, National Institute for Health Development, EstoniaCopyright © 2022 Flores-Lujano, Duarte-Rodríguez, Jiménez-Hernández, Martín-Trejo, Allende-López, Peñaloza-González, Pérez-Saldivar, Medina-Sanson, Torres-Nava, Solís-Labastida, Flores-Villegas, Espinosa-Elizondo, Amador-Sánchez, Velázquez-Aviña, Merino-Pasaye, Núñez-Villegas, González-Ávila, del Campo-Martínez, Alvarado-Ibarra, Bekker-Méndez, Cárdenas-Cardos, Jiménez-Morales, Rivera-Luna, Rosas-Vargas, López-Santiago, Rangel-López, Hidalgo-Miranda, Vega, Mata-Rocha, Sepúlveda-Robles, Arellano-Galindo, Núñez-Enríquez and Mejía-Aranguré. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Manuel Mejía-Aranguré, am1lamlhQGlubWVnZW4uZ29iLm14; Juan Carlos Núñez-Enríquez, amNhcmxvc19udUBob3RtYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.