 Shaojie Li
Shaojie Li Guanghui Cui
Guanghui Cui Kasper Jørgensen
Kasper Jørgensen Zimi Cheng
Zimi Cheng Zihao Li
Zihao Li Huilan Xu
Huilan Xu- 1Xiangya School of Public Health, Central South University, Changsha, China
- 2Department of Integrated Traditional Chinese and Western Medicine, Peking University First Hospital, Beijing, China
- 3Danish Dementia Research Centre, Department of Neurology, University of Copenhagen, Copenhagen, Denmark
- 4West China School of Public Health and West China Fourth Hospital, Sichuan University, Chengdu, China
This study aimed to verify the Chinese version of the Brief Assessment of Impaired Cognition Questionnaire (C-BASIC-Q), and provide a new tool for the future large-scale epidemiological investigation of cognitive function in China. From March to May 2021, a cross-sectional study of 2,144 Chinese community-dwelling older adults (men = 1,075, mean age = 72.01 years, SD = 6.96 years, ranging from 60–99 years) was conducted in Jinan. Exploratory and confirmatory factor analyses were performed to evaluate the factor structure of the C-BASIC-Q. Convergent validity was evaluated by correlations with the Mini-Mental State Examination (MMSE). Internal consistency and test-retest reliability were evaluated using Cronbach's alpha and retest correlations in a sub-sample (n = 129). Linear regression was used to analyze the impact of demographic factors on the MMSE and C-BASIC-Q scores. Measurement invariance was evaluated using a multi-group confirmatory factor analysis. The mean C-BASIC-Q score was 15.94 (SD = 3.43). Factor analysis suggested a three-factor structure of C-BASIC-Q (self-report, orientation, and informant report). The C-BASIC-Q score was significantly positively associated with the MMSE score, showing good convergent validity. Cronbach's alpha of the C-BASIC-Q was 0.862, and the test-retest correlation coefficient was significant (r = 0.952, p < 0.001), indicating good internal consistency and test-retest reliability. Measurement invariance analysis showed that C-BASIC-Q had configural, metric, and scalar invariance across sex, age, residence, education level and marital status. C-BASIC-Q was less affected by age, residence, education, and marital status than the MMSE. In summary, the C-BASIC-Q had good reliability, validity, and measurement invariance, and is a valid tool for evaluating cognitive functioning in Chinese community-dwelling older adults.
Introduction
As a result of economic development and the advancement of medical technology, the average life expectancy of human beings has gradually increased. Concomitantly, the degree of aging of the world's population has continued to increase (1), and age-related decline in cognitive functioning has become a public health problem worldwide. Mild cognitive impairment (MCI) is widely regarded by researchers as an intermediate phase between normal cognitive aging and overt dementia. Data from earlier epidemiological surveys showed that the prevalence of cognitive impairment without dementia was between 5.1 and 35.9% (2). A recent meta-analysis found that the incidence of MCI per 1,000 person-years was 22.5 for ages 75–79 years, 40.9 for ages 80–84 years, and 60.1 for ages 85+ years (3). Cognitive impairment has a great negative impact on the physical and mental health of older adults and their caregivers, not only because it can reduce their quality of life (4, 5), but it also creates a great care and economic burden (6, 7). Studies have found that cognitive impairment in the elderly was greatly affected by midlife or early age cognitive functioning (8). Therefore, early investigation of cognitive function has important public health implications for the prevention of cognitive impairment. In this field, the development and use of cognitive function assessment tools is a core issue.
Currently, cognitive function is generally evaluated by means of commonly used scales such as the Mini-Mental State Examination (MMSE), the Montreal Cognitive Assessment (MoCA), and the clock drawing test (CDT) (9, 10). Among them, the MMSE and MoCA are the most commonly used tools in this field, especially in China. A meta-analysis showed that the MMSE's pooled sensitivity was 0.89 (95% CI, 0.85 to 0.92) and specificity was 0.89 (95% CI, 0.85 to 0.93), which suggests good accuracy for detecting dementia (11). However, the MMSE is susceptible to the education level of participants, is prone to false-positive or false-negative results, and has poor sensitivity in identifying MCI and may not be suitable for screening for MCI in primary care and community research (12). In addition, a recent study found MMSE was less accurate in distinguishing MCI from subjective cognitive decline (SCD); meanwhile, even when the MMSE was used in combination with a quick test of cognitive speed, the MCI and SCD cannot be distinguished with sufficient accuracy (13). To mitigate these limitations of the MMSE, Nasreddine et al. compiled the MoCA specifically for MCI screening (14). A systematic review indicated that the MoCA was superior to the MMSE in identifying MCI (15). Meanwhile, previous study also found that MoCA was more efficacious in identifying subtle cognitive decline than MMSE (16). However, it should be noted that the difficulty level of the MoCA's items is higher, making it difficult for older participants with lower education levels to understand (17), resulting in lower scores which do not accurately reflect their level of cognitive functioning (18). In light of the differences in regional dialects and culture in China, the MoCA is available in multiple versions (19–23) and there is no uniformly recognized version and cut-off value (24–26). In addition, the MMSE and the MoCA have several common limitations, such as too many items, long measurement time, and a heavier survey burden on investigators and participants in community screening and large-scale epidemiological surveys. Therefore, it is necessary to introduce or develop a shorter Chinese version of a cognitive function assessment tool.
In 2019, Jørgensen et al. (27) combined cognitive testing with both patient and informant reports to develop a Brief Assessment of Cognitive Impairment (BASIC), a new brief case-finding tool for dementia and cognitive impairment. BASIC was a case-finding instrument in clinical settings, including patient-directed questions (three questions), Supermarket Fluency (one question), Category Cued Memory Test (one questions), and informant-directed questions (three questions), a total of eight questions (27). However, it should be noted that BASIC may not be appropriate in a community setting because its two cognitive tests take more time and was not easy to manage (need additional tools to cooperate with the test). For example, a stimulus card is needed for the Category Cued Memory Test, which may increase the investigation time and the burden of investigators (28). Obviously, when conducting surveys in community settings, the assessment tool should be easily managed by non-specialists and save time. Therefore, Jørgensen et al. substituted cognitive testing (Supermarket Fluency and Category Cued Memory Test) with questions regarding orientation, and developed a questionnaire version based on BASIC for community settings, the Brief Assessment of Impaired Cognition Questionnaire (BASIC-Q). The questionnaire included three components: self-report, orientation, and informant report, a total of 10 items; its sensitivity was 0.92 and its specificity was 0.97 to detect cognitive impairment, both of which were significantly higher than the sensitivity and specificity of the MMSE (28). In addition, its measurement time is short, which effectively reduces the survey burden on investigators and participants. Currently, there is no research to verify its use on the Chinese population. In only one study, the BASIC was translated into Chinese, and it was validated in stroke patients at a stroke treatment center (29). However, as we mentioned earlier, the Chinese version of BASIC is also not suitable for community settings.
In addition, to the best of our knowledge, no research has focused on the measurement invariance of the BASIC-Q. As a prerequisite for group comparison, measurement invariance refers to whether the meaning of measurement is equivalent between different groups (30). When comparing between groups, only the structure of the measurement was invariant between different groups, and statistical inference could be made (31). Considering that cognitive functions are easily affected by demographic factors such as sex, age, and education level, it is necessary to test the BASIC-Q for measurement invariance across sociodemographic factors.
In large-scale epidemiological surveys with more research content and larger sample sizes, short survey tools can reduce the workload of the survey, reduce the burden on the surveyed and the response bias, and are widely demanded by researchers. Based on the above considerations, in order to provide Chinese researchers with a shorter cognitive function assessment tool, this study aims to verify the Chinese version of the BASIC-Q (C-BASIC-Q) and explore its psychometric properties and measurement invariance.
Materials and Methods
Participants
From March to May 2021, a cross-sectional study of Chinese community-dwelling older adults was conducted in Jinan. A stratified cluster random sampling method was used to select the participants. First, using the 2020 annual per capita gross domestic product (GDP) level of the districts or counties of Jinan City, we divided the 12 districts and counties into three levels: high, medium, and low, with two districts or counties randomly selected from each level. Second, we randomly selected two townships or streets in the six selected districts or counties; therefore, a total of 12 streets or townships were selected. Third, we selected all older adults in two communities from the 12 randomly selected streets or towns to participate in a survey. Participants were included in the survey based on the following criteria: that they were 60 years or older, had lived in the area for more than 6 months, had no hearing or language impairment (self-reported), and voluntarily participated in the survey. Older persons who were clinically diagnosed with severe and terminal diseases or severe cognitive impairment, such as dementia (reported by family members), were excluded.
Before the survey, we communicated with community staff by telephone and determined the investigation time after obtaining their informed consent. We recruited participants by placing posters on publicity boards in the communities. To facilitate the inclusion of participants who were unable to read the questionnaire due to a low educational level, all questionnaires were completed by a uniformly trained investigator, using a face-to-face interview, instead of being filled out by the older adults themselves. A total of 2,201 participants who met the criteria were surveyed. After excluding invalid questionnaires with a wide range of missing content, 2,144 older adults (ranging in age from 60–99 years) participated in this study. The uniformly trained investigators completed the interview survey with the uniformly instructed language. The investigators were all medical undergraduates of grade 3 or above. It should be noted that in the factor structure analysis, we randomly divided the sample into two parts. Sample A (n = 1,072) consisted of 538 men and 534 women and was used for exploratory factor analysis. Sample B (n = 1,072) consisted of 537 men and 535 women and was used for confirmatory factor analysis. Moreover, 129 participants (67 men and 62 women, M = 72.9 years, SD = 7.1 years, ranging from 60–95 years) were selected to complete the retest of the C-BASIC-Q 2 weeks later. Unless otherwise specified, other reliability and validity indicators were based on the complete sample (N = 2,144).
All research procedures followed the principles of the Declaration of Helsinki. The study was approved by the Medical Ethics Committee of Xiangya School of Public Health, Central South University (identification code: XYGW-2020-101).
Translation Procedure
We contacted Dr. Kasper Jørgensen by email and obtained his consent to translate the BASIC-Q into Chinese. First, two psychiatry graduate students were invited to independently translate the English version of the BASIC-Q into Chinese. Second, two professors with more than 10 years' experience in cognitive function research combined the existing Chinese versions of the BASIC to integrate the Chinese version of the questionnaire translated by two graduate students and produced a draft. Third, two English teachers with teaching experience in English-speaking countries and who were not familiar with the scale jointly translated the Chinese version of the scale into English and compared it with the original English version. They confirmed that the sentences and meanings of the translated English version were essentially the same as the original English version. Finally, the C-BASIC-Q was produced and used to evaluate cognitive functioning in the older Chinese adults in our sample.
Measures
Brief Assessment of Impaired Cognition Questionnaire (BASIC-Q)
BASIC-Q was developed by Jørgensen et al. (28), which included three components: self-report (three items), orientation (four items), and informant report (3 items), a total of 10 items. Among them, self-report component uses three-category scoring method (0= to a great extent, 1= to some extent, 2= no). In the orientation component, two scores are possible (0 = wrong answer, 2 = correct answer). The informant report component also uses three-category scoring method (0= much worse, 1= a bit worse, 2= unchanged). The sum of all items gave the total score, ranging from 0 to 20 points. Higher scores indicated lower risks of cognitive impairment. Optimal cutoff score for case-finding of cognitive impairment was 16/17 in a previous study (28).
Mini-Mental State Examination (MMSE)
The MMSE was designed by Folstein et al. (32) to assess participants' cognitive function. The scale includes five dimensions: orientation, short-term memory, attention and calculation ability, recall ability, and language ability. Depending on the participants' answers, two scores are possible (0 = wrong or unable to answer or 1 = true). The sum of all items constituted the total score, ranging from 0 to 30 points. Higher scores indicated better cognitive functioning. With regard to the education level, the MMSE cut-off score for having MCI was <20 points for the illiterate group, <25 points for the primary school group, and <28 for the middle school and higher group (33). In this study, we used the Chinese version of the MMSE (34); Cronbach's alpha was 0.902.
Covariates
We used demographic characteristics, frequently used in previous studies of Chinese older adults (35), as covariates. The covariates were the following: age, sex, residence, education level, and marital status through a self-designed questionnaire survey. Age was categorized into three groups (60–69 years, 70–79 years, and 80 years and above). Residence was categorized as urban vs. rural. Educational level was categorized into three groups (illiteracy, primary school, and middle school and higher). Marital status was categorized as unmarried or married.
Statistical Methods
SPSS version 25 (IBM SPSS Statistics, Armonk, NY, USA) was used to conduct descriptive statistical analysis, Student's t-tests, Pearson's r correlations, internal consistency tests and linear regression. Mplus version 8 was used to conduct the exploratory and confirmatory factor analyses. First, we ranked all participants according to their total C-BASIC-Q score from low to high, selecting the first 27% of participants as the low group, and the last 27% of participants as the high group. Item analysis was performed by comparing the score difference of each item in the high and low groups (used student's t-tests), and the correlation between each item score and the total score. The purpose of item analysis was to determine the homogeneity and discrimination of items to determine whether items need to be deleted. When the results of t test and correlation analysis were statistically significant, it indicated that all items had good homogeneity and differentiation.
Second, we used exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) to evaluate the factor structure of the C-BASIC-Q. Specifically, we first used Mplus software to conduct EFA based robust maximum likelihood and explored three competition models: one factor, two factors, and three factors. Based on the fitting index, we selected an optimal model for the CFA. Given that the chi-square index is sensitive to sample size, the comparative fit index (CFI), Tucker–Lewis index (TLI), root-mean square error of approximation (RMSEA), and standardized root-mean square residual (SRMR) were used to evaluate model fit. The TLI and CFI are >0.900, and the RMSEA and SRMR are <0.080, indicating that the model fit well (36).
Convergent validity was evaluated by correlation with the MMSE score. Internal consistency and test-retest reliability were evaluated using Cronbach's alpha and retest correlations in a sub-sample (n = 129). In addition, in order to explore which MMSE and C-BASIC-Q scores were less affected by education level and age, we used linear regression models to analyze the impact of demographic factors on the MMSE and C-BASIC-Q scores. Finally, measurement invariance was evaluated using multi-group CFA. There are four levels of measurement invariance: configural, metric, scalar, and strict (37). Previous literature reviews suggested that scalar invariance was sufficient to evaluate the comparison between the mean values of latent factors, while strict invariance was more suitable for comparison between the mean values of observed factors (38, 39). Considering that the total score is generally used when comparing the cognitive function of participants with different demographic characteristics, we did not perform a strict invariance test. According to the fit criterion of the measurement invariance model (40), when the change in CFI (ΔCFI) and RMSEA (ΔRMSEA) is <0.010, compliance invariance is indicated.
Results
Descriptive Statistics
The descriptive statistics for the participants are presented in Table 1.
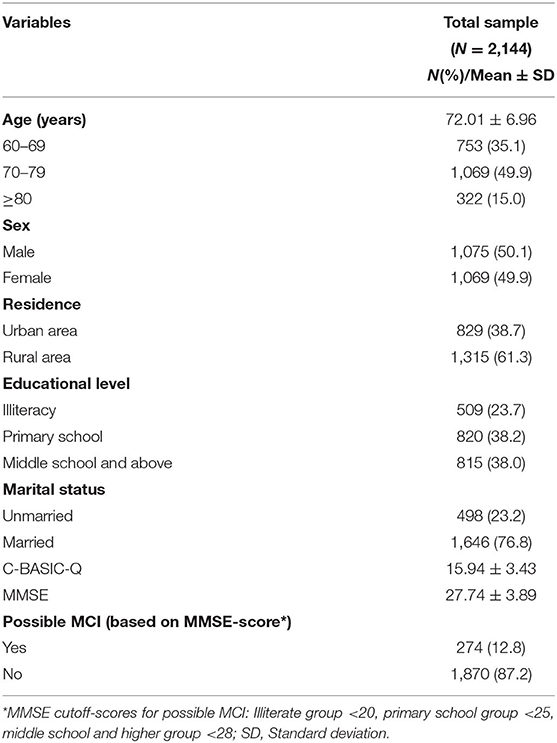
Table 1. Descriptive statistics for the participants.
Item Analysis
The t-test results showed that the score differences of all items of the C-BASIC-Q in the high and low groups were statistically significant. Correlation analysis showed that the scores of all items were significantly and positively correlated with the total score. The data are shown in Table 2.
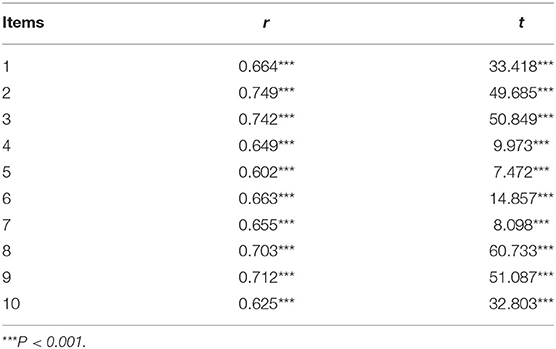
Table 2. Correlation analysis between each item of C-BASIC-Q and the total score of the scale and the results of the high and low group t-test (N = 2,144).
Structural Validity
The fit results of the three competing models obtained using EFA are shown in Table 3. Of the three, the fit index of the three-factor structure model was significantly better than that of both the two-factor and the single-factor structures. Therefore, we used the three-factor structure for the CFA. A preliminary analysis suggested that the initial CFA model of C-BASIC-Q has a poor fit index, so we set a residual correlation (item five with item seven) to correct the model. The results showed that the fit index of the corrected three-factor structure met the model-fit requirements. Above all, the C-BASIC-Q suggested a three-factor structure, namely self-report, orientation, and informant report. The loading of each item of the three-factor structure of the EFA and CFA is presented in Table 4.

Table 3. EFA and CFA fitting indexes of the C-BASIC-Q.
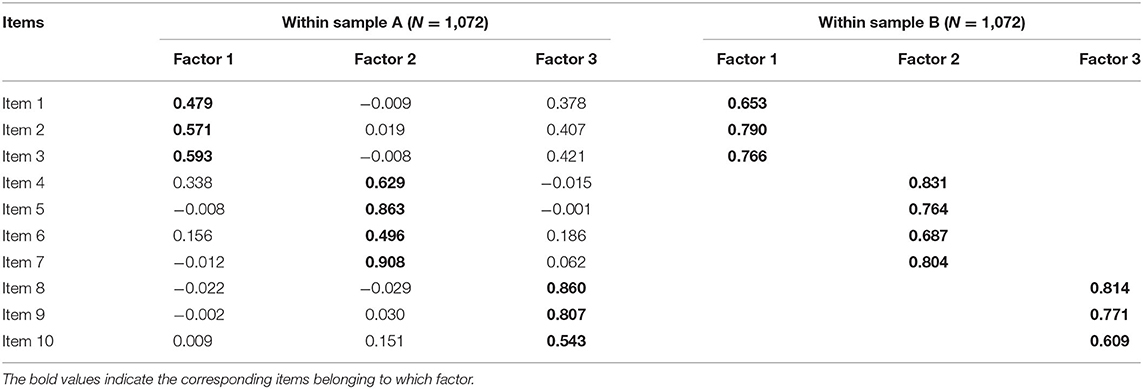
Table 4. Loadings and commonality of each item on three factors in EFA and CFA.
Convergent Validity
The results of correlation analysis showed that the total C-BASIC-Q score was significantly positively associated with the total MMSE score (r = 0.590, p < 0.001).
Internal Consistency and Test-Retest Reliability
Cronbach's alphas of the C-BASIC-Q and its three factors (self-report, orientation, and informant reports) were 0.862, 0.784, 0.840, and 0.782 in the total sample. The test-retest correlation coefficient was significant (r = 0.952, p < 0.001) in the retest sample (n = 129), indicating that the C-BASIC-Q has good internal consistency and test-retest reliability.
Measurement Invariance
Table 5 shows the fit index of the measurement invariance model of the C-BASIC-Q's three-factor model across sex, age, residence, education level, and marital status. All model fit indices meet the fit standard. In addition, from the configural invariance model to the metric invariance model, and then to the scalar invariance model, the ΔCFI and ΔRMSEA were all <0.010. These results supported the identification of configural, metric, and scalar measurement invariance in the C-BASIC-Q across sex, age, residence, education level, and marital status.
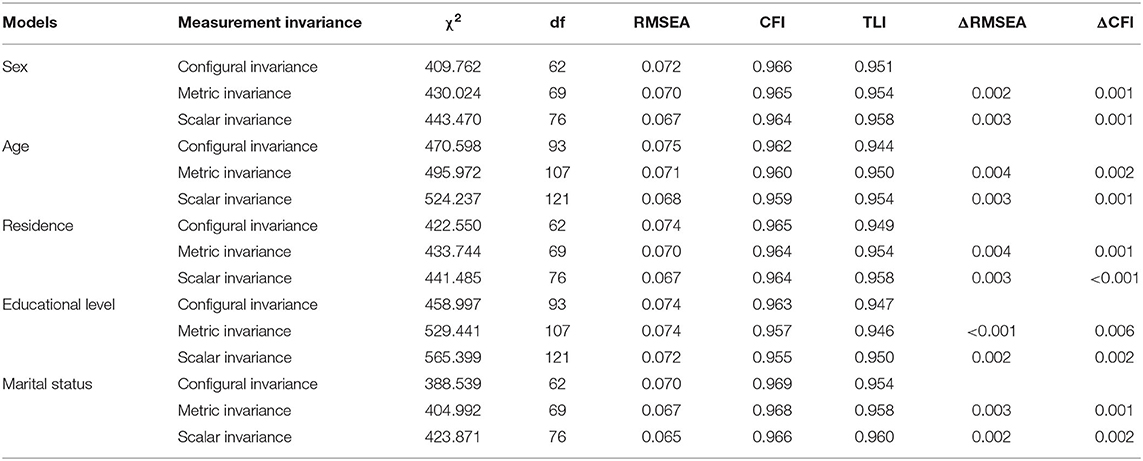
Table 5. Measurement invariances across sex, age, residence, educational level, and marital status.
Factors Related to C-BASIC-Q and MMSE
The status of the C-BASIC-Q according to different participant characteristics is presented in Table 6. The results of linear regression analysis showed that age, residence, education level, and marital status all had an impact on the C-BASIC-Q and the MMSE scores (Table 7). By comparing the coefficients of determination, the impact of the four factors on the C-BASIC-Q was less than the impact on the MMSE (0.076 vs. 0.123).
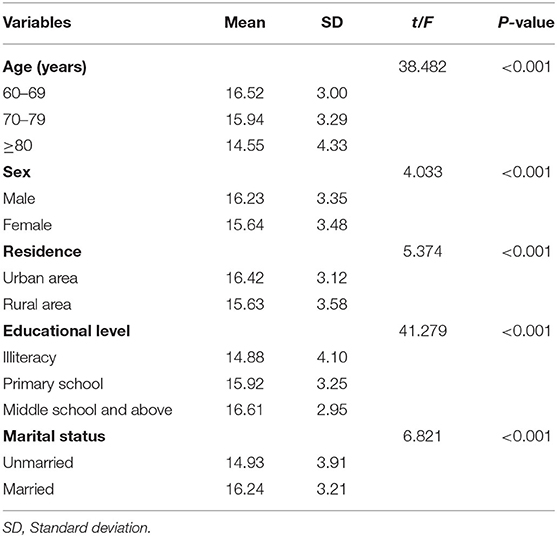
Table 6. The status of C-BASIC-Q by different characteristics.

Table 7. Linear regression analysis for the contributions of sex, age, residence, education level, and marital status on C-BASIC-Q and MMSE.
Discussion
In this study, the BASIC-Q was translated into Chinese for the first time, and it was verified among community-dwelling older adults. This study provides scientific evidence for the application of the C-BASIC-Q in Chinese older adults and even other Chinese speaking people outside China. Our results showed that C-BASIC-Q has a three-factor structure, showing good structural validity. The C-BASIC-Q score was significantly correlated with MMSE, had good convergent validity, and its internal consistency and retest reliability were both good. In addition, its configural, metric, and scalar measurement invariance across sex, age, residence, education level, and marital status were supported. In general, the C-BASIC-Q has good reliability, validity, and measurement invariance, and can be used to evaluate the cognitive functioning of community-dwelling older adults in China.
The results of item analysis showed that each item was significantly positively associated with the C-BASIC-Q total score, and the difference in the scores of each item in the high and low groups was statistically significant, indicating that each item had good homogeneity and discrimination. Because factor structure analysis was not performed in the development of the original scale (28), we divided the total sample into two parts to explore the factor structure of the C-BASIC-Q, which is one of the novel contributions of this study. The results suggest that C-BASIC-Q has a three-factor structure and good structural validity. Interestingly, the items of the three factors of the C-BASIC-Q confirmed the three components of the original scale (i.e., self-report, orientation, and informant report). Therefore, the original three component names were adopted for the Chinese version. Moreover, correlation analysis showed that the C-BASIC-Q was significantly positively correlated with the MMSE; that is, the higher the C-BASIC-Q score, the better the cognitive functioning, showing good convergent validity. In addition, Cronbach's α coefficient of the C-BASIC-Q was 0.863, and the test-retest reliability at the two-week interval was 0.952, indicating that C-BASIC-Q has good internal consistency and stability, and the reliability was good.
Another important contribution of this study is the test of the measurement invariance of the C-BASIC-Q. Future studies can analyze the potential mean differences between different groups by determining the measurement invariance of the C-BASIC-Q. This study found that the C-BASIC-Q had configural, metric, and scalar measurement invariance across sex, age, residence, education level, and marital status. Specifically, the establishment of configural invariance means that the factor structure of the C-BASIC-Q between different groups was the same. Second, the results of metric invariance tests showed that the factor loadings between different groups were equivalent, that is, participants in different groups have the same understanding of each item. Finally, the results of scalar invariance suggested that the intercept of the C-BASIC-Q has cross-group equivalence, that is, the measurement properties of the C-BASIC-Q are the same across different groups. In summary, the evidence of the three invariance measurements indicated that the scores of the C-BASIC-Q are comparable regardless of sex, age, residence, education level, and marital status.
In this study, the differences in the C-BASIC-Q scores of participants of different age, sex, residence, education level, and marital status were statistically significant. Specifically, participants who were younger, male, living in urban areas, had higher education levels, and were married had higher cognitive functioning, which was consistent with the results of previous studies (33, 35). The results of linear regression analysis suggested that age, residence, education level, and marital status all had an impact on the C-BASIC-Q and the MMSE scores. However, it is worth noting that the variance explained by the above four factors on the C-BASIC-Q was lower than on the MMSE. In other words, compared with the MMSE, the C-BASIC-Q was less affected by age, residence, education, and marital status. This means the C-BASIC-Q is more suitable for epidemiological investigations, than the MMSE.
This study had several limitations. First, we did not have a gold standard for identifying MCI and dementia in this sample (that is, the clinician's diagnosis), which made it impossible to infer the cut-off value of the C-BASIC-Q for judging MCI and dementia. In the future, it will be necessary to combine the diagnosis of clinicians with the C-BASIC-Q, and determine the cut-off value of the C-BASIC-Q, which will lay the foundation for future MCI and dementia screening. Second, the sample for this study was drawn from only one city in China, which may not be nationally representative. In the future, scholars can expand the scope of sampling, increase the sample size, and further verify the C-BASIC-Q nationwide in China. Third, this study only verified the C-BASIC-Q in community settings, and it is necessary to conduct psychometric tests in the clinical environment or nursing home environment. Fourth, it has poor adaptability among elderly people living alone because the C-BASIC-Q includes an informant report. In situations where reliable informant reports cannot be obtained, a prorated BASIC-Q score may be used, but with a possible reduction in validity. Finally, since we only selected 129 participants to retest after 2 weeks, the sample size was small and the time-span was short, so a longitudinal invariance test was not performed.
Despite the above-mentioned limitations, this research is groundbreaking in the exploration of the C-BASIC-Q's factor structure and measurement invariance, and provides a reference for future validation of the BASIC-Q in other languages. In addition, we have provided a short, easy-to-use measurement tool for conducting surveys on the cognitive functioning of older adults in the Chinese community, and this is also a starting point for the use of the C-BASIC-Q in the measurement of cognitive functioning in China.
Conclusions
The C-BASIC-Q is a valid tool for evaluating cognitive function in Chinese community-dwelling older adults with good reliability, validity, and measurement invariance.
Data Availability Statement
The datasets can be made available to any interested person(s) contacting the corresponding author via email.
Ethics Statement
The studies involving human participants were reviewed and approved by Medical Ethics Committee of Xiangya School of Public Health, Central South University. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
SL and GC designed the study, conducted surveys, analyzed data, and wrote the first manuscript. KJ provided suggestions on additional statistical analysis and manuscript writing and revised the original manuscript. ZC and ZL contributed to the scale translation process. HX revised the manuscript. All authors read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors thank all the participants and investigators for their efforts.
Abbreviations
C-BASIC-Q, Chinese version of the Brief Assessment of Impaired Cognition Questionnaire; MMSE, Mini-Mental State Examination; MCI, Mild cognitive impairment; EFA, Exploratory Factor Analysis; CFA, Confirmatory Factor Analysis; CFI, Comparative Fit Index; TLI, Tucker–Lewis Index; RMSEA, Root-Mean Square Error of Approximation; SRMR, Standardized Root-Mean Square Residual.
References
1. Saw YM, Saw TN, Than TM, Khaing M, Soe PP, Oo S, et al. Cognitive impairment and its risk factors among Myanmar elderly using the revised Hasegawa's dementia scale: a cross-sectional study in Nay Pyi Taw, Myanmar. PLoS ONE. (2020) 15:e0236656. doi: 10.1371/journal.pone.0236656
2. Ward A, Arrighi HM, Michels S, Cedarbaum JM. Mild cognitive impairment: disparity of incidence and prevalence estimates. Alzheimer's Demen: J Alzheimer's Assoc. (2012) 8:14–21. doi: 10.1016/j.jalz.2011.01.002
3. Gillis C, Mirzaei F, Potashman M, Ikram MA, Maserejian N. The incidence of mild cognitive impairment: a systematic review and data synthesis. Alzheimer's Dement. (2019) 11:248–56. doi: 10.1016/j.dadm.2019.01.004
4. Hill NL, McDermott C, Mogle J, Munoz E, DePasquale N, Wion R, et al. Subjective cognitive impairment and quality of life: a systematic review. Int Psychogeriatr. (2017) 29:1965–77. doi: 10.1017/S1041610217001636
5. Carlozzi NE, Sherman CW, Angers K, Belanger MP, Austin AM, Ryan KA. Caring for an individual with mild cognitive impairment: a qualitative perspective of health-related quality of life from caregivers. Aging Ment Health. (2018) 22:1190–8. doi: 10.1080/13607863.2017.1341468
6. Connors MH, Seeher K, Teixeira-Pinto A, Woodward M, Ames D, Brodaty H. Mild cognitive impairment and caregiver burden: a 3-year-longitudinal study. Am J Geriatric Psych: Official J Am Assoc Geriatric Psych. (2019) 27:1206–15. doi: 10.1016/j.jagp.2019.05.012
7. Lin PJ, Neumann PJ. The economics of mild cognitive impairment. Alzheimer's Demen: J Alzheimer's Assoc. (2013) 9:58–62. doi: 10.1016/j.jalz.2012.05.2117
8. Knopman DS, Gottesman RF, Sharrett AR, Tapia AL, DavisThomas S, Windham BG, et al. Midlife vascular risk factors and midlife cognitive status in relation to prevalence of mild cognitive impairment and dementia in later life: the atherosclerosis risk in communities study. Alzheimer's Demen: J Alzheimer's Assoc. (2018) 14:1406–15. doi: 10.1016/j.jalz.2018.03.011
9. Pottie K, Rahal R, Jaramillo A, Birtwhistle R, Thombs BD, Singh H, et al. Recommendations on screening for cognitive impairment in older adults. CMAJ. (2016) 188:37endations on 1503/cmaj.141165
10. Owens DK, Davidson KW, Krist AH, Barry MJ, Cabana M, Caughey AB, et al. Screening for cognitive impairment in older adults: US preventive services task force recommendation statement. JAMA. (2020) 323:757–63. doi: 10.1001/jama.2020.0435
11. Patnode CD, Perdue LA, Rossom RC, Rushkin MC, Redmond N, Thomas RG, et al. Screening for cognitive impairment in older adults: updated evidence report and systematic review for the US preventive services task force. Jama. (2020) 323:764–85. doi: 10.1001/jama.2019.22258
12. Mitchell AJ, A. meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J Psychiatr Res. (2009) 43:411–31. doi: 10.1016/j.jpsychires.2008.04.014
13. Petrazzuoli F, Vestberg S. Midl8.04.014curacy of the mini-mental state examinaticognitive tests used in primary care cannot accurately differentiate mild cognitive impairment from subjective cognitive decline. J Alzheimer's Dis. (2020) 75:1191–201. doi: 10.3233/JAD-191191
14. Nasreddine ZS, Phillips NA, Bry care cannot accurately differentiate mild co, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriat Soc. (2005) 53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x
15. Pinto TCC, Machado L, Bulgacov TM, Rodrigues-Jrief screening tool for mild cog, et al. Is the montreal cognitive assessment (MoCA) screening superior to the mini-mental state examination (MMSE) in the detection of mild cognitive impairment (MCI) and Alzheimer's disease (AD) in the elderly? Int Psychogeriatr. (2019) 31:491–504. doi: 10.1017/S1041610218001370
16. Pan FF, Huang L, Chen KL, Zhao QH, Guo QH, A. comparative study on the validations of three cognitive screening tests in identifying subtle cognitive decline. BMC Neurol. (2020) 20:78. doi: 10.1186/s12883-020-01657-9
17. O'Driscoll C, Shaikh M. Cross-cultural applicability of the montreal cognitive assessment (MoCA): a systematic review. J Alzheimer's Dis: JAD. (2017) 58:789–801. doi: 10.3233/JAD-161042
18. Carson N, Leach L, Murphy KJ, A. re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores. Int J Geriatr Psychiatry. (2018) 33:379–88. doi: 10.1002/gps.4756
19. Chen X, Zhang R, Xiao Y, Dong J, Niu X, Kong W. Reliability and validity of the Beijing version of the montreal cognitive assessment in the evaluation of cognitive function of adult patients with OSAHS. PLoS ONE. (2015) 10:e0132361. doi: 10.1371/journal.pone.0132361
20. Wei J, Jin X, Chen B, Liu X, Zheng H, Guo R, et al. Comparative study of two short-form versions of the montreal cognitive assessment for screening of post-stroke cognitive impairment in a Chinese population. Clin Interv Aging. (2020) 15:907–14. doi: 10.2147/CIA.S248856
21. Chu LW, Ng KH, Law AC, Lee AM, Kwan F. Validity of the cantonese chinese montreal cognitive assessment in Southern Chinese. Geriatr Gerontol Int. (2015) 15:96–103. doi: 10.1111/ggi.12237
22. Tsai CF, Lee WJ, Wang SJ, Shia BC, Nasreddine Z, Fuh JL. Psychometrics of the montreal cognitive assessment (MoCA) and its subscales: validation of the Taiwanese version of the MoCA and an item response theory analysis. Int Psychogeriatr. (2012) 24:651–8. doi: 10.1017/S1041610211002298
23. Yeung PY, Wong LL, Chan CC, Leung JL, Yung CY, A. validation study of the Hong Kong version of montreal cognitive assessment (HK-MoCA) in Chinese older adults in Hong Kong. Hong Kong Med J = Xianggang yi xue za zhi. (2014) 20:504–10. doi: 10.12809/hkmj144219
24. Huang YY, Qian SX, Guan QB, Chen KL, Zhao QH, Lu JH, et al. Comparative study of two Chinese versions of montreal cognitive assessment for screening of mild cognitive impairment. App Neuropsychol Adult. (2021) 28:88–93. doi: 10.1080/23279095.2019.1602530
25. Tan JP Li N, Gao J, Wang LN, Zhao YM Yu BC, et al. Optimal cutoff scores for dementia and mild cognitive impairment of the ontreal among elderly and oldest-old Chinese population. J Alzheimer's Dis: JAD. (2015) 43:1403–12. doi: 10.3233/JAD-141278
26. Wong A, Law LS, Liu W, Wang Z, Lo ES, Lau A, et al. Montreal cognitive assessment: one cutoff never fits all. Stroke. (2015) 46:3547–50. doi: 10.1161/STROKEAHA.115.011226
27. Jørgensen K, Nielsen TR, Nielsen A, Waldorff FB, Høgh P, Jakobsen S, et al. Brief Assessment of Impaired Cognition (BASIC)-Validation of a new dementia case-finding instrument integrating cognitive assessment with patient and informant report. Int J Geriatr Psychiatry. (2019) 34:1724–33. doi: 10.1002/gps.5188
28. Jørgensen K, Nielsen TR, Nielsen A, Waldorff FB, Waldemar G. Psychiatrypaired Cognition (BASIC)-Validation of a neassessment of impaired cognition questionnaire (BASIC-Q)-development and validation of a new tool for identification of cognitive impairment in community settings. Int J Geriatr Psychiatry. (2020) 35:693–701. doi: 10.1002/gps.5286
29. Yuan XF, Zhang Y, Zhang Y, Wu YH, Shi Y, Cheng Y, et al. Reliability and validity of the Brief Assessment of Impaired Cognition (Chinese version) for stroke patients. App Neuropsychol Adult. (2021) 8:1–7. doi: 10.1080/23279095.2021.1908287
30. Reise SP, Widaman KF, Pugh RH. Confirmatory factor analysis and item response theory: two approaches for exploring measurement invariance. Psychol Bull. (1993) 114:552–66. doi: 10.1037/0033-2909.114.3.552
31. Chen FF, Sousa KH, West SG. Teacher's corner: testing measurement invariance of second-order factor models. Struct Equ Model: A Multidiscip J. (2005) 12:471–92. doi: 10.1207/s15328007sem1203_7
32. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
33. Li H, Jia J, Yang Z. Mini-mental state examination in elderly chinese: a population-based normative study. J Alzheimer's Dis: JAD. (2016) 53:487–96. doi: 10.3233/JAD-160119
34. Katzman R, Zhang MY, Ouang Ya Q, Wang ZY, Liu WT Yu E, et al. A Chinese version of the mini-mental state examination; impact of illiteracy in a Shanghai dementia survey. J Clin Epidemiol. (1988) 41:971–8. doi: 10.1016/0895-4356(88)90034-0
35. Zhang Q, Wu Y, Han T, Liu E. Changes in cognitive function and risk factors for cognitive impairment of the elderly in China: 2005-2014. Int J Environ Res Public Health. (2019) 16:2847. doi: 10.3390/ijerph16162847
36. DA K. Measuring Model Fit (2008). Available online at: http://davidakenny.net/cm/fit.htm (accessed June 7, 2021).
37. Putnick DL, Bornstein MH. Measurement invariance conventions and reporting: tThe state of the art and future directions for psychological research. Develop Rev. (2016) 41:71–90. doi: 10.1016/j.dr.2016.06.004
38. van de Schoot R, Lugtig P, Hox J, A. checklist for testing measurement invariance. Eu J Develop Psychol. (2012) 9:486–92. doi: 10.1080/17405629.2012.686740
39. Vandenberg RJ, Lance CE, A. Review and synthesis of the measurement invariance literature: suggestions, practices, and recommendations for organizational research. Organ Res Methods. (2000) 3:4–70. doi: 10.1177/109442810031002
Keywords: cognitive function, validation, reliability, measurement invariance, older adults, China
Citation: Li S, Cui G, Jørgensen K, Cheng Z, Li Z and Xu H (2022) Psychometric Properties and Measurement Invariance of the Chinese Version of the Brief Assessment of Impaired Cognition Questionnaire in Community-Dwelling Older Adults. Front. Public Health 10:908827. doi: 10.3389/fpubh.2022.908827
Received: 31 March 2022; Accepted: 17 May 2022;
Published: 17 June 2022.
Edited by:
Hans Olav Thulesius, Linnaeus University, SwedenReviewed by:
Ferdinando Petrazzuoli, Lund University, SwedenMichael Kuo, Tung Wah College, Hong Kong SAR, China
Copyright © 2022 Li, Cui, Jørgensen, Cheng, Li and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huilan Xu, eGhsX2NzdUAxNjMuY29t
†These authors have contributed equally to this work