 Linlin Wang1†
Linlin Wang1† Xingzhao Li
Xingzhao Li Yanyan Yang
Yanyan Yang Jun Li
Jun Li- 1Department of Ultrasound, China-Japan Union Hospital of Jilin University, Changchun, China
- 2Department of Pediatrics, China-Japan Union Hospital of Jilin University, Changchun, China
- 3Department of Gastrointestinal Colorectal and Anal Surgery, China-Japan Union Hospital of Jilin University, Changchun, China
- 4Department of Hematology and Oncology, China-Japan Union Hospital of Jilin University, Changchun, China
Background: The coronavirus disease 2019 (COVID-19) pandemic has posed increasing challenges to global health systems. Vaccination against COVID-19 can effectively prevent the public, particularly healthcare workers (HCWs), from being infected by this disease.
Objectives: We aim to understand the factors influencing HCWs' acceptance of COVID-19 vaccines.
Methods: We searched PubMed, Embase and Web of Science to collect literature published before May 15, 2022, about HCWs' acceptance of COVID-19 vaccines. The Newcastle–Ottawa quality assessment scale was used to assess the risk of bias and the quality of the included studies. We utilized Stata 14.0 software for this meta-analysis with a random-effects model, and odds ratios (ORs) with 95% confidence intervals (CIs) were reported. This meta-analysis was conducted in alignment with the preferred reporting items for systematic review and meta-analysis (PRISMA) guideline.
Results: Our meta-analysis included 71 articles with 93,508 HCWs involved. The research showed that the acceptance of vaccines had significantly increased among HCWs compared to non-HCWs (OR = 1.91, 95% CI: 1.16–3.12). A willingness to undergo COVID-19 vaccination was observed in 66% (95% CI: 0.61–0.67) of HCWs. Among the HCWs involved, doctors showed a generally increased intention to be vaccinated compared with nurses (OR = 2.22, 95% CI: 1.71–2.89). Additionally, males were found to hold more positive attitudes toward vaccination than females (OR = 1.81, 95% CI: 1.55–2.12). When the effectiveness of COVID-19 vaccines was improved, the vaccination acceptance of HCWs was greatly increased accordingly (OR = 5.03, 95% CI: 2.77–9.11). The HCWs who were willing to vaccinate against seasonal influenza showed an increased acceptance of COVID-19 vaccines (OR = 3.52, 95% CI: 2.34–5.28). Our study also showed that HCWs who were willing to be vaccinated against COVID-19 experienced a reduced rate of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection (OR = 0.78, 95% CI: 0.66–0.92).
Conclusions: Our analysis revealed that the five factors of occupation, gender, vaccine effectiveness, seasonal influenza vaccines, and SARS-CoV-2 infection presumably affected the acceptance of COVID-19 vaccines among HCWs. It is essential to boost the confidence of HCWs in COVID-19 vaccines for the containment of the epidemic.
Introduction
Rationale
On March 16, 2020, the first mRNA vaccine for coronavirus disease 2019 (COVID-19) developed by Moderna entered the clinical trial stage in the United States. Subsequently, various COVID-19 vaccines, including DNA-based vaccines, have been popularized throughout the world (1). Developing safe and effective vaccines to promote large-scale vaccination is probably the most effective way for humankind to fight against COVID-19 (2).
In 2022, millions of doses of COVID-19 vaccines are now administered each day globally (3). Surprisingly, numerous people showed distrust and concerns about COVID-19 vaccines (4). A large number of studies have shown that some healthcare workers (HCWs) remain skeptical about whether to receive COVID-19 vaccination (5). In one survey, approximately one-sixth of HCWs claimed that they would not choose to be vaccinated against COVID-19 even if mandated (6). The risk of the members of HCWs infected with COVID-19 was nearly three times that of the non-HCWs (7). In some countries, approximately 10% of HCWs are infected with SARS-CoV-2 (8). The acceptance of COVID-19 vaccines among non-HCWs can be easily affected by HCWs; in particular, HCWs with a negative attitude tend not to recommend vaccines to patients (9).
Objectives
We aim, through meta-analysis, to understand the factors influencing HCWs' acceptance of vaccination against COVID-19. Our study may provide insights for promoting future immunization programs worldwide.
Materials and methods
Eligibility criteria
Studies meeting the following criteria were included in the meta-analysis: (1) the content must include the acceptance of HCWs about COVID-19 vaccines, (2) the number of HCWs who are willing and unwilling (including refusal and hesitation) to vaccinate should be recorded separately, and (3) the sample sizes of both the experimental group and the control group were more than 10.
Information from abstracts, comments, reviews, posters and case reports was excluded.
Information sources
All the literature published before May 15, 2022, about the acceptance of HCWs toward COVID-19 vaccines was searched in PubMed, Embase, and Web of Science, regardless of the language of the literature, to collect the most useful information.
Search strategy
The method of “key words” + “free words” was adopted for retrieval. Search terms were limited to the titles and abstracts. Detailed strategies are listed in Supplementary File 1.
Study selection process
Literature collected from the database was imported into NoteExpress software for filtration. After deleting duplicated literature, we first read the titles and abstracts before we eliminated irrelevant pieces. Articles that did not meet the requirements were then further screened based on the abstracts or the full text. Articles that were fairly related were adopted for subsequent data selection.
Data selection process and items
Data extraction was completed independently by two authors. When those two authors disagreed on data selection, they would debate the problem before delivering it to a third author for the final conclusion.
The following data were recorded: the number of HCWs willing and unwilling to be vaccinated against COVID-19; the number of HCWs who had been vaccinated against seasonal influenza in 2019–2020 and who preferred to be vaccinated against the same disease in 2020–2021; the number of HCWs in favor of compulsory COVID-19 vaccination; the number of doctors and nurses willing to receive COVID-19 vaccines; the number of non-HCWs willing to be vaccinated with COVID-19; the number of HCWs willing to be vaccinated with different effective rates (bounded by 70%); the gender, age, and education level of HCWs; the number of HCWs afflicted with chronic diseases; the number of HCWs who contacted closely with COVID-19 patients; and the number of people vaccinated against influenza and the number of COVID-19 cases in the two groups of HCWs who were willing and unwilling to be vaccinated against COVID-19. If an article could extract several groups of data without intersection or the data record research results under different conditions, they were represented by “-A,” “-B” or “-C.”
Study risk of bias assessment
The quality and the risk of bias of the included studies were independently assessed using the Newcastle–Ottawa quality assessment scale. A low risk of bias and high quality were considered if the overall score was equal to or above seven. The assessment was completed by one author and reviewed by another.
Reporting bias assessment
Egger's test was used for quantitative analysis. A p-value < 0.05 indicates the presence of bias.
Synthesis methods
The I2 statistic was used to quantify the heterogeneity among studies. An I2 value <50% indicated mild heterogeneity, while an I2 value ≥ 75% suggested significant heterogeneity. Moderate heterogeneity was considered if 50% ≤ I2 <75%. We conducted subgroup analysis to explore the source of heterogeneity. A random-effects model was used to estimate the effect value. Stata 14.0 software was applied for all analyses. A p-value of z test < 0.05 was considered to be statistically significant.
Effect measures and certainty assessment
In this study, the ratio and odds ratio (OR) were used for data analysis, and the confidence interval (CI) was 95%.
Results
Study selection
A total of 1,170 studies were searched in the database, of which 400 duplicated studies were deleted with NoteExpress software. According to the titles and abstracts, 578 articles irrelevant to this study were eliminated. Of the remaining 192 papers, 121 were excluded after further screening, including comments, reviews, case reports, and papers with insufficient data. Seventy-one articles were finalized for inclusion in our meta-analysis. The flow diagram of the study selection is shown in Figure 1.
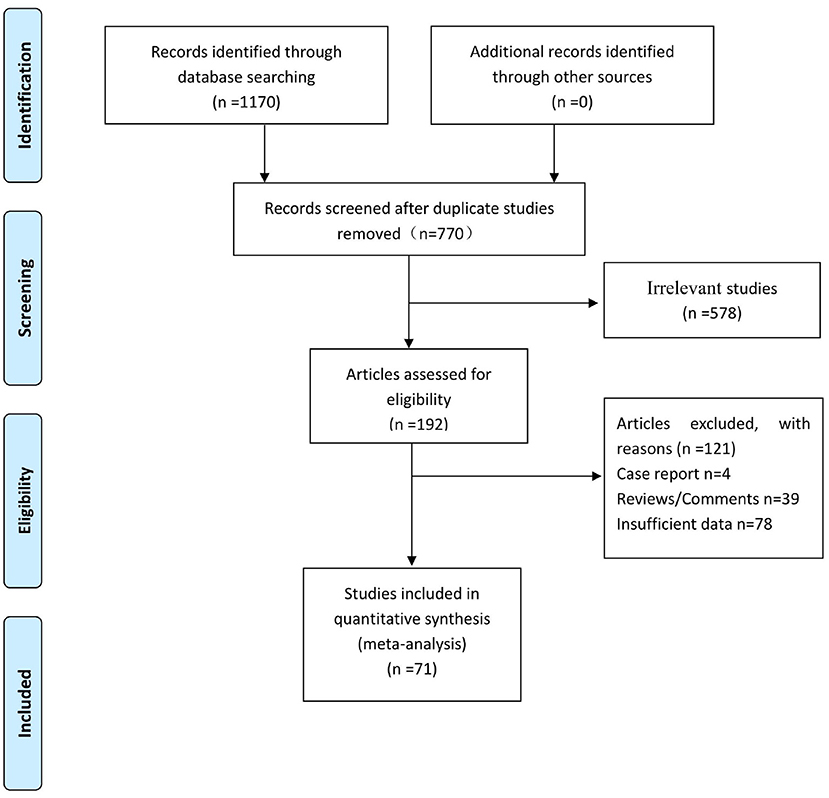
Figure 1. Flow diagram of study selection.
Study characteristics
The HCWs in our study came from various occupations, including doctors, nurses, paramedics, medical teachers, and students. The whole sample we extracted from the literature included 75,345 HCWs and 13,513 non-HCWs, covering 40 countries and regions.
Risk of bias in studies
All the studies included in the Newcastle–Ottawa quality assessment scale indicated a fairly low risk of bias and high quality (Supplementary Table 1).
Results of individual studies
The results of individual studies are presented in structured tables. The information of HCWs and non-HCWs is listed in Table 1. Among HCWS, information on people's willingness to receive COVID-19 vaccines is shown in Table 2.
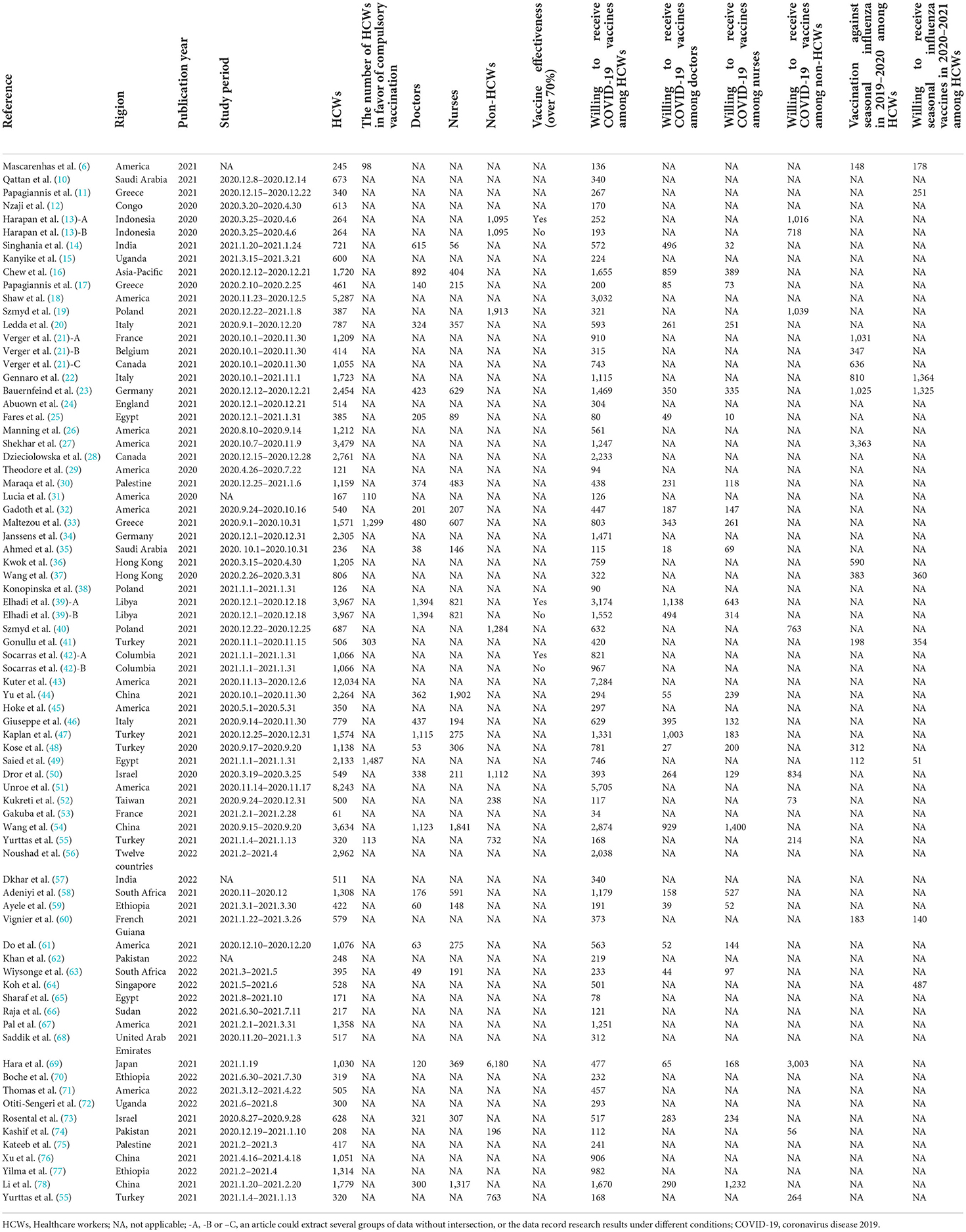
Table 1. The characteristics of HCWs and non-HCWs.
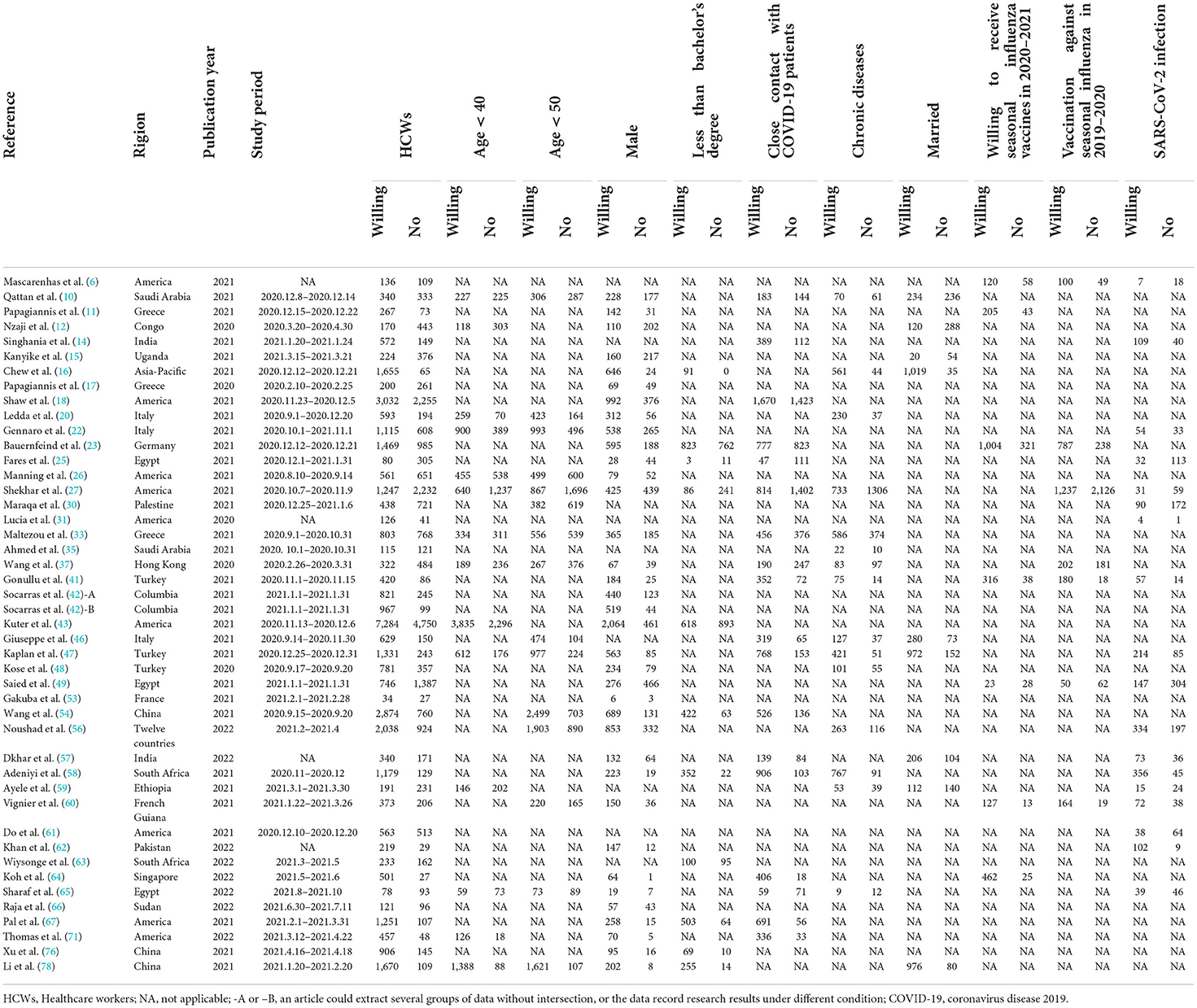
Table 2. The characteristics of HCWs who are willing and unwilling to receive coronavirus disease 2019 vaccines.
Reporting biases
We used Egger's test for reporting bias analysis (Supplementary File 2). The study of the acceptance of HCWs with different education levels about COVID-19 vaccines showed a slight bias (p = 0.049), while other results carried no significant bias.
Certainty of evidence and results of syntheses
We considered the continent where the study was conducted as the basis of subgroup division and explored the source of heterogeneity through subgroup analysis (Figures 2–10). We found that the heterogeneity in some subgroups remained high.
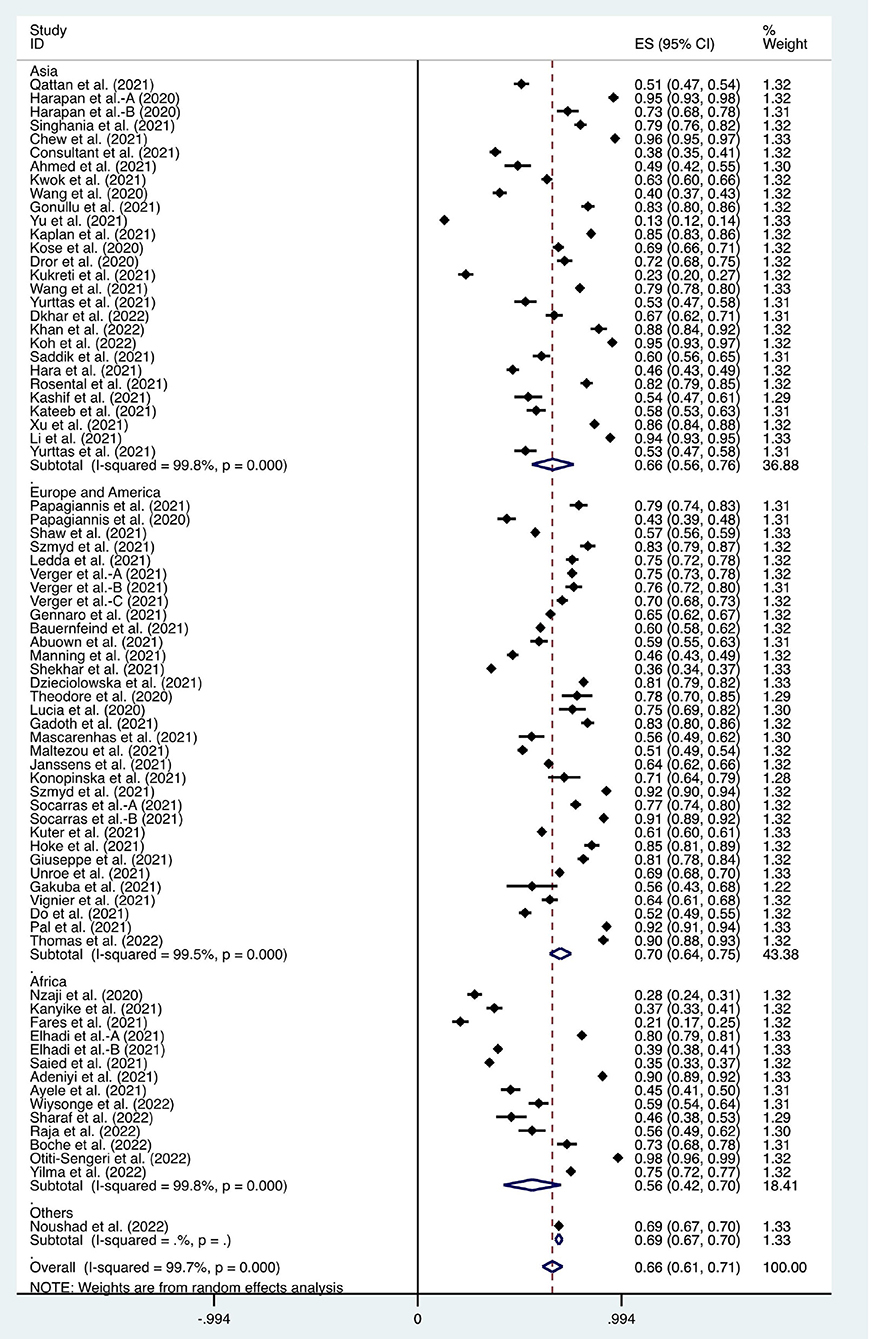
Figure 2. Forest plot of the acceptance of coronavirus disease 2019 vaccines by healthcare workers.
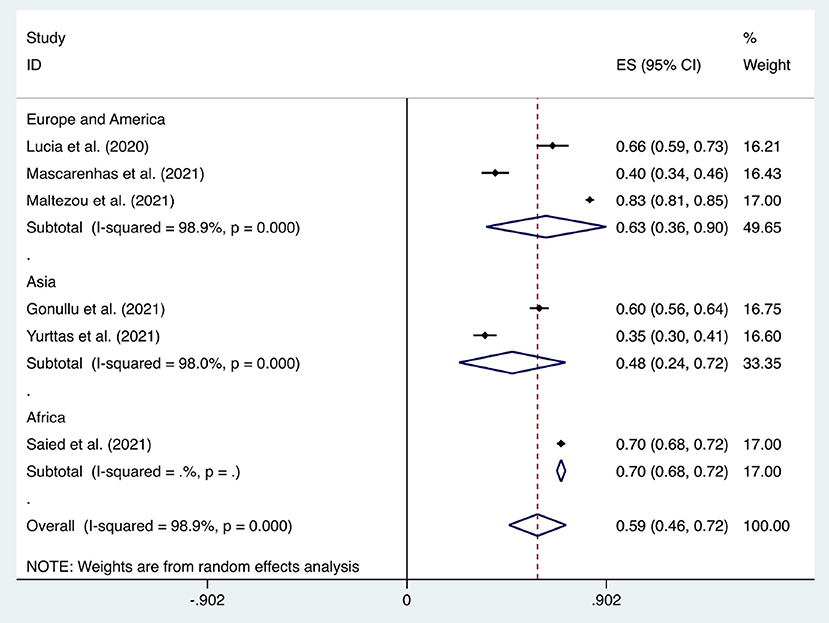
Figure 3. Forest plot of the acceptance of healthcare workers of compulsory vaccination.
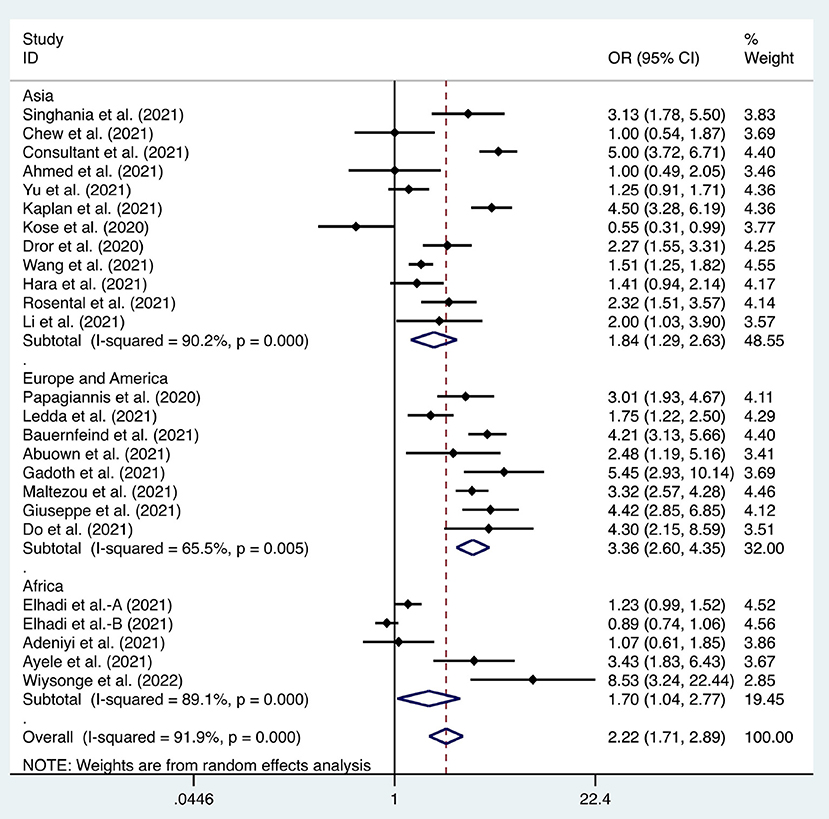
Figure 4. Forest plot of the difference in the willingness between doctors and nurses to receive coronavirus disease 2019 vaccines.
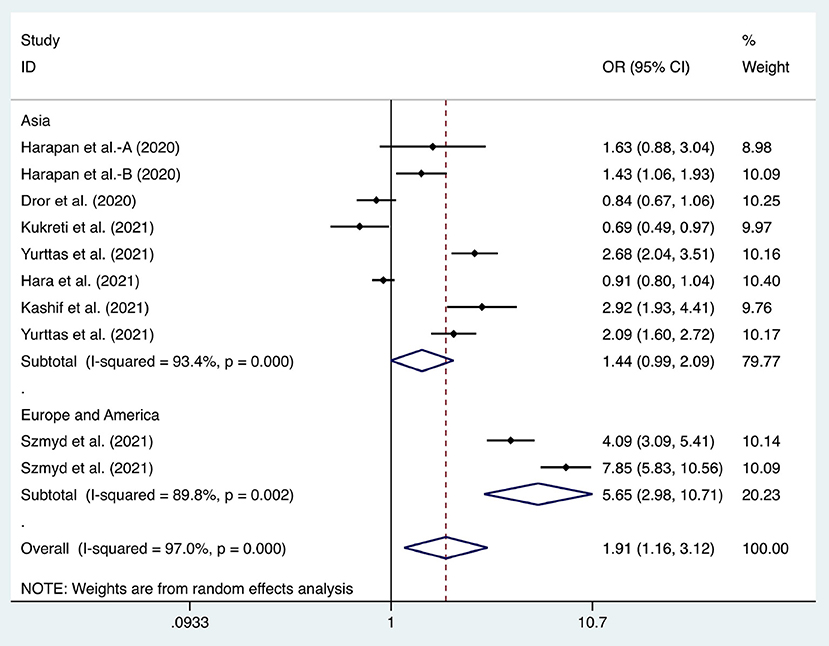
Figure 5. Forest plot of the willingness of healthcare workers (HCWs) and non-HCWs to receive coronavirus disease 2019 vaccines.
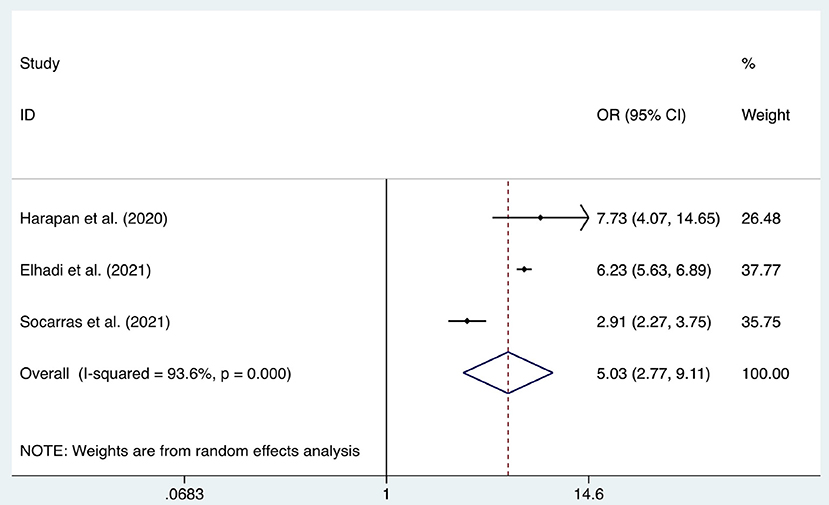
Figure 6. Forest plot of the acceptance of healthcare workers of coronavirus disease 2019 vaccines with different effectiveness (bounded by 70%).
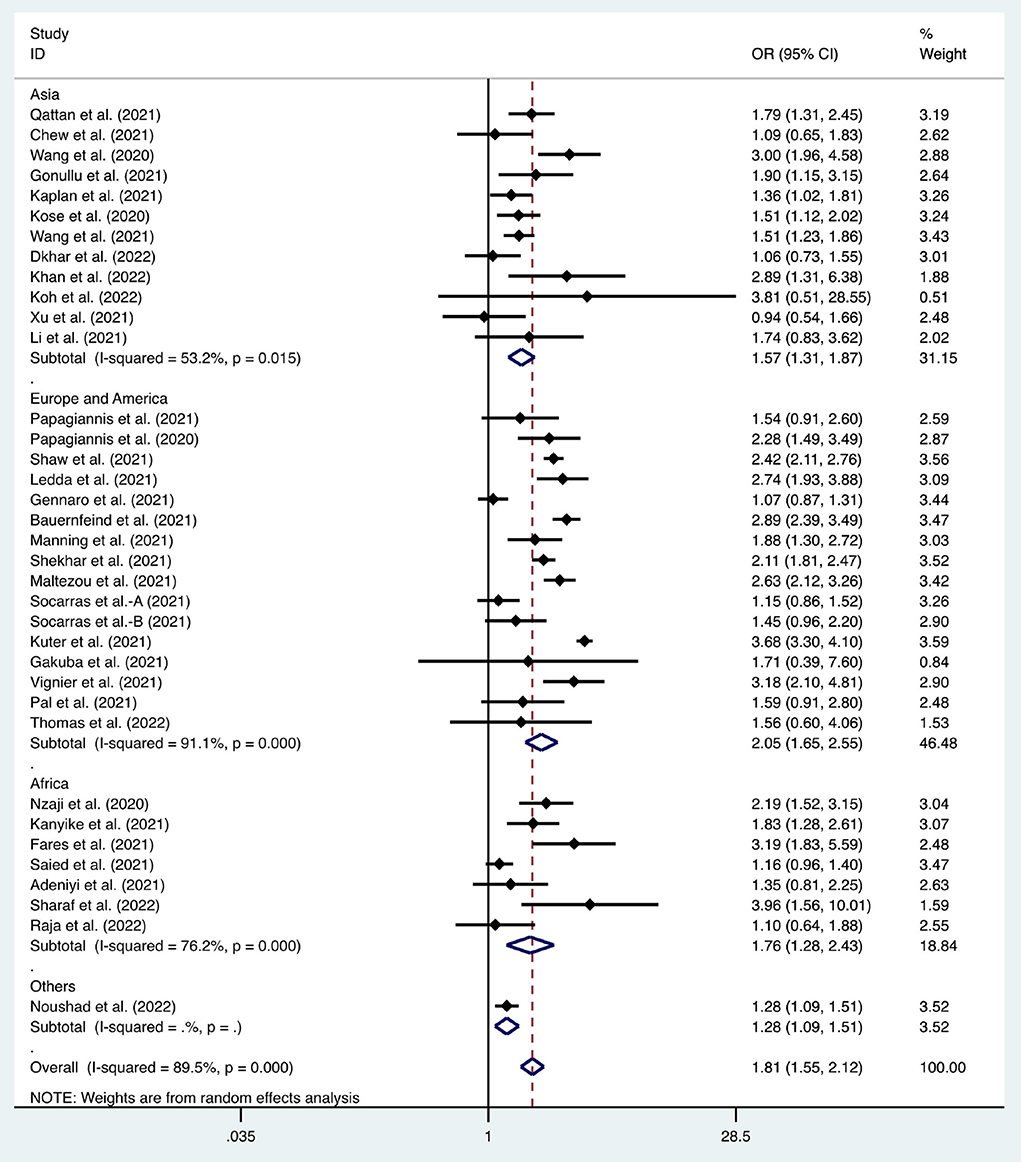
Figure 7. Forest plot of the effect of gender on the willingness of healthcare workers to receive coronavirus disease 2019 vaccines.
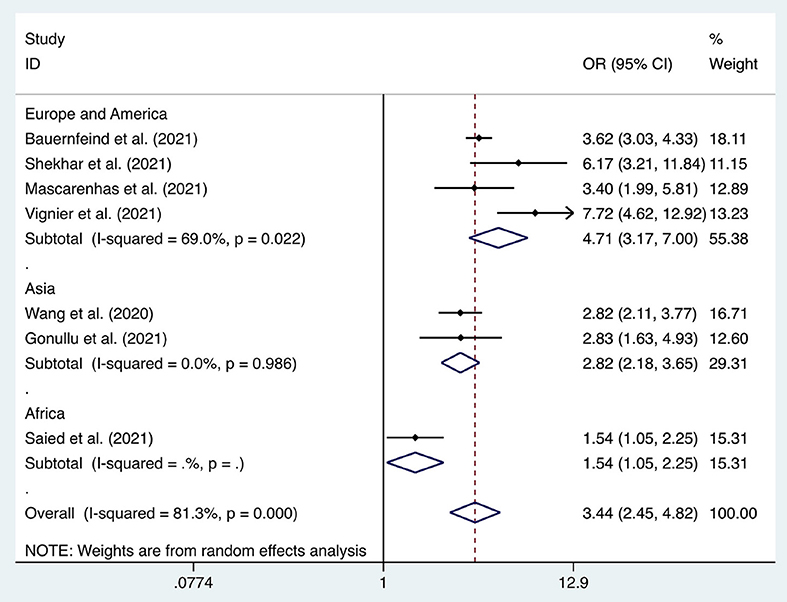
Figure 8. Forest plot of the acceptance of seasonal influenza vaccines by healthcare workers (2019–2020).
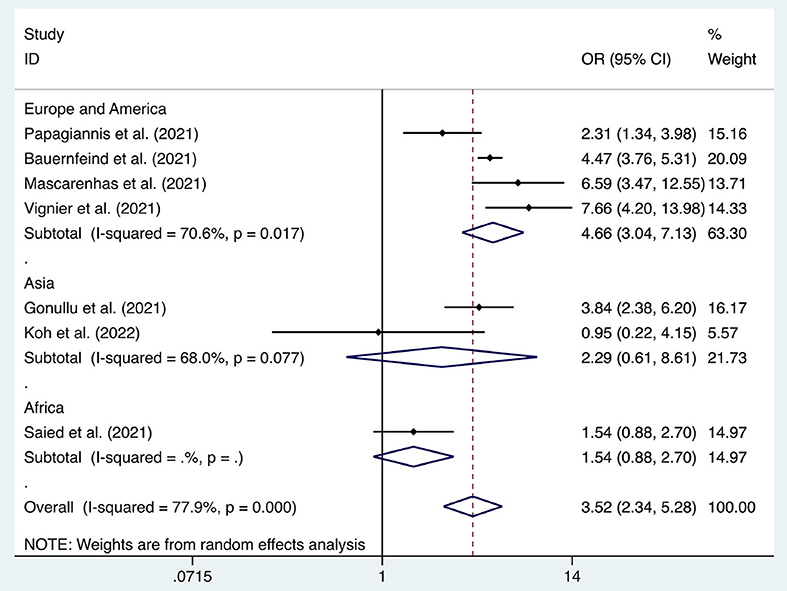
Figure 9. Forest plot of the acceptance of seasonal influenza vaccines by healthcare workers (2020–2021).
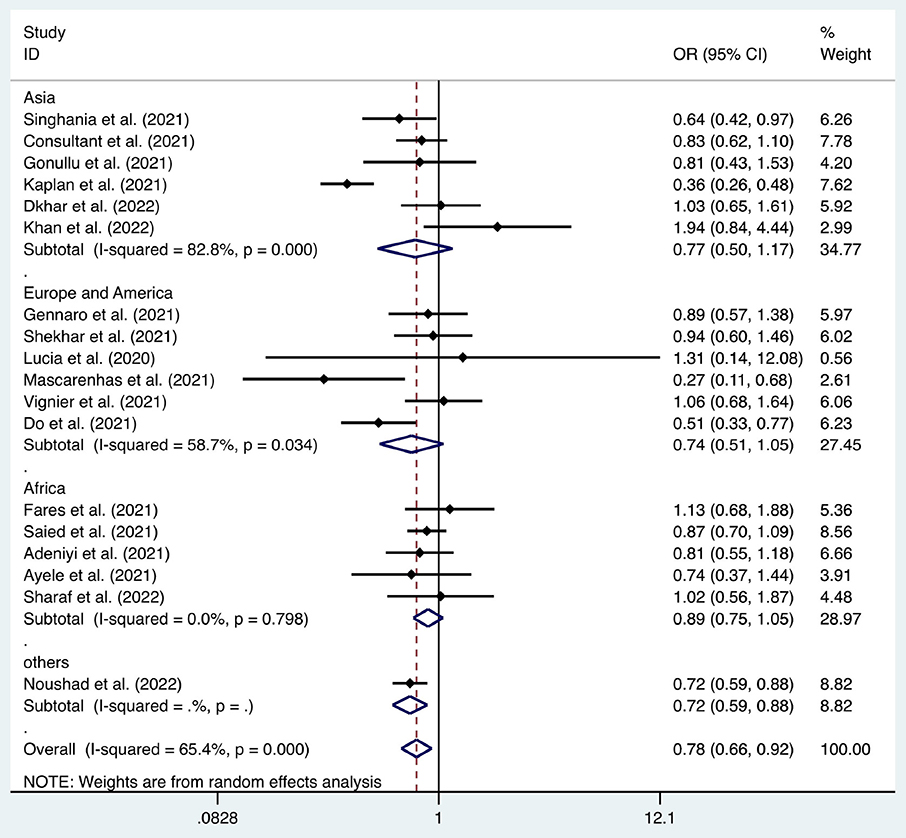
Figure 10. Forest plot of the relationship between healthcare workers' acceptance of the coronavirus disease 2019 vaccination and the infection rate of severe acute respiratory syndrome coronavirus 2.
Seventy-one articles were used to study the acceptance of HCWs about COVID-19 vaccines, which showed that a willingness to undergo COVID-19 vaccination was observed in 66% (95% CI: 0.61–0.67, I2 = 99.7%, Figure 2) of HCWs. A recent study showed that up to 98% of HCWs in Uganda were willing to be vaccinated against COVID-19 (72). However, through subgroup analysis, we found that only 56% (95% CI: 0.42–0.70, I2 = 99.8%, Figure 2) of HCWs in African countries were willing to receive COVID-19 vaccination, which was lower than that in Asian (ratio = 0.66, 95% CI: 0.56–0.76, I2 = 99.8%, Figure 2) and European & American countries (ratio = 0.70, 95% CI: 0.64–0.75, I2 = 99.5%, Figure 2).
Six articles were used to study the acceptance of HCWs about compulsory vaccination, showing that the proportion of HCWs who agreed with this was 59% (95% CI: 0.46–0.72, I2 = 98.9%,s Figure 3). We analyzed 24 articles to examine the variance in willingness to take the COVID-19 vaccine between doctors and nurses, and the results indicated that doctors showed a higher willingness to receive COVID-19 vaccination than nurses (OR = 2.22, 95% CI: 1.71–2.89, I2 = 91.9%, p < 0.001, Figure 4). Nine articles were studied to compare the willingness of HCWs and non-HCWs to receive COVID-19 vaccination, and it was found that the willingness of HCWs was greatly increased compared to that of non-HCWs (OR = 1.91, 95% CI: 1.16–3.12, I2 = 97.0%, p = 0.01, Figure 5). Additionally, by analyzing three other articles, we found that with an increased effectiveness of the vaccines in preventing COVID-19 (bounded by 70%), the willingness of HCWs to receive the vaccination also rose accordingly (OR = 5.03, 95% CI: 2.77–9.11, I2 = 93.6%, p < 0.001, Figure 6). The research revealed that male members of HCWs showed a higher willingness to be vaccinated (OR = 1.81, 95% CI: 1.55–2.12, I2 = 89.5%, p < 0.001, Figure 7). The HCWs with a higher acceptance of COVID-19 vaccines were more inclined to receive seasonal influenza vaccines in 2019–2020 (OR = 3.44, 95% CI: 2.45–4.82, I2 = 81.3%, p < 0.001, Figure 8) and 2020–2021 (OR = 3.52, 95% CI: 2.34–5.28, I2 = 77.9%, p < 0.001, Figure 9). Furthermore, the rate of SARS-CoV-2 infection among HCWs willing to be vaccinated was significantly lower than that among HCWs who showed hesitancy (OR = 0.78, 95% CI: 0.66–0.92, I2 = 65.4%, p < 0.001, Figure 10).
Nine articles were used to study the differences between the willingness of HCWs to receive COVID-19 vaccination and the 2020–2021 seasonal influenza vaccines (OR = 1.71, 95% CI: 0.83–3.52, I2 = 98.9%, p = 0.145, Supplementary Figure 1). Seven articles were used to study the impact of the COVID-19 epidemic on seasonal influenza vaccination (2019–2020 and 2020–2021) (OR = 1.43, 95% CI: 0.81–2.53, I2 = 98.2%, p = 0.214, Supplementary Figure 2), and no significant difference was observed in either study.
Some studies have shown that elderly HCWs are more willing to be inoculated with COVID-19 vaccines (20, 28, 51). Nevertheless, a study from Zhejiang Province, China, showed that a large number of HCWs aged over 50 years experienced SARS in 2003, influenza A (H1N1) in 2009 and avian influenza A (H7N9) in 2013. With the exception of H1N1, the other two were well contained without introducing vaccination, so some people would inevitably assume that vaccination against COVID-19 was probably not necessary (54). Married HCWs were remarkably more willing to be vaccinated for the protection of their families (47). However, a study from Uganda came to the opposite conclusion. Their study revealed that single HCWs showed a higher acceptance of COVID-19 vaccines (15). To solve similar contradictions, we compared the characteristics of HCWs from two groups, one with HCWs who were willing to be inoculated with COVID-19 vaccines and another with those who were not. The results showed that age [(OR = 0.91, 95% CI: 0.75–1.12, I2 = 89.3%, p = 0.145, Supplementary Figure 3) and (OR = 0.85, 95% CI: 0.63–1.14, I2 = 90.1%, p = 0.288, Supplementary Figure 4)], education level (OR = 0.81, 95% CI: 0.54–1.22, I2 = 94.2%, p = 0.315, Supplementary Figure 5), marriage status (OR = 0.96, 95% CI: 0.75–1.23, I2 = 71.9%, p = 0.758, Supplementary Figure 6), close contact with COVID-19 patients (OR = 1.01, 95% CI: 0.77–1.32, I2 = 94.1%, p = 0.959, Supplementary Figure 7), and chronic diseases (OR = 1.19, 95% CI: 0.90–1.59, I2 = 90.6%, p = 0.222, Supplementary Figure 8) did not significantly affect the acceptance of COVID-19 vaccines by HCWs. The factors associated with COVID-19 vaccine acceptance of HCWs are listed in Table 3.
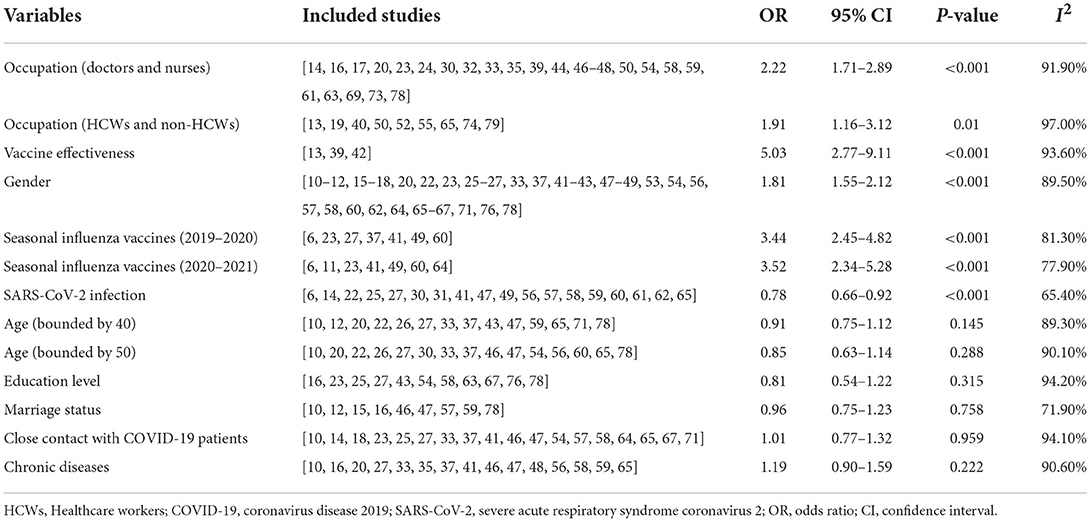
Table 3. The factors associated with COVID-19 vaccine acceptance of HCWs.
Discussion
The vaccine is metaphorically known as the “seatbelt against the disease,” which can effectively protect people against infectious diseases at the lowest cost (79). In improving public health, vaccination functions as one of the most important advances. It successfully promoted the elimination of smallpox worldwide and the control of numerous infectious diseases (e.g., rubella, diphtheria, polio) (80). It is estimated that approximately two to three million deaths can be avoided each year by vaccination (81). Despite this, public distrust of vaccines is widespread. The most typical example is the boycott of polio vaccination in northern Nigeria in 2003–2004 (82). Frontline HCWs are frequently and closely exposed to highly contagious patients with COVID-19, posing them at highly increased risk of infection and transmission. Therefore, they became the primary concern of authorities around the world when they formulated COVID-19 vaccination policies (19). Our research showed that approximately 66% of HCWs were willing to receive COVID-19 vaccines, which might vary among different regions. A report showed that only 21% of HCWs in Egypt held a positive attitude toward COVID-19 vaccines (25). A survey on the Asia Pacific region showed that the acceptance of COVID-19 vaccines by HCWs in six countries, including China and India, approached nearly 96% (16). Since a compulsory vaccination program can effectively increase the overall vaccination coverage rate (83), we considered the views of HCWs on this measure, and the results showed that approximately 59% of HCWs agreed with it. We additionally studied the impact of the COVID-19 epidemic on vaccination against seasonal influenza and the association between the two. The prior experience gained from seasonal influenza vaccination provides a reference and guidance for COVID-19 vaccination. It was noticed that the COVID-19 epidemic did not significantly affect the seasonal influenza vaccination of HCWs; however, interestingly, HCWs who showed a stronger intention to vaccinate against COVID-19 were more likely to receive seasonal influenza vaccination. The experience of influenza vaccination has been known as one of the drivers of accepting COVID-19 vaccines (84). It was also discovered that when the effectiveness of the vaccines changed, the acceptance of the vaccines by HCWs varied accordingly. In our meta-analysis, HCWs demonstrated a higher acceptance of COVID-19 vaccines than non-HCWs. Even in HCWs, the acceptance of COVID-19 vaccines varied among individuals with different occupations. In particular, doctors showed significantly higher acceptance of COVID-19 vaccines than nurses.
It was comparatively found that males were more willing to be vaccinated against COVID-19 than females among HCWs. The higher willingness of males to receive COVID-19 vaccination could be attributed to social and cultural differences and males' risk-taking tendency (85). Some reports indicated that males were at a higher risk of experiencing COVID-19 complications, infections, and even deaths (86). Our study showed that HCWs willing to be vaccinated against COVID-19 experienced a lower risk of infection, probably owing to a high level of protection awareness among them.
The HCWs who remained skeptical about vaccination against COVID-19 were mainly concerned about the efficacy and safety of the vaccines due to the short duration of vaccine development (18, 22, 25, 33). The rapid spread of misleading information about COVID-19 vaccines on various media platforms has aggravated HCWs' doubts about them (10). Since the acceptance of HCWs directly affects the trust of non-HCWs in COVID-19 vaccines, it is necessary to boost their confidence.
Limitations
The data were collected from various countries and regions in the world. Due to the different severities of the outbreak, various prevention and control measures, and cultural and cognitive differences, the heterogeneity of our results was generally high.
People's intention to vaccinate against COVID-19 will change with the epidemic situation (37). Even in the same region, there will be certain variations in the statistical data at different periods.
Conclusions
Our research revealed that a considerable percentage of HCWs remained skeptical about COVID-19 vaccines. Five factors: occupation, gender, vaccine effectiveness, seasonal influenza vaccines, and SARS-CoV-2 infection; significantly affected the willingness of HCWs to be vaccinated against COVID-19. Herein, it is essential to boost the confidence of HCWs in COVID-19 vaccines for the containment of the epidemic.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
Project administration and data curation: JL. Writing-original draft preparation: LW and YW. Writing-review and editing: XC and XL. Software: YY. All authors read and approved the final manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.881903/full#supplementary-material
References
1. Lurie N, Saville M, Hatchett R, Halton J. Developing Covid-19 vaccines at pandemic speed. N Engl J Med. (2020) 382:1969–73. doi: 10.1056/NEJMp2005630
2. Omer SB, Yildirim I, Forman HP. Herd immunity and implications for SARS-CoV-2 control. JAMA. (2020) 324:2095–6. doi: 10.1001/jama.2020.20892
3. Coronavirus, (COVID-19) Vaccinations,. https://ourworldindata.org/covid-vaccinations (accessed May 15, 2022).
4. Vergara RJD, Sarmiento PJD, Lagman JDN. Building public trust: a response to COVID-19 vaccine. J Public Health. (2021) 43:e291–2. doi: 10.1093/pubmed/fdaa282
5. Verger P, Fressard L, Collange F, Gautier A, Jestin C, Launay O, et al. Vaccine hesitancy among general practitioners and its determinants during controversies: a national cross-sectional survey in France. EBioMedicine. (2015) 2:891–7. doi: 10.1016/j.ebiom.2015.06.018
6. Mascarenhas AK, Lucia VC, Kelekar Afonso NM. Dental students' attitudes and hesitancy toward COVID-19. J Dent Educ. (2021) 85:1504–1510. doi: 10.1002/jdd.12632
7. Nguyen LH, Drew DA, Joshi AD, Joshi AD, Guo CG, Ma W, et al. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health. (2020) 5:e475–83. doi: 10.1016/S2468-2667(20)30164-X
8. Centers for Disease Control Prevention. Coronavirus. Available online at: https://www.cdc.gov/coronavirus/about/index.html (accessed March 29, 2020).
9. Arda B, Durusoy R, Yamazhan T, Sipahi OR, Taşbakan M, Pullukçu H, et al. Did the pandemic have an impact on influenza vaccination attitude? a survey among health care workers. BMC Infect Dis. (2011) 11:87. doi: 10.1186/1471-2334-11-87
10. Qattan AMN, Alshareef N, Alsharqi O, Rahahleh NA, Chirwa GC, Al-Hanawi MK. Acceptability of a COVID-19 vaccine among healthcare workers in the kingdom of Saudi Arabia. Front Med. (2021) 8:644300. doi: 10.3389/fmed.2021.644300
11. Papagiannis D, Rachiotis G, Malli F, Papathanasiou IV, Kotsiou O, Fradelos EC, et al. Acceptability of COVID-19 vaccination among greek health professionals. Vaccines. (2021) 9:200. doi: 10.3390/vaccines9030200
12. Nzaji MK, Ngombe LK, Mwamba GN, Ndala DBB, Miema JM, Lungoyo CL, et al. Acceptability of vaccination against COVID-19 among healthcare workers in the democratic republic of the congo. Pragmat Obs Res. (2020) 11:103–9. doi: 10.2147/POR.S271096
13. Harapan H, Wagner AL, Yufika A, Winardi W, Anwar S, Gan AK, et al. Acceptance of a COVID-19 vaccine in southeast asia: a cross-sectional study in Indonesia. Front Public Health. (2020) 8:381. doi: 10.3389/fpubh.2020.00381
14. Singhania N, Kathiravan S, Pannu AK. Acceptance of coronavirus disease 2019 vaccine among health-care personnel in India: a cross-sectional survey during the initial phase of vaccination. Clin Microbiol Infect. (2021) 27:1064–6. doi: 10.1016/j.cmi.2021.03.008
15. Kanyike AM, Olum R, Kajjimu J, Ojilong D, Akech GM, Nassozi DR, et al. Acceptance of the coronavirus disease-2019 vaccine among medical students in Uganda. Trop Med Health. (2021) 49:37. doi: 10.1186/s41182-021-00331-1
16. Chew NWS, Cheong C, Kong G, Phua K, Ngiam JN, Tan BYQ, et al. An Asia-Pacific study on healthcare workers' perceptions of, and willingness to receive, the COVID-19 vaccination. Int J Infect Dis. (2021) 106:52–60. doi: 10.1016/j.ijid.2021.03.069
17. Papagiannis D, Malli F, Raptis DG, Papathanasiou IV, Fradelos EC, Daniil Z, et al. Assessment of knowledge, attitudes, and practices towards new coronavirus (SARS-CoV-2) of health care professionals in Greece before the outbreak period. Int J Environ Res Public Healt. (2020) 17:4925. doi: 10.3390/ijerph17144925
18. Shaw J, Stewart T, Anderson KB, Hanley S, Thomas SJ, Salmon DA, et al. Assessment of U.S. health care personnel (HCP) attitudes towards COVID-19 vaccination in a large university health care system. Clin Infect Dis. (2021) 73:1776–83. doi: 10.1093/cid/ciab054
19. Szmyd B, Karuga FF, Bartoszek A, Staniecka K, Radek M. Attitude and behaviors towards SARS-CoV-2 vaccination among healthcare workers: a cross-sectional study from Poland. Vaccines. (2021) 9:218. doi: 10.3390/vaccines9030218
20. Ledda C, Costantino C, Cuccia M, Maltezou HC, Rapisarda V. Attitudes of healthcare personnel towards vaccinations before and during the COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:2703. doi: 10.3390/ijerph18052703
21. Verger P, Scronias D, Dauby N, Adedzi KA, Gobert C, Bergeat M, et al. Attitudes of healthcare workers towards COVID-19 vaccination: a survey in France and French-speaking parts of Belgium and Canada, 2020. Euro Surveill. (2021) 26:2002047. doi: 10.2807/1560-7917.ES.2021.26.3.2002047
22. Gennaro FD, Murri R, Murri FV, Cerruti L, Abdulle A, Saracino A, et al. Attitudes towards Anti-SARS-CoV2 vaccination among healthcare workers: results from a national survey in Italy. Viruses. (2021) 13:371. doi: 10.3390/v13030371
23. Bauernfeind S, Hitzenbichler F, Huppertz G, Zeman F, Koller M, Schmidt B, et al. Brief report: attitudes towards Covid-19 vaccination among hospital employees in a tertiary care university hospital in Germany in December 2020. Infection. (2021) 49:1307–11. doi: 10.1007/s15010-021-01622-9
24. Abuown A, Ellis T, Miller J, Davidson R, Kachwala Q, Medeiros M, et al. COVID-19 vaccination intent among London healthcare workers. Occup Med. (2021) 71:211–4. doi: 10.1093/occmed/kqab057
25. Fares S, Elmnyer MM, Mohamed SS, Elsayed R. COVID-19 vaccination perception and attitude among healthcare workers in Egypt. J Prim Care Community Health. (2021) 12:1–9. doi: 10.1177/21501327211013303
26. Manning ML, Gerolamo AM, Marino MA, Hanson-Zalot ME, Pogorzelska-Maziarz M. COVID-19 vaccination readiness among nurse faculty and student nurses. Nurs Outlook. (2021) 69:565–73. doi: 10.1016/j.outlook.2021.01.019
27. Shekhar R, Sheikh AB, Upadhyay S, Singh M, Kottewar S, Mir H, et al. COVID-19 vaccine acceptance among health care workers in the United States. Vaccines. (2021) 9:119. doi: 10.3390/vaccines9020119
28. Dzieciolowska S, Hamel D, Gadio S, Dionne M, Gagnon D, Robitaille L, et al. Covid-19 vaccine acceptance, hesitancy and refusal among canadian healthcare workers: a multicenter survey. Am J Infect Control. (2021) 49:1152–7. doi: 10.1016/j.ajic.2021.04.079
29. Theodore DA, Castor D, Sovic B, Castellon M, De A, Gray B, et al. COVID-19 vaccine attitudes among healthcare workers in New York City: preliminary findings from the antibody response monitoring for occupational resilience (ARMOR) study. J Int AIDS Soc. (2021) 24:106. doi: 10.1002/jia2.25659
30. Maraqa B, Nazzal Z, Rabi R, Sarhan N, Al-Shakhra K, Al-Shakhra M, et al. COVID-19 vaccine hesitancy among health care workers in palestine: a call for action. Prev Med. (2021) 149:106618. doi: 10.1016/j.ypmed.2021.106618
31. Lucia VC, Kelekar A, Afonso NM. COVID-19 vaccine hesitancy among medical students. J Public Health. (2020) 43:445–9. doi: 10.1093/pubmed/fdaa230
32. Gadoth A, Halbrook M, Blais RM, Gray A, Tobin NH, Ferbas KG, et al. Cross-sectional assessment of COVID-19 vaccine acceptance among health care workers in Los Angeles. Ann Intern Med. (2021) 174:882–5. doi: 10.7326/M20-7580
33. Maltezou HC, Pavli A, Dedoukou X, Georgakopoulou T, Raftopoulos V, Drositis I, et al. Determinants of intention to get vaccinated against COVID-19 among healthcare personnel in hospitals in Greece. Infect Dis Health. (2021) 26:189–97. doi: 10.1016/j.idh.2021.03.002
34. Janssens U, Kluge S, Marx G, Hermes C, Salzberger B, Karagiannidis C. Einstellung zur impfung gegen SARS-CoV-2 umfrage unter mitarbeitenden in krankenhäusern vor und nach beginn der impfungenindendeutschen krankenhäusern. Med Klin Intensivmed Notfmed. (2021) 116:421–30. doi: 10.1007/s00063-021-00821-4
35. Ahmed G, Almoosa Z, Mohamed D, Rapal J, Minguez O, Khurma IA, et al. Healthcare provider attitudes toward the newly developed COVID-19 vaccine: cross-sectional study. Nurs Rep. (2021) 11:187–94. doi: 10.3390/nursrep11010018
36. Kwok KO Li KK, Wei WI, Tang A, Wong SYS, Lee SS, et al. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: a survey. Int J Nurs Stud. (2021) 114:103854. doi: 10.1016/j.ijnurstu.2020.103854
37. Wang K, Wong ELY, Ho KF, Cheung AWL, Chan EYY, Yeoh EK, et al. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: a cross-sectional survey. Vaccine. (2020) 38:7049–56. doi: 10.1016/j.vaccine.2020.09.021
38. Konopińska J, Obuchowska I, Lisowski L, Dub N, Kozera M, Rekas M, et al. Intention to get COVID-19 vaccinations among ophthalmology residents in Poland: a cross-sectional survey. Vaccines. (2021) 9:371. doi: 10.3390/vaccines9040371
39. Elhadi M, Alsoufi A, Alhadi A, Hmeida A, Alshareea E, Dokali M, et al. Knowledge, attitude, and acceptance of healthcare workers and the public regarding the COVID-19 vaccine: a cross-sectional study. BMC Public Health. (2021) 21:955. doi: 10.1186/s12889-021-10987-3
40. Szmyd B, Bartoszek A, Karuga FF, Staniecka K, Błaszczyk M, Radek M. Medical students and SARS-CoV-2 vaccination: attitude and behaviors. Vaccines. (2021) 9:128. doi: 10.3390/vaccines9020128
41. Gonullu E, Soysal A, Atici S, Engin M, Yeşilbaş O, Kasap T, et al. Pediatricians' COVID-19 experiences and views on the willingness to receive COVID-19 vaccines: a cross-sectional survey in Turkey. Hum Vaccin Immunother. (2021) 17:2389–96. doi: 10.1080/21645515.2021.1896319
42. Socarras JLA, Varela ALV, Lesmes DCQ, Fama-Pereira MM, Serrano-Diaz NC, Vasco M, et al. Perception of COVID-19 vaccination amongst physicians in Colombia. Vaccines. (2021) 9:287. doi: 10.3390/vaccines9030287
43. Kuter BJ, Browne S, Momplaisir FM, Feemster KA, Shen AK, McKenzie JG, et al. Perspectives on the receipt of a COVID-19 vaccine: a survey of employees in two large hospitals in Philadelphia. Vaccine. (2021) 39:1693–700. doi: 10.1016/j.vaccine.2021.02.029
44. Yu Y, Lau JTF, She R, Chen X, Li L, Li L, et al. Prevalence and associated factors of intention of COVID-19 vaccination among healthcare workers in China: application of the health belief model. Hum Vaccin Immunother. (2021) 17:2894–902. doi: 10.1080/21645515.2021.1909327
45. Hoke AM, Keller CM, Calo WA, Sekhar DL, Lehman EB, Kraschnewski JL. School Nurse Perspectives on COVID-19. J Sch Nurs. (2021) 37:2–297. doi: 10.1177/1059840521992054
46. Giuseppe GD, Pelullo CP, Polla GD, Montemurro MV, Napolitano F, Pavia M, et al. Surveying willingness towards SARS-CoV-2 vaccination of healthcare workers in Italy. Expert Rev Vaccines. (2021) 20:881–9. doi: 10.1080/14760584.2021.1922081
47. Kaplan AK, Sahin MK, Parildar H, Guvenc IA. The willingness to accept the COVID-19 vaccine and affecting factors among healthcare professionals: a cross-sectional study in Turkey. Int J Clin Pract. (2021) 75:e14226. doi: 10.1111/ijcp.14226
48. Kose S, Mandiracioglu A, Sahin S, Kaynar T, Karbus O, Ozbel Y. Vaccine hesitancy of the COVID-19 by health care personnel. Int J Clin Pract. (2020) 75:e13917. doi: 10.1111/ijcp.13917
49. Saied SM, Saied EM, Kabbash IA, Abdo SAE. Vaccine hesitancy: beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J Med Virol. (2021) 93:4280–91. doi: 10.1002/jmv.26910
50. Dror AA, Eisenbach N, Taiber S, Morozov NG, Mizrachi M, Zigron A, et al. Vaccine hesitancy: the next challenge in the fight against COVID-19. Eur J Epidemiol. (2020) 35:775–9. doi: 10.1007/s10654-020-00671-y
51. Unroe KT, Evans R, Weaver L, Rusyniak D, Blackburn J, et al. Willingness of long-term care staff to receive a COVID-19 vaccine: a single state survey. J Am Geriatr Soc. (2021) 69:593–9. doi: 10.1111/jgs.17022
52. Kukreti S, Lu MY, Lin YH, Strong C, Lin CY, Ko NY, et al. Willingness of Taiwan's healthcare workers and outpatients to vaccinate against COVID-19 during a period without community outbreaks. Vaccines. (2021) 9:246. doi: 10.3390/vaccines9030246
53. Gakuba C, Sar A, Gaborieau I, Hanouz JL, Verger P. Willingness to get a COVID-19 vaccine among critical care non-medical healthcare workers and impact of a vaccine information session. Anaesth Crit Care Pain Med. (2021) 40:100860. doi: 10.1016/j.accpm.2021.100860
54. Wang J, Feng Y, Hou Z, Lu Y, Chen H, Ouyang L, et al. Willingness to receive SARS-CoV-2 vaccine among healthcare workers in public institutions of Zhejiang Province, China. Hum Vaccin Immunother. (2021) 17:2926–33. doi: 10.1080/21645515.2021.1909328
55. Yurttas B, Poyraz BC, Sut N, Ozdede A, Oztas M, Ugurlu S, et al. Willingness to get the COVID-19 vaccine among patients with rheumatic diseases, healthcare workers and general population in Turkey: a web-based survey. Rheumatol Int. (2021) 41:1105–14. doi: 10.1007/s00296-021-04841-3
56. Noushad M, Rastam S, Nassani MZ, Al-Saqqaf IS, Hussain M, Yaroko AA, et al. A global survey of COVID-19 vaccine acceptance among healthcare workers. Front Public Health. (2022) 9:794673. doi: 10.3389/fpubh.2021.794673
57. Dkhar SA, Jeelani A, Quansar R, Khan SMS. Acceptance of COVID-19 vaccine among healthcare workers before the launch of vaccine in India: an online survey. J Educ Health Promot. (2022) 11:76. doi: 10.4103/jehp.jehp_383_21
58. Adeniyi OV, Stead D, Singata-Madliki M, Batting J, Wright M, Jelliman E, et al. Acceptance of COVID-19 vaccine among the healthcare workers in the eastern cape, south africa: a cross sectional study. Vaccines. (2021) 9:666. doi: 10.3390/vaccines9060666
59. Ayele AD, Ayenew NT, Tenaw LA, Kassa BG, Yehuala ED, Aychew EW, et al. Acceptance of COVID-19 vaccine and associated factors among health professionals working in hospitals of south gondar zone, Northwest Ethiopia. Hum Vaccin Immunother. (2021) 17:4925–33. doi: 10.1080/21645515.2021.2013082
60. Vignier N, Brureau K, Granier S, Breton J, Michaud C, Gaillet M, et al. Attitudes towards the COVID-19 vaccine and willingness to get vaccinated among healthcare workers in french guiana: the influence of geographical origin. Vaccines. (2021) 9:682. doi: 10.3390/vaccines9060682
61. Do TVC, Kammili ST, Reep M, Wisnieski L, Ganti SS, Depa J. COVID-19 vaccine acceptance among rural appalachian healthcare workers (Eastern Kentucky/West Virginia): a cross-sectional study. Cureus. (2021) 13:e16842. doi: 10.7759/cureus.16842
62. Khan S, Uddin A, Imran M, Ali Y, Khan S, Salman Khan M, et al. COVID-19 vaccine acceptance and hesitancy among health care workers (Hcws) in two major urban centers in khyber-pakhtunkhwa, Pakistan. Asia Pac J Public Health. (2022) 34:580–2. doi: 10.1177/10105395221083382
63. Wiysonge CS, Alobwede SM, Katoto PMC, Kidzeru EB, Lumngwena EN, Cooper S, et al. COVID-19 vaccine acceptance and hesitancy among healthcare workers in South Africa. Expert Rev Vaccines. (2022) 21:549–59. doi: 10.1080/14760584.2022.2023355
64. Koh SWC, Liow Y, Loh VWK, Liew SJ, Chan YH, Young D. COVID-19 vaccine acceptance and hesitancy among primary healthcare workers in Singapore. BMC Prim Care. (2022) 23:81. doi: 10.1186/s12875-022-01693-z
65. Sharaf M, Taqa O, Mousa H, Badran A. COVID-19 vaccine acceptance and perceptions among dental teaching staff of a governmental university in Egypt. J Egypt Public Health Assoc. (2022) 97:9. doi: 10.1186/s42506-022-00104-6
66. Raja SM, Osman ME, Musa AO, Hussien AA, Yusuf K. COVID-19 vaccine acceptance, hesitancy, and associated factors among medical students in Sudan. PLoS ONE. (2022) 17:e0266670. doi: 10.1371/journal.pone.0266670
67. Pal S, Shekhar R, Kottewar S, Upadhyay S, Singh M, Pathak D, et al. COVID-19 vaccine hesitancy and attitude toward booster doses among Us healthcare workers. Vaccines. (2021) 9:1358. doi: 10.3390/vaccines9111358
68. Saddik B, Al-Bluwi N, Shukla A, Barqawi H, Alsayed HAH, Sharif-Askari NS, et al. Determinants of healthcare workers perceptions, acceptance and choice of COVID-19 vaccines: a cross-sectional study from the United Arab Emirates. Hum Vaccin Immunother. (2022) 18:1–9. doi: 10.1080/21645515.2021.1994300
69. Hara M, Ishibashi M, Nakane A, Nakano T, Hirota Y. Differences in COVID-19 vaccine acceptance, hesitancy, and confidence between healthcare workers and the general population in Japan. Vaccines. (2021) 9:1389. doi: 10.3390/vaccines9121389
70. Boche B, Kebede O, Damessa M, Gudeta T, Wakjira D. Health professionals' COVID-19 vaccine acceptance and associated factors in tertiary hospitals of south-west Ethiopia: a multi-center cross- sectional study. Inquiry. (2022) 59:469580221083181. doi: 10.1177/00469580221083181
71. Thomas CM, Searle K, Galvan A, Liebman AK, Mann EM, Kirsch JD, et al. Healthcare worker perspectives on COVID-19 vaccines: Implications for increasing vaccine acceptance among healthcare workers and patients. Vaccine. (2022) 40:2612–8. doi: 10.1016/j.vaccine.2022.03.011
72. Otiti-Sengeri J, Andrew OB, Lusobya RC, Atukunda I, Nalukenge C, Kalinaki A, et al. High COVID-19 vaccine acceptance among eye healthcare workers in Uganda. Vaccines. (2022) 10:609. doi: 10.3390/vaccines10040609
73. Rosental H, Shmueli L. Integrating health behavior theories to predict COVID-19 vaccine acceptance: differences between medical students and nursing students. Vaccines. (2021) 9:783. doi: 10.3390/vaccines9070783
74. Kashif M, Fatima I, Ahmed AM, Ali SA, Memon RS, Afzal M, et al. Perception, willingness, barriers, and hesitancy towards COVID-19 vaccine in Pakistan: comparison between healthcare workers and general population. Cureus. (2021) 13:e19106. doi: 10.7759/cureus.19106
75. Kateeb E, Danadneh M, Pokorna A, Klugarova J, Abdulqader H, Klugar M, et al. Predictors of willingness to receive COVID-19 vaccine: cross-sectional study of Palestinian dental students. Vaccines. (2021) 9:954. doi: 10.3390/vaccines9090954
76. Xu B, Gao X, Zhang X, Hu Y, Yang H, Zhou YH. Real-world acceptance of COVID-19 vaccines among healthcare workers in perinatal medicine in China. Vaccines. (2021) 9:704. doi: 10.3390/vaccines9070704
77. Yilma D, Mohammed R, Abdela SG, Enbiale W, Seifu F, Pareyn M, et al. COVID-19 vaccine acceptability among healthcare workers in Ethiopia: do we practice what we preach? Trop Med Int Health. (2022) 27:418–25. doi: 10.1111/tmi.13742
78. Li XH, Chen L, Pan QN, Liu J, Zhang X, Yi JJ, et al. Vaccination status, acceptance, and knowledge toward a COVID-19 vaccine among healthcare workers: a cross-sectional survey in China. Hum Vaccin Immunother. (2021) 17:4065–73. doi: 10.1080/21645515.2021.1957415 s
79. Giubilini A, Savulescu J. Vaccination, risks, and freedom: the seat belt analogy. Public Health Ethics. (2019) 12:237–49. doi: 10.1093/phe/phz014
80. Dubé E. Addressing vaccine hesitancy: the crucial role of healthcare providers. Clin Microbiol Infect. (2017) 23:279–80. doi: 10.1016/j.cmi.2016.11.007
81. Immunization WHO. Available online at: http://www.who.int/topics/immunization/en/ (accessed December 29, 2020).
82. Ghinai I, Willott C, Dadari I. Listening to the rumours: what the northern Nigeria polio vaccine boycott can tell us ten years on. Glob Public Health. (2013) 8:1138–50. doi: 10.1080/17441692.2013.859720
83. Schumacher S, García JS, Cornely OA, Mellinghoff SC. Increasing influenza vaccination coverage in healthcare workers: a review on campaign strategies and their effect. Infection. (2021) 49:387–99. doi: 10.1007/s15010-020-01555-9
84. Hassan L, Kazmi SK, Tahir MJ, Ullah I, Royan HA, Fahriani M, et al. Global acceptance and hesitancy of COVID-19 vaccination: a narrative review. Narra J. (2021) 1:e57. doi: 10.52225/narra.v1i3.57
85. Friedl A, Pondorfer A, Schmidt U. Gender differences in social risk taking. J Econ Psychol. (2020) 77:102182. doi: 10.1016/j.joep.2019.06.005
Keywords: COVID-19, vaccines, meta-analysis, seasonal influenza, healthcare workers
Citation: Wang L, Wang Y, Cheng X, Li X, Yang Y and Li J (2022) Acceptance of coronavirus disease 2019 (COVID-19) vaccines among healthcare workers: A meta-analysis. Front. Public Health 10:881903. doi: 10.3389/fpubh.2022.881903
Received: 23 February 2022; Accepted: 24 August 2022;
Published: 16 September 2022.
Edited by:
Khan Sharun, Indian Veterinary Research Institute (IVRI), IndiaReviewed by:
Abanoub Riad, Masaryk University, CzechiaSameh Attia, Justus-Liebig University Giessen Department of Oral and Maxillofacial Surgery, Germany
Cheryl Cameron, Case Western Reserve University, United States
Copyright © 2022 Wang, Wang, Cheng, Li, Yang and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jun Li, bGp1bjAxQGpsdS5lZHUuY24=
†These authors have contributed equally to this work and share first authorship