
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 21 September 2022
Sec. Public Health Education and Promotion
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.895506
 Justyna Kosydar-Bochenek1
Justyna Kosydar-Bochenek1 Sabina Krupa1
Sabina Krupa1 Dorota Religa2
Dorota Religa2 Adriano Friganovic3,4
Adriano Friganovic3,4 Ber Oomen5Ged Williams6Kathleen M. Vollman7Maria Isabelita C. Rogado8Sandra Goldsworthy9
Ber Oomen5Ged Williams6Kathleen M. Vollman7Maria Isabelita C. Rogado8Sandra Goldsworthy9 Violeta Lopez10
Violeta Lopez10 Elena Brioni11
Elena Brioni11 Wioletta Medrzycka-Dabrowska12*
Wioletta Medrzycka-Dabrowska12*Introduction: A good working climate increases the chances of adequate care. The employees of Emergency in Hospitals are particularly exposed to work-related stress. Support from management is very important in order to avoid stressful situations and conflicts that are not conducive to good work organization. The aim of the study was to assess the work climate of Emergency Health Services during COVID-19 Pandemic using the Abridged Version of the Work Climate Scale in Emergency Health Services.
Design: A prospective descriptive international study was conducted.
Methods: The 24-item Abridged Version of the Work Climate Scale in Emergency Health Services was used for the study. The questionnaire was posted on the internet portal of scientific societies. In the study participated 217 women (74.5%) and 74 men (25.4%). The age of the respondents ranged from 23 to 60 years (SD = 8.62). Among the re-spondents, the largest group were Emergency technicians (85.57%), followed by nurses (9.62%), doctors (2.75%) and Service assistants (2.06%). The study was conducted in 14 countries.
Results: The study of the climate at work shows that countries have different priorities at work, but not all of them. By answering the research questions one by one, we can say that the average climate score at work was 33.41 min 27.0 and max 36.0 (SD = 1.52).
Conclusion: The working climate depends on many factors such as interpersonal relationships, remuneration or the will to achieve the same selector. In the absence of any of the elements, a proper working climate is not possible.
Work climate is the quality of the work environment perceived by employees, which productivity, motivation and employee behavior affects. In the case of healthcare, it also influences the effectiveness or quality of patient care (1). The appropriate working climate is conducive to better organization of work and the proper functioning of the departments. Emergency Units employees are a very vulnerable group to the occurrence of stress. This stress can be related to both emergency situations and the need to make quick and appropriate decisions. With a good working climate, there is less risk of confusion, misunderstandings or organizational errors (1). The COVID-19 pandemic has contributed to an increase in the number of people hospitalized and situations where healthcare workers are tired, burned out, and therefore reflective and irritable. Such situations have a destructive effect on teamwork. Literature reports that a high level of care can be found in places where workers are supported by their employers (2). Considering the responsibility and constant traumatic situations faced by Emergency employees, they may develop post-traumatic stress disorder and depression. (3). A very important issue is the support that employees should receive from decision-makers, but they should also support each other and work as a team. Milton et al. Pointed to opportunities to improve attitudes among ED team members through specific organizational changes and learning from each other (4). During the COVID-19 pandemic, people were isolated from each other and only going to work often gave a sense of “normality” and the possibility of contact with other people (5). Lasalvia et al. found that one year after the COVID-19 outbreak, nurses were most likely to experience anxiety and depression, while residents were most likely to experience burnout (in terms of low work performance). Working in intensive care units was associated with an increased risk of developing severe emotional exhaustion and a cynical approach to work (6). A study by Norkiene et al. which was carried out in the UK and Lithuania, showed that psychosocial support for health professionals should be provided to prevent burnout and loss of personnel during a pandemic, as half of the study participants from two countries with different histories and health systems reported similar proportions of participants considering a career change. If these people acted as intended, it could cause serious problems with staff and healthcare in the UK and Lithuania. The threat of enormous staff shortages in such critical specialties is concerning (7). In studies by Teo et al. teamwork and a sense of appreciation at work were shown to be protective in nature and to serve as targets for the development of organizational interventions to alleviate expected underperformance among frontline health professionals. (8). The impact of a negative psychosocial work environment has been identified as a contributing factor in the occurrence of errors and adverse events in hospitals. Rasmussen et al. showed that the work environment, poor patient safety climate and increased cognitive demands were significantly correlated with adverse events (9). A key element of the literature review by Johnston was that perceptions of the work environment varied by clinical staff and study site, but the high level of autonomy and teamwork balanced the stress of high pressure and heavy workload (10). There are not many instruments to assess the work climate in health care. Most of the work is about the organizational work climate of nurses in the dimension of safety climate or ethical climate. Not much is about work climate in emergency services (1–9). This paper helps to understand the limitations of the work climate and can contribute to improving the work climate in the work of Emergency Health Services. This research allows to discover the elements which limit the work climate.
The purpose of this study was to assess the work climate of Emergency Health Services during COVID-19 Pandemic using the Abridged Version of the Work Climate Scale in Emergency Health Services.
A prospective descriptive study was conducted in an international group. The authors followed the guidelines of the Declaration of Helsinki (World Medical Association, 2013) and STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) (11).
The study was conducted using a standardized questionnaire that was posted on the website of scientific societies. In total, the questionnaire was completed by 291 respondents from 14 countries. The authors had no influence on how many surveys would be collected and from which country. An electronic survey was available but there was no plotted number of results collected.
Two hundred and ninety-one People Working at Emergency Units from 14 Countries Participated in the Study. 217 Women (74.5%) and 74 men (25.4%) Participated in the Study. The age of the Respondents Ranged from 23 to 60 Years (SD = 8.62). Among the re-Spondents, the Largest Group Were Emergency Technicians (85.57%), Followed by Nurses (9.62%), Doctors (2.75%) and Service Assistants (2.06%). As for the Type of Employment Contract, 271 People (93.13%) Had an Indefinite Contract, 11 People (3.78%) Had a Temporary Contract (Part-Time) and 9 People (3.09%) Were on a Training Contract.
The study used the Abridged Version of the Work Climate Scale in EHS, which consists of 24 items divided into 4 elements such as: Work Satisfaction, Productivity / Achievement of aims, Interpersonal relationships and Performance at work. This scale also provided 2 open questions: What is your level of participation in the decisions of the work team? Do you have any suggestions on improving the work climate? In addition to open-ended questions, participants could rate individual statements from 1 to 5, with 1 being low and 5 being the highest possible. An abridged version of the scale consisted of 24 items. Factor 1—Work satisfaction, includes 8 items, Factor 2—productivity / achievement of aims, includes 8 items; Factor 3—Interpersonal relationships, contains 4 items, and Factor 4—Performance at work, also contains 4 items (1).
The Work Climate Scale in Emergency Services: Abridged Version, is the first short and comprehensive scale to measure four work climate factors: work satisfaction (F1), productivity / achievement of aims (F2), interpersonal relations (F3), and performance at work (F4) in the emergency services employee group. This scale is based on a 40-item work climate scale in hospital emergency services (WCSHES) (12). The original scale was developed by Lozano-Lozano (1). The study was conducted on a group of one hundred thirteen EHS workers from two different hospitals in Gibraltar Countryside County. Good psychometric properties were confirmed, obtaining satisfactory results of accuracy and reliability. Unfortunately, one of the limitations of the scale, which the authors emphasize, is its length.
The abridged 24-item version was developed by a research team led by Lozano-Lozano based on a study conducted on a group of 126 emergency health workers in Chile. It is a good tool for assessing the work climate in emergency services, also because of its brevity and simplicity. The reliability rates for the abridged version were very satisfactory (α = 0.94 and ω = 0.94) compared with α = 0.96 and ω = 0.96 for the original version. The correlation of the original version with the criteria was ρXY = 0.68, and the correlation of the abridged 24-item version with the criteria was also ρXY = 0.68, with a model fit of χ2 (248) = 367.84; p <0.01, RMSEA = 0.06 with an interval of 90% from 0.05 to 0.07, SRMR = 0.08, GFI = 0.9, AGFI = 0.96, CFI = 0.98, NFI = 0.95, and NNFI = 0.98 (13). So far, the scale has only been used in a validation study in Chile. Studies with this tool in other populations are recommended (1).
F1 Work satisfaction refers to feelings evoked in workers by their job and their conditions: self-confidence due to the experience, the adequacy of the workday or time for each patient, contentment with relationships with other professionals outside the group and patients and their relatives, pride, success, cohesion, or nervousness facing new circumstances (12).
F2 Productivity/achievement of aims refers to the perception of workers having everything they need to do their job or, on the contrary, lacking what they need to achieve their goals: understanding of the relevance, capabilities, and specialization of others; the value of working in a group; motivation and fulfillment of expectations; recognition of their work as a group; self-improvement; infrastructure; training and the characteristics and functioning of their service; patients' characteristics fitting with their specialization and knowledge of such characteristics; protocols; and coordination with other hospital services (12).
F3 Interpersonal relationships refer to the feelings when workers relate to other members of the group and aspects that influence such feelings: the quality of the communication, their relationship, the level of comfort, their friendship, their conflicts, being recognized for their individual contributions, having the resources they need, following a plan, participating in decisionmaking, and productivity (12).
Finally, F4 Performance at work includes everything related to the development of workers' job placement: the perceived importance of their job and capacity to decide how to improve their performance; the skills and knowledge they use; and their knowledge of their tasks and others' tasks, their individual and group limitations, and their patients (12).
The overall score is obtained by adding the score given foreach item (24 is the lowest possible score and 120 the highest). In the same way, a score can be obtained for each factor by adding up the scores for the corresponding items.
The study was conducted from November 1 to December 20, 2021 as an online survey. The tool was disseminated via messengers, websites, and social media related to emergency medical services and emergency medicine. The tool was made available in English. The information about the study stated that the study is aimed only for people who worked in a hospital during the COVID-19 pandemic.
By completing the questionnaire, the participants expressed their consent to participate in the study, but they could withdraw from the study at any stage of completing the form.
The inclusion criteria were: health care workers from emergency units; adult; people who are working with COVID-19 patients.
An application was submitted to the Bioethics Committee at the University of Rzeszów (KBE No. 09/05/2020) in order to obtain a positive opinion on the study.
All statistical calculations were carried out using the IBM SPSS 23 statistical package (Armonk, NY, USA) and an Excel 2016 preadsheet. The statistical analysis included the baseline measurement adjusted to the variables, mean, standard deviation, N (%). The following rules were adopted: p < 0.05—statistically significant relationship. ANOVA uses F-tests to statistically test the equality of means.
Factor 1 corresponded to Work Satisfaction. The mean work climate score was 33.41 (SD = 1.52). Factor 2 was labeled Productivity / Achievement of aims and was on average 26.95 (SD = 1.11). Factor 3 corresponded to Interpersonal relationships and averaged 16.16 (SD = 1.39). The last Factor 4 was Performance at work and averaged 18.07 (SD = 1.24). In all calculations, the significance level was p ≤ 0.05. ANOVA uses F-tests (F) to statistically test the equality of means.
In the next stage, the work climate was measured for individual variables such as: Gender, Profession, Type of employment contract. Assuming that p < 0.05, no statistical significance was demonstrated in the Factors 1–4 in relation to the variables. The results are presented in Table 1.
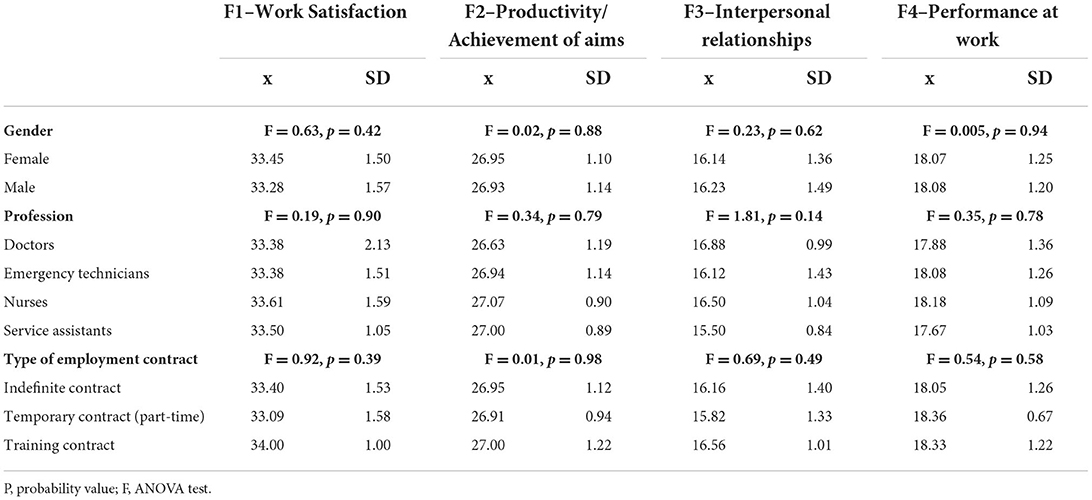
Table 1. Impact of variables: gender, profession, type of employment contract on factors of work climate.
Statistical significance was demonstrated in Factors 1–4 in relation to the variable which was age. Pearson correlation is between age of respondents and work climate variables: work satisfaction, productivity/achievement of aims, interpersonal relationships and performance at work. Static significance (p) values are presented in Table 2.

Table 2. Statistical significance of the age variable in relation to individual factors.
The highest average level of work satisfaction (Factor 1) was demonstrated for workers from Canada and the lowest for workers from San Marino. For Factor 2, the highest average level was again recorded in Canada and the lowest for the residents of San Marino. In Factor 3, related to Interpersonal relationships, the highest average scores were given by employees from Netherland, while the lowest for interpersonal relationships was given by the residents of San Marino. Performance at work (Factor 4) was rated the highest by the residents of England, while the lowest was recorded by participants from Turkey. As for Factors 1–4, statistical significance was demonstrated at each level in relation to the countries that took part in the study. ANOVA uses F-tests (F) to statistically test the equality of means. The results are presented in Table 3.
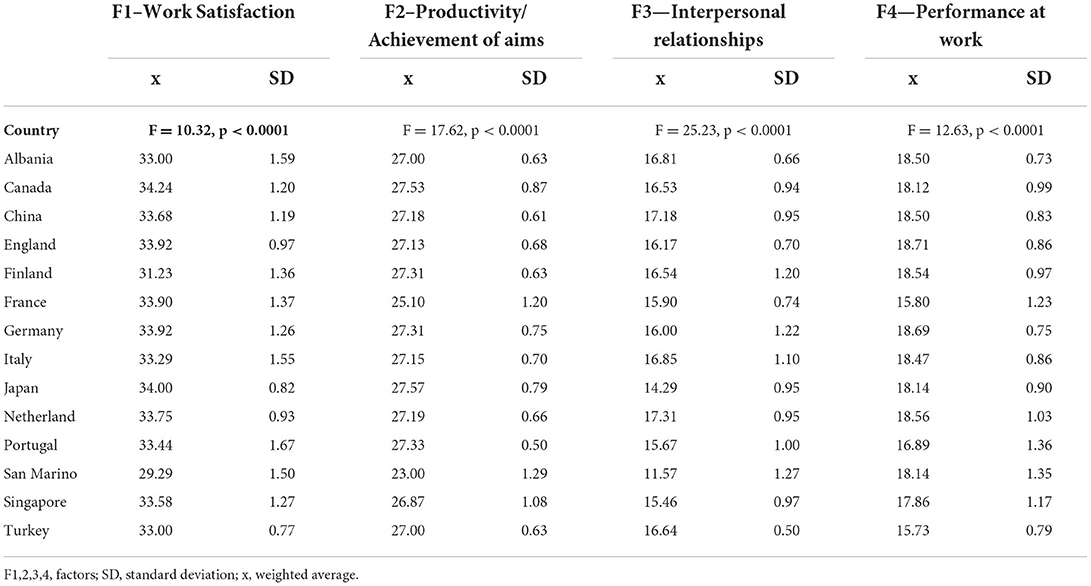
Table 3. Correlations between factors 1–4 and the countries included in the study.
In the next stage, means and standard deviations for the entire population of people participating in the study were analyzed. In Factor 1, the respondents gave the highest scores to the statement “We strive to achieve successful outcomes,” and the lowest to “Relevance of the job of each member.” In Factor 2, the claim “Our work group is known for its productivity” scored the highest, while the claim “The merit of our good job is recognized” received the lowest score. In Factor 3, the highest rated the statement “I feel comfortable with my work group,” and the lowest “We have good communication within the group.” In Factor 4, out of 4 possible statements, the highest scores were “Our patients fit the specialty of our service” and the lowest was “I know my professional shortcomings.” The results of the mean results (x) and standard deviation (SD) are presented in Table 4.
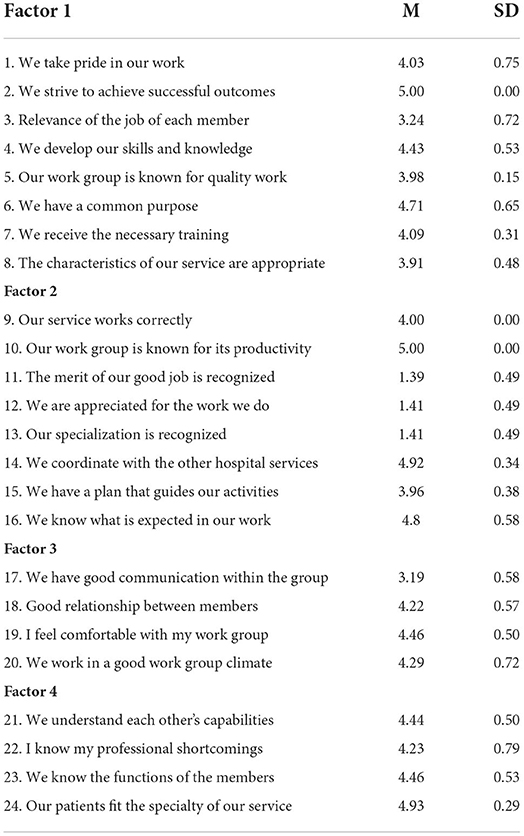
Table 4. Mean (M) and standard deviation (SD) results in the overall population tested in factors 1–4.
Despite the lack of research with the use of the original full version of the tool, it should be stated that the abbreviated version of the scale does not differ from the full version (1).
The study, using the Work Climate Scale in Emergency Services: Abridged Version, was divided into 4 Factors. Work satisfaction was 33.41 (SD = 1.52), productivity / Achievement of aims averaged 26.95 (SD = 1.11), Interpersonal relationships averaged 16.16 (SD = 1.39) and Performance at work averaged 18.07 (SD=1.24). The obtained factors show some similarities to those obtained in previous studies (Table 5).
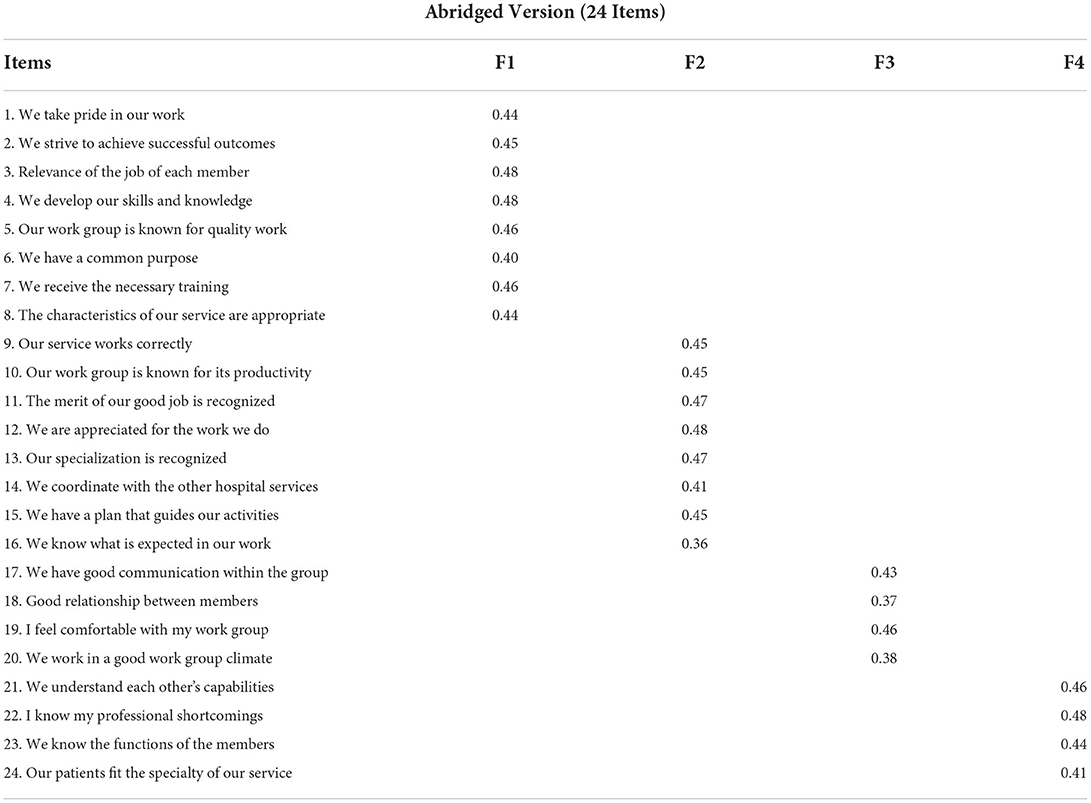
Table 5. Standardized factors loadings obtained in the Confirmatory Factor Analysis, CFA.
The first factor of them was responsible for job satisfaction. In a job satisfaction study, Chinese authors showed average job satisfaction, measuring it on a scale of 1–6. Among the sociodemographic variables, the occupation, education, professional status, length of service, annual income and frequency of night shifts had a significant impact on the level of job satisfaction. Stress at work, the work-family conflict, and the doctor-patient relationship also had a significant impact on job satisfaction (14). Based on the results of the study by Janicijevic et al. it can be seen that employee satisfaction, e.g., with salaries, has almost no impact on patient satisfaction (15) Linn et al. in their study they showed that hospital staff have difficulties meeting the needs of their patients if their own needs are not being met (16). Similar conclusions have also been noted by Hasenfeld et al. (17). In their own research, the respondents highly rated the Factor 1 claim that they strive to achieve successful outcomes. In the study of Javanmardnejad et. al. it has been shown that nurses working in emergency departments do not feel happy. In addition, the findings suggest that their happiness was related to their economic status and closure of duties (18).
In their own research, the respondents highly rated the Factor 1 claim that they strive to achieve successful outcomes. It follows that satisfaction is possible as long as you work on your success every day.
In a study by Joo et. al. show that Korean nurses experience a poorer security climate compared to other countries. One suggestion is to increase the satisfaction of nurses through organizational communication and to promote communication at the organizational level so that individual healthcare professionals are aware of their organisation's vision and policy (19). Similar results were obtained in the broadcasts of Poursadeqiyan et al. and Borhani et al. (20, 21).
Work satisfaction (F1) is one of the factors influencing the working environment in research conducted among the professionals of an emergency department. Work satisfaction has been shown to be related, inter alia, with burnout, ethical sensivity and leadership (22, 23).
Considering Factor two, there is little research that focuses on Productivity and Achievement of aims. In their work, Bipp et al. see a positive relationship between progress in achieving goals and commitment to work, in particular in the case of employees who have achieved goals related to the approach to results that they have planned (24). Mahmoudi et al. showed in their work that when considering achievement motivation and self-efficacy in private and university hospitals, significant differences were observed (25). Setting goals is related to self-confidence, motivation and autonomy, which is mentioned in her work (26, 27). Respondents rated the aspect of Factor 2 the highest, which was responsible for saying that they work group is known for its productivity. The problem Productivity / Achievement of aims (F2) of nurse practitioner and resident physician appeared in the McDonnell study (28).
Factor three focused on Interpersonal relationships. In the work of Orehek et al. it has been shown that interpersonal relations and the pursuit of a goal are closely related (27). Lee et al. stresses that patient safety is threatened by medical errors and adverse events related to misunderstandings among healthcare providers. In addition, the authors note that different relationships between team members lead to different collaborative behaviors, which may impact patient safety outcomes by altering team communication (29). Note the conclusions of Fernandez et al. that effective teamwork is essential to ensure safe and effective healthcare (30). Well-functioning teams adapt to rapidly changing patient factors and the environment, preventing diagnostic and therapeutic errors (31). Interpersonal relationships (F3) are considered in the dimension of communication, teamwork, leadership and decisionmaker (32–34). Our research has shown that satisfaction with the cooperation in the worhplce was rated the highest of the entire Factor 3. In the studies of Eiche et al. Satisfaction with the work of paramedics in the German EMS is low. Dissatisfaction with payment and organizational issues is widespread. The performance mindset is high, but the fear of failure is common. Current and future efforts to create an attractive working environment should reflect these findings (35).
In Factor four, Performance at work was rated. Randhawa et al. in their work, they showed a significant positive relationship between self-effectiveness and work efficiency, which suggests that the higher the self-efficacy specific for a given job, the higher the work efficiency of employees will be (31). Aboagye et al. emphasized that during the pandemic, absenteeism was to a large extent related to work efficiency. In addition, factors that interfere with performance at work must be constantly corrected including working on several jobs, which has a destructive effect on the quality and efficiency of work (36). Performance at work (F4) was described, among others, by in the works of Staempfli et al. heavy workloads, exposure to violence and conflict, and patients with a high medical condition contribute to the difficult working environment for emergency department nurses around the world. Emergency services representatives around the world report low nurse satisfaction and high levels of burnout (37).
Robinson et al. in his research, he compared the effects of productivity, efficiency and overall performance differences between lone assistants and working with residents in the emergency room. Another study found that increased productivity with decreased productivity was reported among Attendants when working with residents. Taking into account aspects related to working with residents, greater effectiveness was observed in group work than in individual work. (38). In a study by Kang et al. In the United States, emergency departments are constantly under pressure to improve operational efficiency and quality in order to obtain financial benefit and maintain a positive reputation. Depending on the structural and operational characteristics of ED, various factors can affect the relationship between performance and quality (39). Karmi et al. showed in the study that the productivity and quality of professional life of emergency nurses were at a moderate and relatively normal level, respectively. The research shows that scientific advancement does not improve the quality of professional life. It is necessary to put in place a plan to improve the productivity and quality of working life of nurses. Such plans should be implemented at the hospital level at every hospital level. The role of creating an environment suitable for a high quality of life plays a key role in the emergency department. It is necessary to conduct more developed research in this environment. (40).
Through the COVID-19 pandemic, research has limitations in interacting with study participants. In addition, when assessing the pre-pandemic research, we can see the impact of the difficult period on the results of research in the EHS group. Considering the number of countries that took part in the survey and the number of people, this number is not very large, but the survey can be successfully repeated on a larger group of employees. The abridged scale is a new tool for assessing the work climate in emergency medical services. There are no studies with the use of the scale, except for the validation study, therefore in the discussion the authors referred to the research on the organizational climate conducted in professional groups with similar working conditions, mainly nurses.
In response to the purpose of the research, the work climate of EHS during COVID-19 Pandemic in 14 countries was assessed using the Abridged Version of the Work Climate Scale in Emergency Health Services. The study of the climate at work shows that countries have different priorities at work, but not all of them. By answering the research questions one by one, we can say that the average climate score at work was 33.41 (SD = 1.52) at the range 24–120. It has been concluded that the emergency services staff investigated here perceive the score of the organizational climate to be low, which is represented by the low score of factors like: work satisfaction, productivity / achievement of aims, interpersonal relationships, performance at work. This raises concerns about the working conditions of emergency services staff as a low perception of work climate indicates that these conditions may not be sufficiently satisfactory to provide them with an adequate work process. This may have an impact on the quality of the health services offered. For this reason, the study of the working climate is important not only for emergency medical services personnel, but also for managers. Work climate analysis allows to verify the quality of the work environment and to determine whether and to what extent the work climate should be improved. to ensure good working conditions and good quality care. Further studies are needed to identify and clarify the specific of work climate in the emergency medical services group.
The highest average level of work satisfaction (Factor 1) was demonstrated for workers from Canada and the lowest for workers from San Marino. For Factor 2, the highest average level was again recorded in Canada and the lowest for the residents of San Marino. In Factor 3, related to Interpersonal relationships, the highest average scores were given by employees from Netherland, while the lowest for interpersonal relationships was given by the residents of San Marino. Performance at work (Factor 4) was rated the highest by the residents of England, while the lowest was recorded by participants from Turkey.
The abbreviated version of the scale reduces the time needed to complete the study, but at the same time retains its value, as mentioned in their study by Lozano-Lozano et al. (1). It is very important to conduct research on the working climate, as it can help to improve and eliminate elements that have a destructive effect on employees. Nowadays it is hard to work with the burden of a pandemic, but at the same time it should be remembered that decision-makers have a very large impact on improving the climate and quality of work in their hospitals.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Conceptualization: JK-B and SK. Methodology: WM-D and SK. Software: AF and BO. Formal analysis: GW and SG. Resources: KV. Data curation: MR and VL. Writing—original draft preparation: EB and JK-B. Writing—review and editing: WM-D, SK, and JK-B. Visualization: GW, WM-D, and JK-B. Supervision: DR. Project administration: JK-B. All authors have read and agreed to the published version of the manuscript.
Author BO was employed by European Specialist Nurses Organization. Authors KV was employed by Advancing Nursing LLC and MR was employed by Critical Care Nurses Association of the Philippines, Inc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lozano-Lozano JA, Chacón-Moscoso S, Sanduvete-Chaves S, Holgado-Tello FP. Work climate scale in emergency services: abridged version. Int J Environ Res Public Health. (2021) 18:6495. doi: 10.3390/ijerph18126495
2. Pincheira FJD, Garcés MEC. Effects of organizational climate and psychosocial risks on happiness at work. Contad Adm. (2018) 63. doi: 10.22201/fca.24488410e.2018.1142
3. Hruska B, Barduhn MS. Dynamic psychosocial risk and protective factors associated with mental health in Emergency Medical Service (EMS) personnel. J Affect Disord. (2021) 282:9–17. doi: 10.1016/j.jad.2020.12.130
4. Miltona J, Chaboyer W, Åberg ND, Andersson AE, Oxelmark L. Safety attitudes and working climate after organizational change in a major emergency department in Sweden. Int Emerg Nurs. (2020) 53:100830. doi: 10.1016/j.ienj.2020.100830
5. El-Hage W, Hingray C, Lemogne C, Yrondi A, Brunault P, Bienvenu T, et al. Les professionnels de santé face à la pandémie de la maladie à coronavirus (COVID-19): quels risques pour leur santé mentale ? [Health professionals facing the coronavirus disease 2019 (COVID-19) pandemic: What are the mental health risks? Encephale. (2020) 46:73–80. doi: 10.1016/j.encep.04, 008.
6. Lasalvia A, Bodini L, Amaddeo F, Porru S, Carta A, Poli R, et al. The sustained psychological impact of the COVID-19 pandemic on health care workers one year after the outbreak—a repeated cross-sectional survey in a tertiary hospital of North-East Italy. Int J Environ Res Public Health. (2021) 18:13374. doi: 10.3390/ijerph182413374
7. Norkiene I, Jovarauskaite L, Kvedaraite M, Uppal E, Phull MK, Chander H, et al. ‘Should I Stay, or Should I Go?' Psychological Distress Predicts Career Change Ideation among Intensive Care Staff in Lithuania and the UK Amid COVID-19 Pandemic. Int J Environ Res Public Health. (2021) 18: 2660. doi: 10.3390/ijerph18052660
8. Nielsen KJ, Pedersen AH, Rasmussen K, Pape L, Mikkelsen KL. Work-related stressors and occurrence of adverse events in an ED. Am J Emerg Med. (2013) 31:504–8. doi: 10.1016/j.ajem.2012.10.002
9. Rasmussen K, Pedersen AHM, Pape L, Mikkelsen KL, Madsen MD, Nielsen KJ. Work environment influences adverse events in an emergency department. Dan Med J. (2014) 61:A4812
10. Johnston A, Greenslade L, Thom J, Carlstrom O, Wallis E, Crilly M, et al. Article: staff perception of the emergency department working environment: Integrative review of the literature. Emergency Med Australasia. (2016) 28:7–26. doi: 10.1111/1742-6723.12522
11. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. (2014) 12:1495–9. doi: 10.1016/j.ijsu.2014.07.013
12. Vatani J, Arami M, Khanikosarkhizi Z, Shahabi Rabori MA, Khandan M, Dehghan N, et al Safety climate and related factors in rehabilitation nurses of hospitals in Iran. Work. (2021) 68:189–96. doi: 10.3233/WOR-203368
13. Giorgi G, Lecca LI, Alessio F, Finstad GL, Bondanini G, Lulli LG, et al. COVID-19-related mental health effects in the workplace: a narrative review. Int J Environ Res Public Health. (2020) 17:7857. doi: 10.3390/ijerph17217857
14. Lu Y, Hu X, Huang X. Job satisfaction and associated factors among healthcare staff: a cross-sectional study in Guangdong Province, China. BMJ Open. (2016) 6:e011388. doi: 10.1136/bmjopen-2016-011388
15. Janicijevic I, Seke K, Djokovic A, Filipovic T. Healthcare workers satisfaction and patient satisfaction—where is the linkage? Hippokratia. (2013) 17:157–62.
16. Linn LS, Brook RH, Clark VA, Davies AR, Fink A, Kosecoff J, et al. Physician and patient satisfaction as factors related to the organization of internal medicine group practices. Med Care. (1985) 23:1171–8. doi: 10.1097/00005650-198510000-00006
18. Javanmardnejad S, Bandari R, Heravi-Karimooi M, Rejeh N, Nia HS, Montazeri A, et al. Happiness, quality of working life, and job satisfaction among nurses working in emergency departments in Iran. Health Qual Life Outcomes. (2021) 19:112. doi: 10.1186/s12955-021-01755-3
19. Yoo J, Chung SE, Oh J. Safety climate and organizational communication satisfaction among Korean Perianesthesia care unit nurses. J perianesthesia Nurs Off J Am Soc PeriAnesthesia Nurses. (2021) 36:24–9. doi: 10.1016/j.jopan.2020.04.009
20. Poursadeqiyan M, Arefi MF, Khaleghi S, Moghaddam AS, Mazloumi E, Raei M, et al. Investigation of the relationship between the safety climate and occupational fatigue among the nurses of educational hospitals in Zabol. J Educ Health Promot. (2020) 28:238. doi: 10.4103/jehp.jehp_309_20
21. Borhani F, Jalali T, Abbaszadeh A, Haghdoost A. Nurses' perception of ethical climate and organizational commitment. Nurs Ethics. (2014) 21:278–88. doi: 10.1177/0969733013493215
22. Sperling D. Ethical dilemmas, perceived risk, and motivation among nurses during the COVID-19 pandemic. Nurs Ethics. (2021) 28:9–22. doi: 10.1177/0969733020956376
23. Schluter J, Winch S, Holzhauser K, Henderson A. Nurses' moral sensitivity and hospital ethical climate: a literature review. Nurs Ethics. (2008) 15:304–21. doi: 10.1177/0969733007088357
24. Bipp T, Kleingeld A, Schelp L. Achievement goals and goal progress as drivers of work engagement. Psychol Rep. (2021) 124:2180–202. doi: 10.1177/0033294120959778
25. Mahmoudi G, Rostami FH, Mahmoudjanlo S, Jahani MA. Relationship of Employees' achievement motivation and quality of working life with their self-efficacy at selected hospitals with a multi-group analysis: moderating role of organizational ownership. Mater Sociomed. (2017) 29:237–41. doi: 10.5455/msm.2017.29.237-241
26. Kleingeld A, van Mierlo H, Arends L. The effect of goal setting on group performance: a meta-analysis. J Appl Psychol. (2011) 96:1289–304. doi: 10.1037/a0024315
27. Orehek E, Forest AL, Barbaro NA. People-as-Means approach to interpersonal relationships. Perspectives on Psychol Sci. (2018) 13:373–89. doi: 10.1177/1745691617744522
28. Zhang N, Gong ZX, Xu Z, Gilal FG. Ethical climate and service behaviours in nurses: The moderating role of employment type,” J Adv Nurs. (2019) 75:1868–76. doi: 10.1111/jan.13961
29. Lee CT, Doran DM. The role of interpersonal relations in healthcare team communication and patient safety: a proposed model of interpersonal process in teamwork. Can J Nurs Res. (2017) 49:75–93. doi: 10.1177/0844562117699349
30. Fernandez R, Grand JA. Leveraging social science-healthcare collaborations to improve teamwork and patient safety. Curr Probl Pediatr Adolesc Health Care. (2015) 45:370–7. doi: 10.1016/j.cppeds.2015.10.005
31. Randhawa G. Work performance and its correlates: an empirical study. J Bus Perspect. (2007) 11:47–55. doi: 10.1177/097226290701100104
32. Lozano JAF, Moscoso SC, Sanduvete-Chaves S, Gil JAP. Main components of organizational climate in an emergency medical service: a qualitative approach. Acción Psicológica. (2013) 10:101–114. doi: 10.5944/ap.10.2.12213
33. Fontova-Almató A, Suñer-Soler R, Salleras-Duran L, Bertran-Noguer C, Congost-Devesa L, Ferrer-Padrosa M, et al. Evolution of job satisfaction and burnout levels of emergency department professionals during a period of economic recession. Int J Environ Res Public Health. (2020) 2:17:921. doi: 10.3390/ijerph17030921
34. Palazoglu CA, Koç Z. Ethical sensitivity, burnout, and job satisfaction in emergency nurses. Nurs Ethics. (2019) 26:809–22. doi: 10.1177/0969733017720846
35. Eiche T, Birkholz F, Konrad T, Golditz J, Keunecke G, Prottengeier J, et al. Job satisfaction and performance orientation of paramedics in German Emergency Medical Services-A Nationwide Survey. Int J Environ Res Public Health. (2021) 18:12459. doi: 10.3390/ijerph182312459
36. Aboagye E, Björklund C, Gustafsson K, Hagberg J, Aronsson G, Marklund S, et al. Exhaustion and impaired work performance in the workplace. J Occupational Environ Med. (2019) 61:e438–44. doi: 10.1097/JOM.0000000000001701
37. Staempfli S, Lamarche K, Perry B. Emergency nursing job satisfaction: Challenges and solutions. Nurs Manage. (2021) 52:14–24. doi: 10.1097/01.NUMA.0000733616.16359.d9
38. Robinson RD, Dib S, Mclarty D, Shaikh S, Cheeti R, Zhou Y, et al. Productivity, efficiency, and overall performance comparisons between attendings working solo versus attendings working with residents staffing models in an emergency department: a large-scale retrospective observational study. PLoS ONE. (2020) 15:e0228719. doi: 10.1371/journal.pone.0228719
39. Kang H, Bastian ND, Riordan JP. Evaluating the relationship between productivity and quality in emergency departments. J Healthc Eng. (2017) 2017:9626918. doi: 10.3113/JSOA.2017.0040
Keywords: work climate, emergency health services, COVID-19, multicenter, pandemic (COVID-19)
Citation: Kosydar-Bochenek J, Krupa S, Religa D, Friganovic A, Oomen B, Williams G, Vollman KM, Rogado MIC, Goldsworthy S, Lopez V, Brioni E and Medrzycka-Dabrowska W (2022) Work climate in emergency health services during COVID-19 pandemic—An international multicenter study. Front. Public Health 10:895506. doi: 10.3389/fpubh.2022.895506
Received: 13 March 2022; Accepted: 16 August 2022;
Published: 21 September 2022.
Edited by:
Luca Simione, National Research Council (CNR), ItalyReviewed by:
Katalin Papp, University of Debrecen, HungaryCopyright © 2022 Kosydar-Bochenek, Krupa, Religa, Friganovic, Oomen, Williams, Vollman, Rogado, Goldsworthy, Lopez, Brioni and Medrzycka-Dabrowska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wioletta Medrzycka-Dabrowska, d2lvbGV0dGEubWVkcnp5Y2thQGd1bWVkLmVkdS5wbA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.