 Marguerite d'Ussel
Marguerite d'Ussel Frédéric Adam2
Frédéric Adam2 François Philippart
François Philippart- 1Chronic Pain Unit, Groupe Hospitalier Paris Saint-Joseph, Paris, France
- 2Department of Anesthesia, Groupe Hospitalier Paris Saint-Joseph, Paris, France
- 3Clinical Research Department, Groupe Hospitalier Paris Saint-Joseph, Paris, France
- 4Université Paris Cité, Paris, France
- 5Department of Intensive Care Medicine and Reanimation, Groupe Hospitalier Paris Saint-Joseph, Paris, France
Introduction: The COVID-19 pandemic has posed an unprecedented challenge worldwide for healthcare workers (HCWs) and other hospital employees. Disruptions in work and personal life may have led to mental health problems. To prevent or limit the severity of such issues, a local initiative has been implemented in a French hospital: a dedicated lounge, also called “Bulle” (literally bubble and meaning safe space) has been created to provide a quiet caring environment and health support. Other similar wellbeing centers have been implemented in other countries, but very little data are available on their practical effectiveness. The purpose of our study was to assess what type of hospital workers have frequented the Bulle and to describe their psychological state in terms of anxiety, depression, and post-traumatic stress disorder (PTSD) just after the first wave, compared to those who had not come to the Bulle.
Methods: From 15 July to 1 October 2020, a cross-sectional survey was conducted among all workers, collecting demographic information, professional data (experience and satisfaction), emotional experience during the first wave of COVID-19, and psychological specificities, including a history of burnout or symptoms of anxiety, depression, and PTSD. We asked them if they had accessed the Bulle or not.
Results: A total of 675 employees (out of 2,408; 28.0%) fully completed the survey. Approximately 199 respondents (29%) reported having accessed the Bulle during the first wave of the pandemic. Significant symptoms of anxiety, depression, and PTSD were reported by, respectively, 41, 20, and 14% of the participants. Logistic regression analysis showed no relationship between the use of the Bulle and the prevalence of later psychological symptoms. However, employees who benefit from the solicitation of the psychological support team in their hospital unit were secondarily more prone to come to the Bulle [odds ratio (OR), 2.24; 95% confidence interval (95% CI): 1.09; 4.59].
Conclusion: Anxiety, depression, and PTSD were common after the first part of the COVID-19 pandemic, and the attendance in quiet and wellbeing spaces seemed easier with direct internal proactive intervention by psychological teams.
Introduction
There has been widespread emotional distress caused by the COVID-19 pandemic. Early events associated with this new and highly infectious virus were a source of anxiety for populations worldwide (1–5). This anxiety could have been explained by the fear of an unknown life-threatening viral pneumonia, the absence of treatment, and confusing information from physicians, scientists, and politicians about sanitary measures, the relevance of lockdown, and the risk of professional and social interactions (6–12). All these changes in daily life and people's increased isolation from normal social interaction and family relationships may have had a psychological impact and led to post-traumatic stress disorder (PTSD) (6, 13).
In addition to the stress factors of the general population, frontline healthcare workers (HCWs) had to face many other specific issues. The excessive number of confirmed and suspected cases, the overwhelming workload, the lack of personal protection equipment, the widespread media coverage, the depletion of specific drugs, and the feeling of being inadequately supported all may have contributed to the mental burden of these HCWs. These lifestyle changes significantly impacted their routine, specifically in terms of job responsibility and social isolation, and notably affected their psychological health and stress levels (14–18). This impacted all HCWs: doctors, nurses, and other medical personnel in contact with suspected or confirmed COVID-19 cases, but also pharmacists, hospital support staff, laboratory technicians, admission/ward clerks, and all hospital workers. The latter HCWs may not have been directly involved in providing assessment or treatment, but may have operated in similarly stressful clinical settings, and were at heightened risk of being infected. The pandemic and all its difficult outcomes have led to a higher risk of anxiety, depression, burnout, and more generally emotional distress among hospital staff (7, 11, 16, 17, 19).
The COVID-19 pandemic has generated an increased sense of urgency to mobilize crisis response provisions to protect the wellbeing of hospital workers. Some hospital trusts have engaged teams to rapidly create respite spaces for staff (20, 21), albeit the same concept has been labeled in many ways: “bubble rooms,” “wobble rooms,” “time-out rooms,” “chill-out rooms,” “safe rooms,” “rainbow rooms,” and “wellbeing centers” (14, 22–25). These facilities are usually located in non-COVID areas and, for frontline workers, provide an opportunity for staff to remove themselves from the clinical environment and gain solace from the pressures of dealing with coronavirus. They are intended to provide an optimistic and positive atmosphere to help staff with the impact of the crisis: small enough to be perceived as “homely” spaces but large enough to maintain privacy and appropriate social distancing (22). Depending on the country or the hospitals, they could be set differently, indoors and/or outdoors, with a garden view (23). The lounges could offer music, refreshments (22, 23), various activities, such as relaxing sessions, physiotherapist interventions (23, 24), or even immersive experiences (25), and learning packages (22). Psychological support could also be provided directly by specialists (23) or suggested by “buddies” helping staff (22). In addition to physical lounges, some teams also provided virtual spaces for HCWs, providing regular online group-based support focused on honest expression of feelings and self-care (26).
Despite the large number of spontaneous interventions to improve the resilience of HCWs during this psychologically distressing time, very little data are available about the use of these wellbeing centers (24). A recent review has shown that only a few countries have published specific psychological support intervention protocols for HCWs. Given the heterogeneity of protocols and the clinical outcomes studied, it is also impossible to determine whether one protocol has better outcomes than the others. The authors of the review conclude that further research is needed to find out the best ways to support the resilience and mental wellbeing of HCWs (27).
In our French hospital, we have also implemented a wellbeing center that we call Bulle (literally bubble, meaning safe space). The purpose of our study was to assess what type of hospital workers have frequented the Bulle and to describe their psychological state in terms of anxiety, depression, and PTSD, just after the first wave, compared to those who had not come to the Bulle. This study can help us to improve our Bulle to attract the most fragile hospital staff and mitigate the psychological impact of the COVID-19 crisis or other difficulties on each of them.
Context
Hospital Structure
The Groupe Hospitalier Saint-Joseph (GHSJ) is a two-site hospital organization (Saint-Joseph and Marie Lannelongue) located in the Great Paris area. During the first wave of the COVID-19 pandemic (between 1 March and 29 May 2020) 1,177 patients had been seen via the emergency ward, 834 were hospitalized, 132 needed intensive care, and 100 died.
Our Bulle Concept
We implemented the Bulle in the early stage of the first wave on 27 March 2020 to support the resilience and mental health of frontline workers by providing targeted and individualized interventions in an adapted environment. The Bulle was designed to favor relaxation and coping against stress, to strengthen camaraderie and support and also to provide professional healthcare. The concept was born out of a medical team working to support self-management in people with chronic pain. This multidisciplinary team served to propose an integrative approach for these patients, to improve their quality of life, and alleviate the emotional difficulties related to their pain. This medical approach is currently recognized in the field of chronic diseases (28, 29), and in particular in oncological support care (28–30). It quickly appeared logical to replicate this approach to the care of the medical and non-medical staff, especially as the healthcare professionals of the team could no longer receive their patients in the hospital, which was only dedicated to COVID-19 infected or emergency patients. To encourage as many staff as possible to come and take care of themselves, we designed the Bulle as a place of resources, quietness, and friendship, as it had been implemented in Toronto during the SARS outbreak (31). Open with free access to all hospital workers from 11.30 am to 8 pm, every day, including public holidays except on weekends, our lounge was managed by health professionals working in our institution. We built the Bulle as a soothing space (comfortable seating, relaxing music, low-level lighting, plants, an aromatherapy pod, etc.), welcoming and friendly with hot or cold drinks and regressive sweets. From the outset, the Bulle has let available self-massage chairs, musical relaxation sessions with the “Music Care” digital tablets (32), micro-nap areas, or creative workshops. Online appointments were also opened for physiotherapy, osteopathic manual therapy to treat or limit the occurrence of musculoskeletal disorders, individual and group sessions of relaxation therapy and hypnosis led by volunteer practitioners from our hospital. We quickly enriched the therapeutic offer by opening consultations with a psychologist, as well as with an anti-smoking doctor.
The Survey
To evaluate the relevance, congruence with hospital employees' expectations, and potential appropriateness of our Bulle, we designed a survey concerning the whole GHSJ staff, i.e., all those who had worked during the first wave. The questionnaire was sent 3 months after the first peak of the pandemic, between 15 July and 1 October.
We used a “Microsoft Forms” online questionnaire due to compliance with French data protection laws and the potential for access control, encryption, and account security. Potential respondents were solicited using the hospital mailing list. A specific link was also made available on the intranet network of the group. At last, a QR code displayed on the screensavers of all computers allowed people to get the survey information and answer it at any moment. The survey included five components that were identified from a literature review (33–36) and a local Delphi method. They were: (the submitted questionnaire is accessible as supporting information—Supplementary Appendix S1).
1. Personal information (demographics, exposure to COVID-19, and history of burnout).
2. Professional experience and fears at the time of the survey.
3. Emotional experience during the first wave, and degree of job satisfaction:
a. Did the COVID-19 crisis make you anxious? If so: for yourself, your family, others, or your work?
b. Were you afraid of infecting your loved ones?
c. Do you usually feel good at work?
d. Do you currently feel good at work?
4. The Hospital Anxiety and Depression Scale (HADS). The HADS is a 14-item auto questionnaire that includes seven items on symptoms of anxiety, and seven items on symptoms of depression (37). A cutoff score >7 was used for each subscale for detecting significant symptoms of anxiety or depression (38, 39). Its French translation has been validated among many populations (40–42).
5. The PTSD Checklist (PCL). The PCL is a 17-item self-report measure reflecting The Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) symptoms of PTSD (43). A cutoff score >44 was used for detecting significant symptoms of PTSD (44). It was made clear in the questionnaire that the stressful event to which respondents were referring was the health crisis [considered to have been over a month old at the time of the survey to consider the symptoms as belonging to a PTSD and not an acute stress state (45)].
From the results of this survey, we extracted data on the staff who had accessed the Bulle (those who came more than two times a month).
The protocol has been performed by following the Declaration of Helsinki and approved by the Groupe Ethique et Recherche Médicale/ Ethics and Medical Research Group (GERM) from the Hospital Paris Saint-Joseph, institutional ethics committee (IRB No. 00012157).
According to French regulations (46) no written informed consent was required and an information note setting out the purpose of the research is sufficient for his category of study.
The authors guarantee the anonymity of all collected data.
Statistical Analysis
All results are reported as numbers (percentage). Variables were compared using either the χ2 test or Fisher's exact test, as appropriate.
The relationship of the characteristics of workers who frequented with attendance or not to the Bulle was assessed using logistic regression. Odds ratios (ORs) and their 95% confidence intervals (95%CIs) were calculated using univariable and multivariable logistic regression models. For the multivariable analysis, variables of interest were selected according to their statistical significance in the univariable analysis (critical p-value for entry into the model: 0.2). Considering the absence of the Bulle at the Hospital Marie Lannelongue location, we excluded Marie Lannelongue workers before analysis.
The analysis was performed with the R software (the R project for statistical computing, https://www.r-project.org/). All tests were two-sided, and the value of p < 0.05 was considered statistically significant.
Results
General Responding Population
The survey was fully completed by 675 of the 2,408 (28.0%) employees working at the HPSJ (Table 1). Most participants were aged from 26 to 50 years, and 82.1% were women. The majority (433; 66.8%) lived with a partner, and 339 (84.8%) had at least one child. Among the respondents, 199 (29.5%) reported that they have accessed the Bulle during the first wave of the pandemic.

Table 1. Sociodemographic and emotional characteristics related to COVID-19 and job satisfaction information according to access to the Bulle, among Paris Saint-Joseph Hospital employees.
Most respondents were caregiving staff (n = 315; 46.7%) (nurses, assistant nurses, and nurse managers); 124 participants (18.4%) were health administrative workers (secretary, logistic manager, and pharmaceutical assistant), 112 (16.6%) were doctors or pharmacists, 57 (8.4%) were other caregivers (physiotherapist, stretcher-bearer, radiologic technologist, and psychologist), 21 (3.1%) were midwives, and 46 (6.8%) had other occupation. The length of professional experience was more than 5 years for 512 participants (75.9%) and 377 (55.9%) were in the same workplace for <5 years. With regard to the work location, 325 respondents (48.2%) reported working in a “COVID-19 Unit” (ward for patients with COVID-19) during the wave, 301 (44.6%) in another clinical unit, 92 (13.6%) worked at home, and 119 (17.6%) worked as non-clinical support places. Among the frontline HCWs, 307 (45.5%) reported having taken care of patients with COVID-19 frequently (every working day) or regularly (at least 1 day a week).
In addition to their shifts, 417 (61.8%) reported that they themselves, a colleague, a friend, or a close relative had been infected with SARS-CoV-2.
Psychological Issues in the Responding Population
Most employees reported a high level of job satisfaction (n = 509; 75.4%). A total of 147 participants (21.8%) reported a previous history of burnout or depression. Most of the participants spoke of overwhelming levels of worry and concern related to COVID-19 first wave (n = 419; 62.1%), especially associated with their family (n = 362, 86.4%), themselves (n = 238; 56.8%), or their working conditions (n = 212; 50.6%). Almost three-quarters of the participants reported being afraid of infecting their relatives (n = 504; 74.7%).
Clinically, significant levels of symptoms of anxiety (according to the HAD A scale > 7 points), depression (according to the HAD D scale > 7 points), and PTSD (according to the PCL scale > 44 points) were found, respectively, in 276 (40.9%), 135 (20.0%), and 94 (13.9%) respondents.
Notably, age was not associated with higher measures of anxiety, depression, or PTSD. Staff younger than 41 years had no more symptoms of anxiety (56.6% vs. 53.4%, p = 0.45), depression (52.5% vs. 47.5%, p = 0.47), or PTSD (60.4% vs. 39.6%, p = 0.22) than older ones.
Characteristics of Employees Who Had Accessed the Bulle
Some characteristics were compared between those who had accessed the Bulle and those who had not. As shown in Table 1, participants who had accessed the Bulle during the first wave were younger, aged 18 and 25 years (14.1 vs. 6.3% p < 0.001). They had shorter professional experience (33.7 vs. 20.2%, p < 0.001) and had been in the same hospital location for less time (66.3 vs. 51.5%, p < 0.001). The Bulle was most likely to be accessed by staff without children than among those with children (21.8 vs. 13.0%, p = 0.035), and among those who worked with patients with COVID-19 than among those who did not (51.8 vs. 42.9%, p = 0.034). Hospital employees who met the psychological support team in their working unit were more likely to access the Bulle than those who did not (21.6 vs. 8.4%, p < 0.001), and more often perceived that this visit had a large emotional benefit (51.2 vs. 25.0%, p = 0.002).
In the multivariable analysis (Table 2), few independent characteristics were found to be statistically different between employees who came at the Bulle and others. Those who met the psychological team in their hospital unit were more prone to come to the Bulle than those who did not (OR, 2.2; 95% CI: 1.1–4.6: p = 0.027). Hospital workers who were remote workers came to the Bulle less often than others (OR 0.10; 95% CI 0.02–0.31; p < 0.001).
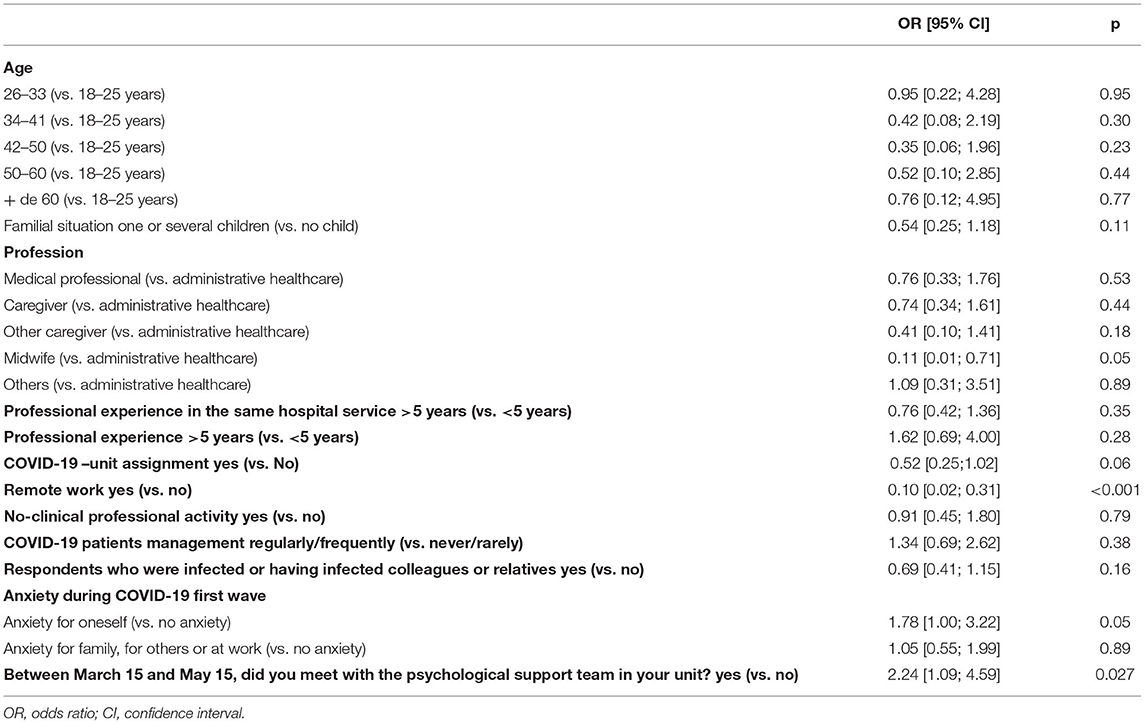
Table 2. Multivariable logistic regression analysis of characteristics of employees associated with access to the Bulle.
The importance of exposure to patients with COVID-19 as an independent factor associated with the use of the Bulle was searched. Our multivariable analysis found no association (OR 1.34; 95% CI 0.69–2.62; p = 0.38).
Discussion
Our study emphasizes the emotional impact of the COVID-19 pandemic on hospital staff. The employees who completed the questionnaire were mainly HCWs, with more than 5 years of experience in their job. Approximately 50% worked in contact with patients with COVID-19 during the first wave. The perception of having been anxious during the first wave was frequent among HCWs who completed the survey, mainly because of the risk of SARS-CoV2 transmission from the hospital to their relatives. High depression scores were observed in 20% of respondents and 41% for anxiety scores.
Other studies in the literature concerning the HCWs during the COVID-19 pandemic reported a prevalence of anxiety from 23 to 51%, and depression from 22 to 50% (47–49), depending on the scales used. A systematic review of 29 studies reported a median prevalence of 24% for anxiety and 21% for depression among HCWs (50). The prevalence of PTSD symptoms among HCWs reported in the literature varied between 71% (51), 21% (52), and 15% (53), which is more than our rate of 14%.
As previously demonstrated by several groups since the beginning of the COVID-19 pandemic, wellbeing centers seem to be efficient and useful (21–23, 25, 54, 55). The protocols are quite different, in terms of setting (historical cloister and garden to unused laboratory), staff (“wellbeing buddies,” psychiatrists, psychologists, social workers, and physical therapists), tools (quiet space, massages, Pilates, relaxation therapy, sensory rooms, etc.). However, the purpose is always similar: to provide a brief break from the global turmoil of healthcare during a hospital frontline work day (22, 23, 25, 56). Current studies emphasize the needs expressed needs by hospital staff and the testimony of individual benefits of one or the other part of the wobble room, such as quietness and psychological support (22). Notably, although associated with multiple biases, a large part of respondents stated that the use of the Bulle has had a positive impact on their emotional status, similar to what has been previously published (22, 56). In the same way, social and administrative workers seem to get benefits from the Bulle. Few previous studies were devoted to this part of the hospital staff (16, 23). However, some surveys found, as we did, that non-clinical hospital workers had high risks for depression, insomnia, anxiety (57), and PTSD (58) during a health crisis. As hospital employees, they suffer from double stress due to both community and potential patient exposure in many situations. It is noteworthy that if administrative jobs offer large opportunities for remote work and thus a lower risk of COVID-19 accidental exposure (59), they are exposed to an increased risk of stress factors associated with social isolation (60). Another reason could be that the logistic staff and others working in the hospital might not be as psychologically prepared as doctors and nurses (58). This observation should let wellbeing centers be freely open to any type of profession. Another interesting point is the reason expressed for anxiety, as a retrospective experience. Regardless of the use of the Bulle, the major reason for this anxiety was the fear of viral transmission to their relatives, rather than their own risk of disease. This is a major issue, already underlined in general studies on the stress of HCWs during the COVID-19 pandemic (61–63).
A remaining question is how to reach our “target population” of most affected persons? (16). In our work, anxiety seems to remain a few months after the first severe wave of the pandemic. Interestingly, our multivariable analysis highlighted the role of intervention of the support team in the probability of accessing the Bulle. This couple of psychologist and medical doctor visited care departments to meet professionals and exchange with them. It was agreed that these couples would promote the Bulle to encourage staff to go there. Distressed workers may suffer from psychological inhibition, and the proactive intervention of trained professionals may increase “recruitment” of the most vulnerable workers. In our survey, meeting this psychological support team, before going to the Bulle, seems to be associated with increased attendance at the wellbeing center, even if such data should be confirmed in prospective studies. At last, we observed that being married and having children were associated with a lower frequency of the use of the Bulle. This point was unexpected. Fear of viral transmission to relatives is associated with increased anxiety and having children would increase anxiety. Considering the possible use of a wellbeing center during working hours, this link seems not to be associated with lack of time, leading us to consider relatives as a protective psychological factor. However, this point is not observed in large studies (16). Nonetheless, small cohorts already showed a potential protective effect of assistance from relatives, families, friends, and even patients (64).
Our work has several limitations. First, it is a retrospective survey on the use of the Bulle center, leading to memory biases. However, considering the evaluation of anxiety, depression, and PTSD at the time of the evaluation questionnaire, the responses are probably relevant for evaluating mental status a few months after the first wave of the pandemic. The voluntary nature of participation in the survey may lead to problems of sample bias (65). Second, in this cross-sectional study, we did not randomize the use of the Bulle, leading to difficulties to evaluate the effect of the wellbeing center on anxiety, depression, or PTSD. Ethical issues led us not to limit access to our center. Conversely, prospective studies about specific tools are acceptable and we plan to confirm the observed benefit with randomized works in the future. Third, due to the survey response rate, there is a unit non-response error that results from a failure to collect information on all units in the selected sample. Unit non-response is a source of non-sampling error that can influence our survey. Estimates based only on respondents may be biased if the characteristics of respondents and non-respondents are not the same.
The choice of scales used to assess an emotional state has been carefully considered: in France, the HAD scale is the reference scale for assessing anxiety and depression in any type of population because it is easy and quick to complete, and its French translation has been validated (40–42), unlike several other international scales assessing the same symptoms.
On the other hand, we have chosen PCL, which refers to DSM-IV rather than the newer version PCL-5 because of the controversy about the causal link between COVID-19 and PTSD. Indeed, frontline hospital staff in a region particularly affected by the epidemic, who had to reorganize all their work, were confronted with much more numerous serious patients than usual, with the risk of transmitting the virus to their relatives due to the lack of personal protective equipment, etc. have been exposed to a particularly stressful event that may meet the DSM-V definition (66)—direct exposure to the traumatic event (TE) or direct witness (of a TE happening to others), repeated or extreme exposure to aversive situations (e.g., caregivers, rescue workers, and hospital staff). Some authors, agree with that point of view (67, 68). However, PTSD should not be considered a concept that applies to COVID-19 in general (69–72). As DSM-V does not allow to consider COVID-19 as a TE responsible for PTSD, we used, as previously done, the DSM-IV parameters as inclusion criteria (31, 73, 74).
Our study has several strengths. This is a large study, which makes the result powerful. The sample studied is homogeneous: all respondents work in the same university hospital in Greater Paris, which was severely affected by the first wave of the pandemic. The distribution of the study population is representative of the total hospital population and includes all types of professions, including administrative staff. The relevance of the implementation of this Bulle innovation by an experienced clinician has been confirmed by the deployment of similar lounges in several other French hospitals subsequently.
It is now necessary to carry out studies to highlight its usefulness and measure its impact on the mental health of hospital staff. We want, for example, to evaluate the impact of the use of Bulle on the level of anxiety, heart rate variability (HRV), and the quality of life over 3 and 6 months.
Conclusion
During the COVID-19 pandemic, a number of wellbeing centers were set up in hospitals around the world. This was an early intervention to mitigate the psychological impact of the COVID-19 crisis on HCWs. Although we cannot recommend one type of intervention over another because no study has been conducted to show their benefits on the hospital workers, high-quality rest spaces should be essential for staff wellbeing. Our survey highlights that wellbeing centers are frequented by staff from all occupational groups and might be promoted equally among them. Potential recruitment of frail workers by specific intervention teams may be relevant. The demonstration of the benefits of these spaces needs to be provided by specific prospective studies.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Institutional Ethics Committee (IRB number 00012157): the GERM (Groupe Ethique et Recherche Médicale/ Ethics and Medical Research Group) from the Hospital Paris Saint-Joseph. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
MU, FA, and FP: data curation, investigation, project administration, visualization, draft writing, and final version correction. MU, FA, FP, AF, and GC: conceptualization, formal analysis, methodology, and validation. AF and GC: review and editing. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank Jean-Patrick Lajonchère, chief manager of our hospital, for allowing us to conduct this investigation and also Xavier Durand, Nathalie Castreau, Alexandra Stulz, and Karen Pinot from the post-crisis psychological support work group for their help in the conception and implementation of the study. The authors would also like to thank Hélène Beaussier, Nesrine BenNasr, Julien Fournier, and Maryline Fleury for their technical and methodological support and Chloé Lacoste, who agreed to carefully proofread the manuscript to avoid language errors.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.913126/full#supplementary-material
References
1. Pereira-Sanchez V, Adiukwu F, El Hayek S, Bytyçi DG, Gonzalez-Diaz JM, Kundadak GK, et al. COVID-19 effect on mental health: patients and workforce. Lancet Psychiatry. (2020) 7:e29–30. doi: 10.1016/S2215-0366(20)30153-X
2. Ransing R, Ramalho R, Orsolini L, Adiukwu F, Gonzalez-Diaz JM, Larnaout A, et al. Can COVID-19 related mental health issues be measured? Brain Behav Immun. (2020) 88:32–4. doi: 10.1016/j.bbi.2020.05.049
3. Adiukwu F, Orsolini L, Gashi Bytyçi D, El Hayek S, Gonzalez-Diaz JM, Larnaout A, et al. COVID-19 mental health care toolkit: an international collaborative effort by early career psychiatrists section. Gen Psychiatry. (2020) 33:e100270. doi: 10.1136/gpsych-2020-100270
4. Fiorillo A, Gorwood P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur Psychiatry J Assoc Eur Psychiatr. (2020) 63:e32. doi: 10.1192/j.eurpsy.2020.35
5. Fiorillo A, Sampogna G, Giallonardo V, Del Vecchio V, Luciano M, Albert U, et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: results from the COMET collaborative network. Eur Psychiatry J Assoc Eur Psychiatr. (2020) 63:e87. doi: 10.1192/j.eurpsy.2020.89
6. Cooke JE, Eirich R, Racine N, Madigan S. Prevalence of posttraumatic and general psychological stress during COVID-19: a rapid review and meta-analysis. Psychiatry Res. (2020) 292:113347. doi: 10.1016/j.psychres.2020.113347
7. Krishnamoorthy Y, Nagarajan R, Saya GK, Menon V. Prevalence of psychological morbidities among general population, healthcare workers and COVID-19 patients amidst the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. (2020) 293:113382. doi: 10.1016/j.psychres.2020.113382
8. Moccia L, Janiri D, Pepe M, Dattoli L, Molinaro M, De Martin V, et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: an early report on the Italian general population. Brain Behav Immun. (2020) 87:75–9. doi: 10.1016/j.bbi.2020.04.048
9. Park CL, Russell BS, Fendrich M, Finkelstein-Fox L, Hutchison M, Becker J. Americans' COVID-19 stress, coping, and adherence to CDC guidelines. J Gen Intern Med. (2020) 35:2296–303. doi: 10.1007/s11606-020-05898-9
10. Pierce M, Hope H, Ford T, Hatch S, Hotopf M, John A, et al. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. Lancet Psychiatry. (2020) 7:883–92. doi: 10.1016/S2215-0366(20)30308-4
11. Sheraton M, Deo N, Dutt T, Surani S, Hall-Flavin D, Kashyap R. Psychological effects of the COVID 19 pandemic on healthcare workers globally: a systematic review. Psychiatry Res. (2020) 292:113360. doi: 10.1016/j.psychres.2020.113360
12. Xiong J, Lipsitz O, Nasri F, Lui LMW, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. (2020) 277:55–64. doi: 10.1016/j.jad.2020.08.001
13. Simon NM, Saxe GN, Marmar CR. Mental health disorders related to COVID-19-related deaths. JAMA. (2020) 324:1493–4. doi: 10.1001/jama.2020.19632
14. Adams JG, Walls RM. Supporting the health care workforce during the COVID-19 global epidemic. JAMA. (2020) 323:1439–40. doi: 10.1001/jama.2020.3972
15. Barello S, Palamenghi L, Graffigna G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. (2020) 290:113129. doi: 10.1016/j.psychres.2020.113129
16. De Kock JH, Latham HA, Leslie SJ, Grindle M, Munoz S-A, Ellis L, et al. A rapid review of the impact of COVID-19 on the mental health of healthcare workers: implications for supporting psychological well-being. BMC Public Health. (2021) 21:104. doi: 10.1186/s12889-020-10070-3
17. Shechter A, Diaz F, Moise N, Anstey DE, Ye S, Agarwal S, et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen Hosp Psychiatry. (2020) 66:1–8. doi: 10.1016/j.genhosppsych.2020.06.007
18. Spoorthy MS, Pratapa SK, Mahant S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic–a review. Asian J Psychiatry. (2020) 51:102119. doi: 10.1016/j.ajp.2020.102119
19. Batra K, Singh TP, Sharma M, Batra R, Schvaneveldt N. Investigating the psychological impact of COVID-19 among healthcare workers: a meta-analysis. Int J Environ Res Public Health. (2020) 17:9096. doi: 10.3390/ijerph17239096
20. Ford S. Trusts Setting Up ‘Wobble Rooms’ to Give Nursing Staff Some Covid-19 Respite. Nurs Times (2020). Available online at: https://www.nursingtimes.net/news/workforce/trusts-setting-up-wobble-rooms-to-give-nursing-staff-with-covid-19-respite-07-05-2020/ (accessed January 24, 2022.
21. Gurney L, Lockington J, Quinn L, MacPhee M. Why do we need wobble rooms during COVID-19? Nurs Leadersh Tor Ont. (2020) 33:45–50. doi: 10.12927/cjnl.2021.26421
22. Blake H, Yildirim M, Wood B, Knowles S, Mancini H, Coyne E, et al. COVID-well: evaluation of the implementation of supported wellbeing centres for hospital employees during the COVID-19 pandemic. Int J Environ Res Public Health. (2020) 17:9401. doi: 10.3390/ijerph17249401
23. Lefèvre H, Stheneur C, Cardin C, Fourcade L, Fourmaux C, Tordjman E, et al. The Bulle: support and prevention of psychological decompensation of health care workers during the trauma of the COVID-19 epidemic. J Pain Symptom Manage. (2021) 61:416–22. doi: 10.1016/j.jpainsymman.2020.09.023
24. Pollock A, Campbell P, Cheyne J, Cowie J, Davis B, McCallum J, et al. Interventions to support the resilience and mental health of frontline health and social care professionals during and after a disease outbreak, epidemic or pandemic: a mixed methods systematic review. Cochrane Database Syst Rev. (2020) 11:CD013779. doi: 10.1002/14651858.CD013779
25. Putrino D, Ripp J, Herrera JE, Cortes M, Kellner C, Rizk D, et al. Multisensory, nature-inspired recharge rooms yield short-term reductions in perceived stress among frontline healthcare workers. Front Psychol. (2020) 11:560833. doi: 10.3389/fpsyg.2020.560833
26. Rimmer A, Chatfield C. What organisations around the world are doing to help improve doctors' wellbeing. BMJ. (2020) 369:m1541. doi: 10.1136/bmj.m1541
27. Buselli R, Corsi M, Veltri A, Baldanzi S, Chiumiento M, Lupo ED, et al. Mental health of health care workers (HCWs): a review of organizational interventions put in place by local institutions to cope with new psychosocial challenges resulting from COVID-19. Psychiatry Res. (2021) 299:113847. doi: 10.1016/j.psychres.2021.113847
28. Chen L, Michalsen A. Management of chronic pain using complementary and integrative medicine. BMJ. (2017) 357:j1284. doi: 10.1136/bmj.j1284
29. Nguyen CT. Integrative medicine as a bridge to physician wellness. Otolaryngol–Head Neck Surg. (2018) 158:987–8. doi: 10.1177/0194599818765126
30. Lin Y-C, Wan L, Jamison RN. Using integrative medicine in pain management: an evaluation of current evidence. Anesth Analg. (2017) 125:2081–93. doi: 10.1213/ANE.0000000000002579
31. Maunder R. The experience of the 2003 SARS outbreak as a traumatic stress among frontline healthcare workers in Toronto: lessons learned. Philos Trans R Soc Lond B Biol Sci. (2004) 359:1117–25. doi: 10.1098/rstb.2004.1483
32. Guétin S, Brun L, Deniaud M, Clerc J-M, Thayer JF, Koenig J. Smartphone-based music listening to reduce pain and anxiety before coronarography: a focus on sex differences. Altern Ther Health Med. (2016) 22:60–3.
33. Chong M-Y, Wang W-C, Hsieh W-C, Lee C-Y, Chiu N-M, Yeh W-C, et al. Psychological impact of severe acute respiratory syndrome on health workers in a tertiary hospital. Br J Psychiatry J Ment Sci. (2004) 185:127–33. doi: 10.1192/bjp.185.2.127
34. Su T-P, Lien T-C, Yang C-Y, Su YL, Wang J-H, Tsai S-L, et al. Prevalence of psychiatric morbidity and psychological adaptation of the nurses in a structured SARS caring unit during outbreak: a prospective and periodic assessment study in Taiwan. J Psychiatr Res. (2007) 41:119–30. doi: 10.1016/j.jpsychires.2005.12.006
35. Lin C-Y, Peng Y-C, Wu Y-H, Chang J, Chan C-H, Yang D-Y. The psychological effect of severe acute respiratory syndrome on emergency department staff. Emerg Med J EMJ. (2007) 24:12–7. doi: 10.1136/emj.2006.035089
36. Wu P, Fang Y, Guan Z, Fan B, Kong J, Yao Z, et al. The psychological impact of the SARS epidemic on hospital employees in China: exposure, risk perception, and altruistic acceptance of risk. Can J Psychiatry Rev Can Psychiatr. (2009) 54:302–11. doi: 10.1177/070674370905400504
37. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
38. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. (2002) 52:69–77. doi: 10.1016/S0022-3999(01)00296-3
39. Olssøn I, Mykletun A, Dahl AA. The hospital anxiety and depression rating scale: a cross-sectional study of psychometrics and case finding abilities in general practice. BMC Psychiatry. (2005) 5:46. doi: 10.1186/1471-244X-5-46
40. Lépine JP, Godchau M, Brun P, Lempérière T. [Evaluation of anxiety and depression among patients hospitalized on an internal medicine service]. Ann Med Psychol. (1985) 143:175–89.
41. Razavi D, Delvaux N, Farvacques C, Robaye E. Screening for adjustment disorders and major depressive disorders in cancer in-patients. Br J Psychiatry J Ment Sci. (1990) 156:79–83. doi: 10.1192/bjp.156.1.79
42. Bocéréan C, Dupret E. A validation study of the hospital anxiety and depression scale (HADS) in a large sample of French employees. BMC Psychiatry. (2014) 14:354. doi: 10.1186/s12888-014-0354-0
43. Yao S-N, Cottraux J, Note I, De Mey-Guillard C, Mollard E, Ventureyra V. [Evaluation of post-traumatic stress disorder: validation of a measure, the PCLS]. L'Encephale. (2003) 29:232–8.
44. Bah AJ, James PB, Bah N, Sesay AB, Sevalie S, Kanu JS. Prevalence of anxiety, depression and post-traumatic stress disorder among Ebola survivors in northern Sierra Leone: a cross-sectional study. BMC Public Health. (2020) 20:1391. doi: 10.1186/s12889-020-09507-6
45. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association (2013).
46. Délibération n° 2018-155 du 3 mai 2018 portant homologation de la méthodologie de référence relative aux traitements de données à caractère personnel mis en œuvre dans le cadre des recherches n'impliquant pas la personne humaine, des études et évaluations dans le domaine de la santé (MR-004) - Légifrance. Available online at: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000037187498 (accessed September 24, 2021).
47. Hu D, Kong Y, Li W, Han Q, Zhang X, Zhu LX, et al. Frontline nurses' burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: a large-scale cross-sectional study. EClinicalMedicine. (2020) 24:100424. doi: 10.1016/j.eclinm.2020.100424
48. Azoulay E, Cariou A, Bruneel F, Demoule A, Kouatchet A, Reuter D, et al. Symptoms of anxiety, depression, and peritraumatic dissociation in critical care clinicians managing patients with COVID-19. A Cross-Sectional Study Am J Respir Crit Care Med. (2020) 202:1388–98. doi: 10.1164/rccm.202006-2568OC
49. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. (2020) 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
50. Muller AE, Hafstad EV, Himmels JPW, Smedslund G, Flottorp S, Stensland SØ, et al. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: a rapid systematic review. Psychiatry Res. (2020) 293:113441. doi: 10.1016/j.psychres.2020.113441
51. Maharaj S, Lees T, Lal S. Prevalence and risk factors of depression, anxiety, and stress in a cohort of australian nurses. Int J Environ Res Public Health. (2018) 16:61. doi: 10.3390/ijerph16010061
52. Zhang R, Hou T, Kong X, Wang G, Wang H, Xu S, et al. PTSD among healthcare workers during the COVID-19 outbreak: a study raises concern for non-medical staff in low-risk areas. Front Psychiatry. (2021) 12:696200. doi: 10.3389/fpsyt.2021.696200
53. Erquicia J, Valls L, Barja A, Gil S, Miquel J, Leal-Blanquet J, et al. Emotional impact of the Covid-19 pandemic on healthcare workers in one of the most important infection outbreaks in Europe. Med Clin Engl Ed. (2020) 155:434–40. doi: 10.1016/j.medcli.2020.07.006
54. Buselli R, Baldanzi S, Corsi M, Chiumiento M, Del Lupo E, Carmassi C, et al. Psychological care of health workers during the COVID-19 outbreak in Italy: preliminary report of an occupational health department (AOUP) responsible for monitoring hospital staff condition. Sustainability. (2020) 12:5039. doi: 10.3390/su12125039
55. Mellins CA, Mayer LES, Glasofer DR, Devlin MJ, Albano AM, Nash SS, et al. Supporting the well-being of health care providers during the COVID-19 pandemic: the copecolumbia response. Gen Hosp Psychiatry. (2020) 67:62–9. doi: 10.1016/j.genhosppsych.2020.08.013
56. Saqib A, Rampal T. Quality improvement report: setting up a staff well-being hub through continuous engagement. BMJ Open Qual. (2020) 9:e001008. doi: 10.1136/bmjoq-2020-001008
57. Wang M, Zhao Q, Hu C, Wang Y, Cao J, Huang S, et al. Prevalence of psychological disorders in the COVID-19 epidemic in China: a real world cross-sectional study. J Affect Disord. (2021) 281:312–20. doi: 10.1016/j.jad.2020.11.118
58. Zhang H, Shi Y, Jing P, Zhan P, Fang Y, Wang F. Posttraumatic stress disorder symptoms in healthcare workers after the peak of the COVID-19 outbreak: a survey of a large tertiary care hospital in Wuhan. Psychiatry Res. (2020) 294:113541. doi: 10.1016/j.psychres.2020.113541
59. Evanoff BA, Strickland JR, Dale AM, Hayibor L, Page E, Duncan JG, et al. Work-related and personal factors associated with mental well-being during the COVID-19 response: survey of health care and other workers. J Med Internet Res. (2020) 22:e21366. doi: 10.2196/21366
60. Galea S, Merchant RM, Lurie N. The mental health consequences of COVID-19 and physical distancing: the need for prevention and early intervention. JAMA Intern Med. (2020) 180:817–8. doi: 10.1001/jamainternmed.2020.1562
61. Cawcutt KA, Starlin R, Rupp ME. Fighting fear in healthcare workers during the COVID-19 pandemic. Infect Control Hosp Epidemiol. (2020) 41:1192–3. doi: 10.1017/ice.2020.315
62. Mohsin SF, Agwan MA, Shaikh S, Alsuwaydani ZA, AlSuwaydani SA. COVID-19: Fear and anxiety among healthcare workers in Saudi Arabia. A cross-sectional study Inquiry. (2021) 58:1–8. doi: 10.1177/00469580211025225
63. Taylor S, Landry CA, Rachor GS, Paluszek MM, Asmundson GJG. Fear and avoidance of healthcare workers: an important, under-recognized form of stigmatization during the COVID-19 pandemic. J Anxiety Disord. (2020) 75:102289. doi: 10.1016/j.janxdis.2020.102289
64. Fang M, Xia B, Tian T, Hao Y, Wu Z. Drivers and mediators of healthcare workers' anxiety in one of the most affected hospitals by COVID-19: a qualitative analysis. BMJ Open. (2021) 11:e045048. doi: 10.1136/bmjopen-2020-045048
65. Alessi EJ, Martin JI. Conducting an internet-based Survey: benefits, pitfalls, and lessons learned. Soc Work Res. (2010) 34:122–8. doi: 10.1093/swr/34.2.122
66. Psychiatry.org - DSM. Available online at: https://psychiatry.org:443/psychiatrists/practice/dsm (accessed June 3, 2022).
67. Dutheil F, Mondillon L, Navel V. PTSD as the second tsunami of the SARS-CoV-2 pandemic. Psychol Med. (2021) 51:1773–4. doi: 10.1017/S0033291720001336
68. Underner M, Perriot J, Peiffer G, Jaafari N. COVID-19 et trouble de stress post-traumatique (TSPT) chez les professionnels de santé. Rev Mal Respir. (2021) 38:216–9. doi: 10.1016/j.rmr.2020.11.014
69. Taylor S, Landry CA, Paluszek MM, Fergus TA, McKay D, Asmundson GJG. Development and initial validation of the COVID Stress Scales. J Anxiety Disord. (2020) 72:102232. doi: 10.1016/j.janxdis.2020.102232
70. Shevlin M, Hyland P, Karatzias T. Is posttraumatic stress disorder meaningful in the context of the COVID-19 Pandemic? a response to van overmeire's commentary on Karatzias et al. (2020). J Trauma Stress. (2020) 33:866–8. doi: 10.1002/jts.22592
71. Kaseda ET, Levine AJ. Post-traumatic stress disorder: a differential diagnostic consideration for COVID-19 survivors. Clin Neuropsychol. (2020) 34:1498–514. doi: 10.1080/13854046.2020.1811894
72. Van Overmeire R. The methodological problem of identifying criterion a traumatic events during the COVID-19 Era: a commentary on Karatzias et al. (2020). J Trauma Stress. (2020) 33:864–5. doi: 10.1002/jts.22594
73. Xu J, Zheng Y, Wang M, Zhao J, Zhan Q, Fu M, et al. Predictors of symptoms of posttraumatic stress in Chinese university students during the 2009 H1N1 influenza pandemic. Med Sci Monit Int Med J Exp Clin Res. (2011) 17:PH60–4. doi: 10.12659/MSM.881836
Keywords: anxiety, burnout, COVID-19, depression, healthcare workers, post-traumatic stress disorder, mental health, wellbeing center
Citation: d'Ussel M, Adam F, Fels A, Chatellier G and Philippart F (2022) Characteristics of Hospital Workers Using a Wellbeing Center Implemented During the COVID-19 Pandemic to Prevent the Emotional Impacts of the Crisis. Front. Public Health 10:913126. doi: 10.3389/fpubh.2022.913126
Received: 07 April 2022; Accepted: 08 June 2022;
Published: 04 July 2022.
Edited by:
Krystyna Kowalczuk, Medical University of Bialystok, PolandReviewed by:
Ravi Philip Rajkumar, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), IndiaRoel Van Overmeire, Vrije University Brussel, Belgium
Copyright © 2022 d'Ussel, Adam, Fels, Chatellier and Philippart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marguerite d'Ussel, bWR1c3NlbEBnaHBzai5mcg==