 Dong Lang1,2
Dong Lang1,2 Chengxu Long3
Chengxu Long3 Shuna Lin1,2Yinghua Xie1,2Fangfei Chen1,2Rui Zhao4Chunping Liu4
Shuna Lin1,2Yinghua Xie1,2Fangfei Chen1,2Rui Zhao4Chunping Liu4 Shangfeng Tang1,2*
Shangfeng Tang1,2*- 1School of Medicine and Health Management, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
- 2Research Center for Rural Health Service, Key Research Institute of Humanities & Social Sciences of Hubei Provincial Department of Education, Wuhan, China
- 3Department of Global Health & Social Medicine, King's College London, London, United Kingdom
- 4China National Health Development Research Center, Beijing, China
Background: Although the Chinese promotion of labor analgesia began in 2018 to improve maternal health, high-quality medical care is difficult to provide to pregnant women when medical staff cannot implement standard labor analgesia procedures. This study aims to examine medical personnel's adherence to labor analgesia protocols and to explore the relationships among adherence, satisfaction, and other factors.
Methods: The data were from a national cross-sectional dataset (N = 13,944) of the 2020 Chinese Labor Analgesia Pilot Evaluation Project. Mediating and moderating effects analyses were used to examine the role of satisfaction as a mediator between support measures and adherence.
Results: There were differences in adherence between different types of medical personnel. Support measures and satisfaction had a positive association with adherence to labor analgesia protocols. Satisfaction had a significant mediating and moderating effect on the relationship between support measures and adherence to labor analgesia standards. Moderating effects of professional titles and attitudes were also observed.
Conclusion: Primary health care policies worth considering include comprehensive incentives for medical institutions to improve the use of labor analgesia by medical personnel. It is also worth considering providing more training opportunities for the staff in anesthesiology departments.
Introduction
Maternal health influences the quality of maternal life, the birth of healthy babies, and the stability of society; thus, it is a global concern (1). Health policies in many countries have made significant progress in improving maternal health (2, 3). The United Nations Sustainable Development Goals (SDGs) proposed accelerating the improvement of maternal health. Maternal health was also a focus of the Global Strategy for Women's, Children's, and Adolescent's Health 2016–2030 led by the WHO. However, in 2020, the global maternal mortality rate was 12/100,000, and the rate was 16.9/100,000 in China (4). Most maternal deaths in developing countries could be prevented if women received timely care during childbirth such as labor analgesia (5). The situation in developing countries is of great concern.
Developing countries have many problems threatening maternal health, while developed countries have successfully reduced maternal deaths by up to 80% through adequate funding, highly qualified personnel, and advanced technology (6). Labor analgesia technology has been shown to effectively promote maternal health (7). There is a disparity between developing and developed countries regarding the prevalence of labor analgesia. The rate of labor analgesia use in developed countries reached above 80% at the beginning of the twenty-first century (8–11). To improve maternal health, many developing countries are promoting labor analgesia (12, 13). However, only a few medical institutions offer adequate pain treatment during childbirth in China, and the rate of labor analgesia was only approximately 10% in 2017 (14). Labor analgesia has just begun to be used as an effective intervention to relieve labor pain in developing countries, and there are many issues that need to be addressed. To motivate further development of labor analgesia, the National Health Commission of China (NHCC) issued the Developing Labor Analgesia Pilot Work in 2018, and 913 hospitals were included in the first pilot in 2019.
A review of the available literature showed that standardized labor analgesia was of great significance for reducing the prevalence of cesarean section, improving the quality of life after labor (15, 16), and meet women's needs for painless labor (17). The committee of labor analgesia experts of the Chinese Medical Doctor Association compiled the Clinical Standardized Management Path for Labor Analgesia in China, which stated that an entire labor analgesia service should include promotion, professional operation, record keeping, and follow-up services (18). However, labor analgesia in China is still in the developing stage, and a large number of medical personnel are still learning basic skills. Irregularities may unavoidably occur during the implementation of labor analgesia. Consequently, determining medical personnel's adherence to standard labor analgesia plays an essential role in improving maternal health. In addition, the evidence suggests that women who chose labor analgesia are affected by the information provided by medical personnel and the quality of the labor analgesia (19–21). Adherence to labor analgesia protocols by medical personnel is essential for both maternal health and the well-being of society. Thus, this study aims to examine the factors related to the administration of labor analgesia, which offers insights to identify target groups, provides information for improving adherence to labor analgesia protocols, and provides implications for other developing countries facing similar issues.
Literature Review
Adherence to Labor Analgesia Protocols and Support Measures
Labor analgesia is crucial for pregnant women to live healthy life (7). Previous studies have identified implementing standardized labor analgesia has contributed to reducing the prevalence of cesarean section and improving pregnant women's physical and mental health (22). However, low-quality labor analgesia may cause serious complications (23); thus, it is important for medical personnel to adhere to analgesia measures. Adherence to labor analgesia protocols is also an important indicator in evaluating the progress and effectiveness of labor analgesia policies (24).
Since the promotion of labor analgesia in China, the influence of support measures on adherence to labor analgesia has been examined rarely. Lack of incentives and unavailability of equipment or personnel will influence labor analgesia adherence (25). Medical personnel often have negative attitudes to labor analgesia due to the scarcity of knowledge (26). It has been reported that incentives reduce the gap between medical personnel's knowledge and clinical practice with a large gain in efficiency (27). Added incentives for labor analgesia implementers could increase medical personnel's enthusiasm and improve the quality of service (28).
In addition, evidence has shown that one of the factors that affect labor analgesia in public hospitals is the lack of medical personnel and detailed charging items that is related to pain relief (29). Related arrangements for labor analgesia consist of four components—adequate personnel, adequate equipment, reasonable medical reimbursement, and charging items (18). Previous research has found that the better the arrangements are, the higher the rate and quality of labor analgesia (30). Based on the discussion above, this study is aimed to evaluate the relationship between support measures on labor analgesia.
Satisfaction With the Implementation of Labor Analgesia
Support measures are probably to have positive effects on departmental collaboration satisfaction and consequently labor analgesia adherence, but the mechanism by which satisfaction relates to the relationship between labor analgesia adherence and support measures has not been specified in the literature. The existing evidence points to relevant perspectives in understanding this relationship. Existing evidence provides work satisfaction is closely related to the quality of medical services (31). Medical personnel with high work satisfaction are more likely to provide high-quality services. Meanwhile, work-related factors have a significant effect on work satisfaction (32). Labor analgesia can only be conducted with multidisciplinary cooperation (33). Specifically, anesthesiologists need to understand the whole process of labor and delivery, and obstetricians need to know the key points and operational techniques of labor analgesia, while midwives spend the longest time with women in labor (34). Highly intensive cooperation can result in timely and correct treatment to ensure maternal safety and guarantee the therapeutic effectiveness of maternal analgesia (35). Numerous studies have demonstrated the positive effects of adequate personnel and reasonable policies on the teamwork of medical personnel (36–38).
Professional development satisfaction exerts a powerful effect on improving the professional skill level of medical personnel (39). Since the NHCC implemented labor analgesia in 2018, medical institutions have implemented incentive measures that attract medical personnel by promoting them to professional positions. Adopting incentives was an excellent policy for those with lower-level professional titles (24, 40), but the incentive effect is limited to experts with senior professional titles. This is because seniors prefer to provide more professional guidance rather than practice labor analgesia (41). In addition, willingness is an indicator of satisfaction (42), and refers to whether medical personnel voluntarily participate in labor analgesia. Medical personnel are more willing to participate in labor analgesia when they are satisfied with the incentives and related arrangements (43). Meanwhile, medical personnel may be more inclined to use labor analgesia because there are fewer side effects and more effective pain treatment than previously reported (44).
So far, no studies have yet evaluated the role of satisfaction in mediating the relationship between support measures and labor analgesia adherence. Based on the discussion above, this study proposes a conceptual framework, as shown in Figure 1, in which support measures affect satisfaction with professional development and departmental collaboration and willingness affect adherence to labor analgesia. standards; that is, departmental collaboration satisfaction, professional development satisfaction, and willingness play mediating roles between support measures and adherence to labor analgesia protocols.
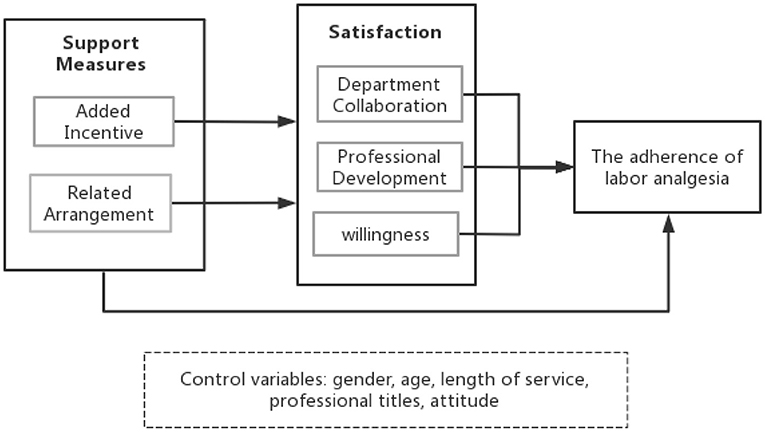
Figure 1. Conceptual framework.
Methods
Data
The Chinese Association of Anesthesiologists surveyed to evaluate the progress and effectiveness of the Chinese national labor analgesia pilot programme with the help of provincial health administrations in 2020. All 913 pilot hospitals were invited to complete the related information in the system for the labor analgesia programme. The cluster sampling method was used for the investigation. All medical personnel in anesthesiology, obstetrics, and midwifery in each pilot hospital were invited to participate in the online questionnaire survey, which was developed by the team from Huazhong University of Science and Technology. Oral consent was obtained from all participants. A total of 13,944 questionnaires were sent out and 12,614 valid questionnaires were collected; the validity rate was 90.46%.
Variables
Adherence to labor analgesia protocols was related to the support measures of the medical institution. As Table 1 shows, total adherence was selected as the dependent variable. Adherence comprised training for medical personnel and prenatal teaching for pregnant women and their family members. It also included four operative preparations: regular preoperative visits and records, adaptation training in the labor analgesia puncture position before labor, monitoring and recording throughout the administration of analgesia, and routine postoperative follow-up and recording after labor. The individual choices in the questionnaire were classified as Yes (1) and No (0). According to these six conditions, adherence to labor analgesia protocols was scored from 0 to 6 points.
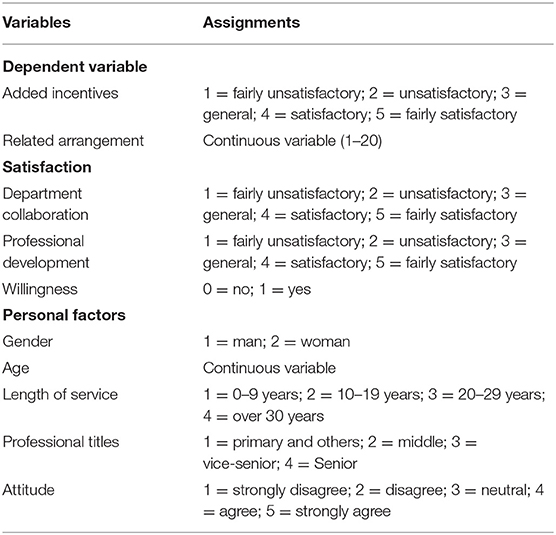
Table 1. Dependent variables and assignments.
Medical institutions' support measures were selected as the independent variable, including added incentives and related arrangements. Added incentives were graded on a scale of 1–5 to indicate “fairly unsatisfactory” to “fairly satisfactory”. According to the Clinical Standardized Management Path for Labor Analgesia, this study created a continuous variable, related arrangement, by adding up adequate staffing sufficient equipment, reasonable health insurance reimbursement, and charging entries, which was scored from 1 to 20 points. According to the availability of the relevant information in the database, the following variables were defined to explore the effect of the mediators and moderators: gender, age, length of service, department, occupation, professional title, and attitude. Among them, the length of service indicated the years that the medical staff had worked in the medical institutions. Attitudes referred to the medical personnel's beliefs about whether labor analgesia is valuable.
Data Analysis
The data analysis consisted of analysis of variance, correlation analysis, mediating effect analysis, and moderating effect analysis. Analysis of variance was used to test the differences in adherence between different groups. Afterward, the Pearson correlation coefficient was used to estimate potential relations between the factors. Finally, mediating effect analysis was carried out to explore the relations between labor analgesia adherence and potential factors based on Baron's three-step method (45). The criteria for mediating effects were as follows: There was statistical significance between the independent variable and the dependent variable and between the independent and mediator variables. Then, the mediator in the regression model that included the independent variable and mediator was statistically significant (46). Similarly to the proposed methods (47), the moderating effect was tested by adding an interaction variable to the regression analysis to test both models. The first model contained potential variables and dependent variables (Model 1) and the second also included an interaction between the two variables (Model 2). And the interaction in Model 2 should be statistically significant when there are moderating effects. The data analysis was performed by SPSS 26.0. The results were regarded as significant when the p-value was < 0.05.
Results
Adherence to Labor Analgesia Protocols
A total of 12,614 medical personnel participated in this survey. As shown in Figure 2, 71.7% of the medical personnel had the highest possible scores for adherence, and medical personnel with low to medium scores (≤ 4) accounted for 11.6% of the total.
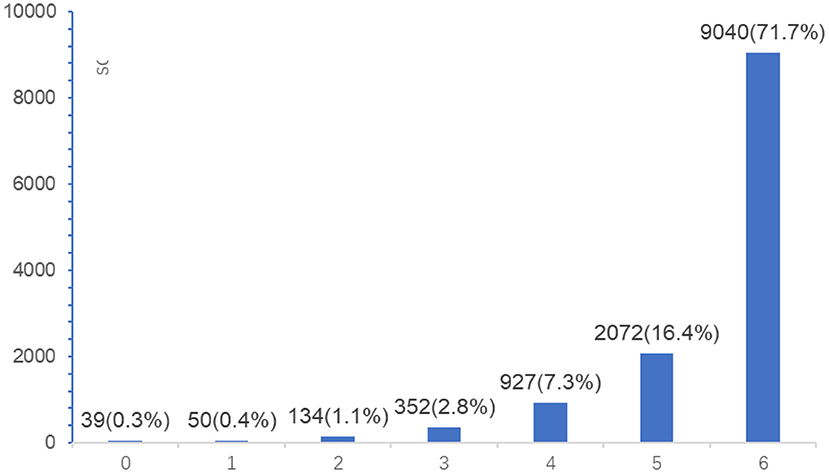
Figure 2. Adherence to labor analgesia protocols among medical personnel.
The Difference in Adherence to Labor Analgesia Protocols
As Table 2 shows, the adherence scores were different among the subgroups with different genders, ages, lengths of service, departments, occupations, professional titles, and attitudes. Female medical staff aged over 48 years or with more than 30 years of working experience had a higher rate of adherence. In addition, midwives and obstetricians with senior professional titles and positive attitudes had better labor analgesia adherence. More details are shown in Table 2.
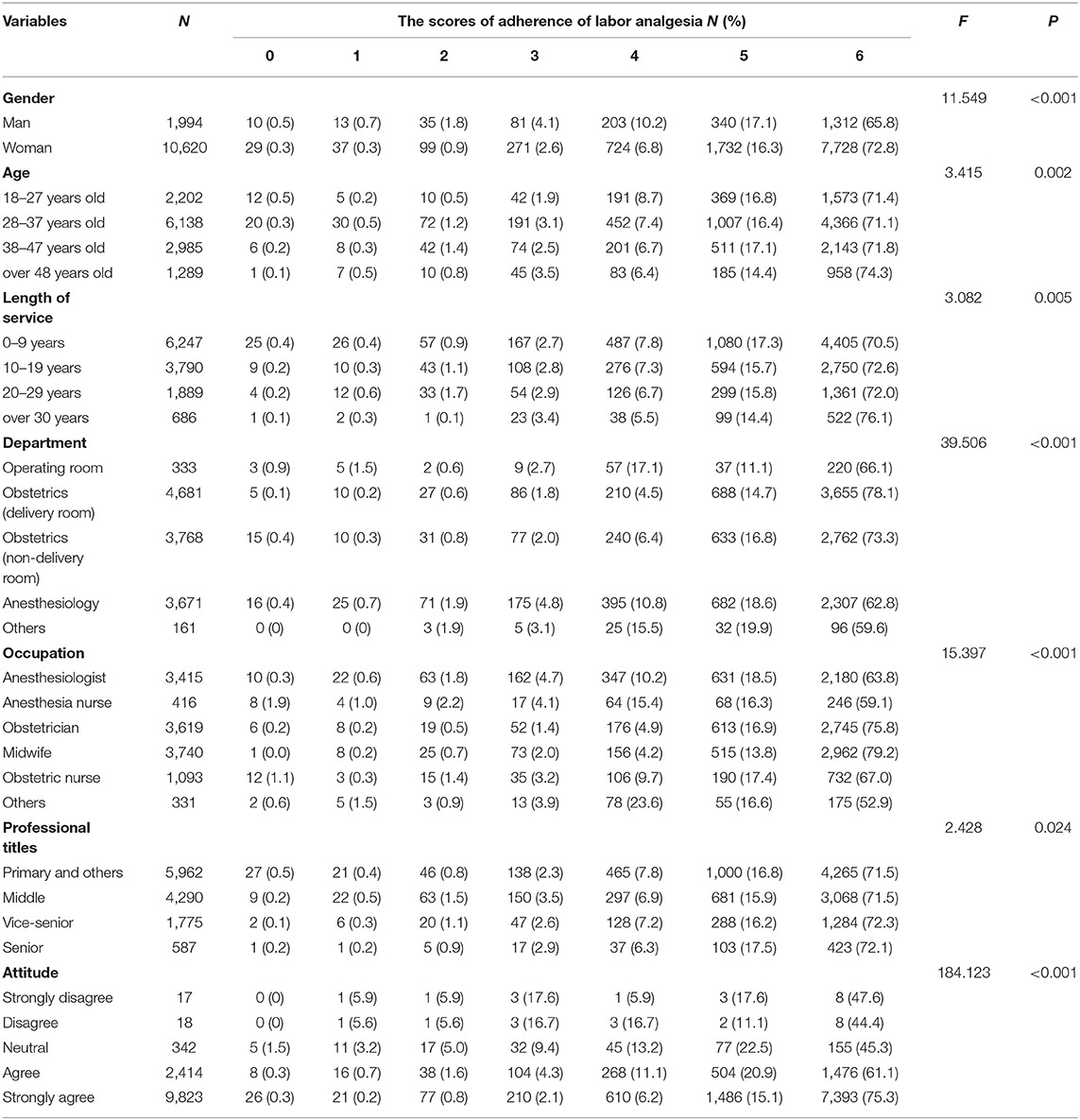
Table 2. Descriptive statistics.
Correlation Analysis Between Labor Analgesia Adherence and Other Factors
As Table 3 illustrates, added incentives and related arrangements were positively correlated with adherence. Correspondingly, department collaboration satisfaction, professional development satisfaction, willingness, and gender were related to adherence and support measures. In addition, a positive attitude was also observed as having a similar correlation with adherence and support measures.
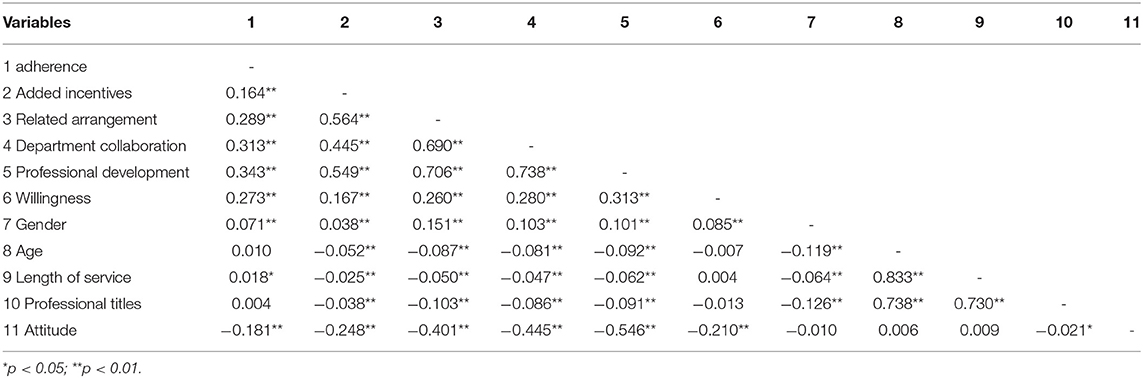
Table 3. Correlations of variables.
Multiple Linear Regression Analysis of Labor Analgesia Adherence
The continuous variables were entered into the multiple linear regression model. The results are shown in Table 4. The multiple linear regression analysis showed the association of added incentives and satisfaction with adherence to labor analgesia policies. However, a correlation between the length of service and professional titles was not found in the model.
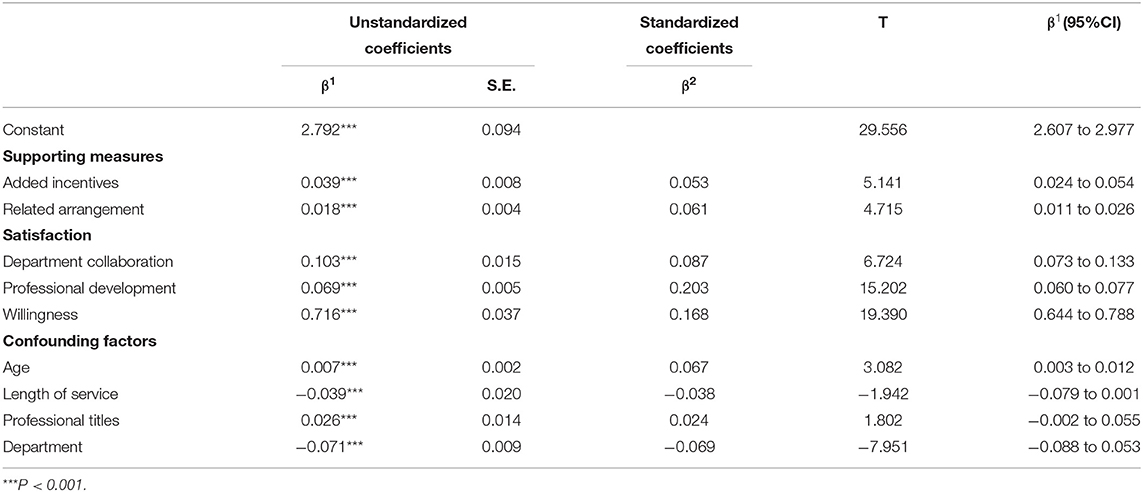
Table 4. Multiple linear regression analysis.
Mediating Effects of Satisfaction on Labor Analgesia Adherence
The estimates derived from the regression model were used to test the conceptual framework. As shown in Table 5, added incentives and related measures had a significant effect on adherence to labor analgesia protocols. Regarding the mediators, the results showed that professional development, department collaboration, and willingness had significant mediating effects on the effect of support measures on adherence to labor analgesia protocols. A significant relationship between support measures and professional development was observed. The correlation coefficient between added incentives and adherence decreased significantly from 0.121 to 0.025 after professional development entered into the regression model. A similar association was seen in analyses of related arrangements.
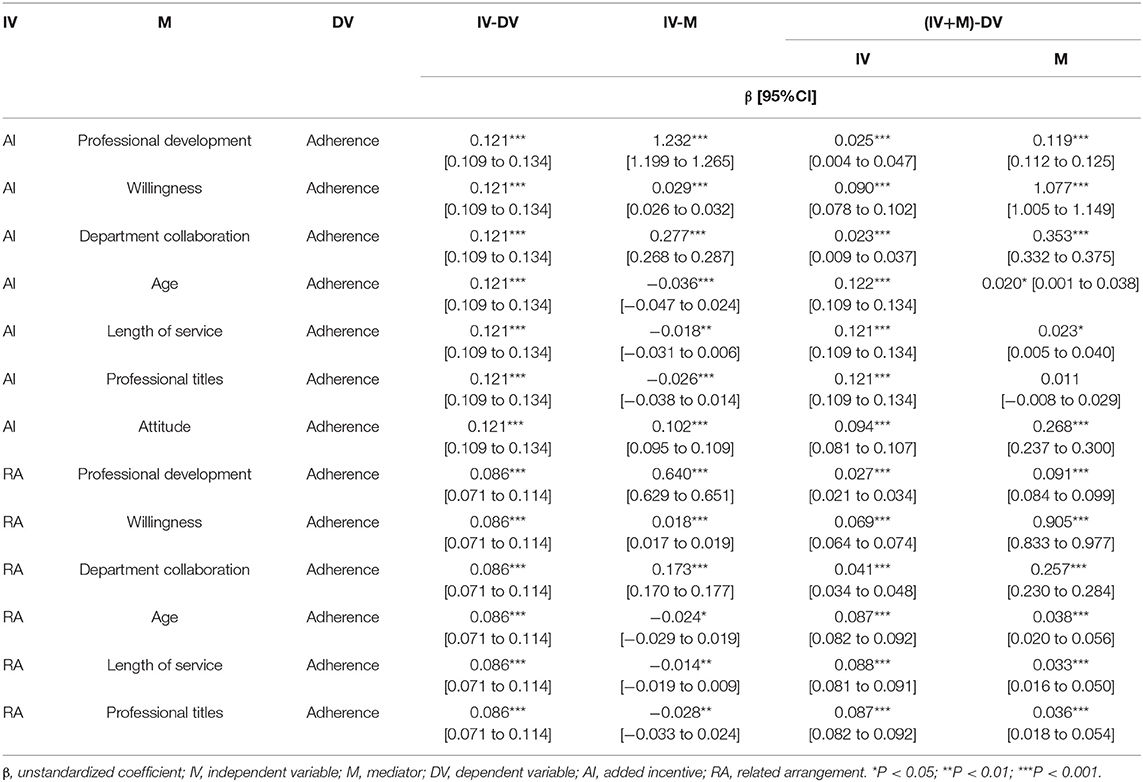
Table 5. Results of mediating effects.
Similarly, department collaboration and willingness mediated the effect of support measures on adherence. The correlation coefficient between added incentives and adherence decreased from 0.121 to 0.090 when willingness was entered into the regression model. In addition, age and length of service positively mediated the relationship between support measures and adherence. A partial mediating effect of professional titles on the relationship between added incentives and adherence was observed.
Moderating Effects of Satisfaction on Labor Analgesia Adherence
As shown in Table 6, Model 1 and Model 2 were developed to estimate the associations among added incentives, professional titles, and the interaction between added incentives and professional titles on adherence. A positive correlation between added incentives and professional titles was observed. The correlation coefficient between added incentives and adherence decreased slightly from 0.121 to 0.109 when professional titles and the interaction between added incentives and professional titles were entered into the regression model. As a result, professional titles moderated the relationship between added incentives and adherence. Likewise, department collaboration moderated the relationship between related arrangements and adherence in Model 3 and Model 4. Attitude had a similar moderating effect in Model 5.
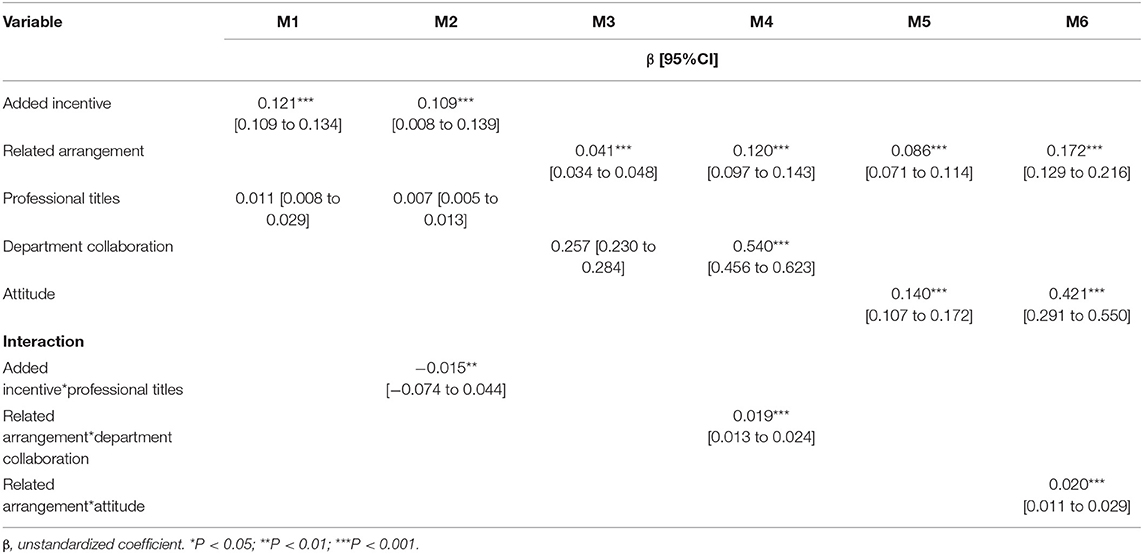
Table 6. Results of moderating effects.
Discussion
Standardized labor analgesia has been recognized as an effective method of promoting safe delivery for pregnant women (48). This study investigated the current situation and associated factors with adherence to labor analgesia protocols by Chinese medical personnel and examined the mediating and moderating effects on satisfaction with adherence. These results are in agreement with a recent study indicating that incentives and related arrangements lead to the improvement of adherence to labor analgesia protocols (49).
The policy, organization, and workforce of labor analgesia need to be further strengthened. Evidence indicates that although the Chinese government strongly supports the development of childbirth analgesia at the national level, it is still in the early stage of implementation, and time is required for further coverage to be developed (18). Based on the medical problems above, it is suggested that the government devote adequate resources and financial support to expand coverage of labor analgesia. In this study, high-scoring medical personnel accounted for 88.1% of the total, but importantly, anesthesiologists and anesthesia nurses had a low level of adherence. A possible explanation is that there is a severe shortage of anesthesiologists (47). There are only 0.5 anesthesiologists per 10,000 people in China, which is far short of the international standard of approximately 2.5 anesthesiologists per 10,000 people (18). However, these trained anesthesiologists are functionally important for improving the level of obstetric anesthesia. The difficulty of obstetric anesthesia and the shortage of staff might contribute to the low adherence to labor analgesia protocols. Thus, medical colleges or associations are suggested to increase anesthesia specialty to expand the scope of anesthesia students and provide more staff training in anesthesiology departments.
Comprehensive incentive measures are conducive to improving satisfaction with labor analgesia in medical personnel. As mentioned above, professional development and willingness played mediating roles in the relationship between supporting measures and adherence (23, 50). This may be explained by the fact that professional development is an important way to develop professional skills and income, which are more attractive to young people with more junior professional titles (40). In addition, comprehensive incentives are likely to improve medical personnel's willingness, which is significantly associated with good knowledge and adherence to labor analgesia standards (39). Comprehensive incentives leading to a sustained improvement in adherence in terms of labor analgesia are expected. These findings suggest that medical institutions should adopt individual incentive measures to improve medical personnel's enthusiasm for the use of labor analgesia in addition to the national-level promotion plan. These insights can help to contribute to the ongoing policy and incentives toward improving adherence to labor analgesia policies, thus addressing pregnant women's needs in the future.
To improve adherence to labor analgesia protocols, capacity-building programmes for medical institutions are recommended to enhance department collaboration and change medical personnel's attitudes. The level of departmental collaboration is an essential way to strengthen doctors' medical skills, which suggests the significance of cooperation between medical teams for treatment (43, 51). In addition, medical personnel's attitudes toward labor analgesia deserve more attention. It was found that the attitude of professionals is significantly related to labor analgesia. Some medical personnel believe that labor analgesia affects pregnant women's health and thus reduces their use of labor analgesia (39). Increasing the risk of illness and delaying delivery are common reasons why medical personnel are unwilling to provide labor analgesia (52). However, the National Association of Obstetricians and Gynecologists (ACOG) passed a series of clinical trials and proved that labor analgesia is unrelated to the incremental maternal prevalence (53, 54). This misunderstanding may be the cause of low adherence (55). Therefore, strengthening training for the target group and enhancing interdepartmental cooperation are suggested for improving low adherence among certain groups, such as anesthesiologists and anesthesia nurses. Meanwhile, labor analgesia in China is currently concentrated mainly in specialty hospitals. It is recommended that general hospitals improve their ability to provide labor analgesia services by preparing specific internal protocols and arranging adequate training for the involved personnel.
Limitation
Some limitations of this study need to be mentioned. First, this study used a cross-sectional survey. It therefore could not determine the long-term status of the adherence to labor analgesia protocols in Chinese medical personnel. A cross-sectional study has limited ability to infer causality and the potential for reverse causation. In addition, retrospective self-assessment may lead to bias, and medical personnel may miss some specific details during the investigation process. In addition, this survey was conducted through a web-based questionnaire, and the quality of the investigation process was difficult to control.
Conclusion
This study aimed to investigate the current situation and associated factors with the adherence to labor analgesia protocols by Chinese medical personnel. The results show that willingness had direct and indirect beneficial effects on adherence to labor analgesia protocols. Satisfaction played an important role in the improvement of labor analgesia. The government should continue to reinforce the promotion of labor analgesia to continue to improve the proportion of financial support. More training opportunities should be provided for more anesthesiologists and anesthesia nurses to enhance knowledge about labor analgesia knowledge. More capacity-building programmes should be launched to improve interdepartmental collaboration. An effective incentive mechanism needs to be designed to attract more medical staff, especially skilled personnel, to participate in labor analgesia work.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
DL: analyzed the data and wrote the original draft preparation. CLo, SL, YX, FC, RZ, and ST: gave the critical feedback. All authors: conceptualization and data collection. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Filippi V, Ronsmans C, Campbell OM, Graham WJ, Mills A, Borghi J, et al. Maternal health in poor countries: the broader context and a call for action. Lancet. (2006) 368:1535–41. doi: 10.1016/S0140-6736(06)69384-7
2. Parkhurst JO, Penn-Kekana L, Blaauw D, Balabanova D, Danishevski K, Rahman SA, et al. Health systems factors influencing maternal health services: a four-country comparison. Health Policy. (2005) 73:127–38. doi: 10.1016/j.healthpol.2004.11.001
3. Green A, Gerein N, Mirzoev T, Bird P, Pearson S, Anh LV, et al. Health policy processes in maternal health: a comparison of Vietnam, India and China. Health Policy. (2011) 100:167–73. doi: 10.1016/j.healthpol.2010.11.016
4. Zhao Q, Chen J, Li F, Li A, Li Q. An integrated model for evaluation of maternal health care in China. PLoS ONE. (2021) 16:e0245300. doi: 10.1371/journal.pone.0245300
5. Kassebaum NJ, Barber RM, Bhutta ZA, Dandona L, Gething PW, Hay SI, et al. Global, regional, and national levels of maternal mortality, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. (2016) 388:1775–812. doi: 10.1016/S0140-6736(16)31470-2
6. Souza J, Tunçalp Ö, Vogel J, Bohren M, Widmer M, Oladapo O, et al. Obstetric transition: the pathway towards ending preventable maternal deaths. BJOG Int J Obstet Gynaecol. (2014) 121:1–4. doi: 10.1111/1471-0528.12735
7. Leighton BL, Halpern SH. The effects of epidural analgesia on labor, maternal, and neonatal outcomes: a systematic review. Am J Obstet Gynecol. (2002) 186:S69–77. doi: 10.1016/S0002-9378(02)70182-8
8. Burnstein R, Buckland R, Pickett JA. A survey of epidural analgesia for labour in the United Kingdom. Anaesthesia. (1999) 54:634–40. doi: 10.1046/j.1365-2044.1999.00894.x
9. Bucklin BA, Hawkins JL, Anderson JR, Ullrich FA. Obstetric anesthesia workforce survey: twenty-year update. Anesthesiology. (2005) 103:645–53. doi: 10.1097/00000542-200509000-00030
10. Harkins J, Carvalho B, Evers A, Mehta S, Riley ET. Survey of the factors associated with a woman's choice to have an epidural for labor analgesia. Anesthesiol Res Pract. (2010) 2010:e356789. doi: 10.1155/2010/356789
11. Stamer UM, Messerschmidt A, Wulf H, Hoeft A. Practice of epidural analgesia for labour pain: a German survey. Eur J Anaesthesiol. (1999) 16:308–14. doi: 10.1046/j.1365-2346.1999.00488.x
12. Okojie N, Isah E. Perception of epidural analgesia for labour among pregnant women in a Nigerian tertiary hospital setting. J West Afr Coll Surg. (2014) 4:142–62.
13. Mohamed RA, Eldien HA. Knowledge and attitude of antenatal women toward analgesia during labor and their choice for mode of delivery. Assiut Sci Nurs J. (2014) 2:110–8. doi: 10.21608/asnj.2014.191985
14. Di G-H, Yao S-L, Wang J, Wu Z-L, Liu H, Wang H. Factors influencing the improvement of neuraxial labor analgesia in China: a questionnaire survey. Chin Med J. (2020) 133:613. doi: 10.1097/CM9.0000000000000529
15. Hung T-H, Hsieh T-T, Liu H-P. Differential effects of epidural analgesia on modes of delivery and perinatal outcomes between nulliparous and multiparous women: a retrospective cohort study. PLoS ONE. (2015) 10:e0120907. doi: 10.1371/journal.pone.0120907
16. Hu L-Q, Zhang J, Wong CA, Cao Q, Zhang G, Rong H, et al. Impact of the introduction of neuraxial labor analgesia on mode of delivery at an urban maternity hospital in China. Int J Gynaecol Obstet. (2015) 129:17–21. doi: 10.1016/j.ijgo.2014.10.030
17. Eidelman A, Hoffmann N, Kaitz M. Cognitive deficits in women after childbirth. Obstet Gynecol. (1993) 81:764–7.
18. Wu J, Ling K, Song W-T, Yao S-L. Perspective on the low labor analgesia rate and practical solutions for improvement in China. Chin Med J. (2020) 133:606–08. doi: 10.1097/CM9.0000000000000660
19. Ibach F, Dyer RA, Fawcus S, Dyer SJ. Knowledge and expectations of labour among primigravid women in the public health sector. South Afr Med J. (2007) 97:461–4.
20. Samarah W, Bsisu I, Al-Masad Q, Maaqbeh B, Younis L, Walid H, et al. Knowledge, misconceptions and attitudes towards labor regional analgesia in a university hospital: a cross-sectional. Res Health Sci. (2019) 4:10. doi: 10.22158/rhs.v4n3p167
21. Narayanappa A, Gurulingaswamy S, Prabhakaraiah U, Kempegowda K, Hanumantharayappa NB. Practice of labor analgesia among anesthesiologists across India: cross-sectional study. Anesth Essays Res. (2018) 12:651–656. doi: 10.4103/aer.AER_74_18
22. Wang Q, Zheng S-X, Ni Y-F, Lu Y-Y, Zhang B, Lian Q-Q, et al. The effect of labor epidural analgesia on maternal–fetal outcomes: a retrospective cohort study. Arch Gynecol Obstet. (2018) 298:89–96. doi: 10.1007/s00404-018-4777-6
23. Behruzi R, Hatem M, Fraser W, Goulet L, Ii M, Misago C. Facilitators and barriers in the humanization of childbirth practice in Japan. BMC Pregnancy Childbirth. (2010) 10:25. doi: 10.1186/1471-2393-10-25
24. Gong Z-K, Zhou C-M, Li H. Exploration and practice on standard technical service for labor analgesia. Matern Child Health Care China (2012) 27:3541–3.
25. Kent JL, Tondravi N, Omar A, Williams K, Clark SM, Bauchat JR. Acceptability and Preferences for Labor Analgesia in Dominican Women. Northwestern Memorial Hospital, Chicago, IL.
26. Geltore TE, Kelbore AG, Angelo AT. Perceptions of obstetric analgesia: a qualitative study among midwives attending normal vaginal deliveries in Durame Hospital, Southern Ethiopia. J Pain Res. (2019) 12:2187–192. doi: 10.2147/JPR.S209913
27. Gertler PJ, Vermeersch C. Using Performance Incentives to Improve Health Outcomes. Rochester, NY: Social Science Research Network (2012). Available online at: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2089240 (accessed May 22, 2022).
28. Benson SG, Dundis SP. Understanding and motivating health care employees: integrating Maslow's hierarchy of needs, training and technology. J Nurs Manag. (2003) 11:315–20. doi: 10.1046/j.1365-2834.2003.00409.x
29. Roro MA, Hassen EM, Lemma AM, Gebreyesus SH, Afework MF. Why do women not deliver in health facilities: a qualitative study of the community perspectives in south central Ethiopia? BMC Res Notes. (2014) 7:556. doi: 10.1186/1756-0500-7-556
30. Kamakshi G, Anju G, Tania S, Priyanka G, Kamya B, Gegal P, et al. Epidural analgesia during labor: Attitudes among expectant mothers and their care providers. Anesth Essays Res. (2018) 12:501. doi: 10.4103/aer.AER_48_18
31. Grol R, Mokkink H, Smits A, Van Eijk J, Beek M, Mesker P, Mesker-Niesten J. Work satisfaction of general practitioners and the quality of patient care. Fam Pract. (1985) 2:128–35. doi: 10.1093/fampra/2.3.128
32. Bovier PA, Perneger TV. Predictors of work satisfaction among physicians. Eur J Public Health. (2003) 13:299–305. doi: 10.1093/eurpub/13.4.299
33. Newsam R. Operating department practitioners and midwives: the undervalued obstetric care collaboration. Br J Midwifery. (2018) 26:714–21. doi: 10.12968/bjom.2018.26.11.714
34. Raab CA, Will SEB, Richards SL, O'Mara E. The effect of collaboration on obstetric patient safety in three academic facilities. J Obstet Gynecol Neonatal Nurs. (2013) 42:606–16. doi: 10.1111/1552-6909.12234
35. Wu J, Yao S-L. Obstetric anesthesia in China: associated challenges and long-term goals. Chin Med J. (2020) 133:505–8. doi: 10.1097/CM9.0000000000000664
36. Kim SE, Kim CW, Lee SJ, Oh JH, Lee DH, Lim TH, et al. A questionnaire survey exploring healthcare professionals' attitudes towards teamwork and safety in acute care areas in South Korea. BMJ Open. (2015) 5:e007881. doi: 10.1136/bmjopen-2015-007881
37. O'Malley AS, Gourevitch R, Draper K, Bond A, Tirodkar MA. Overcoming challenges to teamwork in patient-centered medical homes: a qualitative study. J Gen Intern Med. (2015) 30:183–92. doi: 10.1007/s11606-014-3065-9
38. Boag-Hodgson C, Duong A, Bagley L. Attitudes toward safety and teamwork: benchmarking australian surgeons and nurses. J Patient Saf. (2022) 10:1097. doi: 10.1097/PTS.0000000000001005
39. Geltore TE, Taye A, Kelbore AG. Utilization of obstetric analgesia in labor pain management and associated factors among obstetric caregivers in public health facilities of Kembata Tembaro Zone, Southern Ethiopia. J Pain Res. (2018) 11:3089–97. doi: 10.2147/JPR.S165417
40. Vandendriesen NM, Lim W, Paech MJ, Michael C. Obstetricians' knowledge and attitudes toward epidural analgesia in labour. Anaesth Intensive Care. (1998) 26:563–7. doi: 10.1177/0310057X9802600514
41. Madden KL, Turnbull D, Cyna AM, Adelson P, Wilkinson C. Pain relief for childbirth: the preferences of pregnant women, midwives and obstetricians. Women Birth. (2013) 26:33–40. doi: 10.1016/j.wombi.2011.12.002
42. Chen Q, Yang L, Feng Q, Tighe SS. Job satisfaction analysis in rural China: a qualitative study of doctors in a township hospital. Scientifica. (2017) 2017:e1964087. doi: 10.1155/2017/1964087
43. Sandie CL, Heindel LJ. The knowledge and attitudes of nonanesthesia nurses regarding postoperative epidural analgesia. AANA J. (1999) 67:455–60.
44. Klein MC, Liston R, Fraser WD, Baradaran N, Hearps SJ, Tomkinson J, et al. Attitudes of the new generation of Canadian obstetricians: how do they differ from their predecessors? Birth. (2011) 38:129–39. doi: 10.1111/j.1523-536X.2010.00462.x
45. Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J Pers Soc Psychol. (1986) 51:1173.
46. Deng Z, Lu Y, Wei KK, Zhang J. Understanding customer satisfaction and loyalty: An empirical study of mobile instant messages in China. Int J Inf Manag. (2010) 30:289–300. doi: 10.1016/j.ijinfomgt.2009.10.001
47. Freire C, Ferradás M del M, Núñez JC, Valle A, Vallejo G. Eudaimonic well-being and coping with stress in university students: the mediating/moderating role of self-efficacy. Int J Environ Res Public Health. (2019) 16:48. doi: 10.3390/ijerph16010048
48. Poomalar GK, Sameera L. Awareness of labour analgesia among antenatal women in semi urban area. Int J Reprod Contracept Obstet Gynecol. (2016) 2612–7. doi: 10.18203/2320-1770.ijrcog20162631
49. Ponnusamy R, Reddy HKV, Murugesan R. Awareness, knowledge and attitude about labor analgesia among providers and parturients; a survey based study. Anaesth Pain Intensive Care. (2018) 73–80. Available online at: https://www.apicareonline.com/index.php/APIC/article/view/24
50. Carlton T, Callister LC, Christiaens G, Walker D. Labor and delivery nurses' perceptions of caring for childbearing women in nurse-managed birthing units. MCN Am J Matern Nurs. (2009) 34:50–56. doi: 10.1097/01.NMC.0000343866.95108.fa
51. Lockhart-Wood K. Collaboration between nurses and doctors in clinical practice. Br J Nurs. (2000) 9:276–80. doi: 10.12968/bjon.2000.9.5.6363
52. McCauley M, Stewart C, Kebede B. A survey of healthcare providers' knowledge and attitudes regarding pain relief in labor for women in Ethiopia. BMC Pregnancy Childbirth. (2017) 17:56. doi: 10.1186/s12884-017-1237-4
53. ACOG Committee on Obstetric Practice. ACOG Committee Opinion number 269 February (2002). Analgesia and cesarean delivery rates. American College of Obstetricians and Gynecologists. Obstet Gynecol. (2002) 99:369–70. doi: 10.1016/s0029-7844(01)01770-7
54. American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 209: obstetric analgesia and anesthesia. Obstet Gynecol. (2019) 133:e208–25. doi: 10.1097/AOG.0000000000003132
55. McCauley M, Actis Danna V, Mrema D, van den Broek N. “We know it's labour pain, so we don't do anything”: healthcare provider's knowledge and attitudes regarding the provision of pain relief during labour and after childbirth. BMC Pregnancy Childbirth. (2018) 18:444. doi: 10.1186/s12884-018-2076-7
Keywords: adherence, labor analgesia, personnel medical, maternal health, China
Citation: Lang D, Long C, Lin S, Xie Y, Chen F, Zhao R, Liu C and Tang S (2022) Satisfaction as a Mediator and Its Interaction With Adherence to Labor Analgesia Protocols: A Cross-Sectional Survey of Chinese Medical Personnel. Front. Public Health 10:899515. doi: 10.3389/fpubh.2022.899515
Received: 25 March 2022; Accepted: 03 June 2022;
Published: 28 June 2022.
Edited by:
Mihajlo Jakovljevic, Hosei University, JapanReviewed by:
Franklin Dexter, The University of Iowa, United StatesCelestin Ndikumana, University of Rwanda, Rwanda
Copyright © 2022 Lang, Long, Lin, Xie, Chen, Zhao, Liu and Tang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shangfeng Tang, c2Z0YW5nMjAxOEBodXN0LmVkdS5jbg==