 Andrea Donnell
Andrea Donnell Chandana Unnithan1
Chandana Unnithan1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 12 July 2022
Sec. Digital Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.900733
Background: The potential for digital initiatives for opioid harm reduction is boundless. Synthesized evidence on current interventions and their efficacy are emerging. This scoping review is an effort to aggregate Canadian and Australian digital health initiatives used to prevent opioid-related deaths and minimize harm, prior to and particularly during the pandemic of SARs-COVID-19, when the crisis escalated.
Methods: The Joanna Briggs Institute's methodological framework for conducting scoping reviews was used. Peer reviewed and gray literature published between January 2016 to October 2021 were included. Search translation was performed across CINAHL, Cochrane, SCOPUS, MEDLINE Complete, and ProQuest Public Health with consistent use of key search terms. Citation checks were also conducted. Studies included were written in English and reported on digital technologies to prevent opioid-related harm and/or mortality in participants aged 18 years or older in Australia and Canada.
Results: A total of 16 publications were included in the final analysis (Australia = 5; Canada = 11). The most frequently reported digital technologies were telehealth to support access to treatment (n = 3) and mobile applications for overdose monitoring and prevention (n = 3). Telehealth-delivered opioid replacement therapy demonstrated equal outcomes and treatment retention rates compared to in-person and mobile applications for overdose monitoring demonstrated lifesaving capability through direct linkages with emergency response services.
Conclusions: Digital interventions to minimize opioid crisis related harm and overdose prevention are fast emerging in Australia and Canada. During the pandemic, the crisis escalated in both countries as a public health emergency, and different initiatives were trialed. Digital harm reduction solutions via mobile apps (or SaaS solutions) were found to have the potential to prevent accidental overdose deaths and save lives, if rendered through privacy preserved, secure and trust enabled methods that empower users. Knowledge sharing between the two countries, relating to suitable interventions, may add significant value in combatting the escalating opioid crisis in the post pandemic era.
According to World Health Organization, more than 70% of the 500,000 deaths globally attributable to drug use are related to opioids (1). Globalization is playing a crucial role in the developing opioid epidemic, with high rates of opioid prescription, rising extra-medical (synthetic) opioid use, and diversification of the global opioid markets (including the proliferation of highly toxic synthetic opioids) highlighting the problem as a significant public health crisis. The differing socio-political and historical contexts of opioid crises across countries have undoubtedly influenced experiences and approaches to tackling the problem (1).
Canada is the second largest consumer of prescription opioids in the world, with over 20 million prescriptions for opioids being dispensed per year i.e., equivalent to nearly one prescription for every adult over the age of 18 years. In Australia, the National Drug Research Institute (NDRI) reported that extra-medical opioid use was responsible for 2,203 deaths and 32,000 hospital admissions during 2015–2016 (2). Equating to over 70,000 years of life lost, extra-medical opioid use is estimated to cost the Australian government $15.7 billion a year in both health and social costs. As a result of the escalating harm, Canada declared the developing opioid crisis a public health emergency in 2016, while Australia followed 3 years later in 2019 (2).
While the opioid crisis had been a declared public health emergency in Australia and Canada, during the pandemic period of 2020–2021, there was an escalation of the crisis. In Canada, the deaths by overdose in 2020 had exceeded COVID-19 related deaths, making it a twin crisis. Opioid harm reduction and treatment services faced considerable challenges in maintaining access for people that use drugs. These challenges include restrictions of in-person appointments, closure or reduced hours for needle and syringe programs, increased demand for drug treatment, and redeployment of health care staff to support COVID-19 responses (3–5). These challenges have been linked to increased levels of harm through sharing of injecting equipment and overdoses (3, 4). On the other hand, users of opioids had increased as a direct consequence to lockdowns, quarantines, and related mental health challenges (6). Reducing opioid-related harm measures to restrict supply, has resulted in a lateral substitutive shift in supply from one opioid category to the other (7).
Opioids are typically prescribed to manage pain often after a surgery or injury, or for certain health conditions. For example, Fentanyl is a synthetic opiate narcotic prescription drug used primarily for cancer patients with severe pain. Fentanyl is often added to illicit drugs such as heroin, cocaine, or methamphetamines as a powerful enhancer (2). The end user is often unaware of the potential danger and emergency response within the first 10 min of use is critical to the survival of people who have taken drugs contaminated/laced with Fentanyl (1).
The ongoing opioid public health crisis was further exacerbated by the COVID-19 pandemic (8). From the onset of the COVID-19 pandemic in Canada, 5,148 apparent opioid toxicity deaths occurred between April 2020 and December 2020, representing an 89% increase from the same period in 2019 (9). Similarly, in Australia, rates of self-reported non-fatal heroin overdose among those that regularly use stimulant drugs and regularly inject drugs are also escalating (10). A comparison of Australia and Canada was prudent due to similarity in the demographic profiles, healthcare systems and functions, and data coding for hospital and emergency presentations (11). Both countries have historically faced similar challenges in combating the opioid epidemic; however, the timeline differs as to when the crisis became a public health emergency.
Conversely, the ubiquitous availability of mobile technologies and the internet provide health care with new, innovative ways of working to complement traditional opioid use disorder (OUD) models of care by leveraging people's propensity to use digital devices (12). Digital health is the new umbrella term that encompasses e-health, m-health, health informatics, and integration of IoT devices (Internet of Things is the term used for the networking of devices embedded with sensors, software, and other technologies for connecting and exchanging data with other devices and systems over the internet) (13). A comprehensive understanding of how these technologies align with the strategic goals of both the Australian and Canadian opioid crisis-related public health strategies can provide insights on how digital initiatives can be used to address the current gaps. As studies are still emerging in the field, the objective of this research was to synthesize current/emerging initiatives, identify gaps and share key learnings to address this escalating public health emergency in both countries.
A scoping review of the literature analyzing technologies available to reduce opioid-related harm was undertaken using the PCC framework and PRISMA-ScR protocol (14, 15). The wide range of technologies, methods, and results used in OUD research suggests that the use of a scoping review as described by Peters et al. (14) was the most appropriate methodology.
The detailed protocol was registered on Open Science Framework DOI 10.17605/OSF.IO/QSDZ3 or https://osf.io/qsdz3/?view_only=2a09a035b2a6419aa7668e84a72606cb.
Inclusion criteria were informed using the PCC guideline (16):
(P) Participants- Opioid users (medically and/or illicitly) aged 18 years and older in Australia and Canada.
(C) Concept-Digital health technologies to reduce opioid-related harm and mortality, including electronic technologies such as web or computer-based devices and m-health technologies such as mobile phones, tablet devices, and applications.
(C) Context- opioid-related harm reduction and overdose prevention.
Original articles in English were identified from a systematic search of five bibliographic databases including CINAHL, Cochrane, SCOPUS, MEDLINE Complete, and ProQuest Public Health. An eligibility publication year of 2016- was applied to the search criteria, to align with Canada's declaration of the developing opioid crisis as a public health emergency in 2016 (which Australia followed 3 years later in 2019) (2). All identified articles were transferred to Mendeley, a reference management software, to manage study records and all duplicates were removed.
The search strategy included a set of keywords based on the PCC inclusion criteria of opioid use, digital technologies, and harm reduction identified with the help of a library specialist. Studies were included if they were written in English and reported on digital technologies to prevent opioid-related harm and/or mortality in participants aged 18 years or older in Australia and Canada. The final search strategy for the databases is outlined in Supplementary Table 1.
By applying the eligibility criteria, papers were screened for selection using titles and abstracts. Full-text papers were obtained and screened in their entirety for studies that could not be obviously excluded based on the information outlined in the Title and Abstract. The literature review was conducted by the first author and the results were validated by the third author. Studies that did not mention a specific digital intervention (e.g., scoping reviews of m-health applications in which the specific application is not named and described in detail) and those that did not use mortality or opioid-related harm in the context of addiction or overdose (e.g., HIV or hepatitis prevention) were excluded from the review. Systematic and other scoping reviews were excluded when they did not relate to Australia and Canada, however, reference lists of identified studies were reviewed to identify additional relevant studies and citation tracking was performed. The reviewer also contacted the authors of the primary studies, reviews, and subject matter experts for further information to complete the data extraction table (16).
When the relevant papers were selected, the following data were recorded in a spreadsheet: author(s), year of publication, context/setting, country, database source, aims/purpose, methodology, intervention type, intervention category, sample size, outcomes, and any key findings relevant to the scoping review question. As Australia did not have a specific opioid drug health strategy at the time of writing this paper, the digital interventions highlighted in this study are aligned to the Canadian opioid response: access to treatment; access to harm reduction; awareness and prevention; tainted drug supply (17).
In alignment with the JBI reviewer's manual, this scoping review did not assess the quality of the included studies (16). The goal of this review was to gain an overview of the digital health technologies used in relation to opioid use disorder to reduce harm and mortality, not to assess their technical quality although some relevant statistics are presented on their efficacies.
The results of the scoping review were reported in alignment with the PRISMA-ScR Extension fillable checklist outlined in Supplementary Table 2. Data items were grouped according to types of digital intervention and presented in a tabulated format using the categories of intervention, citation, country, aims, methodology, and key findings, and subsequently aligned according to the core pillars of Australia's and Canada's Opioid Drug Health strategies.
The searches from the five electronic databases hit a total of 1,780 records [MEDLINE (n = 118), SCOPUS (n = 19), CINAHL (n = 20), ProQuest Public Health (n = 1,626), Cochrane Library (n = 7)] that led to a total of 1,699 published studies that were then screened after the removal of duplicates and texts before 2016 that had not been detected with the filters. The full search strategy for all databases and results are included in Supplementary Table 1.
A total of 39 full-text papers were retrieved from the different libraries of which reference lists were checked identifying another potential 47 papers. The full-text screening stage of the potential 86 papers led to 70 being excluded for reasons outlined in the PRISMA flowchart in Figure 1. Therefore, a total of 16 papers were identified as being relevant to the scoping review and were included in the final data extraction and narrative account stage.
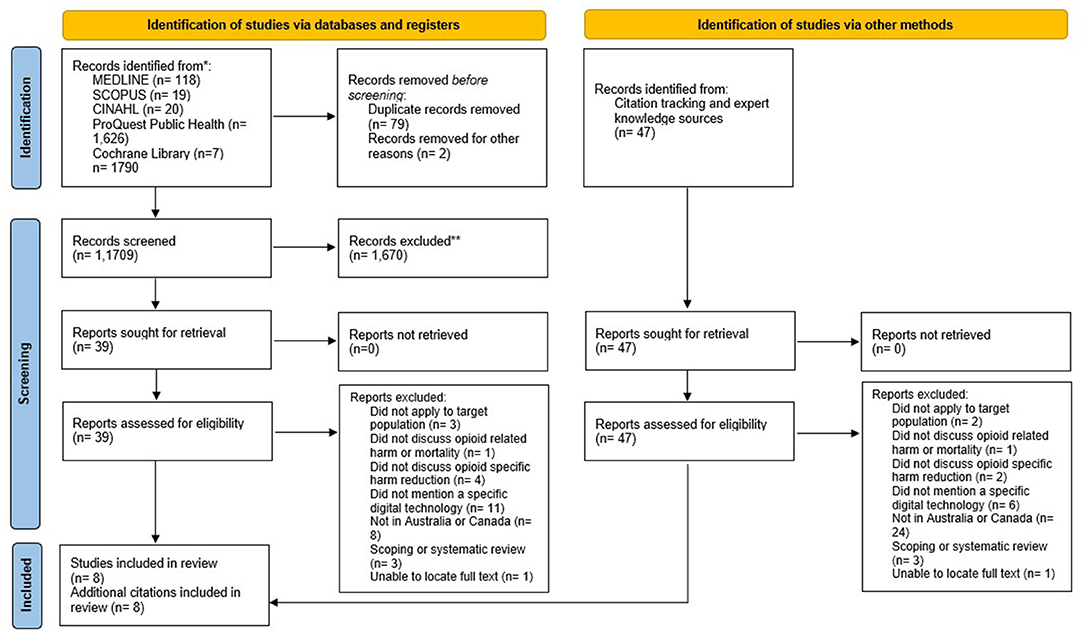
Figure 1. PRISMA-ScR 2020 flow chart of paper identification and selection process.
The research aimed to analyse and synthesize published data on digital interventions that aim to reduce opioid-related harm (mainly overdose death prevention) as well as related harm reduction services, within Australia and Canada. Sixteen papers were included in this review, 5 from Australia and 11 from Canada, and 50% (n = 8) described technologies related to harm reduction, 25% (n = 4) related to education and prevention, 19% (n = 3) related to access to treatment, and 6% (n = 1) related to reducing illicit supply pillars of the drug health strategies. The most frequently reported digital technologies were telehealth to support access to treatment (n = 3) and mobile applications for overdose monitoring and prevention (n = 3), followed by prescription dispensing monitoring programs (n = 2), overdose response buttons (n = 2), and drug checking (n = 2).
The reviewed studies have used three types of study design: 11 used quantitative methods, 1 used qualitative methods, and 2 used mixed methods. Two papers were government papers with no specified methodology. Among the quantitative studies, 7 were action research piloting new technologies, 2 were prospective cohort studies and 2 were retrospective cohort studies. The qualitative and mixed methods studies used a range of semi-structured qualitative interviews (n = 1), pre-post intervention surveys (n = 1), and intervention outcomes testing and surveying (n = 1).
Access to treatment initiatives centers around the active treatment and management of substance use disorders with the goal of cessation or reduction of opioid use (17). Three studies explored digital technologies to support “Access to treatment” for OUD related to telemedicine (18–20). Eibl et al. (18) conducted a retrospective cohort study of patients initiating opioid agonist therapy (OAT) in the province of Ontario, Canada between 2011 and 2012 to understand the retention rates of patients treated via face-to-face vs. via telemedicine. Of the total 3,733 OAT initiating patients, those treated via telemedicine were more likely to be retained in therapy at 1 year than those treated in person at 50 vs. 39%, respectively (n = 1,590; aOR = 1.27; 95% CI 1.14–1.41; p < 0.001). Deacon et al. (19) trialed the use of telehealth to deliver the Australian Treatment Outcomes Profile (ATOP) which is a clinically validated tool used for clinical assessments, care planning, risk screening, and patient-reported outcome measurement in the alcohol and other drugs (AoD) treatment setting. Results found for all ATOP items, nearly all items (76%) reached moderate (0.7) or excellent (0.9) validity when administered over the phone when compared to face-to-face administration.
Morin et al. (20) conducted another retrospective cohort study of 55,924 patients enrolled in OAT in Ontario, Canada between 2011 and 2015 to assess the broader health outcomes of those receiving telemedicine delivered OAT compared to in-person. The findings of the above study reveal that when compared to in-person care, telemedicine was not associated with a higher rate opioid-related emergency department visits (IRR = 1.1, CI: 0.9–1.3) and hospitalisations (IRR = 0.9, 95% CI: 0.9–1.0), 1 year treatment retention (OR = 1.0, 95% CI: 0.9–1.1), or all-cause mortality (OR = 0.9, 95% CI: 0.8–1.0). However, patients who received predominantly telemedicine delivered OAT, had higher rates of overall emergency department presentations (IRR = 1.4, 95% CI: 1.4–1.5, 40% increase), mental health-related emergency department presentations (IRR = 1.5, 95% CI: 1.3–1.6, 50% increase) and mental health hospital admissions (IRR = 1.2, 95% CI: 1.1–1.3, 20% increase) (15).
Among the 4 papers aligned with the “education and prevention” (21–24), 2 were related to prescription dispensing monitoring programs (PDMPs) (21, 23), 1 was related to federal electronic medical records (22) and 1 was related to the digital collection of patients reported outcome measures (PROMs) (24). Of the two PDMPs, one was a federal government paper and did not list any results (21). The second paper evaluated the implementation of SafeScript—the only mandatory real-time PDMP in Australia which is used in Victoria (22). Using data collected through the Burnet Institute's SuperMIX study—a prospective cohort study of about 1,300 people who inject drugs-−20% (48/242) of participants had been refused a prescription of medication that is monitored by SafeScript. Of those that had been refused a script, 36% (16/44) were for the treatment of anxiety and 45% were refused two or more times by prescribers. Eight participants (3%) reported having a prescription for a medication that they were already using withdrawn (23).
The Australian Digital Health Agency (22) described the use of the federal “My Health Record” system that promotes the sharing of health information across state and territory jurisdictional boundaries to inform clinical decision-making. Although no conclusive information on opioid harm minimization is outlined, patient medication and prescription details are available on the system of which 23 million Australians currently use. Nielsen et al. (24) describe a protocol to test the implementation of computer-facilitated Routine Opioid Outcome Monitoring to deliver screening and brief interventions for opioid-related problems in community pharmacy practices in New South Wales and Victoria, Australia.
Access to harm reduction approaches is focused on reducing the level of harm associated with opioid use. The goal is not to promote the cessation of opioid use, but rather to help promote the use of substances in a safe and controlled manner to reduce the degree of harm and chance of overdose (17). The most commonly reported digital health interventions aligned with the “Harm reduction” drug health pillar were mobile applications (often known as Software as a Service or SaaS) for overdose monitoring and prevention (n = 3). The Lifeguard App (25) and BeBrave app (26) are designed to link people who use drugs (PWUD) (particularly alone) to emergency responders. The Lifeguard App was deployed by the Provincial Health Services Authority in BC, Canada in May 2020. As of August 2020, 1,700 people have used the Lifeguard App and recorded 5,200 uses and as of 23 June 2021, the app had saved 41 lives since being launched in the province of British Columbia. This solution is unique in its seamless connection to public health emergency service health responders through 9–1–1 services rendered by the provincial health services authorities and is the only endorsed service by 2 regional governments (in British Columbia and Northwestern Ontario). The BeBrave app reports that the service has received a total of 2,967 calls since 15 May 2020 and 33 rescue missions were undertaken (26). However, the mobile app connects with voluntary emergency response providers, who will then need to connect with 9–1–1 services and not direct with emergency services, which restricts its timely intervention capability. Bristowe et al. (27) outline a similar process to the BeBrave App, in which the user will outline the type of substance they plan on using and an operator will stay on the line checking in every 5–10 min. As this is a protocol, no results have been reported at the time of this paper.
The second most common digital health interventions in this category were the use of wireless overdose response button systems (n = 2), in which residents in supported accommodation (social housing) pushed a button before drug use to request staff to do a safety check on them. This intervention is based on the premise that opioid users are a specific disadvantaged population group residing in subsidized housing facilities. The BRAVE Technology Cooperative (28) reported 189 instances of safer use, 80 overdose reversals, and 160 instances of violence prevention. However, Bardwell et al. (29) conducted semi-structured qualitative interviews (n = 14) to examine the experience of women using this type of digital intervention and found participants were not using this solution as intended for their own drug use. Rather, it was being used for other emergencies such as gender and/or sex-work-related violence. Two papers that described using a combination of chemical analytical methods to provide drug checking services (30, 31). Mema et al. (30) describe drug checking at a major music festival in British Columbia, Canada, using fentanyl immunoassay strips and found that 1.6% (31/1,971) of samples returned a positive result for fentanyl. Those who tested for fentanyl were six times more likely to discard the sample on-site when faced with a positive result. Wallace et al. (31) describes a pilot program for a real time-multi-technology platform for drug checking that utilizes a suite of chemical analytical methods to provide harm-reduction advice in a community setting. As of July 2021, 2,213 samples have been tested of which 816 tested positive for fentanyl. Brave Technology Cooperative (32) describes a pilot program for the use of radar motion sensors in the restrooms of supported housing. As of the time of this paper, there had been no responses triggered.
Reducing illicit supply refers to initiatives that aim to disrupt the illegal and often tainted opioid supply chain (17). Tyndall (33) describes the use of an ATM that uses biometric scanning for people who use drugs to pick up their prescribed medications. No data regarding the uptake or usage was disclosed. The full results and key findings are outlined in Table 1.
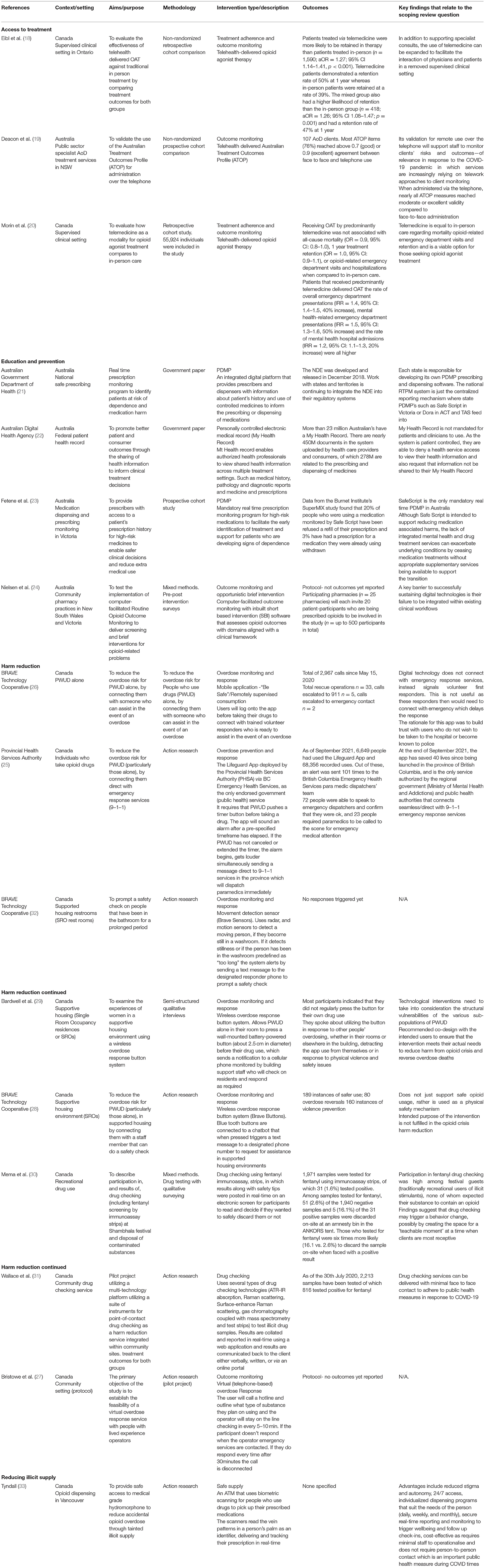
Table 1. Characteristics of included studies.
The issues associated with problematic synthetic opioid use are linked with historical prescribing practices that have coincided with changes in drug use patterns over a long period, which culminates in a crisis (34). For example, an increase in opioid prescribing and utilization followed by rises in heroin use has led to the current widespread fentanyl availability and utilization in Canada. In response to the alarming number of opioid related deaths and dependence, a number of well-intended supply reduction initiatives such as changes to pain management and prescribing guidelines, prescription drug monitoring programs, regulation and up-scheduling of opioid medications, and changes to drug formulations to make them tamper resistant and difficult to use intravenously, resulted in large numbers of people that were opioid dependent unable to obtain prescription opioids (7). The displacement of pharmaceutical opioids without appropriate measures to support the demand side, drove both medical and non-medical opioid users to seek more readily available alternatives, evidenced by a sharp increase in heroin use in Canada between 2010 and 2015 and also heroin related overdoses (7, 34) This phenomenon left large sub-groups of opioids users with a drastically shrinking supply of pharmaceutical opioids. Declining supply with continued demand also drove up market prices, which coupled with socio-economic disadvantage shifted the supply routes to the illicit market (7, 35). Reducing opioid-related harm measures to restrict supply resulted in a lateral substitutive shift in supply from one opioid category to the other (7).
Unlike heroin, which is derived from the poppy plant, synthetic opioids, such as Fentanyl can be manufactured anywhere, and manufacturers are much more easily able to import the required chemicals to produce fentanyl due to poorly regulated global distribution systems. Fentanyl is cheaper to purchase and manufacture, easier to obtain (via crypto markets and via illicit pharmacies online) and the higher potency means suppliers source it in smaller quantities, making it easier to smuggle across international borders to maximize profit and reduce profit loss if intercepted by authorities (35, 36).
Australia's experience with extra-medical opioid use differs from the Canadian experience in the patterns of drug use, trends, illicit markets, and strong border controls. Due to the lower cost of prescription opioids, heroin, and methamphetamine in Australia, this is not a driver for the need to source cheaper alternatives such as Fentanyl, as is in Canada (37, 38). Although prescription opioid use in Australia has increased substantially between 1990 and 2018, the rates are still lower than in Canada. Regardless, there remain serious concerns that Australia is mirroring the same pathway that has contributed to the opioid crisis in Canada. The number of unintentional drug-induced deaths involving opioids has nearly tripled in the last 14 years with the crisis being primarily driven by pharmaceutical prescribing (39). Simultaneously, since 2012 the number of deaths involving heroin has also increased by over 65% (40). Comparatively in Canada, the primary drivers of the opioid crisis have shifted over time from over-prescribing to more toxic synthetic opioids (fentanyl) entering the illicit supply chain (41). As of 2019, the escalating opioid crisis and associated harms were already calling for innovative strategies in both countries.
The findings of this scoping review reveal innovative digital health initiatives for opioid crisis prevention that are emerging in Canada and Australia where it has been declared as a public health emergency which has been exacerbated throughout the SARS COVID-19 pandemic.
COVID-19 has rapidly accelerated the implementation of telehealth in Australia, necessitated by socially distanced health care to protect both health care workers and patients. This has created a unique opportunity to leverage telehealth into routine clinical practice for OUD. The use of telehealth to support people with OUD was recently validated by Deacon et al. (19). Telephone support was identified as superior for this cohort as they do not have to rely on an internet connection and literacy levels as is a requirement for some other remote monitoring initiatives.
Opioid agonist therapy (OAT) is a harm reduction model of care where opioid agonists such as buprenorphine/naloxone or methadone, are substituted to replace more dangerous and addictive opioids to stabilize a person's use and maintain an individual's psychosocial functioning (18). Patients often remain in therapy for several years and are more classified as a maintenance treatment, in which the person will slowly reduce the dosage to safely wean off the medication, by alleviating the opioid withdrawal symptoms (20).
The rigidity of traditional treatment paradigms for opioid use disorder characterized by frequent clinic appointments, supervised dosing, screening, and limited take-home doses of medications poses significant challenges for easily incorporating it into everyday life. The flexibility of telehealth to support opioid agonist therapy adherence offers an effective alternative to in-person care with people 50% more likely to be retained in therapy for 1 year compared to 39% for those treated in person (18). These results support findings from other studies, demonstrating that telemedicine-delivered OAT is a comparable treatment modality with the potential to expand access to treatment for those with opioid use disorder and may be an effective and appropriate alternative to traditional face-to-face treatment modalities (18, 20, 42).
Despite telehealth offering greater flexibility and potential access to services, there are challenges with supporting telehealth engagement among marginalized patients. Telehealth-only models of care have been associated with increased rates of mental health emergency department presentations and hospitalisations (20) highlighting the need for further research to understand the mental health implications of telehealth use for those undertaking OAT. Additionally, the lack of standardized clinical guidance, funding and resource constraints, jurisdictional boundaries and lack of collaboration between governments, continue to pose significant challenges to the successful implementation of holistic telehealth care for PWUD in Australia (43–46).
The use of PDMPs is a core feature of both the Canadian and Australian opioid management strategy and supports safe and accurate prescribing of high-risk and controlled substances following best-practice guidelines to reduce polypharmacy and patient harm (47). PDMPs are available in seven of ten provinces in Canada (36), while in Australia only Victoria (one of eight jurisdictions) has real-time script monitoring (34).
The Australian Government Department of Health (21) describes the rollout of national real-time prescription monitoring (RTPM). Devolved governance means each jurisdiction is responsible for developing/procuring its own PDMP prescribing and dispensing software, resulting in multiple medication systems that are difficult to integrate. With the expansion of electronic medical records and the national My Health Record system (22) there is potential to enable prescription monitoring in some capacity.
My Health Record is a personally controlled universal electronic health record summary that is linked with an Australian resident's Medicare number. The rationale for the introduction of the My Health Record in Australia is to provide a centralized health record for patients to improve the coordination of care, reduce duplication and medication harm, and enhance patient control of their health information to promote shared decision making (22). The system allows individuals and their treating team to upload clinical documents, pathology and diagnostic reports, medication and immunization histories to a secure online record that is controlled by the patient. Only permitted health care providers can access an individual's My Health Record and patients also have the ability to restrict certain information being viewed in their record (22). Therefore, despite the My Health Record System having the future capability for prescription monitoring, the challenge therein lies with the ability of patients to remove information from their health record, such as opioid prescriptions, that works counter intuitively to efforts to reduce users from acquiring medications from clinicians in different states.
SafeScript became mandatory in Victoria in April 2020, making it the only mandatory real-time PDMP in Australia (23). The use of PDMPs globally is well-documented (34, 48–50), however, the evidence of their effectiveness to reduce opioid-related harm and consequences is mixed. Fente et al. (23) explored the effects of SafeScript in Victoria, interviewing 387 people. Since the introduction of SafeScript in April 2019 they found that 20% of participants had been refused a prescription medication that is monitored by Safe Script. Of those that had been refused a script, 36% were for the treatment of anxiety and 45% were refused two or more times by prescribers. Alarmingly, 3% reported having a prescription withdrawn for a medication that they were already using.
A high number of people use medications extra-medically and have comorbid mental health disorders that require multidisciplinary support. Although SafeScript is intended to support reducing medication-associated harms, the lack of integrated mental health and drug treatment services can exacerbate underlying conditions by ceasing medication treatments without appropriate supplementary services being available to support the transition.
The correlation of increased opioid-related mortality following restrictions of prescribed medications is well-documented (34, 47, 51, 52), which highlights the need for ongoing research to understand the impact of RTPM use in Australia and opportunities to better integrate digital health infrastructure to support people who use drugs (23).
A systematic review conducted by Rhodes et al. (47) found that as a standalone feature, PDMPs were ineffective in reducing several indicators of population-level opioid-related harm such as opioid dependence, hospital separations, emergency department utilization, and usage levels of both pharmaceutical and illicit opioid use. Limitations of PDMPs, however, do not necessarily lie with the technology itself but rather the ineffective use of the information generated to inform clinical decision-making. This highlights the need for further formally documented research on the use of PDMPs to combat the opioid crisis and their effectiveness across various populations in Australia to ensure that the results are generalisable.
BRAVE Technology Cooperative (26) and the Provincial Health Services Authority (25) describe the use of mobile apps that link people who use drugs alone to emergency responders, to reverse an overdose. The premise is based on prioritizing the autonomy, anonymity, and privacy of those that use the service to allow them to decide the appropriate emergency response for them in the event of an overdose. Accordingly, BeSafe is a mobile app where the person specifies their location, the drug they are using, whether they have naloxone, and their emergency response plan. This is completed before the person uses drugs. Through the app, the person can call the BeSafe Support Center. The pre-supplied information is hidden from the call supporter unless the operator suspects the caller is overdosing. In the event of a suspected overdose, the caller will be given a 20 s countdown alert advising their information will become available unless they dismiss the alert to indicate that they are ok. If the alert is not dismissed, the caller's location and emergency response plan will be shared with the supporter who uses it to send for help, either someone specified by the caller or emergency services (26). However, the app does not connect directly to emergency health responders as it is operated by a co-op. It also relies on a call center that is operated by voluntary responders who will use their judgement of a suspected overdose.
Conversely, The Lifeguard App was deployed by the Provincial Health Services Authorities via the government emergency services in a provincial health intervention model, in Canada. It combines GPS and geofencing technologies to connect the user to emergency services, in case of an emergency. It requires that the PWUD push a timer in the app before they take any drug. There is facility to extend the timer. If the timer is not canceled within 45 s, an alarm begins, and the emergency paramedic services (in BC, 9–1–1 services) are called. As all information is deleted from the app after a call is linked to the paramedic services, there is privacy preservation and anonymity assurance that has led to the increased uptake of this mobile app (or SaaS digital intervention).
Since May 2020, these 2 apps have had a combined 8,167 calls and saved 66 people from overdoses (26, 53). Despite the success in saving lives, qualitative studies to understand the acceptance of digital health interventions are still emerging. Concerns about security, privacy, and accessibility remain an important consideration, while public health authorities are considering the implementation of novel digital protocols such as blockchain (54). Supporting substance users wish to remain anonymous is essential to avoid the stigma of being identified by family, employers, or law-enforcement authorities. Therefore, they hesitate to use any digital intervention such as the Lifeguard App which may accidentally reveal their identity if a hacker intercepts an emergency call. To mitigate this, public health authorities are considering the development of end-to-end secure transmission methods where a call for reaching emergency services cannot be intercepted as it would be fortified by a layer of blockchain or distributed ledger technologies (DLTs). By working within this secure ecosystem, the users can be assured of their privacy. In addition, permissioned blockchain protocols can be configured with artificial intelligence methods such that users can get support from a pre-approved peer group while remaining anonymous.
Although mobile phones have penetrated 90% of the global market, people with transient lifestyles, and uncertain living and employment arrangements may not have consistent access to mobile technologies, Wi-Fi, or safe spaces to comfortably use the digital health interventions, which impacts the accessibility of these innovations (4, 5, 55). Thorough needs assessments that take into consideration these logistic and functional limitations as well the dangers of drug use, user preferences, interpersonal relationships with friends, and socioeconomic status are necessary to not further divide already marginalized populations.
A pilot of a Wireless overdose response button system, in which people in supported residential accommodation press a wall-mounted battery-powered button before their drug use, triggering a notification to a cellular phone monitored by building support staff who check on them and respond accordingly (28) was reported. The findings show 189 instances of safer use, 80 overdose reversals, and 160 instances of violence prevention. Semi-qualitative interviews to understand the experiences of women using this type of digital technology within a supportive housing environment found that participants did not use the overdose prevention button as intended (using it before individual drug use) rather it was mostly reported to be used for other emergencies such as other residents or guests overdoses and sex-work related violence. This demonstrates that technological interventions for OUD need to be co-designed with intended users and take into consideration the inherent vulnerabilities of sub-populations within this cohort. PWUD need to be empowered to use their agency to assess their levels of perceived risk. This cohort of women did not perceive their overdose risk as high as those around them, demonstrating a unique learning opportunity to tailor interventions to meet the specific needs of women who use drugs alone to avoid gender-based violence (29).
The Brave Technology Cooperative (32) describe the use of passive surveillance in bathrooms in supported accommodation as a means of overdose detection. The Brave sensor uses radar, which uses motion sensors to detect a moving person if they become still in a washroom. If it detects stillness or if the person has been in the washroom predefined as 'too long', the system alerts by sending a text message to the designated responder's phone to prompt a safety check. Despite the success of passive surveillance sensors in the US, the BraveSensor trial in Canada as of July 2021 has yet to trigger any responses (32). Although the potential of this type of digital health intervention is well-understood key ethical and implementation considerations such as liability, data privacy and security, technical accuracy, consent, communication, and stigma pose challenges to the scalability of this type of digital health intervention (56).
Mema et al. (30) describe drug checking at a major music festival in British Columbia using fentanyl immunoassay strips to detect fentanyl in recreational substances. The challenge with deploying mobile technologies for drug-checking is that it is difficult to ensure consistent, reliable results that can be easily interpreted without specialized training (57). Test strips that are simple to use are essential to frontline harm-reduction settings, however, they cannot provide information beyond a binary yes/no result (31). This makes it difficult for people to make truly informed decisions about their level of risk as they have no information about how potent the sample is. Although these interventions do not deter long-term drug-taking, it does empower people to make informed decisions based on risk when fentanyl is detected by providing information on potency (58).
In the pilot protocol outlined by Wallace et al. (31) utilizing multi-model methods is discussed for disseminating drug-checking results, either in-person or through a web-based portal. The rationale for the use of multiple technologies is that the strengths and limitations of each technology complement each other, providing more comprehensive results. These findings are supported by Tupper et al. (58) who conducted a drug checking feasibility study using Fourier transform infrared (FTIR) spectrometer and fentanyl immunoassay strips in Vancouver and found out of 907 samples of heroin tested, 90.6% (822) tested positive for fentanyl. This not only highlighted the prevalence in the Vancouver drug supply but the acceptability and necessity of this type of digital health intervention as a harm-minimization and risk deterrent. Although these interventions do not deter long-term drug-taking, it does empower people to make informed decisions based on risk when fentanyl is detected by providing information on potency (59). Findings suggest that drug checking may trigger a change in behavior, possibly by creating the space for a 'teachable moment' at a time when clients are most receptive (30).
As presented in the findings, Tyndall (33) had highlighted MySafe—a digital health intervention piloted in Vancouver, Canada that functions as an ATM with biometric scanning allowing PWUDs to collect prescriptions and offers real-time tracking of collection. There is tremendous potential to reduce illicit drug supply using this intervention. The reduced stigma, 24/7 access, customized dispension programs, secure real time tracking and reporting, follow-up checks, cost effectiveness with minimal staff requirement to operationalize this contactless solution—are all features that have the potential for scalability to other jurisdictions in Canada and globally. Nonetheless, the lack of formal evidence-based evaluation in academic literature thus far, is a limitation that can be addressed.
This review applied a systematic and rigorous search strategy but was limited in sample size, although the review indicates the potential of digital technologies to address the challenges of the Australian and Canadian opioid crises and the current gaps in approaches to utilizing them effectively. Despite efforts to comprehensively search literature, it is possible that some relevant papers were not included due to search terms or database restrictions. Additionally, some relevant papers may have been inadvertently omitted as this research did not focus on digital health-specific literature that is outside the scope of the public health domain, thus offering differing perspectives.
Furthermore, this review may have limited identification of all the digital technologies and SaaS/SaMD interventions that have been developed in response to the changing needs of opioid users during the COVID-19 pandemic due to publishing delays and challenges with timely dissemination of results from pilot projects. As this topic is evolving, it is recommended that the findings of this review be confirmed with a systematic review when more data is available.
A key challenge with digital health is its dynamic nature. Delays in the dissemination of findings are proving to be a barrier to the scalability and sustainability of such technologies, meaning that these interventions are occurring in isolation, resulting in variations in clinical practice for the management of opioid use disorder.
This review has highlighted the lack of longitudinal studies to understand the long-term impacts of harm-reduction interventional strategies and robust mechanisms and evaluations of digital health implications that target both those that use opioids and healthcare/support workers within the two countries, where the universal health care system is the foundation. The different data sources in this review also produced varying results that limits the ability to quantify the extent of extra-medical use of opioids and associated harm and making it difficult to fathom the extent of the problem and how to best address the crisis.
This study reveals a need for more publications to demonstrate the potential beneficial impacts of digital health interventions to reduce opioid-related harm and mortality. Such studies will assist in developing a best practice foundation for implementing digital health interventions to reduce opioid-related harm across the various subpopulations. In Australia, digital health has become mainstream over 2020–2021, and during the same time, in Canada, digital technologies have been rapidly deployed as harm reduction tools. While the crisis is at different levels in the two countries, some of the initiatives and key learning can be shared across the two countries. This research is an invitation to the public health sector and policy makers to explore such innovations for reducing the harm caused by the opioid crisis.
This review highlights there are gaps in Australia and Canada's approaches in managing their respective opioid crises. The COVID-19 pandemic has created the opportunity to incorporate digital health initiatives into the core strategy of opioid public health measures, however, the lack of credible research and investment in digital interventions means that we are still yet to see its full potential in this space. The digital health interventions outlined in this review including telehealth-delivered opioid replacement therapy, drug checking, digital information sharing have resulted in behavioral changes in drug users. Conversely, Lifeguard App (a mobile app that directly connects to emergency services) has already saved more than 40 lives during the pandemic (53). As we shift into the era of “COVID normal,” the era of socially distanced health care will continue, impacting how people interact with each other and the health care system. There is a need to establish an evidence base that compares the Australian opioid public health crisis with the Canadian context to obtain key learnings that can be shared to prevent opioid-related harm and mortality.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
CU and AD: conceptualization and visualization. AD and JT: methodology. AD: formal analysis, investigation, and writing—original draft. AD, CU, and JT: resources. AD, CU, and FH: writing—review and editing. CU: supervision. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to acknowledge Muhammad Tahir and Prabhathi Basnayaka (Capstone Supervisors) from Torrens University for their support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.900733/full#supplementary-material
1. World Health Organisation. Opioid Overdose. WHO (2020). Available online at: https://www.who.int/news-room/fact-sheets/detail/opioid-overdose (accessed April 3, 2021).
2. National Drug Research Institute. Quantifying the Social Costs of Pharmaceutical Opioid Misuse & Illicit Opioid Use to Australia in 2015/16. Perth: Curtin University (2020). Available online at: https://ndri.curtin.edu.au/NDRI/media/documents/publications/T277.pdf
3. Grebely J, Cerdá M, Rhodes T. COVID-19 and the health of people who use drugs: what is and what could be? Int J Drug Policy. (2020) 83:102958. doi: 10.1016/j.drugpo.2020.102958
4. Dunlop A, Lokuge B, Masters D, Sequeira M, Saul P, Dunlop G, et al. Challenges in maintaining treatment services for people who use drugs during the COVID-19 pandemic. Harm Reduct J. (2020) 17:26. doi: 10.1186/s12954-020-00370-7
5. Dietze P, Peacock A. Illicit drug use and harms in Australia in the context of COVID−19 and associated restrictions: anticipated consequences and initial responses. Drug Alcoh Rev. (2020) 39:297–300. doi: 10.1111/dar.13079
6. Norton A, Kerr T. Applying the lessons of COVID-19 response to Canada's worsening opioid epidemic. EClinicalMedicine. (2020) 29–30:100633. doi: 10.1016/j.eclinm.2020.100633
7. Fischer B, Pang M, Tyndall M. The opioid death crisis in Canada: crucial lessons for public health. Lancet Public Health. (2018) 4:2:e81–2. doi: 10.1016/S2468-2667(18)30232-9
8. Alexander G, Stoller K, Haffajee R, Saloner B. An epidemic in the midst of a pandemic: opioid use disorder and COVID-19. Ann Intern Med. (2020) 173:57–8. doi: 10.7326/M20-1141
9. PHAC. Opioid and Stimulant-Related Harms in Canada. PHAC (2021). Available online at: https://health-infobase.canada. ca/substance-related-harms/opioids-stimulants/ (accessed June 3, 2021).
10. AIHW. Overdose and Misuse. AIHW (2021). Available online at: https://www.aihw.gov.au/reports/alcohol/alcohol-tobacco-other-drugs-australia/contents/impacts/health-impacts#Overdose (accessed April 3, 2021).
11. AIHW. Opioid Harm in Australia and Comparisons Between Australia and Canada. AIHW (2018). Available online at: https://www.aihw.gov.au/getmedia/605a6cf8- 6e53-488e-ac6e-925e9086df33/aihw-hse-210.pdf.aspx?inline=true (accessed April 3, 2021).
12. Carrà G, Crocamo C, Humphris G, Tabacchi T, Bartoli F, Neufeind J, et al. Engagement in the overdose RIsk InfOrmatioN (ORION) e-Health tool for opioid overdose prevention and self-efficacy: a preliminary study. Cyberpsychol Behav Soc Netw. (2017) 20:762–8. doi: 10.1089/cyber.2016.0744
13. World Health Organization. Global Strategy on Digital Health. World Health Organization (2021). Available online at: who.int/docs/default-source/documents/gs4dhdaa2a9f352b0445bafbc79ca799dce4d.pdf
14. Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 11: Scoping reviews. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. JBI (2020). doi: 10.46658/JBIMES-20-12
15. Tricco A, Lillie E, Zarin W, O'Brien K, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:7. doi: 10.7326/M18-0850
16. The Joanna Briggs Institute. The Joanna Briggs Institute Reviewers' Manual 2015: Methodology for JBI Scoping Reviews. Adelaide: The Joanna Briggs Institute (2015). Available online at: https://nursing.lsuhsc.edu/JBI/docs/ReviewersManuals/Scoping-.pdf
17. Government of Canada. Federal Actions on Opioid to Date. Government of Canada (2020). Available online at: https://www.canada.ca/content/dam/hc-sc/documents/services/substance-use/problematic-prescription-drug-use/opioids/responding-canada-opioid-crisis/federal-actions/federal-action-opioids-to-date-dec-eng.pdf (accessed June 3, 2021).
18. Eibl J, Gauthier G, Pellegrini D, Daiter J, Varenbut M, Hogenbirk J, et al. The effectiveness of telemedicine-delivered opioid agonist therapy in a supervised clinical setting. Drug Alcoh Depend. (2017) 176:133–8. doi: 10.1016/j.drugalcdep.2017.01.048
19. Deacon R, Mammen K, Holmes J, Dunlop A, Bruno R, Mills L, et al. Assessing the validity of the Australian treatment outcomes profile for telephone administration in drug health treatment populations. Drug Alcoh Rev. (2020) 39:441–6. doi: 10.1111/dar.13088
20. Morin K, Parrotta M, Eibl J, Marsh D. A retrospective cohort study comparing in-person and telemedicine-based opioid agonist treatment in Ontario, Canada, using administrative health data. Euro Addict Res. (2021) 27:268–76. doi: 10.1159/000513471
21. Australian Government Department of Health. National Real Time Prescription Monitoring (RTPM). Australian Government Department of Health (2020). Available online at: https://www.health.gov.au/initiatives-and-programs/national-real-time-prescription-monitoring-rtpm (accessed June 3, 2021).
22. Australian Digital Health Agency. My Health Record. (2021). Available online at: https://www.digitalhealth.gov.au/initiatives-and-programs/my-health-record (accessed June 3, 2021).
23. Fetene D, Higgs P, Nielsen S, Djordjevic F, Dietze P. The impact of Victoria's real time prescription monitoring system (SafeScript) in a cohort of people who inject drugs. Med J Austral. (2021) 214:234.e1. doi: 10.5694/mja2.50958
24. Nielsen S, Kowalski M, Wood P, Larney S, Bruno R, Shanahan M, et al. Routine opioid outcome monitoring in community pharmacy: pilot implementation study protocol. Res Soc Admin Pharm. (2019) 15:1047–55. doi: 10.1016/j.sapharm.2018.10.024
25. Provincial Health Services Authority. New Lifeguard App Launched to Help Prevent Overdoses. Provincial Health Services Authority (2020). Available online at: http://www.phsa.ca/about/news-stories/news-releases/2020-news/new-lifeguard-app-launched-to-help-prevent-overdoses
26. BRAVE Technology Cooperative,. The Brave App: Reporting. BRAVE Technology Cooperative (2021). Available online at: https://www.brave.coop (accessed June 3, 2021).
27. Bristowe S, Ghosh S, Trew M, Rittenbach K. Virtual overdose response for people who use opioids alone: protocol for a feasibility and clinical trial study. JMIR Res Protoc. (2021) 10:e20183. doi: 10.2196/20183
28. Brave Technology Cooperative,. Brave Button Report. (2019). Available online at: https://www.brave.coop/ (accessed June 3, 2021).
29. Bardwell G, Fleming T, McNeil R, Boyd J. Women's multiple uses of an overdose prevention technology to mitigate risks and harms within a supportive housing environment: a qualitative study. BMC Womens Health. (2021) 21:51. doi: 10.1186/s12905-021-01196-6
30. Mema S, Sage C, Xu Y, Tupper K, Ziemianowicz D, McCrae K, et al. Drug checking at an electronic dance music festival during the public health overdose emergency in British Columbia. Canadian Journal of Public Health. (2018) 109:5–6. doi: 10.17269/s41997-018-0126-6
31. Wallace B, Hills R, Rothwell J, Kumar D, Garber I, Roode T, et al. Implementing an integrated multi-technology platform for drug checking: social, scientific, and technological considerations. Drug Test Anal. (2021) 13:734–46. doi: 10.1002/dta.3022
32. BRAVE Technology Coop,. Non-Contact Overdose Detection. (2021). Available online at: https://www.brave.coop/sensor (accessed June 3, 2021).
33. Tyndall M. Safer opioid distribution in response to the COVID-19 pandemic. Int J Drug Policy. (2020) 83:102880. doi: 10.1016/j.drugpo.2020.102880
34. Brown R, Morgan A. The Opioid Epidemic in North America: Implications for Australia. Canberra, ACT: Australian Institute of Criminology (2012).
35. Donroe JH, Socias ME, Marshal BD. The deepening opioid crisis in North America: historical and current solutions. Curr Addict Rep. (2018) 5:454–63. doi: 10.1007/s40429-018-0228-5
36. Ciccarone D. Fentanyl in the US heroin supply: a rapidly changing risk environment. Int J Drug Policy. (2017) 46:107–11. doi: 10.1016/j.drugpo.2017.06.010
37. Alcohol Drug Foundation. Opioids. Alcohol and Drug Foundation (2020). Available online at: https://adf.org.au/drug-facts/opioids/ (accessed June 3, 2021).
38. Scamvougeras A, Greene S, Norman A, Bonomo Y, Castle D. The fentanyls: a ‘future threat' for Australia? Austral Psychiatry. (2020) 28:545–7. doi: 10.1177/1039856220917074
39. OECD. Addressing Problematic Opioid Use in OECD Countries. OECD (2019). Available online at: https://www.oecd.org/health/addressing-problematic-opioid-use-in-oecd-countries-a18286f0-en.htm (accessed May 30, 2021).
40. Penington Institute,. Australia's Annual Overdose Report 2021. Melbourne, VIC: Penington Institute (2021). Available online at: https://www.penington.org.au/publications/australias-annual-overdose-report-2021/ (accessed August 31, 2021).
41. Government of Canada. Opioid and Stimulant-Related Harms in Canada. (2020). Available online at: https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/ (accessed May 12, 2021).
42. Schramm Z, Leroux B, Radick A, Ventura A, Klein J, Samet J, et al. Video directly observed therapy intervention using a mobile health application among opioid use disorder patients receiving office-based buprenorphine treatment: protocol for a pilot randomized controlled trial. Addict Sci Clin Pract. (2020) 15:30. doi: 10.1186/s13722-020-00203-9
43. Australian Digital Health Agency. Australian Digital Health Strategy. Australian Digital Health Agency (2018). Available online at: https://www.digitalhealth.gov.au/sites/default/files/2020-11/Australia%27s%20National%20Digital%20Health%20Strategy%20-%20Safe%2C%20seamless%20and%20secure.pdf (accessed May 31, 2021).
44. Wong Z, Cross H. Telehealth in cancer care during the COVID−19 pandemic. Med J Austral. (2020) 213:237.e1. doi: 10.5694/mja2.50740
45. Thomas E, Haydon H, Mehrotra A, Caffery L, Snoswell C, Banbury A, et al. Building on the momentum: sustaining telehealth beyond COVID-19. J Telemed Telecare. (2020) 28:301–8. doi: 10.1177/1357633X20960638
46. Koh D,. Victoria's Rapid Adoption of Telehealth Its Challenges. Healthcare IT (2020). Available online at: https://www.healthcareit.com.au/article/victoria%E2%80%99s-rapidadoption-telehealth-and-its-challenges-0 (accessed April 12, 2021).
47. Rhodes E, Wilson M, Robinson A, Hayden J, Asbridge M. The effectiveness of prescription drug monitoring programs at reducing opioid-related harms and consequences: a systematic review. BMC Health Serv Res. (2019) 19:784. doi: 10.1186/s12913-019-4642-8
48. Taha S, Maloney-Hall B, Buxton J. Lessons learned from the opioid crisis across the pillars of the Canadian drugs and substances strategy. Subst Abuse Treat Prevent Policy. (2019) 14:32. doi: 10.1186/s13011-019-0220-7
49. Greer A, Ritter A. Harm reduction and the opioid crisis: emerging policy challenges. Int J Drug Policy. (2019) 71:139–41. doi: 10.1016/j.drugpo.2019.05.015
50. Penington Institute,. Australia's Annual Overdose Report 2020. Melbourne, VIC: Penington Institute (2020). Available online at: https://www.penington.org.au/wpcontent/uploads/Australias-Annual Overdose-Report-2020.pdf
51. Lam T, Kuhn L, Hayman J, Middleton M, Wilson J, Scott D, et al. Recent trends in heroin and pharmaceutical-opioid related harms in Victoria, Australia up to 2018. Addiction. (2020) 115:261–9. doi: 10.1111/add.14784
52. Lalic S, Ilomäki J, Bell JS, Korhonen MJ, Gisev N. Prevalence and incidence of prescription opioid analgesic use in Australia. Br J Clin Pharmacol. (2018) 85:202–15. doi: 10.1111/bcp.13792
53. Provincial Health Services Authority. Lifeguard app usage report- MMHA. Vancouver: Provincial Health Services Authority; 2021 September.
54. Unnithan C,. Saving Lives From the “Other Crisis” During the COVID-19 Pandemic at Lifeguard Digital Health. Digital Think Tank by ICTC (2021). Available online at: https://medium.com/digitalthinktankictc/saving-lives-from-the-other-crisis-during-the-covid-19-pandemic-at-lifeguard-digital-health-5f84d829166b (accessed June 5, 2021).
55. Tsang V, Papamihali K, Crabtree A, Buxton J. Acceptability of technological solutions for overdose monitoring: perspectives of people who use drugs. Subst Abuse. (2019) 42:284–93. doi: 10.1080/08897077.2019.1680479
56. Draanen J, Satti S, Morgan J, Gaudette L, Knight R, Ti L. Using passive surveillance technology for overdose prevention: key ethical and implementation issues. Drug Alcoh Rev. (2021) 41:406–9. doi: 10.1111/dar.13373
57. Impact Canada,. Drug Checking Technology Challenge. (2020). Available online at: https://impact.canada.ca/en/challenges/drug-checking-challenge (accessed April 6, 2021).
58. Tupper K, McCrae K, Garber I, Lysyshyn M, Wood E. Initial results of a drug checking pilot program to detect fentanyl adulteration in a Canadian setting. Drug Alcoh Depend. (2018) 190:242–5. doi: 10.1016/j.drugalcdep.2018.06.020
Keywords: opioid crisis, COVID-19, Australia, Canada, digital health (e-health), mobile apps (SaaS), public health, harm reduction
Citation: Donnell A, Unnithan C, Tyndall J and Hanna F (2022) Digital Interventions to Save Lives From the Opioid Crisis Prior and During the SARS COVID-19 Pandemic: A Scoping Review of Australian and Canadian Experiences. Front. Public Health 10:900733. doi: 10.3389/fpubh.2022.900733
Received: 21 March 2022; Accepted: 19 May 2022;
Published: 12 July 2022.
Edited by:
Anat Gesser-Edelsburg, University of Haifa, IsraelReviewed by:
Motti Haimi, University of Haifa, IsraelCopyright © 2022 Donnell, Unnithan, Tyndall and Hanna. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Donnell, YW5kcmVhX2Rvbm5lbGxAb3V0bG9vay5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.