
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health , 26 July 2022
Sec. Public Health and Nutrition
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.893831
 Julius Nsawir Bonglaisin1*
Julius Nsawir Bonglaisin1* Noella Bajia Kunsoan2,3
Noella Bajia Kunsoan2,3 Patrice Bonny1
Patrice Bonny1 Chelea Matchawe1Bridget Ndakoh Tata1Gerard Nkeunen4Carl Moses Mbofung5
Chelea Matchawe1Bridget Ndakoh Tata1Gerard Nkeunen4Carl Moses Mbofung5Geophagy is the habit of consuming clay soil such as chalk or kaolin. Though it is globally practiced, the safety of those involved is yet to be fully established. It is thought to be highly prevalent in pregnant women because of its antinausea or therapeutic effects. This practice is also thought to be provoked by some nutritional needs, but in modern society its etiology is obscure. The mineralogical and chemical compositions of clay may vary from one region to another and even in all form of rocks clay constitutes. Published articles in geophagy indicate lack of adequate investigations into the toxicity of geophagy, though it is globally practiced and more prevalent in Africa (as a continent) or in Africans migrants. Some studies have helped to identify some minerals that are toxic to human if ingested. In most cases, the potential toxicity emphasized by these studies is based on the detection of the presence of these nuisance elements in the geophagic materials. Scientifically, a lot has been done in the light of detection of toxic matter, but more investigations on metabolic studies are still necessary. The variability of clay content with respect to source motivated this review on geophagy and its potential toxicity to human. This review is aimed at bringing out findings that would enable a better understanding of the toxicity potential of geophagy across context and taxa.
Geophagy or geophagia is the habit of consuming clay such as chalk or kaolin. Commonly referred to as Calabar chalk, ndom, nzu or Calabar stones by some ethnic groups in Nigeria or as mabele by the Lingala people of Congo or by Francophones as craie, poto or argile (1, 2) or Calabar chalk in Cameroon, kaolin consumption varies in intensity from one region to the other. It is more common in children than in adults (3, 4); in women than in men (5, 6); in black race than in white race (5, 7); in rural areas than in urban areas (5, 8, 9); and in pregnant women than normal women (7, 10–12).
In earth science, kaolin is used broadly to cover a range of clay-compounds predominately made up of Kaolinite that is associated with many other minerals that are the products of felspathic rock alteration (13, 14). The Kaolinite and minerals of kaolin vary from sample to sample. Its color varies from white, green, pink, gray, yellow to red with respect to chemical composition. Kaolin is clay material, made of hydrated silicates and known to be stable within natural conditions and its chemical composition, at pure state, is as on Table 1.
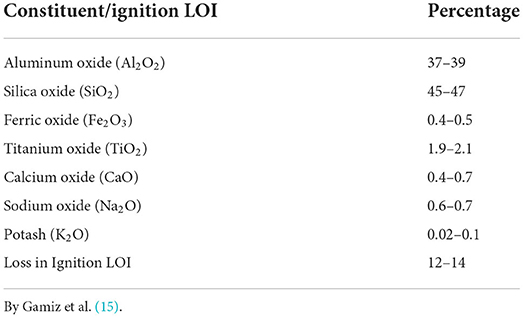
Table 1. Chemical composition of pure kaolin.
It may be contaminated with toxic metals such as lead (Pb), nickel (Ni), cobalt (Co), Cadmium (Cd), chromium (Cr), copper (Cu), Mercury (Hg) Mercury (Hg), zinc (Zn), etc. (13, 16–19).
Kaolin is one of the most abundant clay compound that is also extremely exploited in the world industrially (14). It is highly mined in several countries such as Brazil, Germany, India, China, Bulgaria, Korea, Czech Republic, Australia, South Africa, France, United States of America, Iran and United Kingdom. Kaolin is common in tropical soils especially in soils that are products of chemical weathering of rocks in hot and typically humid climate such as tropical rainforest areas (14).
In Cameroon, kaolin deposits were discovered by Njonfang (20) and Njoya (21) in the following regions: Centre (Etoa, Mvan, Nanga Eboko, etc.); Littoral (Dibamba, Makepe, Mbanga, Dizangué; Douala sedimentary basin, etc.); North West (Bambili, Bali, Mankon, Santa, etc.); South west (Mamfe, Mukunda, Ediki, etc.); West (Mayouom, Balengou, Bana, Lembo, etc.) and in the Northern area of the country (Moufou, Dekounou, Mbe and Gamboukou, Zilling, Doubled, etc.) (20, 21).
Kaolin can be used as filler in the manufacture or production of several goods according to its intrinsic chemical characteristic and the extent to which it is processed. The highest use of this clay is for paper production, especially in ensuring the gloss in paper grades. Kaolin is also used to make toothpaste, ceramics, cosmetics, white bulbs, paints and to reinforce properties of rubber and in adhesives (22, 23). As well, it is used in smoking pipes production in Asia and Europe, in organic farming and applied as spray to crops to prevent damage from insects or sun scald. It is also used like whitewash in traditional stone masonry homes in Nepal, in radiological dating since it contains traces of uranium and thorium and for making of fiber glass, refractories, plastic, mineral wool, etc. (14); for facial masks or soap and to soothe stomach gastritis (24) or for treatment of diarrhea. It is also used for the production of baked bricks and pottery artifacts like in the Bamenda area of Cameroon. The sources and number of published data related to geophagy used in this review are presented on Table 2.
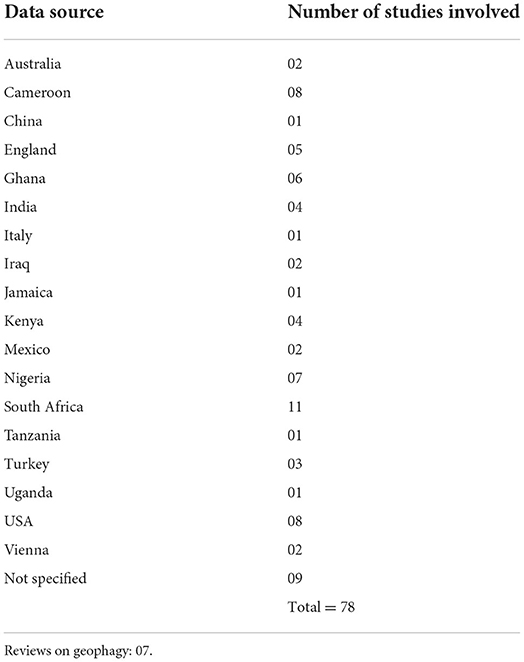
Table 2. Source and number of published data related to geophagy.
Kaolin-eating is common in the rural South of the United States, parts of Latin America, Asia and the Middle East (9, 25, 26). It is also common in Sub-Saharan Africa where several cultures especially farmers and nomad settings consume dirt, mainly clay (5, 27, 28) and in Australia during food scarcity (29). In most cases the habit is common amongst pregnant women. Many experts have suggested that geophagy is highly prevalent in pregnant women, who are either Africans or migrants from this continent, because of its antinausea effects (30–32). Other studies have confirmed this finding through more investigation in women (33, 34). The Medical University of Vienna (35) found that 30–80% of Africans, especially women, eat clayey soil on a regular basis consuming between 100 and 400 g per day. Specifically, 30–50% of women in pregnancy (in hundreds of millions) in many African and rural blacks of South American communities practice clay-eating (33, 34, 36).
In modern societies, geophagy represents eating habit with hidden reasons. Some statements have been raised as reasons for geophagical behavior. Some of these include: (1) clay includes additional micro/macro nutrients that may be absent in the consumer's day to day diet. With this reason, clay would be beneficial to the body if consumed. Such is the case with pregnant women who require 20% more nutrients (37); (2) kaolin or clay has the capacity to detoxify secondary compounds that are often found in foods. Thus clay would be like medicine alleviating some pathologies (38); (3) kaolin or clay prevents the stomach and intestines from harmful biochemical substances and thus ensures resistance to gut disease. Clay is said to have covering role in gastro-enterology (39). These statements are confirmed by studies in some communities, indicating that geophagy could be associated with some positive biochemical effects. Danford (40) tried to describe summarily the four hypotheses most commonly discussed as reasons for clay (kaolin) or soil consumption. These include: nutritional, psychological, cultural and medical or therapeutic. For instance, diarrhea and intestinal parasites have been observed to be treated by ingesting clay or soils (36). Dietary treatment that has been observed to stop the habit of geophagy strongly support the viewpoint point that the practice is prompted by nutritional deficiency (41). However, most of these reports are from specific contexts where studies were carried out and as such cannot be generalized. Thus a generic or global approach without comprehensive data from the various contexts will not be adequate. It would be more appropriate to recommend contexts with comprehensive data, identified as posing no threats for geophagic material. This view point is approved by authors (42, 43) with the standpoint that geophagic material should be accepted as such based on its provenance. Some soils have been identified as posing no threats with respect to heavy metal loads (44).
Globally, authors have tended to conclude on toxicity based on the content of geophagic materials, such as the presence of heavy metals, instead carrying further scientific investigation for adequate scientific evidence as seen on Figure 1. This is a gap that needs to be addressed for proper apprehension of toxicity in future research on geophagy.
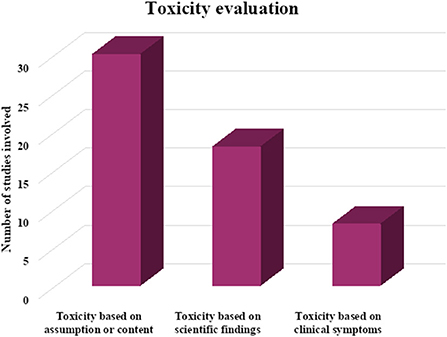
Figure 1. The bases of toxicity of geophagic material in reviewed papers.
Concerning its management or treatment, Jackson et al. (45) suggest that emphasis should be made on both physiological and psychological aspects of the individual. If geophagy emanates from a physiological health condition or mineral deficiency, a thorough examination of the individual's medical history will reveal potential issues and deficiencies that will be tackled in the treatment process. On the psychological aspect, they recommend an examination of the individual's social history for psychological diagnosis and treatment which is only secondary to the physiological treatment process but essential be considered. Waswa and Imungi (27, 46) carried out a randomized control trial amongst boarding secondary school students in Western Kenya. They used traditional food substitute as a soil replacer within the student community. These were alternatives that help impede the practice of geophagy. Therefore, developing a soil replacer within geophagic communities can be a good management for geophagy. In most cases, geophagy goes unnoticed by various health providers because those who practiced it are reluctant to give information on the habit. Indeed, many have been stigmatized and they tend to conceal their eating habit, making management difficult (47).
Though some elements in kaolin within certain thresholds can benefit the body nutritionally for functioning and development (48), some are not essential and might be harmful or toxic instead. The latter are causes of most health challenges encountered during geophagy (49, 50). Those that are important might still be chelated and unavailable nutritionally. Minnich et al. (51) have come up with the hypothesis that kaolin consumption may keep pregnant women from getting enough calories or the right nutrients during pregnancy. The hypothesis is confirmed for some minerals by many scientists. For instance, the role kaolin (clay) plays in iron absorption and assimilation is significantly displayed in studies carried out by some authors (52, 53). They worked with four different types of clay and discovered that Fe ions permeate exchangeably with Ca, Mg, Mn, Na, K and hydrogen ions, leading to the formation of non-absorbable iron compounds. This means that kaolin may sap the body of iron and create anemia. In addition, Dreyer et al. (6) discovered that iron was liberated at pH 2.0 (stomach pH) and absorbed at pH 6.2 (intestinal pH). Hooda et al. (54) used in vitro geophagia simulations in five large samples of soils eaten by the communities of Tanzania, Uganda, India and Turkey (54). Both readily available macro (Mg and Ca) and micro (Cu, Fe, Zn and Mn) nutrients necessary for uptake by the gut and the wellbeing of the body constituted these simulation solutions. They found out that Mg, Mn and Ca found in the simulations were released from the soils with no specific order or logic and other simulations with similar soils were not releasing their Mg, Mn and Ca, but instead absorbed them. The absorption of these metals by the clay involved was observed to increase with increased pH. Similar results were obtained by Alloway (55).
Results from many context and taxa reveal that the habit of geophagy can potentially tamper with iron levels in the body in two ways: (i) the Fe content of the geophagic material might make a significant improvement to Fe intake as such alleviating iron deficiency (48) and (ii) The composition of the geophagic material might hinder through chelation non-haem Fe in the gut by forming complexes that cannot be dissolved, influencing negatively Fe absorption as a whole (56–59) and thus affecting iron metabolism. The former point has made researchers to insinuate that lack of Fe in the body provokes geophagia (60) to meet iron (Fe) requirement.
However, Kambunga et al. (61) in their “review of the nature of some geophagic materials and their potential health effects on pregnant women,” concluded that the negative effects of geophagy in pregnant women far outweigh the health benefits. They also noted that the perceived health effects of geophagy in pregnant women are rather based on mere assumptions than scientific experimental data.
Physiologically, many nutritionists and researchers have viewed geophagy as amongst practices that help provide physical relief from painfulness or distress. In gastro-enterology, clay (kaolin) is suspected to sap toxins from food or bacteria that are related to stomach upset (33, 34, 38, 41, 62). Some kaolin constituents such as benzoic groups, aluminum oxide and magnesium oxide, have attributed antacid characteristics to kaolin, such that it can mitigate pains resulting from gastritis. Furthermore, an author has also observed that kaolin has “covering properties,” and plays a bandaging role in gastro-enterology (39).
Kaolin has been observed to coat the gastro-intestinal tract, preventing it from biological and chemical attacks. It is also potentially therapeutic to esophagitis, colitis and diarrhea (31, 36, 62).
Studies involving some chimpanzees consuming clay-like soil have been observed prior to or after eating some plants possessing anti-malaria properties. Studies that simulated mastication and digestion observed that clay facilitates the release of active anti-malarial components from the leaves of these plants. These soils are also therapeutic toward diarrhea and have been exploited locally for diarrhea treatment (63). According to Tayie et al. (64) some of the motivating and useful reasons for kaolin consumption include their efficiency to alleviate diarrhea, stomach upset or mitigation of nausea and toxemia of pregnancy.
Authors have reported risks involved in eating earth contaminated with animal or human wastes or even eggs of parasites like in the case of worms, that can remain inactive in the soil for years or even radioactive matter (27, 46, 65). Clostridium tetani cells are common in such soils and can pose a further risk. In this light, there is greater susceptibility in children getting infected by bacteria or worms because of their predisposition to soil-eating (66). Authors have also reported that geophagia can bring about teeth damage, the ingestion of contaminated soil, and blockage of human intestines. Studies in Kenya (4) have confirmed these results, with children being the most exposed to geohelminths and trichuriasis (27, 46). Also, incidences of death have been known to occur after the excessive consumption of some clay often due to intestinal occlusion or perforation (5, 22).
A more common problem reported across continents such as Portugal in South America, Iran in the Middle East, Turkey in Eastern Europe, Egypt in North Africa, known as geophagic disease or syndrome observed over 30 years amongst clay consumers was anemia and zinc deficiencies, delayed growth, enlargement of the spleen and liver and retarded sexual maturity (40, 52, 53). Authors have raised the hypotheses that geophagy causes iron deficiency and is also a consequence of lack of iron in the body system (40, 67). The latter hypothesis has been scientifically confirmed (68, 69).
Though apparently there are beneficial effects of kaolin consumption presented by many studies, other studies show that this practice does equally tend to expose consumers to metal contaminants and toxicity (2, 70, 71). Amongst these are heavy metals that are permanent and at the same time most problematic. They distinguished themselves from the other contaminants because of their non-degradability and low migration ability in soils. According to their toxicity they could be divided as follow: strongly toxic: mercury (Hg), uranium (U), indium (In), cadmium (Cd), copper (Cu), thallium (Tl), arsenic (As), vanadium(V), zinc (Zn), nickel (Ni), bismuth (Bi); moderately toxic: manganese (Mn), chromium (Cr), palladium (Pd), lead (Pb), Osmium (Os), tin (Sn), cobalt (Co), molybdenum (Mo), antimony (Sb); and slightly toxic: iron (Fe), germanium (Ge). Some metalloids such as selenium (Se) and antimony (Sb), are also examined as heavy metals. Some of these heavy metals are biologically necessary (Fe, Cu, Zn, Se), while others are not (72), because they have no physiological role. Geochemical studies reveal that some of them exist only as traces (Cd, Tl, Hg etc.), but the others exist in high concentrations such as iron (Fe), manganese (Mn) etc (72).
The scenario of clay contamination by heavy metals has been described by several scientists. Clay (kaolin) often develop negative charges within its layers especially in humid and hot environment and consequently attracts positively charged particles. Contamination is the outcome if these positive charges are toxic to humans, like heavy metals (15, 73). Lead would be a good example of a heavy metal that is attracted by such layers of kaolin, consistently reported by many studies (13, 19). Lead occurs naturally in ground waters, surface waters and soils. Studies have shown lead content of agricultural soils varying from 1 to 135 mg/kg and a median value of 11 mg/kg reported (74). Being a water soluble element, it is obvious lead would be leached or washed by rain water into kaolin mines especially those mines that are along or within streams and rivers. A similar scenario would occur when cultivated farm fields are on a slope above kaolin mining sites. In such farms bioavailability and bioaccessibility of heavy metals to crops should be recommended (44, 75). Contamination with lead would be exceedingly high if the stream or river gaining access to the kaolin mines has initially traversed a city or industry (76, 77). Studies have revealed high Pb concentrations in excess of 1,000 mg/kg in soils within most major cities like Lagoes, Douala etc (78–82). Chaney et al. (83) have reported Pb values as high as 50,000 mg/kg within a city. Mostly, these elevated Pb values found in city soils are suspected to come from industrial wastes, vehicles and the various Pb paints (84). The urban environment has thus become a potentially harmful lead (Pb) source. Lead is among the striking environmental harmful chemicals and is becoming preponderant (85). Other sources of lead (Pb) include Pb arsenate found in insecticide, impurities in different forms of fertilizers and metal extracting activities (86).
Previously, research findings on the practice of geophagia in Africa showed mostly the prevalence of the practice and the reasons for it with little or no information on the toxicological implications. Secondly, there has been lack of consensus globally in published literature on the effects of consumption of kaolin on blood heavy metals levels. While studies by Simpson et al. (7) and Thihalolipavan et al. (87) reported that geophagy leads to high Pb blood levels in female consumers, other studies by Knezevich and Tadic (88), Hassen et al. (89), and by Katsumata et al. (90) portray a contrary view. They reported that kaolin consumption tends to be a detoxifier of heavy metals and poisons. Authors confirmed clay ability to adsorb toxins especially when associated with charcoals (91). This apparent lack of consensus on the effect of consumption of contaminated kaolin compels further need for research. This inconsistency inspired Bonglaisin and collaborators to investigate further on the most contaminant heavy metals (Pb, Cd and Hg). In 2011 and 2015, research activities carried out by these authors showed that Clay (kaolin) at the local sale points contained high values of lead (Pb), cadmium (Cd) and Mercury, and is also highly consumed in Cameroon (13, 19). Further research carried by one of the authors on pregnant rats showed that Pb in this clay can gain access in the bloodstream and as such clay (kaolin) is potentially harmful. Cadmium (Cd) and Hg were observed to bio-accumulate in the liver (92). Similarly, serum levels of Pb and varying concentrations of other heavy metals have been found (93, 94), confirming that toxic heavy metals can be absorbed during toxic clay consumption. Ekosse et al. (43) inferred limited health threats in a study in which they observed low bioavailability of heavy metals in gastrointestinal tract simulation. By implication toxicity effects due to Pb would be common in geophagic communities where these studies were carried out. Lead (Pb) is known to be toxic to some organs like the kidney, liver, nerves, gastrointestinal tract, thyroid gland, brain etc. of human or animal systems that ingested it (95–98). Many studies on Pb contamination of kaolin have been reported in Nigeria (1), Ghana (49, 50), South Africa (43), though Pb content or heavy metal potential toxicity of several clay types have not been investigated in other context and taxa (99).
Iron (Fe) and Pb attached themselves on similar position in many biomolecules and so will compete for the same target or binding sites in the human body (100). Though Pb primarily manifests its toxicity in the human body because of its ability to mimic elemental calcium (Ca), it is also known to tamper with Fe absorption and assimilation in mechanism that are yet to be fully known (100, 101). The dislocation of iron (Fe) by zinc (Zn) in oxygen carrying molecule of the human body (hemoglobin), to form Zn protoporphyrin (100), is an initial effect common with Pb intoxication (101). The consequence is reduced oxygen circulation since elemental Fe bears the burden of carrying in the oxyhaemoglobin molecule (102), with outcome being hypochromic anemia. Lead (Pb) is also known to affect negatively erythropoiesis blocking the maturation of red blood cells (100, 101), influencing their size (microcytic anemia) (103) and their longevity (103). In anemia situation, it would block the hormonal response that targets the normal increase of erythopoiesis (100). Studies on geophagic materials have confirmed these findings (68, 69), indicating that toxic clay has the potential to affect hemoglobin level.
Iodine and lead (Pb) manifest a similar scenario. There is a hormonal mechanism controlling the release of thyroid hormones from the thyroid gland. Thyrotropin that is released from the hypothalamus acts on the pituitary gland to release thyroid-stimulating hormone (TSH). The latter (TSH) as its name implies stimulate the thyroid gland to produce thyroxine (T4). This hormone (T4) regulates TSH output through negative feedback mechanism. When the blood level of T4 drops by its conversion to triiodothyronine (T3) favored by the enzymes deiodinases (104), the release of pituitary TSH is triggered, with outcome being increased thyroid volume (thyroid hyperplasia). Increased T4 brings about the inhibition of TSH and thyrotropin production. The situation that occurs when sufficient iodide is available in the thyroid gland (102). In iodine deficiency, the level of T4 remains low while that of TSH remains high (105).
Environmental chemicals have been observed to alter thyroid hormone levels through mechanisms that are well understood such as interruption of iodine transport, disruption of deiodinases etc. (106). Although authors have primarily focused on chemicals that are structurally similar to T4 like bisphenol, appreciable attention has also been given to heavy metals such as Pb, Hg and Cd. An association between these toxicants with respect to the total and free T4, total and free T3, or TSH have been studied (107–112), asserting the negative effects of these metals on the thyroid. Depending on the mechanism that is being disrupted its proper functioning is often affected causing it to hypertrophy even at normal iodine intake as illustrated on Figure 2.

Figure 2. Goiter illustration by the Centre for Disease Control (CDC), USA.
Lead (Pb) for example is known to have negative effects on blood formation (113, 114). Studies on communities with high lead (Pb) exposure have observed its adverse effects associated with free T4, or T3 (112, 115–117), though there have been inconsistencies as some studies on human revealed no adverse effects on thyroid hormones (118–121).
In sheep, a low dose of lead (Pb) exposure for a long time has confirms Pb effects on thyroid function especially in hypothyroidism (122). A similar study reports increase risk of thyroid damage in wistars albino rats exposed to Pb and Cd (123), with thyroid hypertrophy observed (69) as seen in Figure 2.
Though the crystalline structure of kaolin is held together by hydrogen bonding and Wan der waals forces (124), lead (Pb) type in kaolin determines its bioavailability in the human system. In kaolin all evidence points on ionic form that is held by electrostatics forces (as previously mentioned), and readily available for absorption (15, 73). Generally, the main route of entry for lead (Pb) into the body is through the gastrointestinal track (96). The latter for example occurs when Pb contaminated clay (kaolin) is consumed. An author studied the implications of consuming such clay in albino rats revealing high concentrations of this metal in the liver and the blood as evidence of its intoxication (92).
In humans, absorption of Pb after ingestion is through the same pathway (gastrointestinal). Its absorption varies with the current physiology of the exposure subject, such as Fe status, available Ca, fasting or age. Lead (Pb) absorption also varies with properties such as solubility, mineralogy particle size etc of the lead ingested (125). A rat study using to Pb acetate (100%) as reference, showed the following absorption: 164% for Pb carbonate; 121% for Pb thallate; 62-67% for Pb sulfide, Pb naphthenate, and Pb octoate; 44% Pb chromate and 14% metallic Pb (126).
Lead (Pb) is known to bind to plasma or red blood cells proteins when it reaches the bloodstream. Only a bit of it is transported in the form of free ions. It is then from blood tissue that it is carried to other tissues and it concentrations in these tissues depend on their vascularization and metabolism (127). Human beings do not have any mechanisms specific to Pb management. Lead (Pb) is distributed into human system, because its ionic characteristics more often than not coincide with metal ions that are essential to man's system. The common pole of metals that are distributed into the human system in a similar manner like Pb include cadmium (Cd), mercury(Hg) and aluminum (Al). The toxicity of these metals is based on a partial ionic-molecular mimicry to other ions essential to human. The toxic mechanism of Pb has been confirmed by authors, who reported that Pb2+ has the ability to substitute, at the molecular level for other polyvalent cations like Ca2+ and Zn2+ (128). The transport mechanisms for these metals necessary for human system is used by Pb for penetration into the system (129, 130). It has been observed that the Ca2+ binding sites used by Pb have specific characteristics. For instance, they are wide and evenly charged (131, 132). Many of the zinc-binding sites that are occupied by Pb are formed by sulfur or nitrogen atoms with low coordination numbers (131).
Garza et al. explained that these mimicry interactions of Pb make it interfere with many significant biological processes such as protein maturation, metal transport, ionic conduction, intracellular signaling etc (128). These authors also observed that signaling molecular structures and transport through the membrane are the most affected with Pb neurotoxicity being the outcome. The brain or central nervous system undergo alterations. This is why a prolonged exposure to Pb can end up affecting behavior and walking abilities. The mechanisms by which this happens are complex, but are said to include alterations in the synthesis of neurotransmitters with an eventual damage to neural cells such as astroglia and oligodendrocyte (133). The part of the brain that is responsible for memory and learning in human is mostly the one that manifest greater damage in prolonged Pb exposure (125).
This Pb ability to penetrate human system by substituting for Ca, Zn, and other cations having its ionic form causes Pb to affect the entire environment of the cell, damaging it. It has been proven that these effects result from complex processes engendered by Pb presence in the cell such as genetic regulation, protein synthesis etc or by Pb direct interaction with cell constituents. This scenario, for example, has been observed with some cellular matrix proteoglycans (134, 135) or cell adhesion mediated signals structures that are very important for cell survival but are affected by Pb during their synthesis or maturation (136, 137). Heme-group synthesis has also been observed to be adversely affected by prolonged Pb exposure because of the inhibition of aminolevulinic acid dehydratase (ALAD) a Zn containing enzyme (133). A similar situation occurs when Pb promotes the permeability of the mitochondrial causing the release into the cytoplasm of redox-active proteins such as cytochrome C with cell death as consequence (138).
Lead (Pb), Cd, Hg and Zn are specifically attracted by thiol groups in proteins (139, 140). Prolonged Pb exposure has shown that there is greater affinity for Pb to some proteins molecules more than some essential cations. For instance, ALAD has a greater affinity for Pb than for Zn (usually 2–4) (141–143).
Considering the outcome of this review, there is need for clay or soil characterization and beneficiation for healthy geophagic practices across ecological context and taxa in order to pronounce on their potential toxicity or benefits. Knowledge of the geochemistry of clays might not be sufficient to aid infer the likely adverse health effects as there is need for bioavailability studies of the elements in the various clay types in various contexts to assess the effect of ingestion of the geophagic materials on the geophagic individuals. Conflicting viewpoints regarding the beneficial and consequences of geophagy are still persisting.
Clinical control trials are globally persisting as a gap. We strongly recommend clinical control trials on the potential toxicity of kaolin in order to address the conflicting view points and facilitate good policies.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.893831/full#supplementary-material
1. Ijeoma KH, Onyoche OE, Uju OV, Chukwuene IF. Assessment of heavy metals in edible clays sold in Onitsha Metropolis of Anambra State, Nigeria. British J Appl Sci Tech. (2014) 4:2114–24. doi: 10.9734/BJAST/2014/7946
2. Campbell H. Calabash Chalk (calabar stone, la craie, argile, nzu, mabele). Belfast: Department of Health, Social Service and Public Safety (2002).
3. Saathoff E, Olsen A, Kvalsvig JD, Geissler PW. Geophagy and its association with geohelminth infection in rural schoolchildren from northern KwaZulu-Natal, South Africa. Trans R Soc Trop Med Hyg. (2002) 96:485–90. doi: 10.1016/S0035-9203(02)90413-X
4. Geissler PW, Mwaniki DL. Thiong'o F, Michaelsen, KF, Friis H. Geophagy, iron status and anaemia among primary school children in Western Kenya. Trop Med Int Health. (1998) 3:529–34. doi: 10.1046/j.1365-3156.1998.00272.x
5. Mashao U, Ekosse G, Odiyo J, Bukalo N. Geophagic practice in Mashau Village, Limpopo Province, South Africa. Heliyon. (2021) 7:e06497. doi: 10.1016/j.heliyon.2021.e06497
6. Dreyer MJ, Chaushev PG, Gledhill RF. Biochemical investigation in geophagia. J Soc Med. (2004) 97:48. doi: 10.1177/014107680409700125
7. Simpson E, Mull JD, Longley E, East J. Pica during pregnancy in low-income women born in Mexico. West J Med. (2000) 173:20–4. doi: 10.1136/ewjm.173.1.20
8. George G, Ndip E. Prevalence of Geophagia and its possible implications to health-a study in rural South Africa. In: 2nd International on Environmental Science and Development. IACSIT Press, Singapore (2011).
9. Ekosse GE, de Jager L, Ngole V. Traditional mining and mineralogy of geophagic clay from limpopo and free state provinces, South Africa. African J Biotech. (2010) 9:8058–67. doi: 10.5897/AJB10.296
10. Prince RJ, Luoba AI, Adhiambo P, NgUono J, Geissler PW. Geophagy is common among Luo woman in western Kenya. Trans R Soc Trop Med Hyg. (1999) 93:515–6. doi: 10.1016/S0035-9203(99)90355-3
11. Sapunar J, Fardella P. Visceral larval migrans (Human toxocariasis) cause of hypereosinophilia and visceral granulomas. Boletin Chileno Parasitol. (1999) 54:21–4.
12. Patterson EC, Staszak DJ. Effects of geophagia (kaolin ingestion) on the maternal blood and embryonic development in the pregnant rat. J Nutr. (1977) 107:2020–5. doi: 10.1093/jn/107.11.2020
13. Bonglaisin JN, Mbofung CM, Lantum DN. Intake of lead, cadmium and mercury in kaolin-eating: a quality assessment. J Med Sci. (2011) 11:267–73. doi: 10.3923/jms.2011.267.273
14. DME (Department of Minerals and Energy). South Africa's Mineral Industry 2004/2005. DME (2005). p. 148–54.
15. Gamiz E, Caballero E, Delgado RM, Delgado CFR. Characterization of Spanish kaolin for pharmaceutical use. Chemical and mineralogical composition physico-chemical properties. J PubMed. (1988) 127:114–21.
16. Abbas RA, Sarah IN. Potential source of heavy metals in the geophagic clay (Marl) and its implication on human health in NE Iraq: a pilot study. Iraqi Geol J. (2021) 2021:80–7. doi: 10.46717/igj.54.2C.8Ms-2021-09-27
17. Kortei NK, Koryo-Dabrah A, Akonor PT, Manaphraim NYB, Ayim-Akonor M, Boadi NO, et al. Potential health risk assessment of toxic metals Contamination in clay eaten as pica (geophagia) among pregnant women of Ho in the Volta Region of Ghana. BMC Preg Childbirth. (2020) 20:160. doi: 10.1186/s12884-020-02857-4
18. Fosso-Kankeu E, Netshitanini TL, Abia ALK, Ubomba-Jaswa E, Waanders FB. Application of solar treatment for the disinfection of geophagic clays from markets and mining sites. Afr J Biotechnol. (2015) 14:3313–24. doi: 10.5897/AJB2015.14971
19. Bonglaisin JN, Mbofung CM, Lantum DN. Geophagy and heavy metals (Pb, Cd and Hg) content of local kaolin varieties in the cameroon market: assessment indices for contamination and risk of consumption or toxicity to the population. J Med Sci. (2015) 15:1–9. doi: 10.3923/jms.2015.1.9
20. Njonfang E. Contribution à l'étude de la relation entre la Ligne du Cameroun et la Direction de l'Adamaoua. 1 Pétrologie, géochimie et structure des granitoïdes panafricains de la zone de cisaillement de Foumban-Bankim (Ouest-Cameroun et Adamaoua) 2 Pétrologie et géochimie des formations magmatiques tertiaires associées (Doctoral dissertation, Thèse Doct Etat) Univ Yaoundé I, Cameroun (1998).
21. Njoya A, Nkoumbou C, Grosbois C, Njopwouo D, Njoya D, Courtin-Nomade A, et al. Genesis of Mayouom kaolin deposit (western Cameroon). Appl Clay Sci. (2006) 32:125–40. doi: 10.1016/j.clay.2005.11.005
22. Njopwouo D. Minéralogie et physico-chimie des argiles de Bamkoul et de Balengou (Cameroun). Utilisation dans la polymérisation du système et dans le renforcement du caoutchouc naturel. Thèse d'Etat, Univ de Yaoundé (1984).
23. Ciullo PA. Industrial Minerals and Their Uses: A Handbook and Formulary. Norwich, NY: William Andrew (1996), p. 41-3. doi: 10.1016/B978-081551408-4.50003-X
24. Diamond JM. Evolutionary biology: dirty eating for healthy living. Nature. (1999) 400:120–1. doi: 10.1038/22014
25. Vermeer RE, Frate DA. Geophagia in rural Mississippi: environmental and cultural contexts and nutritional implications. Am J Clin Nutr. (1979) 32:2129–35. doi: 10.1093/ajcn/32.10.2129
26. Grigsby RK, Thyer BA, Waller RJ, Johnston GA Jr. Chalk eating in Middle Georgia: a culture-bound syndrome of pica? South Med J. (1999) 92:190–92. doi: 10.1097/00007611-199902000-00005
27. Waswa J, Imungi JK. Prevalence and predictors of geophagy among adolescent girls in Likuyani District of Kakamega County. J Food Nutr Disor. (2014) 3:4. doi: 10.4172/2324-9323.1000148
28. Walker M. Soil-based organisms support immune system functions from the ground up. Townsend NewsLetter for Doctors and Patients (1997).
29. Ken M, Barb, D,. Geophagy: The Earth Eaters of Lower Southwestern Australia (2017). Available online at: http://www.researchgate.net/publication/279181076_Geophagy_an_assessment_of_implication_for_the_developmet_of_Australian_Indigenous_plant_processing_technologies (accessed March, 2022).
30. Frazzoli C, Pouokam GB, Mantovani A, Orisakwe OE. Health risks from lost awareness of cultural behaviours rooted in traditional medicine: an insight in geophagy and mineral intake. Sci Total Environ. (2016) 566–567:1465-71. doi: 10.1016/j.scitotenv.2016.06.028
31. Johns T, Duquette M. Detoxification and mineral supplementation as functions of geophagy. Am J Clin Nutr. (1991) 53:448–56. doi: 10.1093/ajcn/53.2.448
32. Vermeer DE. Geophagy among the TIV of Nigeria. Ann Assoc Am Geogr. (1966) 56:197–204. doi: 10.1111/j.1467-8306.1966.tb00553.x
33. Tayie FAK, Lartey A. Pica practice among pregnant Ghanaians: relation with infant birth weight and maternal haemoglobin level. Ghana Med J. (1999) 33:67–76.
34. Dominy NJ, Davoust E, Minekus M. Adaptive function of soil consumption: an in-vitro study modeling the human stomach and small intestine. J Exp Biol. (2004) 207:319–24. doi: 10.1242/jeb.00758
35. Medical University of Vienna. Geophagy: “Soil-Eating” as an Addictive Behaviour. ScienceDaily (2016). Available online at: https://www.sciencedaily.com/releases/2016/12/161205085943.htm
36. Vermeer DE, Ferrell RE. Nigerian geophagical clay: a traditional anti-diarrheal pharmaceutical. Science. (1985) 227:634–6. doi: 10.1126/science.3969552
38. Young SL, Sherman PW, Lucks JB. Pelto GH. Why on earth?: Evaluating hypotheses about the physiological functions of human geophagy. Q Rev Biol. (2011) 86:97–120. doi: 10.1086/659884
39. Banenzoue. Réactivité en milieu acide dilué des argiles comestibles au Cameroun: Détermination du fer et du zinc assimilable. Memoire de Maîtrise, Univ. De Yaounde (1992).
40. Danford DE. Pica and nutrition. Annu Rev Nutr. (1982) 2:303–22. doi: 10.1146/annurev.nu.02.070182.001511
41. Walker ARP, Walker BF, Sookaria FI, Canaan RJ. Pica. J R Health. (1997) 117:280–4. doi: 10.1177/146642409711700503
42. Abdul RM, Arhin E. Mineralogy and geochemistry of geophagic soils in Ghana: a review. Eur J Environ Earth Sci. (2020) 1:9. doi: 10.24018/ejgeo.2020.1.3.9
43. Ekosse GIE, Ngole-Jeme VM, Diko ML. Environmental geochemistry of geophagic materials from free State Province in South Africa. Open Geosci. (2017) 9:114–25. doi: 10.1515/geo-2017-0009
44. Chen X, Singh A, Kitts DD. In-vitro bioaccessibility and bioavailability of heavy metals in mineral clay complex used in natural health products. Sci Rep. (2020) 10:8823. doi: 10.1038/s41598-020-65449-4
45. Jackson MS, Adedoyin AC, Winnick SN. Pica disorder among African American women: a call for action and further research. Soc Work Public Health. (2020) 35:261–70. doi: 10.1080/19371918.2020.1791778
46. Waswa J, Imungi JK. Efficacy of millet based product on management of geophagy: a randomized control trial. J Food Nutr Disord. (2014) 3:5. doi: 10.4172/2324-9323.1000152
47. Woywodt A, Kiss A. Geophagia: the history of earth-eating. J R Soc Med. (2002) 95:143–6. doi: 10.1258/jrsm.95.3.143
48. Abrahams PW, Julia AP. Geophagy in the tropics: a literature review. Geogr J. (1996) 162:63–72. doi: 10.2307/3060216
49. Arhin E, Zango MS. Determination of trace elements and their concentrations in clay balls: problem of geophagia practice in Ghana. Environ Geochem Health. (2017) 39:1–14. doi: 10.1007/s10653-016-9801-9
50. Nkansah MA, Korankye M, Darko G, Dodd M. Heavy metal content and potential health risk of geophagic white clay from the Kumasi Metropolis in Ghana. Toxicol Rep. (2016) 3:644–51. doi: 10.1016/j.toxrep.2016.08.005
51. Minnich V, Okcuoglu A, Tarcon Y, Arcasoy A, Cin S, Yorukoglu O, et al. Pica in Turkey: effect of clay upon iron absorption. Am J Clin Nutr. (1968) 21:78–86. doi: 10.1093/ajcn/21.1.78
52. Virginia M, Ayhan O, Yavuz T, Ayten A, Suhru C, Orhan Y, et al. Effect of clay upon iron absorption. Am J Clin Nutr. (1968) 21:78–86.
53. Hooda PS, Henry CJK, Seyoum TA, Armstrong LDM, Fowler MB. The potential impact of geophagia on the bioavailability of iron, zinc and calcium in human nutrition. J Environ Geochem Health. (2002) 24:305–19. doi: 10.1023/A:1020542810334
54. Hooda PS, Henry CJK, Seyoum TA, Armstrong LDM, Fowler MB. The potential impact of soil ingestion on human mineral nutrition. J Sci Total Environ. (2004) 333:75–87. doi: 10.1016/j.scitotenv.2004.04.023
56. Attarha BO, Mikulic S, Harris C, Scolapio JS. Kaolin clay. Anemia Cureus. (2021) 13:e13796. doi: 10.7759/cureus.13796
57. Abrahams PW. Involuntary soil ingestion and geophagia: a source and sink of mineral nutrients and potentially harmful elements to consumers of earth materials. Appl Geochem. (2012) 27:954–68. doi: 10.1016/j.apgeochem.2011.05.003
60. Lanzkowsky P. Investigation into the aetiology and treatment of pica. Arch Dis Child. (1959) 34:140–8. doi: 10.1136/adc.34.174.140
61. Kambunga SN, Candeias C, Hasheela I, Mouri H. Review of the nature of some geophagic materials and their potential health effects on pregnant women: some examples from Africa. Environ Geochem Health. (2019) 41:2949–75. doi: 10.1007/s10653-019-00288-5
62. Hunter JM. Macroterm geophagy and pregnancy clay in South Africa. J Cult Geogr. (1993) 14:69–92. doi: 10.1080/08873639309478381
63. Krief S, Klein N, Fröhlich F. Geophagy: soil consumption enhances the bioactivities of plants eaten by chimpanzees. Naturwissenschaften. (2008) 95:325–31. doi: 10.1007/s00114-007-0333-0
64. Tayie F, Koduah G, Sara M. Geophagia clay soil as a source of mineral nutrients and toxicants. Afr J Food Agric Nutr Develop. (2013) 131:7157–70. doi: 10.18697/ajfand.56.12580
65. Simon SL. Soil ingestion by humans: a review of history, data, and etiology with application to risk assessment of radioactively contaminated soil. Health Phys. (1998) 74:647–72. doi: 10.1097/00004032-199806000-00003
66. Wong MS, Bundy DAP, Golden MHN. The rate of ingestion of Ascaris lumbricoides and Trichuris trichiura eggs and its relationship to infection in two children's homes in Jamaica. Trans Roy Soc Trop Med Hyg. (1991) 85:89–91. doi: 10.1016/0035-9203(91)90172-U
67. Halsted JA. Geophagia in man: its nature and nutritional effects. Am J Clin Nutr. (1968) 21:1384–93. doi: 10.1093/ajcn/21.12.1384
68. Bonglaisin JN, Chelea M, Tsafack TJJ, Djiele PN, Mbofung CM, Lantum DN, et al. Assessment of haemoglobin status and transplacental transport of lead and calcium during geophagy. J Nutr Disorders Ther. (2017) 7:1. doi: 10.4172/2161-0509.1000211
69. Bonglaisin JN, Tsafack TJJ, Chelea M, Djiele PN, Mbofung CM, Lantum DN, et al. Effects of geophagy on hemoglobin level and iodine absorption/assimilation in Albino rats. J Nutr Disorders Ther. (2017) 7:1.
71. Dean JR, Deary ME, Gbefa BK, Scott WC. Characterization and analysis of persistent organic pollutants and major, minor and trace elements in Calabash chalk. Chemosphere. (2004) 57:21–5. doi: 10.1016/j.chemosphere.2004.05.023
72. Sidhu GPS. Heavy metal toxicity in soils: sources, remediation technologies and challenges. Adv Plants Agric Res. (2016) 5:445–6. doi: 10.15406/apar.2016.05.00166
73. Kumari N, Mohan C. Basics of clay minerals and their characteristics properties. Clay Clay Miner. (2021) 24:1–29. doi: 10.5772/intechopen.97672
74. Holmgren GGS, Meyer MW, Chaney RL, Daniels RB. Cadmium, lead, zinc, copper and nickel in agricultural soils of the United States of America. J Environ Qual. (1993) 22:335–48. doi: 10.2134/jeq1993.00472425002200020015x
75. Petruzzelli G, Pedron P, Rosellini F. Bioavailability and bioaccessibility in soil: a short review and a case study. Aims Environ Sci. (2020) 7:208–24. doi: 10.3934/environsci.2020013
76. Nweke FN, Okaka ANC, Offor EC. Lead, zinc and pH concentrations of Enyigba soils in Abakaliki local government area of Ebonyi State, Nigeria. Afr J Biotech. (2008) 7:2441–3. doi: 10.5897/AJB07.537
77. Dan'azumi S, Bichi MH. Industrial pollution and heavy metals profile of Challawa River in Kano, Nigeria. J Appl Sci Environ Sanit. (2010) 5:23–9.
78. Angle CR, Mclntire MS, Colucci AV. Lead in air, dustfall, soil, housedust, milk, and water: correlation of blood lead in urban and suburban school children. Trace Substan Environ Health. (1974) 8:23–9.
79. Johnson DE, Tillery JB, Prevost RJ. Levels of platinum, palladium, and lead in populations of Southern California. Environ Health Perspect. (1975) 12:27–33. doi: 10.1289/ehp.751227
80. Bornschein R. Lead in soil in relation to blood lead levels in children. Trace Substan Environ Health. (1986) 20:322–32.
81. Mielke HW, Adams JL, Reagan PL, Mielke PW. Soil-dust lead and childhood lead exposure as a function of city size and community traffic flow: the case for lead abatement in Minnesota. Environ Geochem Health. (1989) 9(Suppl.):253–71.
82. Usman O, Shuaib A, Dosumu O. Analysis of lead in soil and selected food samples at Kyaure Mechanic Village, Bauchi state, Nigeria. Nig J Pure Appl Sci. (2007) 22:2059–62.
83. Chaney RL, Mielke HW, Sterrett SB. Speciation, mobility and bioavailability of soil lead. In: Proc Intern Conf Lead in Soils: Issues and Guidelines (1989).
84. Madukori CH, Dressman TN. Some biochemical parameters in Gallus domesticus and heavy metal content of oil -polluted areas of Yenagoa, Bayelsa state, Nigeria. J Life Phys Sc. - acta SATECH. (2010) 3:124–8.
85. Bini C. Urban soils and human health. EQA Environ Qual. (2019) 33:1–10. doi: 10.5194/egusphere-egu2020-11255
86. Davies BE. Lead in Heavy Metals in Soils, vol. 17. In: BJ Alloway, editors. Glasgow: Blackie and Son Ltd. (1990) p. 177–96.
87. Thihalolipavan S, Candalla BM, Ehrlich J. Examining pica in NYC pregnant women with elevated blood lead levels. Matern Child Health J. (2013) 17:49–55. doi: 10.1007/s10995-012-0947-5
88. Knezevich DL, Tadic V. Decontamination with clay or alcoholate of pigs percutaneously poisoned with VX and Soman (in Croatian). Vojnosanit Pregl. (1994) 51:488–91.
89. Hassen A, Jamoussi F, Saidi N, Mabrouki Z, Fakhfakh E. Microbial and cooper adsorption by smectitic clay-an experimental study. Environ Technol. (2003) 24:1117–27. doi: 10.1080/09593330309385652
90. Katsumata H, Kaneco S, Inomata K, Itoh K, Funasaka K, Masuyama K, et al. Removal of heavy metals in rinsing wastewater from plating factory by adsorption with economical viable materials. J Environ Manage. (2003) 69:187–91. doi: 10.1016/S0301-4797(03)00145-2
91. Rowland MJ, Cook J. Geophagy: an assessment of implications for the development of Australian indigenous plant processing technologies. Environmental Protection Agency Australian Aboriginal Studies (2002).
92. Bonglaisin JN. Induced geophagy with local kaolin from Cameroon market and heavy metals (lead, cadmium and mercury profile of rat blood, liver, placentas and litters). J Med Sci. (2015) 15:10–7. doi: 10.3923/jms.2015.10.17
93. Akah PA, Zeigbo TO, Oforkansi MN, Onyeto CA. Effect of kaolin consumption on serum heavy metal levels of pregnant women. Int J Sci. (2020) 9:28–32. doi: 10.18483/ijSci.2305
94. Eigbike OC, Imasuen OI, Obomese F, Omoruyi ID. Assessing the bioavailability of some trace and major elements in geophagical clays of south - western and eastern Nigeria: An invitro study. Int J Earth Sc Knowl Appl. (2022) 4:106–15. Available online at: http://www.ijeska.com/index.phy/ijeska
95. Lyons KE, Pahwa R. Handbook of Essential Tremor and Other Tremor Disorders. 1st Ed. Boca Raton, FL: Taylor and Francis Group (2005). p. 22. doi: 10.1201/b14115
96. Garrettson LK. Lead in Clinical Management of Poisoning and Drug Over-Dose. Haddad LM, Winchester JF, editor. Philadelphia: W Saunders Co. (1990) p. 1017–23.
97. Pagliuca A, Mufti GJ, Baldwin D, Lestas AN, Wallis RM, Bellingham AJ. Lead poisoning: clinical, biochemical, and haematological aspects of a recent outbreak. J Clin Pathol. (1990) 43:277–81. doi: 10.1136/jcp.43.4.277
98. Cullen MR, Robins JM, Eskenazi B. Adult inorganic lead intoxication: presentation of 31 new cases and a review of recent advances in the literature. Medicine. (1983) 62:221–47. doi: 10.1097/00005792-198307000-00003
99. Brevik EC, Slaughter L, Singh BR, Steffan JJ, Collier D, Barnhart P, et al. Soil and human health: current status and future needs. Air Soil Water Res. (2020) 13:1–23. doi: 10.1177/1178622120934441
100. Kwong WT, Friello P, Semba RD. Interactions between iron deficiency and lead poisoning: epidemiology and pathogenesis. Sci Total Environ. (2004) 330:21–37. doi: 10.1016/j.scitotenv.2004.03.017
101. Lyn P. Lead toxicity, a review of the literature. Part I: exposure, evaluation, and treatment. Altern Med Rev. (2006) 11:2–22. doi: 10.1186/s12906-021-03471-3
102. Gropper SS, Smith JL, Groff JL. Advanced Nutrition and Human Metabolism. 5th Ed. New York, NY: Cengage Learning (2012). p. 485–623.
103. Kempe DS, Lang PA, Eisele K, Klarl BA, Wieder T, Huber SM, et al. Stimulation of erythrocyte phosphatidylserine exposure by lead ions. Am J Physiol Cell Physiol. (2005) 288:396–402. doi: 10.1152/ajpcell.00115.2004
104. Stathatos N. Thyroid physiology. Med Clin North Am. (2012) 96:165–73. doi: 10.1016/j.mcna.2012.01.007
105. Hetzel BS. The Story of Iodine Deficiency, 1st edn. Great Britain: Oxford Medical Publications (1989). p. 3.
106. Miller MD, Crofton KM, Rice DC, Zoeller RT. Thyroid-disrupting chemicals: interpreting upstream biomarkers of adverse outcomes. Environ Health Perspect. (2009) 117:1033–41. doi: 10.1289/ehp.0800247
107. Pearce EN, Braverman LE. Environmental pollutants and the thyroid. Best Pract Res Clin Endocrinol Metab. (2009) 23:801–13. doi: 10.1016/j.beem.2009.06.003
108. Lamb MR, Janevic T, Liu X, Cooper T, Kline J, Factor-Litvak P. Environmental lead exposure, maternal thyroid function, and childhood growth. Environ Res. (2008) 106:195–202. doi: 10.1016/j.envres.2007.09.012
109. Schell LM, Gallo MV, Denham M, Ravenscroft J, DeCaprio AP, Carpenter DO. Relationship of thyroid hormone levels to levels of polychlorinated biphenyls, lead, p, p'-DDE, and other toxicants in Akwesasne Mohawk youth. Environ Health Perspect. (2008) 116:806–13. doi: 10.1289/ehp.10490
110. Dundar B, Oktem F, Arslan MK, Delibas N, Baykal B, Arslan C, et al. The effect of long-term low-dose lead exposure on thyroid function in adolescents. Environ Res. (2006) 101:140–5. doi: 10.1016/j.envres.2005.10.002
111. Jin Y, Liao Y, Lu C, Li G, Yu F, Zhi X, et al. Health effects in children aged 3-6 years induced by environmental lead exposure. Ecotoxicol Environ Saf. (2006) 63:313–7. doi: 10.1016/j.ecoenv.2005.05.011
112. Robins JM, Cullen MR, Connors BB, Kayne RD. Depressed thyroid indexes associated with occupational exposure to inorganic lead. Arch Intern Med. (1983) 143:220–4. doi: 10.1001/archinte.143.2.220
114. Gurer-Orhan H, Sabir HU, Ozgunes H. Correlation between clinical indicators of lead poisoning and oxidative stress parameters in controls and lead-exposed workers. Toxicology. (2004) 195:147–54. doi: 10.1016/j.tox.2003.09.009
115. López CM, Piñeiro AE, Núñez N, Avagnina AM, Villaamil EC, Roses OE. Thyroid hormone changes in males exposed to lead in the Buenos Aires area (Argentina). Pharmacol Res. (2000) 42:599–602. doi: 10.1006/phrs.2000.0734
116. Singh B, Chandran V, Bandhu HK, Mittal BR, Bhattacharya A, Jindal SK, et al. Impact of lead exposure on pituitary-thyroid axis in humans. Biometals. (2000) 13:187–92. doi: 10.1023/A:1009201426184
117. Tuppurainen M, Wagar G, Kurppa K, Sakari W, Wambugu A, Froseth B, et al. Thyroid function as assessed by routine laboratory tests of workers with long-term lead exposure. Scand J Work Environ Health. (1988) 14:175–80. doi: 10.5271/sjweh.1934
118. Meeker JD, Rossano MG, Protas B, Diamond MP, Puscheck E, Daly D, et al. Multiple metals predict prolactin and thyrotropin (TSH) levels in men. Environ Res. (2009) 109:869–73. doi: 10.1016/j.envres.2009.06.004
119. Erfurth EM, Gerhardsson L, Nilsson A, Rylander L, Schutz A, Skerfving S, et al. Effects of lead on the endocrine system in lead smelter workers. Arch Environ Health. (2001) 56:449–55. doi: 10.1080/00039890109604481
120. Schumacher C, Brodkin CA, Alexander B, Cullen M, Rainey PM, van Netten C, et al. Thyroid function in lead smelter workers: absence of subacute or cumulative effects with moderate lead burdens. Int Arch Occup Environ Health. (1998) 71:453–8. doi: 10.1007/s004200050305
121. Siegel M, Forsyth B, Siegel L, Cullen MR. The effect of lead on thyroid function in children. Environ Res. (1989) 49:190–6. doi: 10.1016/S0013-9351(89)80064-7
122. Badiei K, Nikghadam P, Mostaghni K, Zarifi M. Effect of lead on thyroid function in sheep. Ira J Vet Res. (2009) 10:223–7. Available online at: https://ijvr.shirazu.ac.ir/article_1696_0d0c3ff42cbc25c34d9b1a61611839f5.pdf
123. Ashraf SY, Asma AA. Effects of cadmium (Cd) and Lead (Pb) on the structure and function of thyroid gland. Adv J Environ Sci Technol. (2009) 11:1–8. Available online at: https://www.internationalscholarsjournals.com/articles/effects-of-cadmium-cd-and-lead-pb-on-the-structure-and-function-of-thyroid-gland.pdf
124. Tunega D, Zaoui A. Mechanical bonding and behaviour behind the bending mechanism of kaolinite clay layers. J Phys Chem. (2020) 13:7432–40. doi: 10.1021/acs.jpcc.9b11274
125. ATSDR. Toxicological Profile for Lead. US Department of Health and Human Services: Public Health Service (1999).
126. Davidson KA. Toxicity profiles (1994). Available online at: https://rais.ornl.gov/tox/profiles/lead.shtm (accessed November 1, 2021).
127. Klaassen CD. Heavy metals and heavy-metal antagonists. In: Hardman JG, Limbird LE, Gilman AG editors. The Pharmacological Basis of Therapeuties. 10 ed, Newyork, NY: McGraw hill (2011) 1851–1875.
128. Garza A, Vega R, Soto E. Cellular mechanisms of lead neurotoxicity. Med Sci Monit. (2006) 12:RA57–65. doi: 10.1007/s00204-008-0345-3
129. Bridges CC, Zalups RK. Molecular and ionic mimicry and the transport of toxic metals. Toxicol Appl Pharmacol. (2005) 204:274–308. doi: 10.1016/j.taap.2004.09.007
130. Ballatori N. Transport of toxic metals by molecular mimicry. Environ Health Perspect. (2002) 110 (Suppl. 5):689–94. doi: 10.1289/ehp.02110s5689
131. Frausto da. Silva JR, Williams RJP. The Biological Chemistry of the Elements: The Inorganic Chemistry of Life. 2nd ed. New York: Oxford University Press (2001).
132. Katz AK, Glusker JP, Beebe SA, Bock CW. Calcium ion coordination: a comparison with that of beryllium, magnesium, and zinc. J Am Chem Soc. (1996) 118:5752–563. doi: 10.1021/ja953943i
133. Lidsky TI, Schneider JS. Lead neurotoxicity in children: basic mechanisms and clinical correlates. Brain. (2003) 126:5–19. doi: 10.1093/brain/awg014
134. Bouton CM, Hossain MA, Frelin LP, Laterra J, Pevsner J. Microarray analysis of differential gene expression in lead-exposed astrocytes. Toxicol Appl Pharmacol. (2001) 176:34–53. doi: 10.1006/taap.2001.9274
135. Fujiwara Y, Yamamoto C, Kaji T. Proteoglycans synthesized by cultured bovine aortic smooth muscle cells after exposure to lead: lead selectively inhibits the synthesis of versican, a large chondroitin sulfate proteoglycan. Toxicology. (2000) 154:9–19. doi: 10.1016/S0300-483X(00)00269-9
136. Breen KC, Regan CM. Lead stimulates Golgi sialyltransferase at times coincident with the embryonic to adult conversion of the neural cell adhesion molecule (N-CAM). Toxicology. (1998) 49:71–6. doi: 10.1016/0300-483X(88)90176-X
137. Davey FD, Breen KC. Stimulation of sialyltransferase by subchronic lowlevel lead exposure in the developing nervous system. A potential mechanism of teratogen action. Toxicol Appl Pharmacol. (1998) 151:16–21. doi: 10.1006/taap.1998.8427
138. He L, Poblenz AT, Medrano CJ, Fox DA. Lead and calcium produce rod photoreceptor cell apoptosis by opening the mitochondrial permeability transition pore. J Biol Chem. (2000) 275:12175–84. doi: 10.1074/jbc.275.16.12175
139. Nunes-Tavares N, Valverde RHF, Araujo GMN, Hasson-Voloch A. Toxicity induced by Hg2+ on choline acetyltransferase activity from E. electricus (L.) electrocytes: the protective effect of 2,3 dimercapto-propanol (BAL). Med Sci Monit. (2005) 11:100–5.
140. Greenwood NN, Earnshaw A. Chemistry of the elements. 2nd ed. London: Butterworth-Heinemann. (1999)
141. Magyar JS, Weng TC, Stern CM, Dye DF, Rous BW, Payne JC, et al. Reexamination of lead (II) coordination preferences in sulfur-rich sites: implications for a critical mechanism. J Am Chem Soc. (2005) 127:9495–505. doi: 10.1021/ja0424530
142. Ghering AB, Miller Jenkins LM, Schenck BL, Deo S, Mayer RA, Pikaart MJ, et al. Spectroscopic and functional determination of the interaction of Pb2+ with GATA proteins. J Am Chem Soc. (2005) 127:3751–9. doi: 10.1021/ja0464544
Keywords: geophagy, prevalence, toxicity potential, clay, review
Citation: Bonglaisin JN, Kunsoan NB, Bonny P, Matchawe C, Tata BN, Nkeunen G and Mbofung CM (2022) Geophagia: Benefits and potential toxicity to human—A review. Front. Public Health 10:893831. doi: 10.3389/fpubh.2022.893831
Received: 10 March 2022; Accepted: 30 June 2022;
Published: 26 July 2022.
Edited by:
Luigimaria Borruso, Free University of Bozen-Bolzano, ItalyReviewed by:
Ngambouk Vitalis Pemunta, Linnaeus University, SwedenCopyright © 2022 Bonglaisin, Kunsoan, Bonny, Matchawe, Tata, Nkeunen and Mbofung. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julius Nsawir Bonglaisin, bmp1bGl1c2ZyaWRhQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.