
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health , 03 June 2022
Sec. Public Health Policy
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.907012
 Sara Monteiro Pires1*
Sara Monteiro Pires1* Grant M. A. Wyper2
Grant M. A. Wyper2 Annelene Wengler3
Annelene Wengler3 José L. Peñalvo4Romana Haneef5Declan Moran6
José L. Peñalvo4Romana Haneef5Declan Moran6 Sarah Cuschieri7
Sarah Cuschieri7 Hernan G. Redondo1Robby De Pauw8,9Scott A. McDonald10Lynelle Moon11
Hernan G. Redondo1Robby De Pauw8,9Scott A. McDonald10Lynelle Moon11 Jad Shedrawy12Elena Pallari13Periklis Charalampous14
Jad Shedrawy12Elena Pallari13Periklis Charalampous14 Brecht Devleesschauwer8,15Elena Von Der Lippe3
Brecht Devleesschauwer8,15Elena Von Der Lippe3Objectives: Quantifying the combined impact of morbidity and mortality is a key enabler to assessing the impact of COVID-19 across countries and within countries relative to other diseases, regions, or demographics. Differences in methods, data sources, and definitions of mortality due to COVID-19 may hamper comparisons. We describe efforts to support countries in estimating the national-level burden of COVID-19 using disability-adjusted life years.
Methods: The European Burden of Disease Network developed a consensus methodology, as well as a range of capacity-building activities to support burden of COVID-19 studies. These activities have supported 11 national studies so far, with study periods between January 2020 and December 2021.
Results: National studies dealt with various data gaps and different assumptions were made to face knowledge gaps. Still, they delivered broadly comparable results that allow for interpretation of consistencies, as well as differences in the quantified direct health impact of the pandemic.
Discussion: Harmonized efforts and methodologies have allowed for comparable estimates and communication of results. Future studies should evaluate the impact of interventions, and unravel the indirect health impact of the COVID-19 crisis.
The spread of coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was declared as a pandemic by the World Health Organization (WHO) on the 11th of March 2020 (1). Since the outbreak was first identified in December 2019 in Wuhan, China, the public health and social impact of the disease has evolved to be enormous. It has affected every country, population and person in the world, either directly or indirectly.
Most efforts to understand and compare the health impact of COVID-19 across populations have been made using incidence and mortality-based metrics. However, understanding and quantifying the combined impact of morbidity and mortality is a necessary step to assess both the within-country impact of COVID-19 relative to other causes of disease and injury, in sub-national areas or demographics, and to standardize comparisons between countries. So far, studies of this type have been relatively sparse, presumably due to a mixture of factors, and likely hindered by the need for real-time information, and the lack of analytical capacity and standardized, and robust methods. Summary measures of population health, such as disability-adjusted life years (DALYs), offer a more detailed estimation of the direct impact of the disease in a given population, and can provide future opportunities to assess the indirect impact of the pandemic as a result of preventive measures such as national lockdowns, or of disruption of vital health care services.
The DALY is the key metric in the Global Burden of Disease (GBD) study, a well-resourced and long-standing initiative by the WHO and the Institute for Health Metrics and Evaluation (IHME) (2). The GBD study aims at providing standardized procedures and comparable estimations of a large number of diseases and risk factors across the world. With a narrower scope, local, national, or regional burden of disease studies are useful for quantifying specific populations' health impacts of context-relevant diseases and risk factors, accounting for local characteristics, demographics, and knowledge, and sometimes relying in more granular information complementing GBD's information (3). National burden of disease studies have the advantages of access to country-specific, real-time health and surveillance data, as well as the proximity to local experts on national health systems and public health that are key to the interpretation and usability of the study results. They are also able to involve disease, risk, and methodology experts, as well as facilitate the communication and translation of results to policy making. In Europe, countries such as Belgium, France, Germany, the Netherlands, Scotland, and Sweden, have launched national burden of disease studies in recent years (4–7). Globally, national burden of disease studies (8, 9) and projects dedicated to the burden of specific groups of diseases [for example foodborne diseases (10–14), or infectious diseases more broadly (15)] have also been launched. There is still a pressing need to build capacity in additional countries to estimate the burden of diseases at the national level, and particularly for estimating the burden of new diseases such as COVID-19. As disease burden estimations are dependent on methodological choices such as data collection and metrics used, an international consensus is useful to enhance transparency and produce estimates which are comparable.
The European Burden of Disease Network (burden-eu) was established in 2019 to act as a technical platform for integrating and strengthening capacity in burden of disease assessment across Europe and beyond (16). It is structured in technical and disease-focused working groups. At the moment of writing this review (February 2022), the burden-eu gathers 330 individual members from 53 countries. Capacity building is one of the key pillars of burden-eu, and the ultimate goal of several of its activities. Since the start of the pandemic, burden-eu has developed tools and initiatives to support countries in implementing national burden of COVID-19 disease studies. These included developing and harmonizing methodologies, disseminating technical materials, launching a dedicated working group and online discussion forum, exchanging experiences and supporting capacity building, and assistance with the planning of future burden of disease studies.
We reviewed the approach and output of the burden-eu to supporting countries in estimating the disease burden caused by COVID-19 at national-level. First, we present the use of the consensus methodology, data input requirements, and solutions to data gaps to estimate national-level burden of COVID-19. At a second step, we provide an overview of national-level studies that have carried out COVID-19 disease burden estimations with study periods between January, 2020 and December, 2021 and conducted across the burden-eu countries. Further, we describe the Networks' capacity-building activities and additional actions to address the impact of COVID-19 pandemic by improving data collection and data sharing in the European Union.
In mid-2020, a burden-eu working group convened to establish an approach to support the network's members to establish national studies. First, the group discussed the methodology, data requirements, and resources needed to implement a national study. Based on the output of these discussions, a comprehensive protocol was published on the network's website, and a scientific article was published (17, 18). To present this methodology, share already finalized studies, and discuss challenges and opportunities for future studies, the burden-eu organized a public webinar, which was attended by over 100 participants in November 2020 (19). The network's website collects and continuously posts all published articles related to the burden of COVID-19 (20). The burden-eu also formed the Burden of COVID-19 Task Force, which is open to all network members conducting or interested in implementing national studies. This task force aims to share experiences in national burden of COVID-19 studies; support each other with disease burden calculations, model assumptions and data gaps; harmonize methodologies and align strategies for communicating results; and discuss research and upcoming evidence on long-COVID. The group meets regularly to work toward achieving these aims. Lastly, the burden-eu launched an online discussion forum, where members can post questions and receive answers from peers in an interactive and rapid way.
The protocol to estimate the burden of COVID-19 at national level specified data requirements, reflecting the data availability and quality of data inputs by country, offered solutions to overcome data gaps, and a consensus approach for calculations (17). It presented the approach in three steps: defining study parameters; estimating the impact of morbidity, in terms of years lived with disability (YLD); and estimating the impact of mortality, in terms of years lost to premature death (YLL) (Figure 1).
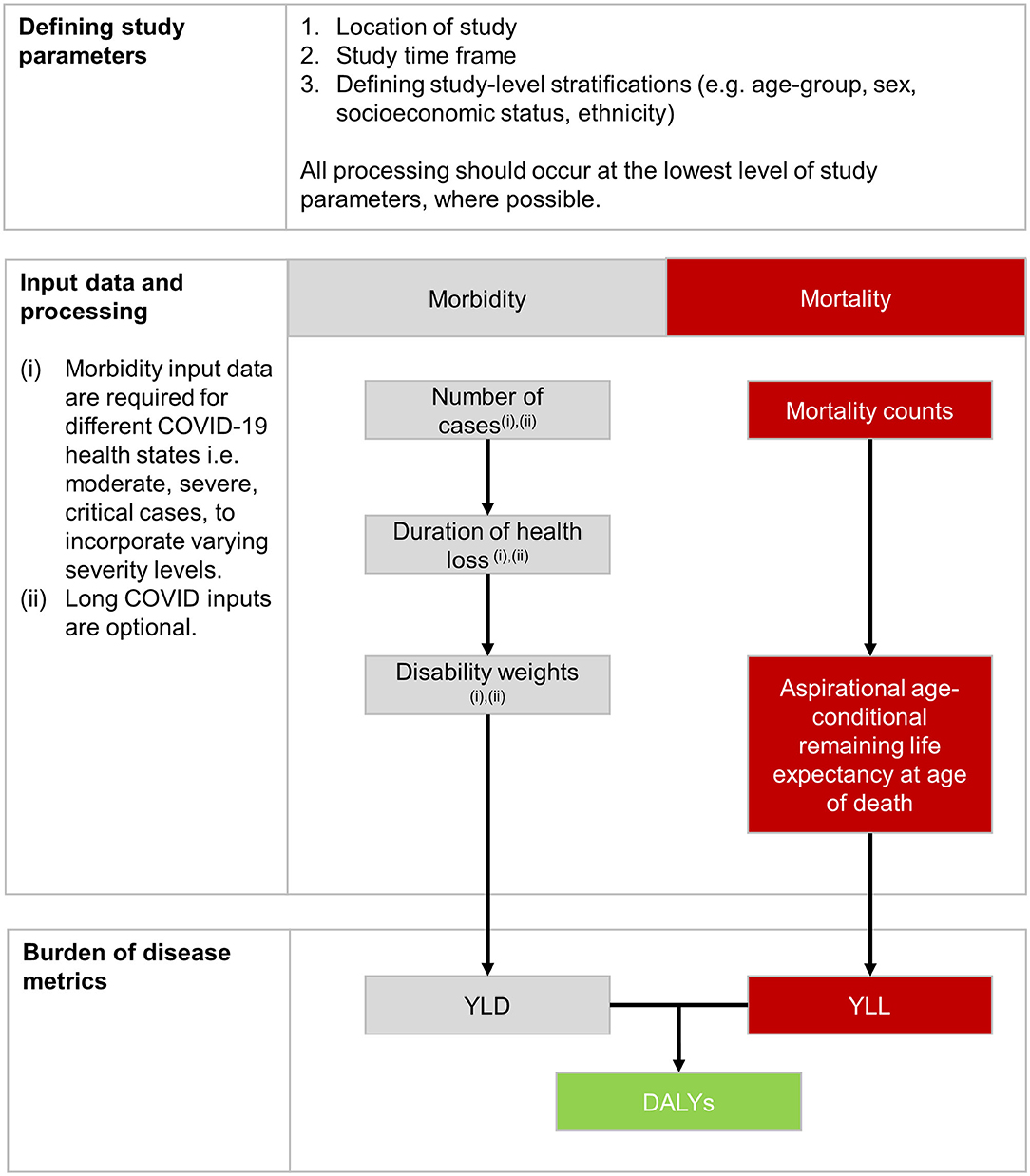
Figure 1. Steps and processes for the calculation of disability adjusted life years (DALYs) of COVID-19 at national level.
DALYs quantify the full population health impact and are calculated by summing YLD and YLL. DALYs can be estimated based on grouped characteristics of interest, such as demographics (e.g., age, sex, socioeconomic status, and ethnicity), geographical region, or time.
Diseases caused by an infectious agent may consist of one or more health outcomes, which can have acute and/or chronic phases, with varied durations. A major methodological choice for calculating YLDs is whether to use an incidence- or prevalence-based approach. An incidence-based approach has been considered the most suitable approach for estimating the burden of infectious diseases (21). In this approach, all health outcomes and the associated disease burden, including those health outcomes occurring long after the acute infection, are assigned to the initial event, i.e., the infection with the agent (22). A wide range of acute symptoms of COVID-19 have been reported, ranging from mild to severe respiratory symptoms; the latter often leading to hospitalization and intensive care (23). Wyper et al. (17) proposed a disease model defining the direct health outcomes of COVID-19, which can be adapted to reflect the data available in each country and evidence that becomes available with time. For example, the model should be adapted to reflect differences in restrictions and triaging across hospitals, regions, and countries, and how the state of the pandemic increases the pressure on the healthcare system, affecting the quality and access to its services. This emphasizes that the distribution of disease incidence across health states is likely to vary by location, as prevention and control strategies have varied during the pandemic (24).
In addition to acute symptoms, a proportion of patients have reported long-lasting symptoms of COVID-19, a multi-faceted condition referred to as post-acute sequelae, post-acute COVID-19 syndrome, or “long-COVID” (25, 26). At the time of writing this review, information on the incidence of the various manifestations of long-COVID and related health outcomes, as well as their duration and severity, were still sparse. Thus, only a few studies have included long-COVID in burden of disease assessments, and the ones that did relied on assumptions and simplifications to overcome data gaps (27–29). Several cohort studies have been launched globally to collect such data; once these data are available, burden of disease estimations can be updated to provide more complete and accurate results of the burden of COVID-19 at national and global levels. The development of an internationally recognized standard definition for long-COVID would greatly facilitate this process (30). In addition, it may be relevant to consider the further development of more granular disability weights. At present, there is a single disability weight to capture post-acute consequences of acute infection, and given the range of symptoms reported for COVID-19, a mild, moderate and severe characterization of disability weights would be a useful development.
When estimating YLL, two inputs are required: the number of deaths; and normative life expectancy. The use of an aspirational life table is the gold standard approach for calculating YLL, as it ensures internationally comparable results, which are particularly important during a public health emergency of international concern (31). It is also essential that YLL is not adjusted for the differences in life expectancy between persons with or without comorbidities. A number of researchers have indicated that such methods are required, but doing so would remove the ability to make comparisons with other diseases or injuries, between different countries, or across time periods. Furthermore, these adjustments could lead to unethical outcomes if the application of public health interventions are guided by YLL, as disadvantaged regions would suffer the most if YLL is adjusted for comorbidities or for lifestyle risk factors; these regions would be deemed to have “less to gain” compared with regions with a lower prevalence of the same comorbidities and/or lifestyle risk factors.
Estimates of the number of deaths will largely depend on data availability. Some countries may have timely mortality data available by mutually exclusive causes of death, in which case the underlying cause of death should be used. Depending on the national death registration policy, some death certificates may indicate ill-defined causes of death. If possible, then redistribution can be considered to refine estimates, in line with methods used for allocating ill-defined deaths to non-COVID-19 causes of death. The definition of COVID-19 deaths may also be a challenge, and vary between countries, despite the standard definition proposed by the WHO (32). Where data allow for estimates to be calculated according to different definitions, it would be preferable to include these as scenario analyses. Doing this would allow for some additional triangulation when interpreting estimates, and may help to provide a bridge between studies that have only have access to a certain mortality definition. The WHO proposed the definition of a death due to COVID-19 as “a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID-19 (e.g., trauma) (32).”
COVID-19 DALY estimates have been published for various countries within the burden-eu. Up to the time of finalizing this review [14th February, 2022], burden of disease estimates from Australia, Denmark, Germany, Ireland, Malta, the Netherlands, Scotland have been published (Table 1); Belgium and France are finalizing their estimates for publication, whilst Cyprus and Sweden have embarked upon data collection for their national study. The methods used are aligned with the guidelines developed by burden-eu for estimating DALYs due to COVID-19.
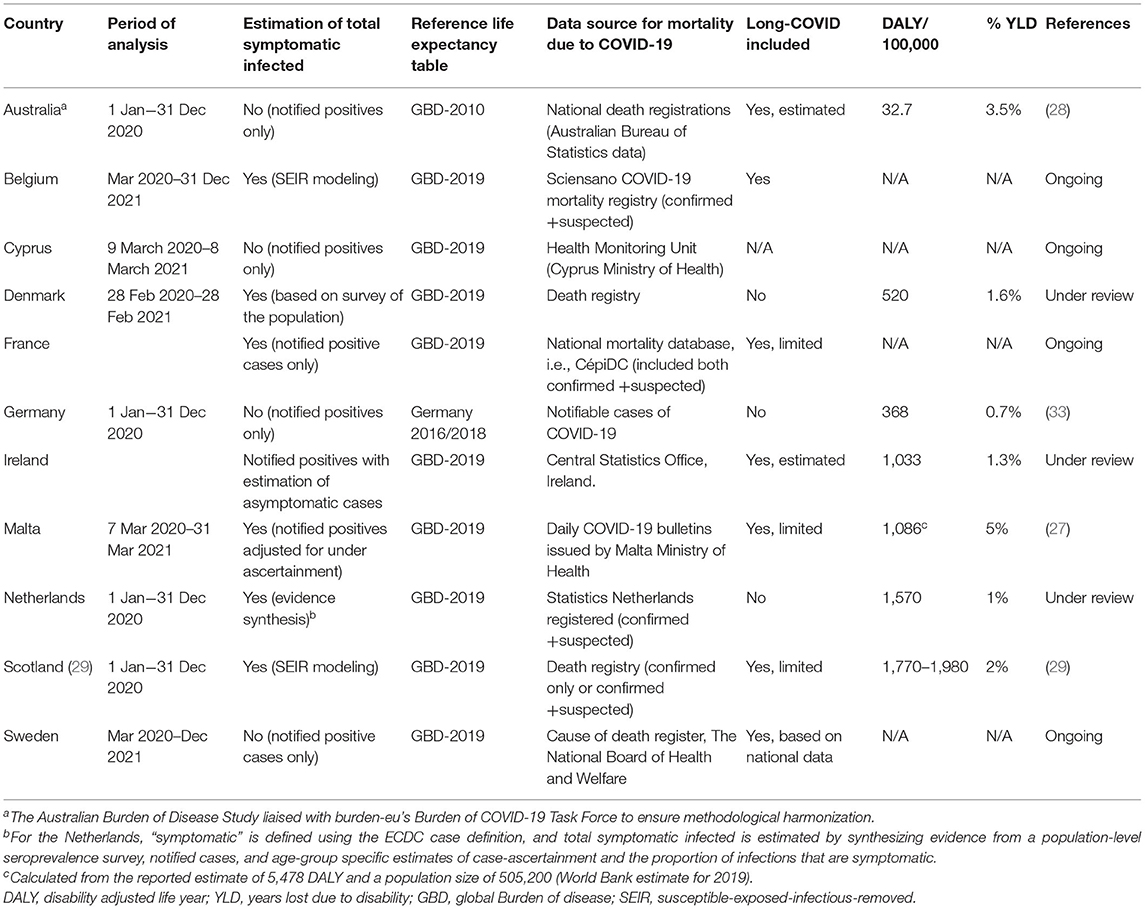
Table 1. Overview of published and ongoing National Burden of COVID-19 studies, methodological characteristics, and main results published between January 2020 and December 2021.
Table 1 maps national-level COVID-19 burden of disease studies undertaken across European countries and beyond over the period between January 2020 and December 2021. Currently available estimates show that the direct burden of COVID-19 has varied across countries, but that the contribution of YLL (i.e., of mortality) to the overall burden has been consistently high (between 95 and 99%). Other studies, not supported by burden-eu, have estimated DALYs of COVID-19 in countries globally, for example in India, Iran, Mexico and Korea (34–37). Aligned with the findings of studies here presented, the estimated burden of disease varied across countries, but the contribution of YLL to overall DALY was large.
To adjust to the type and extent of data available and to overcome data gaps, countries embarking on these disease burden analyses made adaptations to the proposed approaches. Describing these methodological choices is important for well-informed comparisons and for knowledge translation at national and international levels. For example, some studies expanded upon the core health states defined by the consensus model. Scotland, Malta, Ireland, France, and Australia included estimates of post-acute consequences following the acute infection period, based on published transition probabilities and durations. Germany was the only country to define mild cases in YLD calculations. The Netherlands employed adjustment factors to correct for underreporting of hospital admissions and deaths. It was recognized that notified cases greatly underestimated the true incidence of infections, particularly in the first period of the pandemic, and thus evidence from seroprevalence survey data, case-ascertainment, and other sources were synthesized to estimate the cumulative incidence of symptomatic SARS-CoV-2 infection. There were also variations in how the duration of health states were defined. Most countries used durations derived from their national data collections. Ireland used the GBD 2019 duration for lower respiratory infections, due to a lack of national evidence on the duration at each health state level. Scotland used daily prevalence estimates from a Susceptible-Exposed-Infectious-Removed (SEIR) transmission model, and daily hospital prevalence data, so did not require any definition of duration. All studies used the GBD aspirational life expectancy life table to value the loss of life, with the exception of Germany that employed the highest observed age-specific residual life expectancy among all the German federal states based on the 2016/2018 life tables.
The rapid and wide spread of COVID-19 cases, together with the efforts of countries and international health agencies to monitor the disease, and the overflow of patients to medical care have generated a wealth that can help to fully characterize the epidemiology and clinical aspects this new disease. The emergency of pandemic has introduced an unprecedented response by the research community in demand of collaborative data sharing networks to enrich and accelerate informed decision making. International collaboration to collect, store, and manage relevant health and epidemiological data regarding COVID-19 helps filling data gaps and facilitates robust estimations, including burden of disease metrics, that can help and policy evaluation. In response to the emergency calls launched by the European Commission in May 2020, the unCoVer (Unraveling Data for Rapid Evidence-Based Response to COVID-19) project was sponsored as a Coordinated Support Action. The unCoVer is defined as a functional network of 29 partners that was established to bring together European and international expertise to monitor, identify, and facilitate the access and utilization of COVID-19 patient's data, to identify knowledge gaps, underrepresented populations, and proactively seek synergies with complementary clinical databases. The unCoVer's members are capable of collecting and utilizing data derived from the response and provision of care to COVID-19 patients by health systems across Europe and internationally. The data within the network comprise mostly information from electronic medical records from hospitals, but also national surveillance data, and registries, and is reached through a federated data infrastructure that ensures data protection and ethical and legal compliance. Thus far, they integrate information from over 20 databases and a sizeable number of COVID-19 patients, which is anticipated to increase as databases are being continuously updated (38). These data may inform future burden of disease assessments, by gaining a deeper understanding on the disease model and variations among heterogeneous groups of patients, including COVID-19 manifestations in vulnerable population subgroups, and shedding light into post-acute COVID-19 conditions that may add to the YLD component of the DALY.
The scientific network “BoCO-19—The Burden of Disease due to COVID-19” was launched in May 2021, coordinated by the Robert Koch Institute in Germany and is funded for a period of two years (39). The overall aim of BoCO-19 is to harmonize burden of disease methodology for the surveillance of dynamic outbreaks, using COVID-19 as an example. The BoCO-19 has established a functional network of partner institutions from countries from the South-East Europe, Southern Caucasus and Central Asia. The burden-eu serves as an additional project partner, by contribution with the output of discussion of methodologies for measuring the disease burden of COVID-19. The vision of the BoCO-19 project is to provide a scientific a platform for intensive knowledge exchange and application of a consistent methodology considering context-specific conditions toward calculating the burden of the COVID-19 disease in the pandemic monitoring stage. Efforts are also focused on the dissemination of the harmonized methodology and estimates of the disease burden indicators to the wider scientific community.
The initial capacity building activities have allowed national studies to get off the ground and produce initial sets of results. While burden of COVID-19 studies dealt with various data gaps and a number of assumptions made in the face of knowledge gaps, they delivered broadly comparable results that allow for an interpretation of consistencies, as well as differences in the quantified direct health impact of the first year of the pandemic. Furthermore, whilst many experienced with national burden of disease studies have been among those carrying out COVID-19 DALY studies, some countries have had unintended benefits of their COVID-19 studies, which have led to novel advances in their projects. In particular, the French and Irish studies have now launched their independent DALY studies, which can be augmented with future non-COVID-19 assessments.
At first glance, it can seem challenging to validly compare DALY COVID-19 estimates given difference in underlying data sources, data collection systems, degree of ascertainment of the true incidence of infection by reported cases, disability durations, and definitions of mortality due to COVID-19. Close adherence to the aforementioned protocol (17, 18) by several of the national studies has greatly facilitated comparisons of COVID-19 burden across countries. Given that YLL—which is dependent on complete and accurate recording of death due to COVID-19—accounts for the vast majority of the disease burden, attention to cause of death definitions and addressing under-reporting in COVID-19 deaths will have the most impact on the validity of national estimates, and thus also the comparability of estimates.
These findings illustrate how burden of disease indicators, and standardization of approaches where applicable, can be useful for monitoring within- and across-country public health in an ongoing pandemic. As the push for additional countries and regions to follow continues, our efforts to assist countries to translate their results in a within- and across-country setting will also continue through our Knowledge Translation Working Group. These activities will allow for users to see that collaborative benefits can have both local and wider benefits.
At the onset of the pandemic, we assessed the levels of vulnerability to severe outcomes from COVID-19 infection across Europe (40). This indicated that increasing pre-existing levels of vulnerability were likely to lead to inequalities in adverse outcomes due to the differences in demographic construct and population health levels within individual countries. This means that, even when standardizing results, interpretation of the success or failure between comparisons is not always clear cut, because the level of threat faced by individual countries was unequal. Integrating the impact of inequality both within- and across-countries is important as we progress our work. Evidence has indicated that socioeconomic inequality-attributable COVID-19 DALYs are 40% in Scotland, a result which has been borne out of a legacy of systemic inequality (41). As the pandemic has evolved, monitoring inequalities within countries will give indications into how successful attempts have been to mitigate inequalities, e.g., by prioritizing certain groups for vaccination before others. Communicating these results are important for national and local policy-makers, to scale the size of challenges faced on the public health and health and social care systems of a country.
When our activities began, there was no vaccination for COVID-19. While it is certainly not sufficient alone, vaccination remains the primary tool in preventing deaths and severe illness from COVID-19. Previous evidence has indicated the extent of deaths averted through vaccination in countries of Europe (42). Through continuous monitoring of COVID-19 DALYs, an area of interest will be to start to estimate the DALYs averted through vaccination programmes.
Furthermore, efforts thus far have mainly focused on the direct impact of COVID-19. Future studies need to unravel the indirect health impact of the COVID-19 crisis, linked, e.g., to delayed health care use, increases in domestic violence, or decreases in road traffic accidents. Due to its comprehensive nature, the DALY metric would be well-suited to estimate the overall health impact of the crisis, combining both positive and negative health effects, over a wide range of health outcomes. In the near future, we will continue working toward more complete characterization of the risks, severities, and duration of health outcomes, comprising “Long-COVID.”
SP, GW, AW, JP, and EV designed the review and wrote the first version of the manuscript. All authors contributed to the review and provided input to the text. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to acknowledge the networking support from COST Action CA18218 (European Burden of Disease Network; https://www.burden-eu.net) and supported by COST (European Cooperation in Science and Technology; https://www.cost.eu).
1. WHO. WHO Director-General's opening remarks at the media briefing on COVID-19 – 11. (2020). Available online at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-−11-march-2020
2. Murray CJL, Ezzati M, Flaxman AD, Lim S, Lozano R, Michaud C, et al. GBD 2010: design, definitions, and metrics. Lancet. (2012) 380:2063–6. doi: 10.1016/S0140-6736(12)61899-6
3. Haneef R, Schmidt J, Gallay A, Devleesschauwer B, Grant I, Rommel A, et al. Recommendations to plan a national burden of disease study. Arch Public Heal. (2021) 79:1–8. doi: 10.1186/s13690-021-00652-x
4. Rommel A, von der Lippe E, Plaß D, Wengler A, Anton A, Schmidt C, et al. BURDEN 2020—Burden of Disease in Germany at the National and Regional Level. Bundesgesundh Gesundheitsforsch Gesundheitssch. (2018) 61:1159–66. doi: 10.1007/s00103-018-2793-0
5. Hilderink HBM, Plasmans MHD, Poos MJJC, Eysink PED, Gijsen R. Dutch DALYs, current and future burden of disease in the Netherlands. Arch Public Health. (2020) 78:85. doi: 10.1186/s13690-020-00461-8
6. Devleesschauwer B. Country Report: the Belgian National Burden of Disease Study 2020. Eur J Public Health. (2018) 28:cky213.830. doi: 10.1093/eurpub/cky213.830
7. Wyper G, Wyper G, Grant I, Fletcher E, De MT, Moro H, et al. Scottish Burden of Disease (SBOD) study: a population health surveillance system for meaningful action. Eur J Public Health. (2021) 31:ckab164.511. doi: 10.1093/eurpub/ckab164.511
8. Yoon SJ, Go DS, Park H, Jo MW, Oh IH, Kim YE. The Korean National Burden of disease study: from evidence to policy. J Korean Med Sci. (2019) 34(Suppl 1):e89. doi: 10.3346/jkms.2019.34.e89
9. Australian Institute of Health Welfare. Australian Burden of Disease Study: Impact and causes of illness and death in Australia 2018, Summary. Canberra, ACT: Australian Institute of Health and Welfare (2021). Available online at: https://www.aihw.gov.au/reports/burden-of-disease/abds-impact-and-causes-of-illness-and-death-in-aus/summary
10. Pires SM, Jakobsen LS, Ellis-Iversen J, Pessoa J, Ethelberg S. Burden of disease estimates of seven pathogens commonly transmitted through foods in Denmark, 2017. Foodborne Pathog Dis. (2019) 17:322–39. doi: 10.1089/fpd.2019.2705
11. Havelaar AH, Haagsma JA, Mangen MJJ, Kemmeren JM, Verhoef LPB, Vijgen SMC, et al. Disease burden of foodborne pathogens in the Netherlands, 2009. Int J Food Microbiol. (2012) 156:231–8. doi: 10.1016/j.ijfoodmicro.2012.03.029
12. Scallan E, Hoekstra RM, Mahon BE, Jones TF, Griffin PM. An assessment of the human health impact of seven leading foodborne pathogens in the United States using disability adjusted life years. Epidemiol Infect. (2015) 143:2795–804. doi: 10.1017/S0950268814003185
13. Kumagai Y, Gilmour S, Ota E, Momose Y, Onishi T, Bilano VLF, et al. Estimating the burden of foodborne diseases in Japan. Bull World Health Organ. (2015) 93:540–9C. doi: 10.2471/BLT.14.148056
14. Gkogka E, Reij MW, Havelaar AH, Zwietering MH, Gorris LGM. Risk-based estimate of effect of foodborne diseases on public health, Greece. Emerg Infect Dis. (2011) 17:1581–90. doi: 10.3201/eid1709.101766
15. van Lier A, McDonald SA, Bouwknegt M, Kretzschmar ME, Havelaar AH, Mangen M-JJ, et al. Disease burden of 32 infectious diseases in the Netherlands, 2007-2011. PLoS ONE. (2016) 11:e0153106. doi: 10.1371/journal.pone.0153106
16. Devleesschauwer B. European burden of disease network: strengthening the collaboration. Eur J Public Health. (2020) 30:2–3. doi: 10.1093/eurpub/ckz225
17. Wyper GMA, Assunção RMA, Colzani E, Grant I, Haagsma JA, Lagerweij G, et al. Burden of disease methods: a guide to calculate COVID-19 disability-adjusted life years. Int J Public Health. 66:619011. doi: 10.3389/ijph.2021.619011
18. European Burden of Disease Network. Burden of Disease of COVID-19 Protocol for Country Studies. (2021). Available online at: https://www.burden-eu.net/0
19. European Burden of Disease Network. [Webinar] Quantifying COVID-19 Disease Burden [Internet]. (2020). Available online at: https://www.burden-eu.net/activities/webinars/194-quantifying-covid-19-disease-burden
20. European Burden of Disease Network [Internet]. Available online at: https://www.burden-eu.net/outputs/covid-19
21. Wyper GMA, Grant I, Fletcher E, Chalmers N, McCartney G, Stockton DL. Measuring disability-adjusted life years (DALYs) due to COVID-19 in Scotland, 2020. Arch. Public Health. (2022) 80:105. doi: 10.1186/s13690-022-00862-x
22. Devleesschauwer B, Havelaar AH, Maertens De Noordhout C, Haagsma JA, Praet N, Dorny P, et al. DALY calculation in practice: a stepwise approach. Int J Public Health. (2014) 59:571–4. doi: 10.1007/s00038-014-0553-y
23. Hajjar LA, Costa IBS da S, Rizk SI, Biselli B, Gomes BR, Bittar CS, et al. Intensive care management of patients with COVID-19: a practical approach. Ann Intensive Care. (2021) 11:36. doi: 10.1186/s13613-021-00820-w
24. Wyper GMA, Grant I, Fletcher E, Chalmers N, McCartney G, Stockton DL. Prioritising the development of severity distributions in burden of disease studies for countries in the European region [Internet]. Arch. Public Heal. (2020) 78:3. doi: 10.1186/s13690-019-0385-6
26. Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, et al. Post-acute COVID-19 syndrome. Nat Med. (2021) 27:601–15. doi: 10.1038/s41591-021-01283-z
27. Cuschieri S, Calleja N, Devleesschauwer B, Wyper GMA. Estimating the direct Covid-19 disability-adjusted life years impact on the Malta population for the first full year. BMC Public Health. (2021) 21:1827. doi: 10.1186/s12889-021-11893-4
28. Australian Institute of Health Welfare. The First Year of COVID-19 in Australia: Direct and Indirect Health Effects. Canberra, ACT (2021). Available online at: https://www.aihw.gov.au/getmedia/a69ee08a-857f-412b-b617-a29acb66a475/aihw-phe-287.pdf.aspx?inline=true
29. Wyper GMA, Fletcher E, Grant I, McCartney G, Fischbacher C, Harding O, et al. Measuring the direct population impact of COVID-19 in Scotland, 2020: estimating disability-adjusted life years (DALYs) during the first full calendar year. SocArXiv (2021).
30. World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus. Geneva: World Health Organization (2021). Available online at: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1
31. Devleesschauwer B, McDonald SA, Speybroeck N, Wyper GMA. Valuing the years of life lost due to COVID-19: the differences and pitfalls. Int. J. Public Health. (2020) 65:719–20. doi: 10.1007/s00038-020-01430-2
32. World Health Organization. International Guidelines for Certification and Classification (Coding) of COVID-19 as Cause of Death [Internet]. Geneva: World Health Organization (2020). Available online at: https://www.who.int/classifications/icd/Guidelines_Cause_of_Death_COVID-19.pdf
33. Rommel A, Lippe E von der, Plass D, Ziese T, Diercke M, Heiden MA der, et al. The COVID-19 disease burden in Germany in 2020. Dtsch Arztebl Int. (2021) 118:145–51. doi: 10.3238/arztebl.m2021.0147
34. Taheri Soodejani M, Abedi Gheshlaghi L, Bahrevar V, Hosseini S, Lotfi MH. Burden of severe COVID-19 in center of Iran: results of disability-adjusted life years (DALYs). Int J Mol Epidemiol Genet. (2021)12:120–5.
35. Jo M-W, Go D-S, Kim R, Lee SW, Ock M, Kim Y-E, et al. The Burden of disease due to COVID-19 in Korea using disability-adjusted life years. J Korean Med Sci. (2020) 35:e199. doi: 10.3346/jkms.2020.35.e199
36. Salinas-Escudero G, Toledano-Toledano F, García-Peña C, Parra-Rodríguez L, Granados-García V, Carrillo-Vega MF. Disability-adjusted life years for the COVID-19 pandemic in the mexican population. Front Public Health. (2021) 9:686700. doi: 10.3389/fpubh.2021.686700
37. Singh BB, Devleesschauwer B, Khatkar MS, Lowerison M, Singh B, Dhand NK, et al. Disability-adjusted life years (DALYs) due to the direct health impact of COVID-19 in India, 2020. Sci Rep. (2022) 12:2454. doi: 10.1038/s41598-022-06505-z
38. Peñalvo JL, Mertens E, Ademović E, Akgun S, Baltazar AL, Buonfrate D, et al. Unravelling data for rapid evidence-based response to COVID-19: a summary of the unCoVer protocol. BMJ Open. (2021). doi: 10.1136/bmjopen-2021-055630
39. European Burden of Disease Network. BoCO-19: Towards a Harmonization of Population Health Metrics for the Surveillance of Dynamic Outbreaks. European Burden of Disease Network (2021). Available online at: https://www.burden-eu.net/news/spotlight/323-boco-19
40. Wyper GMA, Assunção R, Cuschieri S, Devleeschauwer B, Fletcher E, Haagsma JA, et al. Population vulnerability to COVID-19 in Europe: a burden of disease analysis. Arch Public Health. (2020) 78:47.
41. Wyper GMA, Fletcher E, Grant I, Harding O, de Haro Moro MT, Stockton DL, et al. Inequalities in population health loss by multiple deprivation: COVID-19 and pre-pandemic all-cause disability-adjusted life years (DALYs) in Scotland. Int J Equity Health. (2021) 20:1–7. doi: 10.1186/s12939-021-01547-7
42. Meslé MM, Brown J, Mook P, Hagan J, Pastore R, Bundle N, et al. Estimated number of deaths directly averted in people 60 years and older as a result of COVID-19 vaccination in the WHO European Region, December 2020 to November 2021. Euro Surveill. (2021) 26:2101021. doi: 10.2807/1560-7917.ES.2021.26.47.2101021
Keywords: DALY, disability-adjusted life year, COVID-19, coronavirus, capacity building, European Burden of Disease Network
Citation: Pires SM, Wyper GMA, Wengler A, Peñalvo JL, Haneef R, Moran D, Cuschieri S, Redondo HG, De Pauw R, McDonald SA, Moon L, Shedrawy J, Pallari E, Charalampous P, Devleesschauwer B and Von Der Lippe E (2022) Burden of Disease of COVID-19: Strengthening the Collaboration for National Studies. Front. Public Health 10:907012. doi: 10.3389/fpubh.2022.907012
Received: 29 March 2022; Accepted: 10 May 2022;
Published: 03 June 2022.
Edited by:
Mohd Hafiz Mohd, Universiti Sains Malaysia (USM), MalaysiaReviewed by:
Jomar Fajardo Rabajante, University of the Philippines Los Baños, PhilippinesCopyright © 2022 Pires, Wyper, Wengler, Peñalvo, Haneef, Moran, Cuschieri, Redondo, De Pauw, McDonald, Moon, Shedrawy, Pallari, Charalampous, Devleesschauwer and Von Der Lippe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sara Monteiro Pires, c21waUBmb29kLmR0dS5kaw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.