 Elsabeth Legesse1†
Elsabeth Legesse1† Tadesse Nigussie1†
Tadesse Nigussie1† Derara Girma1*†
Derara Girma1*† Leta Adugna Geleta1†
Leta Adugna Geleta1† Hiwot Dejene1†
Hiwot Dejene1† Berhanu Senbeta Deriba1†
Berhanu Senbeta Deriba1† Tinsae Abeya Geleta1†
Tinsae Abeya Geleta1† Degemu Sahlu1†Mengistu Tesema1†Ayele Tilahun2†
Degemu Sahlu1†Mengistu Tesema1†Ayele Tilahun2† Mukemil Awol3†
Mukemil Awol3† Firanbon Teshome4†
Firanbon Teshome4† Gachana Midaksa5†Feyiso Bati6†
Gachana Midaksa5†Feyiso Bati6†- 1Department of Public Health, College of Health Science, Salale University, Fitche, Ethiopia
- 2Department of Nursing, College of Health Science, Salale University, Fitche, Ethiopia
- 3Department of Midwifery, College of Health Science, Salale University, Fitche, Ethiopia
- 4Department of Health Behavior and Society, Faculty of Public Health, Institute of Health, Jimma University, Oromia, Ethiopia
- 5Department of Public Health, College of Health Sciences, School of Public Health, Mizan Tepi University, Mizan Tepi, Ethiopia
- 6Department of Public Health, College of Health Sciences, Dire Dawa University, Dire Dawa, Ethiopia
Background: Non-communicable diseases (NCDs) are currently the leading cause of morbidity and mortality, posing significant challenges to global healthcare systems. Particularly, the prevalence of NCDs is rising in Ethiopia, resulting in a triple burden of diseases on the health system that disproportionately affects all age groups. Hence, this study aims to determine the level of adequate knowledge of NCDs and associated factors among adult residents of the North Shewa zone, Oromia region, Ethiopia.
Methods: A community-based cross-sectional study with a concurrent mixed-method approach was conducted from April 1, 2021 to May 30, 2021 among 846 residents using the multistage sampling technique. Interviewer administered questionnaire was used to collect quantitative data and a guiding checklist was used to collect qualitative data. Bivariable and multivariable logistic regressions were fitted to compute the association between explanatory variables and knowledge of NCDs. Adjusted odds ratios at 95% confidence interval with a p-value < 0.05 were used to decree statistical significance in multivariable analysis. Also, a thematic framework analysis was used for qualitative data analysis.
Results: A total of 823 subjects have participated in this study making a response rate of 97.3%. The level of adequate knowledge was 33.9% (95%CI: 30.67, 37.13). Higher-income, receiving information from health professionals, owning a TV, having a family member with NCD(s), and marital status were factors significantly associated with adequate knowledge of NCDs.
Conclusion: This study reveals a high level of inadequate knowledge of NCDs despite its foundational ability in tackling the burden of NCDs. As a result, broadening a wider and more comprehensive health promotion strategy for the prevention of triple burden of NCDs would benefit the population. Additionally, special efforts are needed both at the practice and policy levels targeting the disadvantaged groups, such as low-income people, those who do not receive information from health professionals, those who do not own a television, and those who are widowed/divorced, who were found to have less knowledge of NCDs.
Introduction
Non-communicable diseases (NCDs) are a group of conditions that include cardiovascular diseases, chronic respiratory diseases, cancers, and diabetes (1). However, the term “NCDs” has come to refer to a wide range of health concerns, including hepatic, renal, and gastroenterological diseases, endocrine, hematological, and neurological disorders, dermatological conditions, genetic disorders, trauma, mental disorders, and disabilities (e.g., blindness and deafness) (2).
According to the World Health Organization (WHO) (2021), NCDs kill 41 million people each year, accounting for 71% of all deaths worldwide, with 77% of NCD deaths occurring in low- and middle-income countries (LMICs). Subsequently, the most common NCD is cardiovascular disease, which kills 17.9 million people each year, followed by cancer (9.3 million), respiratory disorders (4.1 million), and diabetes (1.5 million) (3). This unnoticed epidemic is a major cause of poverty and a significant impediment to many countries' economic growth (4).
Tobacco use, physical inactivity, harmful alcohol use, and unhealthy diets are all linked to an increased risk of dying from NCDs (3). Furthermore, modifiable risk factors like high blood pressure, obesity, elevated blood sugar level, and high blood cholesterol, as well as non-modifiable risk factors like age, gender, genetic factors, race, and ethnicity, were revealed to increase the risk of NCDs (5–7). Nonetheless, detection, screening, and treatment of NCDs, as well as palliative care, are all important parts of the NCD response (3, 8).
Many NCDs have historically been linked to economic growth and termed “diseases of the rich.” However, nowadays, the burden of NCDs has increased in developing countries (7), while a dramatic decrease in NCDs-related burden is recorded in developed countries (9). As a result of aging, increased unplanned urbanization, and globalization of unhealthy lifestyles, the burden of NCDs and associated risk factors continues to rise in African countries (10).
Concerning knowledge of NCDs, studies conducted among diverse populations in different countries have revealed varying levels of knowledge of NCDs. Accordingly, a good level of knowledge was reported to be 81.2% in Malaysia (11), 57.9% in Bangladesh (12), 46.7% in Spain (13), 43.8% in Saudi Arabia (14), 43% in Sri Lanka (15), 27.7% in Malaysia (16), 25% in China (17), and 12.5% in Myanmar (18). Furthermore, a finding from China indicates chronic diseases knowledge varied from 29.5 to 90.2% (19).
Regarding factors associated with knowledge of NCDs; being females (12, 19), age (11, 12), higher level of education (16, 20, 21), higher wealth index (18), higher income (12), having health insurance (19), having a family history of chronic disease(s) (17–19), participating in society discussion (19), and more frequently gathering with friends/relatives (19), not smoking (12, 15), physical activity (12), receiving NCDs health information and self-care instructions from their physicians (17) were found to heighten the likelihood of having an adequate level of knowledge about NCDs.
In a particular, the prevalence of NCDs is increasing in Ethiopia, resulting in a triple burden of diseases to the health system (i.e., communicable diseases, NCDs, and injuries) that disproportionately affects all age groups (22). Subsequently, the likelihood of dying prematurely from one of the main NCDs is 17.4% for males and 16.9% for females in Ethiopia (23). Furthermore, the country's NCD mortality is primarily attributed to cardiovascular diseases (CVDs) and cancer (24). Concerningly, NCDs have been identified as future threats that Ethiopia's health sector will be unable to address on its own, necessitating multisectoral collaboration (25). Predominantly, inadequate knowledge of NCDs is one of the principal causes of high mortality, along with inadequate screening, early detection, and treatment, and insufficient diagnostic and treatment facilities available in the country (22).
Overall, the epidemic of NCDs poses challenging health consequences for individuals, families, and communities, and threatens to overwhelm healthcare systems (3). Moreover, knowledge gaps about NCDs and their risk factors in the general population are significant barriers to effective NCD prevention and treatment (26). However, despite the enormous challenge that NCDs pose, the level of adequate knowledge and associated factors remain unidentified in Ethiopia (22, 27). As a result, a need for further study on the knowledge of NCDs is suggested (28). Hence, the present study aims to determine the level of adequate knowledge of NCDs and associated factors among adult residents of the North Shewa zone, Oromia region, Ethiopia. Given all of the research gaps and needs for further investigation in Ethiopia, conducting such a study will result in early detection, a reduction in the NCD burden, and guidance in the development of an effective policy.
Methods and Materials
Study Area, Design, and Period
The study was conducted in the North Shewa zone, Oromia region, Ethiopia. The zone has a total area of 10,322.48 km2 and a population density of 138.66 people per km2, with 13 rural districts and two town administrations. Furthermore, the Zone has a total population of approximately 1,639,586 people, of whom 717,552 are men and reside in 521,506 households. Fiche town – the zone's capital – is 112 kilometers north of Addis Ababa –Ethiopia's capital. Additionally, the zone has 64 health centers and five public hospitals that provide health care services to the community. A community-based cross-sectional study design with a concurrent mixed-method approach was conducted from April 1, 2021 to May 30, 2021.
Populations and Eligibility Criteria
A source population consisted of all adults over the age of 18 who were permanent residents (individuals who live at least 6 months) of a selected town in the North Shewa zone. A study population was randomly selected adult residents for a quantitative study. A qualitative study was conducted among purposely selected residents, health care providers, and public health experts.
Sample Size, Sampling Frame, and Participants Recruitment
The sample size was determined using a single population proportion formula in Epi Info STAT CALC. version 7.2 based on the assumptions of a 95% confidence level, 5% margin of error (d), and a 50% proportion (p) of knowledge of NCDs. Because no similar study had previously been conducted in Ethiopia, 50% was taken. After applying a design effect of 2 and a 10% non-response rate, the final sample size obtained was 846. Additionally, a total of five sessions of Focus Group Discussions (FGDs) were conducted among residents in the selected districts. Each FGD was composed of 10 residents. Additionally, 10 In-Depth Interview (IDI) was conducted among health care providers with different professionals and public health experts. Regarding a sampling technique, a multistage sampling technique was used. Towns in the zone were purposely selected since the prevalence of NCDs is high among urban populations. Thirty percent of the towns in the zone were randomly selected by lottery method, namely Fiche, Kuyu, Debretsige, Mukaturi, and Gundomeskel town. Consequently, 30% of their kebeles (small administration units) were included in the study. The sample size was proportionally allocated to each town. Finally, a computer-generated simple random sampling technique was used to select households from the kebeles using house numbers. In a household with more than one adult individual, the lottery method was used to select one of them. For the qualitative part, the purposive sampling technique was employed considering maximum variability with the assumption of obtaining relevant data to supplement the research objectives. The intention was to explore detailed information on NCDs knowledge and healthy lifestyle in society.
Data Collection Tools, Personnel, and Procedures
The data collection tool was developed after reviewing previously done studies and it has four sections including; socio-demographic, exposure to NCDs information, knowledge of NCDs, and practices of healthy lifestyles (15, 29–32). The knowledge measuring tool was reliable in this study (Cronbach-alpha = 0.72). Ten experienced BSc nurses were recruited for data collection, and onsite supervision was provided by five BSc in public health supervisors to facilitate data collection procedures on a daily basis. Data were collected through a face-to-face interview by using a pre-tested questionnaire. Additionally, FGDs and IDIs were used to get participants' experiences related to knowledge of NCDs. By using an open-ended guiding list of questions, five sessions of FGDs were undertaken to explore the knowledge of NCDs and the healthy life practice of the community. The FGDs were moderated by an experienced health professional and note taker. During the discussion, notes were taken and their voices were recorded using a tape recorder. Similarly, 10 sessions of IDIs were conducted among health care providers and public health experts.
Study Variables
The dependent variable of the study was the level of adequate knowledge of NCDs. Knowledge was assessed by 32 questions related to respondents' knowledge about NCDs and their risk factors. Correct answers were given a score of 1 and incorrect answers were given 0. The total possible score ranged from 0 to 32. A cut-off level ≥60%, of the individual percentage scores, was selected as an indicator of adequate knowledge (15). As well, in the current study the tool has an acceptable reliability (Cronbach-alpha = 0.81). The explanatory variables were socio-demographic (age, sex, religion, marital status, educational status, occupational status, income, and ethnicity), exposure information about NCDs (getting information from media, getting information from health professionals, getting information from family members, having family members with NCDs and having friends with NCDs) and behavioral factors (physical activity, alcohol and tobacco use).
Data Processing and Analysis
The collected data were checked for completeness manually and entered, cleaned, and checked by Epi data manager version 4.0.2 and then exported to SPSS version 23 for analysis. Descriptive analysis of different variables was done based on their nature. Bivariable analysis was done using binary logistic regression for all independent variables and a p-value < 0.25 was used to consider candidate variables for the multivariable analysis. Finally, a multivariable binary logistic regression analysis was done to control for possible confounders and to identify factors significantly associated with an adequate level of knowledge of NCDs at a p-value of < 0.05 with a 95% confidence interval adjusted odds ratio. Model fitness was checked using the Hosmer and Lemeshow goodness of fit model and it was fitted (p-value = 0.12). as well, the variance inflation factor was set at five to detect multicollinearity among explanatory variables, and no multicollinearity was found. Besides, before analyzing data, all FGDs and IDIs were transcribed in Afan Oromo text by replaying the recorded voice from tape and the notes taken during discussion. Then, the Afan Oromo version text was translated into English language. Different ideas in the text were merged in their thematic areas and thematic framework analysis was done manually. The results were presented in narration by triangulating with quantitative findings.
Ethical Consideration
Ethical approval was obtained from the ethical review committee of Salale University. A permission letter was obtained from the respective district and kebele administration before data collection. Written informed consent was obtained from each study participant.
Results
Socio-Demographic Characteristics
A total of 823 respondents have completed the study making a response rate of 97.3%. The mean age (standard deviation) of the respondents was 31.83 (11.04) years. Of the total participants, more than half, 443 (53.8%) were females. Regarding marital status, 497 (60.4%) of them were married. Approximately, one-third, 255 (31%) of them attended above secondary education. Furthermore, the majority, 628 (76.3%) of the participants were from the Oromo ethnic group. Additionally, nearly a fourth, 189 (23%) of them were a merchant (Table 1).
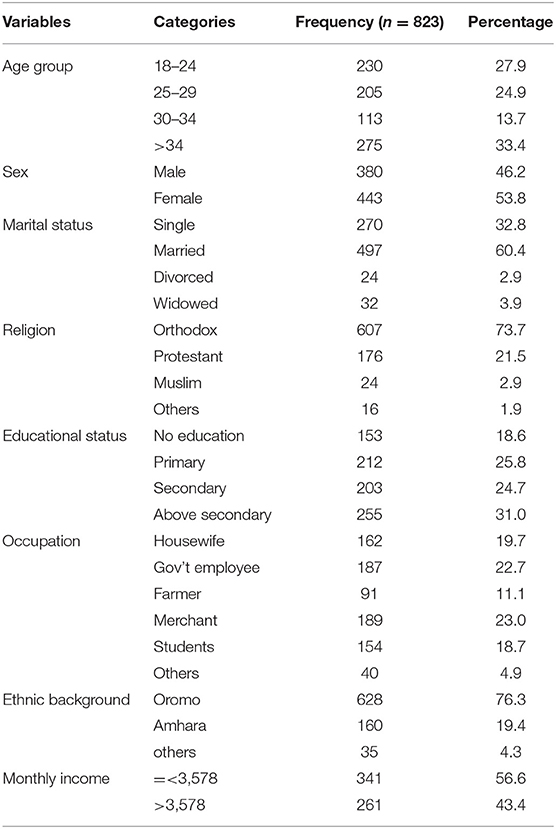
Table 1. Socio-demographic characteristics of adult residents of selected towns in North Shewa zones, Oromia region, central Ethiopia, 2021.
Knowledge of NCDs
On the 32 items tool measuring respondents' knowledge about NCDs, the mean score (standard deviation) of respondents was 14.6 (4.34). Of the total, 279 (33.9%) of the participants had an adequate level of knowledge (Figure 1). Regarding the causes of NCDs, more than two-thirds, 568 (69.0%) stated that NCDs are caused by supernatural power (God). In line with this, a misconception about the cause of the disease was observed among FGD participants. For instance, a 31 years old male discussant said “… Eating vegetables can lead to chronic diseases such as diabetes and hypertension due to their low nutritional value and weakness in increasing protection against these diseases…” Regarding the onset time, about 446 (54.2%) of the study participants said that NCDs onset only at an older age (Table 2). Similarly, participants of IDI explained that there is no sufficient knowledge in the community regarding NCDs. For example, a 34 years old female clinical nurse said that “Because there is a lack of public awareness about these diseases, people seek medical attention after they develop complications…” Also, a male public health expert of 29 years old working at a health center explained that the community has no awareness about NCDs. He has elucidated that “In general, there is a lack of awareness among communities about their health status. They drink as much alcohol as they desire, and no one engages in physical activity... They are unconcerned about NCDs...”
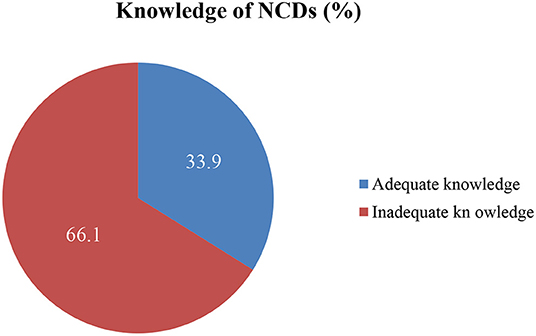
Figure 1. Knowledge level of NCDs among adult residents of selected towns of north Shewa zone, Oromia region, central Ethiopia, 2021.
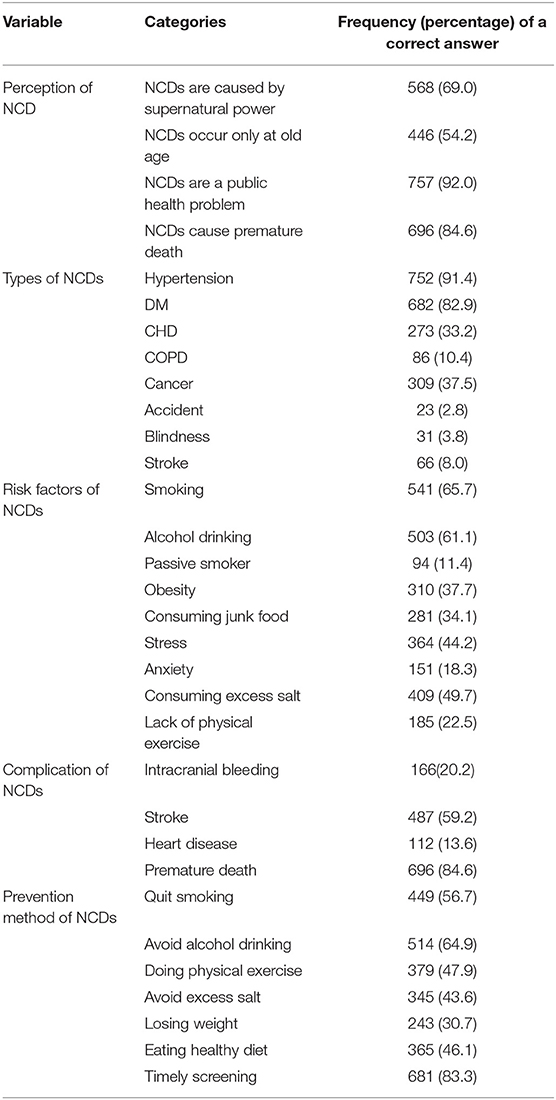
Table 2. Knowledge measuring variables among adult residents of selected towns of north Shewa zone, Oromia region, central Ethiopia, 2021.
Factors Associated With Knowledge of NCDs
In bivariable analysis, variables such as sex, age group, educational status, marital status, income, occupation, presence of TV, getting information from health professionals, having neighbors with NCDs, and presence of a family member(s) with NCDs were significantly associated with the knowledge of NCDs. In multivariable analysis, income, getting information from health professionals, owning a TV, having a family member with NCD, and being widowed/divorced were significantly associated with adequate knowledge of NCDs. Accordingly, respondents who earn a monthly income of ≥3,578 were almost two times more likely to have adequate knowledge about NCDs as compared with those who earn a monthly income of <3,578 (AOR = 1.68, 95% CI: 1.05–2.68). Respondents who received information from health professionals were more than twice more likely to have adequate knowledge of NCDs when compared with those do not receive information from health professionals (AOR = 2.29, 95% CI:1.53–3.45). Moreover, having family members with NCDs was associated with the knowledge of residents i.e., respondents who have family members with NCDs were more than two times more likely to have adequate knowledge of NCDs when compared to their counterparts (AOR = 2.23, 95% CI:1.49–3.35). Besides, respondents who possessed television were more than twice more likely to have adequate knowledge about NCDs as compared to those who don't possess television (AOR = 2.48, 95%CI:1.32–4.65). Additionally, the marital status of the respondents determines the level of NCDs knowledge. Thus, the likelihood of having adequate knowledge among divorced and widowed participants is 0.80 less likely as compared to unmarried participants (AOR = 0.20, 95%CI:0.07–0.59) (Table 3).
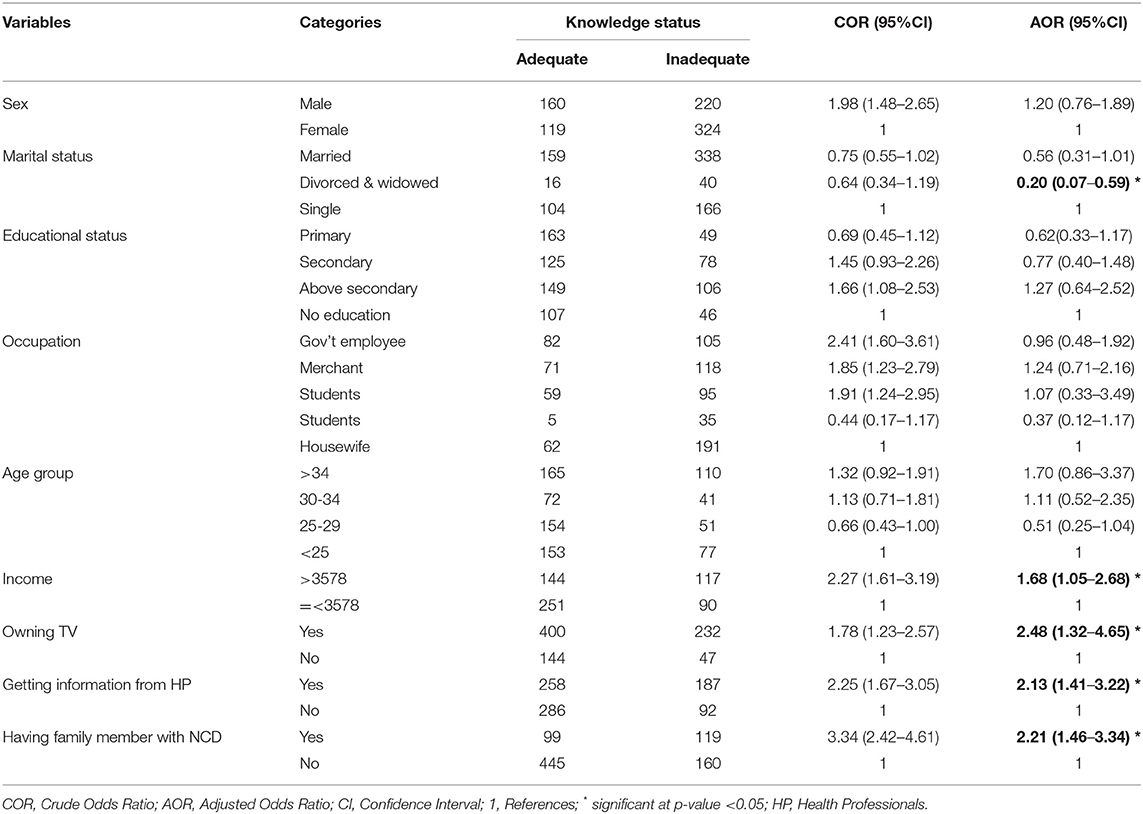
Table 3. Factors associated with knowledge of NCDs among adult residents of selected towns of north Shewa zone, Oromia region, central Ethiopia, 2021.
Exposure to Information About NCDs
Concerning information exposure, all of the study participants heard about NCDs. The majority of the participants, 619 (75.2%) of them heard about NCDs from Television (TV) (Figure 2). Comparable to this a 32 years old male participant in FGD stated that “…I usually watch TV in my spare time, and there are advertisements on TV that promote healthy behavior such as reducing salt consumption, quitting smoking, and receiving immunization against diseases such as the human papillomavirus, which causes cervical cancer.…”
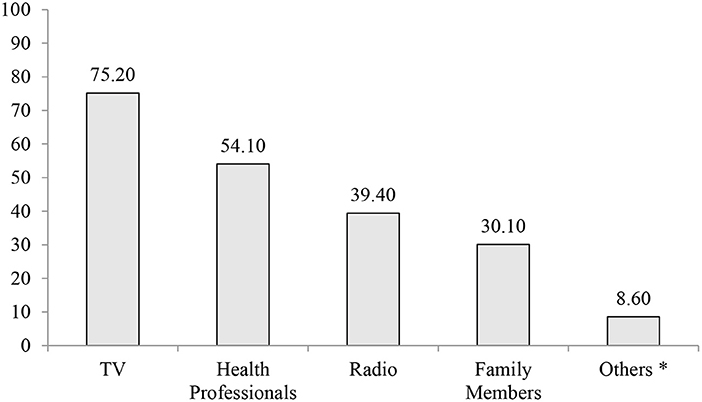
Figure 2. Sources of information about NCDs among adult residents of selected towns of north Shewa zone, Oromia region, central Ethiopia, 2021. *Friends, Neighbors, Newspapers.
Of the total, 218 (26.5%) of study participants have a family member(s) with NCDs. This view is echoed by a 24 years old female FGD participant as; “… My father has been suffering from hypertension and diabetes mellitus. Once upon a time, he was admitted to the hospital due to an extremely high blood sugar level, for which I had been caring for him. And, a nurse told me that such diseases have their roots at a young age and advised me to take preventive measures such as eating vegetables, exercising regularly, avoiding high-fat foods, and getting regular health check-ups.…”
The prevalent NCD was hypertension accounting for 187 (22.7%). This is also evidenced by IDI results. A 41 years old male public health officer stated that “…I've been serving in this community for over 8 years, and the most common NCD I've observed is hypertension, followed by diabetes mellitus…”
Discussion
This study aims to determine the adequate level of knowledge of NCDs and associated factors among adult residents of the North Shewa zone, Oromia region, Ethiopia. Accordingly, the level of adequate knowledge of NCDs among residents was 33.9% (95%CI: 30.67, 37.13). Income, receiving information from health professionals, owning a TV, having a family member with NCD(s), and marital status were factors significantly associated with adequate knowledge of NCDs.
About 33.9% of the participants had an adequate level of knowledge of NCDs. The current study is consistent with a study from Rwanda (35.0%) (21). However, the prevalence of the current study is lower than the studies from Bangladesh (57.9%) (12), Spain (46.7%) (13), Saudi Arabia (43.8%) (14), and Sri Lanka (43%) (15). The variation might be due to differences in the study population, sampling techniques, and sociodemographic characteristics. In contrast, the finding of this study is higher than the study done in Malaysia (27.7%) (16). Utilization of different knowledge measuring tools may result in discrepancies. Additionally, the current magnitude is higher than a study done in China (25%) (17) and much higher than a study from Myanmar (12.5%) (18). The difference might be attributed to variation in a study population and study settings (17).
In a current study, having a family member with NCD(s) had increased the likelihood of NCDs knowledge. This is also evidenced by previous studies (17–19). Because this will lead to improved consideration of disease control for themselves eventually (17). Besides, this might be due to study subjects' involvement in caregiving to family members' with NCD(s) (18). Moreover, receiving information from health professionals increased the chance of adequate NCDs knowledge. The previous study also supports this finding (17). This is because receiving counseling services from health care providers will contribute to a discussion on various health topics, resulting in increased knowledge and understanding of NCDs.
Furthermore, having a higher income has resulted in a higher likelihood of having adequate knowledge of NCDs. This finding was supported by previous studies (12, 18). This could be explained as the presence of a concentration of risky behaviors for NCDs among the poorest residents (18). Additionally, owning a TV as a source of information is significantly associated with adequate knowledge of NCDs. The previous research also found that mass media, including television, has a massive capacity to assist healthy behavioral changes attributed to NCDs (33). Moreover, being widowed/divorced was found to have inadequate knowledge of NCDs in a current study. As a result, being widowed was associated with worse health outcomes (34, 35).
Implications for Policy and Practice
As NCDs are one of the major health and development challenges we face today, investigating a related theme will lead to a deep understanding of the problem and searching for an effective solution like detection, screening, treatment, and palliative care. Particularly, Ethiopia's health system is working to implement awareness-raising programs on NCDs and risk factors for different segments of the population (22). Without knowledge about NCDs and their risk factors, it is difficult to achieve a reduction in the incidence and prevalence of NCDs (36). As a result, determining the level of knowledge about NCDs emphasizes the significance of conducting regular surveillance for NCDs' risk factors and initiating prevention programs (15).
Methodological Consideration
All questionnaires were translated to the local language (Afan Oromo) by two independent bilingual translators and back-translated to English to guarantee consistency. Then it was pre-tested on 5% of the total sample size in the district which was not selected for actual study to evaluate readability, understandability, completeness, and reliability, and modification was made accordingly. Data collectors and supervisors were trained on the objectives of the study, how to collect data, and ethics. Filled questionnaires were checked for completeness and consistency on daily basis. Overall activities of the study were supervised by the supervisors and regulated by the investigators. Despite these, being a cross-sectional study, made it impossible to draw causal inferences. Additionally, a self-report technique was used to assess the knowledge, which may have resulted in recall bias and social desirability bias.
Conclusion
This study reveals a high magnitude of inadequate level of NCDs knowledge despite its foundational ability in tackling the burden of NCDs. As a result, broadening a wider and more comprehensive health promotion strategy for the prevention of double burden of NCDs would benefit the population. Additionally, special efforts are needed both at the practice and policy levels to target disadvantaged groups, such as low-income earners, those who do not receive information from health professionals, those who do not own a television, and those who are widowed/divorced, who were found to have less knowledge of NCDs. More research is needed to elucidate the factors that can lead to poor knowledge about NCDs.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Salale University Institution review board. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors made a significant contribution to the work reported, in the conception, study design, execution, acquisition of data, analysis and interpretation, took part in drafting, critically reviewing the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This research was funded by Salale University, Ethiopia under grant number SU/1270/21/2013.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
CVDS, cardiovascular diseases; LMICs, low- and middle-income Countries; NCDs, non-communicable diseases; WHO, world health organization.
References
1. Allen L. Are we facing a non-communicable disease pandemic? J Epidemiol Glob Health. (2017) 7:5–9. doi: 10.1016/j.jegh.2016.11.001
2. World Health Organization. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. (2013). Available online at: http://apps.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf (accessed 16 December, 2021).
3. World Health Organization. Noncommunicable diseases [Internet]. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed 16 December, 2021).
4. World Health Organization. Noncommunicable diseases [Internet]. (2020). Available online at: https://www.who.int/data/gho/data/themes/noncommunicable-diseases (accessed 16 December, 2021).
5. Kahn SE, Cooper ME, Del Prato S. Pathophysiology and treatment of type 2 diabetes: Perspectives on the past, present, and future. Lancet. (2014) 383:1068–83. doi: 10.1016/S0140-6736(13)62154-6
6. Imamura F, O'Connor L, Ye Z, Mursu J, Hayashino Y, Bhupathiraju SN, et al. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. BMJ. (2015) 351:1–12. doi: 10.1136/bmj.h3576
7. Budreviciute A, Damiati S, Sabir DK, Onder K, Schuller-Goetzburg P, Plakys G, et al. Management and prevention strategies for non-communicable diseases (NCDs) and their risk factors. Front Public Heal. (2020) 8:1–11. doi: 10.3389/fpubh.2020.574111
8. World Health Organization. Status of the health-related SDGs: Monitoring Health for the SDGs. (2017) 29–35. Available online at: http://www.who.int/gho/publications/world_health_statistics/2017/EN_WHS2017_Part2.pdf?ua=1
9. Roth GA, Johnson C, Abajobir A, Abd-Allah F, Abera SF, Abyu G, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. (2017) 70:1–25. doi: 10.1016/j.jacc.2017.04.052
10. Juma K, Juma PA, Shumba C. Non-communicable diseases and urbanization in african cities: a narrative review. In: Public Health in Developing Countries - Challenges and Opportunities. London: IntechOpen (2019). doi: 10.5772/intechopen.89507
11. Ithnin M, Nor NAUM, Nordin NJ, Effendy NM, Sahar MA, Abdullah KHA, et al. Knowledge, attitude, and practice on non-communicable diseases (NCDs) among the adult population in the urban area of Negeri Sembilan, Malaysia. Int J Res Pharm Sci. (2018) 9(Special Issue 2):88–94. doi: 10.26452/ijrps.v9iSPL2.1747
12. Islam MZ, Rahman MM, Moly MAH. Knowledge about non-communicable diseases among selected urban school students. J Armed Forces Med Coll Bangladesh. (2020) 15:90–3. doi: 10.3329/jafmc.v15i1.48654
13. Casariego E, Cebrián-Cuenca AM, Llisterri JL, Micó-Pérez RM, Orozco-Beltran D, Otero-Cacabelos M, et al. OPENCRONIC study. Knowledge and experiences of spanish patients and carers about chronic disease. Int J Environ Res Public Health. (2019) 16:1–9. doi: 10.3390/ijerph16010039
14. Rahamathulla MP, Mohemmed Sha M. Frequency and awareness of risk factors of non-communicable diseases among University students in saudi arabia. Pakistan J Med Sci. (2020) 36:740–5. doi: 10.12669/pjms.36.4.2400
15. Gamage AU, Jayawardana PL. Knowledge of non-communicable diseases and practices related to healthy lifestyles among adolescents, in state schools of a selected educational division in Sri Lanka. BMC Public Health. (2017) 18:1–9. doi: 10.1186/s12889-017-4622-z
16. Ithnin M, Nor NAUM, Juliana N, Effendy NM, Sahar MA, Abdullah KHA, et al. Knowledge, attitude and practices towards lifestyle-related non-communicable diseases (NCDs): a cross-sectional study among indigenous orang asli adults in Negeri Sembilan, Malaysia. IIUM Med J Malaysia. (2020) 19:75–82. doi: 10.31436/imjm.v19i2.1569
17. Tian M, Chen Y, Zhao R, Chen L, Chen X, Feng D, et al. Chronic disease knowledge and its determinants among chronically ill adults in rural areas of Shanxi Province in China: A cross-sectional study. BMC Public Health. 2011;11. doi: 10.1186/1471-2458-11-948
18. Thandar MM, Kiriya J, Shibanuma A, Ong KIC, Tin KN, Win HH, et al. Women's knowledge on common non-communicable diseases and nutritional need during pregnancy in three townships of Ayeyarwaddy region, Myanmar: A cross-sectional study. Trop Med Health. (2019) 47:1–10. doi: 10.1186/s41182-019-0137-x
19. Song Y, Ma W, Yi X, Wang S, Sun X, Tian J, et al. Chronic Diseases Knowledge and Related Factors among the Elderly in Jinan, China. PLoS One. (2013) 8:1–9. doi: 10.1371/journal.pone.0068599
20. Onagbiye SO, Tsolekile LP, Puoane T. Knowledge of Non-communicable Disease Risk Factors among Community Health Workers in South Africa. Open Public Health J. (2020) 13:430–7. doi: 10.2174/1874944502013010430
21. Biraguma J, Mutimura E, Frantz JM. Knowledge about modifiable risk factors for non-communicable diseases adults living with HIV in Rwanda. Afr Health Sci. (2019) 19:3181–9. doi: 10.4314/ahs.v19i4.41
23. World Health organization. Risk of premature death from the four target NCDs-Data by country [Internet]. 2021 [cited 2021 Dec 19]. Available from: https://apps.who.int/gho/data/node.main.A857
24. World Health Organization. Life expectancy and Healthy life expectancy-Data by country and WHO region [Internet]. 2020 [cited 2021 Dec 19]. Available from: https://apps.who.int/gho/data/node.main.688
25. Shiferaw F, Letebo M, Feleke Y, Gelibo T, Getachew T, Defar A, et al. Non-communicable diseases in Ethiopia: Policy and strategy GAPS in the reduction of behavioral risk factors. Ethiop J Heal Dev. (2019) 33:1–10.
26. Boateng D, Wekesah F, Browne JL, Agyemang C, Agyei-Baffour P, De-Graft Aikins A, et al. Knowledge and awareness of and perception towards cardiovascular disease risk in sub-Saharan Africa: A systematic review. PLoS One. (2017) 12:1–21. doi: 10.1371/journal.pone.0189264
27. Ministry of Health-Ethiopia. The Ethiopia Noncommunicable Diseases and Injuries (NCDI) Commission Report Summary: Addressing the Impact of Noncommunicable Diseases and Injuries in Ethiopia. 2018;(November).
28. Federal MoH-Ethiopia. Addressing the impact of Noncommunicable Diseases and Injuries in Ethiopia: Findings and recommendations from the NCDI Commission of Ethiopia. 2018;(November).
29. Samuel OO. Knowledge and Risk Factors Prevalence of Non Communicable Diseases (NCDs) in Nigeria : a case study of Adult population in Delta State. J Appl Biol Biotechnol. (2017) 5:14–20.
30. Elnaem MH, Elkalmi R. Knowledge of the risk factors of non-communicable diseases (NCDs) among pharmacy students : findings from a Malaysian University. 2019;(December). doi: 10.1080/14635240.2019.1602070
31. Sharma G. Knowledge of the risk factors of common non-communicable diseases (NCDs) amongst college students in Delhi, India. 2015;3(3):4273.
32. Al-daboony S. Knowledge, Attitude and Practices towards Noncommunicable Disease Risk Factors among Medical Staff. 2016;16(3).
33. Tabassum R, Froeschl G, Cruz JP, Colet PC, Dey S, Islam SMS. Untapped aspects of mass media campaigns for changing health behaviour towards non-communicable diseases in Bangladesh. Global Health. (2018) 14:10–3. doi: 10.1186/s12992-018-0325-1
34. Perkins JM, Lee H young, James KS, Oh J, Krishna A, Heo J, et al. Marital status, widowhood duration, gender and health outcomes: a cross-sectional study among older adults in India. BMC Public Health [Internet]. 2016;16(1):1–12. Available from: doi: 10.1186/s12889-016-3682-9
35. Schultz WM, Hayek SS, Tahhan AS, Ko YA, Sandesara P, Awad M, et al. Marital status and outcomes in patients with cardiovascular disease. J Am Heart Assoc. (2017) 6:1–10. doi: 10.1161/JAHA.117.005890
Keywords: non-communicable disease, knowledge, associated factors, adult, Ethiopia
Citation: Legesse E, Nigussie T, Girma D, Geleta LA, Dejene H, Deriba BS, Geleta TA, Sahlu D, Tesema M, Tilahun A, Awol M, Teshome F, Midaksa G and Bati F (2022) Level of Adequate Knowledge of Non-communicable Diseases and Associated Factors Among Adult Residents of North Shewa Zone, Oromia Region, Ethiopia: A Mixed-Method Approach. Front. Public Health 10:892108. doi: 10.3389/fpubh.2022.892108
Received: 08 March 2022; Accepted: 27 May 2022;
Published: 23 June 2022.
Edited by:
Melanie Boeckmann, University of Bremen, GermanyReviewed by:
João Ramalho-Santos, University of Coimbra, PortugalKrushna Chandra Sahoo, Regional Medical Research Center (ICMR), India
Copyright © 2022 Legesse, Nigussie, Girma, Geleta, Dejene, Deriba, Geleta, Sahlu, Tesema, Tilahun, Awol, Teshome, Midaksa and Bati. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Derara Girma, ZGVyYXJhZ2lybWEyNCYjeDAwMDQwO2dtYWlsLmNvbQ==
†These authors have contributed equally to this work